Lefamulin versus omadacycline for community acquired bacterial pneumonia: a systematic review and anchored indirect treatment comparison using moxifloxacin as the common comparator
Abstract
Aim: Community-acquired bacterial pneumonia (CABP) remains a major cause of morbidity and mortality worldwide, particularly among elderly and susceptible populations. Escalating antimicrobial resistance among prevalent CABP pathogens in China, combined with safety limitations of existing regimens, underscores the urgent need for novel therapeutic strategies. Lefamulin (LEF) and omadacycline (OMA), recently approved in mainland China, offer promising alternatives, but direct comparative evidence is lacking. This study aims to indirectly compare the clinical efficacy and safety outcomes of LEF versus OMA in the treatment of CABP and to explore subgroup differences in high-risk populations. Materials & methods: A systematic literature review was conducted across PubMed, Embase, the Cochrane Library and ClinicalTrials.gov from inception through March 2024, limited to English-language studies, to identify phase III randomized controlled trials evaluating LEF or OMA in adults with CABP. The Bucher method was used for the indirect comparison, with effect estimates reported as risk ratios (RRs) and 95% CIs. Similarities in trial design and populations supported the transitivity assumption. Primary end points were early clinical response (ECR), investigator-assessed clinical response (IACR) at test of cure (TOC) and treatment-emergent adverse events leading to death. Subgroup analyses were further stratified by patient age (elderly patients), presence of comorbidities and causative pathogens. Results: Three randomized controlled trials involving 2063 patients were included in this study. LEF and OMA demonstrated comparable efficacy in terms of ECR (RR: 1.01, 95% CI: 0.93–1.09) and in terms of IACR at TOC (RR: 0.95, 95% CI: 0.88–1.02). The relative risk of treatment-emergent adverse events leading to death in the LEF group compared with the OMA group was 0.67 (95% CI: 0.15–3.02), with no statistically significant difference observed. In subgroup analysis, LEF demonstrated statistically significant superiority over OMA in treating patients with Haemophilus influenzae infections (RR: 1.28, 95% CI: 1.03–1.60). No other subgroups reached statistical significance. LEF showed a numerical trend toward favoring in multiple subgroups, including the elderly, patients with comorbidities, and those infected with specific pathogens, particularly in the ECR analysis. Meanwhile, OMA demonstrated potential numerical advantages in a few subgroups defined by comorbidities or specific pathogens for IACR at TOC. Conclusions: Both LEF and OMA have been shown to be effective and safe in treating CABP. LEF demonstrated significant benefit in Haemophilus influenzae infections and consistently favorable trends in high-risk or specific infected subgroups. OMA also shows favorable trends in certain patient groups. These findings highlight the need to further accumulate additional clinical data or real-world evidence to support future comparative research. The introduction of novel antibiotics, such as LEF and OMA, represents an important step toward addressing the pressing challenge of antimicrobial resistance and improving outcomes for patients with CABP in China.
Plain language summary
What is this article about?
Community-acquired bacterial pneumonia (CABP) is a common lung infection, especially serious for older adults and those with other health problems. In China, antibiotic resistance makes treatment harder. Two new antibiotics, lefamulin (LEF) and omadacycline (OMA), are now available, but no direct comparison exists. This article reviews research and uses indirect methods to compare their effectiveness for CABP, including in high-risk groups.
What are the results?
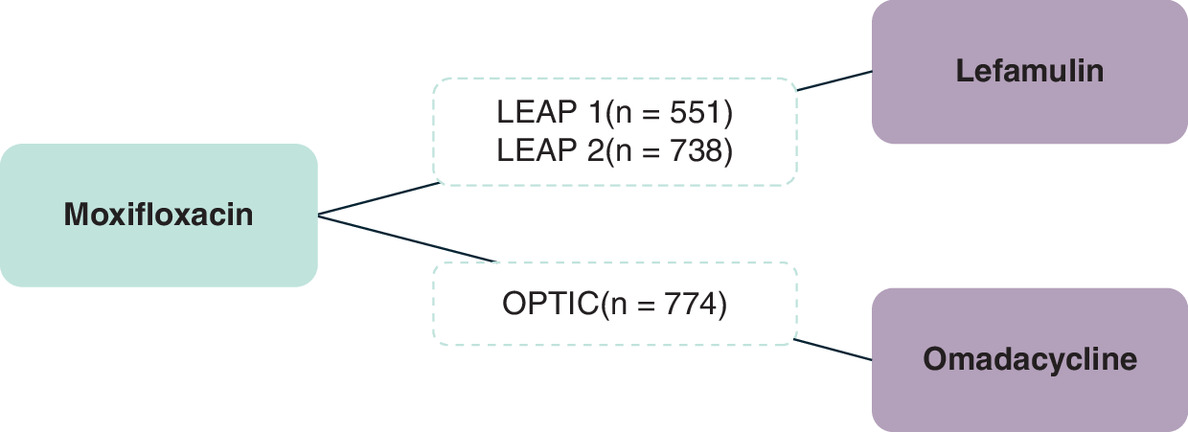
Based on the study objectives, a systematic literature review identified two confirmatory phase III trials for LEF in CABP (LEAP 1 and LEAP 2) and one for OMA (OPTIC). All trials used moxifloxacin as the comparator, enabling an indirect comparison of LEF and OMA through a common comparator. In the overall population, both LEF and OMA demonstrated comparable efficacy. Exploratory subgroup analyses suggested potential differences in efficacy across specific subgroups.
What do the results mean?
The results suggest that both LEF and OMA are effective and safe options for CABP, expanding therapeutic choices and potentially helping to address antimicrobial resistance in China as their innovative mechanism of actions. LEF may offer advantages in certain pathogen-specific subgroups. However, further evidence is needed to guide clinical decision-making and optimize treatment strategies for CABP.
Community-acquired bacterial pneumonia (CABP) is a common respiratory infectious disease [1] characterized by an acute infection of the pulmonary parenchyma in patients who acquire the infection outside of a hospital setting [2]. Streptococcus pneumoniae is generally regarded as the most prevalent causative pathogen of CABP worldwide [3], while Haemophilus influenzae and Mycoplasma pneumoniae are among the most frequently detected pathogens in China [4]. CABP remains one of the most prevalent infectious diseases globally, with elderly individuals constituting a major high-risk group. Epidemiological data from China indicate that the annual incidence in the general population is approximately 7.13 per 1000 persons, whereas in those aged 70–80 years, the incidence rises to 11.90 per 1000 persons, nearly twice that of the general population. CABP is further associated with a substantial case fatality rate, particularly among older patients. Besides, patients with comorbidities such as chronic obstructive pulmonary disease, heart failure and diabetes, are at higher risk for CABP and tend to have poorer prognosis [5].
The initial treatment of CABP is empiric and guided by local epidemiology and resistance patterns. In China, the extended use of conventional antibiotics and the absence of new antibiotics have accelerated resistance among common pathogens. This has led to more frequent treatment failures, as shown by the resistance rates of second-generation cephalosporins, macrolides and tetracyclines to Streptococcus pneumoniae, a common CABP pathogen, which are as high as 39.9–50.7% [6], 88.1–91.3% [6] and 89% [7], respectively. Safety considerations further constrain current regimens. Macrolides have been associated with cardiovascular risks [8] and severe adverse reactions like delirium associated with systemic fluoroquinolones [9]. These findings underscore the need for timely diagnosis and optimized therapeutic strategies in this vulnerable group.
Moreover, antimicrobial resistance (AMR) has been recognized as one of the top ten global public health threats. If left unaddressed, AMR could result in economic losses of up to 100 trillion USD by 2050. This would have far-reaching consequences for human health, global economies, international trade and healthcare systems [10]. The WHO has proposed multiple strategies to mitigate AMR, among which the development of novel antimicrobial agents is considered a cornerstone [11]. However, progress in antibiotic innovation remains limited, resulting in a stagnating research and development (R&D) pipeline. The WHO outlines four criteria for antibiotic innovation: new chemical class, new molecular target, new mechanism of action and absence of cross-resistance. The latest WHO analyses indicated that the majority of newly authorized antibiotics fall short of meeting the WHO-defined innovation criteria [11].
Lefamulin (LEF) and omadacycline (OMA) are the most recently approved antibiotics for CABP in mainland China.
LEF belongs to a novel chemical class and it is one of few antibiotics that meets the WHO-defined innovation criteria. It represents the first pleuromutilin antibiotic approved for systemic use in humans. LEF binds to both the A- and P-sites of the bacterial ribosome through an induced-fit mechanism, thereby limiting cross-resistance and slowing the development of resistance [12]. It exhibits broad-spectrum antibacterial activity against pathogens that commonly cause CABP [13]. And is available in intravenous and oral formulations approved in mainland China. Phase III trials (LEAP 1/2) demonstrated noninferiority to moxifloxacin [14].
In contrast, OMA is classified by the WHO as a notable advancement within an existing antibiotic class. As a third-generation tetracycline, it was developed to overcome resistance to earlier tetracyclines and demonstrates broad-spectrum activity against common CABP pathogens [15]. It is also available in both intravenous and oral formulations, and its efficacy was confirmed in the phase III OPTIC trial, which demonstrated noninferiority to moxifloxacin in adults with CABP [16].
Given China’s escalating antimicrobial resistance and the prolonged lack of newly approved antibiotics with novel mechanisms, there remains a substantial unmet clinical need in the management of CABP. Although OMA and LEF are the two most recently approved novel-class agents for CABP in China, there is currently no head-to-head evidence regarding their relative efficacy and safety. To address this evidence gap, we conducted an anchored indirect treatment comparison (ITC) using moxifloxacin as the common comparator, leveraging data from the pivotal trials of LEF (LEAP 1/2) and OMA (OPTIC). This analytical approach is supported by the methodological comparability of these studies, including similar randomized designs, assessments of disease-severity (e.g., PORT/PSI) and regulatory end points (ECR and IACR at TOC). By generating a comparison between LEF and OMA and evaluating potential subgroup differences, this study provides decision-relevant evidence to support the CABP management in China and may inform the appropriate use of novel antibiotics in clinical practice.
To our knowledge, this is the first ITC comparing LEF and OMA for CABP. We presented a preliminary abstract at ISPOR Europe 2024 (CO111) [17], and this manuscript builds on that work to provide an expanded, peer-reviewed version.
Materials & methods
Systematic literature review
We conducted a systematic literature review (SLR) to identify relevant randomized controlled trial (RCT) evidence on the clinical efficacy and treatment-emergent adverse events (TEAEs) leading to death of LEF and OMA compared with other antibiotics. This SLR was conducted in accordance with the Cochrane criteria and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [18,19]. This review was not registered on a public platform. Nonetheless, we followed established reporting guidance and provide detailed methodological and Supplementary Materials to facilitate independent appraisal.
Literature sources & searches
Searches were conducted across electronic databases to identify English-language articles from inception through March 2024. Databases for published literature included PubMed, Embase and the Cochrane Library, while ClinicalTrials.gov was searched for registered clinical trials.
Study selection criteria
Studies meeting the following inclusion criteria were considered: patients aged 18 years and older with CABP; either OMA or LEF was included in the intervention group; phase III RCTs; and reported at least one outcome of interest. Studies were excluded if they enrolled only pediatric patients; lacked outcome measures of interest; involved overlapping subjects and duplicate data; had no available data; were reviews or meta-analyses or were nonEnglish literature.
Detailed search strategies and PICOS are listed in the supplementary material (Supplementary Tables 1 & 2).
Screening, extraction & quality assessment
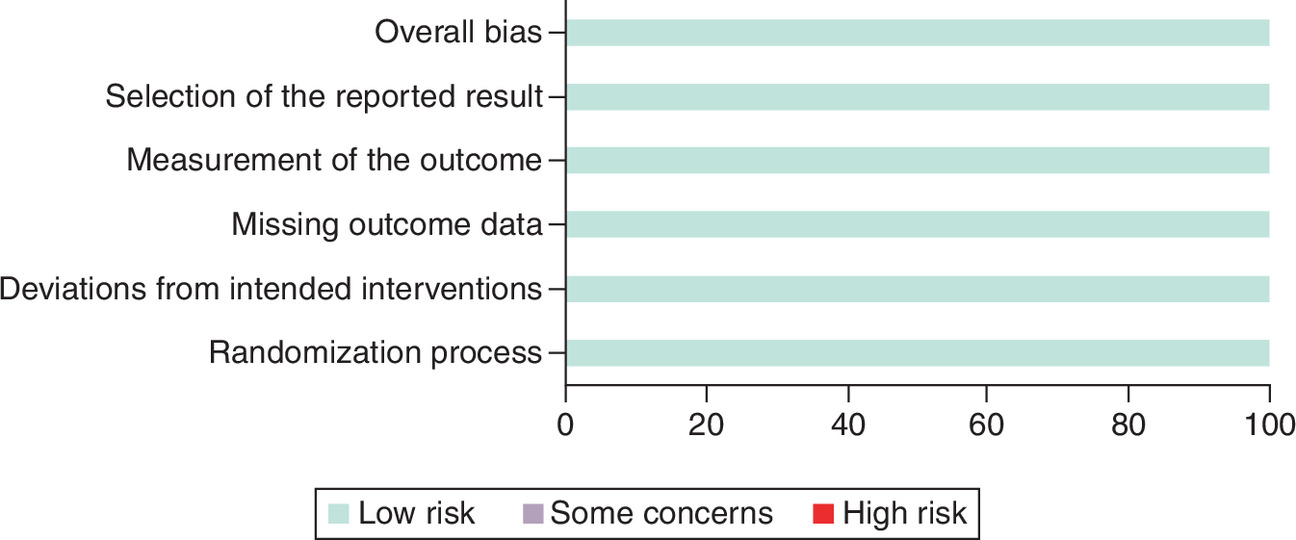
Study screening and data extraction were conducted by two independent investigators, discrepancies were resolved by consensus or involving a third investigator. The extracted information included the study name, publication year, study design, sample size, interventions, baseline characteristics of the population and efficacy outcomes and TEAEs leading to death. The quality assessment of the included studies was conducted using the Cochrane Risk of Bias Tool (RoB 2) [20], which is widely recommended for RCTs as it provides a structured and standardized approach to evaluate potential sources of bias across key domains. Accordingly, following five domains were assessed: bias arising from the randomization process; bias due to deviations from intended interventions; bias due to missing outcome data; bias in the measurement of the outcome and bias in the selection of the reported result. Based on predefined criteria, the risk of bias for each study was categorized as ‘low risk of bias’, ‘some of concern’, or ‘high risk of bias’.
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Indirect treatment comparison (ITC)
Statistical analysis
Due to the limited number of RCTs, the available evidence did not form a closed loop across treatments, rendering a network meta-analysis infeasible. However, the trials were connected via a common comparator (moxifloxacin), which enabled an anchored ITC using the Bucher approach. This method is grounded in the frequentist framework and employs an adjusted ITC approach as proposed by Bucher et al. [21]. Specifically, treatment A is compared with the common comparator C in one RCT, and treatment B is compared with C in another, allowing an indirect comparison between A and B while preserving randomization [22]. Compared with network meta-analysis, which requires a fully connected network of studies [23], the Bucher method is particularly suitable when available evidence is sparse and does not form a closed loop, as in the present analysis.
Statistical heterogeneity among direct comparison studies was assessed using Cochran’s Q test and the I-squared (I2) statistic when two or more RCTs were available for a given treatment contrast [24,25]. For the LEF-to-MOXI comparison, data from the LEAP-1 and LEAP-2 trials were pooled using a random-effects model, with the between-study variance (τ2) estimated by restricted maximum likelihood. Given that τ2 relied on only two studies, the precision of the heterogeneity estimate was limited and therefore interpreted cautiously. In contrast, for the OMA-to-MOXI comparison, only a single RCT (OPTIC) informed the direct evidence; therefore, between-study heterogeneity could not be estimated, and this link was treated as a single-study fixed-effect estimate (i.e., τ2 was set to zero), with the variance derived directly from the trial-level standard error. For binary outcomes such as early clinical response and TEAEs leading to death, effect estimates were expressed as relative risk (RR) with corresponding 95% CIs. We performed all analyses utilizing the ‘network package (version 1.2.1)’ in Stata 14.0 for ITC analysis and Microsoft Excel for forest plot generation.
Analytical population & end points
The primary analyses were conducted using the intention-to-treat (ITT) population to maintain randomization and limit bias, ensuring reliable estimates of comparative effectiveness. If ITT data for a given outcome were not available in the source trial, the modified ITT population was used as reported.
To explore potential effect modifiers, subgroup analyses were planned for clinically relevant categories such as age (≥65 years); comorbid conditions (e.g., diabetes); renal function status and pathogen type.
The outcome measures of interest in this study include The US FDA primary end point: early clinical response (ECR) at 96 h (within a 24 h window) after the first dose of the study drug; The European Medicines Agency co-primary end points: investigator-assessed clinical response (IACR) at 5–10 days (TOC [test of cure]) after the last dose of the study drug and TEAEs leading to death, recorded as a secondary end point, was included to capture critical differences in survival outcomes. All end point definitions were consistently extracted from and aligned across the included studies.
Results
Study characteristics
In total of 136 studies were initially identified through the database searching. Following a full-text review, eight records reposting on three unique RCTs were included. For trials with multiple records, we systematically extracted and synthesized data across all available publications to facilitate subgroup and pooled analyses, as detailed in Table 2. The flow chart of study selection is presented in Figure 1. Overall, there were three RCTs included 2063 patients. The three studies included in this ITC shared highly similar inclusion and exclusion criteria, enrolling adults with radiographically confirmed CABP, acute onset and at least three characteristic symptoms. All studies primarily enrolled patients classified as PSI/PORT risk class II–IV. Key exclusion criteria (e.g., recent antibiotic use, hospital-acquired pneumonia, significant organ dysfunction and immunocompromised status) were consistent across trials. Detailed information can be found in the supplementary material (Supplementary Table 3).
| RCT | Experiment | Control | Age (E/C, years) | Male sex (E/C) | Patient severity | ITC analysis population for ECR outcome (n = E/C) | ITC analysis population for IACR at TOC outcome (n = E/C) |
|---|---|---|---|---|---|---|---|
| OPTIC | OMA (IV, PO) | MOXI (IV, PO) | 61/63 | 53.9%/56.4% | PSI/PORT risk class II–IV | ITT population (n = 386/388): all patients who underwent randomization | ITT population (n = 386/388): all patients who underwent randomization |
| LEAP1 | LEF (IV, PO) | MOXI (IV, PO) | 61/59.6 | 61.6%/58.2% | PSI/PORT risk class III–V | ITT population (n = 276/275): all patients who underwent randomization | Modified ITT population (n = 273/273): All randomized patients who received ≥1 dose of study drug; analyzed based on randomized treatment group |
| LEAP2 | LEF (PO) | MOXI (PO) | 57.4/57.7 | 55.9%/48.9% | PSI/PORT risk class II–V | ITT population (n = 370/368): all patients who underwent randomization | Modified ITT population (n = 368/368): All randomized patients who received ≥1 dose of study drug; analyzed based on randomized treatment group |
PSI/PORT risk class: The Pneumonia Severity Index (PSI), interchangeably referred to as the PORT score, represents a methodologically equivalent framework for CAP severity assessment, as both derive from the same validated scoring system that stratifies patients into five risk classes.
E: Experimental group; C: control group; MOXI: Moxifloxacin; ITT: Intention-to-treat; IV: Intravenous administration; PO: Oral administration; ECR: Early clinical response; IACR at TOC: Investigator-assessed clinical response at test-of-cure.
| Study ID | Publication year | RCT code | Population included in ITC | Ref. |
|---|---|---|---|---|
| Stets et al. | 2019 | OPTIC | Overall population, specific pathogens subgroup | [16] |
| Cornely et al. | 2021 | OPTIC | Renal impairment subgroup | [26] |
| Pai et al. | 2019 | OPTIC | Diabetes mellitus history subgroup | [27] |
| Ramirez et al. | 2018 | OPTIC | Ages ≥ 65 subgroup | [28] |
| File et al. | 2019 | LEAP1 | Overall population, ages ≥ 65 subgroup, renal impairment subgroup, specific pathogens subgroup | [29] |
| Alexander et al. | 2019 | LEAP2 | Overall population, ages ≥ 65 subgroup, renal impairment subgroup, specific pathogens subgroup | [30] |
| File et al. | 2021 | LEAP1/LEAP2 pooled | Diabetes mellitus history subgroup | [14] |
| Paukner et al. | 2022 | LEAP1/LEAP2 pooled | Macrolide-resistant SP subgroup | [31] |
ITC: Indirect treatment comparison; ITT: Intent-to-treat population; S.P.: Streptococcus pneumoniae.
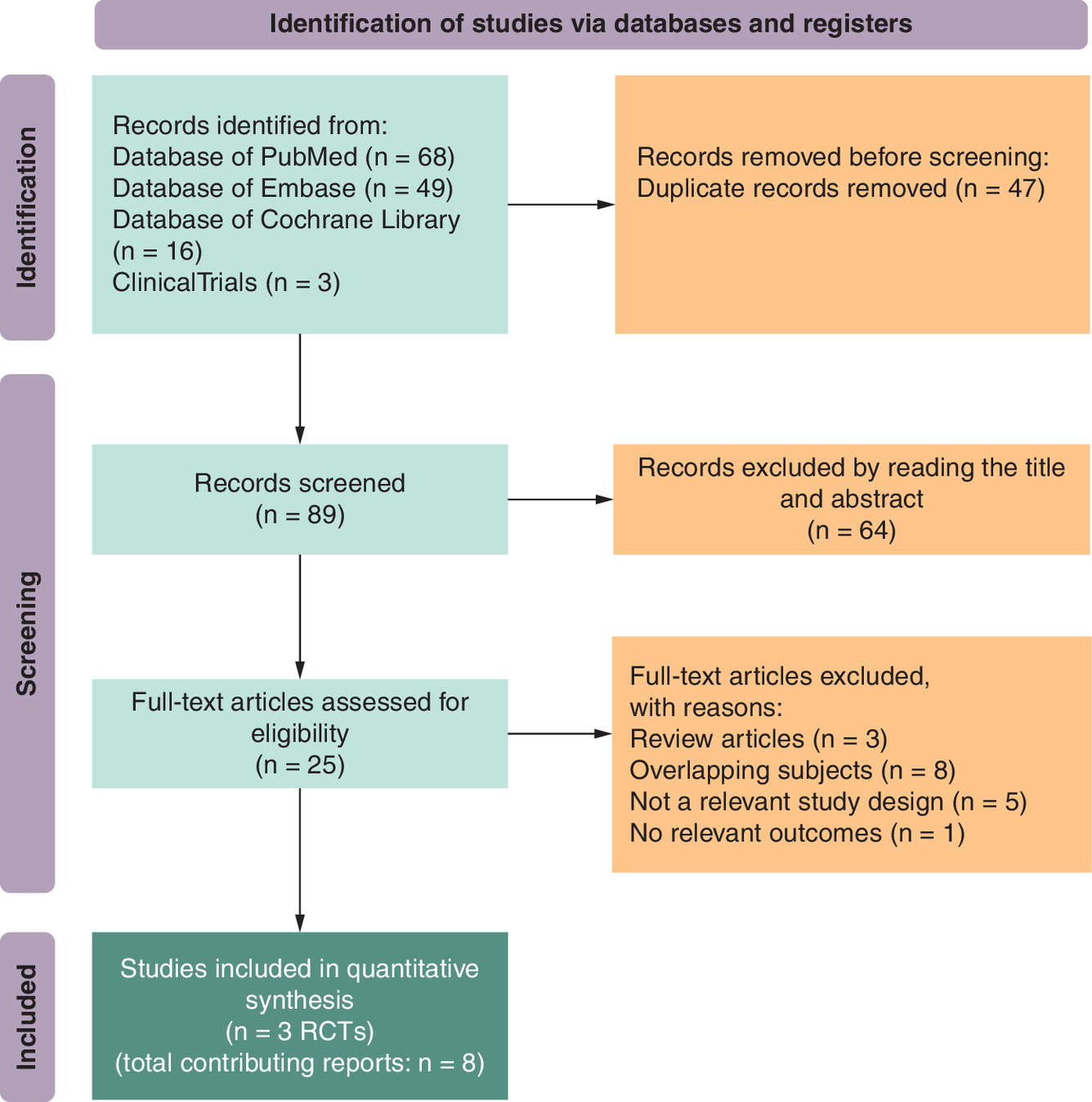
Figure 1. Flow chart of study selection.
RCTs: Relevant randomized controlled trial.
The OPTIC trial directly compared OMA with moxifloxacin, LEAP-1 and LEAP-2 directly compared LEF with moxifloxacin (Figure 2). Table 1 summarizes the baseline characteristics, as well as the definitions and sample sizes of the overall populations used across the three trials.
The characteristics of the included articles for data extraction are summarized in Table 2. The articles by Stets et al., File et al. and Alexander et al. [16,29,30] serve as the primary references for three RCTs, detailing the study designs and overall population results. The remaining articles provide data on various subgroups, including ages ≥ 65, renal impairment, diabetes mellitus history and specific pathogens [26–28]. The studies by File et al. [14] and Paukner et al. [31] were included for the diabetes mellitus history and certain specific pathogens subgroups analysis, which provide the combined results of LEAP1 and LEAP2.
Risk of bias assessment
All included RCTs were assessed as having a low risk of bias using the ROB2 tool (Figure 3). Two reviewers independently assessed the primary publications of the three unique trials, which comprehensively reported study designs and outcomes. Other publications presenting subgroup or pooled analyses derived from these trials were excluded from bias risk assessment, as they provided no additional methodological information beyond the primary reports.
Results in the overall population
Efficacy end points
Both LEF and OMA demonstrated high efficacy in clinical trials. In the overall population (Figure 4), comparable efficacy of ECR (RR: 1.01, 95% CI: 0.93–1.09) and IACR at TOC (RR: 0.95, 95% CI: 0.88–1.02) was found between LEF and OMA, with no statistically significant differences [17].
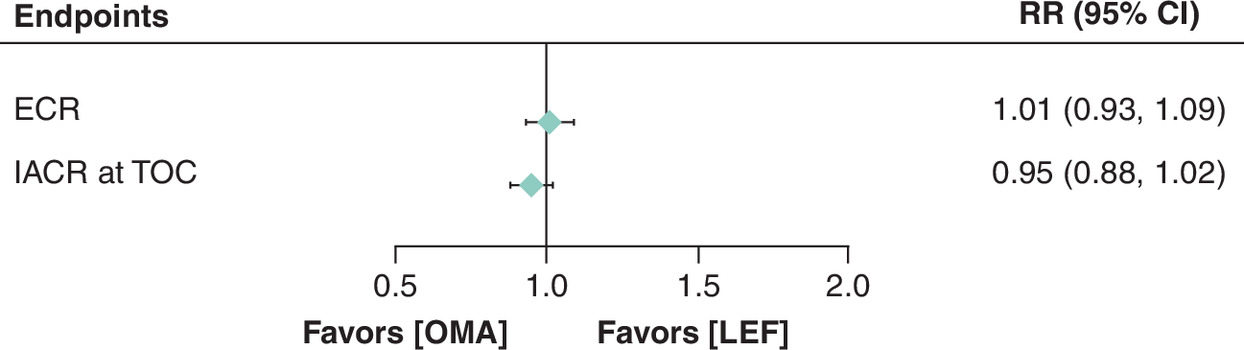
Figure 4. Lefamulin versus omadacycline in early clinical response and investigator-assessed clinical response at test of cure in the overall population.
ECR: Early clinical response; IACR at TOC: Investigator-assessed clinical response at test-of-cure; LEF: Lefamulin; OMA: Omadacycline; RR: Relative risk; CI: Confidence interval.
TEAEs leading to death
A numerical difference in the rate of TEAEs leading to deaths was observed, with LEF showing a lower point estimate than OMA, but this difference did not reach statistical significance (RR: 0.67, 95% CI: 0.15–3.02) (Figure 5). Furthermore, no treatment-related deaths occurred in the LEF trials [14,29], whereas the OMA trial did not specify whether observed deaths were treatment related [16]. It is also noteworthy that 8 deaths in the OMA trials all occurred in patients aged over 65. Collectively, these points suggest a potential trend toward a more favorable safety profile regarding TEAEs leading to death for LEF. However, these findings should be interpreted with caution due to the low event rates and wide confidence intervals.
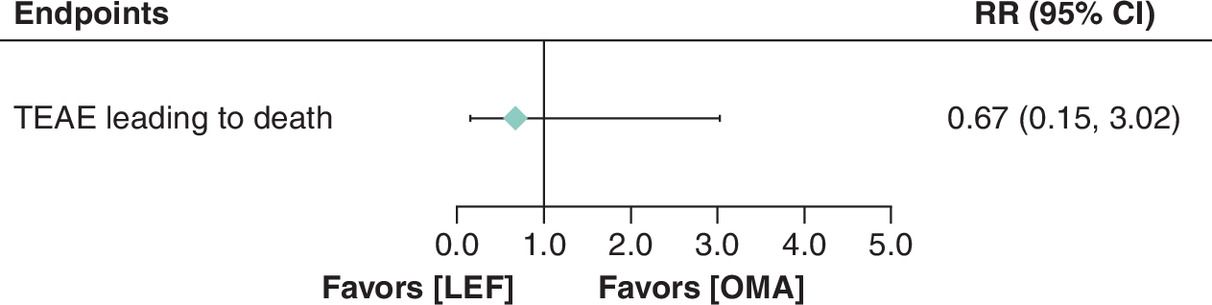
Figure 5. Lefamulin versus omadacycline in TEAEs leading to death in the overall population.
LEF: Lefamulin; OMA: Omadacycline; RR: Relative risk; CI: Confidence interval; TEAE: Treatment-emergent adverse events.
Results in subgroups
Subgroup analyses were performed for four predefined categories: age ≥65 years, renal impairment, history of diabetes mellitus, and pathogen-specific groups. Pathogen-specific subgroups included Streptococcus pneumoniae, macrolide-resistant S. pneumoniae, Haemophilus influenzae, and Mycoplasma pneumoniae. Efficacy end points were analyzed across above mentioned subgroups; ITC of TEAEs leading to death was explored only for the subgroup of patients aged ≥ 65 years due to limited data.
Efficacy end points
In subgroup analyses of ECR (Figure 6), LEF showed a nonsignificant numerical favoring (RR >1) across multiple patient groups compared with OMA. These included patients aged 65 years or older, those with renal impairment or with a history of diabetes mellitus, and those infected with common and atypical pathogens such as Streptococcus pneumoniae (including macrolide-resistant strains) and Haemophilus influenzae. Of these, the largest numerical difference was observed in patients with Haemophilus influenzae (RR: 1.24, 95% CI: 0.91–1.69). Despite these consistent trends, none of the differences reached statistical significance.
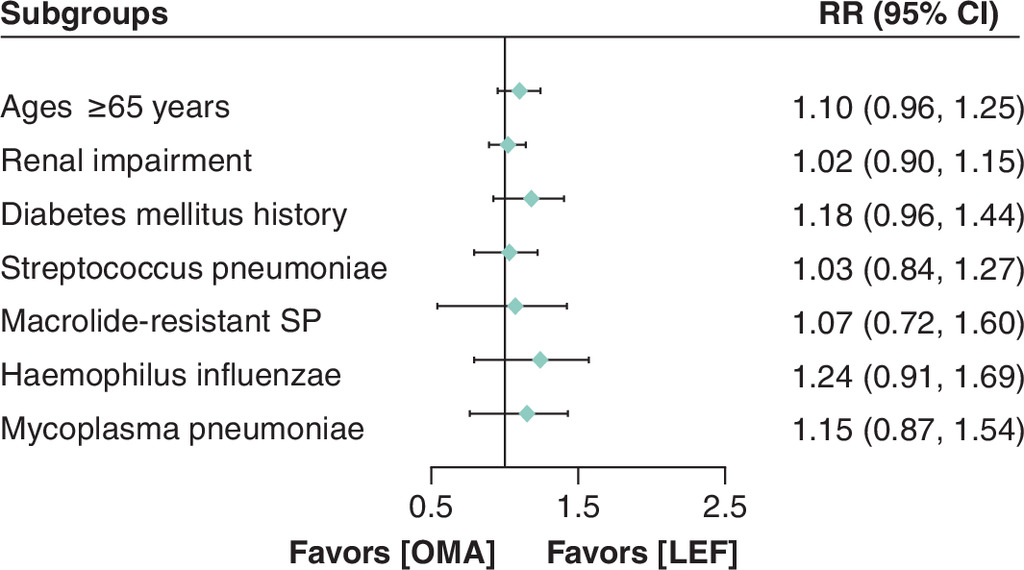
Figure 6. Lefamulin versus omadacycline in early clinical response in different subgroups.
CI: Confidence interval; LEF: Lefamulin; OMA: Omadacycline; RR: Relative risk; SP: Streptococcus pneumoniae.
In the analysis of IACR at TOC (Figure 7), a statistically significant superiority of LEF over OMA was observed exclusively in patients infected with Haemophilus influenzae (RR: 1.28, 95% CI: 1.03–1.60). However, the results for other subgroups did not reach statistical significance and the RR estimates showed variability. Specifically, the results demonstrated a numerical favored OMA (RR <1) in two subgroups: patients with renal impairment and those infected with Mycoplasma pneumoniae. In the remaining subgroups, there was a numerical trend favoring LEF (RR >1).
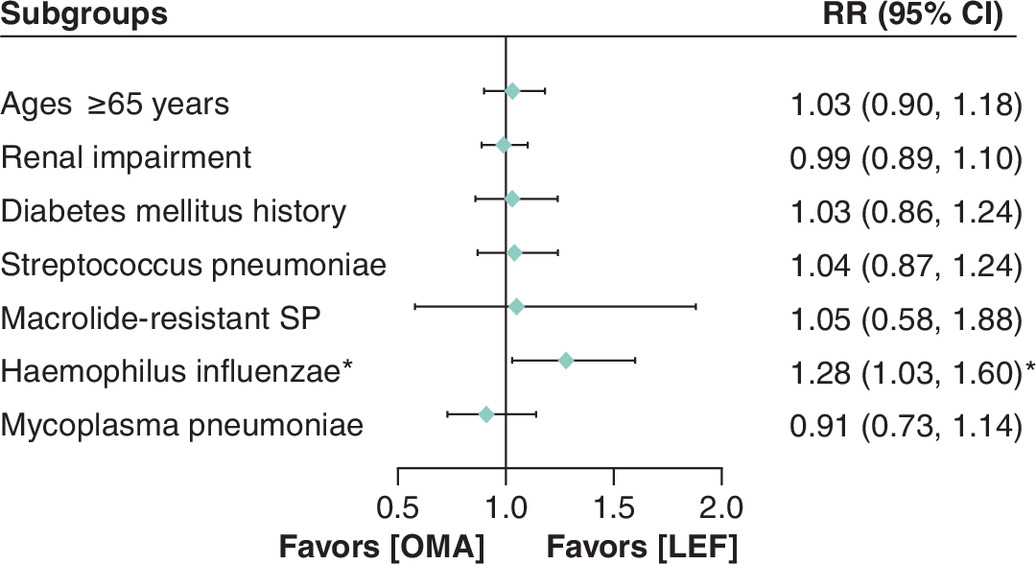
Figure 7. Lefamulin versus omadacycline in investigator-assessed clinical response at test of cure in different subgroups.
*p < 0.05 showed statistically significant differences between the groups.
CI: Confidence interval; LEF: Lefamulin; OMA: Omadacycline; RR: Relative risk; SP: Streptococcus pneumoniae.
TEAEs leading to death
For patients aged 65 years or older (Figure 8), the RR of TEAEs leading to death in the LEF compared with the OMA was 0.74 (95% CI: 0.15–3.66) which was not statistically significant.
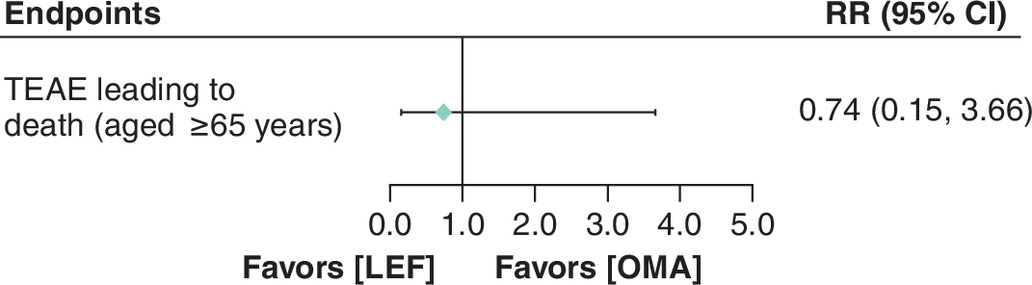
Figure 8. Lefamulin versus omadacycline in TEAEs leading to death in elderly.
LEF: Lefamulin; OMA: Omadacycline; RR: Relative risk; CI: Confidence interval; TEAE: Treatment-emergent adverse events.
Discussion
CABP, a highly prevalent infectious disease, continues to pose a substantial public health burden. It is characterized by worsening hospitalization and mortality rates, particularly affecting vulnerable groups such as infants and the elderly [5]. Meanwhile, AMR has emerged as an increasingly severe global public health issue. Annually, an estimated 4.95 million deaths are associated with resistant infections [32]. China faces a critical AMR crisis, with staggering resistance rates (up to 91.3% for macrolides and 89% for tetracyclines) against key Streptococcus pneumoniae strains, driven by overuse of existing antibiotics and a lack of novel agents [7]. This situation is particularly concerning for high-risk populations, such as the elderly and individuals with comorbidities, who remain in urgent need of safer and more effective treatment regimens for CABP [33–35]. Consequently, addressing the AMR challenge and the therapeutic unmet need in CABP underscores the urgent necessity of developing new antibiotics.
However, most antibiotics approved for the treatment of CABP in mainland China were introduced several decades ago. Commonly guideline-recommended agents [6], such as moxifloxacin (approved in 2003), levofloxacin (approved in 2004), and cephalosporins (e.g., ceftriaxone, approved in 1991), exemplify this trend [36]. Only three new antibiotics have been specifically approved for CABP in mainland China since 2020: LEF, OMA, and ceftobiprole medocaril sodium. Among these, LEF and OMA are the most comparable, given their similar antibacterial spectra and availability in both intravenous and oral formulations, enabling sequential therapy.
Over the past 5 years, there has been a focus on indirectly treatment comparison of empirical antibiotic treatments for adult CABP, with a primary focus on quinolones, macrolides and β-lactams [37–41], while investigations into tetracycline-class agents are limited. Only two studies [42,43] have compared doxycycline, a long-established tetracycline, and have shown no significant difference in clinical cure rates compared with fluoroquinolones or macrolides. There is a significant evidence gap regarding the comparative efficacy and safety of newly approved antibiotics for CABP, particularly within key subgroups defined by baseline patient characteristics or specific pathogens. Therefore, it is imperative to conduct comparative studies to assess the value of these novel antibiotics such as LEF and OMA, to generate robust evidence and inform clinical practice.
This study represents the first ITC to evaluate the comparative efficacy of the novel antibiotics LEF and OMA in patients with CABP, and an earlier version of this work was presented in abstract form at ISPOR [17]. Both LEF and OMA demonstrated high ECR and IACR at TOC in treating CABP patients, with no statistic significant difference observed for the primary end points or in most subgroups. Notably, LEF demonstrated significantly superior IACR at TOC in patients with Haemophilus influenzae compared with OMA, suggesting that LEF was associated with better clinical outcomes in this subgroup. Furthermore, point estimates indicated a numerical trend favoring LEF, particularly for ECR, whereas OMA showed numerical advantages in a few subgroups for IACR at TOC. These observations are likely related to the noninferiority design of the included trials, which may limit the ability to detect statistically significant differences between treatments. Additionally, these findings provide a valuable evidence base that can inform health technology assessment evaluations of novel antibiotics and offer insights for the development of clinical guidelines, thereby supporting healthcare decision-making. However, given the limited subgroup sizes, these observations should be interpreted with caution. Additional real-world evidence from observational studies, head-to-head trials, or expanded pooled analyses would be valuable to complement these findings and provide further comparative insights.
Subgroup analyses provide clinically relevant insights beyond aggregate efficacy estimates. Specific patient populations including the elderly [44], those with renal impairment [45], and individuals with diabetes [46], representing not only high-risk prognostic groups but also key factors influencing clinicians’ treatment selections. Elderly patients often present with challenges such as high rates of polypharmacy, longer drug half-lives and diminished organ function, which collectively lead to poor drug tolerance. Similarly, patients with renal impairment frequently experience metabolic disorders, malnutrition and weakened immune resistance, complicating their treatment. Diabetic patients, on the other hand, have high blood glucose levels that not only weaken their immune system but also promote pathogen growth, resulting in more severe infections. These risk factors collectively necessitate alternative therapeutic approaches with improved safety and efficacy profiles. Consequently, the subgroup findings from this study can provide a reference for the future clinical use of LEF and OMA, thereby helping to optimize personalized treatment strategies for high-risk patients, including the elderly and those with comorbidities.
Pathogen-specific subgroup analyses further provide valuable reference for treatment strategies. Pathogens play a crucial role in the development of CABP and can greatly impact treatment outcomes. Rising resistance in Streptococcus pneumoniae has reached a critical threshold in China, particularly to second-generation cephalosporins, macrolides, and tetracyclines alarmingly high, with resistance rates reaching 39.9%–50.7% [6], 88.1%–91.3% [6], and 89% [7] respectively. Furthermore, the annual detection rate of Haemophilus influenzae has shown an upward trend [47], which predominantly affects elderly patients who are at a higher risk of CABP, severe outcomes, and negative effects on their quality of life after admission, a trend that cannot be ignored [48]. A multicenter prospective study conducted in China revealed that Mycoplasma pneumoniae (11.05%), Haemophilus influenzae (10.67%), Klebsiella pneumoniae (10.43%) and Streptococcus pneumoniae (7.43%) were the top four pathogens with the highest detection rates [4]. Thus, this study focused on subgroup analysis of these common pathogens in China. Klebsiella pneumoniae was not included in the comparison due to a lack of reported data. However, the sample size within these specific-pathogens subgroup was limited, and aside from the result suggesting the superior efficacy of LEF for Haemophilus influenzae infections in the IACR analysis, no other statistically significant differences were observed. These findings highlight the need for future analyses with more robust datasets.
This study also compared TEAE leading to death between LEF and OMA. In two phase III RCTs of LEF, no treatment-related deaths occurred. In the OPTIC phase III RCT of OMA observed an imbalance in mortality, with 8 deaths (2%) in the OMA group compared with 4 deaths (1%) in the moxifloxacin group [16].The difference in mortality rates between the two groups was not explained, nor was it clarified whether it was related to OMA treatment [49]. The OMA label includes a warning to closely monitor CABP patients' clinical response, especially those at higher risk of death [49]. Currently, neither LEF nor OMA has black box warnings for safety risks [49,50]. As more clinical data accumulates, further research on safety characteristics in special populations, such as the elderly and those with comorbidities, is warranted.
Overall, both LEF and OMA are effective and safe treatment options for patients with CABP. Their introduction into China is expected to increase the diversity of antibiotics available, contributing to the mitigation of the serious public health threat posed by AMR. LEF is the first pleuromutilin antibiotic approved for systemic use in humans and is recognized by WHO as an innovative agent. It possesses a novel mechanism that is distinct from other classes, which has the potential to delay the development of resistance. Similarly, OMA, as a modernized tetracycline, may have a lower likelihood of resistance compared with traditional tetracyclines. Thus, prospective surveillance of resistance patterns and investigation of the relationship between novel mechanisms and resistance rates warrant further study.
This study has several limitations. First, the small sample size in subgroup analyses may make it difficult to achieve statistical significance [51], and results should be interpreted cautiously. Second, given the lack of individual patient data, this study used the Bucher method rather than a Matching-Adjusted Indirect Comparison (MAIC), limiting our ability to formally balance effect modifiers across trials. Although we qualitatively assessed transitivity by comparing key design features, baseline severity, comorbidities and end point definitions, the analysis remained restricted to aggregate data. Consequently, residual confounding from unmeasured or inconsistently reported effect modifiers cannot be fully excluded. Third, the evidence synthesis was based on systematic search conducted up to March 2024, which aligns with reporting standards. Upon finalizing the manuscript, the OPTIC-2 (phase IIIb) trial results became publicly available. As this trial may further inform the comparison anchored to moxifloxacin, these data should be included in future analyses to improve the completeness of evidence. Finally, given the limited subgroup sample sizes and lack of multiple-testing adjustment, these analyses are susceptible to false-positive findings. Thus, any significant subgroup signals should be considered as exploratory. Further clinical research on LEF and OMA is needed to generate additional data for comprehensive evaluation.
Conclusion
Both LEF and OMA have demonstrated comparable efficacy and safety profile in treating patients with CABP, with no statistically significant differences in the primary end points. Subgroup analysis showed that LEF was significantly superior to OMA in terms of IACR at TOC in patients infected with Haemophilus influenzae. In other subgroups, including elderly patients, those with comorbidities, or patients with other specific pathogen infections, no statistically significant results were found. LEF exhibited numerical advantages in most subgroups, particularly for ECR, while OMA showed numerical benefits in a few subgroups for IACR at TOC. These findings should be interpreted with caution due to limited data. The introduction of novel antibiotics, such as LEF and OMA, in China represents an important development for public health. This expansion of available treatments is crucial to combat the growing threat of antimicrobial resistance, thereby providing patients with more promising therapeutic options. Additional head-to-head comparison or real-world evidence is needed to guide research and optimize CABP treatment strategies.
Summary points
•
Community-acquired bacterial pneumonia (CABP) remains a major health concern, especially among elderly and high-risk populations in China.
•
Rising antimicrobial resistance among CABP pathogens has limited the effectiveness of traditional antibiotics. Lefamulin (LEF) and omadacycline (OMA) are newly approved antibiotics in China for CABP treatment, LEF belongs to a novel chemical class while OMA is a third-generation tetracycline.
•
The comparative effectiveness between LEF and OMA remains unknown due to the lack of head-to-head trials.
•
This study aims to compare the efficacy and safety of LEF and OMA in treating CABP patients.
•
A systematic review identified three pivotal studies that met the inclusion criteria.
•
An indirect treatment comparison was conducted. The results showed both LEF and OMA demonstrated similar efficacy and safety in CABP, with no statistically significant differences observed in the intention-to-treat population.
•
LEF exhibited numerical advantages in most subgroups, particularly for ECR, while OMA showed numerical benefits in a few subgroups for investigator-assessed clinical response at test of cure.
•
LEF showed statistically significant superiority over OMA in patients infected with Haemophilus influenzae.
•
LEF and OMA are effective and safe options for CABP patients, their introduction expands treatment options for CABP and may help address the challenge of antimicrobial resistance in China.
Author contributions
S Han and HC Li were responsible for study conception. S Han, HC Li, and MY Wu were responsible for data curation. S Han and HC Li performed data analysis and interpretation. MY Wu drafted the manuscript. S Han and HC Li critically reviewed the manuscript drafts. All authors approved the final version of the manuscript.
Acknowledgments
Statistical analysis and proofreading were supported by Hongyu Wang, Sihan Li and Yuxia Wu from Real World Solutions, IQVIA, Shanghai, China.
Financial disclosure
The study is funded by Marubeni Pharmaceuticals (Suzhou, China) Co., Ltd (formerly Sumitomo Pharmaceuticals [Suzhou, China] Co., Ltd).
Competing interests disclosure
M Wu is employed by Marubeni Pharmaceuticals (Suzhou, China) Co., Ltd. (formerly Sumitomo Pharmaceuticals [Suzhou, China] Co., Ltd.), Shanghai, China. The authors declare that the above affiliations have not influenced the objectivity of this study. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 52.44 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Martin-Loeches I, Torres A, Nagavci B et al. ERS/ESICM/ESCMID/ALAT guidelines for the management of severe community-acquired pneumonia. Intensive Care Med. 49(6), 615–632 (2023).
2.
File TM, Ramirez JA. Community-acquired pneumonia. N. Engl. J. Med. 389(7), 632–641 (2023).
3.
Shoar S, Musher DM. Etiology of community-acquired pneumonia in adults: a systematic review. Pneumonia (Nathan) 12, 11 (2020).
4.
Zhang L, Xiao Y, Zhang G et al. Identification of priority pathogens for aetiological diagnosis in adults with community-acquired pneumonia in China: a multicentre prospective study. BMC Infect. Dis. 23(1), 231 (2023).
• Recent multicenter study identifying the most common community-acquired bacterial pneumonia (CABP) pathogens in China, informing subgroup analyses in this article.
5.
Ramirez JA, Chandler TR, Furmanek SP et al. Community-acquired pneumonia in the immunocompromised host: epidemiology and outcomes. Open Forum Infect. Dis. 10(11), ofad565 (2023).
6.
Qu J, Cao B. Guidelines for the diagnosis and treatment of community-acquired pneumonia in adults in China (2016 Edition). Chin. J. Tuberculosis Respir. Dis. 39(4), 253–279 (2016).
• National guideline outlining CABP management and resistance patterns in China, providing context for the study’s rationale.
7.
[Multidisciplinary expert consensus on the rational use of tetracyclines commonly used in clinical practice]. Zhonghua Yi Xue Za Zhi 103(30), 2281–2296 (2023).
8.
Li X, Wang M, Liu G, Zhou L, Wang Z, Li C. Macrolides use and the risk of sudden cardiac death. Expert Rev. Anti-Infect. Ther. 14(6), 535–537 (2016).
9.
Anwar AI, Lu L, Plaisance CJ et al. Fluoroquinolones: neurological complications and side effects in clinical practice. Cureus 16(2), e54565 (2024).
10.
National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on the Long-Term Health and Economic Effects of Antimicrobial Resistance in the United States. Palmer GH, Buckley GJ (Eds). The health and economic burden of resistance. In: Combating Antimicrobial Resistance and Protecting the Miracle of Modern Medicine. National Academies Press, DC, USA (2021).
11.
World Health Organization. Antibacterial agents in clinical and preclinical development: an overview and analysis. 2023. Available from: https://www.who.int/publications/i/item/9789240094000
12.
Zhanel GG, Deng C, Zelenitsky S et al. Lefamulin: a novel oral and intravenous pleuromutilin for the treatment of community-acquired bacterial pneumonia. Drugs 81(2), 233–256 (2021).
• Comprehensive review of lefamulin’s (LEF) novel pleuromutilin mechanism, clinical efficacy, and its role as an innovative antibiotic for CABP treatment.
13.
Eraikhuemen N, Julien D, Kelly A, Lindsay T, Lazaridis D. Treatment of community-acquired pneumonia: a focus on lefamulin. Infect. Dis. Ther. 10(1), 149–163 (2021).
14.
File TM, Alexander E, Goldberg L et al. Lefamulin efficacy and safety in a pooled phase III clinical trial population with community-acquired bacterial pneumonia and common clinical comorbidities. BMC Pulm. Med. 21(1), 154 (2021).
15.
Watkins RR, Deresinski S. Omadacycline: a novel tetracycline derivative with oral and intravenous formulations. Clin. Infect. Dis. 69(5), 890–896 (2019).
16.
Stets R, Popescu M, Gonong JR et al. Omadacycline for community-acquired bacterial pneumonia. N. Engl. J. Med. 380(6), 517–527 (2019).
•• Pivotal Phase III randomized controlled trial (RCT) evaluating the efficacy and safety of omadacycline for CABP, serving as a key data source for indirect comparison.
17.
Wu M, Ding J, Han S, Li H. CO111 Indirect treatment comparisons of lefamulin versus omadacycline for the treatment of community-acquired pneumonia. Value Health 27(12), S35 (2024).
18.
Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
19.
Hutton B, Catalá-López F, Moher D. [The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA]. Med. Clin. (Barc.) 147(6), 262–266 (2016).
20.
Flemyng E, Moore TH, Boutron I et al. Using risk of bias 2 to assess results from randomised controlled trials: guidance from Cochrane. BMJ EBM 28(4), 260–266 (2023).
21.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 50(6), 683–691 (1997).
22.
Kim H, Gurrin L, Ademi Z, Liew D. Overview of methods for comparing the efficacies of drugs in the absence of head-to-head clinical trial data. Brit. J. Clin. Pharma. 77(1), 116–121 (2014).
23.
Macabeo B, Quenéchdu A, Aballéa S, François C, Boyer L, Laramée P. Methods for indirect treatment comparison: results from a systematic literature review. J. Mark. Access Health Policy 12(2), 58–80 (2024).
24.
Higgins JPT. Measuring inconsistency in meta-analyses. BMJ 327(7414), 557–560 (2003).
25.
Kulinskaya E, Dollinger MB. An accurate test for homogeneity of odds ratios based on Cochran's Q-statistic. BMC Med. Res. Methodol. 15(1), 49 (2015).
26.
Cornely OA, File TM, Garrity-Ryan L, Chitra S, Noble R, McGovern PC. Safety and efficacy of omadacycline for treatment of community-acquired bacterial pneumonia and acute bacterial skin and skin structure infections in patients with mild-to-moderate renal impairment. Int. J. Antimicrob. Agents 57(2), 106263 (2021).
27.
Pai MP, Wilcox MH, Curran M, Chitra S, Garrity-Ryan L, McGovern PC. 700. Safety and efficacy of omadacycline in patients with diabetes in phase 3 clinical studies. Open Forum Infect. Dis. 6(Suppl. 2), S316–S317 (2019).
28.
Ramirez J, Garrity-Ryan L, Chitra S et al. Impact of age and gender on efficacy and safety of omadacycline (OMC) vs. moxifloxacin (MOX) in community-acquired bacterial pneumonia (CABP). Presented at: Respiratory infections. European Respiratory Society (15 September 2018).
29.
File TM, Goldberg L, Das A et al. Efficacy and safety of intravenous-to-oral lefamulin, a pleuromutilin antibiotic, for the treatment of community-acquired bacterial pneumonia: the phase III Lefamulin Evaluation Against Pneumonia (LEAP 1) Trial. Clin. Infect. Dis. 69(11), 1856–1867 (2019).
•• Key phase III RCT assessing LEF for CABP, providing primary evidence for efficacy and safety in the indirect comparison.
30.
Alexander E, Goldberg L, Das AF et al. Oral lefamulin vs moxifloxacin for early clinical response among adults with community-acquired bacterial pneumonia: the LEAP 2 Randomized Clinical Trial. JAMA 322(17), 1661 (2019).
• Phase III RCT supporting the efficacy of oral LEF in CABP, included in pooled analysis for subgroup comparisons.
31.
Paukner S, Goldberg L, Alexander E et al. Pooled microbiological findings and efficacy outcomes by pathogen in adults with community-acquired bacterial pneumonia from the Lefamulin Evaluation Against Pneumonia (LEAP) 1 and LEAP 2 phase III trials of lefamulin versus moxifloxacin. J. Glob. Antimicrob. Resist. 29, 434–443 (2022).
32.
Murray CJ, Ikuta KS, Sharara F et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 399(10325), 629–655 (2022).
33.
Faverio P, Aliberti S, Bellelli G et al. The management of community-acquired pneumonia in the elderly. Eur. J. Intern. Med. 25(4), 312–319 (2014).
34.
Pletz MW, Jensen AV, Bahrs C et al. Unmet needs in pneumonia research: a comprehensive approach by the CAPNETZ study group. Respir. Res. 23(1), 239 (2022).
35.
Faulkner CM, Cox HL, Williamson JC. Unique aspects of antimicrobial use in older adults. Clin. Infect. Dis. 40(7), 997–1004 (2005).
36.
PharmaCube Database. Drug approval information for moxifloxacin, levofloxacin, and ceftriaxone. Available from: https://www.pharmcube.com/
37.
Kato H, Hagihara M, Asai N et al. Comparison between ceftriaxone and sulbactam-ampicillin as initial treatment of community-acquired pneumonia: a systematic review and meta-analysis. Antibiotics (Basel) 11(10), 1291 (2022).
38.
Basilim A, Wali H, Rabaan AA, Eljaaly K. Efficacy of empiric macrolides versus fluoroquinolones in community-acquired pneumonia associated with atypical bacteria: a meta-analysis. Respir. Med. Res. 82, 100931 (2022).
39.
Montes-Andujar L, Tinoco E, Baez-Pravia O et al. Empiric antibiotics for community-acquired pneumonia in adult patients: a systematic review and a network meta-analysis. Thorax 76(10), 1020–1031 (2021).
40.
Kurotschka PK, Bentivegna M, Hulme C, Ebell MH. Identifying the best initial oral antibiotics for adults with community-acquired pneumonia: a network meta-analysis. J. Gen. Intern. Med. 39(7), 1214–1226 (2024).
41.
Choi S-H, Cesar A, Snow TAC, Saleem N, Arulkumaran N, Singer M. Respiratory fluoroquinolone monotherapy vs. β-lactam plus macrolide combination therapy for hospitalized adults with community-acquired pneumonia: a systematic review and meta-analysis of randomized controlled trials. Int. J. Antimicrob. Agents 62(3), 106905 (2023).
42.
Montes-Andujar L, Tinoco E, Baez-Pravia O et al. Empiric antibiotics for community-acquired pneumonia in adult patients: a systematic review and a network meta-analysis. Thorax 76(10), 1020–1031 (2021).
43.
Choi S-H, Cesar A, Snow TAC, Saleem N, Arulkumaran N, Singer M. Efficacy of doxycycline for mild-to-moderate community-acquired pneumonia in adults: a systematic review and meta-analysis of randomized controlled trials. Clin. Infect. Dis. 76(4), 683–691 (2023).
44.
Cillóniz C, Rodríguez-Hurtado D, Torres A. Characteristics and management of community-acquired pneumonia in the era of global aging. Med. Sci. 6(2), 35 (2018).
45.
Chen C, Hsu S, Hsieh H et al. Microbial etiology of pneumonia in patients with decreased renal function. PLoS ONE 14(5), e0216367 (2019).
46.
Cilloniz C, Torres A. Diabetes mellitus and pneumococcal pneumonia. Diagnostics 14(8), 859 (2024).
47.
Yan S, Jing K, Hong Z. Antibiotic resistance profile of Haemophilus influenzae and Moraxella catarrhalis in hospitals across China: data from CHINET Antimicrobial Resistance Surveillance Program from 2005 through 2014. Chin. J. Infect. Chemother. 16(2),153-159 (2016).
48.
Yamba Yamba L, Hansen K, Wasserstrom L, Su Y-C, Ahl J, Riesbeck K. The importance of Haemophilus influenzae in community-acquired pneumonia: an emerging pathogen in the elderly regardless of comorbidities compared to Streptococcus pneumoniae. Pneumonia 16(1), 15 (2024).
49.
U.S. Food and Drug Administration (FDA). NUZYRA (omadacycline) Package Insert. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/209816_209817lbl.pdf
50.
U.S. Food and Drug Administration (FDA). XENLETA (lefamulin) Package Insert. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/211672s000,211673s000lbl.pdf
51.
Cuijpers P, Griffin JW, Furukawa TA. The lack of statistical power of subgroup analyses in meta-analyses: a cautionary note. Epidemiol. Psychiatr. Sci. 30, e78 (2021).
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 17 November 2025
Accepted: 12 February 2026
Published online: 13 March 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Lefamulin versus omadacycline for community acquired bacterial pneumonia: a systematic review and anchored indirect treatment comparison using moxifloxacin as the common comparator. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0188
Export citation
Select the citation format you wish to export for this article or chapter.