Cost-effectiveness analysis of the use of faricimab in diabetic macular edema in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Diabetic macular edema (DME) is one of the leading causes of vision impairment in diabetic patients. The aim of this study was to evaluate the cost-effectiveness of faricimab (Vabysmo®), the first bispecific antibody targeting VEGF-A and ANG-2, for treating DME in China. Materials & methods: We conducted a cost-effectiveness analysis from the perspective of the Chinese health system using a Markov model to simulate long-term outcomes in DME patients. The model population was based on the Chinese subgroup from the RHINE trial, with a mean starting age of 58.7 years. Faricimab, administered according to a personalized treatment interval regimen following four initial monthly injections, was compared with aflibercept (every 8 weeks) and with ranibizumab and conbercept (both following a pro-re nata dosing regimen). The model incorporated clinical efficacy, adverse events, quality-adjusted life years and direct costs. Extensive sensitivity analyses (one-way and probabilistic) were performed to assess the robustness of the findings. Results: Over 20 years, faricimab gained 0.42, 0.61, 0.80 incremental quality-adjusted life years compared with aflibercept, conbercept, ranibizumab, while reducing treatment costs by 33,315 Chinese Yuan (CNY), 59,061 CNY and 12,314 CNY, respectively. Sensitivity analyses confirmed the robustness of these results, consistently demonstrating faricimab as a dominant and cost-effective treatment option for DME. Conclusion: This first Chinese cost-effectiveness study of faricimab for DME shows it enhances visual outcomes and reduces costs, supporting its adoption and providing evidence for healthcare decision-making on reimbursement and resource allocation.
Plain language summary
What is this article about?
This study explored the cost-effectiveness of faricimab compared with aflibercept, conbercept and ranibizumab for diabetic macular edema (DME). DME is a diabetes-related eye disease that can cause serious vision loss. Faricimab is the first bispecific antibody targeting VEGF-A/ANG-2 for DME, which may improve treatment adherence by reducing injection frequency and visit burden, thereby supporting better long-term visual outcomes. The study analyzed the costs and effectiveness of these treatments over 20 years from the Chinese health system perspective.
What method were used?
A Markov model was developed to estimate how faricimab performs over time compared with three other anti-VEGF medicines currently used in China – aflibercept, conbercept and ranibizumab. The model used clinical data from Chinese subgroup in the RHINE trial and considered the medical costs and quality-adjusted life years over 20 years from the perspective of the Chinese healthcare system.
What were the results?
Faricimab demonstrated improved vision and quality-adjusted life years for patients compared with other drugs while reducing overall treatment costs. These results were consistent even when different assumptions were tested in sensitivity analyses.
What do the results mean?
This study suggests that faricimab is a cost-effective treatment option for people with DME in China. This evidence can support healthcare decision-makers when determining reimbursement policies and selecting optimal treatment choices for DME patients.
Diabetic macular edema (DME), one of the leading causes of visual impairment among individuals with diabetes mellitus (DM), is typically secondary to diabetic retinopathy (DR) arising from the damage to the blood–retinal barrier, which results in the abnormal accumulation of fluid within the macula’s intraretinal layers [1]. According to International Diabetes Federation [2], there are approximately 4.5 billion patients suffered from DM globally in 2017, with a prevalence of 7.6% among DME adults. As a highly populated country, the number of patients with DM in China reached 1.144 billion in 2017, ranking first in the world. A national prevalence study further indicates that prevalence of DR is 16.3% among diabetic patients, with 0.75% patients having DME [3]. Based on another 5-year prospective study in a Shanghai community, DME patients are more likely to suffer from bilateral disease, accounting for 63.7% of all DME patients [4].
Common treatments available for DME are antivascular endothelial growth factor (VEGF) therapy, laser photocoagulation, glucocorticoids and surgical interventions [5]. Although laser photocoagulation was once regarded as the primary treatment for DME in clinical practice, its ability to improve vision is relatively limited and some studies have even revealed that this treatment may lead to potential complications such as subretinal fibrosis [6,7]. There are three major anti-VEGF agents widely used for DME in China: aflibercept, ranibizumab and conbercept.
Faricimab (Vabysmo®) is the first approved VEGF-A/ANG-2 bispecific antibody for the treatment of people with neovascular age-related macular degeneration, DME and retinal vein occlusion. Compared with traditional anti-VEGF therapies, faricimab can improve and maintain vision with dosing intervals ranging from 1 to 4 months in the first year after four initial monthly doses, which therefore enhances drug retention and improves patient compliance to achieve better long-term visual outcomes. Additionally, Faricimab has a favorable safety profile, as evidenced by the absence of serious adverse reactions in the YOSEMITE and RHINE trials [8,9]. Based on the results from the China subgroup of the RHINE trial [10], both faricimab personalized treatment interval (PTI) treatment group and every 8 weeks (Q8W) treatment group have been demonstrated to be noninferior in change from baseline in visual acuity (BCVA) compared with the aflibercept administered every 8 weeks after loading phase.
Apart from demonstrating clinical effectiveness and safety, cost-effectiveness has become an increasingly important part for the evidence base, especially in the decision of drug reimbursement. Faricimab's clinical effectiveness is well discussed in international settings, while there have been no studies analyzing cost-effectiveness of faricimab in China. To address this gap in knowledge, this study aims to conduct a cost-effectiveness analysis (CEA) to enable an evaluation of the long-term economic benefits of intravitreal faricimab compared with ranibizumab, conbercept and aflibercept in the treatment of DME from a Chinese health system perspective.
Materials & methods
The target patient population for the model was based on the Chinese subgroup of the pivotal RHINE randomized trial of faricimab [10]. The starting age simulated in the base-case model is 58.7 years old, which corresponds to the median age in the RHINE randomized trial. Base-case analyses compared faricimab (PTI) with aflibercept (Q8W), ranibizumab pro re nata (PRN) and conbercept (PRN).
The model incorporated data on effectiveness, mortality, adverse events, quality-adjusted life years (QALYs) and costs to perform a cost–utility analysis with a 4-month cycle length. The analysis was conducted through the Chinese healthcare system perspective, with a societal perspective adopted in the scenario analysis to account for the substantial direct nonmedical costs and indirect costs caused by blindness.
Patient population & interventions
The modelled intervention, comparators and their respective regimens are summarized in Table 1. Given that faricimab and aflibercept are head-to-head in a clinical trial and have the most similar indications, aflibercept was firstly included in the control group. Besides aflibercept, both ranibizumab and conbercept are recommended anti-VEGF drugs by national guidelines and have been included in China’s National Reimbursement Drug List (NRDL). Therefore, this study further assessed the economic evaluation of faricimab in comparison with ranibizumab and conbercept. Faricimab is administered according to PTI regimen after an initial loading phase of four doses given every 4 weeks, in line with the pivotal RHINE randomized trial. According to the VIVID-EAST study [11], aflibercept is administered every eight weeks followed by five initial monthly doses from baseline to week 16. Ranibizumab and conbercept are administered based on a PRN dosing regimen after three initial monthly injections until stable visual acuity was achieved, as required in the REFFINE clinical trial [12] and the Sailing clinical trial [13], respectively. These regimens reflect the recommended treatment approaches in China.
| Treatment | Regimen | Administration |
|---|---|---|
| Faricimab | PTI | IVI |
| Aflibercept | Q8 | IVI |
| Ranibizumab | PRN | IVI |
| Conbercept | PRN | IVI |
IVI: Intravitreal injection; PRN: Pro re nata; PTI: Personalized treatment interval.
Model structure
Three-phase treatment stages
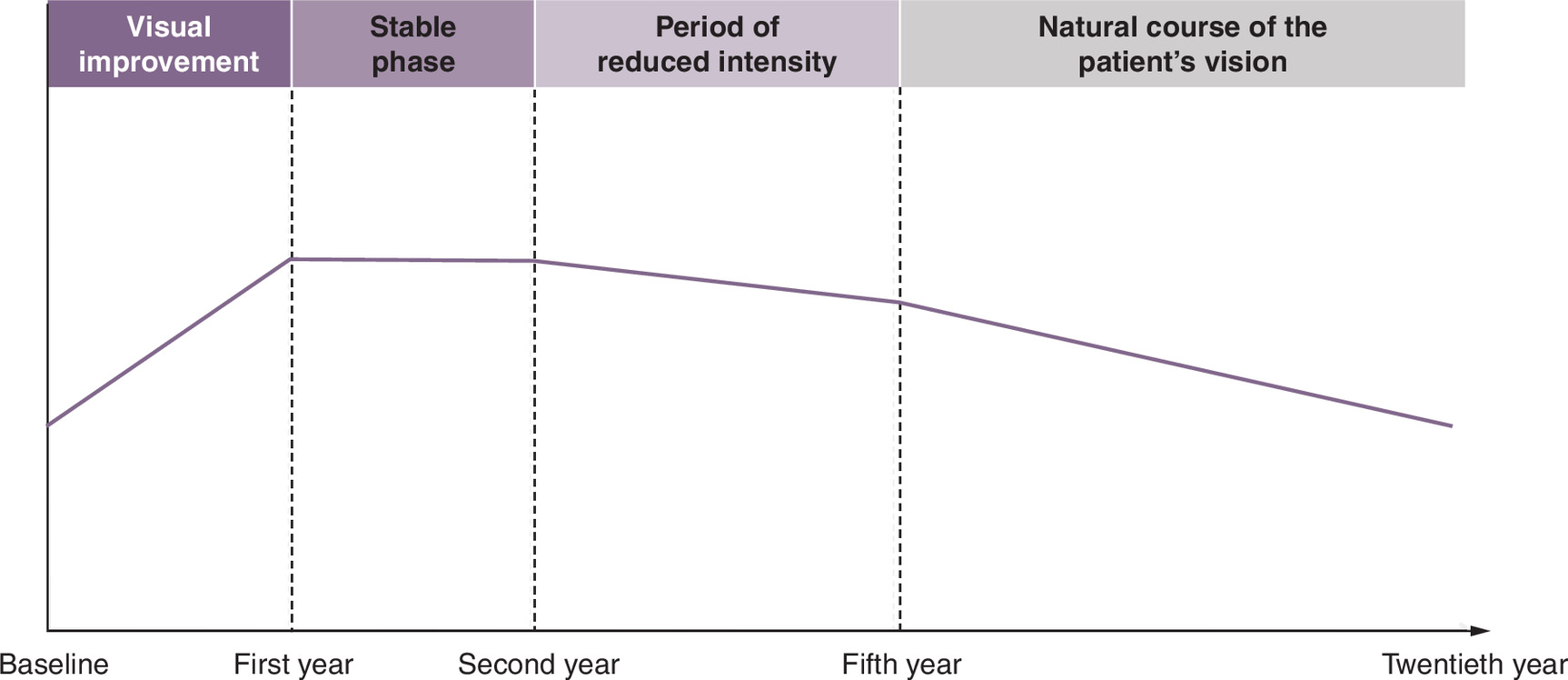
A state-transition Markov model was constructed in Microsoft Excel 2020 to forecast the long-run outcomes of DME patients undergoing intravitreal faricimab, aflibercept, ranibizumab or conbercept. Originally based on a published global model [14] developed for health technology assessment submissions to the National Institute for Health and Care Excellence (NICE), this economic model was subsequently modified in 2024 to align with the Chinese setting. To simulate the disease process and treatment effects, a three-phase approach was adopted according to a five-year real-world study (protocol T study) [15]. This structure was further verified by prior economic evaluations of DME conducted in China and expert consultations to ensure consistency with clinical practice in China (Figure 1). Specifically, the first year is marked by an extended loading phase during which the majority of visual improvements occur; the second year is characterized by stabilized disease progression and maintenance of the visual gains achieved previously. From the third year onward, there is a gradual decline in treatment intensity and long-term maintenance. Additionally, these assumptions were supported by published economic evaluation conducted in China and expert interviews [16]. Consequently, the three-phase model reflects the dynamic nature of disease under treatment.
Model health states
The model is divided into six vision-related health states categorized by best correlated visual acuity (BCVA) scores (>85, 85–71, 70–56, 55–41, 40–26 and ≤25) and one death state, where a lower score implies worse vision (Figure 2). Patients in the cohort could remain stable, remaining in the same health state, or could transition between health states due to improvements or deteriorations in visual acuity. The transitions between health states are further differentiated based on the three-phase treatment stages to reflect the clinical course of the disease. In year 1, patients can move up by two health states (e.g., VA 40–26 to VA 70–56) and down one health state (e.g., VA 70–56 to VA 55–41). In year 2, patients can move up or down one health state, and patients can move down up to two health states from year 3 to year 5. For patients who discontinue treatment or receive treatment beyond 5 years, they were assumed to enter the course of natural disease progression. The transition assumptions were validated in published CEA study.
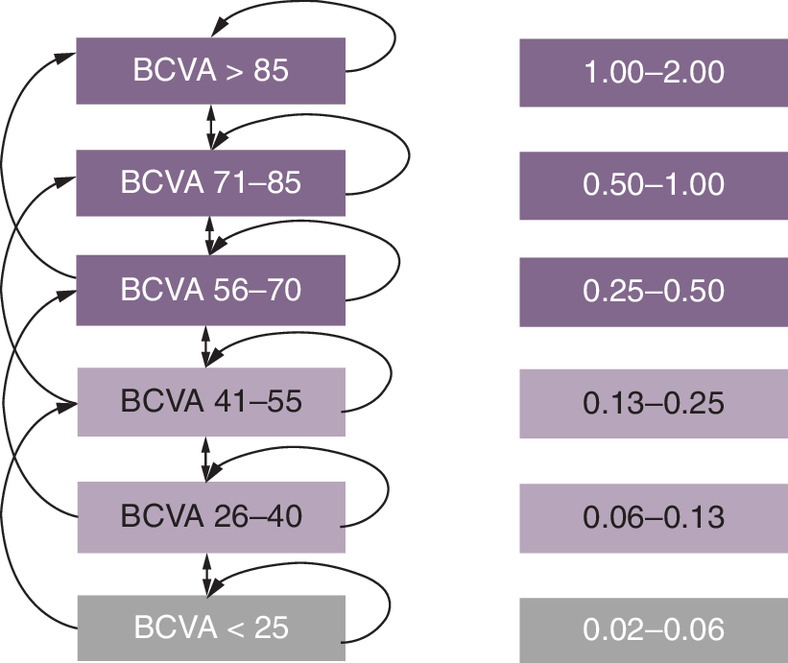
Figure 2. Model structure and transitions between health states.
BCVA: Baseline in visual acuity.
Two-eye model
Due to the bilateral nature of the disease, the quality of life of DME patients is jointly determined by the visual acuity of both eyes, even when only one eye is impaired. Furthermore, the high baseline burden (63.7%) and incidence rate of the second eye (33%) among Chinese patients with DME further demonstrate the necessity of considering both eyes in the model [4]. Consequently, the study adopted a two-eye model recommended by previous systematic reviews and the NICE [14,16–18].
Model inputs & data sources
Baseline characteristics of patients
Baseline characteristics and initial BCVA distribution in the simulated cohort were based on Chinese subgroup of the RHINE trial [10], as shown in Table 2. Additionally, it was assumed that only DME patients whose followed eye is distributed among 70–56, 55–41 and 40–26 vision status groups will receive treatments [17].
| >85 | 85–71 | 70–56 | 55–41 | 40–26 | <= 25 | |
|---|---|---|---|---|---|---|
| Vision distribution of the first eye | 0.00% | 14.47% | 52.63% | 20.39% | 11.84% | 0.66% |
| Vision distribution of the second eye (without DME) | 0.00% | 17.78% | 51.11% | 20.00% | 11.11% | 0.00% |
| Vision distribution of the second eye (with DME) | 0.00% | 13.59% | 54.37% | 19.42% | 11.65% | 0.97% |
| The probability of treatment for the followed eye | 0% | 0% | 100% | 100% | 100% | 0% |
BCVA: Best correlated visual acuity; DME: Diabetic macular edema.
Clinical inputs & transitional probabilities
The transition probabilities varied according to different treatment phases. In the first treatment year, the transition probabilities of faricimab and aflibercept were derived from the Chinese subgroup of the RHINE trial using multistate model package in R. Due to the lack of head-to-head evidence comparing faricimab with conbercept or ranibizumab, we conducted a systematic review and network meta- analysis (NMA) in the Chinese population. A total of four studies [10–13] that satisfied the PICOS criteria were identified, involving faricimab (PTI), aflibercept (Q8W), conbercept (PRN) and ranibizumab (PRN). The details of the NMA are provided in Supplementary Tables 1 & 2.
In treatment year 2, transition probabilities of faricimab and aflibercept were also derived from the Chinese subgroup of the RHINE trial using multistate model, while transitional probabilities in this year were not related to baseline visual acuity scores. The transition probabilities for conbercept and ranibizumab in the second year were assumed to be the same as those of faricimab.
Since there are currently no long-term efficacy data available for anti-VEGF drugs, this study employed the normal cumulative density function to calculate transition probabilities in treatment year 3 and subsequent period, assuming that the decline in BCVA follows normal distribution. This study further assumed that the number of declining BCVA letters from year 3 to year 5 was the same as that observed in year 2 in the Chinese subgroup for faricimab and aflibercept, and that the standard deviation was calculated as the mean change of BCVA divided by 1.96. The transition probabilities of conbercept and ranibizumab were assumed to remain the same as those of faricimab in absence of available data. During the no-intervention phase, there were no differences in transition probabilities for all treatments, and patients were assumed to follow the natural course of the disease.
Background mortality rates of the general Chinese population across different age groups were obtained from the China Population and Employment Statistical Yearbook 2022 [19]. Published studies have shown that low vision and blindness in DME patients are associated with a higher risk of death. Compared with individuals without visual impairment, the mortality risk ratio for DME patients was 2.5, and the mortality risk ratios associated with low vision and blindness were 1.23 (95% CI: 1.16–1.31) and 1.54 (95% CI: 1.26–1.86), respectively [20,21].
Resources use & cost inputs
The direct medical costs included drug acquisition costs, intravitreal injection administration costs, follow-up costs, adverse event costs and supportive care costs. Direct nonmedical costs included transportation costs, food and lodging costs incurred by patients as a result of vision impairment. Indirect costs included productivity loss among patients with poor vision and blindness, as well as among informal caregivers accompanying patients to physicians’ offices or providing care during daily activities.
The unit prices of comparators were derived from the latest winning bid prices on Yaozhi.com, and the unit price of faricimab was based on the National Health Insurance drug price list in 2025. The frequencies of administration in year 1 and year 2 were taken from the Chinese subgroup in the RHINE trial for faricimab and aflibercept, and from the VIVID-EAST study for conbercept, and the number of treatments for ranibizumab was assumed to be the same as that for aflibercept due to the lack of relevant data. In the treatment year from year 3 to year 5, the frequencies of administration were the same for aflibercept, conbercept and ranibizumab (2.2 doses per year) based on the published literature and experts' interviews. Considering that faricimab achieved similar efficacy with fewer administrations compared with aflibercept, the number of faricimab injections was calculated as 1.76 doses per year based on the injection ratio with aflibercept in year 2. The unit costs for intravitreal injection administration costs and follow-up costs were 776 Chinese Yuan (CNY) per injection and 664 CNY per injection, respectively [16,21], and the frequency of follow-up visits for all treatments was assumed to be the same as that of administration proposed by Chinese physicians.
As for adverse events, this study only considered cataract and ocular hypertension (IOP), which have with relatively high treatment costs, and their incidence rates were taken from clinical trials for each anti-VEGF drug. The overall cost of adverse event treatment per patient was derived from the study of Ming et al. [16], which conducted a physician survey in China across 12 cities. In addition, some studies have revealed that blind patients are highly likely to be depressed and falls, thereby incurring corresponding supportive care costs [22–24].
Direct nonmedical costs were differentiated according to BCVA levels; the cost for patients with BCVA below 35 was 51,793 CNY per patient, and 32,445 CNY for those with BCVA above 35 [21,25]. Annual societal costs were computed based on work-loss days and the average daily wage of 244 CNY. The days off for patients and caregivers were derived from published literature, and model inputs for low-vision patients, blind patients, caregivers of low-vision patients and caregivers of blind patients were 124, 350, 57 and 151 days, respectively [16]. Resources use and the corresponding unit cost inputs are presented in Supplementary Tables 3–6.
Utility inputs
The base-case analysis adopted a two-eye utility approach inferred from a previous study [26], since the quality of life of DME patients is related to both eyes. This accepted approach was recommended by NICE and is regarded as more representative of DME patients [17,27]. Specifically, health utility was primarily determined by the visual acuity of the better-seeing eye, with an additional utility decrement applied according to the visual acuity level of the worse-seeing eye. Besides the Czoski-Murray et al.’s study, Brown et al.’s study and Hodgson et al.’s study are also commonly applied in economic evaluation in ophthalmic disease field [28,29]; thus both sources of health utility were further considered in scenario analyses. The health state utilities used in the model analysis are presented in Supplementary Table 5. In addition to health state utilities, disutilities were incorporated for injection events.
Analysis
The main analytic framework was a cost–utility analysis conducted over a 20-year time horizon to comprehensively estimate the relevant costs and health outcomes of faricimab and other anti-VEGF drugs. The primary effectiveness outcome was QALYs, and the incremental cost-effectiveness ratio (ICER) was calculated by dividing the additional costs by additional QALYs between the target intervention and comparators. In the model, an annual discount rate of 5% was applied according to Chinese guideline [30]. The willingness-to-pay (WTP) for China was three-times the gross domestic product per capita in 2023 (89,358 CNY); thus, the threshold was set at 268,074 CNY/QALY.
Sensitivity analyses were performed to evaluate the impact on the ICER caused by uncertainties in model parameters and thus assess the robustness of the model results. The one-way sensitivity analysis considered model inputs such as time horizon, initial age of the cohort and drug prices to identify the most sensitive parameters. All model parameters, except for the price of faricimab (with the lower bound set at 80% of the current price) were varied within the 95% confidence interval or the maximum and minimum values. For parameters whose upper and lower limits cannot be obtained, it was assumed that they fluctuated 20% above and below the baseline value. The probabilistic sensitivity analysis was conducted through 1000-times Monte Carlo simulations to evaluate the impact on the base-case results when multiple model parameters varied simultaneously. The results were visualized using cost-effectiveness acceptability curves to estimate the probability of the target intervention being cost-effective under a range of WTP. Furthermore, scenario analyses were performed based on different perspectives, model structures and sources of parameters. Details are provided in Supplementary Table 8.
Results
Base-case results
We performed an aggregate analysis of the VA distribution among patients who received four different intervention regimens (faricimab, aflibercept, conbercept or ranibizumab) over a 2-year period and compared these distributions to baseline, and the results are presented in the Supplementary Table 9 & Supplementary Figure 1. The results indicated that, for both the first and second years, the faricimab treatment group demonstrated superior visual acuity improvement in the first eye, particularly among patients with VA >85 (9.08%, 8.56%) and VA 85–71 (42.05%, 39.93%), with proportions significantly higher than at baseline. Additionally, the proportions of patients with VA 40–26 (1.98%, 2.52%) and VA ≤25 (0.28%, 0.51%) decreased markedly compared with baseline, suggesting that this treatment regimen effectively enhances visual acuity and delays its decline. Similar trends were observed in the second eye, further corroborating the positive impact of faricimab on visual acuity improvement and delay in visual acuity decline.
In a 20-year lifetime horizon analysis within the Chinese health system, the base-case analysis results (as shown in Table 3) indicate that faricimab yields incremental QALY gains of 0.42, 0.61 and 0.80 compared with aflibercept, conbercept and ranibizumab, respectively. Additionally, the incremental costs associated with faricimab are -33,315 CNY, -59,061 CNY and -12,314 CNY, respectively. These findings demonstrate that faricimab not only provides greater QALY benefits but also significantly reduces treatment costs, positioning it as a dominant treatment option.
| Variables | Faricimab | Aflibercept | Conbercept | Ranibizumab |
|---|---|---|---|---|
| Costs, CNY | 144,313 | 177,629 | 203,374 | 156,628 |
| Incremental cost | / | -33,315 | -59,061 | -12,314 |
| Drug acquisition | 99,514 | 127,286 | 138,782 | 109,195 |
| Admin | 39,690 | 44,727 | 57,839 | 42,774 |
| AE | 1432 | 1216 | 1291 | 513 |
| Visual impairment | 111.25 | 379 | 251.45 | 317.61 |
| Utilities, QALYs | 6.96 | 6.54 | 6.35 | 6.16 |
| Incremental QALYs | / | 0.42 | 0.61 | 0.80 |
| With first eye VA >85 | 0.43 | 0.27 | 0.11 | 0.04 |
| With first eye VA 85–71 | 2.12 | 1.55 | 1.06 | 0.77 |
| With first eye VA 70–56 | 2.19 | 2.05 | 2.28 | 2.25 |
| With first eye VA 55–41 | 1.31 | 1.35 | 1.52 | 1.53 |
| With first eye VA 40–26 | 0.56 | 0.71 | 0.83 | 0.93 |
| With first eye VA ≤25 | 0.36 | 0.62 | 0.55 | 0.62 |
| Incremental cost per QALY, CNY/QALY | / | Faricimab is dominant | Faricimab is dominant | Faricimab is dominant |
| Life-years, year | 10.77 | 10.72 | 10.7 | 10.68 |
| With no VI (no eye below 55 letters) | 5.02 | 3.9 | 3.28 | 2.81 |
| Not in blindness | 10.69 | 10.45 | 10.52 | 10.45 |
AE: Adverse event; CNY: Chinese Yuan; QALY: Quality-adjusted life-year; VA: Visual acuity.
We further detailed the composition of each cost, the QALYs under different VA health states, and the life-years as outcome indicators. In the case of VA >71, faricimab demonstrated 2.54 QALYs, significantly higher than other treatment options: aflibercept (1.82 QALYs), conbercept (1.17 QALYs) and ranibizumab (0.82 QALYs).
Sensitivity & scenario analysis
The results of the one-way sensitivity analyses were summarized in the tornado diagrams shown in Figure 3, highlighting the top ten most sensitive parameters. The results were most sensitive to the discount rate, drug costs, the starting age of the cohort, and the study time horizon. However, within the range of variation, no parameter was able to drive the ICER above 0. The results of the Monte Carlo simulation, comprising 1000 iterations, indicated that faricimab was likely to demonstrate superior efficacy and lower costs compared with aflibercept, conbercept and ranibizumab. Notably, nearly 100% of iterations fell within the southeast quadrant of the cost-effectiveness plane (Figure 4). The cost-effectiveness acceptability curve demonstrated that faricimab exhibited substantial economic advantages (nearly 100%) compared with aflibercept, conbercept and ranibizumab under the pre-specified WTP threshold (Figure 5).
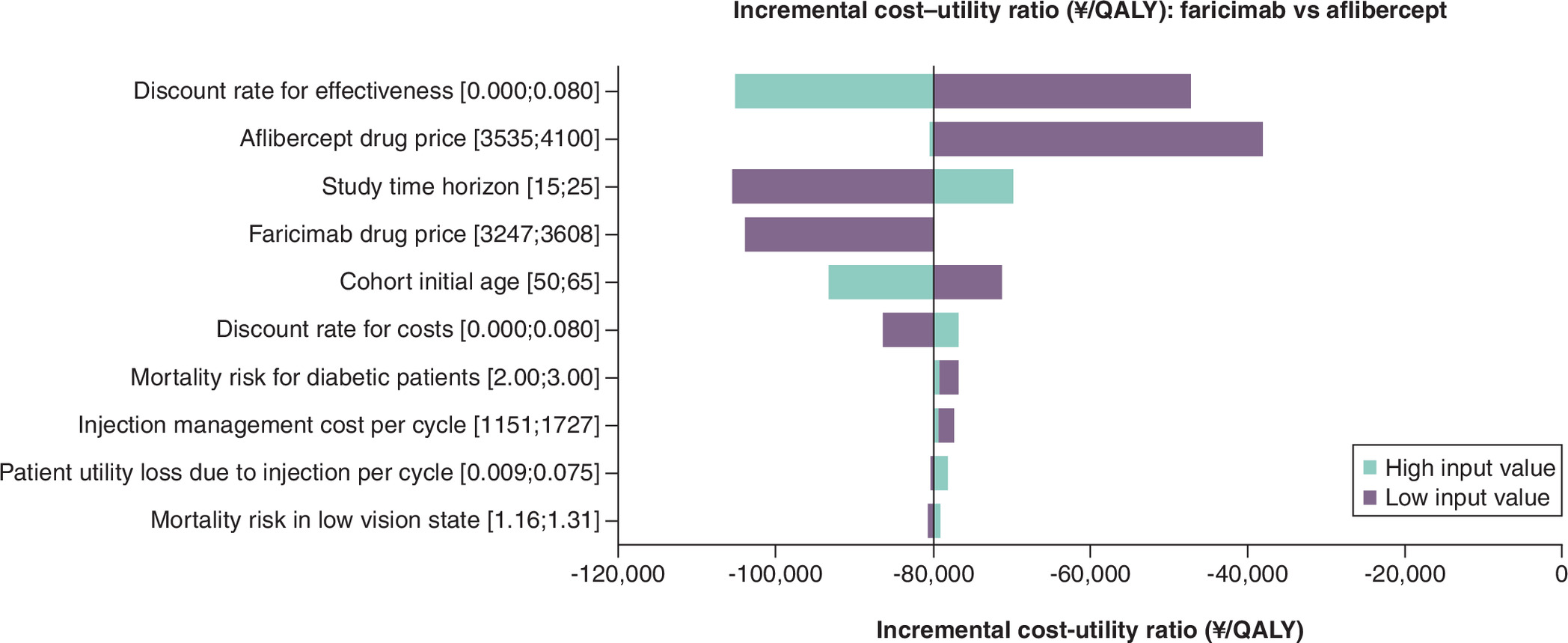
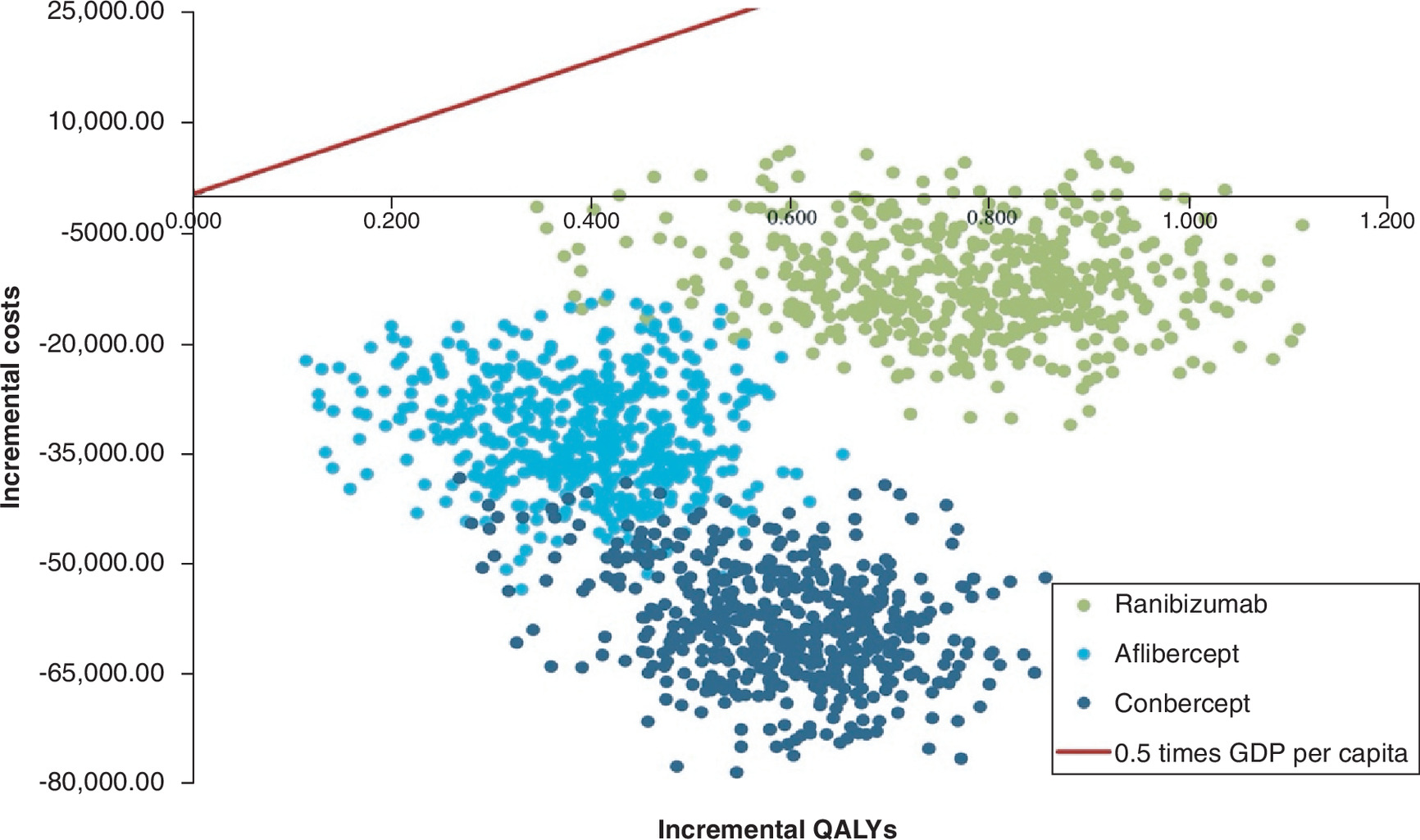
Figure 4. Scatterplots of 1000 iteration of incremental healthcare costs and incremental quality-adjusted life-years.
GDP: Gross domestic product; QALY: Quality-adjusted life year.
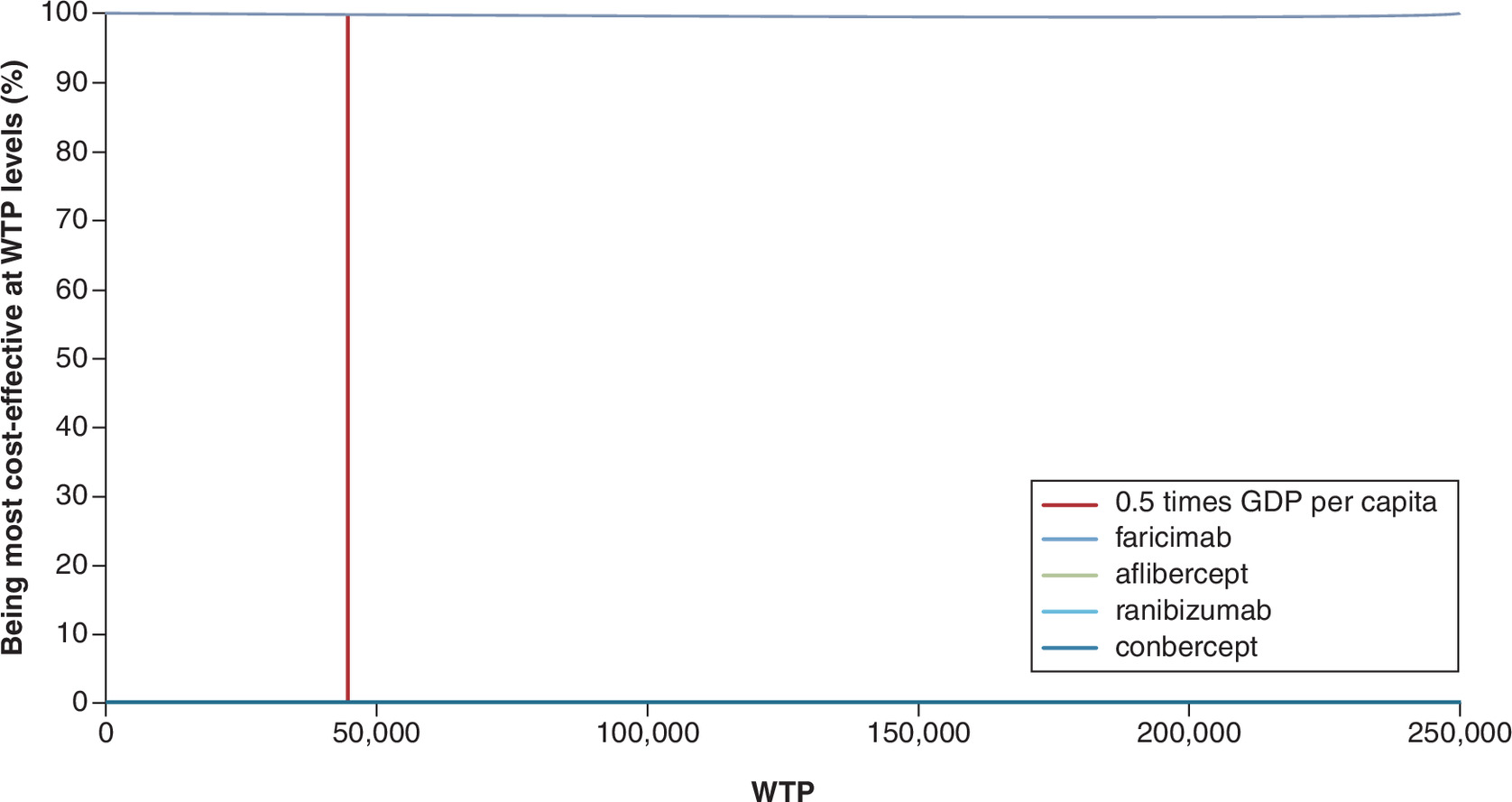
Figure 5. Cost-effectiveness acceptability curve under the health system perspective.
GDP: Gross domestic product; WTP: Willingness to pay.
A scenario analysis was conducted from multiple perspectives, including a societal perspective, a single-eye model, two different sources of utility values and an alternative injection frequency scenario (as shown in Tables 4–8). Regardless of the scenario considered, faricimab consistently demonstrated a dominant advantage over aflibercept, conbercept and ranibizumab. These findings robustly confirm the stability of the base-case results.
| Intervention | QALYs | Total costs | Incremental value | ICER | |
|---|---|---|---|---|---|
| CNY | QALYs | Total costs (CNY) | CNY/QALY | ||
| Faricimab | 6.96 | 203,637 | |||
| Aflibercept | 6.54 | 259,021 | 0.42 | -55,383 | Dominant |
| Conbercept | 6.35 | 297,583 | 0.61 | -93,945 | Dominant |
| Ranibizumab | 6.16 | 261,177 | 0.80 | -57,540 | Dominant |
CNY: Chinese Yuan; ICER: Incremental cost-effectiveness ratio; QALY: Quality-adjusted life-year.
| Intervention | QALYs | Total costs (CNY) | Incremental values | ICER | |
|---|---|---|---|---|---|
| QALYs | Total costs (CNY) | CNY/QALY | |||
| Faricimab | 6.96 | 76,189 | |||
| Aflibercept | 6.76 | 93,688 | 0.21 | -17,499 | Dominant |
| Conbercept | 6.64 | 107,211 | 0.32 | -31,021 | Dominant |
| Ranibizumab | 6.55 | 82,886 | 0.41 | -6696 | Dominant |
CNY: Chinese Yuan; ICER: Incremental cost-effectiveness ratio; QALY: Quality-adjusted life-year.
| Intervention | QALYs | Total costs (CNY) | Incremental values | ICER | |
|---|---|---|---|---|---|
| QALYs | Total costs (CNY) | CNY/QALY | |||
| Faricimab | 7.23 | 144,313 | |||
| Aflibercept | 6.82 | 177,629 | 0.41 | -33,315 | Dominant |
| Conbercept | 6.66 | 203,374 | 0.58 | -59,061 | Dominant |
| Ranibizumab | 6.48 | 156,628 | 0.75 | -12,314 | Dominant |
CNY: Chinese Yuan; ICER: Incremental cost-effectiveness ratio; QALY: Quality-adjusted life-year.
| Intervention | QALYs | Total costs | Incremental values | ICER | |
|---|---|---|---|---|---|
| CNY | QALYs | Total costs (CNY) | CNY/QALY | ||
| Faricimab | 7.31 | 144,313 | |||
| Aflibercept | 6.89 | 177,629 | 0.42 | -33,315 | Dominant |
| Conbercept | 6.58 | 203,374 | 0.73 | -59,061 | Dominant |
| Ranibizumab | 6.35 | 156,628 | 0.97 | -12,314 | Dominant |
CNY: Chinese Yuan; ICER: Incremental cost-effectiveness ratio; QALY: Quality-adjusted life-year.
| Intervention | QALYs | Total costs (CNY) | Incremental values | ICER | |
|---|---|---|---|---|---|
| QALYs | Total costs (CNY) | CNY/QALY | |||
| Faricimab | 6.96 | 129,419 | |||
| Aflibercept | 6.55 | 154,580 | 0.42 | -25,161 | Dominant |
| Conbercept | 6.35 | 180,627 | 0.61 | -51,207 | Dominant |
| Ranibizumab | 6.16 | 132,902 | 0.80 | -3482 | Dominant |
CNY: Chinese Yuan; ICER: Incremental cost-effectiveness ratio; QALY: Quality-adjusted life-year.
Discussion
To the best of our knowledge, this study represents the first effort to evaluate the health impacts and cost-effectiveness of faricimab for DME in China. In terms of cost-effectiveness, faricimab offers a more favorable option for clinicians treating patients with DME. As indicated by previous research [14], faricimab can effectively improve visual acuity while reducing costs. This dual benefit is expected to enhance adherence and quality of life. For instance, better vision enables patients to perform daily tasks more independently, which has been shown to positively impact their overall well-being [31]. The results of this study are valuable for healthcare policymakers and insurance agencies in making more rational decisions regarding drug reimbursement and resource allocation.
The results demonstrate that faricimab shows remarkable efficacy in improving VA in both eyes. In the first and second years, the proportion of patients with VA >85 and 85–71 was higher compared with baseline, while the proportion of patients with VA between 40–26 and VA ≤25 notably decreased. As a bispecific antibody, faricimab simultaneously targets VEGF and Ang-2, and has shown promising effects in stabilizing vascular leakage and improving vision in preclinical and early clinical trials [32]. A 20-year lifetime analysis demonstrates that faricimab, when compared with aflibercept, conbercept and ranibizumab, not only provides superior QALY gains but also reduces treatment costs. In multiple scenario analyses, faricimab consistently emerged as the most cost-effective treatment option.
The one-way sensitivity analysis showed that even when varying parameters such as discount rate, drug costs, starting age and time horizon, faricimab consistently maintained a stable advantage with an ICER remaining below 0. Monte Carlo simulations and cost-effectiveness acceptability curves further confirm that these results are robust over a range of assumptions. Additionally, multiple scenario analyses, whether considering societal costs, using a single-eye model, or adjusting utility values, consistently supported faricimab’s superior long-term cost-effectiveness.
Given the absence of head-to-head trials and the lack of NMAs that simultaneously include faricimab, conbercept and ranibizumab, we included four studies and conducted the NMA based on the Chinese population [10–13]. Utilizing the R netmeta package, this study performed an NMA on key efficacy outcomes, including changes in BCVA, central retinal thickness, the proportion of patients gaining 15 or more letters, and the National Eye Institute 25-item Visual Function Questionnaire (NEI VFQ-25) score. The NMA results demonstrated that faricimab is noninferior to aflibercept (Q8W) and superior to both conbercept and ranibizumab in terms of BCVA improvement among the Chinese population. This analysis provides the most up-to-date indirect comparison of these anti-VEGF agents, highlighting faricimab’s favorable efficacy profile in the Chinese population.
Compared with previously published studies, the cost-effectiveness study of faricimab for DME in China demonstrates several methodological strengths and updates. First, it employed a comprehensive Markov model that integrates a multiphase approach and a two-eye model, capturing the full impact of treatment on patients’ quality of life and aligning with clinical reality. This model structure is similar to the UK study [14] but is tailored to the Chinese healthcare system. Additionally, the study utilized the most recent clinical trial data specific to the Chinese population. Furthermore, this study conducted extensive sensitivity and scenario analyses where model structure was adjusted and utilities were based on an alternative source, providing a thorough assessment of result robustness. All the assumptions in this study were well validated using published NICE health economics guidance, real-world studies, modelling studies and physician interviews, making the assumptions reasonable and consistent with clinical practice.
Meanwhile, we also included a societal perspective, which comprehensively considers the indirect costs associated with DME treatment. Specifically, the study not only accounted for transportation costs and caregiver costs but also incorporated the costs related to blindness, estimated based on the average daily salary. This holistic approach to costing reflects the broader economic impact of DME on patients and society and thus highlights the substantial burden of indirect costs caused by visual impairment and blindness, thereby better supporting the decision-making in healthcare resource allocation.
This study has made important contributions to explore the cost-effectiveness of DME treatment options, but it has several limitations. First, the indirect comparison with conbercept and ranibizumab relied on NMA, which potentially introduces uncertainty into the relative efficacy estimates due to the heterogeneity across trials in study design, patient characteristics and dosing regimens. Second, the clinical trial in the Chinese subgroup had only 2-year follow-up period. Long-term model inputs, including transition probabilities and the number of injections from year 3 to 5 and beyond, were obtained through normal cumulative density function and expert consultation, respectively, lacking real-world validation. Consequently, this long-term assumption may either overestimate or underestimate the absolute magnitude of the estimated QALY gains and cost savings, depending on the real-world disease progression patterns. To reduce model uncertainty, we further assumed identical efficacy across treatment arms from year 3 onward, which may underestimate the clinical advantage of faricimab attributable to its extended durability.
Third, due to the limited natural history studies, we assumed the initial state distribution of patients to be consistent with the Chinese subgroup in the RHINE trial during Markov simulations. Patient recruitment criteria in clinical trials may have led to differences between the trial population and real-world patients, potentially biasing the results by over- or underestimating the visual acuity of patients with poor vision.
Conclusion
The CEA demonstrated that faricimab is a cost-effective treatment for DME in China. Compared with aflibercept, conbercept, and ranibizumab, faricimab provides additional QALYs without causing a substantial economic burden. Notably, faricimab dominates conbercept since it shows an absolute economic advantage when compared with conbercept. The results derived from deterministic and probabilistic sensitivity analysis are robust and further strengthen the cost- effectiveness of faricimab. This study offers the first evidence demonstrating that faricimab is a cost-effective treatment for DME-induced visual impairment in China, serving as a critical reference for both clinical practice and reimbursement decision-making.
Summary points
•
Diabetic macular edema (DME) is a leading cause of vision impairment in diabetic patients. Globally, approximate 4.5 billion people had diabetes in 2017. China had 1.144 billion diabetic patients, of whom 0.75% had DME and 63.7% of DME patients suffered from bilateral disease.
•
Faricimab is the first bispecific antibody targeting VEGF-A/ANG-2 for DME. It uses a personalized treatment interval regimen to improve vision, ensure safety and enhance patient compliance.
•
This study evaluated faricimab’s cost-effectiveness compared with aflibercept, conbercept, ranibizumab in China through Markov model from the Chinese health system perspective, based on the RHINE trial’s Chinese subgroup.
•
In the base case of over a 20-year lifetime horizon, faricimab gained 0.42, 0.61 and 0.80 incremental QALYs compared with aflibercept, conbercept and ranibizumab, while reducing costs by 33,315 Chinese Yuan (CNY), 59,061CNY and 12,314 CNY. Therefore, faricimab was demonstrated as a dominant and cost-effective treatment option for DME.
•
This is the first Chinese cost-effectiveness study of faricimab for DME. Faricimab is cost-effective, providing evidence for clinical practice and healthcare reimbursement decisions.
Author contributions
F Shi and S Tan contributed equally to this work, including developing the study objective, adapting CEA model, collecting model inputs and conducting the modelling analyses and manuscript writing. Y Shu and T Liu validated the model setting and data inputs. Y Xia, C Buehrer provided global model. S Han provided expert consultations on the contents of the manuscript. The manuscript was reviewed and agreed by all coauthors. All the authors approved the final version of the manuscript.
Financial disclosure
This study was funded by Roche, China. Funding was not contingent upon publication of the manuscript.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of this shared data is in accordance with the terms (if any) agreed upon their receipt. The source of this data is: RHINE trial (clinicaltrials.gov identifier: NCT03622593).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 8.89 MB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Bhagat N, Grigorian RA, Tutela A, Zarbin MA. Diabetic macular edema: pathogenesis and treatment. Surv. Ophthalmol. 54(1), 1–32 (2009).
2.
Carracher AM, Marathe PH, Close KL. International Diabetes Federation 2017. J. Diabetes 10(5), 353–356 (2018).
3.
Hou X, Wang L, Zhu D et al. Prevalence of diabetic retinopathy and vision-threatening diabetic retinopathy in adults with diabetes in China. Nat. Commun. 14(1), 4296 (2023).
4.
Jin P, Peng J, Zou H. A 5-year prospective study of Type 2 diabetes patients in Shanghai Xinjing Community1.The incidence and risk factors of diabetic retinopathy and diabetic macular edema in Chinese Type 2 diabetes residents. Chinese J. Exp. Ophthalmol. 34(4), 363–367 (2016).
5.
Chinese Ophthalmological Society. Clinical practice guidelines for diabetic retinopathy in China (2014). Chinese J. Ophthalmol. 50(11), 851–865 (2014).
6.
Treatment techniques and clinical guidelines for photocoagulation of diabetic macular edema. Ophthalmology 94(7), 761–774 (1987).
7.
Smith CW, Guyer DR, D'Amico DJ. Subretinal fibrosis after laser photocoagulation for diabetic macular edema. Am. J. Ophthalmol. 113(6), 652–656 (1992).
8.
Wong TY, Haskova Z, Asik K et al. Faricimab treat-and-extend for diabetic macular edema. Ophthalmology 131(6), 708–723 (2024).
9.
Wykoff CC, Abreu F, Adamis AP et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, Phase III trials. Lancet 399(10326), 741–755 (2022).
10.
Sun X, Li X, Han M. Efficacy, durability, and safety of faricimab in diabetic macular edema (DME): 1-year results from China subpopulation of Phase III RHINE trial. Invest. Ophthalmol. Vis. Sci. 64(8), Poster 2700 (2023).
•• This clinical trial study provides important comparative effectiveness data of intravitreal faricimab of diabetic macular edema in China.
11.
Chen Y-X, Li X-X, Yoon YH et al. Intravitreal aflibercept versus laser photocoagulation in Asian patients with diabetic macular edema: the VIVID-East study. OPTH 14, 741–750 (2020).
12.
on behalf of the REFINE study group, Li X, Dai H et al. Efficacy and safety of ranibizumab 0.5 mg in Chinese patients with visual impairment due to diabetic macular edema: results from the 12-month REFINE study. Graefes Arch. Clin. Exp. Ophthalmol. 257(3), 529–541 (2019).
13.
Liu K, Wang H, He W et al. Intravitreal conbercept for diabetic macular oedema: 2-year results from a randomised controlled trial and open-label extension study. Br. J. Ophthalmol. 106(10), 1436–1443 (2022).
14.
Bührer C, Paling T, Gale R, Paulo T, Bagijn M. Cost-effectiveness of faricimab in the treatment of diabetic macular oedema (DMO): a UK analysis. PharmacoEconomics Open 8(3), 445–457 (2024).
15.
Glassman AR, Wells JA, Josic K et al. Five-year outcomes after initial aflibercept, bevacizumab, or ranibizumab treatment for diabetic macular edema (Protocol T Extension Study). Ophthalmology 127(9), 1201–1210 (2020).
16.
Ming J, Zhang Y, Xu X et al. Cost-effectiveness analysis of intravitreal aflibercept in the treatment of diabetic macular edema in China. J. Comp. Eff. Res. 9(3), 161–175 (2020).
• Provides methods for calculating transitional probabilities.
17.
Elshout M, Webers CAB, Van Der Reis MI, Schouten JSAG. A systematic review on the quality, validity and usefulness of current cost-effectiveness studies for treatments of neovascular age-related macular degeneration. Acta Ophthalmologica 96(8), 770–778 (2018).
• Provides methods for calculating transitional probabilities.
18.
Health economics: National Institute for Health and Care Excellence 2018, NICE (2018).
19.
China Population and Employment Statistics Yearbook – 2022. China Statistics Press (2022).
20.
Christ SL, Lee DJ, Lam BL, Zheng DD, Arheart KL. Assessment of the effect of visual impairment on mortality through multiple health pathways: structural equation modeling. Invest. Ophthalmol. Vis. Sci. 49(8), 3318 (2008).
21.
Liu J, Jiang Y, Ni W, He X. Pharmacoeconomic evaluation of anti- VEGF drugs and laser photocoagulation for the treatment of DME in China. Chin. Pharmaceut. J. 55(5), 402–407 (2020).
22.
Wang J, Chen Z, Song Y. Falls in aged people of the Chinese mainland: epidemiology, risk factors and clinical strategies. Ageing Res. Rev. 9, S13–S17 (2010).
23.
Chen R, Wu B. Cost-effectiveness of intravitreal conbercept versus other treatments for wet age-related macular degeneration. Ann. Transl. Med. 8(15), 939–939 (2020).
24.
Chen R, Hu Z, Qin X, Xu X, Copeland JRM. A community-based study of depression in older people in Hefei, China—the GMS-AGECAT prevalence, case validation and socio-economic correlates. Int. J. Geriat. Psychiatry 19(5), 407–413 (2004).
25.
Guan X, Lin F, Wang L, Ni Q, Shi L. Burden of low vision and blindness in Chinese elder popullation: data from field survey. Value Health 19(7), A565–A566 (2016).
26.
Czoski-Murray C, Carlton J, Brazier J, Young T, Papo NL, Kang HK. Valuing condition-specific health states using simulation contact lenses. Value Health 12(5), 793–799 (2009).
•• Provides utilities for base-case study.
27.
Maniadakis N, Konstantakopoulou E. Cost effectiveness of treatments for diabetic retinopathy: a systematic literature review. Pharmacoeconomics 37(8), 995–1010 (2019).
28.
Hodgson R, Reason T, Trueman D et al. Challenges associated with estimating utility in wet age-related macular degeneration: a novel regression analysis to capture the bilateral nature of the disease. Adv. Ther. 34(10), 2360–2370 (2017).
29.
Brown GC. Utility values and age-related macular degeneration. Arch. Ophthalmol. 118(1), 47 (2000).
30.
Liu G. China Guidelines for Pharmacoeconomic Evaluations: A Manual (2022). (1st Edition). China Market Press (2020).
31.
Coyne KS. The impact of diabetic retinopathy: perspectives from patient focus groups. Fam. Pract. 21(4), 447–453 (2004).
32.
Sharma A, Kumar N, Kuppermann BD, Bandello F, Loewenstein A. Faricimab: expanding horizon beyond VEGF. Eye 34(5), 802–804 (2020).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 20 November 2025
Accepted: 11 February 2026
Published online: 18 March 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost-effectiveness analysis of the use of faricimab in diabetic macular edema in China. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0190
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Livio Vitiello, Giuseppe Giannaccare, Enrico Borrelli, Giulia Coco, Flavia Chiosi, Filippo Lixi, Mario Troisi, Vincenzo Gagliardi, Eleonora D’Aniello, Alfonso Pellegrino, Claudio Iovino, Faricimab: current evidence for the treatment of retinal vein occlusion, Graefe's Archive for Clinical and Experimental Ophthalmology, 10.1007/s00417-026-07304-2, (2026).