Treatment burden and healthcare resource utilization in patients with chronic rhinosinusitis with nasal polyps who did or did not undergo functional endoscopic sinus surgery: a US real-world retrospective cohort study
Publication: Journal of Comparative Effectiveness Research
Abstract
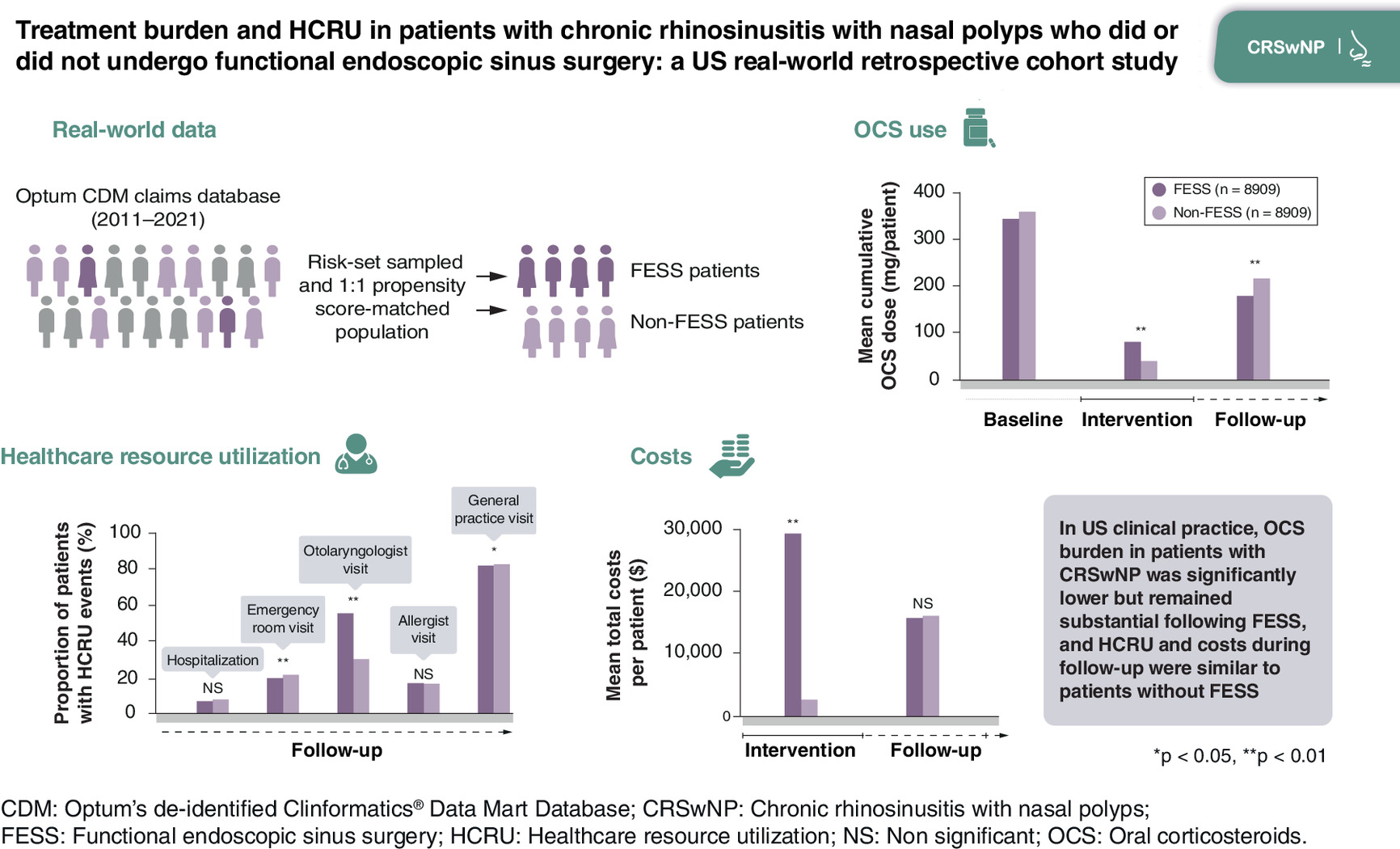
Aim: To compare oral corticosteroid (OCS) burden and healthcare resource utilization (HCRU) in patients with chronic rhinosinusitis with nasal polyps undergoing functional endoscopic sinus surgery (FESS; intervention) versus not undergoing FESS. Materials & methods: Retrospective cohort study using US claims data (Optum’s de-identified Clinformatics® Data Mart Database; 2011–2021). Groups were propensity score (PS) matched to adjust for confounding. OCS burden (cumulative dose in mg prednisone equivalents) and HCRU were assessed during baseline (365 days pre-index), intervention (days 0–44), and follow-up (days 45–365); costs during intervention and follow-up. Results: Before PS-matching, both groups had substantial comorbidity burden (>50% allergic rhinitis; >25% asthma) and over half of patients had used OCS (65% [FESS] vs 52% [non-FESS]; p < 0.01). After PS-matching (n = 8909 per group), OCS cumulative dose during follow-up was 18% lower among FESS versus non-FESS patients (mean difference: -40 mg per patient [95% CI: -57, -23; p < 0.01]). Similar proportions of patients filled OCS prescriptions during follow-up (35% [FESS], 36% [non-FESS]) and in these patients, OCS burden remained high (mean [SD] cumulative dose 521 [786] vs 612 [906] mg, respectively). Mean total healthcare costs per patient during the intervention period were $28,832 (FESS) and $2537 (non-FESS), but similar during follow-up ($15,659 and $15,926, respectively). HCRU was similar in follow-up, except more FESS patients visited an otolaryngologist (57% vs 32%, p < 0.01). Conclusion: In US clinical practice, OCS burden in patients with chronic rhinosinusitis with nasal polyps was significantly lower but remained substantial following FESS, and HCRU and costs during follow-up were similar to matched patients without FESS.
Plain language summary
What was the aim of this research?
To compare the burden of medications, visits, procedures and costs between patients with chronic rhinosinusitis with nasal polyps who did nor did not undergo polyp removal surgery.
How was the research carried out?
Anonymized administrative health-claim data were analyzed through the year before and up to 3 years after surgery. To allow for a fair comparison between patients who did and did not have surgery, patients were matched according to a range of factors including age, gender, race and prior use of medications.
What were the results?
Between 45 and 365 days after surgery, patients had an 18% lower average cumulative dose of oral corticosteroids (OCS) compared with patients who did not have surgery. The proportion of patients with prescriptions for OCS was similar between the surgery and nonsurgery groups (35% and 36%, respectively). Similarly, there was little difference in the use of other medications. Otolaryngologist visits were more common for patients who had surgery than those who did not. Costs were similar after surgery between the surgery and no-surgery groups through 3 years of follow-up.
What do the results of the study mean?
This study found that OCS use was lower over the 3 years after sinus surgery but remained substantial for both the surgery and nonsurgery patient groups. Further, surgery only marginally reduced costs during the follow-up period. These results serve as evidence for policymakers and healthcare providers when deciding the most cost-effective way to treat patients with chronic rhinosinusitis with nasal polyps.
Graphical and video abstract
Supplementary Material
File (supplementary materials.docx)
- Download
- 223.04 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Claeys N, Teeling MT, Legrand P et al. Patients unmet needs in chronic rhinosinusitis with nasal polyps care: a patient advisory board statement of EUFOREA. Front. Allergy 2, 761388 (2021).
2.
Khan A, Vandeplas G, Huynh TMT et al. The Global Allergy and Asthma European Network (GALEN) rhinosinusitis cohort: a large European cross-sectional study of chronic rhinosinusitis patients with and without nasal polyps. Rhinology 57(1), 32–42 (2019).
3.
Bachert C, Bhattacharyya N, Desrosiers M, Khan AH. Burden of disease in chronic rhinosinusitis with nasal polyps. J. Asthma Allergy 14, 127–134 (2021).
4.
Bhattacharyya N, Villeneuve S, Joish VN et al. Cost burden and resource utilization in patients with chronic rhinosinusitis and nasal polyps. Laryngoscope 129(9), 1969–1975 (2019).
5.
Benson VS, Germain G, Chan RH et al. Elucidating the real-world burden of chronic rhinosinusitis with nasal polyps in patients in the USA. OTO Open 6(4), 2473974X221128930 (2022).
6.
Lourijsen ES, Fokkens WJ, Reitsma S. Direct and indirect costs of adult patients with chronic rhinosinusitis with nasal polyps. Rhinology 58(3), 213–217 (2020).
7.
Wahid NW, Smith R, Clark A, Salam M, Philpott CM. The socioeconomic cost of chronic rhinosinusitis study. Rhinology 58(2), 112–125 (2020).
• Highlights the substantial healthcare resource utilization (HCRU), out-of-pocket expenditures and lost work time for patients with CRS.
8.
Bhattacharyya N. Incremental health care utilization and expenditures for chronic rhinosinusitis in the United States. Ann. Otol. Rhinol. Laryngol. 120(7), 423–427 (2011).
•• This study comparing HCRU of patients with and without CRS found that CRS is associated with substantial increases in HCRU owing to office-based and prescription expenditures, and imposes a high cost on national healthcare.
9.
Fokkens WJ, Lund VJ, Hopkins C et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 58(Suppl. 29), 1–464 (2020).
10.
Peters AT, Bengtson LGS, Chung Y et al. Clinical and economic burden of chronic rhinosinusitis with nasal polyposis: a U.S. administrative claims analysis. Allergy Asthma Proc. 43(5), 435–445 (2022).
•• This administrative claims analysis highlights the prevalence of oral corticosteroid (OCS) use among patients with chronic rhinosinusitis with nasal polyps (CRSwNP).
11.
Hox V, Lourijsen E, Jordens A et al. Benefits and harm of systemic steroids for short- and long-term use in rhinitis and rhinosinusitis: an EAACI position paper. Clin. Transl. Allergy 10, 1 (2020).
12.
Waljee AK, Rogers MA, Lin P et al. Short term use of oral corticosteroids and related harms among adults in the United States: population based cohort study. BMJ 357, j1415 (2017).
13.
Yao TC, Huang YW, Chang SM et al. Association between oral corticosteroid bursts and severe adverse events: a nationwide population-based cohort study. Ann. Intern. Med. 173(5), 325–330 (2020).
14.
Yasir M, Goyal A, Sonthalia S. Corticosteroid adverse effects. Statpearls. StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC (2023).
15.
Slack R, Bates G. Functional endoscopic sinus surgery. Am. Fam. Physician 58(3), 707–718 (1998).
16.
Snidvongs K, Kalish L, Sacks R et al. Sinus surgery and delivery method influence the effectiveness of topical corticosteroids for chronic rhinosinusitis: systematic review and meta-analysis. Am. J. Rhinol. Allergy 27(3), 221–233 (2013).
17.
DeConde AS, Mace JC, Levy JM et al. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope 127(3), 550–555 (2017).
18.
Loftus CA, Soler ZM, Koochakzadeh S et al. Revision surgery rates in chronic rhinosinusitis with nasal polyps: meta-analysis of risk factors. Int. Forum Allergy Rhinol. 10(2), 199–207 (2020).
19.
Pundir V, Pundir J, Lancaster G et al. Role of corticosteroids in functional endoscopic sinus surgery–a systematic review and meta-analysis. Rhinology 54(1), 3–19 (2016).
20.
Han JK, Silver J, Dhangar I, Veeranki P, Deb A. Quantifying corticosteroid burden in chronic rhinosinusitis with nasal polyps: a retrospective US database study. Ann. Allergy Asthma Immunol. 134(6), 685–693 (2024).
21.
Mansi A, Bui R, Chaaban MR. Oral corticosteroid regimens in the management of chronic rhinosinusitis. Ear Nose Throat J. 101(2), 123–130 (2022).
22.
Lourijsen ES, Reitsma S, Vleming M et al. Endoscopic sinus surgery with medical therapy versus medical therapy for chronic rhinosinusitis with nasal polyps: a multicentre, randomised, controlled trial. Lancet Respir. Med. 10(4), 337–346 (2022).
•• This randomized controlled trial from the Netherlands of ESS versus medical therapy alone found a similar substantial burden of OCS following surgery as found in our US study.
23.
Price DB, Trudo F, Voorham J et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J. Asthma Allergy 11, 193–204 (2018).
24.
Davis GE, Zeiger RS, Emmanuel B et al. Systemic corticosteroid-related adverse outcomes and health care resource utilization and costs among patients with chronic rhinosinusitis with nasal polyposis. Clin. Ther. 44(9), 1187–1202 (2022).
25.
Rudmik L, Soler ZM, Mace JC, Schlosser RJ, Smith TL. Economic evaluation of endoscopic sinus surgery versus continued medical therapy for refractory chronic rhinosinusitis. Laryngoscope 125(1), 25–32 (2015).
•• This analysis concluded that functional endoscopic sinus surgery (FESS) becomes cost-effective versus continued medical therapy within the third year after surgery.
26.
Nanayakkara JP, Igwe C, Roberts D, Hopkins C. The impact of mental health on chronic rhinosinusitis symptom scores. Eur. Arch. Otorhinolaryngol. 270(4), 1361–1364 (2013).
27.
Schlosser RJ, Gage SE, Kohli P, Soler ZM. Burden of illness: a systematic review of depression in chronic rhinosinusitis. Am. J. Rhinol. Allergy 30(4), 250–256 (2016).
28.
Mullol J, Mariño-Sánchez F, Valls M, Alobid I, Marin C. The sense of smell in chronic rhinosinusitis. J. Allergy Clin. Immunol. 145(3), 773–776 (2020).
29.
Marin C, Alobid I, Fuentes M, López-Chacón M, Mullol J. Olfactory dysfunction in mental illness. Curr. Allergy Asthma Rep. 23(3), 153–164 (2023).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 1 May 2025
Accepted: 6 January 2026
Published online: 11 February 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Treatment burden and healthcare resource utilization in patients with chronic rhinosinusitis with nasal polyps who did or did not undergo functional endoscopic sinus surgery: a US real-world retrospective cohort study. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0065
Export citation
Select the citation format you wish to export for this article or chapter.