Incidence and costs of cardiac device infections: retrospective analysis using German health claims data
Abstract
Aim: Estimate incidence and costs of cardiac device infections (CDIs) in Germany. Materials & methods: Patients had an implantable cardioverter defibrillator implanted over 2010–2013 and were followed to December 2014 using German health insurance claims data. A case-controlled analysis was performed using propensity score matching methods. Results: Risk of CDI 12 months post-implant was 3.4% overall, either 2.9% for de novo procedures versus 4.4% for replacement procedures. Mean 3-year incremental expenditure per patient for patients with CDI compared with controls was €31,493 for de novo implant patients and €33,777 for replacement patients. Mean incremental expenditure was €59,419 per patient with a major infection. Conclusion: CDIs are highly expensive to manage, reinforcing the need for strategies to reduce their occurrence.
Implantable cardioverter defibrillator (ICD) therapy and cardiac resynchronization therapy (CRT) are increasingly used, with implant rates per million that increased over the period 2011–2015 from 112 to 131 for ICDs (17% increase) and from 81 to 103 for CRT (CRT-pacemaker [CRT-P] and CRT-defibrillator [CRT-D]) devices (27% increase) in the European country members of the European Society of Cardiology [1]. These devices are recommended for selected patients in guidelines from specialty medical societies and health technology assessment agencies [2–4]. There is an extensive body of evidence that demonstrates benefits including prolonged survival, improved quality of life and cost–effectiveness.
Implantation of cardiac devices carries a risk of adverse events. These are classifiable as access-related (e.g., pneumothorax, hemothorax and hematoma), lead-related (e.g., perforation, displacement, fracture and endocarditis), generator-related (e.g., generator failure, migration and erosion) and pocket infection. Complete removal of all hardware is recommended in medical society guidelines and other scientific documents for patients with established cardiac device-related infection (CDI), and this includes cases in which a localized pocket infection occurs in the absence of signs of systemic infection, due to high relapse rates observed with retained hardware [5–7]. On the other hand, cardiac implantable electronic device (CIED) removal is not required for superficial or incisional infection at the pocket site if there is no involvement of the device.
A large randomized controlled trial (DANISH study) recently reported an infection rate of 4.9% in a cohort of 556 ICD/CRT-D patients over a median follow-up of 5.6 years [8]. Serious device infections occurred in 2.7% of patients, defined as requiring lead extraction or lifelong antibiotic treatment or causing death. Worryingly, the number of CDI cases has been increasing: national healthcare data for the USA reported the number of hospitalizations due to CDI rose from 5308 in the year 2003 to 9948 in 2011 [9]. The increase is attributed to multiple factors including increased use of CRT devices (which have three leads and a higher risk of infection), patients with more comorbidities and increased life expectancy of patients leading to more device replacement procedures.
CDI can be deadly, while treating CDI is complex and expensive. For all device types, hospital inpatient mortality is reported to be significantly higher following device procedures complicated by device infection, versus those without infection [10]. Studies also have recently reported elevated long-term mortality following CDI. A USA study based on Medicare inpatient admissions data found that 1-year mortality was between 26.5 and 35.1% depending on device type, an increment compared with patients without CDI of 8.7–15.2% [10]. A European study observed that 1-year mortality for CDI cases was 16.9%, with risk of mortality more than doubled compared with patients who did not experience CDI (hazard ratio: 2.4), with multivariate analysis to control for potential confounding factors [11].
European data on resource use and costs associated with CDI are sparse. In the USA, incremental healthcare expenditures for patients with CDI within 12 months of implant are estimated at €44,099 ($47,885) for initially implanted patients and €41,913 ($45,512) for replacement patients [12]. Notably, these costs included large proportions of all implanted patients (38.4% of initial and 47.2% of replacement cohorts) with superficial infections treated out-of-hospital and without device-related intervention.
The purpose of this study was to estimate the incidence and incremental healthcare expenditures for patients receiving ICD and CRT-D therapies who experience a CDI during the first year after their device implantation.
Methods
Setting & data source
The analysis was based on anonymized billing data collected from German statutory health insurances (SHIs). The database used for this analysis comprised 2.8 million people, 3.5% of the nationwide population. It was adjusted with regard to age, sex and morbidity distribution so that it was representative of the German SHI population. In Germany, health claims are submitted by healthcare providers working for the SHI. These billing data include the ICD-10-GM (German modification of International Classification of Diseases) codes for the classification of diseases, the German version of the International Classification of Procedures in Medicine codes (OPS), the German diagnosis related group codes for inpatient billing, as well as the German national drug codes (ATC codes) for outpatient drugs prescribed. The data on costs were the amounts reimbursed by SHIs to healthcare providers (known in the USA as payment), thus using payment data gives the cost analysis the perspective of the SHI. Using these data is in accordance with the methods for health economic evaluations in Germany [13]. Average costs are presented for six different categories: inpatient care (hospitalization), outpatient care, prescribed pharmaceuticals (outpatient setting), sick pay (payment of a percentage of a regular salary when someone is unable to work), remedies and medical aids (such as massages, shoe inserts, walkers) and total costs. Inpatient care costs are based on German diagnosis related groups, which provide lump sum reimbursement payments to hospitals for whole inpatient episodes of care.
Study design
The objectives were to estimate the incidence of CDI in patients implanted with ICD or CRT-D devices and report associated healthcare payer costs. Patients eligible for inclusion had an ICD or CRT-D implant in the 4-year period 2010–2013 and all were followed up to 31 December 2014. At least 12 months’ continuous enrollment was required before the implant index visit.
A before-and-after analysis was completed for patients with CDI to characterize resource use and costs 12 months before and after CDI, with subjects acting as their own controls. The date of CDI served as the index date for this analysis. Second, a case-controlled analysis was performed to estimate incremental costs for patients with and without a CDI, using a propensity score matching (PSM) methodology. The date of CIED implant served as the index date for this analysis. Data were extracted for 12 months prior to implant with minimum and maximum follow-up postimplant of 12–36 months. Information on patient baseline characteristics, comorbidities, severity of infection and treatment pathways were analyzed.
Study populations
Eligible patients had a record of an initial ICD/CRT-D implant or replacement (full system implant or generator only) during the calendar years 2010–2013 (list of implant procedure codes in Supplementary Table 1). CIED patients were classified in two mutually exclusive groups according to German OPS procedure codes: de novo implant or replacement implant.
For patients undergoing de novo implant, infections were counted if they occurred on the same day (outpatient) or during the same hospital stay of the device implantation or within 365 days thereafter.
For the replacement cohort, it was not possible to discern from hospital episode codes regarding a single hospital stay whether a patient underwent a replacement procedure in response to a CIED infection or if their infection arose within the same stay as a device replacement procedure. It was assumed that if an infection code was present for an index device replacement stay, the replacement was the result of an infection that initiated before the replacement visit. Hence for the device replacement cohort, infections were only counted if they occurred after the index device replacement stay.
Definition of cardiac implantable electronic device infection
CDI was defined by two conditions occurring ≤365 days after initial or replacement implant:
A device infection was coded (ICD-10-GM T82.7, infection and inflammatory reaction due to other cardiac and vascular devices, implants and grafts); or
A less specific infection diagnosis code was used (see list of other infection diagnosis codes in Supplementary Table 1) in combination with a CIED-related procedure code for removal or revision of a device during the same hospital stay.
Once identified as a patient with a CDI, patients were retrospectively classified as having either a minor or major infection as follows:
Minor: without a device procedure within 8 weeks after documented infection
Major: with a device-related procedure within 8 weeks, with or without a re-implantation
The 8-week threshold was selected based on clinical practice.
A second method to discriminate severity of infection was to classify CDI patients into those treated in an ambulatory setting only (no hospital admission related to infection) versus those with a hospital admission.
Statistics
Three types of statistical tests were employed. T-tests were used for calculating differences in means. Fisher's exact test was used for analysis of contingency tables, such as share of male patients in the CDI group compared with the group without CDI. Binomial tests were used for dichotomous data: for instance, 95% CIs for major and minor infections were calculated using a binomial test.
Mortality or switching of health insurance provider can reduce the size of patient cohorts over the course of 3-year follow-up in an SHI healthcare claims database. We calculated mean per patient costs based on cumulative costs per cohort divided by the starting size of each cohort.
Data were stored and analyzed using Microsoft Office Excel® 2010 (Microsoft Corporation, WA, USA) and SAS® (Version 9.2; SAS Institute Inc., NC, USA).
In order to estimate incremental costs associated with a CDI, patients with an infection were matched to similar patients who did not experience an infection using PSM techniques, which balanced potential confounding variables between the two groups [14]. The matching technique used was a kernel matching with an Epanechnikov function [15]. Kernel matching is a nonparametric matching estimator that uses weighted averages of all individuals in the control group (CG) to construct the counterfactual outcome. Using a weighted average instead of matching individual patients generally results in a lower variance. Weights depend on the distance between each individual from the CG [16]. Paired patients have their index event in the same year and the same duration of follow-up. The defined covariates for the matching have been set as follows: age, sex, de novo or replacement implantation, ambulatory or in-hospital implantation and the following costs measured over the 12-month period prior to device implant: mean outpatient costs, inpatient costs and sick pay.
Results
Rate of cardiac implantable electronic device infection
Patients who had a record of an ICD or CRT-D implant or generator replacement during the period 2009–2013 numbered 4699 (3233 de novo and 1466 replacement). There were 158 CDIs in the 12 months after implantation, an annual risk of 3.4% (95% CI: 2.8–3.9%). The risk differed for de novo and replacement implants: 2.9% (95% CI: 2.2–3.3%) for de novo and 4.4% (95% CI: 3.6–5.8%) for replacements (p < 0.01), see Table 1).
| Cardiac implantable electronic device infection rate | Overall | De novo | Replacement | Significance |
|---|---|---|---|---|
| ICD/CRT-D implants | 4699 | 3233 | 1466 | |
| Infections | 158 (3.4%) | 93 (2.9%) | 65 (4.4%) | p < 0.01 |
| 95% CI | 2.8–3.9% | 2.2–3.3% | 3.6–5.8% | |
| Severity class | Major | Minor | ||
| Major infection | 68 (43.0%) | 90 (57.0%) | ||
| 95% CI | 34.9–50.8% | 49.2–65.3% | ||
| Treatment setting | Hospitalized | Ambulatory | ||
| Hospitalized infection | 95 (60.1%) | 63 (39.9%) | ||
| 95% CI | 51.2–67.2% | 32.8–48.8% |
CRT-D: Cardiac resynchronization therapy-defibrillator; ICD: Implantable cardioverter defibrillator.
Split by definitions of severity, 57.0% (95% CI: 49.2–65.3%) were minor infections and 43.0% (95% CI: 34.7–50.8%) were major infections. CDIs were treated with ambulatory care only in 40% (95% CI: 32.8–48.8%) of cases and in a hospital inpatient setting in 60% (95% CI: 51.2–67.2%) of cases. Considering infection severity and treatment setting in combination, 70% of all minor infections were treated in the ambulatory sector and 30% were treated in the inpatient sector; whereas all major infections were treated in hospital.
Before-and-after observational analysis (prior to propensity score matching)
Patients who experienced a CDI, compared with those who did not (prior to PSM), had significantly higher rates of several known risk factors for CDI: kidney disease, having malignancies or being immunocompromised or taking oral anticoagulant drugs (Supplementary Table 2).
With patients acting as their own controls, costs were €15,822 higher per patient in the 12 months after infection (all severities) than the 12 months before after exclusion of the cost of index device implantation: 29,195 versus €13,373 (p < 0.05; Figure 1). The higher cost was driven by hospital inpatient care (98%).
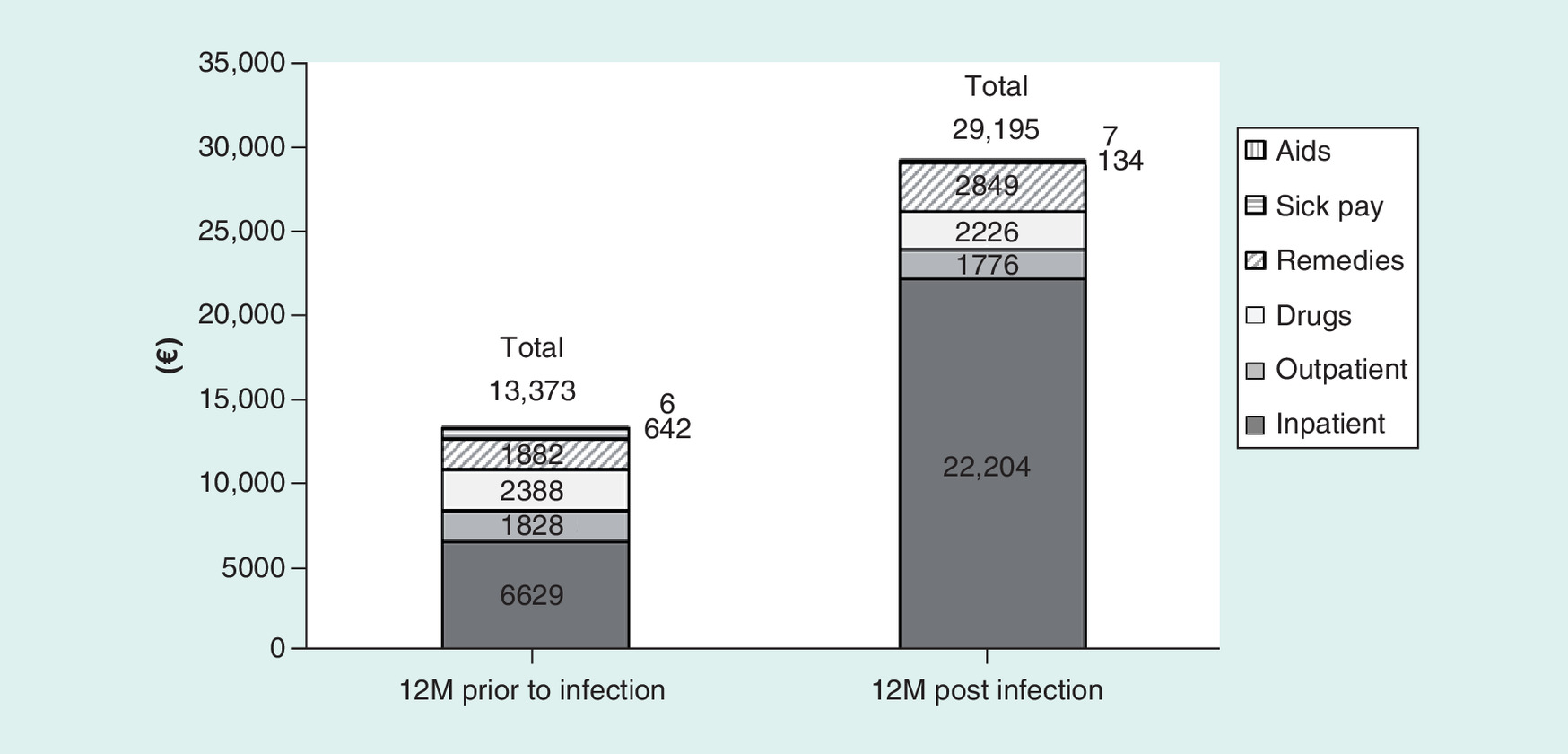
Figure 1. Average cost per patient, 12 months before and after infection.
Initial implant costs excluded from 12 months prior to infection.
Case-controlled analysis
PSM created infection groups (IGs) and CGs of equal size (146 patients each); 12 patients with CDI were unable to be matched to controls. Characteristics of the two matched groups were well balanced (Supplementary Table 2).
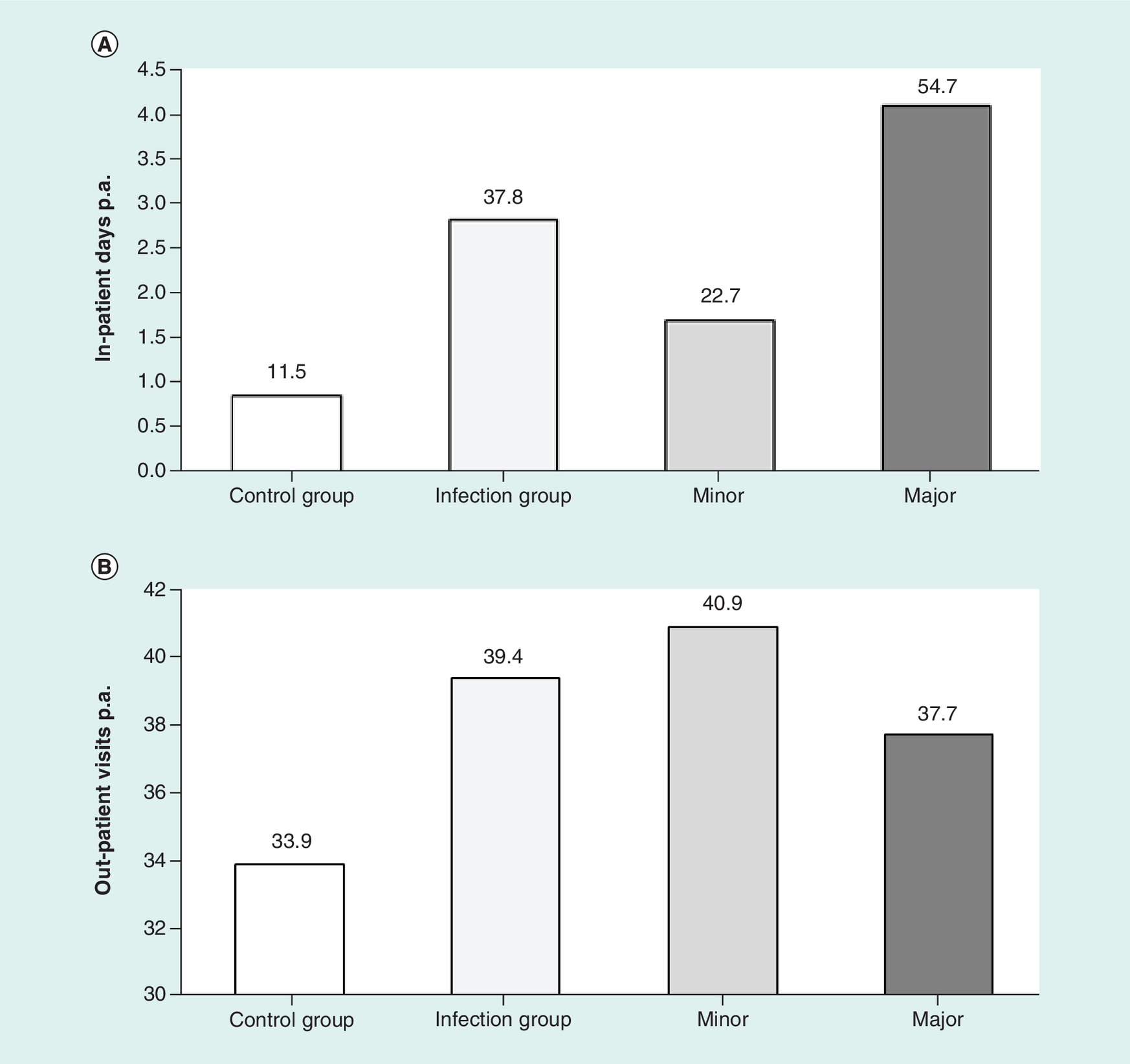
Estimated rates of healthcare utilization were greater in the 12 months following implantation for those with an infection compared with matched controls (Figure 2):
2.9 (IG) compared with 1.2 (CG) hospital inpatient stays (p < 0.01).
3.8 hospital inpatient stays for patients with major infections, compared with 2.0 stays for minor infections (p < 0.01).
37.8 (IG) versus 11.5 hospital inpatient days (CG) (p < 0.01).
54.7 inpatient days for patients with major infections, compared with 22.7 days in hospital for minor infections (p < 0.01).
39.4 (IG) versus 33.9 outpatient visits (CG) (p = 0.03).
Estimated 3 year incremental healthcare expenditures (from date of implantation) for patients with an infection (IG) of any severity, compared with the CG patients without an infection, were €31,493 (p < 0.01) for de novo implant patients and €33,777 (p < 0.01) for replacement patients (Figure 3). The index date for this analysis was the implantation rather than the infection, thus if a patient had a CDI identified 11 months postimplant (for example), the costs associated with management of the infection spill-over into year 2; 81–84% of the difference in 3-year cumulative expenditure occurred within the 2-year period.
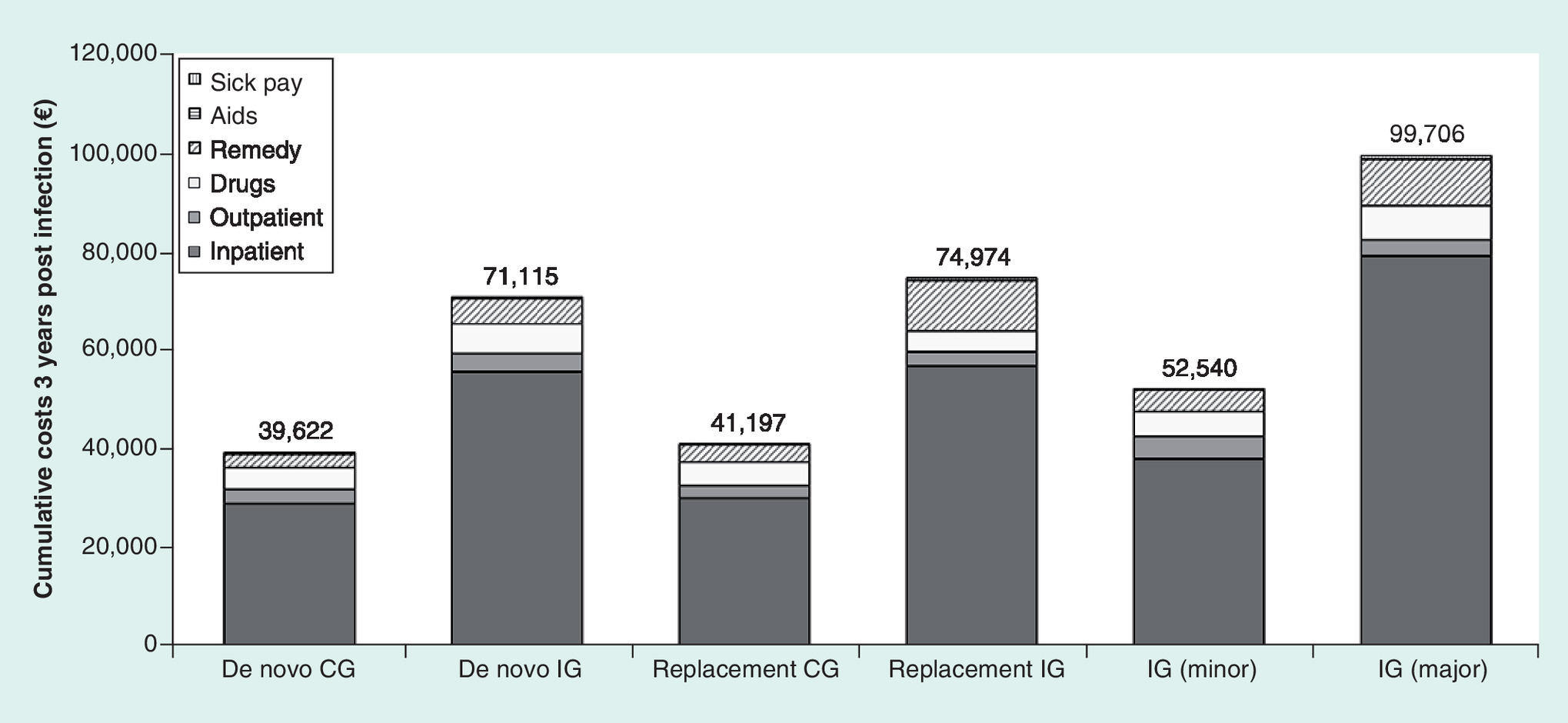
Figure 3. Average cumulative 3-year cost per patient infection group and control group.
CG: Control group; IG: Infection group.
Cumulative costs per patient were higher for patients with a major infection (€99,706; CI: €81,632–117,780), than for patients with a minor infection (€52,540; 95% CI: €40,706–64,373) (p < 0.01). Incremental expenditures by infection severity compared with controls were €12,249 for minor infections and €59,419 for major infections.
Discussion
This retrospective analysis of 4699 patients implanted with ICD and CRT-D devices using German health claims data found an overall rate of CDI of 3.4% in the first 12 months after implantation. The rate was higher for replacement as opposed to de novo implants (4.4 vs 2.9%), as reported in previous studies [12,17].
Assessed for severity, 57% were considered minor infections defined as without a device procedure within 8 weeks after documented infection. Similar rates of nonremoval of devices were observed in a recent study of CDIs also using health insurance claims data [12]. These are high rates of conservative management, given the recommendations from medical societies in favor of complete device system removal due to increased mortality in case of nonremoval [5–7]. It would be valuable to further investigate health outcomes in these patients, which was beyond the scope of this claims data analysis. Only 40% of CDIs were treated with ambulatory care only, which may suggest a potential to reduce expenditures in the treatment of minor infections, provided that appropriate treatment is provided according to guidelines and without delay.
Two approaches were used to estimate the costs of a CDI: a before-and-after analysis and a case-controlled analysis. Before-and-after analyses may be subject to ‘regression to the mean’ bias; an exacerbation of symptoms might have precipitated the decision to implant a device, thus patients could have unusually high healthcare costs in the 12 months prior to implantation, which could lead to a potential underestimate of the incremental costs of an infection in the postimplant time-period. The second methodology used was a case-controlled analysis, using PSM to create patient cohorts with similar characteristics, with and without CDI. In this analysis, the device implant date was the index date and healthcare expenditures were obtained for the following 3 years. This methodology avoids a potential regression to the mean effect.
Definition of CDI, duration of follow-up, sample size, CDI prevention strategies and other aspects of study design have varied in the literature, making comparisons between studies problematic. The results of this study are generally consistent with published evidence. In a recent randomized trial of ICD therapy (the DANISH study), CDI was recorded in 4.9% of patients over a median follow-up of over 5 years (67.6 months) [8]. In a study of 316 patients with CRT implantation in a single center in France, the prevalence of CDI was 4.3% at 2.6 years (1.7% per year incidence) [18]. In a study of 2476 patients implanted with ICD or CRT-D devices in a single center in The Netherlands, 2.6% underwent device and lead extraction for CDI during a median follow-up of 30 months [11].
Information about healthcare utilization and costs associated with CDI is scarce in Europe. The current study is the largest to date to estimate CDI treatment costs in Europe. It is the first study taking into account healthcare expenditure associated with infection management after hospital discharge, with a maximum follow-up period of 3 years after infection. Moreover, average per patient costs have been estimated according to severity of infection and costs were broken down into six categories (hospitalization, outpatient care, pharmaceuticals in outpatient setting, sick pay, remedies and medical aids).
A single-institution study in England of 24 CDIs requiring device removal calculated a cost of €36,931 (£30,958) per CDI [19]. A study of CDI in seven pacemaker patients in Germany estimated a mean additional hospital cost of €7091 [20]. In an administrative claims database analysis in the USA, similar in methodology to our study, the estimated incremental healthcare expenditures for patients with an infection were €44,099 ($47,885) for de novo implants and €41,913 ($45,512) for replacement patients [12].
It is important that data pertaining to CIED infections are accurately collected and reported at a national level, in order to improve quality of care for patients. Few studies have been performed on the costs of CDIs and there is a critical need for better data to estimate total healthcare costs.
Strategies to prevent CIED infection should be a priority for healthcare providers and payers. Two large trials are ongoing which may define new standards of care for prevention of CIED infection: PADIT and WRAP-IT. The Prevention of Arrhythmia Device Infection Trial (PADIT) is a 12,800 patient trial to test the comparative effectiveness of an existing preprocedural antibiotic regimen versus a novel dosing regimen for high-risk procedures. High-risk patients are defined as any patient undergoing CRT implant or any re-intervention on an incumbent device. The World-wide Randomized Antibiotic Envelope Infection Prevention Trial (WRAP-IT) is a randomized, single blinded clinical study in up to 7764 subjects, to evaluate the ability of the TYRX™ Absorbable Antibacterial Envelope (Medtronic Infection Control, NJ, USA) to reduce major CIED infections through 12 months postprocedure following CIED generator replacement, upgrade, revision or de novo CRT-D implant.
Increased understanding and awareness of risk factors for CDI is important to inform individualized decisions about device implants. In some cases, it may be possible to address a risk factor (such as oral anticoagulant use). Often, the risk factors are largely unavoidable, and in that case it makes financial sense to target the use of technologies such as antibiotic envelopes to those patients at high-risk of CDI. In our study, some risk factors for CDI were more common in patients with CDI versus those without; notably, kidney disease, having malignancies or being immunocompromised or taking oral anticoagulant drugs. This adds to an already extensive literature about risk factors for CDI [21].
Limitations
The analysis was conducted using data from several SHIs comprising approximately 2.8 million people, 3.5% of the nationwide population. Similarly, the number of implants included in this study is estimated to represent 3.6% (4699) of the total number of ICDs implanted in Germany in the period 2009–2013 (129,000).
The analysis is based on anonymized billing data from a German health claims database; such databases were designed primarily to enable appropriate hospital financing and not for epidemiological purposes. The accuracy of the information depends on physician coding practices and the quality of data could differ between health units or regions.
Information was not available about periprocedural use of intravenous antibiotic prophylaxis in each patient, which significantly reduces CDI and is recommended practice [5–7,22]. Furthermore, microbiologic culture results were unknown for each case of CDI and therefore we were unable to demonstrate the role of different bacteria.
For the device replacement cohort, infections were only counted if they occurred after the index device replacement stay; for hospital stays where a CDI was documented with no prior record of a CDI in that patient, and a replacement procedure was conducted during the same stay, it was not possible to discern whether the patient came directly into hospital for a replacement procedure due to CDI, or the patient had come for a planned replacement (for instance due to battery depletion) and developed a CDI after surgery and prior to discharge. This limitation may underestimate the CDI rate for replacement procedures, and conversely overestimate the rate for de novo implants. However, this may only have had a small effect, because it is uncommon for CDI to be diagnosed within the same stay as the implant procedure [11,23].
We defined minor CDI as without a device procedure within 8 weeks after documented infection. However, 30% of minor CDI in this study were managed with inpatient care and we acknowledge a limitation of our definition and recognize that some minor CDIs were serious.
Mean cumulative costs per patient over 3 years were estimated without adjustment for a decreasing number of patients still present in the SHI database over the course of the follow-up period, due to mortality or switching of health insurance provider. This approach makes the results applicable for SHI companies to quantify the budget impact of CDIs. However, the average cost per patient based on the whole starting cohort, from an SHI perspective, underestimates the mean cost of surviving patients, which should be kept in mind for using these cost data in Markov-type cost–effectiveness models.
Conclusion
CDIs are a serious and life-threatening complication occurring with an increasing frequency. Risk of infection observed in this study of ICD and CRT-D devices was 3.4%. Mean incremental costs were €31,493 for de novo implant patients and €33,777 for replacement patients for a payer perspective. Mean cumulative 3-year costs per patient with major infections were €99,706, an incremental cost of €59,419 compared with controls.
Incidence of cardiac device infection (CDI) observed in Germany was 3.4% overall within 1 year of implant, with a higher risk for replacement procedures than new implants (4.4 vs 2.9%; p < 0.01).
Rates of conservative treatment are high, which may be a cause for concern given the known mortality risks of nonremoval of the complete device system.
Expenditures for patients with an infection of any severity, compared with the controls, were increased by €31,493 for de novo implant patients and €33,777 for replacement patients. Costs for major infections (requiring a device procedure) were much higher (€59,419).
These cost data are useful for evaluation of cost–effectiveness of new methods to prevent CDI.
To improve quality of care for patients, it is important in the future that data pertaining CDI and other outcomes in device patients are collected and reported accurately in daily practice.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Financial & competing interests disclosure
This work was funded by Medtronic International Trading Sàrl, Switzerland. S Ludwig and W Lux are an employee and CEO of HGC GesundheitsConsult GmbH, which received funding from Medtronic International Trading Sarl to perform this study. B Brown and A Witthohn are employees of Medtronic International Trading Sarl and Medtronic GmbH, respectively. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Supplementary Material
File (supplementary material.docx)
- Download
- 32.41 KB
References
1.
Raatikainen MJ, Arnar DO, Merkely B, Camm AJ, Hindricks G. Access to and clinical use of cardiac implantable electronic devices and interventional electrophysiological procedures in the European Society of Cardiology Countries: 2016 report from the European Heart Rhythm Association. Europace 18(Suppl. 3), III1–III79 (2016).
2.
Ponikowski P, Voors AA, Anker SD et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 18(8), 891–975 (2016).
3.
Priori SG, Blomström-Lundqvist C, Mazzanti A et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 36(41), 2793–2867 (2015).
4.
NICE technology appraisal guidance 314, June 2014. Implantable cardioverter defibrillators and cardiac resynchronisation therapy for arrhythmias and heart failure (review of TA95 and TA120). www.nice.org.uk/guidance/ta314
5.
Kusumoto FM, Schoenfeld MH, Wilkoff BL et al. HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm (2017) (Epub ahead of print).
6.
Habib G, Lancellotti P, Antunes MJ et al. 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 36(44), 3075–3128 (2015).
7.
Sandoe JA, Barlow G, Chambers JB et al. Guidelines for the diagnosis, prevention and management of implantable cardiac electronic device infection. Report of a joint working party project on behalf of the British Society for Antimicrobial Chemotherapy (BSAC, host organization), British Heart Rhythm Society (BHRS), British Cardiovascular Society (BCS), British Heart Valve Society (BHVS) and British Society for Echocardiography (BSE). J. Antimicrob. Chemother. 70(2), 325–359 (2015).
8.
Køber L, Thune JJ, Nielsen JC et al. Defibrillator implantation in patients with nonischemic systolic heart failure. N. Engl. J. Med. 375(13), 1221–1230 (2016).
9.
Sridhar AR, Lavu M, Yarlagadda V et al. Cardiac implantable electronic device-related infection and extraction trends in the US. Pacing Clin. Electrophysiol. 40(3), 286–293 (2017).
10.
Sohail MR1, Henrikson CA, Braid-Forbes MJ, Forbes KF, Lerner DJ. Mortality and cost-associated with cardiovascular implantable electronic device infections. Arch. Intern. Med. 171(20), 1821–1828 (2011).
11.
de Bie MK, van Rees JB, Thijssen J et al. Cardiac device infections are associated with a significant mortality risk. Heart Rhythm 9, 494–498 (2012).
12.
Sohail MR, Eby EL, Ryan MP, Gunnarsson C, Wright LA, Greenspon AJ. Incidence, treatment intensity and incremental annual expenditures for patients experiencing a cardiac implantable electronic device infection: evidence from a large US payer database 1-year postimplantation. Circ. Arrhythm Electrophysiol. 9(8), pii, e003929 (2016).
13.
IQWiG Institute for Quality and Efficiency in Healthcare. General Methods. Version 4.2 (2015). www.iqwig.de/download/IQWiG_General_Methods_Version_%204–2_no_longer_valid.pdf
14.
Johnson NL, Crown W, Martin BC, Dormuth CR, Siebert U. Good research practices for comparative effectiveness research: analytic methods to improve causal inference from nonrandomized studies of treatment effects using secondary data sources. Report of the ISPOR Retrospective Database Analysis Task Force – Part III. Value Health 12(8), 1062–1073 (2009).
15.
Pan W, Bai H. Propensity Score Analysis: Fundamentals and Developments. The Guilford Press, NY, USA (2015).
16.
Caliendo M, Kopeinig S. Some practical guidance for the implementation of propensity score matching. J. Econ. Surveys 22(1), 31–72 (2008).
17.
Johansen JB, Jorgensen OD, Moller M et al. Infection after pacemaker implantation: infection rates and risk factors associated with infection in a population-based cohort study of 46299 consecutive patients. Eur. Heart J. 32, 991–998 (2011).
18.
Romeyer-Bouchard C, Da Costa A, Dauphinot V et al. Prevalence and risk factors related to infections of cardiac resynchronization therapy devices. Eur. Heart J. 31(2), 203–210 (2010).
19.
Ahsan SY, Saberwal B, Lambiase PD et al. A simple infection-control protocol to reduce serious cardiac device infections. Europace 16, 1482–1489 (2014).
20.
Kuehn C, Graf K, Heuer W et al. Economic implications of infections of implantable cardiac devices in a single institution. Eur. J. Cardiothorac. Surg. 37(4), 875–879 (2010).
21.
Polyzos KA, Konstantelias AA, Falagas ME. Risk factors for cardiac implantable electronic device infection: a systematic review and meta-analysis. Europace 17(5), 767–777 (2015).
22.
de Oliveira JC, Martinelli M, Nishioka SA et al. Efficacy of antibiotic prophylaxis before the implantation of pacemakers and cardioverter-defibrillators: results of a large, prospective, randomized, double-blinded, placebo-controlled trial. Circ. Arrhythm. Electrophysiol. 2, 29–34 (2009).
23.
Deharo JC, Quatre A, Mancini J et al. Long-term outcomes following infection of cardiac implantable electronic devices: a prospective matched cohort study. Heart 98, 724–731 (2012).
Information & Authors
Information
Published In
Copyright
© 2017 Future Medicine Ltd.
History
Received: 1 October 2017
Accepted: 30 October 2017
Published online: 14 November 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Incidence and costs of cardiac device infections: retrospective analysis using German health claims data. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0080
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Benito Baldauf, Kerstin Bode, Ernest W. Lau, Marzia Giaccardi, Ojan Assadian, Philippe Chévalier, Christelle Haddad, Andreas Klöss, Roberto Cemin, Reinhard Vonthein, Hendrik Bonnemeier, Trends in cardiac implantable electronic device infections: 2015 to 2019, BMC Cardiovascular Disorders, 10.1186/s12872-026-06124-w, 26, 1, (2026).
- Mantė Agnė Rimkienė, Diana Sudavičienė, Gediminas Račkauskas, Paulius Jurkuvėnas, Veronika Gorevska, Julius Stukas, Germanas Marinskis, Evidence-Based Strategies for the Prevention of Cardiac Implantable Electronic Device Infections: An Up-to-Date Narrative Review, Medicina, 10.3390/medicina62050991, 62, 5, (991), (2026).
- Md Shajedur Rahman Shawon, Behnoosh Hosseinloui Khalaj, Michelle Hill, Gabrielle Challis, Liesl Strachan, Louisa Jorm, Economic Burden Associated With Cardiac Implantable Electronic Device ( CIED ) Infections in New South Wales, Australia: A Population‐Based Study Using Linked Administrative Data , Journal of Arrhythmia, 10.1002/joa3.70237, 41, 6, (2025).
- Benito Baldauf, Roberto Cemin, Mauro Biffi, Antonio Rapacciuolo, Giulio Zucchelli, Maria Grazia Bongiorni, Ernesto Casorelli, Gianfranco Mitacchione, Felix Hohendanner, Emanuele Durante-Mangoni, Veronica Dusi, Paul William Xavier Foley, Angelo Pan, Giuseppe Arena, Archana Rao, Sebastian Spencker, Alexander Steger, Carlo Tascini, Valerio Zacà, Federico Migliore, Ojan Assadian, Marzia Giaccardi, Hendrik Bonnemeier, Kerstin Bode, Addressing Complications in Cardiac Implantable Electronic Devices: A Guideline to Prevention of CIED Infection, Journal of Cardiovascular Development and Disease, 10.3390/jcdd12100406, 12, 10, (406), (2025).
- Simon Christie, Michael McGregor, Andrew D. Krahn, Cardiac implantable electronic device infection, Trends in Cardiovascular Medicine, 10.1016/j.tcm.2025.02.001, 35, 5, (310-316), (2025).
- Sathvika Mudigonda, Ethan Hagarty, Lucy Lei, Elissa Rennert-May, Jacqueline Joza, Derek V Exner, Jason Andrade, Satish R Raj, Derek S Chew, Cost-effectiveness of an intraoperative antibacterial envelope in preventing cardiac implantable device-associated infections: a systematic review, Europace, 10.1093/europace/euaf121, 27, 7, (2025).
- Shmaila Saleem-Talib, Crispijn P R Hoevenaars, Nadine Molitor, Vincent J van Driel, Jeroen van der Heijden, Alexander Breitenstein, Harry van Wessel, Mathijs S van Schie, Natasja M S de Groot, Hemanth Ramanna, Leadless pacing: a comprehensive review, European Heart Journal, 10.1093/eurheartj/ehaf119, 46, 21, (1979-1990), (2025).
- Benito Baldauf, Reinhard Vonthein, Ernest W. Lau, Marzia Giaccardi, Ojan Assadian, Philippe Chévalier, Christelle Haddad, Kerstin Bode, Andreas Klöss, Roberto Cemin, Hendrik Bonnemeier, Prevalence of cardiac implantable electronic device infections in Germany in 2015, Scientific Reports, 10.1038/s41598-024-82622-1, 14, 1, (2024).
- Mauro Biffi, Andreas Götte, Jay Wright, Emilce Trucco, Didier Klug, Andrew Turley, Francisco Costa, David Duncker, Cardiac implantable electronic device infection awareness – A European survey amongst implanting physicians, International Journal of Cardiology, 10.1016/j.ijcard.2024.132454, 415, (132454), (2024).
- Reinhard Vonthein, Benito Baldauf, Stefan Borov, Ernest W. Lau, Marzia Giaccardi, Ojan Assadian, Christelle Haddad, Philippe Chévalier, Kerstin Bode, Paul Foley, Honey Thomas, Niall G. Campbell, Stephanie Fichtner, Luca Donazzan, Felix Pescoller, Rainer Oberhollenzer, Roberto Cemin, Hendrik Bonnemeier, Taurolidine-containing solution for reducing cardiac implantable electronic device infection-early report from the European TauroPace™ registry, Journal of Cardiothoracic Surgery, 10.1186/s13019-024-03059-1, 19, 1, (2024).
- See more