Cost assessment of treatment of acute myocardial infarction and angiographically visible coronary thrombus
Abstract
Aim: Study was aimed to assess the real-world costs of manual thrombectomy (MT) in selected ST-segment elevation myocardial infarction patients with intracoronary thrombus (IT). Methods: Study group (IT+) comprised 51 patients with MT applied and control group (IT-) comprised 56 patients without IT who underwent angioplasty alone. Costs comprised hospital care and cost of disposable materials used during primary angioplasty. Results: Complex management of patients with IT is more expensive, though allows to achieve clinical outcomes comparable to low-risk ST-segment elevation myocardial infarction patients without IT. Conclusion: A complex pharmaco-interventional strategy, with glycoprotein IIB/IIIA inhibitor and MT, though more expensive, may prove cost-effective.
ST-segment elevation myocardial infarction (STEMI) is one of the leading causes of mortality and morbidity. Despite the tendency to reduce mortality observed in recent years, the number of deaths remains high. Myocardial infarction survivors might have impaired left ventricle systolic function and they frequently develop overt heart failure or arrhythmia [1].
The preferred method of treatment of patients with STEMI is the primary percutaneous angioplasty, which is aimed at restoration of a normal blood flow at the level of coronary microcirculation [2]. Despite the great development in the interventional procedures, a large percentage of patients treated with percutaneous coronary intervention (PCI), has microcirculation impairment in the infarct area. One of the causes of this condition is thrombus covering ruptured atherosclerotic plaque clearly seen in the coronary angiogram. Patients with STEMI and visible thrombus in the culprit artery are predisposed to restenosis, peripheral embolism, slow-flow syndrome, no-reflow phenomenon and postprocedural heart failure. Larger thrombus is correlated with higher mortality, worse immediate results of angioplasty and worse long-term outcomes [3–5].
Several approaches of thrombus removal were examined, but the use of distal protection devices or mechanical thrombectomy is no longer recommended [2]. Intravenous or intracoronary administration of glycoprotein IIB/IIIA inhibitors is fully justified in patients with massive intracoronary thrombus (IT) [2]. Manual thrombectomy (MT), though recommendations for its application were downgraded after publication of results of the TASTE trial [6], it still might be considered in selected population of patients [7]. Noman et al. [8] in their retrospective analysis of factors favored the use of MT in STEMI patients and have identified operator- and procedure-related predictors like: operator's experience, his volume, vessel diameter, lesion length and initial epicardial flow thrombolysis in myocardial infarction (TIMI) 0/I. In the long run, they have reported on significantly reduced mortality in the group of STEMI patients in whom adjunctive MT was applied. Thus, nonroutine, selective use of MT in high-risk STEMI patients is in line with current recommendations and seems to offer benefit for these patients. MT might offer another cost-effective gain by substitution of balloon predilation during primary angioplasty [9]. We can assume then that STEMI patients with large thrombus burden are a high-risk population and require more intensive pharmacotherapy, more sophisticated interventional armamentarium, thus consume more of the financial resources. So far, we have not found any data addressing the cost–effectiveness of complex management of selected STEMI patients with large thrombus burden with adjunctive MT during primary angioplasty. The aim of the study was to assess the real-world costs of treatment of patients with angiographically visible thrombus in comparison to cost of treatment of patients without thrombus.
Materials & methods
Study population
A total of 107 patients with STEMI between January 2009 and January 2012 were enrolled into this case–control study (Figure 1). Our department serves a 24-h primary PCI service for a population of >400,000 people. Diagnosis of STEMI was based on chest pain lasting more than 20 min, ST-segment elevation in electrocardiography or positive findings for myocardial necrosis markers. Clinical, demographic, angiographic and data relevant to invasive strategy were obtained from medical records and from repeat review of archived angiographies. Study group comprised 51 patients with angiographic evidence of thrombus in culprit coronary artery. These were all patients in whom MT was applied after exclusion of patients with missing data. Control group comprised 56 patients without visible thrombus in culprit artery who were matched using propensity score matching for age and culprit vessel. MT preceded further angioplasty in study group; patients from control group underwent angioplasty alone.
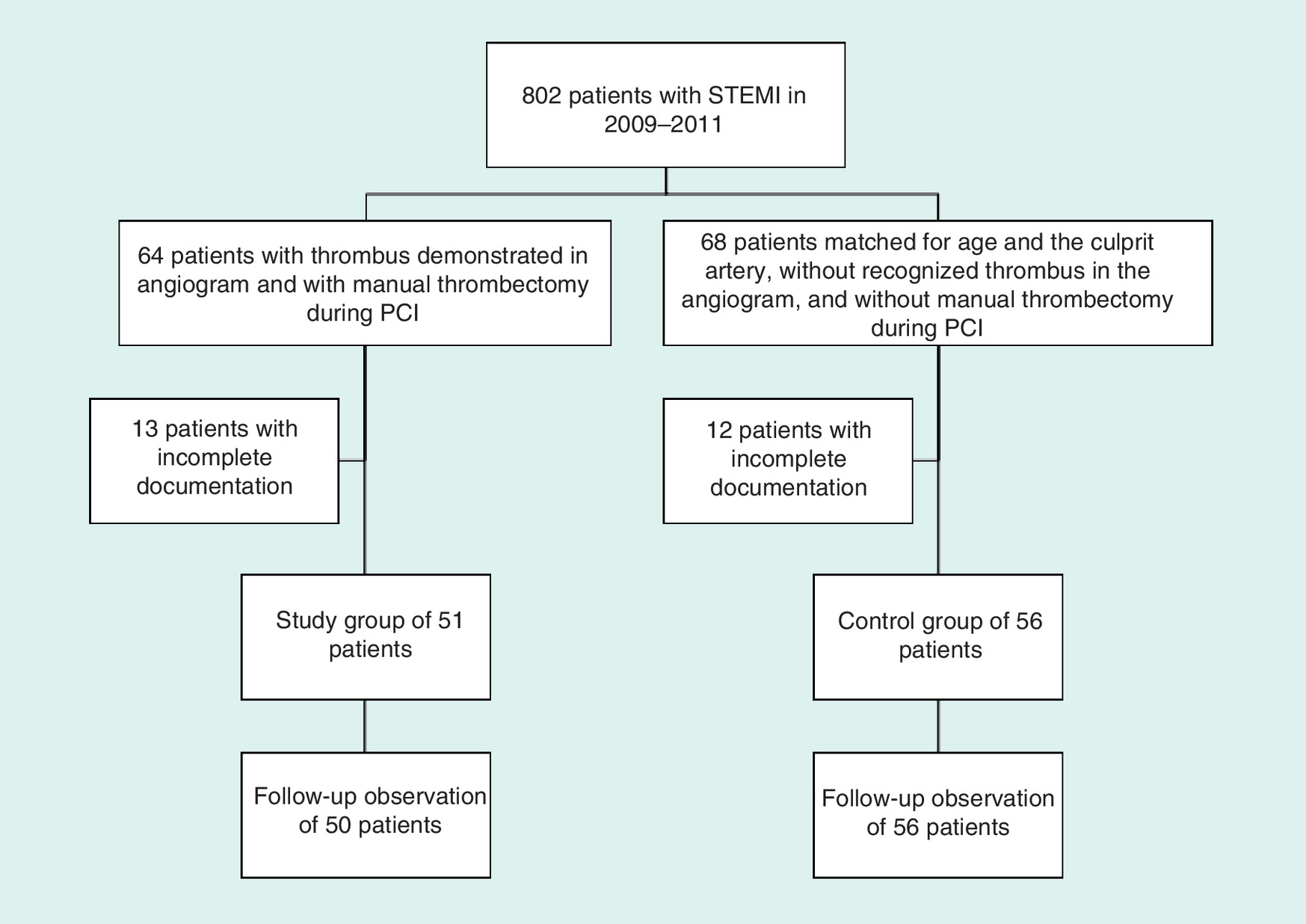
Figure 1. Study flow chart.
PCI: Percutaneous coronary intervention; STEMI: ST-segment elevation myocardial infarction.
We have used TIMI flow definitions for describing pre- and post-PCI epicardial flow [10]. For thrombus classification we have used a score proposed by Gibson et al. [5]. In patients presenting with an occluded infarct-related artery (grade 5 thrombus, essentially no flow), thrombus was reclassified into one of the other categories after flow achievement with either guidewire crossing or a small (diameter 1.5 mm) deflated balloon passage or dilation [4]. Myocardial blush grade was evaluated according to Van't Hof et al. [11] and was judged in the final angiogram. Myocardial perfusion was assessed electrocardiographically according to Van't Hof et al. [12]. For assessment of infarct size we utilized peak activity of creatine kinase and troponin (T) concentration area under the curve (AUC) measured at admission, at 12, 22 and 72 h. AUC was calculated with formula:
TpAUC = 0.5*Tp0 + 0.5*Abs(Tp12 - Tp0) + 0.5*Tp12 + 0.5*Abs(Tp24 - Tp12) + 2*Tp72 + Abs(Tp72 - Tp24), where Tp0, Tp12, Tp24 and Tp72 are respective troponin concentrations, and Abs is the absolute value of the subtraction. AUC was expressed in ng/l*24 h.
Informed, written consent was obtained from all participants. The study was approved by Bioethics Committee at Medical University of Silesia.
Long-term outcomes
Patient's follow-up was based on in person outpatient visits and telephone contacts. Major adverse cardiovascular events were recorded. In just a few cases of patients in which we could not contact them, we have asked National Health Fund for their vital status. All-cause deaths, reinfarction, target vessel revascularization and a sum of these events were considered as complete observations. Follow-up was censored at 48 months in January 2016.
Cost assessment & simulation of cost–effectiveness analysis
We have used real-world cost and have presented them as hospital expenditures. They were calculated directly for each individual patient, summing up number of person-days spent in hospital with cost of disposable materials used during primary angioplasty. All disposable materials, radiographic contrast and glycoprotein IIB/IIIA inhibitors were acquired by tendering. The prices analyzed are the net prices and are presented in Polish zloty's (PLN). In the period 2009–2012, three types of aspiration catheters were used: Hunter (IHT Cordynamic, Barcelona, Spain), Diver CE (Invatec Innovative Technologies, Roncadelle, Italy) and Export (Medtronic, MN, USA). Their net price ranged between 590.00 and 665.00 PLN. The use of adjunctive thrombectomy was at the operator's decision and the type of aspiration catheter available at the shelf. The use of abciximab or integriline was at the operator's choice. Cost–effectiveness ratio was calculated with equation:
where CIT+ is the total cost of treatment of study group, CIT- is total cost of treatment of control group, MACEIT+ is number of major adverse cardiovascular events (MACE) in study group during follow-up, and MACEIT- is number of MACE in control group in follow-up [13]. Cost–effectiveness ratio was calculated for all-cause mortality, target-vessel revascularization and cumulative MACE. It was unaccountable for reinfarction, because in follow-up equal number of reinfarctions occurred in both groups, thus denominator was zero. It is presented as the sum of money spent for saving one life, for prevention of one target vessel revascularization and for prevention of one episode of cumulative MACE.
Statistical analysis
For the purpose of this analysis we have selected all the patients in whom MT was used, control group was selected from the remaining STEMI patients using propensity score matching for age and culprit vessel in 1:1 proportion and applying the nearest neighbor rule. Quantitative data are presented as the means and standard deviations, and categorical data are presented as numbers and percentages. Data were analyzed for normal distribution with the Kolmogorov–Smirnov test and for homogeneity of variances with Levene's test. Groups were compared with a Student's t-test, Mann–Whitney U test or χ2 test with Yates correction. Nonparametric correlation as well as linear regression analysis was used to assess relationships between the variables. Kaplan–Meier survival analysis with log-rank test was used to compare the incidence of major adverse cardiovascular events between the groups in the follow-up. Cox proportional hazard modeling was used to analyze the predictors of long-term prognosis. Differences in the means or frequencies were considered significant when p < 0.05. Statistica 12 (Statsoft Inc., OK, USA), equipped with the Medical Package (Statsoft Polska, Kraków, Poland) was used for data analysis.
Results
Baseline presentation & procedural results
Both groups were well matched according to clinical and demographic baseline characteristics (Table 1). Both groups had similar number of diseased vessels. The groups were different according to initial TIMI thrombus score and TIMI flow classification: TIMI flow 0 was significantly more frequently observed in study group. There was longer fluoroscopy time and radiation dose in study group. Abciximab was more frequently administered in the study group. There was a comparable rate of direct stent implantation in both groups. Final TIMI flow was comparable in both groups. Myocardial perfusion grade (MBG) 3 was achieved in 18 patients from study group and 35 patients from control group. Study group had significantly higher rate of angiographically visible distal embolization (Table 2). Complete ST resolution was observed in 20 patients from study group and 34 patients from control group. Peak CKMB activity and AUC of troponin concentration were similar in both groups (Table 3).
| Patient characteristic | Study group, IT+ (n = 51) | Control group, IT- (n = 56) | χ2 | Student's t-test |
|---|---|---|---|---|
| Age, years, X ± SD | 63.9 ± 12.6 | 64.4 ± 10.8 | – | NS |
| Sex (M/F) | 34/17 | 37/19 | NS | – |
| Hypertension, n (%) | 41 (80.4) | 33 (56.9) | 0.0284 | – |
| Diabetes, n (%) | 19 (37.3) | 16 (28.5) | NS | – |
| Smoking, n (%) | 19 (37.3) | 26 (46.4) | NS | – |
| Family history, n (%) | 17 (33.2) | 23 (41.1) | NS | – |
| Prior myocardial infarction, n (%) | 11 (21.6) | 9 (16.1) | NS | – |
| Prior PCI, n (%) | 11 (21.6) | 9 (16.1) | NS | – |
| Prior CABG, n (%) | 2 (3.9) | 1 (1.8) | NS | – |
| Valvular heart diseases, n (%) | 9 (17.6) | 6 (10.7) | NS | – |
| Atrial fibrillation, n (%) | 5 (9.8) | 6 (10.7) | NS | – |
| Clinical and laboratory data | ||||
| BMI (kg/m2) | 28.5 ± 4.3 | 28.2 ± 6.2 | – | NS |
| Blood pressure (mmHg): – Systolic – Diastolic | 131.4 ± 34.2 81.5 ± 24.3 | 133.3 ± 38.7 77.8 ± 21.6 | – – | NS NS |
| Heart rate at admission (beats per min) | 78.8 ± 19.2 | 77.6 ± 21.1 | – | NS |
| Duration of infarction (min) | 261 ± 107 | 252 ± 93 | – | NS |
| Killip classification; n (%): – Killip I – Killip II–IV | 49 (96.1) 2 (3.9) | 54 (96.4) 2 (3.6) | NS – | – – |
| LVEF (%), X ± SD | 44.9 ± 10.8 | 45.0 ± 11.7 | – | NS |
| Creatinine, μmol/l, X ± SD | 79.4 ± 17.2 | 83.4 ± 20.9 | – | NS |
| Total cholesterol (mg %), X ± SD | 212.4 ± 64.2 | 204.3 ± 67.9 | – | NS |
| HDL cholesterol (mg %), X ± SD | 43.2 ± 12.3 | 40.4 ± 11.9 | – | NS |
| Triglycerides (mg %), X ± SD | 189.2 ± 164.2 | 168.7 ± 155.8 | – | NS |
| Drugs at discharge | ||||
| Acetylsalicylic acid; n (%) | 51 (100) | 56 (100) | NS | – |
| Beta-adrenergic blockers, n (%) | 49 (96.08) | 51 (91.07) | NS | – |
| ACEI; n (%) | 43 (84.31) | 53 (94.64) | NS | – |
| Statin; n (%) | 46 (90.2) | 54 (96.42) | NS | – |
| Clopidogrel; n (%) | 51 (100) | 56 (100) | NS | – |
| Diuretics; n (%) thiazide Potassium-sparing | 7 (13.72) 13 (25.49) | 14 (25.00) 12 (24.21) | NS NS | – – |
ACEI: Angiotensin-converting enzyme inhibitor; CABG: Coronary artery bypass graft operation; HDL: High-density lipoprotein; IT: Intracoronary thrombus; LVEF: Left ventricle ejection fraction; NS: Not significant; PCI: Percutaneous coronary intervention.
| Angiographic data | Study group, IT+ (n = 51) | Control group, IT- (n = 56) | χ2 |
|---|---|---|---|
| Coronary arteries with stenosis n (%): | |||
| – 1 | 7 (13.73) | 17 (30.36) | NS |
| – 2 | 15 (29.41) | 15 (26.79) | NS |
| – 3 | 17 (33.33) | 10 (17.86) | NS |
| – ≥4 | 12 (23.53) | 14 (25.0) | NS |
| Culprit artery n (%): | |||
| – LAD | 19 (37.25) | 26 (46.43) | NS |
| – Cx | 5 (9.80) | 11 (19.64) | NS |
| – RCA | 27 (52.95) | 19 (33.93) | NS |
| Initial flow in the culprit artery in TIMI classification; n (%): | |||
| – 0 | 39 (76.47) | 22 (39.29) | 0.0002 |
| – I | 2 (3.92) | 5 (8.93) | NS |
| – II | 4 (7.84) | 8 (14.23) | NS |
| – III | 6 (11.77) | 21 (37.5) | 0.005 |
| Thrombus in culprit artery in TIMI classification; n (%): | |||
| – TIMI 0 | 0 (0) | 33 (58.92) | 0.0000 |
| – TIMI I | 0 (0) | 1 (1.79) | NS |
| – TIMI II | 2 (3.92) | 0 (0) | 0.0000 |
| – TIMI III | 7 (13.73) | 0 (0) | 0.0000 |
| – TIMI IV | 3 (5.88) | 0 (0) | 0.0000 |
| TIMI V, including reclassification: | 39 (76.47) | 22 (39.29) | NS |
| – TIMI 0 | 0 (0) | 23 (41.07) | 0.0000 |
| – TIMI I | 0 (0) | 0 (0) | NS |
| – TIMI II | 10 (19.61) | 0 (0) | 0.0000 |
| – TIMI III | 10 (19.61) | 0 (0) | 0.0000 |
| – TIMI IV | 19 (37.25) | 0 (0) | 0.0000 |
| Duration of the procedure (min), X ± SD | 55.42 ± 23.96 | 56.44 ± 36.05 | NS† |
| Fluoroscopy time (min), X ± SD | 8.8 ± 3.4 | 7.3 ± 2.6 | 0.025† |
| Radiation dose (mGy), X ± SD | 1527.4 ± 873.8 | 1024.2 ± 645.1 | 0.0069† |
| Contrast used (ml), X ± SD | 199 ± 78 | 180 ± 77 | NS |
| Number of patients with glycoprotein IIB/IIIA inhibitor; n (%), including: | 31 (60.8) | 15 (26.8) | 0.0000 |
| – Abciximab | 21 (41.78) | 9 (16.07) | 0.008 |
| – Integrilin | 10 (19.61) | 6 (10.73) | NS |
| Direct stenting; n (%) | 10 (19.61) | 11 (19.64) | NS |
| Patients with balloon predilatation during angioplasty; n (%), including: | |||
| – 0 balloon | 13 (25.49) | 14 (25.00) | NS |
| – 1 balloon | 21 (41.18) | 22 (39.29) | NS |
| – 2 balloons | 13 (25.49) | 15 (26.79) | NS |
| – 3 balloons | 2 (3.92) | 1 (1.79) | NS |
| – ≥4 balloons | 2 (3.92) | 4 (7.13) | NS |
| Patients with stent implantation; n (%) including: | 42 (82.35) | 46 (82.14) | NS |
| – 1 stent | 25 (49.01) | 30 (53.57) | NS |
| – 2 stents | 14 (27.45) | 14 (25.00) | NS |
| – 3 stents | 2 (3.92) | 1 (1.79) | NS |
| – 4 stents | 1 (1.96) | 1 (1.79) | NS |
| Patients with drug-eluting stent implantation n (%) | 5 (9.80) | 8 (14.23) | NS |
| Patients with IABP; n (%) | 2 (3.92) | 2 (3.57) | NS |
| Final flow in culprit artery in TIMI classification (%): | |||
| – 0 | 2 (3.92) | 5 (8.93) | NS |
| – I | 3 (5.88) | 1 (1.79) | NS |
| – II | 12 (23.53) | 5 (8.92) | NS |
| – III | 34 (66.67) | 45 (80.36) | NS |
| Myocardial blush grade MBG after the procedure; n (%): | |||
| – 0 | 9 (17.65) | 6 (10.71) | NS |
| – 1 | 8 (15.69) | 5 (8.93) | NS |
| – 2 | 16 (31.37) | 10 (17.86) | NS |
| – 3 | 18 (35.29) | 35 (62.5) | 0.009 |
| Patients with peripheral embolism; n (%) | 18 (35.29) | 10 (17.86) | 0.009 |
| Patients with angiographic success; n (%) | 32 (62.75) | 45 (80.36) | NS |
†Mann–Whitney U test.
Cx: Circumflex artery; IABP: Intra-aortic balloon pump; IT: Intracoronary thrombus; LAD: Left-anterior descending artery; MBG: Myocardial perfusion grade; NS: Not significant; RCA: Right coronary artery; SD: Standard deviation; TIMI: Thrombolysis in myocardial infarction.
| Myocardial perfusion/infarct size | Study group, IT+ (n = 51) | Control group, IT- (n = 56) | Mann–Whitney U test |
|---|---|---|---|
| ST-segment resolution; n (%): | |||
| – None | 17 (32.5) | 11 (20.0) | 0.0426† |
| – Partial | 14 (27.5) | 11 (20.0) | – |
| – Complete | 20 (40.0) | 34 (60.0) | – |
| CKMB at admission (IU/l), X ± SD | 120.7 ± 177 | 142.2 ± 233 | NS |
| CKMB max (IU/l), X ± SD | 198.0 ± 191 | 219 ± 275 | NS |
| Troponin at admission (ng/l), X ± SD | 1340.8 ± 2497.1 | 2214.5 ± 4431.1 | NS |
| Troponin 12 h (ng/l), X ± SD | 2354.9 ± 2504.6*p < 0.001 | 4230.6 ± 6578.1#p < 0.001 | NS |
| Troponin 24 h (ng/l), X ± SD | 4066.7 ± 3314.8*p = 0.005 | 3617.0 ± 5307.6#p = 0.036 | NS |
| Troponin 72 h (ng/l), X ± SD | 944.5 927.2*p = 0.5000 | 1498.2 ± 1672.4#p = 0.237 | NS |
| Troponin AUC over time 0–72 h (ng/l*24 h), X ± SD | 79,591.6 ± 69796.6 | 124,198.5 ± 116,042.4 | NS |
†χ2 test.
*Significance in comparison to troponin at admission in study group.
#Significance in comparison to troponin at admission in control group.
AUC: Area under the curve; NS: Not significant; SD: Standard deviation.
Length of hospital stay in study group was 2.2 days (27.5%) longer in comparison to control group (10.2 ± 7.1 vs 8.0 ± 6.4; p = 0.0019; Table 4). Age and the duration of invasive procedure were independent predictors of the length of hospital stay.
| Duration and cost of hospitalization | Study group, IT+ (n = 51) | Control group, IT- (n = 56) | Mann–Whitney U test |
|---|---|---|---|
| Duration of hospitalization (days), X ± SD | 10.2 ± 7.1 | 8.0 ± 6.4 | 0.0019 |
| Cost of hospitalization in the ward (PLN), X ± SD | 3902.0 ± 2722 | 3050.4 ± 2421.6 | 0.017 |
| The total cost per patient (PLN), X ± SD | 6761.85 ± 3224.55 | 5048.25 ± 3264.55 | 0.007 |
PLN: Polish zloty; SD: Standard deviation.
Long-term outcomes
Mean follow-up was 639.1 ± 431.7 days and the longest observation time was 1412 days. There was no MACE observed during hospital stay. In the follow-up, seven deaths, ten repeat myocardial infarctions and 19 repeat target-vessel revascularizations occurred (Table 5).
| MACE n (%) | Study group, IT+ (n = 51) | Control group, IT- (n = 56) | Difference, IT+ - IT- | CER (PLN) | Dominance |
|---|---|---|---|---|---|
| Deaths during hospitalization | 0 | 0 | NA | NA | – |
| Reinfarctions during hospitalization | 0 | 0 | NA | NA | – |
| Repeat culprit artery revascularization during hospitalization | 0 | 0 | NA | NA | – |
| Adverse events during hospitalization | 0 | 0 | NA | NA | – |
| Deaths in follow-up | 4 (8.0) | 3 (5.34) | 1 | 62,152.35 | – |
| Reinfarctions in follow-up | 5 (10) | 5 (9) | 0 | NA | – |
| Repeat culprit artery revascularization in follow-up | 7 (14) | 12 (21.4) | -5 | -12,430.47 | No |
| Adverse events in follow-up | 11 (22.0) | 15 (26.8) | -4 | -15,538.09 | No |
| Total cost of treatment of entire group (PLN) | 344,854.35 | 282,702.00 | 62,152.35 | – | – |
CER: Cost–effectiveness ratio; MACE: Major adverse cardiovascular events; NA: Not available; PLN: Polish zloty.
Kaplan–Meier analysis did not reveal any differences between the groups in the rate of MACE (Figure 2).
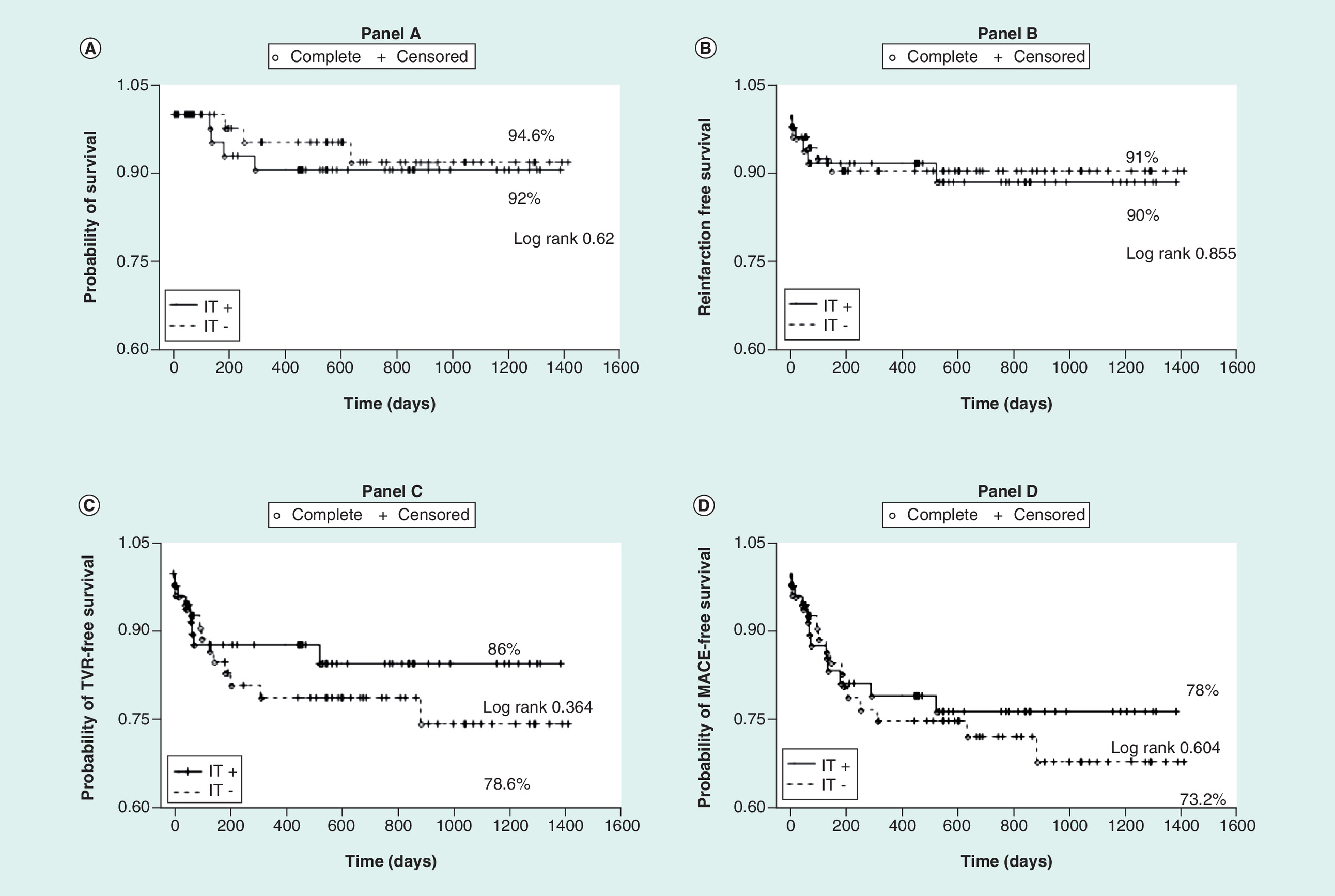
Figure 2. Kaplan–Meier event free survival curves.
(A) Overall survival; (B) reinfarction-free survival; (C) target-vessel revascularization-free survival; and (D) composite event-free survival.
IT: Intracoronary thrombus; MACE: Major adverse cardiovascular events; TVR: Target-vessel revascularization.
Univariate Cox proportional hazard analysis disclosed age, female gender, number of diseased vessels and diabetes as risk factors of death, however, the only independent factors in multivariate analysis were age and diabetes. The risk factors of MACE occurrence in the follow-up are impaired myocardial perfusion MBG <3 and lack of angiographic success in univariate analysis, whereas MBG <3 continues to affect the long-term outcome in multivariate analysis.
Costs & simulation of cost–effectiveness analysis
Length of hospital stay directly translates to the cost of hospital stay (3902 ± 2722 PLN vs 3050.4 ± 2421.6; p = 0.017 in study vs control group respectively; see Table 4). Summing up with procedural costs increases the whole expenses further by 2859.85 PLN in study group, and by 1997.85 PLN in control group. Treatment of patients from study group is higher by 1713.6 PLN than treatment of control group patients.
Procedural expenses are minor component of the global costs, hospital care expenses are dominant cost-consuming elements. While the complex management of patients with IT is financially ineffective in saving lives, though it is cost-effective in preventing one target vessel revascularization (saves -12,430.47 PLN) and preventing one cumulative major adverse cardiovascular events in the 4 year long follow-up (saves -15,538.09 PLN; see Table 5).
Discussion
To our knowledge this is a first study assessing the costs of interventional treatment of high-risk STEMI patients with IT. We have shown that despite the worse direct results of primary coronary angioplasty and higher hospitalization and treatment costs, the long-term outcomes in the study and control groups are comparable. Moreover, in our robust simulation of cost–effectiveness analysis, costly complex treatment initially, turns out to be cost-effective eventually in preventing repeat target vessel revascularization and avoiding cumulative MACE. As a complex treatment we recognize use of glycoprotein IIB/IIIA inhibitor and MT as adjunct to angioplasty. We have used two inhibitors in our study: abciximab or eptifibatide. Based on our results, we are not able to point out which of them is better or safer from clinical perspective. The evidence of equal efficacy of both drugs comes from several studies. Either Zeymer et al. [14] or Singh et al. [15] in their randomized comparisons of abciximab and eptifibatide, have concluded that both of the drugs are comparably effective in completely reducing ST-segment elevation, have comparable long-term incidence of major adverse cardiovascular events and have similar safety profile with comparable incidence of bleeding. Thus, eptifibatide being much cheaper than abciximab on Polish pharmaceutical market, may be an attractive, cost saving alternative in the treatment of high-risk STEMI patients. Complete cost–effectiveness analysis of the use of eptifibatide as an adjunct therapy to high-risk percutaneous coronary angioplasty was published recently [16]. Dewilde et al. have analyzed the subpopulation of high-risk patients undergoing implantation of stent from the ESPRIT trial [17] with patient-level utility data from a published Dutch study [18]. The authors have concluded that eptifibatide is likely to be a dominant strategy leading to quality-adjusted life years gained and generating cost savings from both the hospital and the third-party payer perspective. Eptifibatide offsets its additional treatment costs by avoiding costly repeat procedures and leads to positive quality-adjusted life years gained by preventing cardiovascular events lending themselves to transient or permanent lower quality of life [16]. However, the direct translation of these results into clinical practice of STEMI management is impossible, because of completely different populations in our and ESPRIT studies, the advent of drug eluting stent era, new oral antiplatelet drugs and recommendation for transradial access with reduced bleeding risk [19].
The second issue in selecting the right gear for complex primary PCI is the effectiveness of MT in removing or reducing the thrombus burden. We have used three different aspiration catheters similar to glycoprotein IIB/IIIA inhibitors, we are not able to recommend the most effective one. While in vivo comparison of two aspiration catheters by Vlaar et al. [20] has proven their equal effectiveness, in vitro tests have shown their limited and diverse effectiveness in thrombus removal [21,22]. The optical coherence tomography substudy of the TOTAL trial has failed to show the improved reduction of thrombus burden with the use of MT over the angioplasty alone [23]. In line with these observations, several papers have been published, which have documented effectiveness of sequential approach with more than one device [24,25] or successful use of extension ‘mother-and-child’ catheter for effective thrombus removal [26]. It is obvious that the use of multiple aspiration catheters or even single extension catheter (which is much more expensive than aspiration catheters in Poland) will increase procedural cost.
The costs of hospital stay constitute the majority (∼60%) of hospital expenses in our study. As they are related to patient's age and invasive procedure duration, we have no significant influence on these variables. Indeed, from the hospital's perspective early discharge would have tremendous impact on cost savings. We may only suggest that younger patients with uncomplicated primary angioplasty may be the candidates for early discharge, but we are not able to provide precise cut-off values for age and duration of angioplasty to be valid indicators. There are several publications [27–29] which give some hints on identification of postinfarction patients feasible for early discharge. Jones et al. [28] suggest that discharge of low-risk patients even 2 days after successful primary PCI is feasible and safe.
Conclusion
Complex pharmaco-interventional strategy, with glycoprotein IIB/IIA inhibitor and MT, in high-risk STEMI patients with IT has worse immediate outcomes and is more expensive, though it allows to achieve clinical outcomes comparable to a low-risk STEMI patients without IT.
Future perspective
So far, we have shown that complex pharmaco-interventional strategy (with one of the two glycoprotein IIB/IIA inhibitors and any of the three aspiration catheters used in this study) in high-risk STEMI patients although more expensive yet allow to achieve clinical outcomes comparable to low-risk STEMI patients. Because of a series of uncertainties concerning the use of less expensive eptifibatide, use of single dedicated, yet of questionable efficacy aspiration catheter, facing the growing evidence of successful thrombus removal with more than one device, we should revisit our strategy. Thoroughly designed prospective, randomized trial focusing on following issues: multicentricity, pharmacologic approach, thrombus removal and cost–effectiveness analysis would provide the best answer to the aforementioned doubts. Multicentricity is important for significant variability in costs reported for interventional procedures reported by different cath labs [30]. The suggested pharmacologic approach should comprise unfractionated heparin, double bolus of eptifibatide and ticagrelor. Procedural protocol should recommend radial access with 6F sheath and guiding catheter. If TIMI flow 0 or I persists after wiring the occlusion, than 6F compatible dedicated aspiration catheter should be used, and if unsuccessful, sequential use of extension catheter should be attempted. Balloon predilation should be considered to allow crossing the occlusion with thrombectomy/extension catheter. Prospective follow-up of patients should comprise more different end points like new-onset heart failure, and should include safety data on bleeding. Cost–effectiveness analysis should be based on quality-adjusted life years gained and present both financial perspectives either of hospital or insurance provider.
Limitations of the study
There are several limitations of our study which we have to acknowledge. First, we have enrolled small number of patients, thus study may be underpowered to detect real differences in incidences of major adverse cardiovascular events. Second, we have calculated costs of primary treatment during the index hospital stay, thus we are not able to infer on the costs of subsequent unplanned hospital admissions, outpatient visit, sick leaves and the respective economic load of insurance provider. Third, retrospective model of our study allows us to calculate cost savings of prevention of repeat ischemia-driven target vessel revascularization or MACE and the most reliable assessment of cost–effectiveness is quality-adjusted life years gained analysis. Fourth, we do not have the reference group of patients with IT who were treated with angioplasty alone. Since we have introduced thrombectomy to our cath lab, it is used in justified cases and there are no patients with thrombus who would not have adjunctive thrombectomy applied during the study period. We have such patients who were treated with angioplasty only, but this is a case before year 2009. Though, the issue is that when we have analyzed the suitability of this population of patients for comparison we have found substantial differences in their pharmacological and interventional treatment.
We have assessed the real-world costs of manual thrombectomy (MT) in selected ST-segment elevation myocardial infarction patients.
Management of patients with intracoronary thrombus is cost-consuming due to higher cost of procedural resources and longer hospital stay.
Complex pharmaco-interventional strategy of glycoprotein IIB/IIIA with MT use in high-risk patients allows to achieve long-term outcomes comparable with low-risk ST-segment elevation myocardial infarction patients.
The simulation of cost–effectiveness analysis of complex pharmaco-interventional strategy seems to be cost-effective, providing savings on target vessel revascularization and major cardiovascular events prevented in long term follow-up.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Coles AH, Fisher KA, Darling C et al. Recent trends in postdischarge mortality among patients with an initial acute myocardial infarction. Am. J. Cardiol. 110(8), 1073–1077 (2012).
2.
Members ATF, Steg PG, James SK et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). Eur. Heart J. 33(20), 2569–2619 (2012).
3.
Singh M, Reeder GS, Ohman EM et al. Does the presence of thrombus seen on a coronary angiogram affect the outcome after percutaneous coronary angioplasty? An angiographic trials pool data experience. J. Am. Coll. Cardiol. 38(3), 624 (2001).
4.
Sianos G, Papafaklis MI, Daemen J et al. Angiographic stent thrombosis after routine use of drug-eluting stents in ST-segment elevation myocardial infarction. The Importance of thrombus burden. J. Am. Coll. Cardiol. 50(7), 573–583 (2007).
5.
Gibson CM, De Lemos JA, Murphy SA et al. Combination therapy with abciximab reduces angiographically evident thrombus in acute myocardial infarction: a TIMI 14 substudy. Circulation 103(21), 2550–2554 (2001).
6.
Fröbert O, Lagerqvist B, Olivecrona GK et al. Thrombus aspiration during ST-segment elevation myocardial infarction. N. Engl. J. Med. 369(17), 1587–1597 (2013).
7.
Windecker S, Kolh P, Alfonso F et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 35(37), 2541–2619 (2014).
8.
Noman A, Egred M, Bagnall A, Spyridopoulos I, Jamieson S, Ahmed J. Impact of thrombus aspiration during primary percutaneous coronary intervention on mortality in ST-segment elevation myocardial infarction. Eur. Heart J. 33(24), 3054–3061 (2012).
9.
Dudek D, Mielecki W, Burzotta F et al. Thrombus aspiration followed by direct stenting: a novel strategy of primary percutaneous coronary intervention in ST-segment elevation myocardial infarction. Results of the Polish–Italian–Hungarian Randomized Thrombectomy Trial (PIHRATE Trial). Am. Heart J. 160(5), 966–972 (2010).
10.
Chesebro JH, Knatterud G, Roberts R et al. Thrombolysis in Myocardial Infarction (TIMI) Trial, Phase I: a comparison between intravenous tissue plasminogen activator and intravenous streptokinase. Clinical findings through hospital discharge. Circulation 76(1), 142–154 (1987).
11.
Van't Hof AWJ, Liem A, Suryapranata H et al. Angiographic assessment of myocardial reperfusion in patients treated with primary angioplasty for acute myocardial infarction: myocardial blush grade. Circulation 97(23), 2302–2306 (1998).
12.
Van't Hof AWJ, Liem A, De Boer M-J, Zijlstra F. Clinical value of 12-lead electrocardiogram after successful reperfusion therapy for acute myocardial infarction. Lancet 350(9078), 615–619 (1997).
13.
Rascati KL. Essentials of Pharmacoeconomics. Lippincott Williams & Wilkins, Baltimore, MD, USA (2014).
14.
Zeymer U, Margenet A, Haude M et al. Randomized comparison of eptifibatide versus abciximab in primary percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction: results of the EVA-AMI Trial. J. Am. Coll. Cardiol. 56(6), 463–469 (2010).
15.
Singh HS, Dangas GD, Guagliumi G et al. Comparison of abciximab versus eptifibatide during percutaneous coronary intervention in ST-segment elevation myocardial infarction (from the HORIZONS-AMI trial). Am. J. Cardiol. 110(7), 940–947 (2012).
16.
Dewilde S, Bruggenjurgen B, Nienaber C, Senges J, Welte R, Willich SN. Cost–effectiveness of adjunctive eptifibatide in patients undergoing coronary stenting in Germany. Eur. J. Health Econ. 13(4), 381–391 (2012).
17.
O'Shea JC, Hafley GE, Greenberg S et al. Platelet glycoprotein IIB/IIIA integrin blockade with eptifibatide in coronary stent intervention: the ESPRIT trial: a randomized controlled trial. JAMA 285(19), 2468–2473 (2001).
18.
Van Stel HF, Buskens E. Comparison of the SF-6D and the EQ-5D in patients with coronary heart disease. Health Qual. Life Outcomes 4, 20 (2006).
19.
Pasala T, Sattayaprasert P, Bhat PK, Athappan G, Gandhi S. Clinical and economic studies of eptifibatide in coronary stenting. Ther. Clin. Risk Manage. 10, 603–614 (2014).
20.
Vlaar PJ, Svilaas T, Vogelzang M et al. A comparison of 2 thrombus aspiration devices with histopathological analysis of retrieved material in patients presenting with ST-segment elevation myocardial infarction. JACC Cardiovasc. Interv. 1(3), 258–264 (2008).
21.
Pioud V, Lorgis L, Collin B et al. Coronary thrombectomy, technical comparison of two systems on a laboratory bench: the impact of bends, angles and thrombus age. EuroIntervention 6(6), 729–734 (2011).
• Elementary paper documenting limited and different efficacy of aspiration catheters.
22.
Hara H, Nakamura M, Komatsu H et al. Comparison of the in vitro performance of 6 and 7 French aspiration catheters. EuroIntervention 2(4), 487–492 (2007).
• Elementary paper documenting different efficacy of aspiration catheters.
23.
Bhindi R, Kajander OA, Jolly SS et al. Culprit lesion thrombus burden after manual thrombectomy or percutaneous coronary intervention-alone in ST-segment elevation myocardial infarction: the optical coherence tomography sub-study of the TOTAL (ThrOmbecTomy versus PCI ALone) trial. Eur. Heart J. 36(29), 1892–1900 (2015).
•• In vivo documentation of limited efficacy of aspiration catheter in thrombus removal.
24.
Tomasik A, Tyrała K, Paniczek M, Nowalany-Kozielska E. Manual aspiration catheters with different in vivo efficacy in acute myocardial infarction: a study of two cases. Gazz. Med. Ital. Arch. Sci. Med. 175(11), 491–495 (2016).
25.
Carey BC, Blankenship JC. A sequential approach to the management of a massive intracoronary thrombus in ST elevation myocardial infarction: a case report. Angiology 58(1), 106–111 (2007).
•• Describes the measure to improve the success rate of thrombus removal.
26.
Mani AJ. Novel use of a guide extension mother-and-child catheter for adjunctive thrombectomy during percutaneous coronary intervention for acute coronary syndromes. J. Invasive Cardiol. 26(6), 249–254 (2014).
•• Describes the measure to improve the success rate of thrombus removal.
27.
Agarwal S, Parashar A, Garg A, Ellis SG, Tuzcu EM, Kapadia SR. Length of stay and long-term mortality following ST elevation myocardial infarction. Catheter Cardiovasc. Interv. 86(Suppl. 1), S1–S7 (2015).
28.
Jones DA, Rathod KS, Howard JP et al. Safety and feasibility of hospital discharge 2 days following primary percutaneous intervention for ST-segment elevation myocardial infarction. Heart 98(23), 1722–1727 (2012).
29.
Debinski M, Kondys M, Buszman PE. Risk assessment in patients with ST elevation myocardial infarction treated with primary percutaneous coronary angioplasty. Does reduced duration of hospital stay affect the prognosis? Kardiologia Polska 75(7), 635–640 (2017).
30.
Dziki B, Miechowicz I, Iwachow P et al. Cath lab costs in patients undergoing percutaneous coronary angioplasty – detailed analysis of consecutive procedures. Kardiologia Polska 75(9), 914–921 (2017).
Information & Authors
Information
Published In
Copyright
© 2018 Andrzej Tomasik.
History
Received: 18 November 2017
Accepted: 9 January 2018
Published online: 29 January 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost assessment of treatment of acute myocardial infarction and angiographically visible coronary thrombus. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0094
Export citation
Select the citation format you wish to export for this article or chapter.