Comparing efficacy of enteral nutrition plus ranitidine and enteral nutrition alone as stress ulcer prophylaxis
Abstract
Aim: Adequacy of enteral nutrition (EN) alone as stress ulcer prophylaxis (SUP) is controversial. The aim of this study was to compare efficacy of EN alone and ranitidine plus EN as SUP. Method: Critically ill adults with indications to receive SUP were randomized to ranitidine 50 mg IV every 8 h plus EN (SUP) or EN alone (non-SUP) group for 7 days. Besides, endoscopy was performed at the time of recruitment and on day 7. Results: During the study period, only one patient in each group of SUP and non-SUP experienced gastrointestinal bleeding. At the time of recruitment, gastric erosion and erythema were the most endoscopic findings in the SUP and non-SUP groups. These findings did not significantly change at the end of the study (p = 0.21). Conclusion: EN was at least effective as ranitidine plus EN as SUP.
Critically ill patients are at increased risk for stress-related ulcer and subsequent gastrointestinal (GI) bleeding. Severity of acute illnesses, organ failure, medications, hemodynamic instability, hypoxemia, vasopressors, mechanical ventilation and long term fasting are main predisposing factors for stress ulcer in these patients [1–3]. Although upper GI lesions were detected within 3 days of intensive care unit (ICU) admission in most critically ill patients but bleeding was uncommon [4–7]. Depending on depth and distribution of the lesions, stress ulcers can lead to significant hemodynamic instability [8–11]. Clinically significant GI bleeding was reported in 2–4% of critically ill patients [12–15].
Catecholamine release, vasoconstriction, hypovolemia, decrease in cardiac output, inflammatory cytokines, endothelin and decrease in nitric oxide production, moves blood away from viscera to vital organs and leads to GI mucosa ischemia [17–20]. Prolonged splanchnic hypoperfusion decreases bicarbonate production, GI motility and thereafter delayed acid clearance that interfere with mucosal healing [19–26]. According to American Society of Health-System Pharmacists recommendations, ventilation more than 48 h and coagulopathy are two main predisposing factors for stress related mucosal bleeding in critically ill patients [27,28].
For more than 40 years, stress ulcer prophylaxis (SUP) was proposed to prevent mucosal damage and GI bleeding in acute illnesses [29–31]. SUP is recommended to maintain gastric pH above 4, that has been proven to reduce the risk of mucosal injury and GI bleeding [26,32]. However, widespread use of acid suppressing agents was associated with serious complications such as pneumonia and Clostridium difficile infection [33–36].
Following restoring of blood flow and stimulating epithelial cells renewal, enteral nutrition (EN) has critical role in preventing mucosal atrophy and GI bleeding. It is highly recommended to start EN within 24–48 h of ICU admission [30,37–39]. However, effect of EN on gastric pH has not been fully described [31,40,41].
Adequacy of EN alone as SUP in critically ill patients has not been yet compared with ranitidine plus EN. The aim of this study was to compare efficacy and safety of EN alone and ranitidine plus EN as SUP in critically ill patients.
Method
Design
This open-label randomized clinical trial was performed from May 2016 to June 2017 in general ICU of Imam Khomeini Hospital Complex, a tertiary academic hospital, affiliated to Tehran University of Medical Sciences, Tehran, Iran. The study was approved by the Ethical Committee of Tehran University of Medical Sciences (Ethical code number: IR.TUMS.REC.1395.2592) and all recruited patients or one of their first-degree family members signed the study informed consent. The study also was registered as a clinical trial (IRCT code number: IRCT201604213449N21).
Patients
Adult (≥18 years old) critically ill patients were assessed within 24 h of ICU admission and who had indications to receive SUP [27,28] with no contraindication for starting EN were recruited. Patients with EN intolerance (defined as gastric residual volume more than 200 ml between the gavage schedules), severe burn, recent (during last month) GI bleeding, history of gastric ulcer, gastric or duodenal ulcer on endoscopy, receiving therapeutic dose of anticoagulants or corticosteroids and closed head trauma were excluded.
Intervention
Patients were assigned to receive either ranitidine 50 mg every 8 h as slow intravenous injection plus EN (SUP group) or only EN without ranitidine (non-SUP group) according to the simple randomization method. Random numbers were generated using excel software. Nutritional support was started within 24 h of ICU admission. Each patient received a standard EN formula (EnteraMeal product, Karen Company, Tehran, Iran) through a nasogastric tube. Each serving size (1 scoop = 33 g) of the formula provide 150 Kcal and contain 20.5 g carbohydrate, 5.3 g protein, 5.3 g total fat, vitamins and minerals. Enteral feeding was started as 50 ml every 3 h and gradually was increased to the nutritional goal (200–250 ml every 3 h or 25 kcal/kg/day) during the first 24 h. Each dose of formula was administered through nasogastric tube as intermittent bolus nutrition. The duration of intervention was 7 days and patients were followed for 28-day ICU complications.
Demographic data, baseline diseases, cause of ICU admission, severity of illness (Acute Physiology and Chronic Health Evaluation [APACHE] score), organ function (Sequential Organ Failure Assessment [SOFA] score), vital signs (temperature and hemodynamic parameters), oxygenation status (arterial blood gas [ABG]), laboratory parameters (cell blood count, partial thromboplastin time, international normalized ratio) and medications were collected from the patients’ medical records and daily ICU charts. Also daily calorie and protein intakes of patients were calculated.
Bedsides, endoscopy was performed at the time of recruitment and on day 7. Primary endpoint of the study was incidence of GI bleeding. Episodes of pneumonia, diarrhea and sepsis were considered as secondary end points. Duration of ICU stay and 28-day mortality also were assessed in this study.
Patients were daily assessed for any episode of overt GI bleeding (coffee ground gastric secretions, hematemesis or melena), respiratory infections (pneumonia), sepsis and diarrhea. Coffee ground was defined as brown blood spots in gastric lavage. Criteria for pneumonia were new or progressive lung infiltration on chest imaging and at least two of the following; purulent secretions, temperature above 38.5°C, positive tracheal or plural fluid culture, leukocytosis or leukopenia [42]. If diarrhea occurred, stool was evaluated for C. difficile toxins using ELISA. Sepsis was considered if criteria of international guideline for management of severe sepsis and septic shock were met [43].
Statistical analysis
All statistical assessments were done using SPSS version 17 software. Normal distributions of variables were checked according Kolmogorov–Smirnov test. Continuous data were expressed as mean ± standard deviation (SD) and categorical data were presented as percentage. Independent t-test and χ2 test (or Fisher's exact test in cases which more than 25% of categories had expected frequencies under 5) were used for the comparison of patients’ continuous and categorical data, respectively. The p < 0.05 was considered statistically significant.
Results
Comparing demographic & baseline data
During the study period, 69 patients were screened for enrollment and 11 individuals did not have inclusion criteria of the study. From included patients, eight patients were excluded due to EN intolerance, ICU discharge and death (Figure 1). Finally 50 patients (25 patients in each group) completed the study period. From included patients, 30 (60%) and 20 (40%) were male and female respectively (p = 0.38). Mean ± SD of age of patients in the SUP and non-SUP groups were 68.60 ± 15.58 and 60.00 ± 18.82 years, respectively (p = 0.85). Cardiovascular diseases (66%) and diabetes mellitus (20%) were common baseline diseases and respiratory failure (44%), hemodynamic instability (40%) and loss of consciousness (16%) were main causes of ICU admission. Baseline diseases, cause of ICU admission, APACHE and SOFA scores, laboratory and clinical parameters are summarized in Tables 1 & 2. There was no statistically significant difference between the groups regarding the baseline patients’ characteristics. Heparin prophylaxis (92 vs 90%), antibiotics (92 vs 100%), N-acetylcysteine (32 vs 40%), vasopressors (32 vs 28%) and antiepileptic drugs (24 vs 28%) were common administered drugs in the SUP and non-SUP groups respectively (p = 0.10).
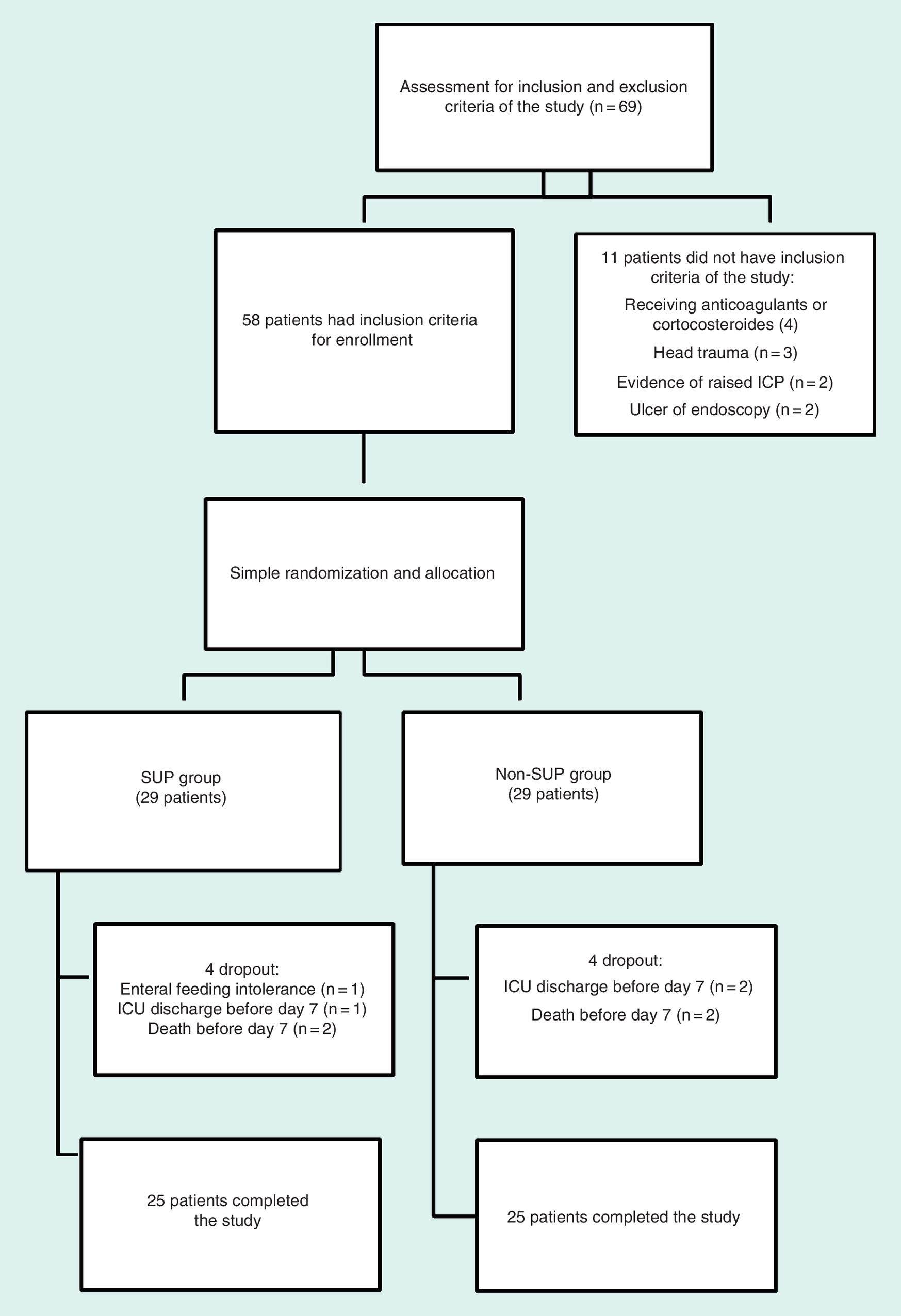
Figure 1. Consort flowchart of the study.
ICU: Intensive care unit; SUP: Stress ulcer prophylaxis.
| Parameter; mean ± SD or n (%) | SUP (n = 25) | Non-SUP (n = 25) |
|---|---|---|
| Age (years) | 68.60 ± 15.58 | 60.00 ± 18.82 |
| Sex (female:male) | 11:14 | 9:16 |
| Weight (kg) | 71.36 ± 11.00 | 68.08 ± 11.33 |
| APACHE (mean ± SD) | 18.28 ± 5.31 | 17.12 ± 5.43 |
| SOFA (mean ± SD) | 8.76 ± 3.38 | 7.56 ± 2.04 |
| Baseline diseases | ||
| None | 4 (16) | 5 (20) |
| CVD | 16 (64) | 17 (68) |
| DM | 1 (4) | 9 (36) |
| Respiratory diseases | 3 (12) | 3 (12) |
| CKD | 3 (12) | 1 (4) |
| Neurologic diseases | 2 (8) | 1 (4) |
| Rheumatologic diseases | 3 (12) | 1 (4) |
| Causes of ICU admission | ||
| Respiratory failure | 12 (48) | 10 (40) |
| Hemodynamic instability | 9 (36) | 11 (44) |
| Loss of consciousness | 4 (16) | 4 (16) |
†Baseline characteristics of patients were compared. No statistically significant difference was detected between the groups. The p-values for all comparisons were over 0.05.
APACHE: Acute Physiology and Chronic Health Evaluation; CKD: Chronic kidney disease; CVD: Cardiovascular disease; DM: Diabetes mellitus; ICU: Intensive care unit; SD: Standard deviation; SOFA: Sequential Organ Failure Assessment; SUP: Stress ulcer prophylaxis.
| Parameter | SUP (n = 25) | Non-SUP (n = 25) |
|---|---|---|
| Patients with at least one episode of acidosis | 8 (32) | 8 (32) |
| Patients with at least one episode of alkalosis | 17 (68) | 13 (52) |
| Patients with at least one episode of leukopenia | 4 (16) | 1 (4) |
| Patients with at least one episode of leukocytosis | 20 (80) | 22 (88) |
| Patients with at least one episode of anemia (Hgb under 7 g/dl) | 3 (12) | 6 (24) |
| Patients with at least one episode of thrombocytopenia | 10 (40) | 10 (40) |
| Mean arterial pressure (mmHg) | 91.12 ± 8.92 | 91.40 ± 9.10 |
| Patients with coagulopathy | 14 (56%) | 11 (44) |
| Urea (mg/dl) | 77.67 ± 42.40 | 53.57 ± 26.44 |
| Serum creatinine (mg/dl) | 1.33 ± 0.58 | 1.13 ± 0.44 |
| INR | 1.44 ± 0.41 | 1.30 ± 0.42 |
| Albumin (g/dl) | 2.31 ± 0.54 | 2.75 ± 0.56 |
| Total bilirubin (mg/dl) | 0.98 ± 0.54 | 0.90 ± 0.55 |
| Alanine aminotransferase (U/l) | 44.37 ± 22.87 | 41.16 ± 31.11 |
| Aspartate aminotransferase (U/l) | 32.80 ± 16.60 | 51.16 ± 28.20 |
| Alkaline phosphatase (U/l) | 241.40 ± 75.00 | 289.67 ± 88.19 |
†Laboratory parameters of patients were compared at the time of recruitment. For all comparisons p-values were more than 0.05.
Hgb: Hemoglobin; INR: International normalized ratio; SUP: Stress ulcer prophylaxis.
Mean daily calorie and protein intakes in patients in SUP and non-SUP groups were comparable [(1416.80 ± 542.61 vs 1497.00 ± 551.75 Kcal/day) and (52.30 ± 18.24 vs 56.41 ± 20.46 g/day), respectively].
Primary end points
Coffee ground secretion (GI bleeding) was detected in one patient in each group of SUP and non-SUP (p = 0.75). At the time of recruitment, gastric erosion and erythema were the most endoscopic findings in the SUP and non-SUP groups (8 and 16% vs 4 and 12%, respectively, p = 0.34). These findings did not significantly change at the end of the study (12 vs 12% and 12 vs 8%, respectively, p = 0.21).
Secondary end points
There was no significant difference between the groups considering pneumonia, sepsis and diarrhea episodes (Table 3).
| Endpoint | SUP (n = 25) | Non-SUP (n = 25) |
|---|---|---|
| Pneumonia (%) | 9 (36) | 7 (28) |
| Other infections (%) | 3 (12) | 6 (24) |
| Clostridium difficile diarrhea | ||
| Sepsis (%) | 4 (16) | 3 (12) |
| Coffee ground | 1 (4) | 1 (4) |
| Hematemesis | – | – |
| Melena | – | – |
†GI bleeding (coffee ground, hematemesis and melena) and infections (pneumonia, sepsis, C. difficile and other infections) were considered as primary and secondary end points of the study respectively. No statistically significant difference was detected between the groups. All p-values were more than 0.05.
SUP: Stress ulcer prophylaxis.
Days of mechanical ventilation in SUP and non-SUP groups were 11.60 ± 7.43 and 15.04 ± 7.17, respectively (p = 0.10). Length of ICU stay was comparable between the groups (15.19 ± 12.81 vs 13.00 ± 11.98 days, respectively; p = 0.57). In this study, 28-day ICU mortality rates in SUP and non-SUP groups were 32 and 20%, respectively (p = 0.26).
According to incidence of GI mucosal injury in critically ill patients [4–7] and considering α = 0.05 and β = 0.80, the sample size of the study was calculated as 29 patients in each group. However, eight patients were excluded during the study period. Therefore, the power of study was calculated as 71%.
Discussion
This was the first study that compared EN alone and ranitidine plus EN in preventing stress-related mucosal injuries in critically ill patients. In this study, EN alone was effective as ranitidine plus EN as SUP. GI bleeding episodes did not differ between the SUP and non-SUP groups.
Imbalance between aggressive and defensive mucosal factors is proposed as mechanism of stress-related mucosal injury. Gastric acid overproduction and reflux of acid toward stomach are main known aggressive factors. Mucosal integrity, blood flow, bicarbonate secretion and epithelial cells renewal are the most effective defensive parameters [27,44]. Restoring blood flow to gastric mucosa has critical role in preventing mucosal damage. Early EN, adequate hydration, oxygenation and hemodynamic supports are main factors that regulate gastric mucosal perfusion [26]. Starting EN, as soon as possible, decreased incidence of stress ulcer in critically ill patients [16,45]. By enhancing gastric blood flow, increase in gastric PH and decreasing mucosal ischemia, EN showed important role in preventing of stress ulcer in critically ill patients [5,31]. Another important effect of early EN is repairing and retaining mucosal integrity through GI tract. This property also prevents bacterial and endotoxins translocation via mucosal barriers [38,44]. Pharmacological agents (proton pump inhibitors and histamine type-2 receptors blockers) that routinely used for SUP do not have any direct effect on mucosal integrity and the defensive barriers.
Critically ill patient with trauma who received EN within 24 h of ICU admission had much lower mucosal permeability than the control group [46]. EN stimulates cell renewal pathway and epithelialization [19,47].
Protective effect of EN against stress ulcer was compared with antacids and cimetidine in 1983. In this study, EN was more effective than antacids and cimetidine in preventing GI bleeding [48]. In recent published study, pantoprazole did not add more benefit than EN for prevention of stress ulcer in critically ill patients [49].
In our study also no patient experienced significant GI bleeding. Coffee ground secretions detected in two (4%) of the patients. None of these patients had ulcers in repeated endoscopy.
In a study in 2013, Palm et al. discontinued SUP in critically ill patients who tolerated EN. GI bleeding was considered as endpoint of the study. In this study, the incidence of clinically important GI bleeding was 0.5%. They concluded that pharmacologic SUP can be stopped in surgical and trauma critically ill patients when tolerate EN [22]. In a randomized double-blind clinical trial in 2016, no significant difference in the incidence of overt GI bleeding, pneumonia, C. difficile diarrhea or days of ICU stay was detected in patients who received EN or pantoprazole [16].
However, in an old study, patients who received EN as SUP experienced more GI bleeding events. Although this study had control group but the patients were not randomly included. Patients in the EN group were older and had more predisposing factors for GI bleeding than the control group [50].
Although patients with burn or head trauma had severe stress and other risk factors for stress-related mucosal injury, but EN exhibited prophylactic effect. Severely burn patients who were under EN support had less bleeding events than those received cimetidine or antacid [51].
Comparing with parenteral nutrition, EN was more effective in preventing GI bleeding episodes in head trauma patients. Also sepsis was more common in the parenteral nutrition group than the EN group. GI tract is one of the main sources of bacteria and endotoxins that following translocation can cause nosocomial infections and sepsis. Delaying in initiation of EN may cause GI mucosal atrophy. On the other hand, acid suppressing agents promote GI bacterial replication and growth by increasing intragastric pH. These two parameters are main factors that facilitate bacterial translocation in patients who received parenteral nutrition concomitant with pharmacological SUP [47].
Respiratory tract infection (pneumonia) is the most common infection in critically ill patients. Aspiration is main route for entrance of bacteria to respiratory system. Critically ill patients are more vulnerable to aspiration pneumonia due to baseline diseases, severity of illnesses, intubation, position on bed, medications, interventions, feeding intolerance and ileus. Delay in initiation of EN was associated with increased risk of pneumonia [52].
Delay in starting EN is commonly due to concerns regarding vomiting and risk of aspiration. However, in patients with secured airway early initiation of EN is logical [53].
Correlations between use of pharmacologic SUP and increasing risk of aspiration pneumonia and C. difficile infection have been reported in other populations [7,54]. Gastric acidity is a natural defense against bacteria replication through GI tract. Spores of C. difficile bacteria but not vegetative (pathogenic) forms are stable in acidotic gastric PH. In alkaline conditions, vegetative forms were 10-fold more than spores [55]. Risk of C. difficile infection has not been compared between EN and acid suppressing agents in well-designed, controlled, paralleled study. However, no episode of C. difficile associated diarrhea was detected in our study.
Our study was first one that compared EN alone and EN plus ranitidine as SUP in critically ill patients. Also for the first time bedside endoscopy was applied for evaluation of the effectives of SUP in this setting. However, this study had some limitation. It was an open labeled, no placebo-controlled study with limited sample size. Also gastric PH monitoring was not considered in this study.
Conclusion
Few studies compared EN and acid suppressants agents as SUP in critically ill patients. Effectiveness of EN or acid suppressants agents was assessed subjectively. No study considered endoscopy findings. In our study EN was at least effective as ranitidine plus EN in preventing stress-related GI bleeding. Also risk of complications including pneumonia, sepsis and diarrhea were comparable between the groups.
Future perspective
Only few studies support efficacy and safety of EN as SUP in critically ill patients. More well-designed multicenter studies with adequate sample size are required to define efficacy and safety of EN as SUP.
Critically ill patients are at increased risk for stress related ulcer and subsequent gastrointestinal (GI) bleeding. In this study, effectiveness of enteral nutrition (EN) alone and ranitidine plus EN as GI bleeding prophylaxis was compared in critically ill patients.
Methods
Patients were assigned to receive either ranitidine 50 mg every 8 h as slow intravenous injection plus EN (SUP group; n = 25) or only EN without ranitidine (non-SUP group, n = 25). Bedsides endoscopy was performed at the time of recruitment and on day 7. Primary outcome of the study was incidence of GI bleeding.
Results
During the study period number of patients with GI bleeding were comparable between the groups (p = 0.75). At the time of recruitment, gastric erosion and erythema were the most endoscopic findings in the SUP and non-SUP groups (8 and 16% vs 4 and 12%, respectively, p = 0.34). These findings did not significantly change at the end of the study (12 vs 12% and 12 vs 8%, respectively, p = 0.21).
Conclusion
EN was at least effective as ranitidine plus EN in preventing stress related GI mucosal injury.
Financial & competing interests disclosure
This study is the result of a PharmD student thesis and supported by Tehran University of Medical Sciences, Iran. The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Avendaño-Reyes JM, Jaramillo-Ramírez H. Prophylaxis for stress ulcer bleeding in the intensive care unit. Rev. Gastroenterol. Mex. 79(1), 50–55 (2014).
2.
Mousavi M, Dashti-Khavidaki S, Khalili H, Farshchi A, Gatmiri M. Impact of clinical pharmacy services on stress ulcer prophylaxis prescribing and related cost in patients with renal insufficiency. Int. J. Pharm. Pract. 21(4), 263–269 (2013).
3.
Marker S, Krag M, Møller MH. What's new with stress ulcer prophylaxis in the ICU? Intensive Care Med. 43(8), 1132–1134 (2017).
•• News in stress ulcer prophylaxis (SUP) in the intensive care unit.
4.
Faust AC, Echevarria KL, Attridge RL. Prophylactic acid-suppressive therapy in hospitalized adults: indications, benefits, and infectious complications. Crit. Care Nurse 37(3), 18–29 (2017).
•• Review of acid-suppressive therapy in hospitalized adults.
5.
Hurt RT, Frazier TH, McClave SA et al. Stress prophylaxis in intensive care unit patients and the role of enteral nutrition. JPEN J. Parenter. Enteral. Nutr. 36(6), 721–731 (2012).
6.
MacLaren R, Campbell J. Cost–effectiveness of histamine receptor-2 antagonist versus proton pump inhibitor for stress ulcer prophylaxis in critically ill patients. Crit. Care Med. 42(4), 809–815 (2014).
7.
Somberg L, Morris J Jr, Fantus R et al. Intermittent intravenous pantoprazole and continuous cimetidine infusion: effect on gastric pH control in critically ill patients at risk of developing stress-related mucosal disease. J. Trauma 64(5), 1202–1210 (2008).
8.
Spirt MJ. Acid suppression in critically ill patients: what does the evidence support? Pharmacotherapy 23, 87S–93S (2003).
9.
Singh H, Houy TL, Singh N, Sekhon S. Gastrointestinal prophylaxis in critically ill patients. Crit. Care Nurs. Q. 4, 291–301 (2008).
10.
Huang J, Cao Y, Liao C, Wu L, Gao F. Effect of histamine-2-receptor antagonists versus sucralfate on stress ulcer prophylaxis in mechanically ventilated patients: a meta-analysis of 10 randomized controlled trials. Crit. Care 14(5), R194 (2010).
11.
Constantin VD, Paun S, Ciofoaia VV, Budu V, Socea B. Multimodal management of upper gastrointestinal bleeding caused by stress gastropathy. J. Gastrointestin. Liver Dis. 18(3), 279–284 (2009).
12.
Krag M, Perner A, Wetterslev J. Stress ulcer prophylaxis in the intensive care unit trial: detailed statistical analysis plan. Acta Anaesthesiol. Scand. 61(7), 859–868 (2017).
13.
Lat I, Micek S, Janzen J. Off-label medication use in adult critical care patients. J. Crit. Care 26(1), 89–94 (2011).
14.
Cook DJ, Fuller HD, Guyatt GH. Risk factors for gastrointestinal bleeding in critically ill patients. Canadian Critical Care Trials Group. N. Engl. J. Med. 330(6), 377–381 (1994).
15.
Krag M1, Perner A, Møller MH. Stress ulcer prophylaxis in the intensive care unit. Curr. Opin. Crit. Care. 22(2), 186–190 (2016).
16.
Selvanderan SP, Summers MJ, Finnis ME. Pantoprazole Or Placebo for stress Ulcer Prophylaxis (POP-UP): randomized double-blind exploratory study. Critical Care Med. 44(10), 1842–1850 (2016).
• Pantoprazole or placebo for SUP.
17.
Buendgens L, Koch A, Tacke F. Prevention of stress-related ulcer bleeding at the intensive care unit: risks and benefits of stress ulcer prophylaxis. World J. Crit. Care Med. 5(1), 57–64 (2016).
• Risks and benefits of SUP.
18.
Björne H, Govoni M, Törnberg DC. Intragastric nitric oxide is abolished in intubated patients and restored by nitrite. Crit. Care Med. 33(8), 1722–1727 (2005).
19.
Bardou M, Quenot JP, Barkun A. Stress-related mucosal disease in the critically ill patient. Nat. Rev. Gastroenterol. Hepatol. 12(2), 98–107 (2015).
20.
Tabeefar H, Beigmohammadi MT, Javadi MR et al. Effects of pantoprazole on systemic and gastric pro- and anti-inflammatory cytokines in critically ill patients. Iran J. Pharm. Res. 11(4), 1051–1058 (2012).
21.
Martindale RG. Contemporary strategies for the prevention of stress-related mucosal bleeding. Am. J. Health Syst. Pharm. 62(10 Suppl. 2), S11–S17 (2005).
22.
Palm NM, McKinzie B, Ferguson PL et al. Pharmacologic stress gastropathy prophylaxis may not be necessary in at-risk surgical trauma icu patients tolerating enteral nutrition. J. Intensive Care Med. pii:0885066616678385 (2016) (Epub ahead of print).
23.
Krag M, Perner A, Wetterslev J. Stress ulcer prophylaxis in the intensive care unit: an international survey of 97 units in 11 countries. Acta Anaesthesiol. Scand. 59(5), 576–585 (2015).
24.
Plummer MP, Blaser AR, Deane AM. Stress ulceration: prevalence, pathology and association with adverse outcomes. Crit. Care 18(2), 213 (2014).
25.
Ali T, Harty RF. Stress-induced ulcer bleeding in critically ill patients. Gastroenterol. Clin. North Am. 38(2), 245–265 (2009).
26.
Brophy GM, Brackbill ML, Bidwell KL. Prospective, randomized comparison of lansoprazole suspension, and intermittent intravenous famotidine on gastric pH and acid production in critically ill neurosurgical patients. Neurocrit. Care 13, 176–181 (2010).
27.
ASHP Therapeutic Guidelines on Stress Ulcer Prophylaxis. ASHP Commission on Therapeutics and approved by the ASHP Board of Directors on November 14, 1998. Am. J. Health Syst. Pharm. 56, 347–379 (1999).
28.
Khalili H, Dashti-Khavidaki S, Haj Hossein Talasaz A. Descriptive analysis of a clinical pharmacy intervention to improve the appropriate use of stress ulcer prophylaxis in a hospital infectious disease ward. J. Manag. Care Pharm. 16(2), 114–121 (2010).
29.
Marker S, Perner A, Wetterslev J et al. Stress ulcer prophylaxis versus placebo or no prophylaxis in adult hospitalised acutely ill patients; protocol for a systematic review with meta-analysis and trial sequential analysis. Syst. Rev. 6(1), 118 (2017).
30.
Heyland DK, Dhaliwal R, Drover JW. Canadian Critical Care Clinical Practice Guidelines Committee. Canadian clinical practice guidelines for nutrition support in mechanically ventilated, critically ill adult patients. JPEN J. Perenter. Enteral Nutr. 27, 355–373 (2003).
31.
Pilkington KB, Wagstaff MJ, Greenwood JE. Prevention of gastrointestinal bleeding due to stress ulceration: a review of current literature. Anaesth. Intensive Care 40, 253–259 (2012).
32.
Lenz K, Buder R, Firlinger F, Lohr G, Voglmayr M. Effect of proton pump inhibitors on gastric pH in patients exposed to severe stress. Wien Klin. Wochenschr. 127, 51–56 (2015).
33.
Khorvash F, Abbasi S, Meidani M, Dehdashti F, Ataei B. The comparison between proton pump inhibitors and sucralfate in incidence of ventilator associated pneumonia in critically ill patients. Adv. Biomed. Res. 3, 52 (2014).
34.
Miano TA, Reichert MG, Houle TT, MacGregor DA, Kincaid EH, Bowton DL. Nosocomial pneumonia risk and stress ulcer prophylaxis: a comparison of pantoprazole vs ranitidine in cardiothoracic surgery patients. Chest 136(2), 440–447 (2009).
35.
Frandah W, Colmer-Hamood J, Mojazi Amiri H, Raj R, Nugent K. Oropharyngeal flora in patients admitted to the medical intensive care unit: clinical factors and acid suppressive therapy. J. Med. Microbiol. 62, 778–784 (2013).
36.
Herzig SJ, Howell MD, Ngo LH, Marcantonio ER. Acid-suppressive medication use and the risk for hospital-acquired pneumonia. JAMA 301, 2120–2128 (2009).
37.
Anbar R. Enteral nutrition. World Rev. Nutr. Diet 105, 50–58 (2013).
38.
Lu T, Guan J. Combined application of nasogastric tubes and nasointestinal tubes in neurosurgical intensive care patients with stress ulceration: a novel solution to treatment and early enteral nutrition. Springer Plus 5(1), 1769 (2016).
39.
Kreymann K, Berger M, Deutz N. ESPEN guidelines on enteral nutrition: intensive care. Clin. Nutr. 25, 210–223 (2006).
40.
Bonten MJ, Gaillard CA, van Tiel FH. Continuous enteral nutrition counteracts preventative measures for gastric colonisation in intensive care patients. Crit. Care Med. 22, 939–944 (1994).
41.
MacLaren R, Jarvis CL, Fish DN. Use of enteral nutrition for stress ulcer prophylaxis. Ann. Pharmacother. 35(12), 1614–1623 (2001).
42.
Piriyapatsom A, Lin H, Pirrone M et al. Evaluation of the infection-related ventilator-associated events algorithm for ventilator-associated pneumonia surveillance in a trauma population. Respir. Care 61(3), 269–276 (2016).
43.
Rhodes A, Evans LE, Alhazzani W et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 43(3), 304–377 (2017).
44.
Garrow JS, James WPT, Ralph A. Human Nutrition and Dietetics. 10th Edition. Churchill Livingstone, Edinburgh, UK (2000).
45.
Faisy C, Guerot E, Diehl JL. Clinically significant gastrointestinal bleeding in critically ill patients with and without stress-ulcer prophylaxis. Intensive Care Med. 29(8), 1306–1313 (2003).
46.
Kompan L, Kremzar B, Gadzijev E. Effects of early enteral nutrition on intestinal permeability and the development of multiple organ failure after multiple injury. Intensive Care Med. 25, 157–161 (1999).
47.
Fan M, Wang Q, Fang W et al. Early enteral combined with parenteral nutrition treatment for severe traumatic brain injury: effects on immune function, nutritional status and outcomes. Chin. Med. Sci. J. 31(4), 213–220 (2016).
48.
Pingleton SK, Hadzima SK. Enteral alimentation and gastrointestinal bleeding in mechanically ventilated patients. Crit. Care Med. 11(1), 13–16 (1983).
49.
El-Kersh K, Jalil B, McClave SA et al. Enteral nutrition as stress ulcer prophylaxis in critically ill patients: a randomized controlled exploratory study. J. Crit. Care 43, 108–113 (2017).
50.
Gurman G, Samri M, Sarov B. The rate of gastrointestinal bleeding in a general ICU population: a retrospective study. Intensive Care Med. 16, 44–49 (1990).
51.
Raff T, Germann G, Hartmann B. The value of early enteral nutrition in the prophylaxis of stress ulceration in the severely burned patient. Burns 23(4), 313–318 (1997).
52.
Cinotti R, Dordonnat-Moynard A, Feuillet F et al. Risk factors and pathogens involved in early ventilator-acquired pneumonia in patients with severe subarachnoid hemorrhage. Eur. J. Clin. Microbiol. Infect. Dis. 33, 823–830 (2014).
53.
Albert BD, Zurakowski D, Bechard LJ et al. Enteral nutrition and acid-suppressive therapy in the PICU: impact on the risk of ventilator-associated pneumonia. Pediatr. Crit. Care Med. 17(10), 924–929 (2016).
54.
Marik PE, Vasu T, Hirani A. Stress ulcer prophylaxis in the new millennium: a systematic review and meta-analysis. Crit. Care Med. 38(11), 2222–2228 (2010).
55.
Jump RL, Pultz MJ, Donskey CJ. Vegetative Clostridium difficile survives in room air on moist surfaces and in gastric contents with reduced acidity: a potential mechanism to explain the association between proton pump inhibitors and C. difficile-associated diarrhea? Antimicrob. Agents Chemother. 51(8), 2883–2887 (2007).
56.
UpToDate. Stress ulcer prophylaxis in the intensive care unit. www.uptodate.com/contents/stress-ulcer-prophylaxis-in-the-intensive-care-unit?source=search_result&search=stress+ulcer+prophylaxis&selectedTitle=1∼106.
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 29 November 2017
Accepted: 18 January 2018
Published online: 18 May 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparing efficacy of enteral nutrition plus ranitidine and enteral nutrition alone as stress ulcer prophylaxis. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0098
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Priscila Sole, Stress Ulcer Prophylaxis in Critical Care: Evidence, Risk Stratification, and Clinical Implications, Cureus, 10.7759/cureus.106746, (2026).
- Nobuaki Shime, Taka-aki Nakada, Tomoaki Yatabe, Kazuma Yamakawa, Yoshitaka Aoki, Shigeaki Inoue, Toshiaki Iba, Hiroshi Ogura, Yusuke Kawai, Atsushi Kawaguchi, Tatsuya Kawasaki, Yutaka Kondo, Masaaki Sakuraya, Shunsuke Taito, Kent Doi, Hideki Hashimoto, Yoshitaka Hara, Tatsuma Fukuda, Asako Matsushima, Moritoki Egi, Shigeki Kushimoto, Takehiko Oami, Kazuya Kikutani, Yuki Kotani, Gen Aikawa, Makoto Aoki, Masayuki Akatsuka, Hideki Asai, Toshikazu Abe, Yu Amemiya, Ryo Ishizawa, Tadashi Ishihara, Tadayoshi Ishimaru, Yusuke Itosu, Hiroyasu Inoue, Hisashi Imahase, Haruki Imura, Naoya Iwasaki, Noritaka Ushio, Masatoshi Uchida, Michiko Uchi, Takeshi Umegaki, Yutaka Umemura, Akira Endo, Marina Oi, Akira Ouchi, Itsuki Osawa, Yoshiyasu Oshima, Kohei Ota, Takanori Ohno, Yohei Okada, Hiromu Okano, Yoshihito Ogawa, Masahiro Kashiura, Daisuke Kasugai, Ken-ichi Kano, Ryo Kamidani, Akira Kawauchi, Sadatoshi Kawakami, Daisuke Kawakami, Yusuke Kawamura, Kenji Kandori, Yuki Kishihara, Sho Kimura, Kenji Kubo, Tomoki Kuribara, Hiroyuki Koami, Shigeru Koba, Takehito Sato, Ren Sato, Yusuke Sawada, Haruka Shida, Tadanaga Shimada, Motohiro Shimizu, Kazushige Shimizu, Takuto Shiraishi, Toru Shinkai, Akihito Tampo, Gaku Sugiura, Kensuke Sugimoto, Hiroshi Sugimoto, Tomohiro Suhara, Motohiro Sekino, Kenji Sonota, Mahoko Taito, Nozomi Takahashi, Jun Takeshita, Chikashi Takeda, Junko Tatsuno, Aiko Tanaka, Masanori Tani, Atsushi Tanikawa, Hao Chen, Takumi Tsuchida, Yusuke Tsutsumi, Takefumi Tsunemitsu, Ryo Deguchi, Kenichi Tetsuhara, Takero Terayama, Yuki Togami, Takaaki Totoki, Yoshinori Tomoda, Shunichiro Nakao, Hiroki Nagasawa, Yasuhisa Nakatani, Nobuto Nakanishi, Norihiro Nishioka, Mitsuaki Nishikimi, Satoko Noguchi, Suguru Nonami, Osamu Nomura, Katsuhiko Hashimoto, Junji Hatakeyama, Yasutaka Hamai, Mayu Hikone, Ryo Hisamune, Tomoya Hirose, Ryota Fuke, Ryo Fujii, Naoki Fujie, Jun Fujinaga, Yoshihisa Fujinami, Sho Fujiwara, Hiraku Funakoshi, Koichiro Homma, Yuto Makino, Hiroshi Matsuura, Ayaka Matsuoka, Tadashi Matsuoka, Yosuke Matsumura, Akito Mizuno, Sohma Miyamoto, Yukari Miyoshi, Satoshi Murata, Teppei Murata, Hiromasa Yakushiji, Shunsuke Yasuo, Kohei Yamada, Hiroyuki Yamada, Ryo Yamamoto, Ryohei Yamamoto, Tetsuya Yumoto, Yuji Yoshida, Shodai Yoshihiro, Satoshi Yoshimura, Jumpei Yoshimura, Hiroshi Yonekura, Yuki Wakabayashi, Takeshi Wada, Shinichi Watanabe, Atsuhiro Ijiri, Kei Ugata, Shuji Uda, Ryuta Onodera, Masaki Takahashi, Satoshi Nakajima, Junta Honda, Tsuguhiro Matsumoto, The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2024, Journal of Intensive Care, 10.1186/s40560-025-00776-0, 13, 1, (2025).
- Nobuaki Shime, Taka‐aki Nakada, Tomoaki Yatabe, Kazuma Yamakawa, Yoshitaka Aoki, Shigeaki Inoue, Toshiaki Iba, Hiroshi Ogura, Yusuke Kawai, Atsushi Kawaguchi, Tatsuya Kawasaki, Yutaka Kondo, Masaaki Sakuraya, Shunsuke Taito, Kent Doi, Hideki Hashimoto, Yoshitaka Hara, Tatsuma Fukuda, Asako Matsushima, Moritoki Egi, Shigeki Kushimoto, Takehiko Oami, Kazuya Kikutani, Yuki Kotani, Gen Aikawa, Makoto Aoki, Masayuki Akatsuka, Hideki Asai, Toshikazu Abe, Yu Amemiya, Ryo Ishizawa, Tadashi Ishihara, Tadayoshi Ishimaru, Yusuke Itosu, Hiroyasu Inoue, Hisashi Imahase, Haruki Imura, Naoya Iwasaki, Noritaka Ushio, Masatoshi Uchida, Michiko Uchi, Takeshi Umegaki, Yutaka Umemura, Akira Endo, Marina Oi, Akira Ouchi, Itsuki Osawa, Yoshiyasu Oshima, Kohei Ota, Takanori Ohno, Yohei Okada, Hiromu Okano, Yoshihito Ogawa, Masahiro Kashiura, Daisuke Kasugai, Ken‐ichi Kano, Ryo Kamidani, Akira Kawauchi, Sadatoshi Kawakami, Daisuke Kawakami, Yusuke Kawamura, Kenji Kandori, Yuki Kishihara, Sho Kimura, Kenji Kubo, Tomoki Kuribara, Hiroyuki Koami, Shigeru Koba, Takehito Sato, Ren Sato, Yusuke Sawada, Haruka Shida, Tadanaga Shimada, Motohiro Shimizu, Kazushige Shimizu, Takuto Shiraishi, Toru Shinkai, Akihito Tampo, Gaku Sugiura, Kensuke Sugimoto, Hiroshi Sugimoto, Tomohiro Suhara, Motohiro Sekino, Kenji Sonota, Mahoko Taito, Nozomi Takahashi, Jun Takeshita, Chikashi Takeda, Junko Tatsuno, Aiko Tanaka, Masanori Tani, Atsushi Tanikawa, Hao Chen, Takumi Tsuchida, Yusuke Tsutsumi, Takefumi Tsunemitsu, Ryo Deguchi, Kenichi Tetsuhara, Takero Terayama, Yuki Togami, Takaaki Totoki, Yoshinori Tomoda, Shunichiro Nakao, Hiroki Nagasawa, Yasuhisa Nakatani, Nobuto Nakanishi, Norihiro Nishioka, Mitsuaki Nishikimi, Satoko Noguchi, Suguru Nonami, Osamu Nomura, Katsuhiko Hashimoto, Junji Hatakeyama, Yasutaka Hamai, Mayu Hikone, Ryo Hisamune, Tomoya Hirose, Ryota Fuke, Ryo Fujii, Naoki Fujie, Jun Fujinaga, Yoshihisa Fujinami, Sho Fujiwara, Hiraku Funakoshi, Koichiro Homma, Yuto Makino, Hiroshi Matsuura, Ayaka Matsuoka, Tadashi Matsuoka, Yosuke Matsumura, Akito Mizuno, Sohma Miyamoto, Yukari Miyoshi, Satoshi Murata, Teppei Murata, Hiromasa Yakushiji, Shunsuke Yasuo, Kohei Yamada, Hiroyuki Yamada, Ryo Yamamoto, Ryohei Yamamoto, Tetsuya Yumoto, Yuji Yoshida, Shodai Yoshihiro, Satoshi Yoshimura, Jumpei Yoshimura, Hiroshi Yonekura, Yuki Wakabayashi, Takeshi Wada, Shinichi Watanabe, Atsuhiro Ijiri, Kei Ugata, Shuji Uda, Ryuta Onodera, Masaki Takahashi, Satoshi Nakajima, Junta Honda, Tsuguhiro Matsumoto, The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2024, Acute Medicine & Surgery, 10.1002/ams2.70037, 12, 1, (2025).
- Pan Zhang, Siyang Wang, Tingting Zhi, Naobei Ye, Haonan Sun, Xingyu Qin, Shuhan Xu, Ruiqin Zhang, Appropriateness and inappropriate medication predictors of stress ulcer prophylaxis in the intensive care unit, Frontiers in Pharmacology, 10.3389/fphar.2024.1401335, 15, (2025).
- Avery Parman, Jamie L. Miller, Stephen Neely, Peter N. Johnson, Neha Gupta, Rates of Stress Ulcer Prophylaxis Deprescribing in Children Receiving Usual versus High-Dose Corticosteroids in the Pediatric Intensive Care Unit with Status Asthmaticus, Hospital Pharmacy, 10.1177/00185787241267723, 59, 6, (677-683), (2024).
- Ingrid Toews, Salman Hussain, John L Z Nyirenda, Maria A Willis, Lucia Kantorová, Simona Slezáková, Minyahil Tadesse Boltena, John Victor Peter, Luis Eduardo Santos Fontes, Miloslav Klugar, Behnam Sadeghirad, Joerg J Meerpohl, Pharmacological interventions for preventing upper gastrointestinal bleeding in people admitted to intensive care units: a network meta-analysis, BMJ Evidence-Based Medicine, 10.1136/bmjebm-2024-112886, 30, 1, (22-35), (2024).
- Mark Borthwick, Anders Granholm, Søren Marker, Mette Krag, Theis Lange, Matt P. Wise, Stepani Bendel, Frederik Keus, Anne Berit Guttormsen, Joerg C. Schefold, Jørn Wetterslev, Anders Perner, Morten Hylander Møller, Associations between enteral nutrition and outcomes in the SUP‐ICU trial: Protocol for exploratory post hoc analyses , Acta Anaesthesiologica Scandinavica, 10.1111/aas.14194, 67, 4, (481-486), (2023).
- Alexa Rae Roberts, Meghan Roddy, Michael John Wilsey, Scott Daniel McKinley, Beatriz Sanchez-Teppa, Anthony Alexander Sochet, Stress Ulcer Prophylaxis for Critical Asthma, Pediatrics, 10.1542/peds.2021-054527, 149, 4, (2022).
- Moritoki Egi, Hiroshi Ogura, Tomoaki Yatabe, Kazuaki Atagi, Shigeaki Inoue, Toshiaki Iba, Yasuyuki Kakihana, Tatsuya Kawasaki, Shigeki Kushimoto, Yasuhiro Kuroda, Joji Kotani, Nobuaki Shime, Takumi Taniguchi, Ryosuke Tsuruta, Kent Doi, Matsuyuki Doi, Taka‐aki Nakada, Masaki Nakane, Seitaro Fujishima, Naoto Hosokawa, Yoshiki Masuda, Asako Matsushima, Naoyuki Matsuda, Kazuma Yamakawa, Yoshitaka Hara, Masaaki Sakuraya, Shinichiro Ohshimo, Yoshitaka Aoki, Mai Inada, Yutaka Umemura, Yusuke Kawai, Yutaka Kondo, Hiroki Saito, Shunsuke Taito, Chikashi Takeda, Takero Terayama, Hideo Tohira, Hideki Hashimoto, Kei Hayashida, Toru Hifumi, Tomoya Hirose, Tatsuma Fukuda, Tomoko Fujii, Shinya Miura, Hideto Yasuda, Toshikazu Abe, Kohkichi Andoh, Yuki Iida, Tadashi Ishihara, Kentaro Ide, Kenta Ito, Yusuke Ito, Yu Inata, Akemi Utsunomiya, Takeshi Unoki, Koji Endo, Akira Ouchi, Masayuki Ozaki, Satoshi Ono, Morihiro Katsura, Atsushi Kawaguchi, Yusuke Kawamura, Daisuke Kudo, Kenji Kubo, Kiyoyasu Kurahashi, Hideaki Sakuramoto, Akira Shimoyama, Takeshi Suzuki, Shusuke Sekine, Motohiro Sekino, Nozomi Takahashi, Sei Takahashi, Hiroshi Takahashi, Takashi Tagami, Goro Tajima, Hiroomi Tatsumi, Masanori Tani, Asuka Tsuchiya, Yusuke Tsutsumi, Takaki Naito, Masaharu Nagae, Ichiro Nagasawa, Kensuke Nakamura, Tetsuro Nishimura, Shin Nunomiya, Yasuhiro Norisue, Satoru Hashimoto, Daisuke Hasegawa, Junji Hatakeyama, Naoki Hara, Naoki Higashibeppu, Nana Furushima, Hirotaka Furusono, Yujiro Matsuishi, Tasuku Matsuyama, Yusuke Minematsu, Ryoichi Miyashita, Yuji Miyatake, Megumi Moriyasu, Toru Yamada, Hiroyuki Yamada, Ryo Yamamoto, Takeshi Yoshida, Yuhei Yoshida, Jumpei Yoshimura, Ryuichi Yotsumoto, Hiroshi Yonekura, Takeshi Wada, Eizo Watanabe, Makoto Aoki, Hideki Asai, Takakuni Abe, Yutaka Igarashi, Naoya Iguchi, Masami Ishikawa, Go Ishimaru, Shutaro Isokawa, Ryuta Itakura, Hisashi Imahase, Haruki Imura, Takashi Irinoda, Kenji Uehara, Noritaka Ushio, Takeshi Umegaki, Yuko Egawa, Yuki Enomoto, Kohei Ota, Yoshifumi Ohchi, Takanori Ohno, Hiroyuki Ohbe, Kazuyuki Oka, Nobunaga Okada, Yohei Okada, Hiromu Okano, Jun Okamoto, Hiroshi Okuda, Takayuki Ogura, Yu Onodera, Yuhta Oyama, Motoshi Kainuma, Eisuke Kako, Masahiro Kashiura, Hiromi Kato, Akihiro Kanaya, Tadashi Kaneko, Keita Kanehata, Ken‐ichi Kano, Hiroyuki Kawano, Kazuya Kikutani, Hitoshi Kikuchi, Takahiro Kido, Sho Kimura, Hiroyuki Koami, Daisuke Kobashi, Iwao Saiki, Masahito Sakai, Ayaka Sakamoto, Tetsuya Sato, Yasuhiro Shiga, Manabu Shimoto, Shinya Shimoyama, Tomohisa Shoko, Yoh Sugawara, Atsunori Sugita, Satoshi Suzuki, Yuji Suzuki, Tomohiro Suhara, Kenji Sonota, Shuhei Takauji, Kohei Takashima, Sho Takahashi, Yoko Takahashi, Jun Takeshita, Yuuki Tanaka, Akihito Tampo, Taichiro Tsunoyama, Kenichi Tetsuhara, Kentaro Tokunaga, Yoshihiro Tomioka, Kentaro Tomita, Naoki Tominaga, Mitsunobu Toyosaki, Yukitoshi Toyoda, Hiromichi Naito, Isao Nagata, Tadashi Nagato, Yoshimi Nakamura, Yuki Nakamori, Isao Nahara, Hiromu Naraba, Chihiro Narita, Norihiro Nishioka, Tomoya Nishimura, Kei Nishiyama, Tomohisa Nomura, Taiki Haga, Yoshihiro Hagiwara, Katsuhiko Hashimoto, Takeshi Hatachi, Toshiaki Hamasaki, Takuya Hayashi, Minoru Hayashi, Atsuki Hayamizu, Go Haraguchi, Yohei Hirano, Ryo Fujii, Motoki Fujita, Naoyuki Fujimura, Hiraku Funakoshi, Masahito Horiguchi, Jun Maki, Naohisa Masunaga, Yosuke Matsumura, Takuya Mayumi, Keisuke Minami, Yuya Miyazaki, Kazuyuki Miyamoto, Teppei Murata, Machi Yanai, Takao Yano, Kohei Yamada, Naoki Yamada, Tomonori Yamamoto, Shodai Yoshihiro, Hiroshi Tanaka, Osamu Nishida, The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2020 (J‐SSCG 2020), Acute Medicine & Surgery, 10.1002/ams2.659, 8, 1, (2021).
- Moritoki Egi, Hiroshi Ogura, Tomoaki Yatabe, Kazuaki Atagi, Shigeaki Inoue, Toshiaki Iba, Yasuyuki Kakihana, Tatsuya Kawasaki, Shigeki Kushimoto, Yasuhiro Kuroda, Joji Kotani, Nobuaki Shime, Takumi Taniguchi, Ryosuke Tsuruta, Kent Doi, Matsuyuki Doi, Taka-aki Nakada, Masaki Nakane, Seitaro Fujishima, Naoto Hosokawa, Yoshiki Masuda, Asako Matsushima, Naoyuki Matsuda, Kazuma Yamakawa, Yoshitaka Hara, Masaaki Sakuraya, Shinichiro Ohshimo, Yoshitaka Aoki, Mai Inada, Yutaka Umemura, Yusuke Kawai, Yutaka Kondo, Hiroki Saito, Shunsuke Taito, Chikashi Takeda, Takero Terayama, Hideo Tohira, Hideki Hashimoto, Kei Hayashida, Toru Hifumi, Tomoya Hirose, Tatsuma Fukuda, Tomoko Fujii, Shinya Miura, Hideto Yasuda, Toshikazu Abe, Kohkichi Andoh, Yuki Iida, Tadashi Ishihara, Kentaro Ide, Kenta Ito, Yusuke Ito, Yu Inata, Akemi Utsunomiya, Takeshi Unoki, Koji Endo, Akira Ouchi, Masayuki Ozaki, Satoshi Ono, Morihiro Katsura, Atsushi Kawaguchi, Yusuke Kawamura, Daisuke Kudo, Kenji Kubo, Kiyoyasu Kurahashi, Hideaki Sakuramoto, Akira Shimoyama, Takeshi Suzuki, Shusuke Sekine, Motohiro Sekino, Nozomi Takahashi, Sei Takahashi, Hiroshi Takahashi, Takashi Tagami, Goro Tajima, Hiroomi Tatsumi, Masanori Tani, Asuka Tsuchiya, Yusuke Tsutsumi, Takaki Naito, Masaharu Nagae, Ichiro Nagasawa, Kensuke Nakamura, Tetsuro Nishimura, Shin Nunomiya, Yasuhiro Norisue, Satoru Hashimoto, Daisuke Hasegawa, Junji Hatakeyama, Naoki Hara, Naoki Higashibeppu, Nana Furushima, Hirotaka Furusono, Yujiro Matsuishi, Tasuku Matsuyama, Yusuke Minematsu, Ryoichi Miyashita, Yuji Miyatake, Megumi Moriyasu, Toru Yamada, Hiroyuki Yamada, Ryo Yamamoto, Takeshi Yoshida, Yuhei Yoshida, Jumpei Yoshimura, Ryuichi Yotsumoto, Hiroshi Yonekura, Takeshi Wada, Eizo Watanabe, Makoto Aoki, Hideki Asai, Takakuni Abe, Yutaka Igarashi, Naoya Iguchi, Masami Ishikawa, Go Ishimaru, Shutaro Isokawa, Ryuta Itakura, Hisashi Imahase, Haruki Imura, Takashi Irinoda, Kenji Uehara, Noritaka Ushio, Takeshi Umegaki, Yuko Egawa, Yuki Enomoto, Kohei Ota, Yoshifumi Ohchi, Takanori Ohno, Hiroyuki Ohbe, Kazuyuki Oka, Nobunaga Okada, Yohei Okada, Hiromu Okano, Jun Okamoto, Hiroshi Okuda, Takayuki Ogura, Yu Onodera, Yuhta Oyama, Motoshi Kainuma, Eisuke Kako, Masahiro Kashiura, Hiromi Kato, Akihiro Kanaya, Tadashi Kaneko, Keita Kanehata, Ken-ichi Kano, Hiroyuki Kawano, Kazuya Kikutani, Hitoshi Kikuchi, Takahiro Kido, Sho Kimura, Hiroyuki Koami, Daisuke Kobashi, Iwao Saiki, Masahito Sakai, Ayaka Sakamoto, Tetsuya Sato, Yasuhiro Shiga, Manabu Shimoto, Shinya Shimoyama, Tomohisa Shoko, Yoh Sugawara, Atsunori Sugita, Satoshi Suzuki, Yuji Suzuki, Tomohiro Suhara, Kenji Sonota, Shuhei Takauji, Kohei Takashima, Sho Takahashi, Yoko Takahashi, Jun Takeshita, Yuuki Tanaka, Akihito Tampo, Taichiro Tsunoyama, Kenichi Tetsuhara, Kentaro Tokunaga, Yoshihiro Tomioka, Kentaro Tomita, Naoki Tominaga, Mitsunobu Toyosaki, Yukitoshi Toyoda, Hiromichi Naito, Isao Nagata, Tadashi Nagato, Yoshimi Nakamura, Yuki Nakamori, Isao Nahara, Hiromu Naraba, Chihiro Narita, Norihiro Nishioka, Tomoya Nishimura, Kei Nishiyama, Tomohisa Nomura, Taiki Haga, Yoshihiro Hagiwara, Katsuhiko Hashimoto, Takeshi Hatachi, Toshiaki Hamasaki, Takuya Hayashi, Minoru Hayashi, Atsuki Hayamizu, Go Haraguchi, Yohei Hirano, Ryo Fujii, Motoki Fujita, Naoyuki Fujimura, Hiraku Funakoshi, Masahito Horiguchi, Jun Maki, Naohisa Masunaga, Yosuke Matsumura, Takuya Mayumi, Keisuke Minami, Yuya Miyazaki, Kazuyuki Miyamoto, Teppei Murata, Machi Yanai, Takao Yano, Kohei Yamada, Naoki Yamada, Tomonori Yamamoto, Shodai Yoshihiro, Hiroshi Tanaka, Osamu Nishida, The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2020 (J-SSCG 2020), Journal of Intensive Care, 10.1186/s40560-021-00555-7, 9, 1, (2021).