Covariate selection and adjustment for efficacy and safety endpoints in indirect comparative effectiveness analyses of CAR-T-cell therapies for large B-cell lymphoma: a systematic review
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Several CAR-T cell therapies have received regulatory approval from both the US FDA and the EMA for the treatment of large B-cell lymphoma. However, direct comparative trials between CAR-T cell therapies are lacking, mainly due to different clinical development timelines and availabilities as well as substantial resource requirements and difficulties in recruiting sufficiently large and homogeneous cohorts from a highly pre-treated patient population. Consequently, indirect treatment comparisons (ITCs) play a critical role in evaluating the relative benefits of CAR-T cell therapies. However, ITCs are inherently susceptible to confounding, underscoring the importance of systematically identifying and appropriately adjusting for key prognostic factors, and treatment effect modifiers. Materials & methods: A systematic literature search was conducted in PubMed/MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) in November 2025. Database-specific search strategies using controlled vocabulary (MeSH and Emtree) were applied. Records were deduplicated prior to screening. Studies published in English or German were eligible. Two reviewers independently screened titles/abstracts and full texts using predefined criteria, with disagreements resolved by consensus. Results: A total of 27 publications met the inclusion criteria. Most studies used unanchored matching-adjusted indirect comparisons, followed by propensity score-based methods and network meta-analyses. The extent of covariate adjustment varied widely, ranging from no adjustment to extensive multivariable adjustment with up to 19 covariates. Commonly adjusted factors included demographics, disease severity, clinical status and treatment history. Efficacy outcomes most frequently assessed overall and progression-free survival and response rates, whereas safety outcomes were reported less consistently and were rarely covariate-adjusted, limiting comparative interpretation. Covariates were selected based on clinical expertise and/or literature review; however, no study provided a detailed description of the identification methodology. Conclusion: Although the selection of variables for adjustment frequently targeted recognized prognostic factors, the underlying processes lacked methodological transparency and were often constrained by data availability or undocumented expert opinion. Consequently, this resulted in substantial heterogeneity across studies. Notably, even fundamental covariates routinely required in health technology assessments, such as age, sex and disease severity, were inconsistently addressed, further limiting the comparability and robustness of the reported ITCs. To enhance the reliability and comparability of ITC results, standardized approaches for covariate identification and adjustment are urgently needed.
Plain language summary
The introduction of chimeric antigen receptor T-cell (CAR-T) therapies has transformed the treatment landscape for relapsed or refractory large B-cell lymphoma. However, direct head-to-head comparisons of CAR-T cell therapies in large B-cell lymphoma are lacking, primarily due to the limited pool of eligible patients and the logistical complexities of conducting multi-arm trials in a highly specialized treatment setting. As a result, indirect treatment comparisons have been applied which combine clinical outcomes from separate studies. These comparisons can be biased if differences between patients in the different comparator arms, such as age, disease severity or prior treatments, are not properly addressed. This review examined published studies comparing CAR-T cell therapies indirectly. A total of 27 studies met the inclusion criteria, utilizing a range of statistical methods and adjusting for different patient and disease characteristics. While many clinically relevant factors were considered, the selection and adjustment of these factors varied widely and were often poorly described. Standardized and transparent approaches are needed to improve the reliability of indirect comparisons.
Chimeric antigen receptor T-cell (CAR-T) therapy is an advanced form of adoptive cell therapy in which a patient’s T cells are collected via apheresis, genetically modified ex vivo to express a tumor-specific receptor, and reinfused to eliminate malignant cells [1,2]. The first CAR-T products approved for clinical use, Axicabtagene ciloleucel (Yescarta®) and Tisagenlecleucel (Kymriah®), received US FDA authorization in 2017 and 2018, respectively, and EMA authorization in 2018, for the treatment of relapsed or refractory diffuse large B-cell lymphoma (DLBCL) following two or more prior lines of therapy. DLBCL, the most common subtype of non-Hodgkin lymphoma (NHL), accounts for approximately a third of all NHL cases worldwide and constitutes the largest entity within the group of LBCL [3].
Regulatory approvals have since broadened the CAR-T landscape. The FDA (2021) and EMA (2022) approved Lisocabtagene maraleucel (Breyanzi®) for the same indication. Both agencies later expanded the label of axicabtagene ciloleucel in 2022 to second-line treatment for patients with early relapse within 12 months of frontline rituximab-based chemoimmunotherapy. Lisocabtagene maraleucel received corresponding approvals in 2022 (FDA) and 2023 (EMA), supported by trials demonstrating superior outcomes for CAR-T therapy compared with high-dose chemotherapy followed by autologous stem cell transplantation (ASCT) [4,5]. In addition, relmacabtagene autoleucel is approved for the treatment of r/r LBCL in China only [6].
Despite these advances, direct head-to-head randomized controlled trials comparing CAR-T products remain unavailable. The high cost of CAR-T therapy that often exceeds $300,000 per treatment in the US [7,8] with additional inpatient and adverse event management costs approaching $160,000, further limits the feasibility of such trials [9]. Consequently, indirect treatment comparisons (ITCs) have become central to evaluating the comparative effectiveness and cost-effectiveness of CAR-T therapies. However, ITCs are prone to confounding bias, whereby differences in patient or disease characteristics can influence both treatment assignment and outcomes [10].
In unanchored ITCs (based on single-arm trials), adjustment for both prognostic factors and treatment effect modifiers is required, while anchored ITCs (which share a common comparator arm) require adjustment for effect modifiers only [11,12]. Identifying these variables typically involves a structured literature review and expert clinical validation [13], consistent with guidance from major health technology assessment (HTA) agencies [14,15].
Given the substantial clinical and economic burden of DLBCL [16,17], understanding how confounding is addressed in published ITCs is essential to improving the validity and comparability of CAR-T evidence synthesis. The objective of this study is to conduct a systematic literature review of published ITCs of CAR-T therapies in LBCL including DLBCL to identify confounding variables used for adjustment. By summarizing the factors most frequently accounted for, this study aims to support more transparent, methodologically consistent and policy-relevant comparative evaluations of CAR-T therapy.
Materials & methods
This study represents a methodological update and expansion of a previous review [18] which was limited to the PubMed database. The current systematic search was extended to include PubMed (including Medical Literature Analysis and Retrieval System Online [MEDLINE]), Excerpta Medica Database (EMBASE), and the Cochrane Library, specifically the Cochrane Central Register of Controlled Trials (CENTRAL) and adheres to the PRISMA guidelines [19]. The PICO is described in Table 1.
| Parameter | Inclusion criteria | Exclusion criteria | |
|---|---|---|---|
| Population | Adult patients with LBCL and DLBCL | A1 | Wrong population |
| Intervention | CAR T-cell therapies including: tisagenlecleucel (Kymriah), axicabtagene ciloleucel (Yescarta), lisocabtagene maraleucel (Breyanzi) | A2 | Wrong intervention |
| Control group | Any treatment (feasible for an indirect comparison) | A3 | Comparator not suitable for indirect comparison |
| Outcome | ITC methods with focus on methodological evaluation of how studies perform confounder and effect modifier adjustment for clinical efficacy and safety Including but not limited to: Adjusted/unadjusted Indirect treatment comparison NMA MAIC Network meta-regression The Bucher method STC Propensity score matching Detailed information to be extracted: ITC methods Identified variables Endpoints included in ITCs Types of variables included: Differentiation between confounders, prognostic factors and treatment effect modifiers Variable selection methods Techniques for adjustment/weighting | A4 A5 A6 | No indirect treatment comparison No de novo ITC Wrong endpoints |
| Publication-type | Full publications with primary data | A7 | Wrong publication type |
| Language | English, German | A8 | Other languages |
CAR-T: Chimeric antigen receptor T-cell; DLBCL: Diffuse large B-cell lymphoma; ITC: Indirect treatment comparison; LBCL: Large B-cell lymphoma; MAIC: Matching-adjusted indirect comparison; NMA: Network meta-analysis; PICO: Population Intervention Comparison and Outcome; STC: Simulated treatment comparison.
The search strategy was tailored to the specific requirements and controlled vocabularies of each database (e.g., MeSH terms for PubMed and Emtree terms for EMBASE). As a representative example, the full search strategy for PubMed is provided in Table 2; the strategies for all other databases followed this master protocol and were adapted accordingly and are reported in Supplementary Tables 1 & 2. Searches were performed independently for each database, and the retrieved records were exported and managed using reference management software, with duplicates identified and removed prior to screening. Studies published in English or German were considered eligible for inclusion.
| # | Search in PUBMED | Results |
|---|---|---|
| #1 | diffuse large b cell lymphoma[All Fields] OR “diffuse large b-cell lymphoma"[All Fields] OR “diffuse large B?cell lymphoma” [All Fields] OR “large B-cell lymphoma"[All Fields] OR “large B cell lymphoma"[All Fields] OR “large B?cell lymphoma” [All Fields] OR “dlbcl"[All Fields] OR “dlbcls"[All Fields] OR “LBCL"[All Fields] or “diffuse lymphoma” OR (diffuse large b cell lymphoma[MeSH Terms]) OR (lymphoma, large b cell, diffuse[MeSH Terms]) OR (b cell lymphoma[MeSH Terms]) | 69,002 |
| #2 | ((“CAR T”) OR (“CAR-T”)) OR “chimeric antigen receptor T-cell therap*” OR (chimeric antigen receptor therapy[MeSH Terms]) OR (tisagenlecleucel) OR (tisa-cel) OR (tisacel) OR (tisa?cel) OR (Kymriah) OR (axicabtagene * ciloleucel) OR (“axicabtagene ciloleucel”) OR “axi-cel” OR axicel OR axi?cel OR (Yescarta) OR (“lisocabtagene maraleucel”) OR (lisocabtagene maraleucel) OR (liso-cel) OR (lisocel) OR (liso?cel) OR (Breyanzi) | 27,531 |
| #3 | (“indirect comparison*”) OR (“indirect” AND “comparison*”) OR “ITC” OR (“treatment comparison*”) OR (“treatment” AND “comparison*”) OR (“simulated treatment comparison*”) OR “STC” OR (“network meta analys*”) OR (“network-meta-analys*”) OR “NMA” OR (“adjusted comparison*”) OR (“adjusted” AND “comparison*”) OR (“matching adjusted indirect comparison*”) OR “MAIC” OR (“comparing efficacy”) OR (“Bucher*” AND “comparison*”) OR (“Bayesian*” AND “comparison*”) OR (“real world comparison*”) OR (“comparative efficacy”) OR ((“comparative” OR “comparing”) AND “efficacy”) OR (network meta analysis as topic[MeSH Terms]) OR (network meta analysis[MeSH Terms]) OR (Propensity score matching) OR (propensity score[MeSH Terms]) | 599,155 |
| #4 | #1 AND #2 AND #3 | 139 |
| #5 | #4 NOT (animals[mesh] NOT humans[mesh]) | 137 |
| #6 | #5 AND (english[lang] OR german[lang]) | 137 |
Two reviewers independently screened the titles and abstracts of all identified records to assess eligibility according to predefined inclusion and exclusion criteria. Any discrepancies between the reviewers were resolved through discussion until consensus was reached. The same independent, dual-review process was applied during the full-text assessment of potentially relevant articles. The search was conducted in November 2025.
Results
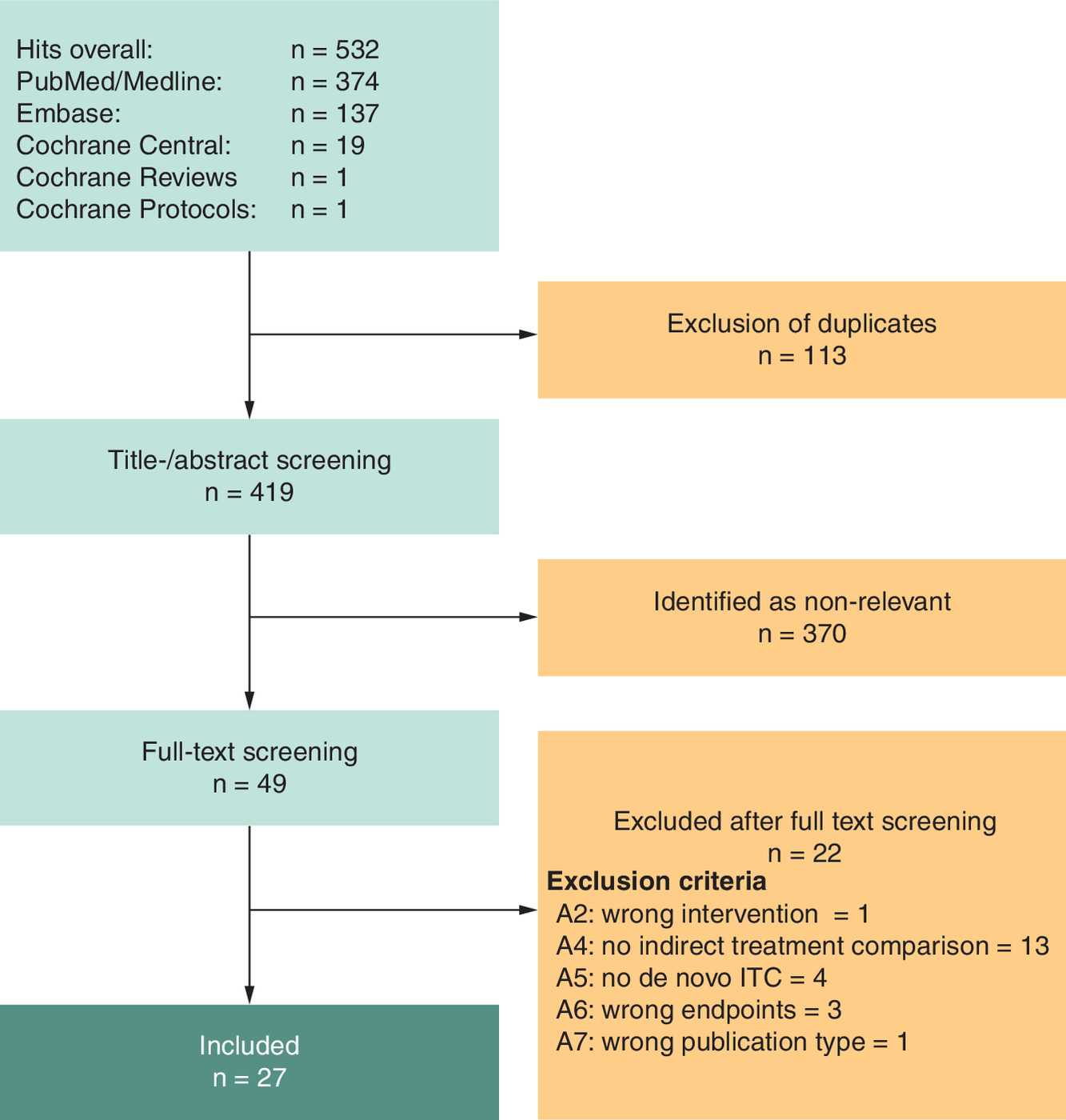
The search identified 27 publications (Figure 1). Excluded papers after full-text review were documented in the Supplementary Table 3.
Identified publications are summarized in Table 3. The table is structured with eight columns, each describing a specific aspect of a study comparison. From left to right, the columns are: Author – identifies the author(s) of the study. Comparison type – indicates the type or design of the comparison being made (e.g., head-to-head and placebo-controlled). Intervention – describes the treatment, exposure or strategy being evaluated. Comparator – specifies the control or alternative intervention against which the intervention is compared. Endpoints (efficacy) – lists the outcomes used to assess the effectiveness of the intervention. Number of variables (efficacy) – reports how many efficacy-related variables or measures were analyzed. Endpoints (safety) – lists the outcomes used to evaluate safety or adverse effects. Number of variables (safety) – reports how many safety-related variables or measures were analyzed.
| Author | Comparison type | Intervention | Comparator | Endpoints efficacy | Variables efficacy, n | Endpoints safety | Variables safety, n | Ref. |
|---|---|---|---|---|---|---|---|---|
| Abramson et al. (2025) | MAIC (anchored) | Lisocabtagene maraleucel | Axicabtagene ciloleucel | Event-free survival Effect modifiers: Absolute lymphocyte count Age Ann Arbor stage Bone marrow involvement Cell of origin Disease histology Eastern Cooperative Oncology Group performance status Region Relapsed or refractory status Secondary age-adjusted International Prognostic Index Sex Sum of the product of perpendicular diameters Overall survival Effect modifiers: Absolute lymphocyte count Age Disease histology Region Relapsed or refractory status Secondary age-adjusted International Prognostic Index Sex Sum of the product of perpendicular diameters | 12 | Cytokine release syndrome (all grades) Prognostic factors: Age Bilirubin levels Left ventricular ejection fraction Secondary age-adjusted International Prognostic Index Neurological events (all grades) Prognostic factors: Age Bilirubin levels Left ventricular ejection fraction Serious adverse events Prognostic factors: Age Left ventricular ejection fraction Secondary age-adjusted International Prognostic Index | 4 | [20] |
| Asghar et al. (2024) | Network meta-analysis (NMA) | Pooled CAR-T | Standard of care (SoC) | Event-free survival Effect modifiers: Age Non-Hodgkin lymphoma subtype Prior response status | 3 | 0 | 0 | [21] |
| Cartron et al. (2022) | MAIC (unanchored) | Lisocabtagene maraleucel | Tisagenlecleucel | Overall response rate Confounders: Disease histology Eastern Cooperative Oncology Group performance status Overall survival Confounders: Bridging therapy Disease histology Eastern Cooperative Oncology Group performance status International Prognostic Index score Prior allogeneic hematopoietic stem cell transplantation Prior autologous hematopoietic stem cell transplantation Refractory status to last therapy Secondary central nervous system lymphoma Progression-free survival Confounders: Disease histology Eastern Cooperative Oncology Group performance status | 8 | Cytokine release syndrome (all grades) Confounders: Eastern Cooperative Oncology Group performance status Prior lines of therapy, n Prior allogeneic hematopoietic stem cell transplantation Secondary central nervous system lymphoma | 4 | [22] |
| Ghosh et al. (2025) | Propensity score weighting/IPTW | Lisocabtagene maraleucel | Conventional second-line chemotherapy | Duration-of-response Confounders: Ann Arbor disease stage Bulky disease Event-free survival Confounders: Ann Arbor disease stage Bulky disease Overal response rate Confounders: Age Ann Arbor disease stage Bulky disease Disease histology Eastern Cooperative Oncology Group performance status Race Sex Overall survival Confounders: Age Ann Arbor disease stage Bulky disease Disease histology Eastern Cooperative Oncology Group performance status Race Sex Progression-free survival Confounders: Age Ann Arbor disease stage Bulky disease Disease histology Eastern Cooperative Oncology Group performance status Race Sex | 7 | 0 | 0 | [23] |
| Gong et al. (2023) | Network meta-analysis (NMA) | Axicabtagene ciloleucel | Standard of care (SoC) | No variable-level adjustments were performed because the analysis was based solely on aggregate data reported in the included studies. | 1 | No variable-level adjustments were performed because the analysis was based solely on aggregate data reported in the included studies. | 0 | [24] |
| Kim et al. (2024) | Network meta-regression (NMR) | Pooled CAR-T | Bispecific antibody | Complete response rate Confounders: Age ≥65 years Double-hit or triple-hit lymphoma Median age Transformed lymphoma | 4 | 0 | 0 | [25] |
| Locke et al. (2025) | MAIC (unanchored) | Axicabtagene ciloleucel | Standard of care (SoC) | Complete response rate Prognostic factors: Age Eastern Cooperative Oncology Group performance status International Prognostic Index Primary refractory status Prior lines of therapy Refractory to stem cell transplant Sex | 7 | 0 | 0 | [26] |
| Overall response rate Prognostic factors: Age Eastern Cooperative Oncology Group performance status International Prognostic Index Primary refractory status Prior lines of therapy Refractory to stem cell transplant Sex Overall survival Prognostic factors: Age Eastern Cooperative Oncology Group performance status International Prognostic Index Primary refractory status Prior lines of therapy Refractory to stem cell transplant Sex | ||||||||
| Lunning et al. (2024) | Propensity score matching | Axicabtagene ciloleucel | Chemoimmuno therapy (CIT) | Complete response rate Confounders: Age Disease histology Disease stage at initial diagnosis Eastern Cooperative Oncology Group performance status Prior autologous stem cell transplantation Refractory to all prior lines of therapy Overall response rate Confounders: Age Disease histology Disease stage at initial diagnosis Eastern Cooperative Oncology Group performance status Prior autologous stem cell transplantation Refractory to all prior lines of therapy Overall survival Confounders: Age Disease histology Disease stage at initial diagnosis Eastern Cooperative Oncology Group performance status Refractory to all prior lines of therapy | 6 | 0 | 0 | [27] |
| Maloney et al. (2021) | MAIC (unanchored) | Lisocabtagene maraleucel | Axicabtagene ciloleucel | Complete response rate Prognostic factors: Bulky disease Eastern Cooperative Oncology Group performance status Extranodal disease Prior autologous HSCT Refractory status to last therapy Secondary CNS involvement Tumor burden Overall response rate Prognostic factors: Absolute lymphocyte count Bridging therapy use | 18 | Cytokine release syndrome (all grades) Prognostic factors: Baseline grade ≥3 anemia Baseline grade ≥3 neutropenia Baseline grade ≥3 thrombocytopenia Bridging therapy use Eastern Cooperative Oncology Group performance status Prior lines of therapy, n Prior allogeneic HSCT Secondary CNS involvement Tumor burden | 9 | [28] |
| Creatinine clearance Disease histology Disease stage Eastern Cooperative Oncology Group performance status Left ventricular ejection fraction Prior lines of therapy, n Prior allogeneic HSCT Prior autologous HSCT Refractory status to last therapy Secondary CNS involvement Sex Tumor burden Overall survival Prognostic factors: Age Bridging therapy use Bulky disease Eastern Cooperative Oncology Group performance status International Prognostic Index score Refractory status to last therapy Secondary CNS involvement Tumor burden Progression-free survival Prognostic factors: Bulky disease Creatinine clearance Eastern Cooperative Oncology Group performance status International Prognostic Index score Refractory status to last therapy Secondary CNS involvement Tumor burden | ||||||||
| Maziarz et al. (2022) | Propensity score weighting/IPTW | Tisagenlecleucel | Historical control treatments | Overall response rate Confounders: Age at initial diagnosis Ann Arbor disease stage Extranodal site involvement Relapses, n Time to 2L start after diagnosis Overall survival Confounders: Age at initial diagnosis Ann Arbor disease stage Extranodal site involvement Relapses, n Time to 2L start after diagnosis | 5 | 0 | 0 | [29] |
| Messori et al. (2022) | Naive unadjusted cross-trial | Axicabtagene ciloleucel | Tisagenlecleucel | No variable-level adjustment was performed because the authors explicitly stated that the Shiny method used for the analysis does not support multivariate modeling, limiting the comparison to a naive unadjusted cross-trial analysis. | 0 | No variable-level adjustment was performed because the authors explicitly stated that the Shiny method used for the analysis does not support multivariate modeling, limiting the comparison to a naive unadjusted cross-trial analysis. | 0 | [30] |
| Nowakowski et al. (2023) | Propensity score matching | Other | Multiple novel and standard therapies | Overall survival Confounders: Age Anemia Ann Arbor stage Eastern Cooperative Oncology Group performance status History of primary refractoriness Neutropenia Prior autologous stem cell transplant Prognostic factors: Elevated lactate dehydrogenase Prior lines of therapy, n Refractoriness to last therapy Progression-free survival Confounders: Anemia Ann Arbor stage Neutropenia Prognostic factors: Age Eastern Cooperative Oncology Group performance status History of primary refractoriness Prior autologous stem cell transplant | 10 | 0 | 0 | [31] |
| Oluwole et al. (2020) | MAIC (unanchored) | Axicabtagene ciloleucel | Tisagenlecleucel | Overall survival Confounders: Bridging chemotherapy Prognostic factors: Cell of origin Disease stage Eastern Cooperative Oncology Group performance status International Prognostic Index Refractory status | 6 | Cytokine release syndrome (all grades) Prognostic factors: Cell of origin Disease stage Eastern Cooperative Oncology Group performance status International Prognostic Index Refractory status | 5 | [32] |
| Oluwole et al. (2022) | MAIC (unanchored) | Axicabtagene ciloleucel | Lisocabtagene maraleucel | Overall survival Progression-free survival Duration of response Overall response rate Complete response rate Partial response rate Patient characteristics: ECOG performance score Best response to last treatment Bridging therapy B-cell lymphoma subtype Prior therapies, n Prior autologous stem cell transplant (auto-SCT) Tumor burden (SPD) Age LDH level | 9 | Cytokine release syndrome (grade 1–2) Cytokine release syndrome (grade ≥3) Neurological events (grade 1–2) Neurological events (grade ≥3) Patient characteristics: ECOG performance score Best response to last treatment Bridging therapy B-cell lymphoma subtype Prior therapies, n Prior autologous stem cell transplant (auto-SCT) Tumor burden (SPD) Age LDH level | 9 | [33] |
| Oluwole et al. (2024) | Network meta-analysis (NMA) | Axicabtagene ciloleucel | Salvage chemotherapy | Overall response rate Confounders: Age Disease stage International Prognostic Index (IPI) NHL subtype Prior lines of therapy, n Prior autologous stem cell transplant Refractory to last line of therapy Relapse within 12 months of ASCT Sex Overall survival Confounders: Age CNS involvement Disease stage Eastern Cooperative Oncology Group performance status International Prognostic Index (IPI) NHL subtype Non-Hodgkin lymphoma subtype Prior lines of therapy, n Relapses, n Post-treatment stem cell transplant Primary refractory disease Prior allogeneic stem cell transplant Prior autologous stem cell transplant Refractory to ≥2 consecutive lines of therapy Refractory to last line of therapy Relapse within 12 months of ASCT Sex Status of disease Time to second line of therapy | 19 | 0 | 0 | [34] |
| Rosenthal et al. (2024) | Propensity score weighting/IPTW | Other | Multiple novel and standard therapies | Complete response rate Confounders: Age Prior lines of therapy, n Previous stem cell transplant Primary refractory status Refractory to last line of therapy Sex Time since discontinuation of last line of therapy Overall response rate Confounders: Age Prior lines of therapy, n Previous stem cell transplant Primary refractory status Refractory to last line of therapy Sex Time since discontinuation of last line of therapy | 7 | 0 | 0 | [35] |
| Overall survival Confounders: Age Prior lines of therapy, n Previous stem cell transplant Primary refractory status Refractory to last line of therapy Sex Time since discontinuation of last line of therapy Progression-free survival Confounders: Age Prior lines of therapy, n Previous stem cell transplant Primary refractory status Refractory to last line of therapy Sex Time since discontinuation of last line of therapy | ||||||||
| Salles et al. (2021) | MAIC (unanchored) | Lisocabtagene maraleucel | Salvage chemotherapy | Complete response rate Prognostic factors: Age Disease histology Disease stage International Prognostic Index score Prior autologous hematopoietic stem cell transplantation Relapsed or refractory status to last therapy Sex Overall response rate Prognostic factors: Age Disease histology Disease stage International Prognostic Index score Prior autologous hematopoietic stem cell transplantation Relapsed or refractory status to last therapy Sex Overall survival Prognostic factors: Age Disease histology Disease stage International Prognostic Index score Prior autologous hematopoietic stem cell transplantation Relapsed or refractory status to last therapy Sex | 7 | 0 | 0 | [36] |
| Salles et al. (2025) | MAIC (unanchored) | Other | Axicabtagene ciloleucel | Complete response rate Prognostic factors: Age ≥65 years Ann Arbor disease stage III-IV Eastern Cooperative Oncology Group performance status Primary refractory disease Refractory to ≥2 consecutive lines of therapy Relapse within 12 months of ASCT Sex Overall response rate Prognostic factors: Age ≥65 years Ann Arbor disease stage III-IV Eastern Cooperative Oncology Group performance status Primary refractory disease Refractory to ≥2 consecutive lines of therapy Relapse within 12 months of ASCT Sex Overall survival Prognostic factors: Age ≥65 years Ann Arbor disease stage III-IV Eastern Cooperative Oncology Group performance status Primary refractory disease Refractory to ≥2 consecutive lines of therapy Relapse within 12 months of ASCT Sex Progression-free survival Prognostic factors: Age ≥65 years Ann Arbor disease stage III-IV Eastern Cooperative Oncology Group performance status Primary refractory disease Refractory to ≥2 consecutive lines of therapy Relapse within 12 months of ASCT Sex | 7 | 0 | 0 | [37] |
| Schuster et al. (2022) | MAIC (unanchored) | Tisagenlecleucel | Lisocabtagene maraleucel | Complete response rate Confounders: Age Eastern Cooperative Oncology Group performance status Histology Lactate dehydrogenase Left ventricular ejection fraction Never achieved complete response with prior therapy Prior lines of therapy, n Prior stem cell transplant Refractory status to prior therapies Sex | 12 | 0 | 0 | [38] |
| Overall response rate Confounders: Age Eastern Cooperative Oncology Group performance status Histology Lactate dehydrogenase Left ventricular ejection fraction Never achieved complete response with prior therapy Prior lines of therapy, n Prior stem cell transplant Received bridging chemotherapy Refractory status to prior therapies Sex Sum of product diameter Overall survival Confounders: Age Eastern Cooperative Oncology Group performance status Histology Lactate dehydrogenase Left ventricular ejection fraction Never achieved complete response with prior therapy Prior lines of therapy, n Prior stem cell transplant Received bridging chemotherapy Refractory status to prior therapies Sex Sum of product diameter Progression-free survival Confounders: Age Eastern Cooperative Oncology Group performance status Histology Lactate dehydrogenase Left ventricular ejection fraction Never achieved complete response with prior therapy Prior lines of therapy, n Prior stem cell transplant Refractory status to prior therapies Sex | ||||||||
| Seo et al. (2025) | MAIC (unanchored) | Other CD19-directed or CD19-containing dual-target construct | Tisagenlecleucel | Complete response rate Prognostic factors: Age Eastern Cooperative Oncology Group performance status Histological subtype International Prognostic Index score Relapse to prior therapy Overall response rate Prognostic factors: Age Eastern Cooperative Oncology Group performance status Histological subtype | 9 | 0 | 0 | [39] |
| International Prognostic Index score Relapse to prior therapy Overall survival Prognostic factors: Age Bridging chemotherapy Cell of origin Disease stage Double or triple hit status Eastern Cooperative Oncology Group performance status Histological subtype International Prognostic Index score Relapse to prior therapy Progression-free survival Prognostic factors: Age Cell of origin Disease stage Double or triple hit status Eastern Cooperative Oncology Group performance status Histological subtype International Prognostic Index score Relapse to prior therapy | ||||||||
| Van Le et al. (2023) | Propensity score weighting/IPTW | Lisocabtagene maraleucel | Conventional therapies | Complete response rate Confounders: Age Bulky disease Disease stage Extranodal disease Prior lines of therapy, n Sex Overall response rate Confounders: Age Bulky disease Chemotherapy refractory status Disease stage Extranodal disease Prior lines of therapy, n Prior lines of therapy per year, n Sex Time from diagnosis to index date Prognostic factors: Best response to prior therapy Prior hematopoietic stem cell transplantation Overall survival Confounders: Age Bulky disease Chemotherapy refractory status Disease stage Extranodal disease Prior lines of therapy, n Prior lines of therapy per year, n Sex Time from diagnosis to index date Prognostic factors: Best response to prior therapy | 11 | 0 | 0 | [40] |
| Prior hematopoietic stem cell transplantation Progression-free survival Confounders: Age Bulky disease Chemotherapy refractory status Disease stage Extranodal disease Prior lines of therapy, n Prior lines of therapy per year, n Sex Time from diagnosis to index date Prognostic factors: Best response to prior therapy Prior hematopoietic stem cell transplantation | ||||||||
| Weinstein et al. (2021) | MAIC (unanchored) | Pooled CAR-T | Axicabtagene ciloleucel | Progression-free survival Prognostic factors: Age Disease stage Extranodal disease status Histology Prior lines of therapy, n Refractory status | 6 | Cytokine release syndrome (Grade ≥3) Prognostic factors: Age Disease stage Extranodal disease status Histology Prior lines of therapy, n Refractory status Neurological events (Grade ≥3) Prognostic factors: Age Disease stage Extranodal disease status Histology Prior lines of therapy, n Refractory status | 6 | [41] |
| Zhang et al. (2020) | MAIC (unanchored) | Tisagenlecleucel | Axicabtagene ciloleucel | Overall survival Confounders: Bridging chemotherapy use Bulky disease Lymphodepleting chemotherapy regimen Sex Prognostic factors: Disease stage Prior autologous stem cell transplant (ASCT) | 6 | 0 | 0 | [42] |
| Jacobson et al. (2024) | Other | Axicabtagene ciloleucel | Tisagenlecleucel | The specific adjustment variables used in the primary meta-analysis were not listed, as the analysis pooled adjusted hazard ratios reported by individual included studies | 0 | The specific adjustment variables used in the primary meta-analysis were not listed, as the analysis pooled adjusted hazard ratios reported by individual included studies | 0 | [43] |
| Kim et al. (2025) | MAIC (unanchored) | Axicabtagene ciloleucel | Conventional therapies | Overall survival Prognostic factors: Age Deauville score Disease stage Eastern Cooperative Oncology Group performance status Histological disease type International Prognostic Index Sex | 7 | 0 | 0 | [44] |
| Progression-free survival Prognostic factors: Age Deauville score Disease stage Eastern Cooperative Oncology Group performance status Histological disease type International Prognostic Index Sex | ||||||||
| Liao et al. (2024) | Other | Axicabtagene ciloleucel | Tisagenlecleucel | No adjustment variables were reported or used in the meta-analysis model itself; the study relies on the crude or reported estimates from the included literature. | 0 | No adjustment variables were reported or used in the meta-analysis model itself; the study relies on the crude or reported estimates from the included literature. | 0 | [45] |
| Neelapu et al. (2021) | Augmented inverse probability weighting | Axicabtagene ciloleucel | Salvage chemotherapy | Overall response rate Confounders: Age Disease stage Disease type International Prognostic Index (IPI) score Prior lines of chemotherapy, n Primary refractory status Refractory to 2 or more consecutive lines of chemotherapy Relapse within 12 months of autologous stem cell transplant Sex Overall survival Confounders: Age Disease stage Disease type International Prognostic Index (IPI) score Prior lines of chemotherapy, n Primary refractory status Refractory to 2 or more consecutive lines of chemotherapy Relapse within 12 months of autologous stem cell transplant Sex | 9 | 0 | 0 | [46] |
AE: Adverse event; ASCT: Autologous stem cell transplantation; CAR-T: Chimeric antigen receptor T-cell; CIT: Chemoimmunotherapy; CNS: Central nervous system; CR: Complete response; CRS: Cytokine release syndrome; DoR: Duration of response; ECOG: Eastern Cooperative Oncology Group; EFS: Event-free survival; HSCT: Hematopoietic stem cell transplantation; IPI: International Prognostic Index; IPTW: Inverse probability of treatment weighting; LDH: Lactate dehydrogenase; MAIC: Matching-adjusted indirect comparison; NHL: Non-Hodgkin lymphoma; NMA: Network meta-analysis; NMR: Network meta-regression; ORR: Overall response rate; OS: Overall survival; PFS: Progression-free survival; PR: Partial response; SoC: Standard of care; SPD: Sum of the product of perpendicular diameter.
In some studies, effect modifiers and prognostic factors were not clearly distinguished; in such cases, variables were classified as confounders for the purpose of this review.
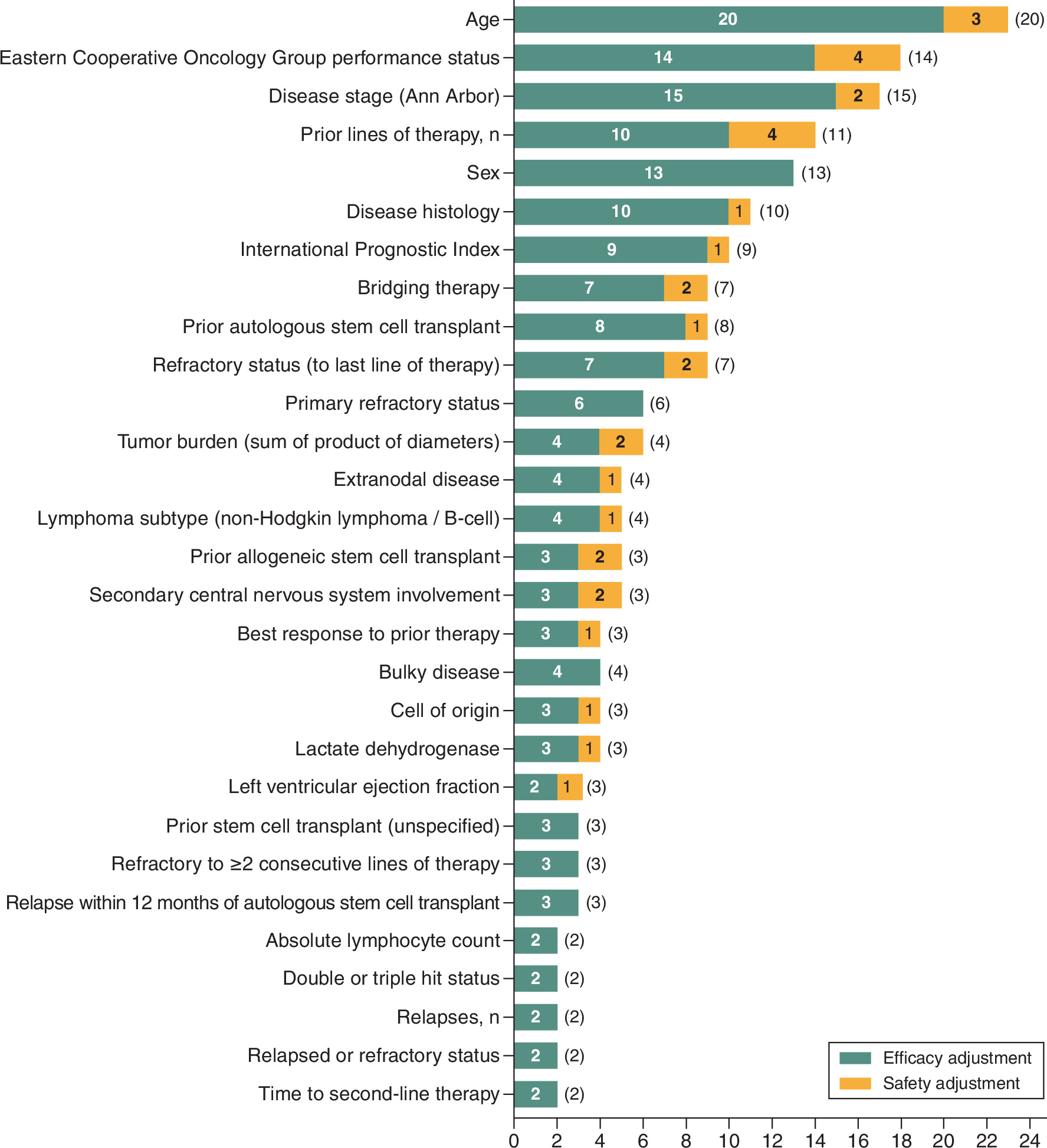
Across the included studies, matching-adjusted indirect comparison (MAIC) approaches were the most frequently applied analytical method, the majority of which were unanchored, with the exception of Abramson et al. [20], which used an anchored design. These were followed by propensity score-based approaches, including matching and inverse probability of treatment weighting as well as network meta-analyses (NMA). The extent of covariate adjustment varied substantially between studies. Some analyses relied exclusively on aggregate data or naive cross-trial comparisons and therefore implemented no variable-level adjustment, whereas others incorporated extensive multivariable adjustment, with the number of covariates ranging from 3 to 19 across multiple endpoints. Despite this variability, there was notable consistency in the types of covariates selected for adjustment. Most studies accounted for patient demographic characteristics, particularly age and sex, alongside disease severity and biological factors, including disease stage, histology, tumor burden, central nervous system involvement and International Prognostic Index (IPI) score. Measures of clinical status, most commonly Eastern Cooperative Oncology Group (ECOG) performance status, were also routinely included, as were elements of treatment history, such as number of prior lines of therapy, prior stem cell transplantation, refractory status and use of bridging therapy (BT). The frequency with which each covariate was used across studies, and the gap between efficacy and safety adjustment, is illustrated in Figure 2. Each bar shows the number of studies that adjusted for the given covariate in efficacy models (dark) and safety models (light). The italic value in parentheses denotes the number of unique studies that adjusted for the covariate in either domain (because some covariates are used in both efficacy and safety in the same study). Only covariates adjusted for in ≥2 unique studies are displayed (n = 29). An additional 26 covariates were each used by a single study only and are therefore omitted. The ‘Age’ row consolidates four age-related operationalizations reported across the 27 studies (age, age ≥65 years, age at initial diagnosis, median age); each study contributes once.
Efficacy analyses most frequently evaluated overall survival (OS), a highly relevant treatment attribute in DLBCL [47], as well as progression-free survival, event-free survival and response-based endpoints, including overall response and complete response rates. In contrast to efficacy, safety outcomes were evaluated less consistently across studies. When reported, analyses primarily focused on cytokine release syndrome and neurological events. Only a minority of studies incorporated covariate-adjusted safety analyses, limiting the ability to draw robust comparative conclusions. Among studies that adjusted for safety outcomes, commonly identified predictors included age, disease burden, ECOG performance status, and aspects of prior treatment history, such as tumor burden. Many network meta-analyses and propensity score-based studies did not incorporate adjustments for safety outcomes, thereby limiting cross-study comparisons of adverse event profiles.
Notably, although most publications reported that prognostic factors and effect modifiers were identified through clinical expertise and a literature review, none provided a detailed description of the identification process, including the search strategy or validation methods.
Discussion
Through our SLR review, we identified 27 ITCs on CAR-T therapies for DLBCL. The number of adjustment variables ranged from 0 to 19 for efficacy variables.
Ten ITCs used IPI or its age-adjusted variant for adjustment of efficacy outcomes such as OS. Although the IPI was already introduced in 1993, it continues to be the most commonly used prognostic model in DLBCL and remains the principal tool for patient selection, risk stratification and therapy decision in contemporary clinical trials [48]. In its initial development, the IPI classified patients into four risk categories using five clinical factors: age, Ann Arbor disease stage, ECOG, serum lactate dehydrogenase levels, and the number of extranodal disease sites [49]. Both IPI and its updated versions (R-IPI, NCCN-IPI) have been validated and are strongly associated with progression-free survival, OS, and, in some cases, neurotoxicity in patients treated with CAR-T therapies [50]. Individual components, including age, ECOG and tumor burden, independently influence outcomes, as confirmed by real-world cohorts and registry data [51]. While sex is included in most ITCs, it appears to have minimal impact on outcomes [52]. Diagnosis was identified as a confounder in most ITCs, encompassing histological classification and NHL subtypes, as well as biologically defined disease characteristics, including the cell of origin, double/triple hit status, and the molecular subtype. BT, used as covariate in seven ITCs, is often administered during CAR-T manufacturing due to high tumor burden or rapidly progressing disease. Response to BT predicts better remission and survival [53]. Bulky disease or high metabolic tumor volume was also recognized as a prognostic factor associated with an unfavorable disease course [54], though definitions varied across studies.
While the confounders identified across the reviewed studies are broadly accepted as clinically meaningful, there was pronounced heterogeneity in both the number and type of variables used for adjustment. This variability reflects the absence of standardized guidance for covariate selection in ITCs within this indication. Notably, several variables that are routinely emphasized in HTAs including age, sex, baseline disease severity, and functional status were not consistently incorporated. Such inconsistencies underscore the discretionary nature of covariates selection in many ITCs and raise concerns regarding the comparability and robustness of some of the published results.
Compounding this issue, most studies failed to provide transparent descriptions of how covariate were identified, prioritized or validated. This lack of methodological transparency limits reproducibility and hinders critical appraisal. The challenge is further amplified by the large number of potential confounders relevant in this therapeutic area, as highlighted by a recent comprehensive literature review that identified a wide range of demographic, clinical, biological and treatment-related factors influencing outcomes in DLBCL [55]. Despite this complexity, some ITCs relied on a comparatively narrow set of adjustment variables. In some cases, this might be driven by limitations in data availability, particularly when individual patient data were inaccessible, or by assumptions that certain prognostic factors were not sufficiently influential to warrant inclusion. However, excluding relevant covariates can lead to residual confounding and biased estimates of relative treatment effects. Prior methodological research has demonstrated that the adequacy of covariate adjustment substantially affects the validity of indirect and unanchored comparisons [56,57].
The implications of adjustment extend beyond comparative effectiveness research and are especially critical in the context of economic evaluation. ITCs frequently serve as key inputs for cost–effectiveness analyses (CEAs), which in turn inform payer and reimbursement decisions. Inadequate or inconsistent adjustment at the ITC stage may propagate bias into CEAs, ultimately affecting estimates of incremental cost–effectiveness ratios and value-for-money conclusions. In line with this concern, a recent meta-analysis of published CEAs in this indication reported marked heterogeneity in cost–effectiveness results, which may partially reflect differences in the quality, transparency, and rigor of the underlying ITCs [58].
Because primary studies did not consistently distinguish between confounders, prognostic factors and effect modifiers, variables of unspecified role were retained under a default label of confounder in our extraction, and role-specific inferences at the variable level should be interpreted with caution.
Taken together, from a clinical perspective, age, ECOG, tumor burden, IPI score, the response on BT and refractory disease status remain key prognostic factors influencing outcomes in CAR-T-treated DLBCL patients. These variables should continue to inform patient selection, risk stratification and therapeutic decision-making in both clinical practice and trial design. The observed heterogeneity in covariate adjustment limits the interpretability of indirect comparisons. These findings highlight a need for the development and adoption of standardized methodological frameworks for covariate identification and selection in ITCs. Such frameworks should promote transparent reporting, systematic identification of confounders, prognostic factors and effect modifiers and alignment with HTA expectations. Strengthening methodological consistency in ITCs would improve the credibility of comparative and economic evidence and support more informed and reliable decision-making in regulatory and reimbursement settings.
Summary points
•
Several CAR-T cell therapies are approved for large B-cell lymphoma, but direct head-to-head trials are lacking due to logistical and clinical challenges.
•
Indirect treatment comparisons are therefore essential for evaluating relative effectiveness, though they are prone to confounding.
•
A systematic literature review was conducted across major databases in November 2025, with dual independent screening and predefined criteria.
•
A total of 27 studies met inclusion criteria, using methods such as unanchored matching-adjusted comparisons, propensity scores and network meta-analyses.
•
The extent of covariate adjustment varied widely, from none to up to 19 variables across studies.
•
Commonly adjusted covariates included demographics, disease severity, clinical status and prior treatments.
•
Efficacy outcomes (e.g., overall and progression-free survival) were frequently reported, while safety outcomes were less consistent and rarely adjusted.
•
Overall, there was substantial heterogeneity and limited methodological transparency in covariate selection, highlighting the need for standardized approaches to improve indirect treatment comparison reliability and comparability.
Financial disclosure
The study was supported by Miltenyi Biomedicine, Germany.
Competing interests disclosure
J Mahlich, S Riou and S Rungaldier were employees of Miltenyi Biomedicine GmbH during conduct of study. J Jost and S Walzer received funding from Miltenyi Biomedicine. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 39.01 KB
References
Papers of special note have been highlighted as: • of interest
1.
Gotti M, Defrancesco I, D'Angelo M et al. Cancer immunotherapy using chimeric antigen receptor expressing T-Cells: present and future needs of clinical cancer centers. Front. Immunol. 11, 565236 (2020).
2.
Boyiadzis MM, Dhodapkar MV, Brentjens RJ et al. Chimeric antigen receptor (CAR) T therapies for the treatment of hematologic malignancies: clinical perspective and significance. J. Immunother. Cancer 6(1), 137 (2018).
3.
Zelenetz AD, Gordon LI, Wierda WG et al. Diffuse large B-Cell lymphoma version 1.2016. J. Natl Compr. Canc. Netw. 14(2), 196–231 (2016).
4.
Shargian L, Raanani P, Yeshurun M et al. Chimeric antigen receptor T-cell therapy is superior to standard of care as second-line therapy for large B-cell lymphoma: a systematic review and meta-analysis. Br. J. Haematol. 198(5), 838–846 (2022).
5.
Locke FL, Miklos DB, Jacobson CA et al. Axicabtagene ciloleucel as second-line therapy for large B-cell lymphoma. N. Engl. J. Med. 386(7), 640–654 (2022).
6.
Ying Z, Yang H, Guo Y et al. Relmacabtagene autoleucel (relma-cel) CD19 CAR-T therapy for adults with heavily pretreated relapsed/refractory large B-cell lymphoma in China. Cancer Med. 10(3), 999–1011 (2021).
7.
Chihara D, Liao L, Tkacz J et al. Real-world experience of CAR T-cell therapy in older patients with relapsed/refractory diffuse large B-cell lymphoma. Blood 142(12), 1047–1055 (2023).
8.
Fiorenza S, Ritchie DS, Ramsey SD et al. Value and affordability of CAR T-cell therapy in the United States. Bone Marrow Transplant. 55(9), 1706–1715 (2020).
9.
Jagannath S, Joseph N, Crivera C et al. Component costs of CAR-T therapy in addition to treatment acquisition costs in patients with multiple myeloma. Oncol. Ther. 11(2), 263–275 (2023).
10.
Steinke D. Essentials of pharmacoepidemiology. In: Clinical Pharmacy Education, Practice and Research. Dixon T (Ed.). Elsevier, Amsterdam,The Netherlands 203–214 (2019).
11.
Phillippo DM, Ades AE, Dias S et al. Methods for population-adjusted indirect comparisons in health technology appraisal. Med. Decis. Making 38(2), 200–211 (2018).
12.
Phillippo DM, Dias S, Elsada A et al. Population adjustment methods for indirect comparisons: a review of National Institute for Health and Care Excellence Technology appraisals. Int. J. Technol. Assess. Health Care 35(3), 221–228 (2019).
13.
Pufulete M, Mahadevan K, Johnson TW et al. Confounders and co-interventions identified in non-randomized studies of interventions. J. Clin. Epidemiol. 148, 115–123 (2022).
• Establishes a standardized reference framework for confounder selection and validation.
14.
IQWIG. General Methods – version 7.0, Cologne. (2023). Available at: https://www.iqwig.de/methoden/general-methods_version-7-0.pdf
• Guidelines for confounder selection from a health technology assessment agency perspective.
15.
Vanier A, Fernandez J, Kelley S et al. Rapid access to innovative medicinal products while ensuring relevant health technology assessment. Position of the French National Authority for Health. BMJ Evid. Based Med. 29(1), 1–5 (2024).
16.
Borchmann P, Heger JM, Mahlich J et al. Healthcare resource utilization and associated costs of German patients with diffuse large B-cell lymphoma: a retrospective health claims data analysis. Oncol. Ther. 11(1), 65–81 (2023).
17.
Borchmann P, Heger JM, Mahlich J et al. Survival outcomes of patients newly diagnosed with diffuse large B-cell lymphoma: real-world evidence from a German claims database. J. Cancer Res. Clin. Oncol. 149(10), 7091–7101 (2023).
18.
Riou S, Rungaldier S, Mahlich J. Identification of adjustment variables in indirect comparisons: a rapid review of CAR-T therapies for diffuse large B-cell lymphoma. Cancers 17(8), 1335 (2025).
19.
Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. PLOS Med. 18(3), e1003583 (2021).
20.
Abramson J, Kamdar M, Liu F et al. Matching-adjusted indirect comparison of lisocabtagene maraleucel versus axicabtagene ciloleucel for second-line treatment of patients with early relapsed or refractory large B-cell lymphoma. Leuk. Lymphoma 66(12), 2200–2213 (2025).
21.
Asghar K, Zafar M, Holland E et al. A systematic review and meta-analysis on utilizing anti-CD19 chimeric antigen receptor T-cell therapy as a second-line treatment for relapsed and refractory diffuse large B-cell lymphoma. Front. Oncol. 14, 1407001 (2024).
22.
Cartron G, Fox C, Liu F et al. Matching-adjusted indirect treatment comparison of chimeric antigen receptor T-cell therapies for third-line or later treatment of relapsed or refractory large B-cell lymphoma: lisocabtagene maraleucel versus tisagenlecleucel. Exp. Hematol. Oncol. 11, 17 (2022).
23.
Ghosh N, Sehgal A, Liu F et al. Comparative efficacy of lisocabtagene maraleucel in the PILOT study versus second-line chemotherapy regimens in the real world. Haematologica 110, 693–705 (2025).
24.
Gong I, Aminilari M, Landego I et al. Comparative effectiveness of salvage chemotherapy regimens and chimeric antigen T-cell receptor therapies in relapsed and refractory diffuse large B cell lymphoma: a network meta-analysis of clinical trials. Leuk. Lymphoma 64, 1643–1654 (2023).
25.
Kim J, Cho J, Lee M et al. CAR T cells vs bispecific antibody as third- or later-line large B-cell lymphoma therapy: a meta-analysis. Blood 144, 629–638 (2024).
26.
Locke F, Ball G, Ray M et al. Efficacy of axicabtagene ciloleucel compared to historical treatments for relapsed/refractory diffuse large B-cell lymphoma of Asian descent: a matching adjusted indirect comparison of ZUMA-1 vs REAL-TREND. Hematol. Oncol. 43, e70100 (2025).
27.
Lunning M, Wang H, Hu Z et al. Benefit of axicabtagene ciloleucel versus chemoimmunotherapy in older patients and/or patients with poor ECOG performance status with relapsed or refractory large B-cell lymphoma after 2 or more lines of prior therapy. Am. J. Hematol. 99, 880–889 (2024).
28.
Maloney D, Kuruvilla J, Liu F et al. Matching-adjusted indirect treatment comparison of liso-cel versus axi-cel in relapsed or refractory large B cell lymphoma. J. Hematol. Oncol. 14, 140 (2021).
29.
Maziarz R, Zhang J, Yang H et al. Indirect comparison of tisagenlecleucel and historical treatments for relapsed/refractory diffuse large B-cell lymphoma. Blood Adv. 6, 2536–2547 (2022).
• Example of expert-driven confounder selection with transparent ranking criteria.
30.
Messori A, Chiumente M, Mengato D. Chimeric antigen receptor T cells in large B-cell lymphoma: analysis of overall survival based on reconstructed patient-level data. Clin. Ther. 44, 1626–1632 (2022).
31.
Nowakowski G, Yoon D, Mondello P et al. RE-MIND2: comparative effectiveness of tafasitamab plus lenalidomide versus polatuzumab vedotin/bendamustine/rituximab (pola-BR), CAR-T therapies, and lenalidomide/rituximab (R2) based on real-world data in patients with relapsed/refractory diffuse large B-cell lymphoma. Ann. Hematol. 102, 1773–1787 (2023).
32.
Oluwole O, Jansen J, Lin V et al. Comparing efficacy, safety, and preinfusion period of axicabtagene ciloleucel versus tisagenlecleucel in relapsed/refractory large B Cell Lymphoma. Biol. Blood Marrow Transplant. 26, 1581–1588 (2020).
33.
Oluwole O, Chen J, Chan K et al. Matching-adjusted indirect comparison of axi-cel and liso-cel in relapsed or refractory large B-cell lymphoma. Leuk. Lymphoma 63, 3052–3062 (2022).
34.
Oluwole O, Neelapu S, Ray M et al. Network meta-analysis of CAR T-Cell therapy for the treatment of 3L+ R/R LBCL after using published comparative studies. Expert Rev. Anticancer Ther. 24, 457–465 (2024).
35.
Rosenthal A, Munoz J, Jun M et al. Comparisons of treatment outcomes of epcoritamab versus chemoimmunotherapy, polatuzumab-based regimens, tafasitamab-based regimens, or chimeric antigen receptor T-cell therapy, in third-line or later relapsed/refractory large B-cell lymphoma. J. Hematol. Oncol. 17(1), 69 (2024).
36.
Salles G, Spin P, Liu F et al. Indirect treatment comparison of liso-cel vs. salvage chemotherapy in diffuse large B-cell lymphoma: TRANSCEND vs. SCHOLAR-1. Adv. Ther. 38, 3266–3280 (2021).
37.
Salles G, Fox C, Hamadani M et al. Indirect comparison of epcoritamab versus axicabtagene ciloleucel in chimeric antigen receptor T-cell-eligible and -naive patients with relapsed/refractory diffuse large B-cell lymphoma. Clin. Lymphoma Myeloma Leuk. 25, e986.e4–e994.e4 (2025).
38.
Schuster S, Zhang J, Yang H et al. Comparative efficacy of tisagenlecleucel and lisocabtagene maraleucel among adults with relapsed/refractory large B-cell lymphomas: an indirect treatment comparison. Leuk. Lymphoma 63, 845–854 (2022).
39.
Seo H, Yoo W, Jung K et al. Comparative effectiveness of anbalcabtagene autoleucel versus tisagenlecleucel in patients with relapsed/refractory diffuse large B-cell lymphoma. Cancer Res. Treat. doi: (2025) (Epub ahead of print).
40.
Van Le H, Van Naarden Braun K, Nowakoski G et al. Use of a real-world synthetic control arm for direct comparison of lisocabtagene maraleucel and conventional therapy in relapsed/refractory large B-cell lymphoma. Leuk. Lymphoma 64, 573–585 (2023).
41.
Weinstein B, Muresan B, Solano S et al. Efficacy and safety of innovative experimental chimeric antigen receptor (CAR) T-cells versus axicabtagene ciloleucel (Yescarta) for the treatment of relapsed/refractory large B-cell lymphoma (LBCL): matching adjusted indirect comparisons (MAICs) and systematic review. Innov Pharm. 12(4), doi (2021) (Epub ahead of print).
42.
Zhang J, Li J, Ma Q et al. A review of two regulatory approved anti-CD19 CAR T-cell therapies in diffuse large B-cell lymphoma: why are indirect treatment comparisons not feasible? Adv. Ther. 37, 3040–3058 (2020).
43.
Jacobsen C, Munoz J, Sun F et al. Real-world outcomes with chimeric antigen receptor T cell therapies in large B cell lymphoma: a systematic review and meta-analysis. Transpl. Cell. Ther. 30, 77.e1–77.e15 (2024).
44.
Kim J, Bea S, Choi Y et al. Effectiveness of axicabtagene ciloleucel versus conventional treatments as first-line therapy for high-risk large B-cell lymphoma: an external comparator study. BMC Cancer 25, 1681 (2025).
45.
Liao C, Zeng L, Lu S et al. Comparison of the efficacy and safety of axi-cel and tisa-cel based on meta-analysis. J. Cancer 15, 5729–5741 (2024).
46.
Neelapu S, Locke F, Bartlett N et al. Comparison of 2-year outcomes with CAR T cells (ZUMA-1) vs salvage chemotherapy in refractory large B-cell lymphoma. Blood Adv. 5, 4149–4155 (2021).
47.
Arai Y, Bolt T, Onishi H et al. Willingness to pay for treatment attributes in diffuse large B-cell lymphoma: a discrete choice study in Japan. Clin. Drug Invest. 46, 619–630 (2026).
48.
Sehn L, Salles G. Diffuse large B-cell lymphoma. N. Engl. J. Med. 384, 842–858 (2021).
49.
Jelicic J, Juul-Jensen K, Bukumiric Z et al. Prognostic indices in diffuse large B-cell lymphoma: a population-based comparison and validation study of multiple models. Blood Cancer J. 13, 157 (2023).
50.
Garcia-Recio M, Wudhikarn K, Pennisi M et al. The International Prognostic Index is associated with outcomes in diffuse large B cell lymphoma after chimeric antigen receptor T cell therapy. Transplant. Cell. Ther. 27(3), 233–240 (2021).
51.
Di Blasi R, Le Gouill S, Bachy E et al. Outcomes of patients with aggressive B-cell lymphoma after failure of anti-CD19 CAR T-cell therapy: a DESCAR-T analysis. Blood 140(24), 2584–2593 (2022).
52.
Vercellino L, Di Blasi R, Kanoun S et al. Predictive factors of early progression after CAR T-cell therapy in relapsed/refractory diffuse large B-cell lymphoma. Blood Adv. 4, 5607–5615 (2020).
53.
Roddie C; Neill L, Osborne W et al. Effective bridging therapy can improve CD19 CAR-T outcomes while maintaining safety in patients with large B-cell lymphoma. Blood Adv. 7, 2872–2883 (2023).
54.
Thieblemont C, Chartier L; Dührsen U et al. A tumor volume and performance status model to predict outcome before treatment in diffuse large B-cell lymphoma. Blood Adv. 6, 5995–6004 (2022).
55.
Schleifenbaum JK, Heger JM, Jost J et al. Systematic literature review to identify prognostic factors of efficacy and safety outcomes of chimeric antigen receptor T-Cell therapies in diffuse large B-Cell lymphoma. J. Cancer Res. Clin. Oncol. 151(7), 203 (2025).
56.
Shi AX, Zivich PN, Chu H. A comprehensive review and tutorial on confounding adjustment methods for estimating treatment effects using observational data. Appl. Sci. 14(9), 3662 (2024).
57.
Fewell Z, Davey Smith G, Sterne JA. The impact of residual and unmeasured confounding in epidemiologic studies: a simulation study. Am. J. Epidemiol. 166(6), 646–655 (2007).
58.
Loftus TJ, Cho JY, Meraz M et al. Cost-effectiveness of chimeric antigen receptor T-cell therapy for relapsed or refractory large B-cell lymphoma: a systematic review and meta-analysis. J. Med. Econ. 28(1), 2216–2235 (2025).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 February 2026
Accepted: 22 May 2026
Published online: 26 June 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Covariate selection and adjustment for efficacy and safety endpoints in indirect comparative effectiveness analyses of CAR-T-cell therapies for large B-cell lymphoma: a systematic review. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2026-0033
Export citation
Select the citation format you wish to export for this article or chapter.