Lung cancer screening in Lithuania: a cost-effectiveness analysis
Abstract
Aim: This study aimed to assess the cost-effectiveness of the annual volumetric-enabled low-dose computed tomography (LDCT) lung cancer screening (LCS), based on the NELSON screening outcomes, versus no screening for the asymptomatic high-risk population in Lithuania. Materials & methods: The previously established model with a decision tree with an integrated state-transition Markov trace was adapted to assess the health benefits and the financial consequences of LCS from the Lithuanian healthcare system perspective. Individuals aged 50–74 years and with a smoking history underwent LCS with LDCT in the screening arm, and it was compared with the absence of screening across a lifetime horizon. The primary outcomes included the clinical benefits (lung cancer cases detected per stage and premature lung cancer deaths averted), direct costs (recruitment, diagnostic and treatment costs) of LCS implementation, quality-adjusted life years, life-years and the incremental cost-effectiveness ratio. One-way sensitivity analysis and probabilistic sensitivity analysis were conducted to ascertain the result's robustness. Results: Annual LCS with volumetric-enabled LDCT for 170,808 eligible individuals in Lithuania resulted in 6117 additional early-stage (I and II) lung cancers detected and 1874 averted late-stage (III and IV) lung cancers, leading to 2606 premature lung cancer deaths averted and 21,639 life-years gained at an uptake rate of 46.5%. The incremental cost-effectiveness ratio was €1372 per quality-adjusted life year with incremental costs of €21.1 million and 15,391 quality-adjusted life years gained. The results were robust based on sensitivity and scenario analyses. Conclusion: This study demonstrated that annual LCS with volumetric-enabled LDCT for a high-risk population could be cost-effective compared with no screening in Lithuania.
Plain language summary
What is this article about?
Several lung cancer screening (LCS) studies have been carried out worldwide, with the two largest studies showing that screening people at high risk can reduce deaths from lung cancer. In 2024, Lithuania launched a pilot LCS study to assess feasibility, organization and clinical effectiveness in 2024. In evaluating the introduction of a new screening program, cost-effectiveness analysis plays a central role in informing national screening decisions. Therefore, our study assessed both the health benefits and the economic impact of the LCS program in Lithuania by conducting a cost-effectiveness analysis.
What were the results?
The study found that LCS leads to better health outcomes for high-risk individuals. Although screening increases healthcare costs, these additional costs are considered acceptable. Overall, LCS was shown to be cost-effective compared with no screening. The incremental cost-effectiveness ratio was €1372 per quality-adjusted life year gained.
What do the results mean?
These results suggest that implementing LCS in Lithuania could be a better approach for diagnosing lung cancer than the current clinical pathway without screening. The findings provide valuable evidence for policymakers and healthcare decision-makers and support the consideration of launching a LCS program in Lithuania.
Lung cancer is the most diagnosed cancer worldwide and the leading cause of cancer-related mortality, with 1.8 million deaths in 2022 [1]. In Lithuania, lung cancer is the fourth most prevalent cancer accounting for approximately 9% of all new cancer cases [1]. Tobacco smoking is the most relevant risk factor related to lung cancer [2]. In Lithuania, the prevalence of smoking among men significantly exceeds that of women, with male smoking rates being more than three-times higher (29% vs 9.5%) [3]. This disparity is reflected in lung cancer incidence rates, which are markedly higher in men (53.5 per 100,000) compared with women (7.3 per 100,000) [2].
Cancer mortality in Lithuania is above the European average [4]. Lung cancer stands as the leading cause of cancer-related mortality in Lithuania, with low overall survival (OS) [5]. This is primarily attributable to the high proportion of patients diagnosed at an advanced stage, in fact the 5-year relative survival rate for advanced stage lung cancer remains below 10% compared with 43% in case of early diagnoses [5]. Lithuania’s preventable and treatable mortality rates are above the Europe average but have decreased in the last decade [4], due to improved public health policies, such as prevention and screening programs. Screening with low-dose computed tomography (LDCT) for high-risk individuals can facilitate the detection of lung cancer at earlier stages, subsequently improving the prospects for successful treatment and reducing lung cancer-specific mortality. This is supported by two large randomized controlled trials, the National Lung Screening Trial (NLST) conducted in the US [6] and the Dutch–Belgian Lung Cancer Screening Study (NELSON [NEderlands-Leuvens Longkanker Screenings ONderzoek]) in Europe [7]. Both the NLST and NELSON studies demonstrated significant reductions in lung cancer-specific mortality attributable to LDCT screening. The NLST reported a 20% reduction in lung cancer mortality, while the NELSON trial showed a 24% reduction in men [6,7]. Additionally, early-stage lung cancer detection using CT screening is corroborated by other smaller randomized European trials [8–13].
The European Council has advised Member States to explore the (financial) feasibility and effectiveness of quality-controlled lung cancer screening (LCS) with LDCT in 2022 [14]. The implementation of an LCS program in Lithuania has been initiated, engaging pulmonary specialists, the National HealthCare System, and representatives from the National Health Insurance Fund (NHIF) [2] and the first results of the Lithuanian LCS pilot have been published [15]. The NHIF currently provides reimbursement for several cancer screening programs. However, LCS is not encompassed within the current reimbursement scheme. This study evaluates the cost-effectiveness of implementing a population-based LCS program using volumetric-enabled LDCT compared with no screening for an asymptomatic, high-risk population in Lithuania, from a healthcare system perspective. Cost-effectiveness analysis is a key tool for informing national screening decisions and has become standard for assessing healthcare interventions [16], and this study provides to our knowledge the first country-specific assessment for Lithuania. For this analysis, we build on our group's previous LCS evaluations in the UK [17]. The Lithuanian analysis applies the original UK modeling structure to a Lithuanian context. The novelty of this study lies in applying an established LCS modeling framework to Lithuania to assess its policy relevance in a new national setting. Conducting a country-specific cost-effectiveness analysis is essential because differences in demographics, epidemiology, healthcare systems and costs can substantially alter the feasibility of implementing a screening program for national decision-makers.
Materials & methods
This study was based on a previously established and validated model, developed in Microsoft Excel Microsoft Corporation (2018), consisting of a decision tree and a state-transition Markov model [17]. The decision tree simulated the identification and diagnosis of lung cancer patients, while the state-transition Markov model demonstrated the transition of lung cancer patients between health states over time, based on the natural history of lung cancer. Detailed figures illustrating the decision tree and Markov model used in this analysis are available in the previous publication [17], providing a detailed visual representation of the model structure and transitions. Given the comprehensive publication of core model specifications elsewhere [17], the subsequent section provided a condensed overview of the methods, primarily emphasizing the localized Lithuanian data inputs utilized in this analysis.
Model structure & design
A validated decision tree and state-transitioned Markov model were used to simulate a no screening and a screening scenario [17]. The no screening scenario reflected the current clinical pathway for Lithuanian lung cancer patients. In a Markov model, individuals are evenly assigned to health states at the start to ensure a balanced comparison of transitions, costs and health outcomes across different strategies. However, it was observed in the model that LCS detected more lung cancer patients compared with the no screening arm where lung cancer patients were diagnosed after clinical presentation, as previously explained by Pan et al. [17]. Therefore, a branch named ‘missed individuals’ was added to the no screening arm. This branch consisted of an asymptomatic cohort defined as the ‘missed individuals’. These individuals were asymptomatic patients with preclinical disease. For the missed individuals, it was assumed that they followed the OS rates of patients with lung cancer stage II. This approach applies a conservative assumption for undiagnosed cases in the no-screening arm, avoiding survival overestimation while preventing underestimation of the benefits of LCS. However, no direct costs would be applied to them, as they were not diagnosed (yet), and therefore did not undergo any diagnostic procedures or treatment. For the screening scenario, the NELSON study volumetric protocol and screening outcomes were used to stimulate the detection of lung cancer for LCS participants. Additionally, in the screening scenario, a branch of nonparticipants, who were diagnosed through clinical presentation, was included. The analysis utilized one screening cohort, wherein individuals eligible for screening in a given year were followed throughout their lifetime. Individuals without a lung cancer diagnosis would enter the next screening round in the following year, as annual screening is the recommended method [18]. Individuals diagnosed with lung cancer and the missed individuals would enter the state-transition Markov model. The Markov model included three health states: preprogression, postprogression and death. The preprogression state represented the phase following diagnosis, during which patients remained until disease progression occurred. Individuals transitioned to the postprogression state upon disease progression, as they were not cured by the initial treatment. Additionally, individuals from the pre- and post-progression state transited to the death health state (lung cancer mortality and all-cause mortality). The Markov model was based on the natural history of lung cancer, and used to stimulate disease progression, long-term survival, and treatment costs for lung cancer patients by stage at diagnosis [17]. Therefore, the Markov trace was designed with a 3-month cycle to correspond with the lung cancer treatment and follow-up timeline [19]. The model included 17 annual screening rounds, starting from the mean age of participants in the NELSON study (58 years), and stopped at the upper boundary of the age inclusion criteria for a scan (74 years) [20].
The study followed the Lithuanian and Baltic guidelines for economic evaluations and health technology assessment [21,22]. The base case analysis was conducted from the healthcare payer perspective with a lifetime horizon. Quality-adjusted life years (QALYs) and life years (LYs) gained were designated as the principal health outcome measures to illustrate the changes in health-related quality of life and life expectancy attributed to the implementation of LCS. In addition, the incremental cost-effectiveness ratio (ICER) was reported to represent the economic value of LCS with LDCT compared with no screening. The willingness to pay (WTP) per QALY gained for medical procedures in Lithuania ranges from one to three-times the gross domestic product (GDP) per capita, translating to a threshold between €23,806–71,417, as the GDP per capita was €23,806 in Lithuania in the year 2022 [3,23]. A 3.5% discount rate was applied to both health and costs outcomes, thereby following the Lithuanian national health technology assessment guidelines [22].
Model inputs
The model inputs included screening outcomes, eligible population, lung cancer epidemiology, survival data, utilities and costs. The paragraphs below describe the data input used for the analysis. Lithuanian-specific data were used when available. International sources were used to compensate for data scarcity in Lithuania. The screening outcomes were based on the NELSON study and therefore did not diverge from the core model described previously [17]. The main model inputs are presented in Table 1.
| Parameter | Base-case value | PSA distribution | Ref. |
|---|---|---|---|
| Discount rate for costs | 3.5 % | Fixed | [22] |
| Discount rate for health outcomes | 3.5 % | Fixed | [22] |
| Time horizon | Lifetime (42 years) | Fixed | |
| Screening uptake rate | 46.5 % | Beta | [24–26] |
| Stage distribution | |||
| Stage I | 9.1% | Dirichlet | [27] |
| Stage II | 13.1% | Dirichlet | [27] |
| Stage III | 32.3% | Dirichlet | [27] |
| Stage IV | 45.5% | Dirichlet | [27] |
| Total population | 2,830,097 | Gamma | [3] |
| Population aged 50–74 years | 32.39% | Beta | [28] |
| Male | 46.60 % | Beta | [3] |
| Female | 53.40 % | Beta | [3] |
| Smoking rate | 18.6 % | Beta | [3] |
| Lung cancer incidence aged 50–74 years | 1100 | Gamma | local experts‡ |
| Costs | |||
| Recruitment costs | |||
| Information package | €2.51 | Gamma | [29] |
| Screening costs | |||
| CT scan | €42.48 | Gamma | [29] |
| Diagnostic costs per person | |||
| Screening round 1 | €2536 | Gamma | [29], local experts‡ |
| Screening round 2 onwards | €2478 | Gamma | [29], local experts‡ |
| No screening | €2920 | Gamma | [29], local experts‡ |
| Treatment costs per cycle | |||
| Stage I | |||
| Pre-progression state | |||
| First half-year (per cycle) | €1426 | Gamma | [30], local experts‡ |
| Follow-up costs year 1–2 (per cycle) | €33 | Gamma | [29,31] |
| Follow-up costs year 3–5 (per cycle) | €16 | Gamma | [29,31] |
| Post-progression state (one-time cost) | €16,696 | Gamma | [30,32–37], local experts‡ |
| Follow-up costs (per cycle) | €22 | Gamma | [30] |
| Stage II | |||
| Pre-progression state | |||
| First half-year (per cycle) | €1755 | Gamma | [30], local experts |
| Follow-up costs year 1–2 (per cycle) | €33 | Gamma | [29,31] |
| Follow-up costs year 3–5 (per cycle) | €16 | Gamma | [29,31] |
| Post-progression state (one-time cost) | €16,696 | Gamma | [30,32–37], local experts‡ |
| Follow-up costs (per cycle) | €22 | Gamma | [30] |
| Stage III | |||
| Pre-progression state | |||
| First year (per cycle) | €10,374 | Gamma | [30,32–37], local experts‡ |
| Second year (per cycle) | €1159 | Gamma | [30,32–37], local experts‡ |
| Follow-up (per cycle) | €22 | Gamma | [30] |
| Post-progression state (one-time cost) | €618 | Gamma | [30] |
| Follow-up (per cycle) | €22 | Gamma | [30] |
| Stage IV | |||
| Pre-progression state | |||
| First year (per cycle) | €14,640 | Gamma | [30,32–37], local experts‡ |
| Second year (per cycle) | €1728 | Gamma | [30,32–37], local experts‡ |
| Follow-up (per cycle) | €22 | Gamma | [30] |
| Post-progression state (one-time cost) | €538 | Gamma | |
| Follow-up (per cycle) | €22 | Gamma | [30] |
| End of life | €2393 | Gamma | [38] |
| Utilities | |||
| Pre-progression state | |||
| Stage I | 0.71 | Beta | [39] |
| Stage II | 0.68 | Beta | [39] |
| Stage III | 0.67 | Beta | [39] |
| Stage IV | 0.66 | Beta | [39] |
| Post-progression state | |||
| Stage I | 0.67 | Beta | [39] |
| Stage II | 0.67 | Beta | [39] |
| Stage III | 0.66 | Beta | [39] |
| Stage IV | 0.66 | Beta | [39] |
| Lung cancer-free participants† | |||
| Age-dependent utility values | |||
| 45–54 | 0.94 | Beta | [40] |
| 55–64 | 0.90 | Beta | [40] |
| 65–74 | 0.86 | Beta | [40] |
| ≥75 | 0.76 | Beta | [40] |
| Survival | |||
| OS (5-year survival rate) | |||
| Stage I | 54.8% | NA | [41] |
| Stage II | 28.6% | NA | [41] |
| Stage III | 10.6% | NA | [41] |
| Stage IV | 2.2% | NA | [41] |
| D/PFS (1-year D/PFS rate) | |||
| Stage I | 50% | NA | [42] |
| Stage II | 50% | NA | [43] |
| Stage III | 10.5% | NA | [44] |
| Stage IV | 1.4% | NA | [32,45,46] |
| Background mortality | |||
| Life expectancy by age | General population | Beta | [47] |
†
Lung cancer-free participants refer to people who either do not have lung cancer or have not been identified with lung cancer.
‡
An overview of the local experts can be found in S6 Table.
CT: Computed tomography; D/PFS: Disease/progression-free survival; NA: Not applicable; OS: Overall survival; PSA: Probabilistic sensitivity analysis.
Epidemiological data & eligible population
The eligible population was calculated based on the age inclusion criteria outlined by the NELSON study (50–74 years), and the smoking behaviors. The Lithuanian population aged 50–74 years was 916,668, and the local smoking rate was 18.6%, regardless of the pack years, for both sexes in the year 2022 [3,28]. Consequently, the total population eligible for screening amounted to 170,808 in Lithuania. The screening participants were estimated to be 79,426 based on an uptake rate of 46.5%, which was determined by the uptake rates observed in the current national screening programs for breast, colorectal and prostate cancer in Lithuania [24–26]. Real-world evidence from the NHS England LCS Programme demonstrated a comparable uptake rate of 49%, supporting the feasibility of achieving participation rates within this range in routine LCS practice [48]. The adherence rate was assumed to be 100%, based on a study evaluating the cost-effectiveness of LCS with LDCT [49]. The number of lung cancers detected in the no screening arm was calculated by the lung cancer incidence rate in the age category 50–74 and the current stage distribution at the time of diagnosis [27].
Survival
OS data was obtained from the Lithuanian Cancer Registry database and used to calculate the transition probability of patients transiting from the post-progression to death health state [41]. This registry covered the entire territory of Lithuania and contained comprehensive data concerning patient demographics and tumor characteristics, tracking all cancer patients until their death. The survival analysis included patients with primary invasive lung cancer (International Classification of Diseases, Tenth Revision [ICD-10] C34) diagnosed between 2013 and 2017, the most recent period with complete data. Patients were followed up until 31 October 2022. Among the extracted survival data, patients diagnosed before the age of 75 were categorized by the stage at diagnosis. Patients who died due to other causes than lung cancer were included in the analysis. Missed individuals were assumed to follow the OS rates of patients with lung cancer stage II.
Disease-free survival (DFS) and progression-free survival (PFS) were used to inform the transition probabilities of patients transiting from the pre- to post-progression health state in the Markov trace. DFS data for stage I patients were derived from a retrospective study conducted in the UK [42]. For stage II patients DFS rates were obtained from a clinical trial for early-stage lung cancer patients receiving surgery and chemotherapy [43]. PFS data for stage III and IV patients were synthesized from various clinical trials, representing the different lung cancer types and treatment options [32,44–46,50,51].
To reflect a lifetime horizon, survival extrapolation was performed using the statistical method supported by the NICE Technical Support Document and Guyot et al. using R Studio (2022.12.0 + 353) [52,53]. Details about distribution functions fitted per extrapolated survival curve are presented in Supplementary Table 1. Background mortality was used to account for all-cause mortality in the model and was based on life tables for Lithuania for the year 2020 and applied to both the screening and no screening arm [47].
Utilities
Lung cancer stage-specific utility values were obtained from a study using the British matrix, as suggested by the experts in the absence of the local data recommended by national guidelines [22,39]. For individuals in the preprogression state, the utility estimates were 0.71, 0.68, 0.67 and 0.66 for stages I, II, III and IV, respectively. The utility value of stage III lung cancer was applied (0.67) to progressive stage I and II patients in postprogression state, whereas the utility value of stage IV lung cancer (0.66) was used for progressive stage III and IV patients in the postprogression state, reflecting the disease deterioration [39]. Age-dependent utility norms for the general population were applied to those without a lung cancer diagnosis. In the absence of Lithuanian-specific life tables, EQ-5D index values from Poland were used as proxies because the two countries exhibit comparable population health characteristics, including life expectancy, population ageing and healthcare expenditure, as well as analogous cultural and healthcare systems, as suggested by the experts [40,54].
Costs
Direct costs, which encompassed recruitment, screening, diagnostic workup and treatment costs, were included to evaluate the cost-effectiveness of LCS from a healthcare perspective. Costs derived from international sources in the absence of Lithuania-specific data were adjusted to the Lithuanian context using purchasing power parities (PPP) and inflated to 2022 values in accordance with the Lithuanian health technology assessment guidelines [22,55,56]. Specifically, all costs were first inflated to 2022 price levels. Costs reported in Polish currency were then converted into US dollars by dividing the Polish costs by Poland’s PPP, after which the resulting US dollar values were converted into Lithuanian costs by multiplying them by Lithuania’s PPP.
Recruitment costs, consisting of an information package, were retrieved from the pricelist published by the Lithuanian NHIF and applied to the eligible screening population [29]. Screening costs were calculated based on the unit costs for an LDCT scan, which were obtained from the NHIF pricelist [29].
Diagnostic procedures for lung cancer patients consist of imaging studies with chest CT or FDG-PET, percutaneous cytologic analysis or biopsy, bronchoscopy, surgical procedures, among which endobronchial ultrasound is the most operated one, as well as the pulmonologist consultation and lung cancer tissue genetic testing. The unit costs per diagnostic procedure were derived from the NHIF pricelist and clinical experts [29]. Additionally, clinical experts were consulted to provide the utilization values per diagnostic procedure, reflecting the situation in the Vilnius (Lithuanian capital) area. The weighted diagnostic costs per person were calculated based on these costs and utilization per procedure (Supplementary Table 2) and were applied to screening participants who received a positive or a false-positive CT scan result in the screening arm and to those individuals who experienced lung cancer-related symptoms in the no screening arm. Additional costs of a pulmonologist consultation were applied to patients in the no screening arm, as they were diagnosed through clinical presentations.
The lung cancer pathway and utilization values were obtained from Lithuanian clinical experts. For stage I and II lung cancer patients in the pre-progression state, the first-line treatment options consisted of surgery with or without (neo) adjuvant chemotherapy and radiotherapy. For stage III and IV lung cancer patients, besides the conventional therapies, novel treatments (immunotherapy and targeted therapy) were also included in the treatment pathway. Respiratory surgery costs were provided by the Lithuanian clinical experts. Due to the lack of Lithuanian-specific costing data, radiotherapy and chemotherapy for lung cancer were retrieved from a Polish costing study as Poland is economically similar to Lithuania [30]. Novel treatment costs per patient were calculated based on costs retrieved from Lithuania’s NHIF [33], and median or mean treatment durations published by international clinical trials [32,34–37]. One-time the cycle cost of first-line stage III patients was applied to stage I and II patients entering the post-progression state in the Markov trace, mimicking the treatments that stage I and II patients receive as their cancer progress or recurs. Radiotherapy and chemotherapy costs were applied to stage III and IV patients entering the post-progression state [30]. More information regarding the treatment costs and utilization values is reported in Supplementary Table 3. For all patients follow-up costs after first- and second-line treatment were taken into account. Follow-up costs for stage I and II patients after first-line treatment included pulmonologist consultation and CT scan costs in the first 5 years after the initial treatment, which corresponds to the guideline of the European Society of Medical Oncology (ESMO) (Supplementary Table 4) [31]. For post-progression stage I and II patients and all stage III and IV patients, the follow-up costs were obtained from a Polish costing study [30]. End-of-life costs were obtained from a British study and applied to all patients who died from lung cancer, as this was the best available source [38].
Sensitivity analyses
One-way (univariant) sensitivity analysis (OSA) was performed using a variance of 20% on deterministic parameters to identify the principal determinates influencing the ICER, and the results are presented in a tornado diagram. Probabilistic sensitivity analysis (PSA) was conducted by 1000 iterations to evaluate model uncertainty, and the results are presented in an incremental cost-effectiveness scatterplot.
Scenario analysis
Several scenario analyses were conducted to explore the cost-effectiveness of LCS under different costs, clinical estimates, and different assumptions in the model structure. The cost-effectiveness was tested under various CT scan costs and immunotherapy costs. Additionally, the cost-effectiveness of LCS was investigated by applying lower diagnostic costs for false-positive screened individuals while the diagnostic remained unchanged for the true-positive cases, given the uncertainty regarding variations in the diagnostic follow-up pathway for false-positive screened individuals. Another scenario focused on the cost-effectiveness by increasing the background mortality rate, as the general health of smoking individuals is overall reduced, leading to a higher background mortality rate [57]. Additionally, a scenario was included that investigated screening-associated disutility [58]. Lastly, variations in the lung cancer incidence in the screening and no screening arm were analyzed as the Lithuanian lung cancer incidence is not in line with the incidence in the Dutch NELSON study population which affected the screening performance data in our study [59,60]. All the parameters used in scenario analyses are summarized in Supplementary Table 5 and all scenario analyses are listed in Table 3.
Results
Base-case results
Annual LCS with volumetric-enabled LDCT resulted in an increment of 6117 early-stage (I and II) lung cancers and a reduction of 1874 late-stage (III-IV) lung cancers for one screening cohort over a lifetime horizon in Lithuania. Consequently, early detection of lung cancer led to 2606 premature lung cancer deaths averted, resulting in 21,639 LYs gained, 15,391 QALYs gained and 0.96 QALY gained per lung cancer patient.
The recruitment costs and screening costs for an LCS program were approximately €0.4 million and €38.1 million, respectively. Over a lifetime horizon, LCS led to a reduction in treatment costs amounting to €37.8 million, primarily attributed to a decrease of €64.0 million in the treatment costs associated with late-stage (III and IV) lung cancer. The total incremental costs were approximately €21.1 million. This resulted in an ICER of €1372 per QALY gained for annual screening in Lithuania from a healthcare payer perspective (Table 2).
| Clinical and health outcomes | Screening | No screening | Incremental |
|---|---|---|---|
| Lung cancer diagnoses | |||
| Total | 16,083 (100%) | 11,840 (100%) | 4243 |
| Stage I | 7169 (45%) | 1080 (9.1%) | 6089 |
| Stage II | 1606 (10%) | 1578 (13.3%) | 28 |
| Stage III | 3621 (23%) | 3809 (32.2%) | -188 |
| Stage IV | 3687 (23%) | 5373 (45.4%) | -1686 |
| Missed individuals | NA | 4,243 | NA |
| Stage III and IV averted | 1874 | ||
| Lung cancer deaths | |||
| Total | 11,393 | 13,999 | -2606 |
| Stage I | 3321 | 500 | 2820 |
| Stage II | 1097 | 1077 | 20 |
| Stage III | 3393 | 3567 | -175 |
| Stage IV | 3583 | 5220 | -1638 |
| Missed individuals | NA | 3634 | NA |
| Life Years | |||
| Total | 2,195,320 | 2,173,681 | 21,639 |
| Stage I | 39,309 | 5896 | 33,414 |
| Stage II | 5512 | 5370 | 141 |
| Stage III | 5018 | 5254 | -236 |
| Stage IV | 2497 | 3636 | -1138 |
| Missed individuals | NA | 10,541 | NA |
| Lung cancer-free individuals† | 2,142,985 | 2,142,985 | 0 |
| QALYs | |||
| Total | 1,882,749 | 1,867,358 | 15,391 |
| Stage I | 29,741 | 4459 | 25,282 |
| Stage II | 4075 | 3967 | 108 |
| Stage III | 3357 | 3515 | -158 |
| Stage IV | 1648 | 2399 | -751 |
| Missed individuals | NA | 9089 | NA |
| Lung cancer-free individuals† | 1,843,928 | 1,843,928 | 0 |
| Cost outcomes (€) | |||
| Total | €386,774,935 | €365,658,478 | €21,116,457 |
| Recruitment costs | €428,729 | – | €428,729 |
| Screening costs | €38,120,648 | – | €38,120,648 |
| Diagnostic costs | €71,046,593 | €50,706,113 | €20,340,481 |
| Treatment costs | €277,178,965 | €314,952,365 | €-37,773,400 |
| Stage I | €30,649,255 | €4,604,976 | €26,044,278 |
| Stage II | €7,268,733 | €7,103,921 | €164,812 |
| Stage III | €110,515,073 | €115,783,743 | €-5268,670 |
| Stage IV | €128,745,904 | €187,459,724 | €-58,713,821 |
| Health economic outcomes | |||
| ICER per QALY | €1372 | ||
| NMB‡ | €345,286,878 |
†
Lung cancer-free individuals refer to the screening participants who do not have lung cancer.
‡
Calculated based on one-time the GDP (€23,806).
ICER: Incremental cost-effectiveness ratio; NA: Not applicable; NMB: Net monetary benefit; QALYs: Quality-adjusted life year.
| Scenario name | Screening | No screening | Incremental total costs | Incremental QALYs | ICER | ||
|---|---|---|---|---|---|---|---|
| Total costs | Total QALYs | Total costs | Total QALYs | ||||
| Base case | €386,774,935 | 1,882,749 | €365,658,478 | 1,867,358 | €21,116,457 | 15,391 | €1372 |
| Time horizon - 5 year | €161,360,805 | 675,831 | €151,055,279 | 675,070 | €10,305,526 | 762 | €13,525 |
| Time horizon - 10 year | €279,182,129 | 1158,514 | €263,621,538 | 1154,953 | €15,560,591 | 3561 | €4369 |
| Time horizon - 15 year | €360,828,338 | 1,485,292 | €341,589,894 | 1,477,813 | €19,238,444 | 7479 | €2572 |
| Decrease discount rate (costs: 0%, health outcomes: 0%) | €488,971,210 | 2649,956 | €462,723,124 | 2622,861 | €26,248,085 | 27,095 | €969 |
| Increase discount rate (costs: 6%, health outcomes: 6%) | €333,965,873 | 1,547,052 | €315,415,215 | 1,536,248 | €18,550,659 | 10,804 | €1717 |
| Screening uptake rate of 25% | €379,298,025 | 1,885,862 | €367,746,862 | 1,877,587 | €11,551,163 | 8275 | €1396 |
| Screening uptake rate of 75% | €396,686,187 | 1,878,623 | €362,890,155 | 1,853,799 | €33,796,033 | 24,825 | €1361 |
| Adherence rate of 90% | €381,674,936 | 1,884,817 | €367,034,411 | 1,875,300 | €14,640,525 | 9517 | €1538 |
| Adherence rate of 70% | €378,390,537 | 1,886,440 | €368,273,875 | 1,881,420 | €10,116,663 | 5019 | €2016 |
| Adherence rate of 50% | €377,395,553 | 1,887,053 | €368,788,281 | 1,883,693 | €8,607,272 | 3,360 | €2562 |
| OS for missed individuals equals stage I patients | €386,774,935 | 1,882,749 | €365,658,478 | 1,871,891 | €21,116,457 | 10,859 | €1945 |
| OS for missed individuals equals stage III patients | €386,774,935 | 1,882,749 | €365,658,478 | 1,863,438 | €21,116,457 | 19,312 | €1093 |
| OS for missed individuals equals stage IV patients | €386,774,935 | 1,882,749 | €365,658,478 | 1,860,817 | €21,116,457 | 21,932 | €963 |
| Reduction of LC incidence in screening population according to LC incidence ratio between Lithuania and The Netherlands | €342,228,966 | 1,896,167 | €369,270,500 | 1,885,113 | -€27,041,535 | 11,054 | -€2446 |
| Adjust the lung cancer incidence in the non-screened population to match the incidence rate observed in The Netherlands (0.86%) | €510,715,976 | 1,857,844 | €600,512,022 | 1,839,226 | -€89,796,046 | 18,618 | -€4823 |
| Increase background mortality by 100% | €334,024,144 | 1,454,154 | €315,220,705 | 1,444,736 | €18,803,439 | 9419 | €1996 |
| Include increase OS for stage III and IV patients by an HR of 0.9 | €390,521,046 | 1,882,838 | €371,091,914 | 1,867,470 | €19,429,131 | 15,368 | €1264 |
| Include increase OS for stage III and IV patients by an HR of 0.8 | €394,265,368 | 1,882,927 | €376,522,917 | 1,867,583 | €17,742,451 | 15,345 | €1156 |
| Include screening-associated disutility | €386,774,935 | 1,881,265 | €365,658,478 | 1,867,358 | €21,116,457 | 13,907 | €1518 |
| Decrease CT scan costs by 50% (€21) | €367,714,611 | 1,882,749 | €365,658,478 | 1,867,358 | €2,056,133 | 15,391 | €134 |
| Increase CT scan costs by 10% (€47) | €390,587,000 | 1,882,749 | €365,658,478 | 1,867,358 | €24,928,522 | 15,391 | €1620 |
| Increase CT scan costs by 50% (€64) | €405,835,259 | 1,882,749 | €365,658,478 | 1,867,358 | €40,176,781 | 15,391 | €2610 |
| Double CT scan costs (€84.96) | €424,895,583 | 1,882,749 | €365,658,478 | 1,867,358 | €59,237,105 | 15,391 | €3849 |
| Double recruitment costs (€5.02) | €387,203,664 | 1,882,749 | €365,658,478 | 1,867,358 | €21,545,186 | 15,391 | €1400 |
| Decrease immunotherapy unit costs by 50% | €299,851,737 | 1,882,749 | €257,671,611 | 1,867,358 | €42,180,125 | 15,391 | €2741 |
| Decrease diagnostic costs for false positive individuals by 50% (€1213) | €375,682,991 | 1,882,749 | €365,658,478 | 1,867,358 | €10,024,513 | 15,391 | €651 |
†
The positive screening outcomes were decreased using a ratio based on the difference between the lung cancer incidence in Lithuania and The Netherlands.
CT: Computed tomography; HR: Hazard ratio; LC: Lung cancer; OS: Overall survival.
Sensitivity analyses
OSA showed that the most influential parameter was the costs provided in the first 6 months to individuals in stage IV pre-progression state, varying the ICER from €748 to €1996 per QALY. Other key drivers were the screening costs, diagnostic costs provided to the false-positive individuals, stage I treatment costs, utility value for stage I pre-progression patients, smoking rate and diagnostic costs for the screening and no screening arm. All ICER variations of the OSA were under the WTP threshold of €23,806 per QALY, equal to one-time the GDP per capita in Lithuania (Figure 1). PSA resulted in a probabilistic ICER of €1303 per QALY with a cost-effectiveness probability of 100%. Figure 2 shows the outcomes of the probabilistic simulations and the cost-effectiveness acceptability curve in which all outcomes were under the WTP threshold.
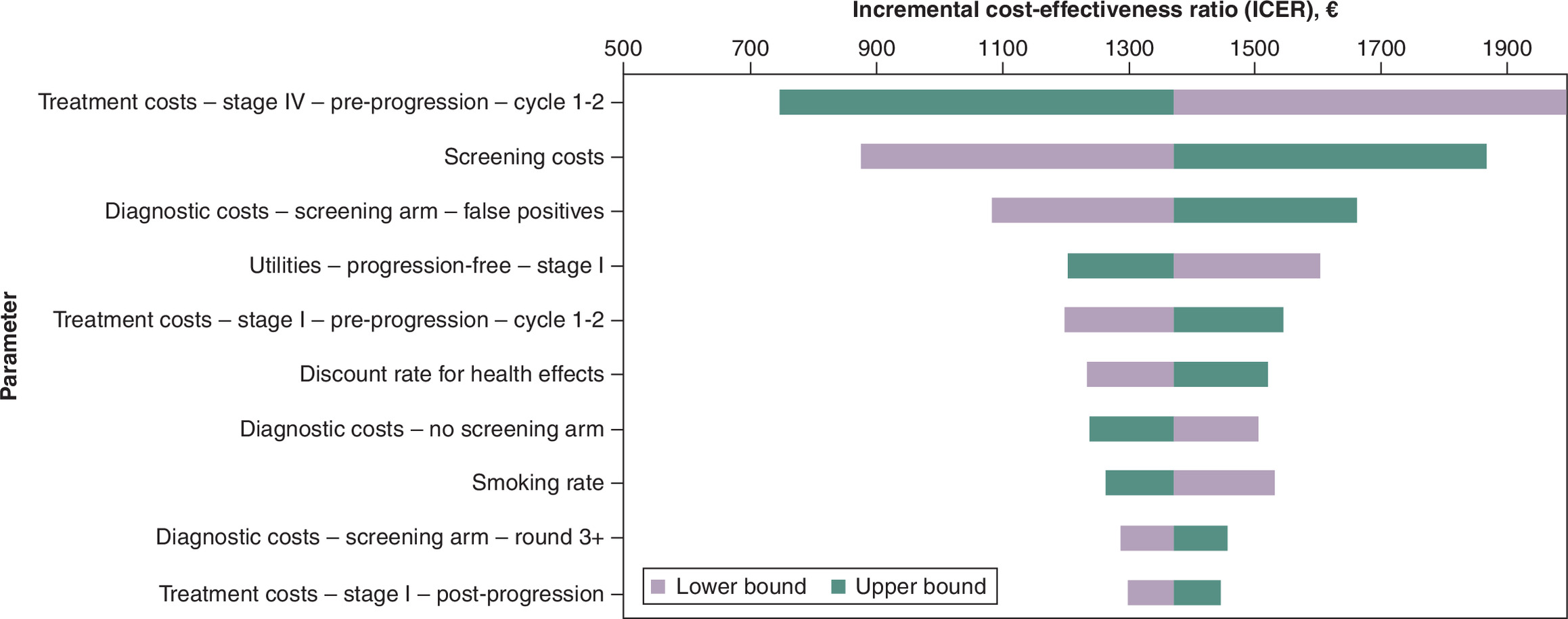
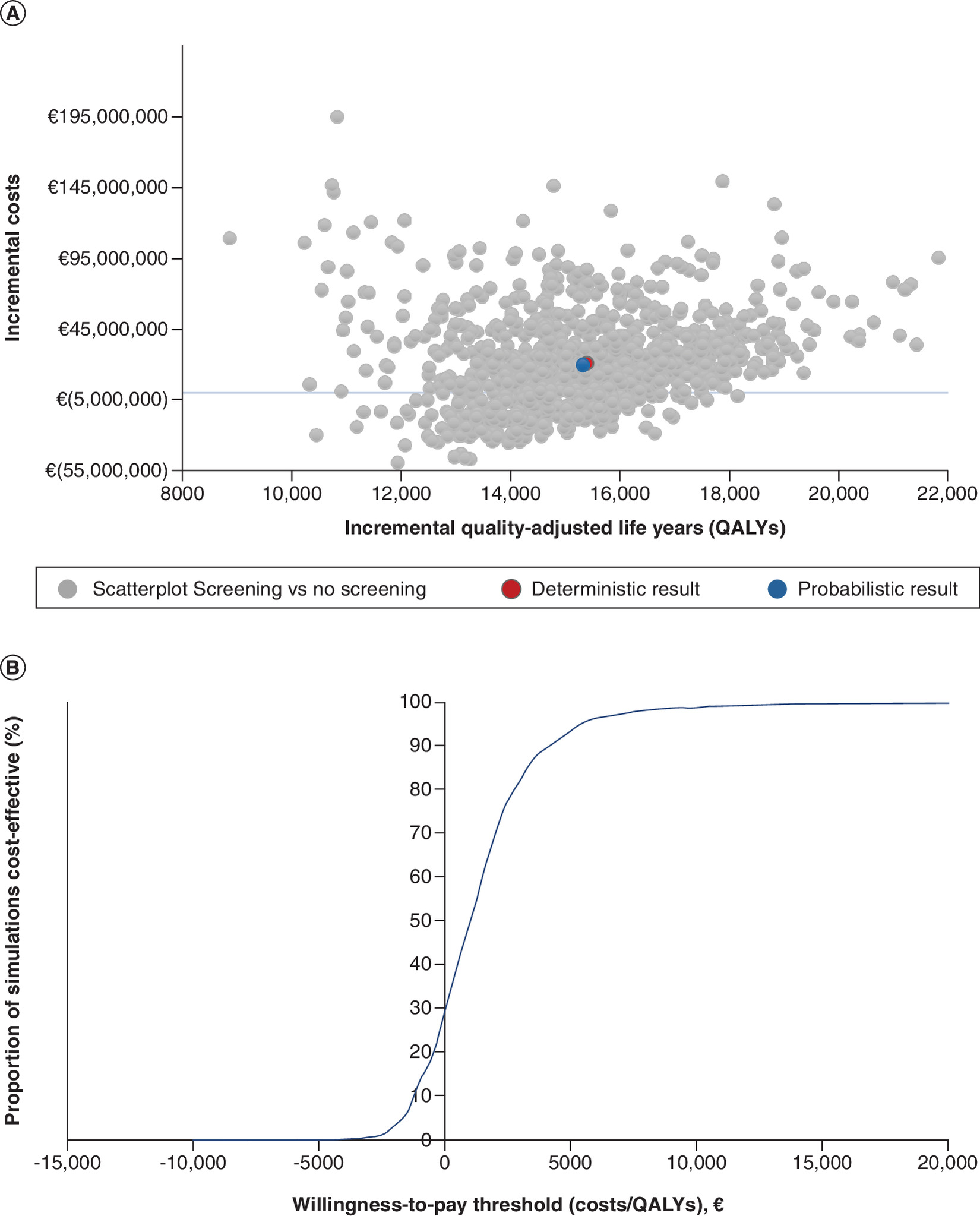
Figure 2. Results obtained from 1000 Monte Carlo simulations for the probabilistic sensitivity analysis.
(A) Incremental cost-effectiveness scatterplot. (B) Cost-effectiveness acceptability curve.
QALY: Quality-adjusted life year.
Scenario analysis
All scenario outcomes fell below the WTP threshold (one-time the GDP of €23,806), as presented in Table 3. The major impact of CT scan costs on the ICER is shown by the fact that an increase in CT scan costs by 50% resulted in an increased ICER of €2610 per QALY. Meanwhile, lowering the diagnostic costs for false-positive cases by 50% resulted in a decreased ICER of €651 per QALY. The scenario focusing on the lung cancer incidence in Lithuania showed that increasing the lung cancer incidence rate in the Lithuanian population, resulted in total cost savings (€89.8 million) and more incremental QALYs gained (18,618).
Discussion
This study provided evidence on the cost-effectiveness of LCS with volumetric-enabled LDCT screening for high-risk individuals, compared with no screening in Lithuania. The base case analysis revealed an ICER of €1372 per QALY, with incremental costs of €21.1 million and incremental QALYs of 15,391. In addition, LCS resulted in 6117 more lung cancers detected at an early stage, and 2606 premature lung cancer cases averted. Sensitivity analysis indicates that results are robust, showing an average probabilistic ICER of €1303 per QALY. The PSA demonstrated a broad range of incremental costs. Although all PSA simulations remained below the willingness-to-pay threshold, the variation in incremental cost (-€56.5 million to +195 million) indicates uncertainty regarding the potential budget impact of nationwide implementation, likely driven by variability in model assumptions and key input parameters.
This is to our knowledge the first analysis evaluating the cost-effectiveness of LCS in Lithuania. Our findings are consistent with the existing literature. A systematic review showed that most of the studies reported that LCS would be cost-effective [49]. Cost-effectiveness studies from Poland and Hungary showed an ICER of €1354 per life year and €6968 per QALY [30,61]. Compared with a German study (ICER: €30,291 per QALY) our cost-effectiveness ICER appears relatively low. This may be explained by our inclusion of costly late-stage immunotherapy, the relatively lower CT scan costs in Lithuania compared with Germany, and our use of a lifetime time horizon versus the 15-year horizon in the German study [62].
The sensitivity analysis indicated that lung cancer stage IV treatment costs had the biggest impact on the ICER, primarily explained by the elevated expense related to immunotherapy. Reducing the immunotherapy costs by 50% resulted in an ICER of €2741 per QALY, surpassing the base case ICER and aligning more closely with the studies that did not incorporate late-stage immunotherapy costs [49,61].
Secondly, the CT scan costs (€42) were an influential parameter affecting the ICER. However, these costs might increase over time, as with each repetition of LDCT, the assessment duration is prolonged due to the necessity for radiologists to compare with prior scans. Nevertheless, scenario analyses revealed that increasing the CT scan costs by 10% and doubling the CT scan costs increased the ICER to €1620 and €3849 per QALY, respectively, indicating that this rise in CT scan costs resulted in marginal changes in the ICER. Conversely, LDCT LCS could potentially be more cost-effective with the usage of artificial intelligence (AI) guided imaging reading. Introducing the use of AI guided imaging reading in a volume-based LDCT screening program reduces radiologists' workload by shortening the time of lung nodule detection and assessment of its size dynamics and improves the screening performance [63].
It was observed that the increased incidence rate due to screening was 35.8%. This over-exceeding screen-detected lung cancer is also seen in other countries, such as The Netherlands where the NELSON was performed [7]. This may be attributed to asymptomatic patients in the no screening scenario, in whom the underlying disease remained undetected. Therefore, to provide a conservative estimate of the benefits provided by LCS, we also included this asymptomatic cohort in the no-screening arm and called them “missed individuals”. However, the proportion of the missed individuals in Lithuania amounted to 24.6%. This might be partially explained by the mismatch of the high smoking rate in Lithuania decades ago (41.2% in the year 2000), and the lung cancer incidence nowadays (0.52%), as the counterparts in The Netherlands were 32% smoking rate in the year 2000 and 0.87% incidence nowadays [64]. The trend in incidence correlates with the high tobacco consumption decades ago [65]. The discrepancy between lung cancer incidence and smoking rate could be due to other competing mortality outcomes such as ischemic heart disease [66]. Therefore, we have employed scenario analysis to explore a higher lung cancer incidence in the no-screening arm, and results showed more health gain and cost-saving compared with the base case.
The low participation rate (5.8%) and adherence rate of the implemented LCS screening program in the United Status are causing some concerns [67,68]. However, in Europe, the participation rate seemed more favorable with 53.0% and 51.1% for the UK LCS pilot and the NELSON study, respectively [69,70]. Various uptake rates and adherence rates were tested in our analysis, revealing that high uptake rates would yield more health advantages and efficient utilization of resources allocated to screening. An uptake rate of 25% resulted in 0.58 QALY gained per lung cancer patient compared with 1.34 QALY gained per lung cancer patient at an uptake rate of 75%. To achieve high uptake rates personalized recruitment strategies have been proven to increase the coverage of screening programs [71]. Therefore, a centrally organized information system, covering the recruitment of participants, is recommended when implementing LCS in Lithuania, as the current running nationwide screening programs in Lithuania have limited coverage and participation [72,73]. Evidence from LCS pilot studies suggests that the implementation of such systems may involve substantial infrastructural requirements, including a robust data management system and the allocation of additional administrative resources for program coordination. These resources are needed to support key functions such as patient navigation, reminder systems, provider education, targeted awareness initiatives, appointment scheduling, and systematic recall [74,75].
Most limitations of this model mirror those observed in the original UK model [17]. Additionally, although a literature search was performed for the best Lithuania-specific available data, studies on quality of life and costing data were lacking. Therefore, data sources from the UK and Poland were used as an alternative for missing data. These limitations were mitigated by OSA and PSA. One of the strengths of the model was the Lithuanian OS data used to reflect the local context. This data included patients diagnosed between 2013 to 2017 and were followed up till 2022. For the costing part, we did include novel therapies for stage III and IV patients while the increased use of novel therapies for lung cancer treatment started after 2017, indicating that the local OS data partly reflects the introduction of novel therapies. Moreover, to enhance treatment accessibility and improve life expectancy of cancer patients, changes to pharmaceutical policies have been introduced by the Lithuanian government since 2017 [72]. This change aimed to benefit all individuals who face out-of-pocket pharmaceutical expenses. Therefore, the analysis potentially underestimates the health outcomes for stage III and IV patients, as improvements in OS data are expected since 2017, indicating a potential overestimation of the ICER.
Currently, the chest LDCT is underutilized in an LCS program. Extending screening to lung cancer, chronic obstructive pulmonary disease, and cardiovascular disease is likely to improve the cost-effectiveness and health benefits [76–78]. Furthermore, screening in the high-risk population defined solely by age and smoking behaviors may not be socially fair, as lung cancer also occurs among ever- and never-smokers and an increasing trend of lung cancer among never-smokers has been observed [79,80]. In addition, due to the strict eligibility criteria, LCS misses out on more than 50% of lung cancers [81,82]. This was supported by a prospective cohort study which showed a higher cumulative lung cancer diagnosis hazard in the screening group who were selected irrespective of their smoking history [83]. Therefore, further implementation studies could focus on expanding the target group for screening, as well as the detection of other comorbidities alongside lung cancer concurrently through the LDCT, as envisioned by the Lithuanian lung cancer experts and representatives. Thereafter, further investigations into the cost-effectiveness of LCS under the new findings and insights could be carried out to pave the way for evidence-based decision-making.
Conclusion
This study provides evidence that annual LCS with volume-based LDCT compared with no screening for a high-risk population could be cost-effective in Lithuania. Premature lung cancer deaths were averted, resulting in QALYs and LYs gained. The screening and diagnostic costs were the main drivers for the incremental costs. Although we aimed to included only Lithuanian-specific data, some inputs were derived from other countries due to unavailable local data. Future screening studies should focus on the optimization of the program and further investigations into the cost-effectiveness of such optimized LCS program. This could include investigating a central information and recruitment system to increase the screening uptake rate, monitoring the potential over-exceeding screen-detected lung cancers and the possibility of extending screening to other diseases such as chronic obstructive pulmonary disease, and cardiovascular disease.
Summary points
•
Cancer mortality in Lithuania is above the European average. Lung cancer stands as the leading cause of cancer-related mortality in Lithuania, with low overall survival. Screening with low-dose computed tomography for high-risk individuals can facilitate the detection of lung cancer at earlier stages, subsequently reducing lung cancer-specific mortality.
•
This study evaluated the long-term clinical and economic outcomes of an annual lung cancer screening (LCS) program compared with no screening, adopting a lifetime horizon and the Lithuanian healthcare system perspective.
•
A validated cost-effectiveness model originally developed for the UK was adapted to the Lithuanian context and informed by data from the Dutch–Belgian NELSON trial. The model comprised a decision tree with an integrated Markov structure reflecting lung cancer progression across stages I–IV, including transitions to post-progression and death.
•
Overall survival data was obtained from real-world data registered by National Cancer Institute of Lithuania.
•
The total incremental cost of the LCS program was €21.1 million. The primary contributors that affect the ICER the most were treatment costs for stage IV patients and CT scan costs for the screening. Also, the CT scan costs for screening were the primary contributor to the overall program costs.
•
Annual LCS using increased the detection of 6117 early-stage (I and II) lung cancers while reducing the number of 1874 late-stage (III and IV) cases over a lifetime horizon in Lithuania. This shift toward earlier detection consequently averted 2606 premature lung cancer deaths in the screened cohort.
•
The screening program yielded 15,391 incremental QALYs and 21,639 additional life-years. On a per-patient basis, this equates to 0.96 QALY gained for each individual diagnosed with lung cancer, demonstrating the health benefits of screening.
•
The results demonstrate that annual LCS represents a potentially cost-effective strategy in Lithuania, yielding an ICER of €1372 per QALY gained in comparison to no screening.
Author contributions
HT Berge, G Piazza and X Pan contributed to the conception and design of study. HT Berge, G Piazza and T Bukšnys conducted the data acquisition. HT Berge, G Piazza and D Ramaker were responsible for the data analysis. All authors reviewed and participated in the interpretation of the data. E Danila provided critical feedback and supervision throughout the research process. HT Berge and G Piazza drafted the manuscript. All authors participated in the data validation, data interpretation and critical revision of the paper. Final approval of the manuscript was given by all authors.
Financial disclosure
This work was funded by AstraZeneca PLC, UK.
Competing interests disclosure
H ten Berge, G Piazza, D Ramaker and X Pan are employed by iDNA. T Bukšnys is employed by AstraZeneca. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 144.75 KB
References
Papers of special note have been highlighted as: • of interest
1.
International Agency for Research on Cancer. Cancer Today. (2024). (Accessed 24 September 2025). https://gco.iarc.who.int
2.
Gedvilaitė V, Danila E, Cicėnas S, Smailytė G. Lung cancer in Lithuania. J. Thorac. Oncol. 15(9), 1401–1405 (2020).
3.
Official Statistics Portal. Database Indicators. (Accessed 6 December 2022). https://osp.stat.gov.lt/statistiniu-rodikliu-analize#/
4.
OECD/European Commission. EU Country Cancer Profile: Lithuania 2025. EU Country Cancer Profiles, OECD Publishing, France (2025).
5.
Gedvilaitė V, Danila E, Cicėnas S, Smailytė G. Lung cancer survival in Lithuania: changes by histology, age, and sex from 2003–2007 to 2008–2012. Cancer Control 26(1), 1073274819836085 (2019).
• Shows the low survival rates of late stage diagnosed lung cancer patients in Lithuania.
6.
The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 365(5), 395–409 (2011).
7.
de Koning HJ, van der Aalst CM, de Jong PA et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 382(6), 503–513 (2020).
• The NELSON trial, the largest European lung cancer study, demonstrates that low-dose CT screening significantly reduces lung cancer mortality.
8.
Kerpel-Fronius A, Monostori Z, Kovacs G et al. Nationwide lung cancer screening with low-dose computed tomography: implementation and first results of the HUNCHEST screening program. Eur. Radiol. 32(7), 4457–4467 (2022).
9.
Becker N, Motsch E, Gross ML et al. Randomized study on early detection of lung cancer with MSCT in Germany: study design and results of the first screening round. J. Cancer Res. Clin. Oncol. 138(9), 1475–1486 (2012).
10.
Infante M, Lutman FR, Cavuto S et al. Lung cancer screening with spiral CT: baseline results of the randomized DANTE trial. Lung Cancer 59(3), 355–363 (2008).
11.
Pegna AL, Picozzi G, Falaschi F et al. Four-year results of low-dose CT screening and nodule management in the ITALUNG trial. J. Thorac. Oncol. 8(7), 866–875 (2013).
12.
Pastorino U, Rossi M, Rosato V et al. Annual or biennial CT screening versus observation in heavy smokers: 5-year results of the MILD trial. Eur. J. Cancer Prev. 21(3), 308–315 (2012).
13.
Field JK, Duffy SW, Baldwin DR et al. The UK Lung Cancer Screening Trial: a pilot randomised controlled trial of low-dose computed tomography screening for the early detection of lung cancer. Health Technol. Assess. 20(40), 1–146 (2016).
14.
European Council - Council of the European Union. Council updates its recommendation to screen for cancer. (Accessed 12 December 2022). https://www.consilium.europa.eu/en/press/press-releases/2022/12/09/council-updates-its-recommendation-to-screen-for-cancer/
15.
Danila E, Krynke L, Ciesiūnienė A et al. The Lithuanian Lung Cancer Screening Model: results of a pilot study. Cancers (Basel) 17(12), 1956 (2025).
• This pilot study demonstrates that lung cancer screening (LCS) is feasible, well-organized and clinically valuable.
16.
Knudsen AB, McMahon PM, Gazelle GS. Use of modeling to evaluate the cost-effectiveness of cancer screening programs. J. Clin. Oncol. 25(2), 203–208 (2007).
17.
Pan X, Dvortsin E, Baldwin DR et al. Cost-effectiveness of volume computed tomography in lung cancer screening: a cohort simulation based on Nelson study outcomes. J. Med. Econ. 27(1), 27–38 (2024).
• We used the model framework developed in this study to evaluate the cost-effectiveness of LCS in Lithuania.
18.
Veronesi G, Baldwin DR, Henschke CI et al. Recommendations for implementing lung cancer screening with low-dose computed tomography in Europe. Cancers (Basel) 12(6), doi: (2020) (Epub ahead of print).
19.
National Institute for Health and Care Excellence. Lung cancer: diagnosis and management. NICE Guideline NG122. (2019). https://www.nice.org.uk/guidance/ng122
20.
Horeweg N, Van Der Aalst CM, Vliegenthart R et al. Volumetric computed tomography screening for lung cancer: three rounds of the NELSON trial. Eur. Respir. J. 42(6), 1659–1667 (2013).
21.
Behmane D, Lambot K, Irs A. Baltic guideline for economic evaluation of pharmaceuticals (Pharmacoeconomic Analysis). (2002). (Accessed 2 December 2022). https://www.ispor.org/heor-resources/more-heor-resources/pharmacoeconomic-guidelines/pe-guideline-detail/baltic-(latvia-lithuania-estonia)
22.
Minister of Health Protection of the Republic of Lithuania. Regarding the approval of the description of the procedure for incorporation of medicinal products and medical aid equipment in the compensation lists and their change. (2022). (Accessed 26 July 2023). https://www.e-tar.lt/portal/lt/legalAct/TAR.E83CFAB10E7B/asr
23.
Iino H, Hashiguchi M, Hori S. Estimating the range of incremental cost-effectiveness thresholds for healthcare based on willingness to pay and GDP per capita: a systematic review. PLoS One 17(4), e0266934 (2022).
24.
Steponaviciene L, Vincerzevskiene I, Briediene R, Urbonas V, Vanseviciute-Petkeviciene R, Smailyte G. Breast cancer screening program in Lithuania: interval cancers and program sensitivity after 7 years of mammography screening. Cancer Control 26(1), 1073274819874122 (2019).
25.
Dulskas A, Poskus T, Kildusiene I et al. National colorectal cancer screening program in Lithuania: description of the 5-year performance on population level. Cancers (Basel) 13(5), 1129 (2021).
26.
Patasius A, Krilaviciute A, Smailyte G. Prostate cancer screening with PSA: ten years' experience of population based early prostate cancer detection programme in Lithuania. J. Clin. Med. 9(12), 3826 (2020).
27.
Gedvilaitė V, Danila E, Cicėnas S, Smailytė G. Lung cancer survival in Lithuania: changes by histology, age, and sex from 2003–2007 to 2008–2012. J. Thorac. Oncol. 15(9), 1401–1405 (2020).
28.
United Nations – Department of Economic and Social Affairs. World Population Prospects 2022, Summary of Results. NY, USA (2022).
29.
Public Hospital Fund under the Ministry of Health (VLK). Prices of compensatory services. (2022). (Accessed 5 December 2022). https://ligoniukasa.lrv.lt/lt/veiklos-sritys/gydymo-istaigoms-ir-partneriams/kompensuojamuju-paslaugu-kainos/sveikatos-prieziuros-paslaugu-bazines-kainos%20%20%E2%80%9EBrangieji%20tyrimai%20ir%20proced%C5%ABros,%20teikiami%20ambulatorin%C4%97mis%20s%C4%85lygomis%20bei%20taikant%20ilgalaik%C4%AF%20ir%20(ar)%20reabilitacin%C4%AF%20gydym%C4%85%E2%80%9C,%202022
30.
Kanarkiewicz M, Szczęsny TJ, Krysiński J, Buciński A, Kowalewski J, Pawłowicz Z. Cost-effectiveness analysis of lung cancer screening with low-dose computerised tomography of the chest in Poland. Contemp. Oncol. 19(6), 480 (2015).
31.
Postmus PE, Kerr KM, Oudkerk M et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 28(Suppl. 4), iv1–iv21 (2017).
32.
Soria J-C, Ohe Y, Vansteenkiste J et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N. Engl. J. Med. 378(2), 113–125 (2018).
33.
National Health Insurance Fund under the Ministry of Health. Medicines and medical aids (MPP). (Accessed 11 July 2023). https://ligoniukasa.lrv.lt/lt/veiklos-sritys/gyventojams-1/vaistai-ir-medicinos-pagalbos-priemones-mpp
34.
Reck M, Rodríguez-Abreu D, Robinson AG et al. Updated analysis of KEYNOTE-024: pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J. Clin. Oncol. 37(7), 537–546 (2019).
35.
Gadgeel S, Rodríguez-Abreu D, Speranza G et al. Updated analysis From KEYNOTE-189: pembrolizumab or placebo plus pemetrexed and platinum for previously untreated metastatic nonsquamous non-small-cell lung cancer. J. Clin. Oncol. 38(14), 1505–1517 (2020).
36.
Socinski MA, Nishio M, Jotte RM et al. IMpower150 final overall survival analyses for atezolizumab plus bevacizumab and chemotherapy in first-line metastatic nonsquamous NSCLC. J. Thorac. Oncol. 16(11), 1909–1924 (2021).
37.
Mok T, Camidge DR, Gadgeel SM et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Ann. Oncol. 31(8), 1056–1064 (2020).
38.
Round J, Jones L, Morris S. Estimating the cost of caring for people with cancer at the end of life: a modelling study. Palliat. Med. 29(10), 899–907 (2015).
39.
Tramontano AC, Schrag DL, Malin JK et al. Catalog and comparison of societal preferences (utilities) for lung cancer health states: results from the Cancer Care Outcomes Research and Surveillance (CanCORS) study. Med. Decis. Making 35(3), 371–387 (2015).
40.
Golicki D. General population reference values for the EQ-5D-5L index in Poland: estimations using a Polish directly measured value set. Pol. Arch. Intern. Med. 131(5), 484–486 (2021).
41.
National Cancer Institute of Lithuania (NVI). Cancer Registry. (2022). https://registras.nvi.lt/lt/
42.
McPherson I, Bradley NA, Govindraj R, Kennedy ED, Kirk AJB, Asif M. The progression of non-small cell lung cancer from diagnosis to surgery. Eur. J. Surg. Oncol. 46(10 Pt A), 1882–1887 (2020).
43.
Felip E, Altorki N, Zhou C et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB–IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, Phase 3 trial. Lancet 398(10308), 1344–1357 (2021).
44.
Antonia SJ, Villegas A, Daniel D et al. Durvalumab after chemoradiotherapy in stage iii non–small-cell lung cancer. N. Engl. J. Med. 377(20), 1919–1929 (2017).
45.
Horn L, Mansfield AS, Szczęsna A et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N. Engl. J. Med. 379(23), 2220–2229 (2018).
46.
Gandhi L, Rodríguez-Abreu D, Gadgeel S et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung cancer. N. Engl. J. Med. 378(22), 2078–2092 (2018).
47.
Human Mortality Database. Lithuania. (2022). (Accessed 23 February 2024). https://www.mortality.org/Country/Country?cntr=LTU
48.
Lee RW, Nair A, Balata H et al. Implementation of the NHS England Lung Cancer Screening Programme over 5 years. Nat. Med. 32(5), 1817–1826 (2026).
49.
Grover H, King W, Bhattarai N, Moloney E, Sharp L, Fuller L. Systematic review of the cost-effectiveness of screening for lung cancer with low dose computed tomography. Lung Cancer 170, 20–33 (2022).
50.
Harrison PT, Vyse S, Huang PH. Rare epidermal growth factor receptor (EGFR) mutations in non-small cell lung cancer. Semin. Cancer Biol. 61, 167–179 (2020).
51.
Rosell R, Moran T, Queralt C et al. Screening of epidermal growth factor receptor mutation in lung cancer. N. Engl. J. Med. 361(10), 958–967 (2009).
52.
Latimer N. NICE DSU Technical Support Document 14: survival analysis for economic evaluations alongside clinical trials – extrapolation with patient-level data. Report by the Decision Support Unit (2011). https://www.ncbi.nlm.nih.gov/books/NBK395885/pdf/Bookshelf_NBK395885.pdf
53.
Guyot P, Ades AE, Beasley M, Lueza B, Pignon J-P, Welton NJ. Extrapolation of survival curves from cancer trials using external information. Med. Decis. Making 37(4), 353–366 (2017).
54.
OECD. EU Country Cancer Profile: Poland 2023, EU Country Cancer Profiles. OECD Publishing, France (2023).
55.
OECD. Purchasing power parities (PPP). (Accessed 5 July 2023). https://www.oecd.org/en/data/indicators/purchasing-power-parities-ppp.html
56.
Eurostat. HICP - inflation rate. (Accessed 16 March 2023). https://ec.europa.eu/eurostat/databrowser/view/tec00118/default/table?lang=en
57.
Centers for Disease Control and Prevention. Health Effects of Cigarette Smoking. (2021). (Accessed 27 July 2023). https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/index.htm
58.
Snowsill T, Yang H, Griffin E et al. Low-dose computed tomography for lung cancer screening in high-risk populations: a systematic review and economic evaluation. Health Technol. Assess. 22(69), 1–276 (2018).
59.
World Health Organization – International Agency for Research on Cancer. Estimated number of new cases in 2020, lung both sexes, ages 50–74. (2020). (Accessed 3 August 2023). https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=population&mode_population=countries&population=900&populations=900&key=asr&sex=0&cancer=15&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=10&ages_group%5B%5D=14&group_cancer=0&include_nmsc=0&include_nmsc_other=1
60.
Horeweg N, Van Der Aalst CM, Vliegenthart R et al. Volumetric computed tomography screening for lung cancer: three rounds of the NELSON trial. Eur. Respir. J. 42(6), 1659–1667 (2013).
61.
Nagy B, Szilberhorn L, Győrbíró DM et al. Shall we screen lung cancer with low-dose computed tomography? Cost-effectiveness in Hungary. Value Health Reg. Issues 34, 55–64 (2023).
62.
Hofer F, Kauczor H-U, Stargardt T. Cost-utility analysis of a potential lung cancer screening program for a high-risk population in Germany: a modelling approach. Lung Cancer 124, 189–198 (2018).
63.
Lancaster HL, Zheng S, Aleshina OO et al. Outstanding negative prediction performance of solid pulmonary nodule volume AI for ultra-LDCT baseline lung cancer screening risk stratification. Lung Cancer 165, 133–140 (2022).
64.
MacroTrends. World Smoking Rate 2000–2023. (2023). (Accessed 15 June 2023). https://www.macrotrends.net/countries/WLD/world/smoking-rate-statistics
65.
Liutkute V, Veryga A, Štelemekas M, Midttun NG. Burden of smoking in Lithuania: attributable mortality and years of potential life lost. Eur. J. Public Health 27(4), 736–741 (2017).
• Smoking-related diseases pose a major public health problem in Lithuania, causing a substantial mortality burden that affects men nine times more than women.
66.
OECD/European Observatory on Health Systems and Policies. Lithuania: Country Health Profile 2021, State of Health in the EU, OECD Publishing, Paris/European Observatory on Health Systems and Policies, Brussels (2021).
67.
American Lung Association. State of Lung Cancer 2022. Chicago, IL, USA (2022). https://www.lung.org
68.
Barbosa EJM, Yang R, Hershman M. Real-world lung cancer CT screening performance, smoking behavior, and adherence to recommendations: lung-RADS category and smoking status predict adherence. AJR Am. J. Roentgenol. 216(4), 919–926 (2021).
69.
Ruparel M, Quaife SL, Dickson JL et al. Lung Screen Uptake Trial: results from a single lung cancer screening round. Thorax 75(10), 908–912 (2020).
70.
Yousaf-Khan U, Horeweg N, Van Der Aalst C, Ten Haaf K, Oudkerk M, De Koning H. Baseline characteristics and mortality outcomes of control group participants and eligible non-responders in the NELSON Lung Cancer Screening Study. J. Thorac. Oncol. 10(5), 747–753 (2015).
71.
Paulauskiene J, Stelemekas M, Ivanauskiene R, Petkeviciene J. The cost-effectiveness analysis of cervical cancer screening using a systematic invitation system in Lithuania. Int. J. Environ. Res. Public Health 16(24), 5035 (2019).
• In Lithuania, a systematic invitation approach is more effective in increasing the participation rate for screening compared to an opportunistic invitation approach.
72.
OECD. EU Country Cancer Profile: Lithuania 2023, EU Country Cancer Profiles. OECD Publishing, France (2023).
73.
Basu P, Ponti A, Anttila A et al. Status of implementation and organization of cancer screening in The European Union Member States—Summary results from the second European screening report. Int. J. Cancer 142(1), 44–56 (2018).
74.
Djuric O, Venturelli F, Bassi MC et al. Recruitment strategies and outcomes in lung cancer screening programmes: a scoping review. Eur. Radiol. doi: (2026) (Epub ahead of print).
75.
Burzić A, O'dowd EL, Baldwin DR. How to translate quality standards into good lung cancer screening programmes: the UK experience. Br. J. Hosp. Med. (Lond.) 87(4), 53142 (2026).
76.
Gaudio C, Tanzilli A, Mei M et al. Concomitant screening of coronary artery disease and lung cancer with a new ultrafast-low-dose computed tomography protocol: a pilot randomised trial. Sci. Rep. 9(1), 13872 (2019).
77.
Yip R, Jirapatnakul A, Hu M et al. Added benefits of early detection of other diseases on low-dose CT screening. Transl. Lung Cancer Res. 10(2), 1141–1153 (2021).
78.
Behr CM, Koffijberg H, Degeling K, Vliegenthart R, IJzerman MJ. Can we increase efficiency of CT lung cancer screening by combining with CVD and COPD screening? Results of an early economic evaluation. Eur. Radiol. 32(5), 3067–3075 (2022).
79.
Debieuvre D, Molinier O, Falchero L et al. Lung cancer trends and tumor characteristic changes over 20 years (2000–2020): results of three French consecutive nationwide prospective cohorts' studies. Lancet Reg. Health Eur. 22, 100492 (2022).
80.
Kerpel-Fronius A, Tammemägi M, Cavic M et al. Screening for lung cancer in individuals who never smoked: an International Association for the Study of Lung Cancer Early Detection and Screening Committee Report. J. Thorac. Oncol. 17(1), 56–66 (2022).
81.
Nemesure B, Plank A, Reagan L, Albano D, Reiter M, Bilfinger TV. Evaluating efficacy of current lung cancer screening guidelines. J. Med. Screen. 24(4), 208–213 (2017).
82.
Wu GX, Goldstein L, Kim JY, Raz DJ. Proportion of non-small-cell lung cancer patients that would have been eligible for lung cancer screening. Clin. Lung Cancer 17(5), e131–e139 (2016).
83.
Osarogiagbon RU, Liao W, Faris NR et al. Evaluation of lung cancer risk among persons undergoing screening or guideline-concordant monitoring of lung nodules in the Mississippi Delta. JAMA Netw. Open 6(2), e230787 (2023).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 February 2026
Accepted: 22 June 2026
Published online: 16 July 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Lung cancer screening in Lithuania: a cost-effectiveness analysis. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2026-0034
Export citation
Select the citation format you wish to export for this article or chapter.