Comparability and stability of holotranscobalamin levels in capillary and venous blood
Publication: Journal of Patient Centricity
Abstract
Aim: Self-collected capillary blood offers several advantages over phlebotomy samples. However, evidence that venous and capillary serum are comparable for many routine analytes is limited. In this study, we aimed to determine whether capillary sampling could serve as an alternative to venous sampling for assessing vitamin B12 levels as holotranscobalamin (HoloTC). We also investigated whether this analyte remained stable in unspun capillary blood for 3 days at ambient temperatures, allowing samples to be returned via the postal system. Materials & methods: Matched pairs of capillary and venous blood samples were collected from 25 patients to determine HoloTC. One set was processed on day 0, and the other was stored at ambient temperature and processed on day 3 to mimic postal samples. Self-collected capillary blood was compared with phlebotomist-collected venous samples using correlation, Passing–Bablok regression, Bland-Altman and reference change value analysis. Results: Correlation, Passing–Bablok and Bland–Altman analyses showed that HoloTC levels in capillary and venous serum were comparable, and reference change value analysis showed that the analyte was stable in unspun blood for at least 3 days at ambient temperature. Conclusion: We believe this is the first published study to assess whether capillary blood sampling is an acceptable alternative to venous sampling for measuring HoloTC concentration. Our data indicate no significant difference in results between venous HoloTC concentrations measured on day 0 and those measured in self-collected capillary blood stored as whole blood at room temperature for at least 3 days before analysis.
Plain language summary
What is the article about?
Vitamin B12 is an essential nutrient, but deficiency is common and often challenging to diagnose. Prompt diagnosis and treatment of B12 deficiency protects against a number of illnesses, including anemia and possible nerve damage. Markers of B12 status include the measurement of total B12 or ‘active B12’. Active B12 is the form used directly by the body, and as such, this marker has been shown to improve early detection of deficiency in some patient groups.
What methodology/protocol is described?
Taking blood from a vein with a needle is the usual way doctors collect blood for tests, but this process can be expensive and inconvenient because people have to go to a clinic or hospital, and trained staff are required to perform it. Because of this, simpler methods that allow patients to self-collect blood at home using painless capillary blood collection devices are gaining popularity and may provide at-risk groups with easier access to diagnose B12 deficiency and monitor treatment.
Why is this important?
This article provides evidence supporting the use of capillary testing for serum B12 using the Roche Active B12 assay.
Vitamin B12 is an essential dietary nutrient for humans, and a deficiency can affect multiple systems, including the bone marrow, leading to megaloblastic anemia [1,2]. The terminal ileum is the main site of vitamin B12 absorption, and this process is aided by intrinsic factor (IF), produced by the gastric parietal cells. Causes of deficiency are numerous and include gastric atrophy, H. pylori, Crohn’s disease, drugs that affect absorption, and a strict vegan diet without corrective supplementation [1–3].
The resultant dyserythropoiesis leads to abnormal laboratory findings in several routine tests, including macrocytic red cells and hypersegmented neutrophils [1]. Symptoms of deficiency typically include fatigue, visual disturbance and memory loss. However, skin hyperpigmentation, glossitis and infertility have also been reported [1–5].
In the UK, the prevalence of vitamin B12 deficiency is approximately 6% in individuals under 60 years of age and nearly 20% in those over 60 years of age [1]. However, a shift in the population toward vegetarianism and veganism could increase these figures. Routine screening of unselected patients for vitamin B12 deficiency is not recommended, but may be useful in specific situations, especially during pregnancy [6–8]. In these cases, a level below 133 pmol/l confirms vitamin B12 deficiency using a total B12 assay, it is noted that in some cases, second-line testing may be required [7,8].
In serum, vitamin B12 exists in two forms. It can be bound to haptocorrin to form holohaptocorrin or to transcobalamin to form holotranscobalamin (HoloTC). Cells can only take up vitamin B12 in the form of HoloTC; hence, it is often called Active B12 [7–12].
Although not yet widely used, HoloTC measurement is an emerging method for detecting deficiency, and there is growing evidence that it is a better marker than total B12 for detecting early vitamin B12 deficiency [11–13]. Furthermore, HoloTC has been shown to be the most effective indicator of vitamin B12 status, suggesting that HoloTC may be suitable for screening vitamin B12 deficiency in at-risk groups [11,13].
Routine vitamin B12 and HoloTC status is typically assessed in venous serum and plasma. However, conventional in-clinic collection is not always feasible or preferred by patients [14–17]. As such, alternative patient-centric sampling strategies are becoming widely available [15,16].
There are a number of barriers that can affect the success of blood sample collection in the clinical setting, including limited clinic opening hours [17] and geographic and physical inaccessibility, which would particularly affect older adults and those with mobility issues [18,19], all of whom have been identified as at-risk groups of vitamin B12 deficiency [11–13].
Self-collected capillary blood (CBT) enables at-home sampling without requiring patients to visit a clinical setting [19,20], and, because of its patient-centric nature, CBT has been shown to be preferred over venous collection in several studies [21–23].
There is also a growing body of evidence suggesting that, in many cases, capillary blood is comparable to venous blood [24], and although very few manufacturers list capillary blood as an approved matrix in their instructions for use, this is changing [25], and there is now government interest in this mode of patient testing [26].
Using self-collected capillary samples with back-to-laboratory testing opens several novel possibilities. However, for the full potential of this method to be realized, it is imperative to assess analyte stability, thereby enabling samples collected at home to be transferred to the laboratory via postal services.
Our aim in this study was therefore to establish the validity of measuring HoloTC concentrations in capillary blood as a viable alternative to venous blood, using two sets of samples. In the first pair (venous and capillary), both samples were processed and tested on day 0. In contrast, the second pair (venous and capillary) was stored as whole blood at room temperature (18–22°C) and then processed and tested on day 3. This second set of samples was used to mimic samples sent via the postal network.
Materials & methods
Twenty-five generally well patients (17 females and 8 males, aged 21–52 years) who had requested HoloTC testing as part of a wellness panel were asked to provide two venous and two capillary samples. The number of patients aligns with the Clinical and Laboratory Standards Institute document on the assessment of equivalence of specimen types for medical laboratories [27] and recent UK recommendations for validating capillary blood samples [28], which state that a minimum of 20 paired samples is required with justification. All aspects of this study were conducted in accordance with the Declaration of Helsinki (2013), and individuals were included only after informed consent.
Sample collection & preparation
All participants received diagrammatic guidance on performing effective capillary sampling (see Supplementary Figure 1), and self-collection was performed immediately after venous sampling. Venous samples were collected by a trained phlebotomist using Becton Dickinson (Oxford, UK) serum separator tubes, while capillary samples were collected using Becton Dickinson Microtainer serum separator tubes and 2 mm self-retracting safety lancets. One pair of matched venous and capillary samples was centrifuged together at 2000 g for 10 min within 4 h of collection, and all samples were analyzed together within 9 h of collection, using the Roche (Burgess Hill, UK) Elecsys Active B12 assay on a Cobas platform. The second set of whole-blood samples was stored at room temperature (18–22°C) for 3 days before centrifugation and then tested together on the same platform. HoloTC was analyzed according to the manufacturer’s recommendations. Samples were excluded based on the hemolytic, icterus and lipemia indices as reported by the analyzer (Roche Diagnostics).
Experimental design
Comparability studies were conducted by measuring HoloTC concentrations in paired venous and capillary samples obtained simultaneously from the patient and analyzed on day 0. For stability studies, the second set of paired samples (venous and capillary) was stored as whole blood at 18–22°C and analyzed on day 3. Comparisons were made between venous and capillary HoloTC concentrations on day 0 to establish a baseline, and between venous day 0 and capillary day 3 HoloTC concentrations. A full list of the raw data is shown in Table 1. It is noted that the Checklist for Reporting Stability Studies (CRESS), produced by the European Federation for Clinical Chemistry and Laboratory Medicine Working Group for the Preanalytical Phase was used as a framework for reporting results [29]
| Patient | Day 0 venous | Day 0 capillary | Day 3 venous | Day 3 capillary | Difference day 0 venous vs day 3 capillary, % |
|---|---|---|---|---|---|
| 1 | 95 | 102 | 99 | 104 | -8.65 |
| 2 | 72 | 69 | 70 | 73 | -1.37 |
| 3 | 67 | 72 | 67 | 66 | 1.52 |
| 4 | 60 | 58 | 61 | 57 | 5.26 |
| 5 | 76 | 79 | 73 | 81 | -6.17 |
| 6 | 81 | 76 | 73 | 79 | 2.53 |
| 7 | 61 | 75 | 58 | 67 | -8.96 |
| 8 | 48 | 52 | 52 | 55 | -12.73 |
| 9 | 82 | 79 | 80 | 74 | 10.81 |
| 10 | 55 | 53 | 56 | 55 | 0.00 |
| 11 | 74 | 71 | 71 | 78 | -5.13 |
| 12 | 96 | 99 | 99 | 99 | -3.03 |
| 13 | 150 | 149 | 149 | 148 | 1.35 |
| 14 | 95 | 102 | 99 | 104 | -8.65 |
| 15 | 154 | 156 | 155 | 152 | 1.32 |
| 16 | 85 | 82 | 77 | 80 | 6.25 |
| 17 | 57 | 55 | 55 | 53 | 7.55 |
| 18 | 82 | 87 | 82 | 84 | -2.38 |
| 19 | 82 | 84 | 86 | 85 | -3.53 |
| 20 | 55 | 54 | 55 | 56 | -1.79 |
| 21 | 68 | 67 | 70 | 68 | 0.00 |
| 22 | 78 | 78 | 80 | 79 | -1.27 |
| 23 | 65 | 68 | 69 | 68 | -4.41 |
| 24 | 67 | 69 | 69 | 68 | -1.47 |
| 25 | 72 | 69 | 70 | 73 | -1.37 |
Venous day 0 correlation to capillary day 0: r = 0.996, venous day 0 to capillary day 3: r = 0.987.
Statistical analysis
Mean difference was determined using Bland–Altman plots [30] to compare venous and capillary samples on days 0 and 3. The Pearson correlation coefficient and Passing–Bablok plots were also used to assess the strength of the relationship [31] and the level of agreement between HoloTC concentrations in venous and capillary blood.
In addition, reference change values (RCVs) were used to assess whether results from venous and capillary samples were interchangeable [32,33]. RCVs account for both analytical and biological variation, and their use alongside Bland–Altman and the EFLM total allowable error (TAE) calculations is recommended [28]. To determine the RCV, the assay CV% was calculated from 12 months of data for the Roche Active B12 internal quality control (PreciControl Active B12 ref 07713223190), yielding a combined CV of 3.4% across two levels. The intra-individual biological variation (CVi) for HoloTC is 13%, while the inter-individual biological variation (CVg) is 24.6% [34]. This yields an optimal TAE of 8.8%, a desirable TAE of 17.7%, and a minimum TAE of 26.5%. Statistical analyses were performed using the Analyse-It method validation edition (Analyse-It, Leeds, UK).
Results
Twenty-five paired samples (two capillary and two venous) were obtained from generally healthy people. Results for HoloTC ranged from 48 to 156 pmol/l.
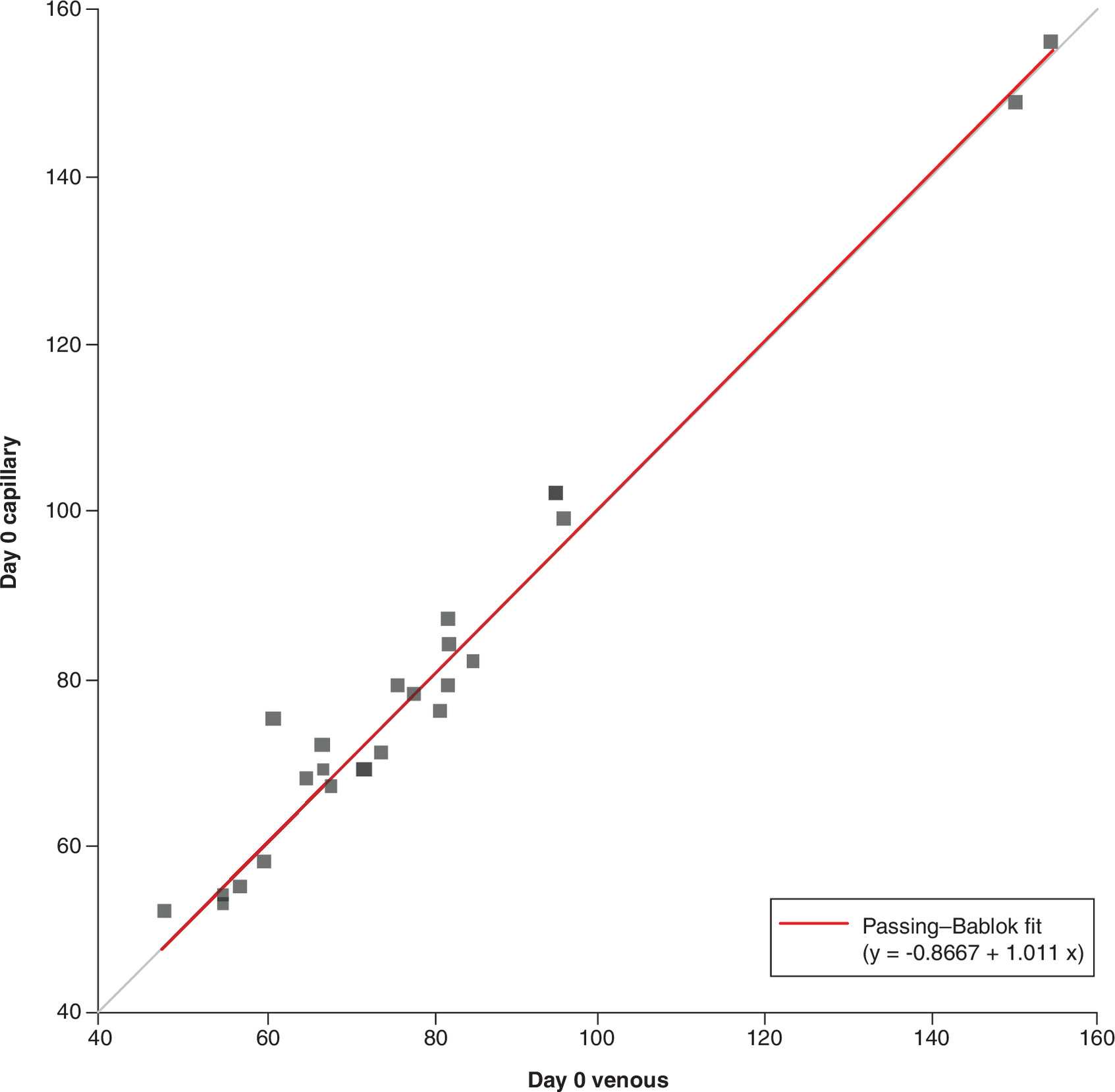
Figure 1. The Passing–Bablok plot of venous and capillary serum determinations of HoloTC concentration on day 0.
The Passing–Bablok plot of venous and capillary serum determinations of HoloTC concentration on day 0 (correlation coefficient r = 0.996, n = 25) shows a constant negative bias of 0.86 pmol/l and a 1.1% positive proportional bias. No significant difference between venous and capillary serum is identified, as the 95% CI encompasses 1 for the slope and 0 for the intercept.
HoloTC: Holotranscobalamin.
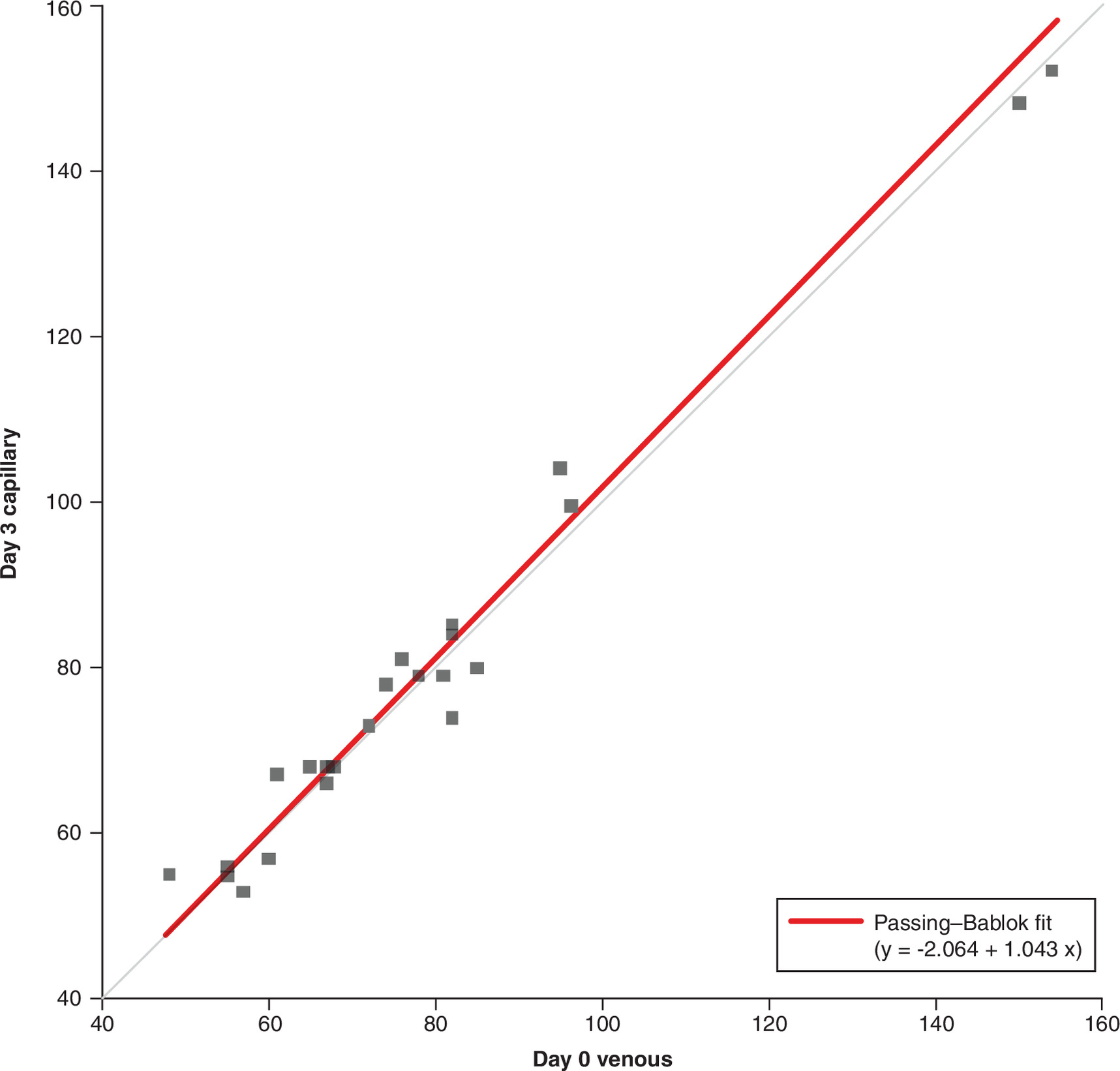
Figure 2. A Passing–Bablok plot comparing venous HoloTC levels on day 0 with capillary serum HoloTC levels on day 3.
A Passing–Bablok plot comparing venous HoloTC levels on day 0 with capillary serum HoloTC levels on day 3 (correlation coefficient r = 0.987, n = 25) shows a constant negative bias of 2.1 pmol/l and a 4.3% positive proportional bias. No significant difference is identified between venous day 0 and capillary day 3 serum, as the 95% CI encompasses 1 for the slope and 0 for the intercept.
HoloTC: Holotranscobalamin.
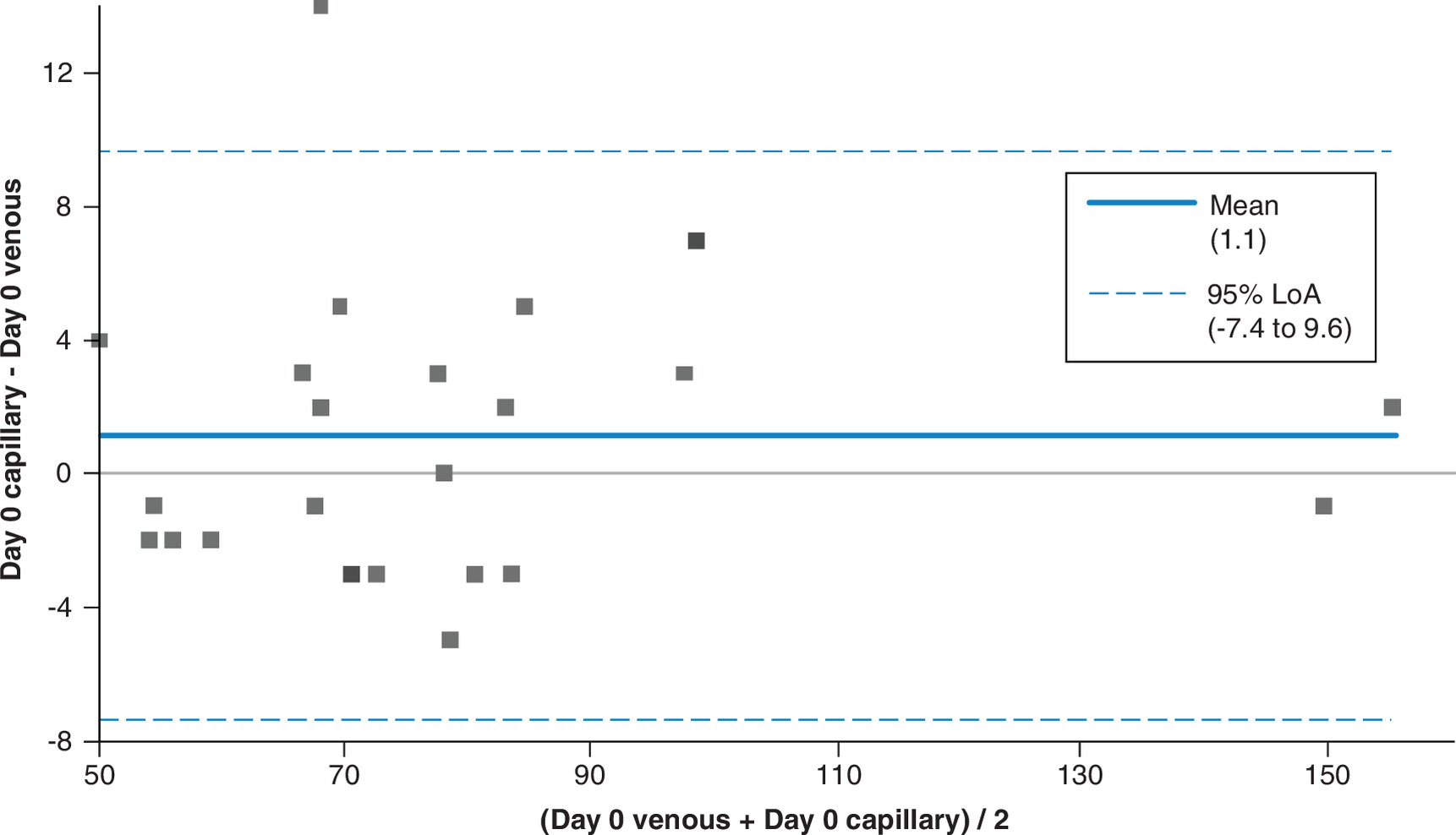
Figure 3. Bland–Altman plot of venous and capillary serum determinations of HoloTC concentration on day 0.
Bland–Altman plot of venous and capillary serum determinations of HoloTC concentration on day 0. Bland–Altman plot of agreement between venous and capillary determinations (n = 25) indicates a positive bias of 1.1 pmol/l. Limits of agreement are shown as blue dotted lines; the line of identity is shown as a solid blue line.
HoloTC: Holotranscobalamin.
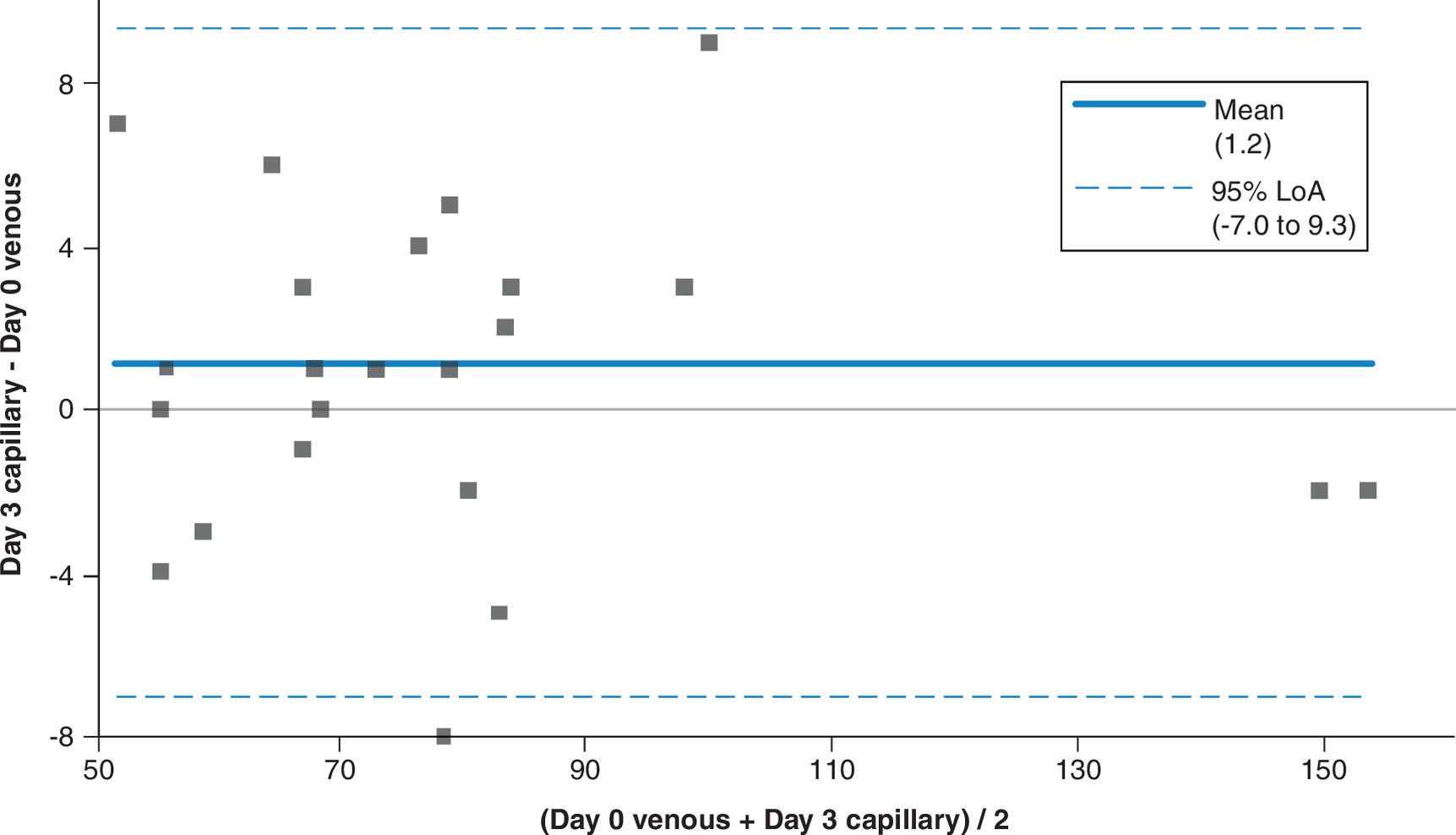
Figure 4. A Bland–Altman plot comparing venous HoloTC levels on day 0 with capillary serum HoloTC levels on day 3.
A Bland–Altman plot comparing venous HoloTC levels on day 0 with capillary serum HoloTC levels on day 3 (n = 25) indicates a positive bias of 1.2 pmol/l. Blue dotted lines represent the limits of agreement; the line of identity is shown as a solid blue line.
HoloTC: Holotranscobalamin.
Across the concentration range (48–156 pmol/l), the results were highly comparable. Our findings demonstrate satisfactory agreement between capillary and venous serum HoloTC concentrations on both day 0 and day three. Correlation coefficients of r = 0.996 (p < 0.001) and r = 0.987 (p < 0.001) were observed between venous and capillary samples on day 0 and between venous serum on day 0 and capillary serum on day three, respectively. Bland–Altman analysis shows good agreement with a slight bias of 1.2 pmol/l (95% CI: -0.56–2.88) between venous samples analyzed on day 0 and capillary samples analyzed on day 3. The venous day 0 and day 3 bias was 0.1 pmol/l (95% CI: -1.48 to -1.32).
Our data showed that HoloTC is stable in capillary whole blood stored at ambient temperature for at least 3 days. The RCV for HoloTC measured by the Roche method is (35% and -26%), these are the levels that, if exceeded, denote a significant clinical increase or decrease. None of the patient samples exceeded the positive or negative RCV, suggesting no significant changes over the study periods. In addition, only three samples exceeded the optimum TAE of 8.8% (sample 7: 8.96%, sample 8: 12.73% and sample 9: 10.81%), and no samples exceeded the desirable TAE of 17.7%.
Discussion
There is growing evidence supporting the use of HoloTC to diagnose early vitamin B12 deficiency, particularly in at-risk groups [10–13]. Taking this into account, where regular testing is required, i.e., for patient monitoring, capillary blood sampling may offer advantages over traditional venous sampling, as it does not require attendance at primary or secondary care facilities.
Studies have shown that capillary sampling is preferred to venous collection in several situations [15,22,23]. Given that capillary sampling lends itself to self-collection, with samples returned to the laboratory for testing and, hence, to remote healthcare opportunities, any analyte selected must remain stable in whole blood for several days after collection, thereby allowing samples to be returned via postal services. Although numerous papers have validated the use of capillary blood for infectious disease testing [35–37], there is currently a limited but growing body of literature on the comparability and stability of analytes between capillary and venous blood [24]. This trend will no doubt increase now that some assay manufacturers are beginning to list capillary serum as an approved matrix in their instructions for use [25].
Our study is the first to compare capillary and venous samples for determining serum HoloTC concentration, while also providing whole-blood stability data. Our findings show very good agreement between capillary and venous serum HoloTC concentrations on both day 0 and day 3. Correlation coefficients of r = 0.996 (p < 0.001) and 0.987 (p < 0.001) were observed between venous and capillary samples on day 0 and between venous serum on day 0 and capillary serum on day three, respectively. In addition, Passing–Bablok, Bland–Altman and RCV analyses showed no clinically relevant bias between these matrices on either day 0 or day 3.
These results are particularly important when investigating populations with concerns about the use of more invasive venous sampling techniques or the costs and resources required for phlebotomy. This sampling method reduces the need for patients to visit primary care or outpatient clinics for blood tests, potentially reducing nonattendance rates and supporting underserved populations.
However, some limitations of the study are noted. We have only controlled for the transport time routinely used by the UK’s Royal Mail Tracked 24 service, in which over 95% of samples are returned within 72 h (own unpublished data). Further work over a longer timescale might be necessary in other countries where samples are in transit for more than 3 days. Likewise, due to the difficulty in obtaining serial capillary samples, we were only able to perform stability studies within a limited temperature range. The data presented covers a broad range of HoloTC concentrations (48–156 pmol/l), which typically reflect levels observed in our patient cohort; however, we have no data at very low concentrations, and the study would be improved by obtaining samples with lower HoloTC concentrations. Furthermore, although the sample numbers meet the minimum requirements specified in the CSLI EP35 guidance document and the recently published UK recommendations for validating capillary blood samples in routine clinical laboratories [26,27], additional samples, particularly from the deficient range, would strengthen this study’s findings.
Conclusion
This proof-of-concept study has several strengths: first, we obtained a wide range of HoloTC concentrations; second, all samples met the acceptance criteria. All but three samples were within the optimal TAE range, and all were within the desirable TAE range. Both venous and capillary samples stored as whole blood for 3 days at room temperature were shown to be highly stable and comparable to venous blood analyzed on day 0.
The Roche Active B12 instruction for use states that this analyte is stable at 15–25°C for 5 days [38]; this applies only to venous serum, and Roche does not provide stability data for whole blood. This paper, therefore, also provides additional venous stability data for HoloTC for routine analysis.
The growth of self-collected capillary testing has made it essential for each laboratory offering this service to undertake a similar validation process during assay acceptance to confirm comparability between matrices. Recommendations for performing this type of validation in the clinical laboratory were, until quite recently, limited, but this has changed with the UK recommendations for the validation and adoption of capillary blood testing in the routine clinical laboratory [28]. The evidence presented here will help promote the use of capillary samples in routine pathology.
•
In the UK, the prevalence of vitamin B12 deficiency is approximately 6% in individuals under 60 years of age and nearly 20% in those over 60 years of age.
•
Holotranscobalamin (HoloTC), also known as Active B12, has been identified as a more precise marker for detecting early vitamin B12 deficiency.
•
Routine vitamin B12 status is typically assessed using venous serum. However, conventional in-clinic collection is not always feasible or preferred by patients and self-collected capillary blood samples that are then returned to the laboratory for testing may be a viable alternative, especially for patient monitoring.
•
There is currently a lack of evidence to confirm venous and capillary vitamin B12 levels are comparable, or if HoloTC is stable in whole blood over several days, that would be required to return these samples via the postal network.
•
This proof-of-concept study obtained a wide range of paired HoloTC concentrations and showed that venous and capillary blood are comparable for assessing vitamin B12 levels and that HoloTC levels are stable in whole blood at ambient temperatures for at least 3 days.
•
This study, therefore, supports the use of capillary sampling to determine HoloTC concentration as an alternative to venous sampling.
Financial disclosure
The author(s) received no financial and/or material support for this research or the creation of this work.
Competing interest disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing assistance disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research disclosure
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
Data transparency statement
The authors certify that this manuscript reports the original results of a real-world evidence study. A prespecified study protocol was developed and is available within the paper. Deidentified data underlying the findings of this study are available within the paper. No preregistration was reported for this study. The analytic code used in the analysis are not publicly available. Reporting checklists were not provided for this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Hunt A, Harrington D, Robinson S. Vitamin B12 deficiency. BMJ 349, g5226 (2014).
2.
Stabler SP. Clinical practice. Vitamin B12 deficiency. N. Engl. J. Med. 368(2), 149–160 (2013).
3.
Dali-Youcef N, Andrès E. An update on cobalamin deficiency in adults. QJM 102(1), 17–28 (2009).
4.
Othman I, Tai E, Kuganasan S, Abu N. Vision loss as a presenting symptom of vitamin B12 deficiency. Cureus 16(5), e60113 (2024).
5.
Toh BH, van Driel IR, Gleeson PA. Pernicious anaemia. N. Engl. J. Med. 337(20), 1441–1448 (1997).
6.
NICE guideline - NG239. Vitamin B12 deficiency in over 16s: diagnosis and management. Published: 6 March 2024. (Accessed 21 Jan 2026). https://www.nice.org.uk/guidance/ng239
7.
Sands T, Jawed A, Stevenson E, Smith M, Jawaid I. Guideline Committee. Vitamin B12 deficiency: NICE guideline summary. BMJ 385, q1019 (2024).
8.
Harrington DJ, Stevenson E, Sobczyńska-Malefora A. The application and interpretation of laboratory biomarkers for the evaluation of vitamin B12 status. Ann. Clin. Biochem. Int. J. Lab. Med. 62(1), 22–33 doi: (2025) (Epub ahead of print).
9.
Devalia V, Hamilton MS, Molloy AM. British Committee for Standards in Haematology. Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Br. J. Haematol. 166(4), 496–513 (2014).
10.
O'Leary F, Samman S. Vitamin B12 in health and disease. Nutrients 2(3), 299–316 (2010).
11.
Nexo E, Hoffmann-Lücke E. Holotranscobalamin, a marker of vitamin B12 status: analytical aspects and clinical utility. Am. J. Clin. Nutr. 94(1), S359–S365 (2011).
12.
Bondu JD, Nellickal AJ, Jeyaseelan L, Geethanjali FS. Assessing diagnostic accuracy of serum holotranscobalamin (Active-B12) in comparison with other markers of vitamin B12 deficiency. Indian J. Clin. Biochem. 35(3), 367–372 (2020).
13.
Al Aisari F, Al-Hashmi H, Mula-Abed WA. Comparison between serum holotranscobalamin and total vitamin B12 as indicators of vitamin B12 status. Oman. Med. J. 25(1), 9–12 (2010).
14.
Syed ST, Gerber BS, Sharp LK. Travelling towards disease: transportation barriers to health care access. J. Commun. Health 38, 976–993 (2013).
15.
Collier BB, Brandon WC, Chappell MR et al. Comparing capillary blood collection technologies: assessing patient experience, device performance, & clinical accuracy. Bioanalysis 17(21), 1329–1336 (2025).
16.
Wentzensen N, Massad LS, Clarke MA et al. Enduring consensus cervical cancer screening and management guidelines committee. Self-collected vaginal specimens for HPV testing: recommendations from the enduring consensus cervical cancer screening and management guidelines committee. J. Low. Genit. Tract. Dis. 29(2), 144–152 (2025).
17.
Zhou Y, Abel G, Warren F, Roland M, Campbell J, Lyratzopoulos G. Do difficulties in accessing in-hours primary care predict higher use of out-of-hours GP services? Evidence from an English National Patient Survey. Emerg. Med. J. 32(5), 373–378 (2015).
18.
Yazdi-Feyzabadi V, Sabermahani M, Borhaninejad V, Iranmanesh M. Breaking barriers: challenges faced by the older adults in accessing primary healthcare in a developing country. BMC Geriatr. 25(1), 946 (2025).
19.
Groenendijk WN, Griffin TP, Islam MN et al. Remote capillary blood collection for HbA1c measurement during the COVID-19 pandemic: a laboratory and patient perspective. Diabet. Med. 39, e14897 (2022).
20.
Ansari S, Abdel-Malek M, Kenkre J et al. The use of whole blood capillary samples to measure 15 analytes for a home-collect biochemistry service during the SARS-CoV-2 pandemic: a proposed model from Northwest London Pathology. Ann. Clin. Biochem. 58, 411–421 (2021).
21.
Lattin MT, DiBianco LP, Holcomb Z et al. Painless, needle-free capillary blood collection for fertility hormone monitoring. Fertil. Steril. 124(5 Pt 2), 1124–1126 (2025).
22.
Schuchardt C, Müller F, Hafke A et al. Pain and feasibility of capillary self-blood collection in general practice: a cross-sectional investigative study. Eur. J. Gen. Pract. 31, 2501309 (2025).
23.
Boffel L, Van Mensel A, Pauwels J et al. Self-sampling by adolescents at home: assessment of the feasibility to successfully collect blood microsamples by inexperienced individuals. AAPS J. 26(4), 75 (2024).
24.
Schröder D, Hafke A, Hummers E et al. Comparison of laboratory results and pain perception in self-sampled capillary blood versus venous blood sampling: a systematic review and meta-analysis. Clin. Biochem. 138, 110965 (2025).
25.
Capillary blood testing project - first wave of claim extensions MN-RDS-CoreLab-2025-381. (Accessed 12 March 2026). https://productandsafetycare.roche.com/
26.
GOV.UK Department of Health & Social Care. Market engagement for transdermal capillary blood sampling solutions. (Accessed 13 April 2025). https://www.find-tender.service.gov.uk/Notice/012031-2026
27.
CLSI EP35. (Accessed 17 Mar 2026). https://clsi.org/shop/standards/ep35/
28.
Woolley T, Hepburn S, Perkins K. UK recommendations for the validation and adoption of capillary blood testing within the routine clinical laboratory: consensus opinion from the LabMed Patient-centred testing and sampling (PaCTS) group. Ann. Clin. Biochem. Int. J. Lab. Med. 0(ja).
29.
Cornes M, Simundic AM, Cadamuro J et al. The CRESS checklist for reporting stability studies: on behalf of the European Federation of Clinical Chemistry and Laboratory Medicine (EFLM) Working Group for the Preanalytical Phase (WG-PRE). Clin. Chem. Lab. Med. 59(1), 59–69 (2020).
30.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 8476, 307–310 (1986).
31.
Bilić-Zulle L. Comparison of methods: Passing and Bablok regression. Biochem. Med. (Zagreb) 21(1), 49–52 (2011).
32.
McCormack JP, Holmes DT. Your results may vary: the imprecision of medical measurements. BMJ 368, m149 (2020).
33.
Fokkema MR, Herrmann Z, Muskiet FA et al. Reference change values for brain natriuretic peptides revisited. Clin. Chem. 52(8), 1602–1603 doi: (2006) (Epub ahead of print).
34.
Brokner M, Hager HB, Lindberg M. Biological variation of holotranscobalamin and cobalamin in healthy individuals. Scand. J. Clin. Lab. Invest. 77(6), 433–436 (2017).
35.
Bajis S, Maher L, Treloar C et al; LiveRLife Study Group. Acceptability and preferences of point-of-care finger-stick whole-blood and venepuncture hepatitis C virus testing among people who inject drugs in Australia. Int. J. Drug Policy 61, 23–30 (2018).
36.
Bielen R, KocÖM Busschots D, Verrando R, Nevens F, Robaeys G. Validation of hepatitis C virus RNA detection using capillary blood by finger prick (GenXpert system)-hepatitis C fingerprick study. J. Viral Hepat. 27(7), 709–714 (2020).
37.
Mavedzenge SN, Davey C, Chirenje T et al. Finger prick dried blood spots for HIV viral load measurement in field conditions in Zimbabwe. PLoS ONE 10(5), e0126878 (2015).
38.
Elecsys Active B12 IFU 08717028500 V1.0, Roche Diagnostics. (2024). (Accessed 16 June 2026). https://elabdoc-prod.roche.com/eLD/api/downloads/15db4c71-f572-ec11-0d91-005056a772fd?countryIsoCode=gb
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 21 January 2026
Accepted: 25 June 2026
Published online: 9 July 2026
Keywords:
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparability and stability of holotranscobalamin levels in capillary and venous blood. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/jpc-2026-0006
Export citation
Select the citation format you wish to export for this article or chapter.