Health care resource use in the management of patients with relapsed/refractory diffuse large B-cell lymphoma – Canadian perspective
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Epcoritamab, the first subcutaneous (SC) bispecific approved for relapsed/refractory diffuse large B-cell lymphoma (R/R-DLBCL), offers potential advantages in terms of healthcare resource utilization (HCRU) associated with its SC administration. This study aimed to estimate HCRU and associated costs of R/R-DLBCL treatments, to inform health technology assessment agencies, institutional decision makers and healthcare professionals (HCP) from both a Canadian and Quebec perspective. Secondary objectives included using a societal perspective and estimating chair time and HCP time involved in administering treatments. Materials & methods: A 1-year costing analysis was developed comparing epcoritamab to other R/R-DLBCL treatments, including glofitamab, CAR-T cell therapies, chemotherapy, Pola-BR and Tafa-Len. HCRU and associated costs included pretreatment, administration, monitoring, and adverse event management. Acquisition costs of active treatments were excluded. Multiple time horizons were assessed. Model inputs were retrieved from product labels and validated by clinical experts to reflect practice. Results: From the Canadian and Quebec healthcare system perspective, total 1-year HCRU costs ranged from $11,009 to $54,946 and $10,041 to $54,362, respectively. Epcoritamab ranked as the second least costly comparator after chemotherapy, with notable HCRU savings driven by low administration costs of SC injections and adverse event management costs. Epcoritamab ranked similarly from a societal perspective and scenario analysis evaluating a 2-year time-horizon. Epcoritamab had the lowest annual chair time and HCP time, freeing up resources and HCP availability. Conclusion: Considering the highly constrained Canadian healthcare system, SC epcoritamab offers substantial HCRU-related cost saving, chair time savings and HCP time savings when compared with other available treatments, making it an effective, efficient and patient-centric treatment option for R/R-DLBCL in Canada.
Plain language summary
What is this article about?
Treatments for relapsed/refractory diffuse large B-cell lymphoma (R/R-DLBCL) include a wide array of therapies, each with their own dosing schedules, methods of administration, adverse event rates and monitoring requirements. Epcoritamab, the first subcutaneous (SC) treatment for R/R-DLBCL, has recently received marketing authorization from Health Canada. However, to date, no study has assessed the healthcare resources utilization and associated costs of a novel therapy like epcoritamab versus other R/R-DLBCL treatments. Given the crisis surrounding Canada's healthcare system and workforce, it is imperative to optimize treatment management to alleviate the strain on the healthcare system. Therefore, we performed this research to assess the healthcare resources utilization and associated costs of epcoritamab versus other R/R-DLBCL treatments, to better understand the impact of these treatments on the healthcare system.
What were the results?
From both the Canadian and Quebec healthcare system perspective, epcoritamab was found to be the second least costly treatment option compared with other current and novel treatments for R/R-DLBCL. Epcoritamab was also assessed as the treatment with the least total chair time and healthcare personnel time, due to its SC mode of administration.
What do the results mean?
The healthcare resources saved with SC epcoritamab compared with other treatments in R/R-DLBCL could help alleviate the strain on the Canadian healthcare system. This could allow resources to be redirected to other institutional priorities, and thereby enhance the accessibility and standard of healthcare services provided to Canadian patients.
Diffuse large B-cell lymphoma (DLBCL) is a type of non-Hodgkin’s lymphoma (NHL) [1]. DLBCL is the most common type of aggressive NHL, accounting for approximately 30% of all NHL cases [2]. DLBCL can occur at any age, with the median age of patients being diagnosed around 67 years old [1,3]. At diagnosis, 30–40% of DLBCL cases are localized, while the remaining are diagnosed with widespread disease, involving lymph nodes and other parts of the body [1].
First-line treatment consists of R-CHOP (rituximab in combination with cyclophosphamide, doxorubicin, vincristine and prednisone), a widely used monoclonal antibody and chemotherapy combination. While approximatively 50% of patients with DLBCL treated with R-CHOP may expect to be cured, 30–50% of patients will be resistant or will experience relapse on this treatment [4]. Patients with relapsed/refractory DLBCL (R/R-DLBCL) who are eligible for transplant may receive high-dose chemotherapy and autologous stem cell transplantation. However, chimeric antigen receptor T-cell (CAR-T) therapy has recently replaced autologous stem cell transplantation for transplant eligible patients with primary refractory disease or a relapse within 1 year of first line therapy based on a reduced risk of mortality [5]. Transplant ineligible R/R-DLBCL patients may receive strategies that combine monoclonal antibodies with chemotherapy such as polatuzumab vedotin in combination with bendamustine and rituximab (Pola-BR), tafasitamab in combination with lenalidomide (Tafa-Len) or platinum-based regimen such as or similar to gemcitabine-oxaliplatin plus rituximab (R-GemOX) [4]. Transplant ineligible R/R-DLBCL patients who have received at least two prior lines of systemic therapy may receive the above mentioned therapies, as well as CAR-T therapy (i.e., tisagenlecleucel [tisa-cel], axicabtagene ciloleucel [axi-cel] or lisocabtagene maraleucel [liso-cel]) [4]. Bispecific monoclonal antibodies have now entered the Canadian treatment landscape in DLBCL after at least two prior lines of therapy. Epcoritamab and glofitamab both target CD3 on T-lymphocytes and CD20, a protein found on the surface of certain types of immune system cells, including B cells [6]. Epcoritamab is delivered subcutaneously (SC) until disease progression or intolerance, whereas glofitamab is infused intravenously (IV) for a fixed duration [6–10].
To date, no published Canadian healthcare resources utilization (HCRU) studies in R/R-DLBCL exist to assess the HCRU and associated costs of a novel therapy such as bispecific monoclonal antibodies versus other R/R-DLBCL treatments, each with different dosing schedules, administration routes, adverse event (AEs) rates and monitoring requirements. Furthermore, no previous studies have performed an analysis from the institutional decision maker’s perspective, including the cost of staff time, consumables and facility costs. Given the crisis surrounding Canada’s healthcare system and workforce, largely due to staff shortages caused by burnout, resignations and early retirement, it is imperative to prioritize treatment management and provide support to alleviate the strain on the healthcare system in any feasible way [11,12].
As such, the primary objective of this study was to assess HCRU and estimate associated costs of HCRU of approved R/R-DLBCL treatments for patients who are transplant ineligible and have received at least two prior lines of systemic therapy, to inform Canadian institutional decision makers, health technology agencies (CADTH and INESSS) and healthcare professionals. Of note, this study is a follow-up of a previously published USA model comparing costs of epcoritamab with many potential comparators in the management of patients with R/R-DLBCL after two or more lines of therapy and represents an adaptation of the model to a Canadian and Quebec healthcare system perspective [13]. Secondary objectives included estimating HCRU and associated costs of R/R-DLBCL treatments using a societal perspective and estimating the time required to receive and administer R/R-DLBCL treatments, from a patient and institution perspective.
Materials & methods
Patient population
Comparative treatments
Epcoritamab was compared with treatments approved by Health Canada for the treatment of patients with transplant ineligible R/R-DLBCL, who have received at least two prior lines of systemic therapy. If treatments have received a negative recommendation from CADTH or INESSS, they were excluded as potential comparators, within their respective perspective. The comparators are specific for the Canadian (Ontario) and Quebec healthcare systems perspectives. The Canadian comparators include:
Note that tafasitamab received a negative recommendation from CADTH in October 2022, and pCPA negotiations were not pursued. Therefore, it was not considered as a comparator from a Canadian perspective [19].
Quebec comparators were the same, with the exception that Tafa-Len which has received a positive INESSS recommendation [20] and was therefore included, while Pola-BR has received a negative recommendation from INESSS in May 2021, and was consequently not considered as a comparator from a Quebec perspective [21].
Perspective
The costing study provided cost estimates from the healthcare system and societal perspectives, for both the Canadian and Quebec perspectives. The healthcare system perspective included direct medical costs only while the societal perspective included direct and indirect cost (patient and caregiver lost productivity and patient out-of-pocket costs).
Time horizon
The base-case model was based on a 1-year time horizon, in order to capture all essential HCRU and associated costs. The model also allowed for different time horizons including first 30 days, 6 months and 2 years. A scenario analysis was also included using the median treatment duration of each comparator for the time horizon. The choice of these time horizons was deliberate, aiming to evaluate how costs were influenced with varying timeframes. For instance, for CAR-T cell therapies, most of the costs occur in the first month of treatment, while for epcoritamab, a 2-year time-horizon would allow to capture a fuller extent of HCRU and associated costs, accounting for different durations on treatment. In fact, the median treatment duration of epcoritamab was reported as 5 cycles of 28 days (equivalent to 4.6 months) in the EPCORE-NHL-1 trial, with approximately 13.4% of DLBCL patients still on treatment at 26 cycles (2 years) [6].
HCRU & associated costs
The values of the costing study were obtained from multiple sources, specific for the Canadian and Quebec healthcare system perspectives. When available, HCRU information was retrieved first from the treatment product monograph. If not available, the most recent data from literature (including follow-up studies) was used instead. Note that additional parameters were considered based on Canadian practice and validation conducted by clinical experts. One clinical expert in Ontario and one in Quebec were selected to review model inputs and results for clinical validity. Of note, costs were adjusted to 2023 Canadian dollars, using all items Consumer Price Index for Statistics Canada [22].
Pretreatment/premedications
Pretreatment and premedications were established for each comparator. Information was retrieved from product monographs (when available), Cancer Care Ontario (CCO) regimens or clinical trials, as appropriate. Required pretreatment and premedications for each comparator are presented in supplementary material, Supplementary Table 1.
CAR-T therapy associated costs
CAR T-cell therapies require leukapheresis, cryopreservation, bridging therapy as well as lymphodepleting therapy. All patients in the tisa-cel arm were assumed to incur the cost of leukapheresis and cryopreservation procedures. Cryopreservation was not required for axi-cel and liso-cel as they are manufactured using fresh apheresis products [23]. Unit costs of cryopreservation and leukapheresis are presented in Table 1.
| Cost parameters | Canadian input | Quebec input | Reference | Ref. |
|---|---|---|---|---|
| CAR-T therapy associated costs | ||||
| Leukapheresis | $2759.00 | $1423.10 | CADTH Axi-cel DLBCL Report; INESSS (Quebec) DLBCL HTA recommendation | [16,57] |
| Cryopreservation | $279.45 | $281.38 | ||
| Weighted average cost of bridging therapy | $12,811 | $12,881 | See Supplementary Material Table 2 | |
| Outpatient drug administration unit costs | ||||
| CAR-T therapies: physician fee (per visit) | $105.15 | $266.95 | Ministry of Health of Ontario. Schedule of Benefits. Code G359; Manuel des médecins spécialistes. Code 16054 | [24,25] |
| Injectable chemotherapy: physician fee (per visit) | $75.00 | $22.25 | Ministry of Health of Ontario. Schedule of Benefits. Code G345; Manuel des médecins spécialistes. Code 00734 | [24,25] |
| Subcutaneous: physician fee – subcutaneous (per visit) | $3.89 | $0.00 | Ministry of Health of Ontario. Schedule of Benefits. Code G372; RAMQ does not pay for this fee | [24] |
| Nurse average wage (per min) | $0.67 | $0.62 | Government of Canada, Job Bank (NOC 31301)]; Statistics Canada, Table 14-10-0043-01 | [26,27] |
| Pharmacist average wage (per min) | $0.89 | $0.97 | Government of Canada, Job Bank (NOC 31120); Statistics Canada, Table 14-10-0043-01 | [26] |
| Infusion chair time (per min) | $0.90 | $0.89 | Pettigrew (2016) | [28] |
| Inpatient administration costs | ||||
| Hospitalization | $1397.54 | $1395.25 | CIHI, 2016 | [58] |
| ICU | $4422.86 | $4415.64 | CIHI, 2016 | [58] |
| Professional fee costs inputs | ||||
| Consultation visit Initial Repeat | $166.50 $105.25 | $239.85 $56.85 | Schedule of Benefit for physician services, code A445 (initial), code A446 (repeat); Manuel des Médecins spécialistes, code 09160 (initial), 19152 (repeat) | [24,25] |
| Nurse follow-up call | – | $18.60 | Government of Canada, Job Bank (NOC 31301); Assuming 30 min per follow-up call | [27] |
| CT scan | $303.20 | $154.20 | Schedule of Benefits for physician services, code X125, X126, X233; Manuel des services de laboratoire en établissement, code 08262, code 08268 | [24,25] |
| PET scan | $255.20 | $136.70 | Schedule of Benefit for physician services, code J705]; Manuel des services de laboratoire en établissement, Code 08778 | [24,25] |
| Workforce inputs | ||||
| Average hourly wage, $/hour | $31.96 | $30.96 | Statistics Canada | [29] |
| Average usual hours worked per day, hours | 7.56 | 7.44 | Statistics Canada | [30] |
| Average employment rate for caregivers, % | 62.1% | 62.3% | Statistics Canada | [59] |
| Out-of-pocket costs | $217.85 | $181.58 | See Supplementary Material Table 17 | |
Axi-cel: Axicabtagene ciloleucel; CADTH: Canadian Agency for Drugs and Technologies in Health; CAR-T: Chimeric antigen receptor T-cell; CT: Computed tomography; CIHI: Canadian Institute for Health Information; DLBCL: Diffuse large B-cell lymphoma; ICU: Intensive care unit; INESSS: Institut national en santé et services sociaux; PET: Positron emission tomography; RAMQ: Regie de assurance maladie du Quebec.
Bridging chemotherapy is administered to stabilize the disease while waiting for CAR-T manufacturing. In line with CADTH report of axi-cel as well as clinical expert input, the proportion of patients requiring bridging therapy was assumed equal for all CAR-T therapies [31]. Based on clinical expert input, for both the Canadian and Quebec perspectives, 75% of patients of all CAR-T therapies were assumed to receive bridging therapy. The cost of bridging therapy was based on a basket of treatments defined by clinical experts, as detailed in the supplementary material, Supplementary Table 2.
Lymphodepleting treatment is administered to facilitate the activity and the expansion of CAR-T cells. Based on clinical expert input, 75% of patients are assumed to receive lymphodepleting therapy for all CAR-T cell therapies in Canada and 100% of patients in Quebec, considering that some patients cannot safely tolerate the standard lymphodepleting regimen. Lymphodepleting therapy was assumed to be fludarabine and cyclophosphamide for all CART-T cells, with specific regimens for each treatment in line with respective clinical trials [32–35].
Costs of all medications required for pretreatment (including bridging therapy and lymphodepleting therapy) were retrieved from the Ontario Drug Benefit Formulary for the Canadian perspective, and from the Régie de l'assurance maladie du Quebec (RAMQ) from the Quebec perspective (Supplementary Table 3) [36,37]. When not available from provincial formularies, IQVIA Delta PA was used instead [38]. Of note, price estimates were used for treatments that have not yet received reimbursement from provincial drug plans.
Drug administration resource use
For oral therapies, no administration costs were considered. For injectable regimens, costs were differentiated for outpatient and inpatient administration.
Outpatient administration costs
Administration costs in an outpatient setting consisted of delivery costs (i.e., physician fee), nursing workload costs, pharmacy workload costs and infusion chair time costs. Table 1 shows the unit costs of drug delivery (per visit), nursing workload (per min), pharmacy workload (per min) and infusion chair time (per min) [24–28]. The durations in minutes were estimated based on infusion time in the Mayo Clinic CAR-T Cell Therapy Program for CAR-T therapies, from the monographs published by CCO as well as clinical experts’ input, where applicable (Supplementary Table 4) [10,39–42].
Inpatient administration costs
Administration costs in an inpatient setting consisted of infusion/treatment-related hospitalization and intensive care unit admission, for each comparator. Unit cost for hospitalization and intensive care unit are presented in Table 1 [43]. The proportion of patients requiring hospitalization and ICU for each treatment, along with length of stay, were based on literature and clinical experts' input (Supplementary Table 5).
Follow-up & monitoring costs
Routine follow-up and monitoring frequencies, including consultation visits, nurse call follow-ups, CT scans, positron emission tomography (PET) scans and laboratory tests per treatment, were derived from individual treatment product monographs as well as CCO regimens and validated by clinical experts [44]. Unit costs of these medical services are presented in Table 1 (unit cost of laboratory tests in Supplementary Table 10), while the frequency per treatment cycle, are presented in the supplementary material (Supplementary Tables 6–9).
Management of adverse events
The frequency of AEs for each treatment regimen was retrieved from their respective clinical trials or product monograph. Only grades 3 and 4 AEs in at least 5% of patients were considered, as reported in Supplementary Table 11 [10,32–34,45–47]. Considering the severity of immune effector cell-associated neurotoxicity syndrome (ICANS), all grade AEs were retrieved (includes all neurological events). The proportion of AEs managed inpatient or outpatient was validated by clinical experts and unit costs per event are presented in Supplementary Table 12 [43,48].
In addition, the study separately modelled the costs associated with all grade cytokine release syndrome as it could be associated with substantial resource use. The unit cost per dose as well as administration costs of tocilizumab are presented in Supplementary Table 13, while the frequency of all-grade cytokine release syndrome and utilization of tocilizumab are presented in Supplementary Table 14 [38,49,50].
Costs of productivity impairment
For the societal perspective analysis, productivity impairment for patients and caregivers as well as out-of-pocket costs were considered. For both patients and caregivers, data on employment and salaries was retrieved from Statistics Canada (Table 1) [29,30].
Productivity impairment for patients
Productivity impairment for Canadian patients was calculated considering the average employment rate for patients with DLBCL and the percentage of work impairment during treatment administration (Supplementary Table 15), as well as the time during treatment with work impairment, over the specified time horizon of the model. The estimation of work impairment during treatment for patients was established based on the following assumptions, validated with clinical experts:
•
Epcoritamab: Assuming 2 full days off work for the first full injection (hospitalization), followed by a full day of work lost for every other injection.
•
Glofitamab: Assuming 1 day lost for pretreatment with obinutuzumab, 2 full days off work for first injection (hospitalization), followed by a full day of work lost for every injection.
•
CAR-T cells: Assuming time lost equivalent to 1 month prior and 1 month following CAR-T cell injection.
•
Tafa-Len: Assuming one full day of work lost per injection.
•
Chemotherapy & Pola-BR: Assuming patients receiving chemotherapy will not be able to work over the entire treatment duration [51].
Productivity impairment for caregivers
Productivity impairment for caregivers was calculated considering the proportion of patients requiring caregiver assistance, the proportion of unpaid assistance from a partner/relative/friend, the average time missed off work and the average employment rate for caregivers. Summary of inputs related to productivity impairment for caregivers are presented in Supplementary Table 16.
Out-of-pocket costs
Out-of-pocket costs included travelling costs, parking costs as well as the cost of accommodation and meal expenses for patients residing in rural areas. Total out-of-pocket costs (Table 1) was calculated based on the average number of infusion visits over the selected time horizon. Summary of inputs related to out-of-pocket costs are presented in Supplementary Table 17.
Results
Base-case results
Total annual costs – Canada
Healthcare system perspective
Over a 1-year time horizon, total annual costs of HCRU (excluding drug costs) of R/R-DLBCL treatments for patients who are transplant ineligible and have received at least two prior lines of systemic therapy ranged from $11,009 to $54,946, with CAR-T cell therapies representing the most resource-intensive treatments (Figure 1A & Supplementary Table 19). Overall, epcoritamab was the second least costly ($13,941) comparator, after R-GemOX. Additionally, epcoritamab was considered the most cost-saving option, based on costs related to SC administration (savings of $1725 to $19,410) and AEs management (savings of $230 to $14,887) (Supplementary Table 20). In terms of monitoring costs, epcoritamab is slightly more expensive than other comparators, considering it is administered until disease progression or unacceptable toxicity. Overall, epcoritamab incurred savings versus CAR-T cell therapies (-63% to -75%), followed by glofitamab (-38%) and Pola-BR (-18%), while being costlier than R-GemOX (27%).
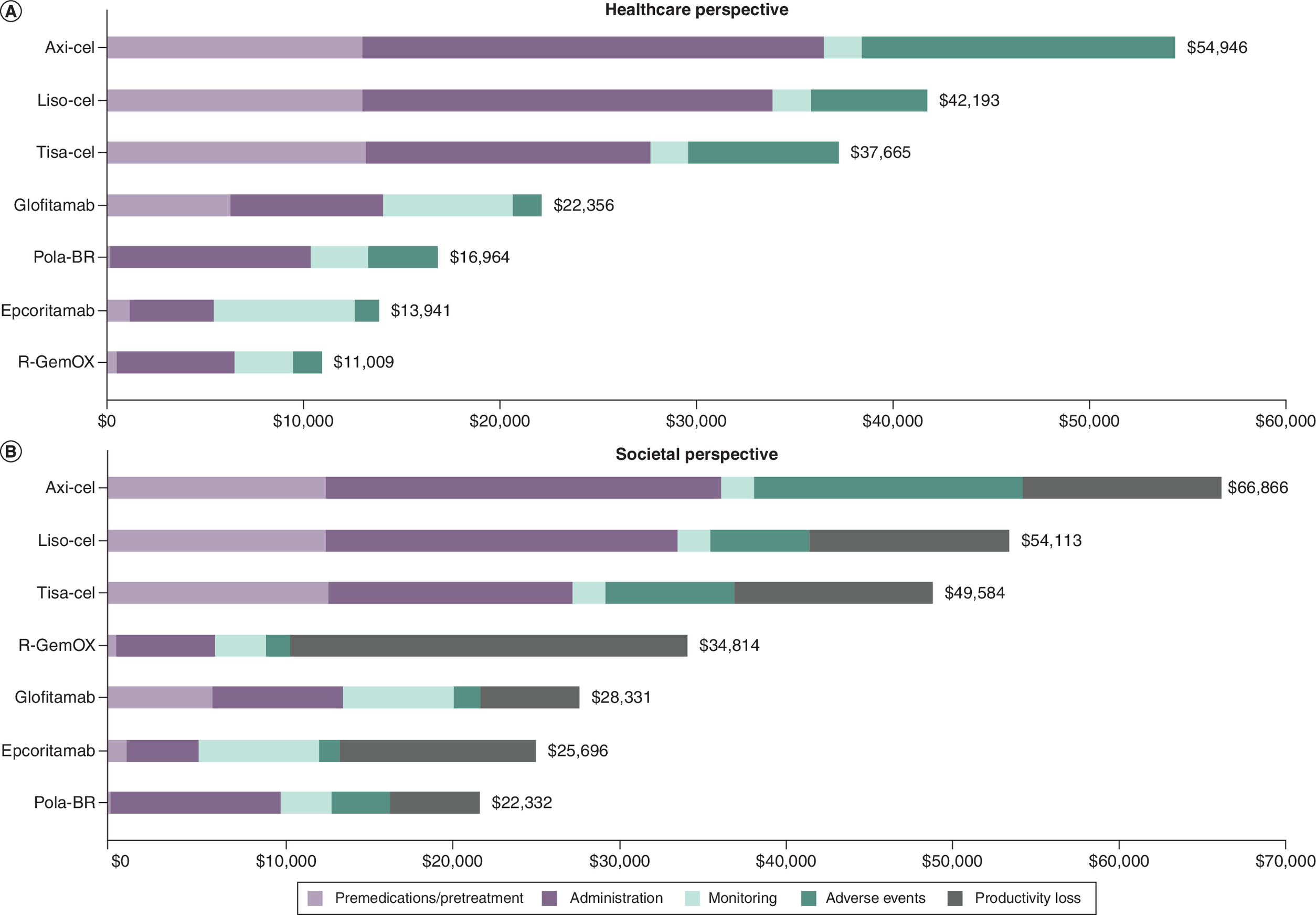
Figure 1. Total healthcare resource utilization costs for Canada.
(A) Total costs of healthcare resource utilization from a Canadian healthcare system perspective, including the cost of premedications, administration, monitoring and adverse events. (B) Total costs of healthcare resource utilization from a Canadian societal perspective, including premedications, administration, monitoring, adverse events as well as productivity loss.
Axi-Cel: Axicabtagene ciloleucel; CAR-T: Chimeric antigen receptor T-cell; Liso-Cel: Lisocabtagene maraleucel; Pola-BR: Polatuzumab vedotin in combination with bendamustine and rituximab; R-GemOX: Gemcitabine-oxaliplatin plus rituximab; Tisa-Cel: Tisagenlecleucel.
Societal perspective
Similar results were obtained from the Canadian societal system perspective, as each cost category was identical to the healthcare system perspective, but in addition to costs related to productivity impairment for each comparator. Costs of productivity impairment for R-GemOX were the highest with a total of $23,804, followed by CAR-T cell therapies ($11,920) and epcoritamab ($11,756). The total and incremental costs related to productivity impairment are presented in Supplementary Tables 19 & S20, respectively. Similar to the Canadian healthcare perspective, epcoritamab ranked the second least costly comparator in terms of HCRU to treat patients with R/R-DLBCL, after Pola-BR, as presented in Figure 1B.
Productivity impairment is slightly higher for epcoritamab than for glofitamab due to a greater number of administrations over the treatment course (29 vs 15). This reflects continuous dosing until disease progression or unacceptable toxicity for epcoritamab, compared with a fixed 12-cycle regimen for glofitamab. Despite higher productivity loss associated with epcoritamab, total annual HCRU costs from a societal perspective are lower than those of glofitamab. Glofitamab incurs higher HCRU costs due to the time and resource requirements associated with IV administration. As shown in Supplementary Table 4, glofitamab requires substantially more nurse time (64 vs 10 min), pharmacist time (28 vs 5 min) and chair time (120 vs 30 min) compared with epcoritamab. In addition, IV administration is associated with higher physician fees and increased management of infusion-related reactions. Overall, the lower HCRU costs observed with epcoritamab offset the higher productivity loss costs compared with glofitamab, from a societal perspective.
Total annual costs – Quebec
Healthcare system perspective
Total annual costs of HCRU from the Quebec healthcare system perspective resembled the Canadian situation: epcoritamab was the second least costly ($10,500) comparator, again after R-GemOX. In Quebec, the total annual costs of HCRU of R/R-DLBCL treatments ranged from $10,041 to $54,362, with CAR-T cell therapies representing once more the most resource-intensive treatments (Figure 2A & Supplementary Table 19). When compared with all other treatment options, epcoritamab was considered the most cost-saving option in every treatment cost category, excepted for monitoring (i.e., epcoritamab slightly more expensive than other comparators) and premedications (only R-GemOX was less costly), as shown in Supplementary Table 20. Overall, epcoritamab incurred savings versus CAR-T cell therapies (-72% to -81%), glofitamab (-43%) and Tafa-Len (-29%), while being more slightly costlier than R-GemOX (5%).
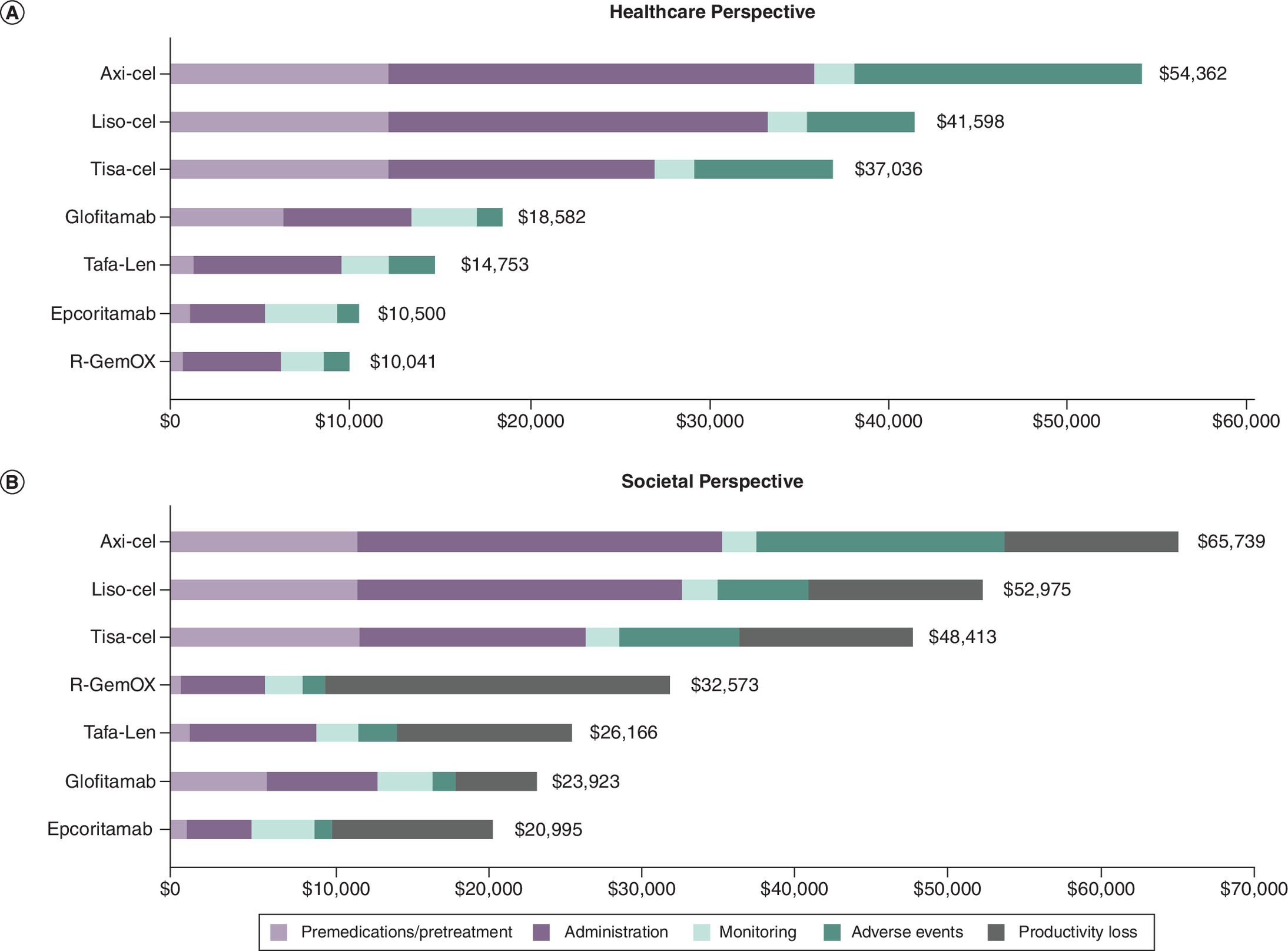
Figure 2. Total healthcare resource utilization costs for Quebec.
(A) Total costs of healthcare resource utilization from a Quebec healthcare system perspective, including the cost of premedications, administration, monitoring and adverse events. (B) Total costs of healthcare resource utilization from a Quebec societal perspective, including premedications, administration, monitoring, adverse events as well as productivity loss.
Axi-Cel: Axicabtagene ciloleucel; CAR-T: Chimeric antigen receptor T-cell; Liso-Cel: Lisocabtagene maraleucel; R-GemOX: Gemcitabine-oxaliplatin plus rituximab; Tafa-Len: Tafasitamab in combination with lenalidomide; Tisa-Cel: Tisagenlecleucel.
Societal perspective
From a societal perspective, total annual costs of HCRU ranged from $20,995 to $65,739, with epcoritamab being the least costly ($20,995) comparator (Figure 2B), reducing total costs between 12 and 68% compared with all other R/R-DLBCL treatments available in Quebec (Supplementary Table 20).
Chair time & HCP time per patient
The present study set out to estimate the time required to receive and administer current and novel R/R-DLBCL treatments, from a patient and institutional perspective. Over a 1-year period, the total infusion chair time plus healthcare professional (HCP; including nurse and pharmacist) time associated to each comparator ranged from 1215 to 7781 min (Figure 3). Epcoritamab represented the comparator associated with the least total chair time and HCP time combined (1215 min), as depicted in the Figure 3. For each comparator regimen, chair time contributed the most to total time spent per patient. Notably, as a SC treatment, epcoritamab was the comparator associated with the least total chair time (810 min). Results revealed that for every 100 hypothetical patients treated with epcoritamab, epcoritamab could potentially free up capacity to treat between 90 and 589 more patients (Table 2). Results were similar from a Quebec perspective.
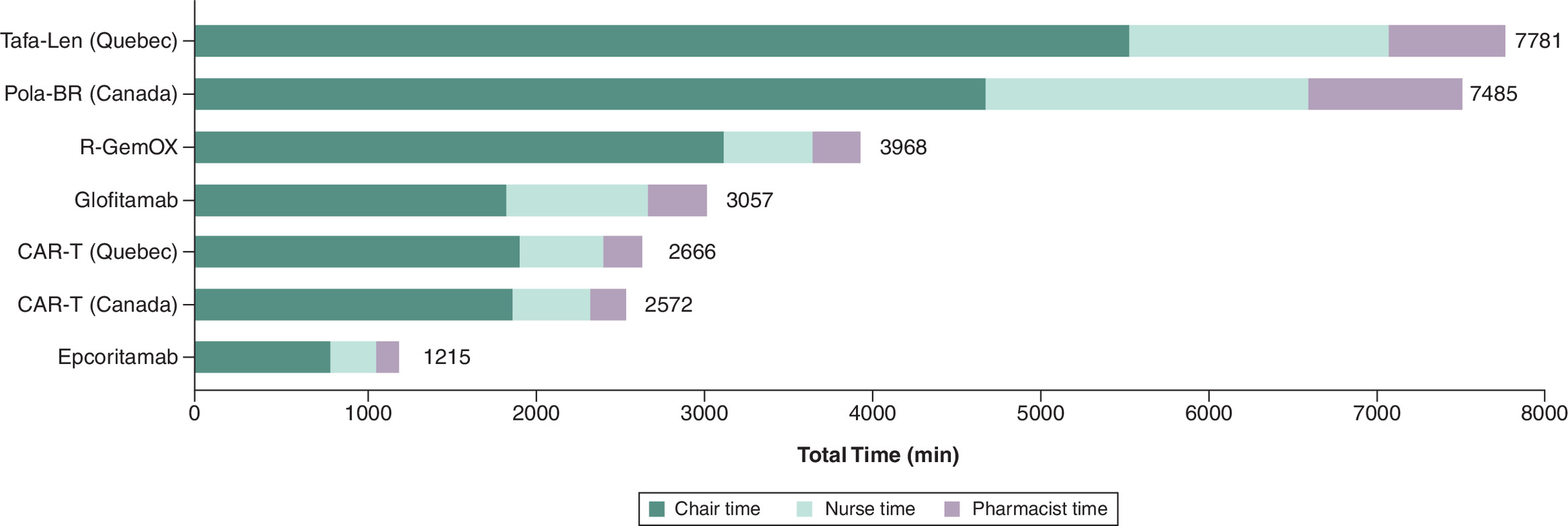
Figure 3. Total chair and healthcare personnel time.
(A) Total time based on chair time as well as healthcare personnel time, including nurse, pharmacist, from the Canadian perspective. (B) Total time based on chair time as well as healthcare personnel time, including nurse, pharmacist, from the Quebec perspective.
Axi-Cel: Axicabtagene ciloleucel; CAR-T: Chimeric antigen receptor T-cell; Liso-Cel: Lisocabtagene maraleucel; Pola-BR: Polatuzumab vedotin in combination with bendamustine and rituximab; R-GemOX: Gemcitabine-oxaliplatin plus rituximab; Tafa-Len: Tafasitamab in combination with lenalidomide; Tisa-Cel: Tisagenlecleucel.
| Comparator | Total chair time (min) | Incremental time (min) | Increased patient capacity per 100 hypothetical patients treated† |
|---|---|---|---|
| Epcoritamab | 810 | Reference | Reference |
| Glofitamab | 1860 | 1050 | 130 |
| CAR-T (Canada) | 1536 | 726 | 90 |
| CAR-T (Quebec) | 1581 | 771 | 95 |
| Pola-BR (Canada) | 4725 | 3915 | 483 |
| R-GemOX | 3165 | 2355 | 291 |
| Tafa-Len (Quebec) | 5580 | 4770 | 589 |
†
Calculated by multiplying the incremental time per patient by 100, and dividing by the estimated chair time per patient of epcoritamab.
CAR-T: Chimeric antigen receptor T-cell; Pola-BR: Polatuzumab vedotin + bendamustine + rituximab; R-GemOX: Rituximab + Gemcitabine + Oxaliplatin; Tafa-Len: Tafasitamab + lenalidomide.
Patient time saved based on productivity impairment
According to Prica (2021), the average employment rate for patients with R/R-DLBCL is estimated at 66% [52]. Therefore, it is important to note that not all R/R-DLBCL patients will experience work-related productivity impairment, considering a substantial number of patients are already retired at diagnosis. Specifically, for employed patients, the total treatment-associated annual productivity impairment (in days) per patient was estimated to be the highest for R-GemOx (112 days), followed by CAR-T cells (60 days), Tafa-Len (31 days), epcoritamab (29 days), glofitamab (15 days) and Pola-BR (13 days). The productivity impairment of epcoritamab is slightly higher than glofitamab due to the higher number of treatment administrations, considering epcoritamab is administered until disease progression or unacceptable toxicity while glofitamab is administered for 12 cycles of 21 days. However, despite the higher number of administrations, the total annual costs of HCRU from a societal perspective remain less expensive for epcoritamab compared with glofitamab, mostly because of the long administration time and resources required to administer IV glofitamab compared with SC epcoritamab. It is also noteworthy to mention that a conservative assumption was used to calculate productivity impairment, assuming one full day of work lost per administration, for both epcoritamab and glofitamab. Considering that the chair time of epcoritamab was estimated at 30 min due to its SC injection and glofitamab at 240 min, aligned with its product monograph for IV infusion, patients spend shorter time periods in outpatient clinics per administration with epcoritamab compared with glofitamab, which increases patient convenience and allows additional time from their day off work to rest and attend to their personal needs [53–55].
Sensitivity analyses
Time horizon
As differences exist in treatment duration between the comparators (e.g., some use a fixed set of cycles, others, like epcoritamab, are prescribed until disease progression), sensitivity analyses were conducted to model different time horizons (i.e., first 30 days, 6 months, 1-year, 2-years and median treatment duration [Supplementary Table 18]). Supplementary Table 22 presents the disaggregated results by comparator for all available time horizons and perspectives, while Supplementary Table 23 reflects the diverse rankings of epcoritamab versus its comparators based on total HCRU costs. From a Canadian perspective, epcoritamab ranked as the least and second least resource-intensive comparator in 30% and 60% of cases, respectively. From a Quebec perspective, epcoritamab ranked as the least and second least resource-intensive comparator in 40% and 40% of cases, respectively.
Subcutaneous rituximab
According to clinical experts, some Canadian provinces could be using rituximab SC instead of rituximab IV for Pola-BR and R-GemOx regimens. Therefore, a sensitivity analysis using rituximab SC was conducted. Total costs over a 1-year time-horizon were similar to the base-case Canadian and Quebec healthcare system perspectives, with each comparator obtaining the same ranking (Supplementary Table 19).
Excluding first dose hospitalization for epcoritamab & glofitamab
Despite monitoring in hospital for the first dose of epcoritamab and glofitamab was reported in their respective clinical trials, this might not be reflective of clinical reality and is not indicated within their product monographs [6–10]. For this reason, a sensitivity analysis was conducted to exclude the assumption of hospitalization upon first dose administration. Total costs over a 1-year time-horizon were similar to the base-case Canadian and Quebec healthcare system perspectives, with each comparator obtaining similar ranking (Supplementary Table 24).
Discussion
To our knowledge, this is the first study to estimate HCRU and the associated costs for the management of R/R-DLBCL from both the Canadian and Quebec healthcare system and societal perspectives. This study included current and novel treatments, including options that will be relevant to the evolving treatment landscape. Epcoritamab demonstrated compelling results in the treatment of patients with R/R-DLBCL who are transplant ineligible and have received at least two prior lines of systemic therapy. When analyzed from a Canadian and Quebec healthcare system perspective, SC epcoritamab required less HCRU and was also associated with lower total annual costs of HCRU compared with all novel therapies with the exception of chemotherapy.
Epcoritamab is the only R/R-DLBCL treatment solely available as a SC injection. As such, this study investigated if the mode of administration of epcoritamab had a positive effect on the time required to receive and administer this treatment. Although the treatment is given until disease progression or intolerance, epcoritamab was the comparator associated with the least total chair time. Taken together, this illustrates epcoritamab's ability to reduce the consumption of resources, including staff time (i.e., nurse and pharmacist) and chair time, and improving the institutional practice efficiency, despite its increased dosing frequency. Considering the constraints and limited capacity of the healthcare system in Canada, specifically with regards to shortages of hospital staff [56], the resources saved with the use of epcoritamab could allow redirecting resources to other institutional priorities, thereby enhancing the accessibility and standard of healthcare services provided to patients. Additionally, by facilitating the treatment process, epcoritamab enhances the convenience for patients.
To acknowledge the differences in treatment duration between the comparators, sensitivity analyses were conducted to model different time horizons (i.e., first 30 days, 6 months, 1-year, 2-year and median treatment duration), for both the Canadian and Quebec healthcare and societal perspectives. For example, according to a 2-year time horizon, patients treated with epcoritamab would continue their treatment throughout the entire time period, while patients treated with glofitamab would only receive treatment for 12 cycles (33 weeks). Results of these analyses demonstrated that from Canadian and Quebec perspectives, epcoritamab ranked as the second and third least costly comparator from a healthcare and societal perspective, respectively, over a 2-year time horizon. The 2-year time horizon is a conservative analysis, considering that the majority of patients are no longer on epcoritamab treatment at the 2-year mark (only 13.4 % of DLBCL patients on treatment at 26 cycles [2 years]), with an estimated mean treatment duration of 5 cycles of 28 days reported in the EPCORE-NHL-1 trial [6].
Additionally, considering possible institutional variations in step-up dosing hospitalization requirements for epcoritamab and glofitamab, a sensitivity analysis excluding hospitalization for the first dose was performed. While the relative ranking of comparators remained consistent with the base-case analysis, total HCRU costs were reduced. Excluding first dose hospitalization decreased total HCRU costs by $1356 for epcoritamab and $1036 for glofitamab from a Canadian healthcare system perspective. Additional reductions in HCRU costs were observed from a Canadian societal perspective, with similar results from a Quebec perspective. Although the cost difference between epcoritamab and glofitamab remained comparable, these findings demonstrate that eliminating step up dosing hospitalization further reduces HCRU costs and associated burden on the healthcare system.
This study represents a valuable addition to the field of HCRU for the management of R/R-DLBCL in Canada. Strengths of this study included validation of study inputs by Canadian clinical experts and the conduct of robust scenario analyses to verify the core assumptions. The study also included drugs approved for R/R DLBCL in Canada, regardless of funding status to allow for a comprehensive comparison of HCRU costs reflected in clinical practice. It is also crucial to acknowledge that certain limitations may impact the accuracy and applicability of the results. First, the model incorporated treatments that have not yet received reimbursement from provincial drug plans, and assumptions regarding their use were largely informed by clinical expert opinion. Consequently, real-world utilization patterns may differ once these therapies become publicly funded. Also, for the Canadian perspective, cost inputs were primarily derived from Ontario-based and may not capture regional variation across Canada in areas such as travel subsidies, workforce compensation, home care delivery models, resource availability and provincial reimbursement policies, thereby limiting national generalizability. Applicability to other healthcare systems (e.g., USA and Europe) and care settings (community vs academic) may also be limited. In addition, this study focused solely on assessing HCRU costs and did not incorporate differences in PFS or OS. Accordingly, HCRU costs should not be interpreted as indicative of improved survival outcomes or quality of life, which remain key considerations in treatment decision-making. Drug acquisition costs were also excluded from this analysis to allow for a more detailed assessment of administration- and management-related resource use, which may limit the relevance of results for stakeholders seeking a comprehensive evaluation of total treatment costs. Furthermore, it is also important to emphasize that this study primarily serves a descriptive purpose. While it provides valuable insights into the economic aspects of the healthcare interventions, some of the assumptions and cost scenarios established may not be applicable to all patients. The variability in patient characteristics, treatment responses (including rates of AEs based on limited follow-up data from clinical trials), and healthcare settings may limit the generalizability of the findings in a real-world setting. The rapidly changing therapeutic and workflow landscape for bispecific antibodies in Canada may further affect the future applicability of the model assumptions. For example, recently emerging therapies, such as glofitamab in combination with GemOx, were not included, as they were not available at the time this study was conducted. Finally, this analysis was restricted to a single line of therapy and did not account for costs associated with disease progression or subsequent lines of treatment over extended time horizons. Future studies evaluating 3-, 5- and 10-year time horizons could help to further characterize the full lifetime HCRU and associated economic burden for R/R-DLBCL.
Conclusion
In summary, epcoritamab not only offers valuable HCRU-related cost savings but also substantial time savings when compared with available treatments described in this study, making it an effective, efficient and patient-centric treatment option for R/R-DLBCL in Canada. Additionally, in contrast to other IV treatment alternatives, epcoritamab, as a SC injection, allows to facilitate the treatment process and enhance convenience for patients.
Summary points
•
Epcoritamab is the first subcutaneous (SC) bispecific monoclonal antibody approved by Health Canada for relapsed/refractory diffuse large B-cell lymphoma (R/R-DLBCL), after two or more lines of systemic therapy and in patients who have previously received or are unable to receive CAR-T cell therapy and are transplant ineligible.
•
This study estimated the healthcare resource utilization (HCRU) and associated costs of current and novel R/R-DLBCL treatments for patients who are transplant ineligible and have received at least two prior lines of systemic therapy, using a Canadian and Quebec healthcare system perspective.
•
HCRU and associated costs included pretreatment, drug administration, follow-up and monitoring, adverse event management as well as productivity impairment from a societal perspective.
•
From a Canadian healthcare system perspective, epcoritamab was found to be the second least costly comparator after chemotherapy and the second least costly after Pola-BR from a societal perspective.
•
From a Quebec healthcare system perspective, epcoritamab was found to be the second least costly comparator after chemotherapy and the least costly comparator from a societal perspective.
•
Epcoritamab is the comparator with least total chair time and healthcare personnel time combined.
•
The SC administration of epcoritamab enables notable savings in terms of HCRU and HCRU related costs.
•
Considering the highly constrained Canadian healthcare system, epcoritamab offers substantial HCRU savings and related cost savings making it an attractive, efficient and patient-centric treatment option for R/R-DLBCL.
Author contributions
Author K Guinan was responsible for study conception and design, acquisition of data, data analysis and drafting and revision of the manuscript. Authors M Ham and M Pelletier were responsible for study conception and design, acquisition of data and data analysis. Authors J Lachaine, D Tankala, NP Roc, S Barakat, A Klil-Drori and AW Wang were responsible for study conception and design, project coordination and reviewing the manuscript. Authors I Fleury and D MacDonald were responsible for study conception and design, data analysis and reviewing the manuscript.
Acknowledgments
The authors thank Willemieke Kouwenhoven for revising the manuscript.
Financial disclosure
This study was funded by AbbVie Corporation, H4S 1Z1, Canada.
Competing interests disclosure
K Guinan is an employee of PeriPharm Inc. and J Lachaine is a partner at PeriPharm Inc., a company that has served as a consultant to AbbVie and has received funding from AbbVie. M Pelletier and M Ham were employees of PeriPharm Inc. at the time this study was developed. D Tankala, NP Roc, S Barakat and AW Wang are employees of AbbVie Corporation. Employees of AbbVie may hold equity. A Klil-Drori was an employee of AbbVie Corporation at the time this study was developed and may hold equity. I Fleury and D MacDonald received an honorarium from AbbVie. No honoraria or payments were made for authorship. D MacDonald has received consultancy fees from Abbvie, Astra Zeneca, Beigene/BeOne, Eli Lilly, Kite/Gilead, Pfizer and Roche. I Fleury has received consultancy fees from Abbvie, Astrazeneca, Beigene, BMS, Gilead, Incyte, Kyowa Kirin, Lilly, Pfizer, Roche as well as speaker fees from Abbvie, Astrazeneca, Beigene, Gilead, Incyte, Lilly, Pfizer and Roche. J Lachaine received research funding from AbbVie, Pfizer, Merck, Duchesnay, Novartis and Idorsia. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Willemieke Kouwenhoven received funding from PeriPharm Inc.
Ethical conduct of research
This study did not involve human participants or animal experiments, and all research procedures adhered to recognized ethical standards for scientific integrity and responsible research conduct.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 212.63 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Canadian Cancer Society. Diffuse large B-cell lymphoma 2023. https://cancer.ca/en/cancer-information/cancer-types/non-hodgkin-lymphoma/what-is-non-hodgkin-lymphoma/diffuse-large-b-cell-lymphoma
2.
Lymphoma Canada. Diffuse large B cell lymphoma (DLBCL) 2023. https://www.lymphoma.ca/diffuse-large-b-cell-lymphoma/
• Provides information on the guidelines for treatment of patients with relapsed/refractory diffuse large B-cell lymphoma (R/R-DLBCL) in various provinces of Canada, such as what type of chemotherapy treatment to use and which patients are eligible for a cell transplant.
3.
Sapkota SSH. Non-Hodgkin lymphoma 2023. (updated 24 February 2023). https://www.ncbi.nlm.nih.gov/books/NBK559328/#:∼:text=Overall%2C%20Non%2DHodgkin%20lymphoma%20is,median%20age%20being%2067%20years
4.
Lymphoma Canada. Canadian evidence-based guidelines for the treatment of relapsed/refractory diffuse large B-cell lymphoma 2023. https://z9a2f9c2.rocketcdn.me/wp-content/uploads/2021/09/LymphomaCanada_Guideline_Relapsed_Refractory_DLBCL_VF_Digital.pdf
5.
Westin JR, Oluwole OO, Kersten MJ et al. Survival with axicabtagene ciloleucel in large B-cell lymphoma. N. Engl. J. Med. 389(2), 148–157 (2023).
6.
Thieblemont C, Karimi YH, Ghesquieres H et al. Epcoritamab in relapsed/refractory large B-cell lymphoma: 2-year follow-up from the pivotal EPCORE NHL-1 trial. Leukemia 38(12), 2653–2662 (2024).
•• Evaluates the response rate of adults with relapsed or refractory CD20+ large B-cell lymphoma treated with epcoritamab.
7.
Falchi L, Carlo-Stella C, Morschhauser F et al. Glofitamab monotherapy in pts with relapsed/refractory (R/R) large B-cell lymphoma (LBCL): extended follow-up and landmark analyses from a pivotal Phase II study. J. Clin. Oncol. 41(Suppl. 16), Abstract 7550 (2023).
8.
Dickinson MJ, Carlo-Stella C, Morschhauser F et al. Glofitamab for relapsed or refractory diffuse large B-Cell Lymphoma. N. Engl. J. Med. 387(24), 2220–2231 (2022).
• Evaluates the response, the duration of response, the survival and the safety of glofitamab in patients with DLBCL. It was found that more than half of the patients had an adverse event of grade 3 or 4.
9.
AbbVie Corporation. Product monograph including patient information: EPKINLY (epcoritamab) 2023. https://www.abbvie.ca/content/dam/abbvie-dotcom/ca/en/documents/products/EPKINLY_PM_EN.pdf
10.
Hoffmann-La Roche Limited. Product monograph including patient medication information: Columvi (glofitamab) 2023. https://pdf.hres.ca/dpd_pm/00070059.PDF
11.
Flood CM, Thomas B, McGibbon E. Canada's primary care crisis: Federal Government Response. Healthc. Manage. Forum 36(5), 327–332 (2023).
12.
Canadian Medical Association. Canada's health care crisis: what we need now 2022. https://www.cma.ca/latest-stories/canadas-health-care-crisis-what-we-need-now
13.
Lei M, Li Q, O'Day K, Meyer K, Wang A, Jun M. Practice efficiency associated with epcoritamab for the treatment ofpatients with relapsed or refractorye B-cell lymphoma from an institutional perspective. Blood 142(Suppl. 1), 7254 (2023).
•• This micro-cost analysis evaluates the practice efficiency of treating patients with R/R-DLBCL with epcoritamab.
14.
Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH reimbursement recommendation: lisocabtagene maraleucel (Breyanzi).
15.
Novartis Pharmceuticals Canada Inc. Product monograph including patient medication information: KYMRIAH (Tisagenlecleucel). (2018).
16.
Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH reimbursement recommendation: axicabtagene ciloleucel (Yescarta). (June 2023).
17.
Hoffmann-La Roche Limited. Product monograph including patient medication information: POLIVY (Polatuzumab vedotin for injection). (2023).
18.
Pan-Canadian Oncology Drug Review. pCODR Expert Review Committee (pERC) finale recommendation: polatuzumab vedotin (Polivy). (2021).
19.
Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH reimbursement recommendation: tafasitamab (Minjuvi). (October 2022).
20.
Institut National d'excellence and sante et services sociaux (INESSS). Avis transmis au ministre: MINJUVI (Lymphome diffus à grandes cellules B). (October 2022).
21.
Institut National d'excellence and sante et services sociaux (INESSS). Avis transmis au ministre: POLIVY (Lymphome diffus à grandes cellules B). (May 2021).
22.
Statistics Canada. Consumer Price Index by product group, monthly, percentage change, not seasonally adjusted, Canada, provinces, Whitehorse, Yellowknife and Iqaluit 2023. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1810000413
23.
Locke F, Go W, Neelapu S. Development and use of the anti-CD19 chimeric antigen receptor T-cell therapy axicabtagene ciloleucel in large B-cell lymphoma: a review. JAMA Oncol. 6(2), 281–290 (2020).
24.
Ontario Ministry of Health and Long-Term Care. Laboratories and diagnostics branch. Schedule of benefits for laboratory services (Effective 24 July 2023). https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/sob_lab_2023.pdf
25.
Régie de l'assurance maladie du Quebec (RAMQ). Manuel des médecins spécialistes – Rémunération à l'acte 2023. https://www.ramq.gouv.qc.ca/fr/professionnels/medecins-specialistes/manuels/Pages/remuneration-acte.aspx
26.
Government of Canada. Wages for pharmacists (NOC 3131). Wage data updated on November 17th, 2021. https://www.jobbank.gc.ca/wagereport/occupation/18196
27.
Government of Canada. Wages, Registered Nurse in Canada 2022. https://www.jobbank.gc.ca/marketreport/wages-occupation/993/ca
28.
Pettigrew M, Kavan P, Surprenant L, Lim HJ. Comparative net cost impact of the utilization of panitumumab versus cetuximab for the treatment of patients with metastatic colorectal cancer in Canada. J. Med. Econ. 19(2), 135–147 (2016).
29.
Statistics Canada. Employee wages by industry, annual (Table: 14-10-0064-01) 2023. https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1410006401
30.
Statistics Canada. Average usual and actual hours worked in a reference week by type of work (full- and part-time), annual (Table: 14-10-0043-01) 2023. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1410004301
31.
Canadian Agency for Drugs and Technologies in Health (CADTH). Axicabtagene ciloleucel for diffuse large B-Cell lymphoma: economic review report. (2019).
32.
Abramson JS, Palomba ML, Gordon LI et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet 396(10254), 839–852 (2020).
33.
Schuster SJ, Bishop MR, Tam CS et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-Cell lymphoma. N. Engl. J. Med. 380(1), 45–56 (2019).
34.
Neelapu SS, Locke FL, Bartlett NL et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-Cell lymphoma. N. Engl. J. Med. 377(26), 2531–2544 (2017).
35.
Locke FL, Ghobadi A, Jacobson CA et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, Phase I–II trial. Lancet Oncol. 20(1), 31–42 (2019).
36.
Ontario Ministry of Health and Long-Term Care. Ontario drug benefit (ODB) formulary 2023. https://www.formulary.health.gov.on.ca/formulary/
37.
Régie de l'assurance maladie du Quebec (RAMQ). Liste des medicaments. (6 July 2023).
38.
IQVIA Delta PA. (12 July 2023).
39.
40.
Cancer Care Ontario. R-GemOx Regimen 2022. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/67996
41.
Cancer Care Ontario. Drug formulary - BEND+POLA+RITU. (2022). https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/62866
42.
Cancer Care Ontario. Drug formulary - LENA+TAFA. (2022). https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/71931
43.
Canadian Institute for Health Information. Patient cost estimator. (2019). https://www.cihi.ca/en/patient-cost-estimator
44.
Cancer Care Ontario. Drug formulary: funded evidence-informed regimens 2023. https://www.cancercareontario.ca/en/drugformulary/regimens
45.
Sehn LH, Herrera AF, Flowers CR et al. Polatuzumab vedotin in relapsed or refractory diffuse large B-Cell lymphoma. J. Clin. Oncol. 38(2), 155–165 (2020).
46.
Salles G, Duell J, González Barca E et al. Tafasitamab plus lenalidomide in relapsed or refractory diffuse large B-cell lymphoma (L-MIND): a multicentre, prospective, single-arm, phase 2 study. Lancet Oncol. 21(7), 978–988 (2020).
47.
Corazzelli G, Capobianco G, Arcamone M et al. Long-term results of gemcitabine plus oxaliplatin with and without rituximab as salvage treatment for transplant-ineligible patients with refractory/relapsing B-cell lymphoma. Cancer Chemother. Pharmacol. 64(5), 907–916 (2009).
48.
Ontario Ministry of Health and Long-Term Care. Ontario case costing analysis tool. (2018).
49.
BC Cancer. Tocilizumab (interim monograph) 2021. http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Tocilizumab_interim%20monograph.pdf
50.
BC Cancer. BC cancer guidelines for prevention and treatment of chemotherapy-induced nausea and vomiting in adults 2022. http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Supportive%20Care/SCNAUSEA_Protocol.pdf
51.
Cancer Care Ontario. Drug Formulary - Regimens 2022. https://www.cancercareontario.ca/en/drugformulary/regimens?f%5B0%5D=field_type_of_cancer%3A626
52.
Prica A, Hay AE, Crump M et al. Evaluating the indirect costs of care associated with salvage chemotherapy for relapsed and refractory aggressive-histology lymphoma: a subset analysis of the Canadian Cancer Trials Group (CCTG) LY.12 Clinical Trial. Curr. Oncol. 28(2), 1256–1261 (2021).
53.
Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH reimbursement recommendation (Draft): epcoritamab (Epkinly). (2024).
54.
De Cock E, Kritikou P, Sandoval M et al. Time savings with rituximab subcutaneous injection versus rituximab intravenous infusion: a time and motion study in eight countries. PLoS ONE 11(6), e0157957 (2016).
55.
Rummel M, Kim TM, Aversa F et al. Preference for subcutaneous or intravenous administration of rituximab among patients with untreated CD20þ diffuse large B-cell lymphoma or follicular lymphoma: results from a prospective, randomized, open-label, crossover study (PrefMab). Ann. Oncol. 28, 836–842 (2017).
56.
Drummond D, Sinclair D, Gratton J. Troubles in Canada's health workforce: the why, the where, and the way out of shortages. CD Howe Institute, Canada (2022).
•• Assesses the challenges present in the Canadian healthcare system, therefore highlights the importance of having therapies available that help save resources.
57.
Institut national d'excellence en santé et services sociaux (INESSS). Tisagenlecleucel pour le traitement du lymphome diffus à grandes cellules B récidivant ou réfractair. (2019). https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Therapies_cellulaires/INESSS_Avis_Kymriah_LDGCB.pdf
58.
nCanadian Institute for Health Informatio. Care in Canadian ICUs. (2016). https://secure.cihi.ca/free_products/ICU_Report_EN.pdf
59.
Statistics Canada. Labour force characteristics by province, monthly, seasonally adjusted - Table: 14-10-0287-03. (2023). https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1410028703
Information & Authors
Information
Published In
Copyright
© 2026 AbbVie Corporation. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 December 2025
Accepted: 8 April 2026
Published online: 20 April 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Health care resource use in the management of patients with relapsed/refractory diffuse large B-cell lymphoma – Canadian perspective. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0187
Export citation
Select the citation format you wish to export for this article or chapter.