Health economic analysis of pulsed field ablation compared to conventional thermal ablation for patients with paroxysmal atrial fibrillation in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate the cost-utility of pulsed field ablation (PFA) compared with radiofrequency ablation (RFA) and cryoablation, respectively, in Chinese patients with paroxysmal atrial fibrillation. Materials & methods: Patients with paroxysmal atrial fibrillation at different levels of atrial arrhythmia burden (<0.1%, 0.1–9.9%, ≥10%) may experience various atrial arrhythmia burden states after undergoing ablation. A decision tree model was developed to simulate this process from a healthcare perspective, where patients could undergo a repeat ablation or experience a nonfatal stroke. Transition probabilities, clinical outcome and quality of life data were obtained from published sources and confirmed by expert physicians. Cost data were estimated from a survey of clinicians at tertiary hospitals, based on actual clinical practices. The uncertainty of results was explored through one-way sensitivity analysis and probabilistic sensitivity analysis by Monte Carlo simulation. The secondary outcome, return on investment, was calculated from hospital administrator perspective, as net revenue divided by total cost of certain ablation type. Results: PFA demonstrated favorable cost–effectiveness compared with both RFA and cryoablation under the three-times China’s per capita GDP threshold. When compared with RFA, PFA yielded an incremental 0.016 quality-adjusted life years (QALYs) (0.859 vs 0.842) with an incremental cost–effectiveness ratio of ¥37,000 per QALY gained. This cost–effectiveness was primarily driven by savings of ¥1558 in weighted repeat ablation surgery costs and ¥506 in long-term medication costs for anti-arhythmic and anticoagulants. When compared with cryoablation, PFA resulted in an incremental 0.006 QALYs (0.859 vs 0.852) with an incremental cost–effectiveness ratio of ¥231,167 per QALY gained, mainly attributed to savings of ¥1300 in repeat ablation surgery costs and ¥133 in long-term medication costs. As a secondary outcome, PFA yielded a return on investment of 0.313. Conclusion: PFA was likely to be more cost effective than both radiofrequency ablation and cryoablation in China. The study suggests that PFA represents a high-value intervention that aligns superior clinical outcomes with favorable hospital financial sustainability, supporting its prioritized adoption in the management of atrial fibrillation in China.
Plain language summary: Health economic benefits of pulsed field ablation for patients with a common heart rhythm disorder in China
What is this article about?
This article investigates the economic value of a new heart ablation technology called pulsed field ablation (PFA) for treating patients with paroxysmal atrial fibrillation (a common type of irregular heartbeat) in China. We compared the costs and health outcomes of PFA against two established ablation techniques: radiofrequency ablation and cryoablation. The goal was to determine if the new PFA technology provides good value for money for the Chinese healthcare system.
What were the results?
Over a 1-year period, treatment with PFA was found to be more cost-effective than both traditional methods. Although the initial procedure cost for PFA was slightly higher, patients receiving PFA required fewer repeat procedures, had fewer complications, and incurred lower long-term medication costs. Patients treated with PFA also experienced a very small but meaningful improvement in quality of life. The results were confirmed through analyses that tested how sensitive the findings were to changes in key assumptions, showing that the conclusion is robust.
What do the results mean?
These results suggest that from a cost–effectiveness perspective, PFA is an economically favorable first-line treatment option for paroxysmal atrial fibrillation in China. Adopting PFA could lead to better outcomes for patients and more efficient use of healthcare resources compared with currently standard thermal ablation techniques.
Atrial fibrillation (AF) is the most common cardiac arrhythmia, with paroxysmal atrial fibrillation (PAF) accounting for approximately 30% of all AF cases [1]. In China, the prevalence of AF among adults aged ≥18 years is 1.6%, increasing significantly with age. AF patients face elevated risks of thromboembolism, stroke, transient ischemic attacks and higher hospitalization and mortality rates, leading to substantial disease burden and economic costs.
Thermal ablation has emerged as a minimally invasive procedure with several modalities available, including radiofrequency ablation (RFA), cryoablation and pulsed field ablation (PFA). The recent ADVENT trial [2] a prospective, multicenter, randomized study, demonstrated that PFA is noninferior to traditional thermal ablation (RFA and cryoablation) regarding the primary efficacy end point in paroxysmal AF patients. Secondary analyses [3] revealed that PFA may offer advantages in both efficacy and safety profiles.
Traditionally, ablation success has been evaluated using a dichotomous end point – freedom from arrhythmia recurrence lasting ≥30 s at 12 months. However, this definition has limitations in clinical relevance, particularly with continuous monitoring technologies. Atrial arrhythmia burden (AA burden), defined as the percentage of time a patient experiences arrhythmias during monitoring. Each patient’s total AA burden is estimated as the greater of two calculated values: the percentage of AA over the total duration of available Holter monitoring data, or the percentage of weeks with AA detected by transtelephonic monitors out of the total number of weeks with recorded transtelephonic monitors. Based on these calculations, AA burden values are categorized into three risk groups: <0.1% (very low risk), 0.1–9.9% (moderate risk) and ≥10% (high risk), each with distinct clinical implications. Studies have shown that post-ablation AA burden offers a more comprehensive assessment of therapeutic efficacy than the traditional 30 s threshold.
Despite evidence supporting the clinical benefits of PFA, its economic evaluation compared with conventional thermal ablation has not been conducted in China. This study aims to assess the economic value of PFA versus RFA and cryoablation for patients with paroxysmal AF through a cost–effectiveness analysis as primary end point and return on investment (ROI) analysis as secondary end point, providing evidence to inform decision-making on interventions and medical resource allocation in China.
Materials & methods
Cost–utility analysis
Model strategy & assumptions
A decision tree model was developed using Microsoft Excel to evaluate the cost-utility of PFA compared with RFA and cryoablation separately for the treatment of paroxysmal AF. The analysis was conducted from the perspective of the Chinese healthcare system with a 1-year time horizon.
The study population consisted of patients with drug-resistant paroxysmal AF receiving their first ablation procedure. These patients were assumed to have characteristics similar to those in the ADVENT trial, with a mean age of 62 years and a male proportion of 65.6%.
The model simulated the progression of paroxysmal AF patients following their first ablation procedure (Figure 1). After the first ablation, patients transitioned into one of three health states based on residual AA burden: <0.1%, 0.1–9.9%, or ≥10%. A key assumption was that patients with residual AA burden less than 0.1% after ablation would not require redo ablation. Meanwhile, those with AA burden of 0.1–9.9% or ≥10% were likely to undergo redo ablation, with the probability depending on both their AA burden status and the initial ablation method. Following the redo ablation, patients could transition to either the same or an improved (lower) AA burden state, but not to a worse one. The model restricted each patient to only once redo ablation within the 1-year period.
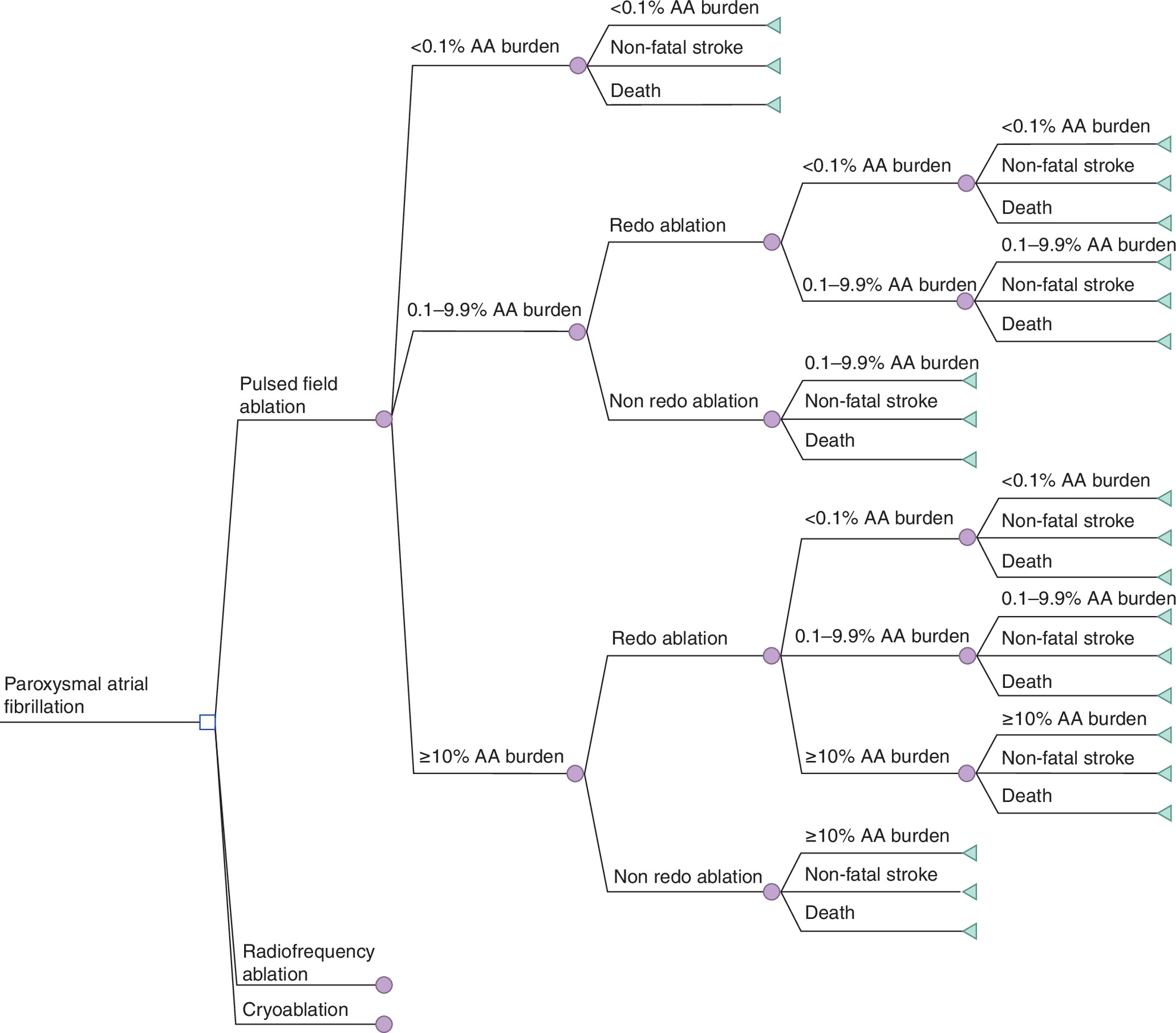
Figure 1. Structure of the decision-tree model for cost–effectiveness analysis.
AA Burden: Atrial arrhythmia burden.
Mortality during the 1-year time horizon was primarily attributed to natural causes, as death directly resulting from ablation procedures is rare in patients with atrial fibrillation. The model adopted age- and sex-adjusted natural mortality rates from Chinese population data [4] as the mortality rates used in the model. Death events were considered to occur concurrently with nonfatal stroke events.
All model inputs were primarily derived from published literature, with clinical expert opinion filling data gaps from two tertiary hospitals in China.
Clinical effectiveness
The probability of patients being in different AA burden categories after initial and redo ablations and redo ablation rates (Table 1) were key clinical effectiveness inputs. Data for these probabilities were normalized after removing 5% of outliers, derived from the ADVENT trial [2], with values extracted from graphs using Engauge Digitizer 12.1 and validated by physicians. The trial demonstrated that PFA resulted in both lower redo ablation rates and higher proportions of patients achieving lower AA burden classifications compared with Cryo and RFA. Since the three AA burden categories were constrained to sum to 100% at each decision point and exhibited inherent proportional relationships, these distribution parameters were treated as fixed values and not subjected to one-way sensitivity analysis.
| Parameters | Base case | Lower estimate | Upper estimate | Distribution type | Distribution Par 1 | Distribution Par 2 | Ref. |
|---|---|---|---|---|---|---|---|
| Proportion of patients with different AA burden status under different ablation methods (not included in DSA) | |||||||
| PFA_<0.1% | 84.33% | Not included in DSA | Dirichlet | 0.558 | [3] | ||
| PFA_0.1–9.9% | 11.27% | Dirichlet | 0 | [3] | |||
| PFA_≥10% | 4.40% | Dirichlet | 0.003 | [3] | |||
| RFA_<0.1% | 75.50% | Dirichlet | 0.068 | [3] | |||
| RFA_0.1–9.9% | 12.84% | Dirichlet | 0.67 | [3] | |||
| RFA_≥10% | 11.66% | Dirichlet | 0.048 | [3] | |||
| Cryo_<0.1% | 76.82% | Dirichlet | 0.046 | [3] | |||
| Cryo_0.1–9.9% | 20.32% | Dirichlet | 0 | [3] | |||
| Cryo_≥10% | 2.86% | Dirichlet | 0 | [3] | |||
| Proportion of patients with different AA burden status after different redo ablation modalities (not included in DSA) | |||||||
| PFA_0.1–9.9% transfers to: | Not included in DSA | – | |||||
| <0.1% | 80.00% | Dirichlet | 0.032 | Physician survey | |||
| 0.1–9.9% | 20.00% | Dirichlet | 0.626 | Physician survey | |||
| PFA_≥10% transfers to: | |||||||
| <0.1% | 65.00% | Dirichlet | 0.476 | Physician survey | |||
| 0.1–9.9% | 25.00% | Dirichlet | 0.003 | Physician survey | |||
| ≥10% | 10.00% | Dirichlet | 0 | Physician survey | |||
| RFA_0.1–9.9% transfers to: | |||||||
| <0.1% | 70.00% | Dirichlet | 0.252 | Physician survey | |||
| 0.1–9.9% | 30.00% | Dirichlet | 0.037 | Physician survey | |||
| RFA_≥10% transfers to: | |||||||
| <0.1% | 60.00% | Dirichlet | 0.117 | Physician survey | |||
| 0.1–9.9% | 25.00% | Dirichlet | 0.001 | Physician survey | |||
| ≥10% | 15.00% | Dirichlet | 0.001 | Physician survey | |||
| Cryo_0.1–9.9% transfers to: | |||||||
| <0.1% | 75.00% | Dirichlet | 1.262 | Physician survey | |||
| 0.1–9.9% | 25.00% | Dirichlet | 0.518 | Physician survey | |||
| Cryo_≥10% transfers to: | |||||||
| <0.1% | 62.00% | Dirichlet | 0.02 | Physician survey | |||
| 0.1–9.9% | 30.00% | Dirichlet | 0.064 | Physician survey | |||
| ≥10% | 8.00% | Dirichlet | 0 | Physician survey | |||
| Proportion of patients with different AA burden status receiving redo ablation | |||||||
| PFA_0.1–9.9% | 9.22% | 0.075 | 0.111 | Beta | 90.692 | 893.414 | [3] |
| RFA_0.1–9.9% | 9.51% | 0.077 | 0.115 | Beta | 90.395 | 860.151 | [3] |
| Cryo_0.1–9.9% | 14.80% | 0.12 | 0.178 | Beta | 85.048 | 489.449 | [3] |
| PFA_≥10% | 38.24% | 0.309 | 0.459 | Beta | 61.382 | 99.156 | [3] |
| RFA_≥10% | 33.43% | 0.27 | 0.401 | Beta | 66.234 | 131.886 | [3] |
| Cryo_≥10% | 59.90% | 0.075 | 0.111 | Beta | 39.499 | 26.440 | [3] |
AA: Atrial arrhythmia; Cryo: Cryoablation; DSA: Deterministic sensitivity analysis; PFA: Pulsed field ablation; RFA: Radiofrequency ablation.
Stroke
Nonfatal stroke rates were stratified according to patients' AA burden status (Table 2). For patients with <0.1% AA burden who did not undergo redo ablation after initial PFA, a stroke rate of 0.12% was derived from a large retrospective cohort study [5]. To determine stroke rates for higher AA burden categories, we used risk ratios calculated from another retrospective study that examined ischemic stroke rates across three AF burden tertiles (1.90%, 2.60% and 3.80% for AF burden ranges of 0.01–2.03%, 2.05–11.28% and 11.36–99.99%, respectively) [6]. By calculating the ratios of 2.60/1.90 and 3.80/1.90, we established relative risks of 1.37 and 2.00 for our model’s 0.1–9.9% and ≥10% AA burden categories compared with the <0.1% category. Applying these ratios to our baseline stroke rate of 0.12% yielded stroke rates of 0.16 and 0.24% for the 0.1–9.9% and ≥10% AA burden categories after initial PFA, respectively.
| Parameters | Base case | Lower estimate | Upper estimate | Distribution type | Distribution Par 1 | Distribution Par 2 | Ref. |
|---|---|---|---|---|---|---|---|
| Post initial ablation | |||||||
| PFA_<0.1% | 0.12% | 0.001 | 0.001 | Beta | 98.08 | 5064.08 | [5] |
| RR of <0.1% (RFA vs PFA) | 1.3 | 1.064 | 1.573 | Beta | -31.30 | 7.22 | Physician survey |
| RR of <0.1% (Cryo vs PFA) | 1.2 | 0.982 | 1.452 | Beta | -21.20 | 3.53 | Physician survey |
| PFA_0.1–9.9% | 0.16% | 0.001 | 0.002 | Beta | 99.83 | 60696.60 | [5] |
| RR of 0.1–9.9% (RFA vs PFA) | 1.3 | 1.064 | 1.573 | Lognormal | 0.26 | 0.10 | Physician survey |
| RR of 0.1–9.9% (Cryo vs PFA) | 1.2 | 0.982 | 1.452 | Lognormal | 0.18 | 0.10 | Physician survey |
| PFA_≥10% | 0.24% | 0.002 | 0.003 | Beta | 99.76 | 41465.91 | [5] |
| RR of ≥10% (RFA vs PFA) | 1.3 | 1.064 | 1.573 | Lognormal | 0.26 | 0.10 | Physician survey |
| RR of ≥10% (Cryo vs PFA) | 1.2 | 0.982 | 1.452 | Lognormal | 0.18 | 0.10 | Physician survey |
| Post redo ablation | |||||||
| PFA_<0.1% | 0.13% | 0.001 | 0.002 | Beta | 99.87 | 79164.21 | Physician survey [5] |
| RR of <0.1% (RFA vs PFA) | 1.3 | 1.064 | 1.573 | Lognormal | 0.26 | 0.10 | Physician survey |
| RR of <0.1% (Cryo vs PFA) | 1.2 | 0.982 | 1.452 | Lognormal | 0.18 | 0.10 | Physician survey |
| PFA_0.1–9.9% | 0.17% | 0.001 | 0.002 | Beta | 99.83 | 57796.73 | Physician survey [5] |
| RR of 0.1–9.9% (RFA vs PFA) | 1.3 | 1.064 | 1.573 | Lognormal | 0.26 | 0.10 | Physician survey |
| RR of 0.1–9.9% (Cryo vs PFA) | 1.2 | 0.982 | 1.452 | Lognormal | 0.18 | 0.10 | Physician survey |
| PFA_≥10% | 0.25% | 0.002 | 0.003 | Beta | 99.75 | 39481.79 | Physician survey [5] |
| RR of ≥10% (RFA vs PFA) | 1.3 | 1.064 | 1.573 | Lognormal | 0.26 | 0.10 | Physician survey |
| RR of ≥10% (Cryo vs PFA) | 1.2 | 0.982 | 1.452 | Lognormal | 0.18 | 0.10 | Physician survey |
Cryo: Cryoablation; PFA: Pulsed field ablation; RFA: Radiofrequency ablation; RR: Relative risk.
For patients undergoing redo ablation, stroke rates were adjusted based on expert clinical opinion, with a 1.05-fold increase applied to the rates observed in patients without redo ablation. To estimate stroke rates for RFA and Cryoablation, relative risk values of 1.3 and 1.2 were applied using PFA as the reference treatment, respectively.
Costs
Costs included procedure fees (initial and once redo ablation), complications management, nonfatal stroke treatment (acute and maintenance phases) and medication expenses (antiarrhythmic and anticoagulants) (Table 3).
| Parameters | Base case | Lower estimate | Upper estimate | Distribution type | Distribution Par 1 | Distribution Par 2 | Ref. |
|---|---|---|---|---|---|---|---|
| Per-procedure cost of ablation (CNY/procedure) | |||||||
| PFA | ¥65,000.00 ($8904.11) | Not included in sensitivity analysis | Physician survey | ||||
| RFA | ¥65,000.00 ($8904.11) | Physician survey | |||||
| Cryo | ¥65,000.00 ($8904.11) | Physician survey | |||||
| Cost per complication management (CNY/episode) | |||||||
| PFA | ¥51.28 ($7.02) | 41.7 | 61.8 | Gamma | 100 | 0.51 | [7–9] |
| RFA | ¥238.01 ($32.60) | 193.7 | 286.9 | Gamma | 100 | 2.38 | [8–10] |
| Cryo | ¥109.43 ($14.99) | 93.2 | 138.0 | Gamma | 100 | 1.15 | [8–11] |
| Annual cost of complication management (CNY/year) | |||||||
| PFA | ¥42.65 ($5.84) | 34.7 | 51.4 | Gamma | 100 | 0.43 | [7,8,12] |
| RFA | ¥168.26 ($23.05) | 136.9 | 202.8 | Gamma | 100 | 1.68 | [8–10,12] |
| Cryo | ¥143.94 ($19.72) | 117.1 | 173.5 | Gamma | 100 | 1.44 | [8–10,12] |
| Cost management of nonfatal stroke | |||||||
| Acute phase (CNY/episode) | ¥35,479.50 ($4860.21) | 28,867.5 | 42763.1 | Gamma | 100 | 354.80 | [13] |
| Post-stroke (CNY/year) | ¥7500.00 ($1027.40) | 6102.3 | 9039.7 | Gamma | 100 | 75.00 | [8] |
| Daily cost of standard-dose drugs (CNY/day) | |||||||
| AADs | ¥10.00 ($1.37) | 3 | 30 | Gamma | 100 | 0.10 | Physician survey |
| Anticoagulants | ¥15.15 ($2.08) | 0.3 | 30 | Gamma | 100 | 0.15 | Physician survey |
| Duration of postoperative oral AADs use grouped by AA burden status (days) | |||||||
| <0.1% | 90 | 72.4 | 107.6 | Normal | 90.0 | 9.0 | Physician survey |
| 0.1–9.9% | 182.5 | 146.7 | 218.3 | Normal | 182.5 | 18.3 | Physician survey |
| ≥10% | 365 | Excluded from sensitivity analysis | Physician survey | ||||
| Duration of postoperative oral anticoagulants use grouped by AA burden status (days) | |||||||
| <0.1% | 75 | 60.3 | 89.7 | Normal | 75.0 | 7.5 | Physician survey |
| 0.1–9.9% | 365 | Not included in sensitivity analysis | Physician survey | ||||
| ≥10% | 365 | Physician survey | |||||
AA: Atrial arrhythmia; AAD: Antiarrhythmic drug; Cryo: Cryoablation; PFA: Pulsed field ablation; RFA: Radiofrequency ablation.
According to the public medical service price lists in major Chinese provinces and expert survey, the procedure fees for different types of ablation are identical. PFA incurs additional ¥3000 anesthesia costs during the procedure. According to the public medical service price list in major Chinese provinces, the procedure fees for RFA and Cryo ablation are identical (PFA has not yet been included in the list). Additionally, under centralized volume-based procurement policies that have substantially reduced the costs of key consumables for ablation procedures, the model assumed equivalent procedure fees across all three ablation techniques.
Complication management costs accounted for cardiovascular-related complications (cardiac tamponade and pericardial effusion), cerebrovascular-related complications (stroke and transient ischemic attack) and neurological-related complications (phrenic nerve palsy). For each ablation modality, weighted complication costs were derived by multiplying complication-specific treatment expenditures by their respective incidence rates. These weighted complication costs represent the aggregate expenditure for managing all three categories of complications, accounting for their varying frequencies and associated treatment costs. The complication rates for PFA were extracted from a recent clinical trial [7], and the rates for RFA and Cryo were sourced from a published meta-analysis [10]. Each ablation procedure incurred short-term post-operative costs. Long-term costs referred to expenses associated with lasting sequelae requiring ongoing treatment, such as persistent phrenic nerve palsy. The weighted complication costs varied between different ablation modalities, primarily due to differences in complication incidence rates across techniques. Nonfatal stroke costs also comprised both acute treatment expenses and long-term sequelae management costs.
Medication costs included expenditures for antiarrhythmic drugs (AADs) and anticoagulants, calculated by multiplying the daily medication cost by the duration of treatment. Since treatment patterns differ across AF burden categories, the calculation of medication costs considered both the daily drug costs and duration of medication specific to each burden state. These estimates were provided by clinical experts considering the proportion of brand-name, generic and bulk procurement drugs used in real-world clinical practice.
Patients in all three AF burden states received standard-dose oral AADs and anticoagulants for 3 months prior to the ablation However, post-procedure medication durations varied by AA burden state. For AADs, post-ablation treatment with a standard dose was prescribed for 90 days in patients with <0.1% AA burden, approximately 6 months in those with 0.1–9.9% AA burden, and for a full year in those with ≥10% AA burden. For anticoagulants, post-ablation standard-dose therapy was administered for 75 days in patients with <0.1% AA burden and 365 days in those with ≥10% AA burden. Patients with 0.1–9.9% AA burden received low-dose anticoagulation for 365 days, with daily costs calculated as half of the standard-dose cost.
Time period
According to physician estimates, hospitalization for an ablation procedure lasted approximately 1 week. For patients requiring redo ablation, the interval between the initial and next ablation was estimated to be 6 months, and the time between ablation and stroke occurrence was approximately 3 months. The acute phase of a nonfatal stroke required a hospital stay of approximately 3 weeks (Table 4).
| Parameters | Base case | Lower estimate | Upper estimate | Distribution type | Distribution Par 1 | Distribution Par 2 | Ref. |
|---|---|---|---|---|---|---|---|
| Length of stay (days) | |||||||
| Per ablation | 7.5 | 6.2 | 9.1 | Normal | 7.7 | 0.7 | Physician survey |
| Acute phase stroke | 21.0 | 16.8 | 25.2 | Normal | 21.1 | 2.1 | Physician survey |
| Time to event (days) | |||||||
| Initial ablation–redo ablation | 182.5 | 182.5 | 365 | Normal | 182.5 | 18.3 | Physician survey |
| Redo ablation–stroke | 90 | 30 | 365 | Normal | 90.0 | 9.0 | Physician survey |
| Initial ablation (non redo)–stroke | 90 | 30 | 365 | Normal | 90.0 | 9.0 | Physician survey |
Utilities
Utility values were assigned to different AA burden states based on published literature (Table 5). For a redo ablation procedure, the disutility of 0.15 was applied to reflect the short-term impact associated with the minimally invasive intervention. Disutility of stroke event was 0.3 [14] and the utility of poststroke events was 0.582 [15].
| Parameters | Base case | Lower estimate | Upper estimate | Distribution type | Distribution Par 1 | Distribution Par 2 | Ref. |
|---|---|---|---|---|---|---|---|
| Utility | |||||||
| <0.1% AA burden | 0.89 | 0.86 | 0.90 | Beta | 10.62 | 1.38 | [15] |
| 0.1–9.9% AA burden | 0.77 | 0.70 | 0.82 | In the PSA, the utility values maintain the same ratios as in the base case relative to the <0.1% AA burden. | [16,17] | ||
| ≥10% AA burden | 0.66 | 0.55 | 0.69 | [18] | |||
| Post-stroke | 0.15 | 0.12 | 0.18 | Beta | 84.85 | 480.82 | Physician survey |
| Disutility | |||||||
| Acute phase stroke | 0.30 | 0.24 | 0.36 | Beta | 69.70 | 162.63 | [14] |
| Redo ablation | 0.58 | 0.51 | 0.65 | Beta | 84.85 | 480.82 | [14] |
AA: Atrial arrhythmia; PSA: Probabilistic sensitivity analysis.
ROI analysis
A decision-analytic model was developed to evaluate the ROI of PFA compared with RFA and cryoablation for the treatment of paroxysmal AF in Chinese hospitals. The model adopted a hospital perspective, focusing on direct medical costs and revenue generation under Diagnosis-Related Groups reimbursement schedules, and capturing outcomes of a single ablation procedure.
The ROI was calculated as the net monetary benefit (NMB) divided by the investment cost for each ablation strategy. NMB was defined as hospital revenue minus total costs. For each ablation strategy, the ROI ratio was computed as (revenue - costs) ÷ costs. Both cost and revenue data are collected from hospital survey.
Results
Cost–utility analysis
Base-case results
Base-case analysis demonstrated that for patients with PAF 1 year after initial ablation, PFA yielded an incremental cost of ¥592 compared with RFA (¥72,702 vs ¥72,110), along with a QALY gain of 0.016. This resulted in an incremental cost–effectiveness ratio (ICER) of ¥35,912.8 per QALY gained, which was 0.38-times of China’s per capita GDP threshold (Table 6).
| Ablation methods | |||
|---|---|---|---|
| PFA | RFA | Incremental | |
| Total costs | ¥72,702.4 | ¥72,110.3 | ¥592.1 |
| Ablation procedure cost | ¥68,000.0 | ¥65,000.0 | ¥3,000.0 |
| Weighted post-ablation complication-related costs | ¥95.3 | ¥418.5 | ¥-323.1 |
| Weighted redo ablation costs | ¥1769.3 | ¥3327.6 | ¥-1558.4 |
| Weighted nonfatal stroke-related costs | ¥55.2 | ¥76.1 | ¥-20.8 |
| Weighted continued use of AADs and anticoagulants costs | ¥2782.6 | ¥3288.1 | ¥-505.5 |
| Total QALYs | 0.859 | 0.842 | 0.017 |
| Incremental cost–effectiveness ratio | 35,912.8/QALY | ||
AAD: Antiarrhythmic drug; ICER: Incremental cost–effectiveness ratio; PFA: Pulsed field ablation; QALY: Quality-adjusted life year; RFA: Radiofrequency ablation.
When compared with cryoablation, PFA yielded an incremental cost of ¥1387 compared with RFA (¥72,702 vs ¥71,316), along with a QALY gain of 0.006 (Table 7). This resulted in an incremental cost–effectiveness ratio (ICER) of ¥225,364.1 per QALY gained, which was 2.35-times of China’s per capita GDP threshold. Therefore, PFA was economically favorable compared with both conventional thermal ablations under the three-times China’s per capita GDP threshold (¥287,247).
| Ablation methods | |||
|---|---|---|---|
| PFA | Cryoablation | Incremental | |
| Total costs | ¥72,702.4 | ¥71,315.8 | ¥1386.6 |
| Ablation procedure cost | ¥68,000.0 | ¥65,000.0 | ¥3000.0 |
| Weighted post-ablation complication-related costs | ¥95.3 | ¥263.8 | ¥-168.5 |
| Weighted redo ablation costs | ¥1769.3 | ¥3069.7 | ¥-1300.4 |
| Weighted nonfatal stroke-related costs | ¥55.2 | ¥67.1 | ¥-11.9 |
| Weighted continued use of AADs and anticoagulants costs | ¥2782.6 | ¥2915.2 | ¥-132.6 |
| Total QALYs | 0.859 | 0.852 | 0.006 |
| Incremental cost–effectiveness ratio (ICER) | 225,364.1/QALY | ||
AAD: Antiarrhythmic drug; ICER: Incremental cost–effectiveness ratio; PFA: Pulsed field ablation; QALY: Quality-adjusted life year.
Sensitivity analysis results
Deterministic sensitivity analysis
Parameter ranges in the one-way sensitivity analysis were primarily based on 95% CIs of parameter estimates or upper and lower limits reported in relevant literature. When standard errors were not reported in the literature, they were assumed to be 10% of the base value or were determined through clinical expert opinion.
One-way sensitivity analysis comparing PFA with RFA demonstrated that model results were most sensitive to the proportion of patients undergoing repeat ablation after initial RFA who had ≥10% AA burden (Figure 2). When compared with cryoablation, model results were sensitive to utility values across all three AA burden states and the proportion of patients undergoing repeat ablation after initial RFA who had ≥10% AA burden (Figure 3).
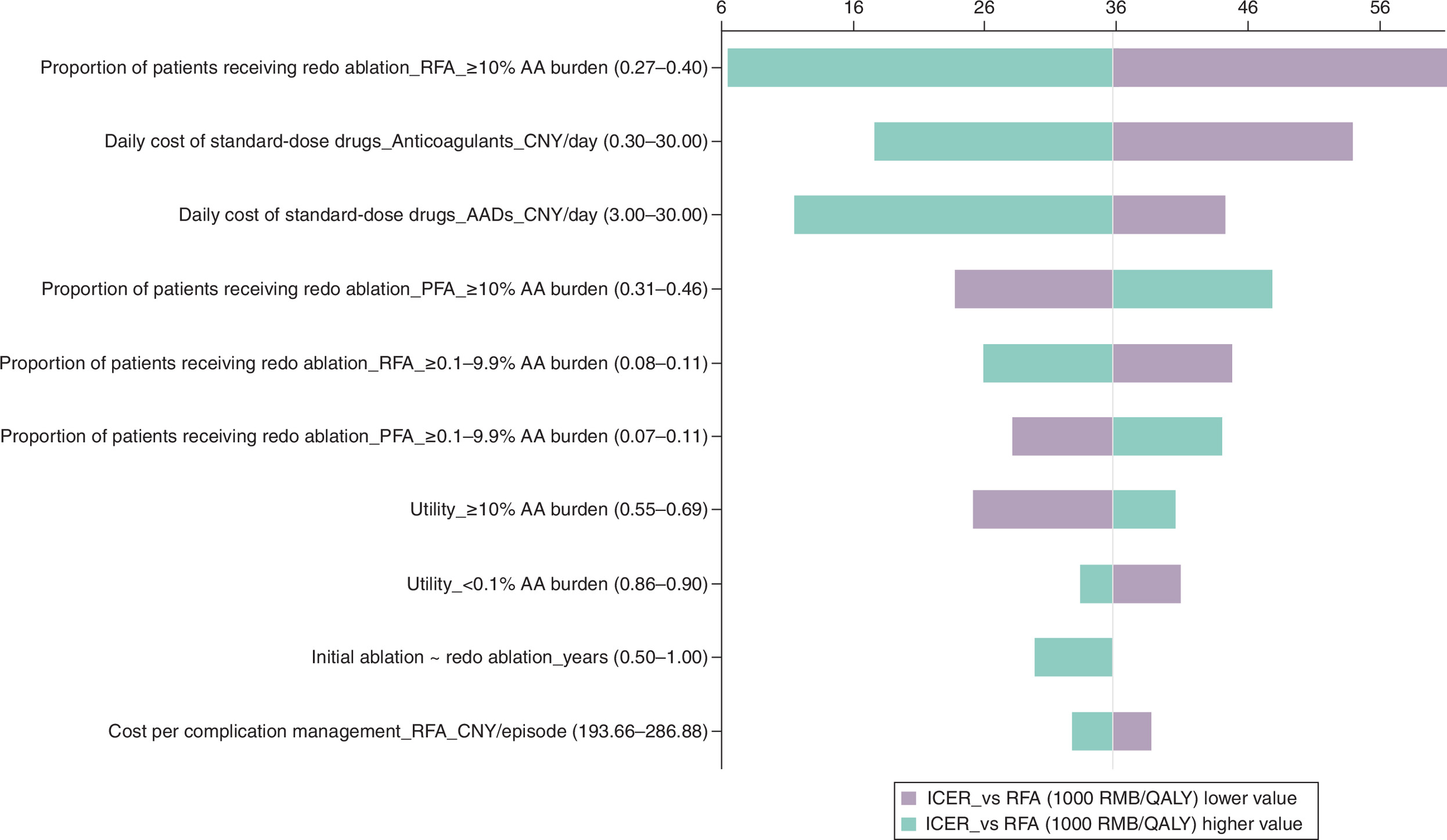
Figure 2. Tornado diagram for deterministic sensitivity analysis (pulsed field ablation vs radiofrequency ablation).
AA: Atrial arrhythmia; AAD: Antiarrhythmic drug; ICER: Incremental cost–effectiveness ratio; PFA: Pulsed field ablation; QALY: Quality-adjusted life year; RFA: Radiofrequency ablation.
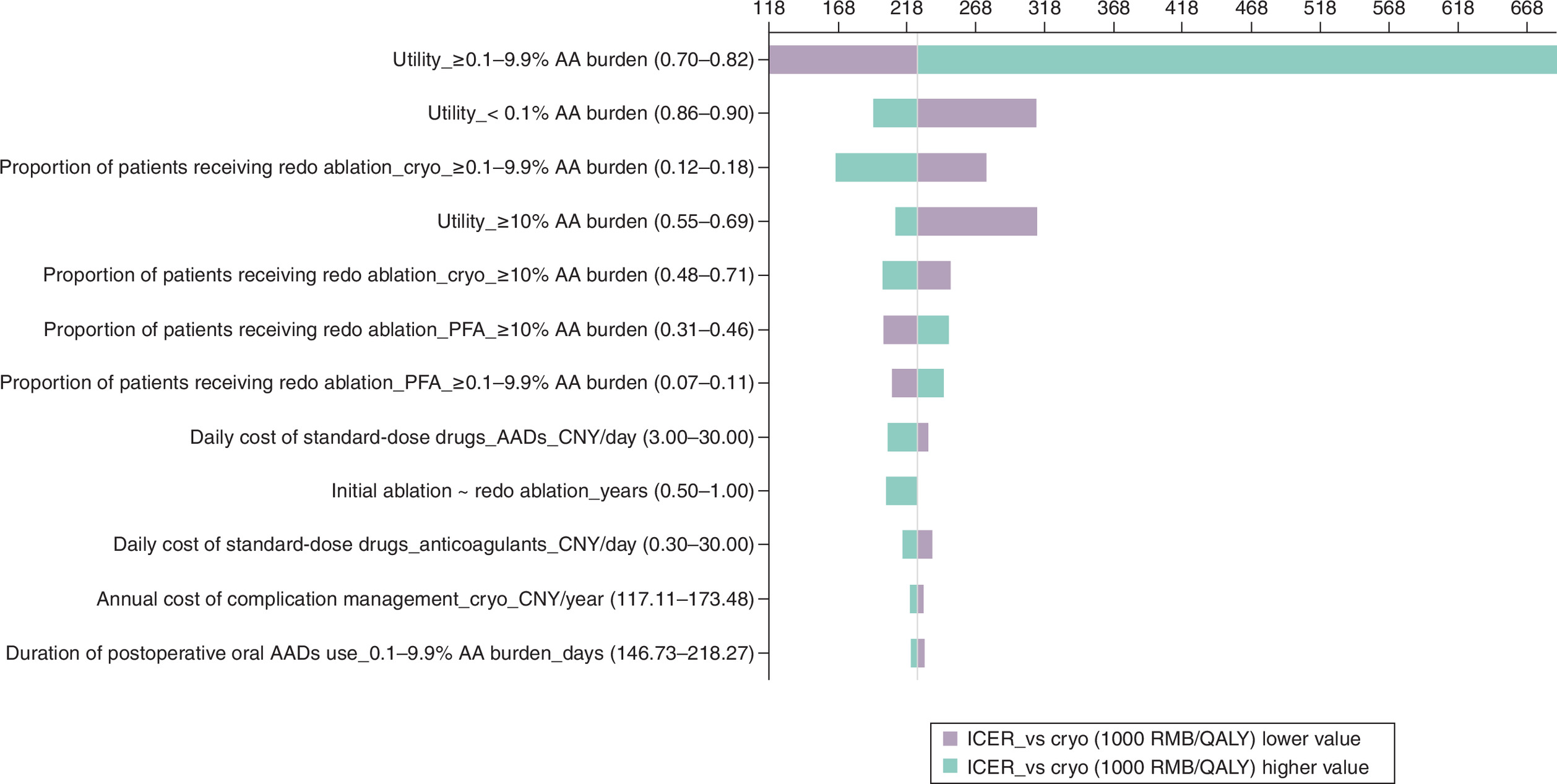
Figure 3. Tornado diagram for deterministic sensitivity analysis (pulsed field ablation vs cryoablation).
AA: Atrial arrhythmia; AAD: Antiarrhythmic drug; Cryo: Cryoablation; ICER: Incremental cost–effectiveness ratio; PFA: Pulsed field ablation: QALY: Quality-adjusted life year.
Probabilistic sensitivity analysis
Probabilistic sensitivity analysis (PSA) employed 3000 Monte Carlo simulations to simultaneously vary parameters within their possible ranges. During simulation, parameters were randomly sampled according to their assumed distributions: rate-related parameters followed Beta distributions, continuous variable followed Normal distributions and relative risk values followed Lognormal distributions.
PSA results comparing PFA to RFA showed that the vast majority of scatter points were located in the fourth quadrant, demonstrating that PFA had absolute economic dominance over RFA and confirming the robustness of the model results (Figures 4 & 5). Due to the nearly equivalent QALYs between PFA and cryoablation groups, the scatter points were evenly distributed on both sides of the Y-axis, but as the PFA group had lower costs, the vast majority of points were located below the X-axis. Eighty percent of scatter points fell below China’s three-times per capita GDP threshold, indicating a 80% probability that PFA was more cost-effective than cryoablation, demonstrating that the base-case result is relatively robust.
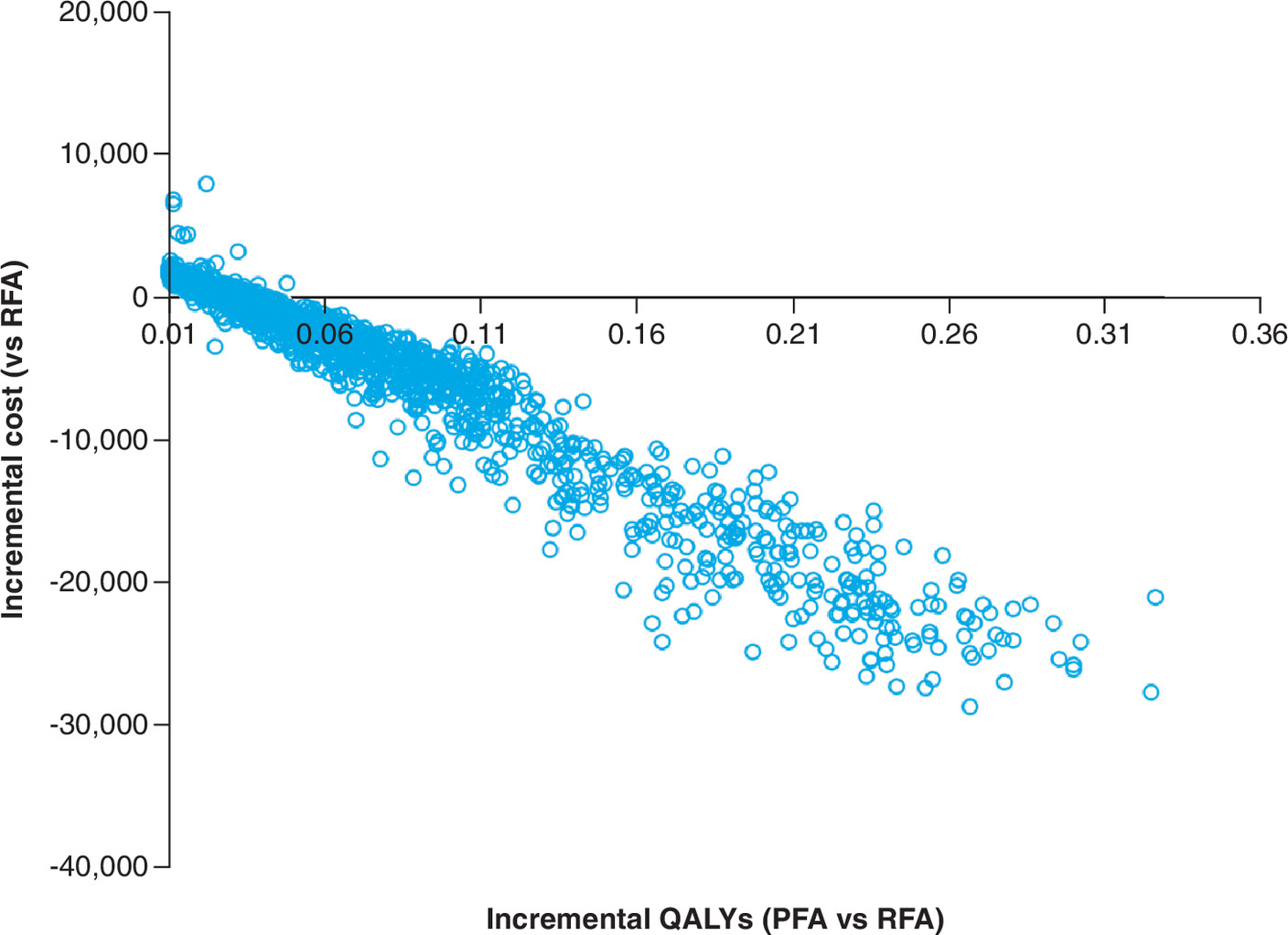
Figure 4. Incremental cost–effectiveness scatter plot for probabilistic sensitivity analysis (pulsed field ablation vs radiofrequency ablation).
PFA: Pulsed field ablation; QALY: Quality-adjusted life year; RFA: Radiofrequency ablation.
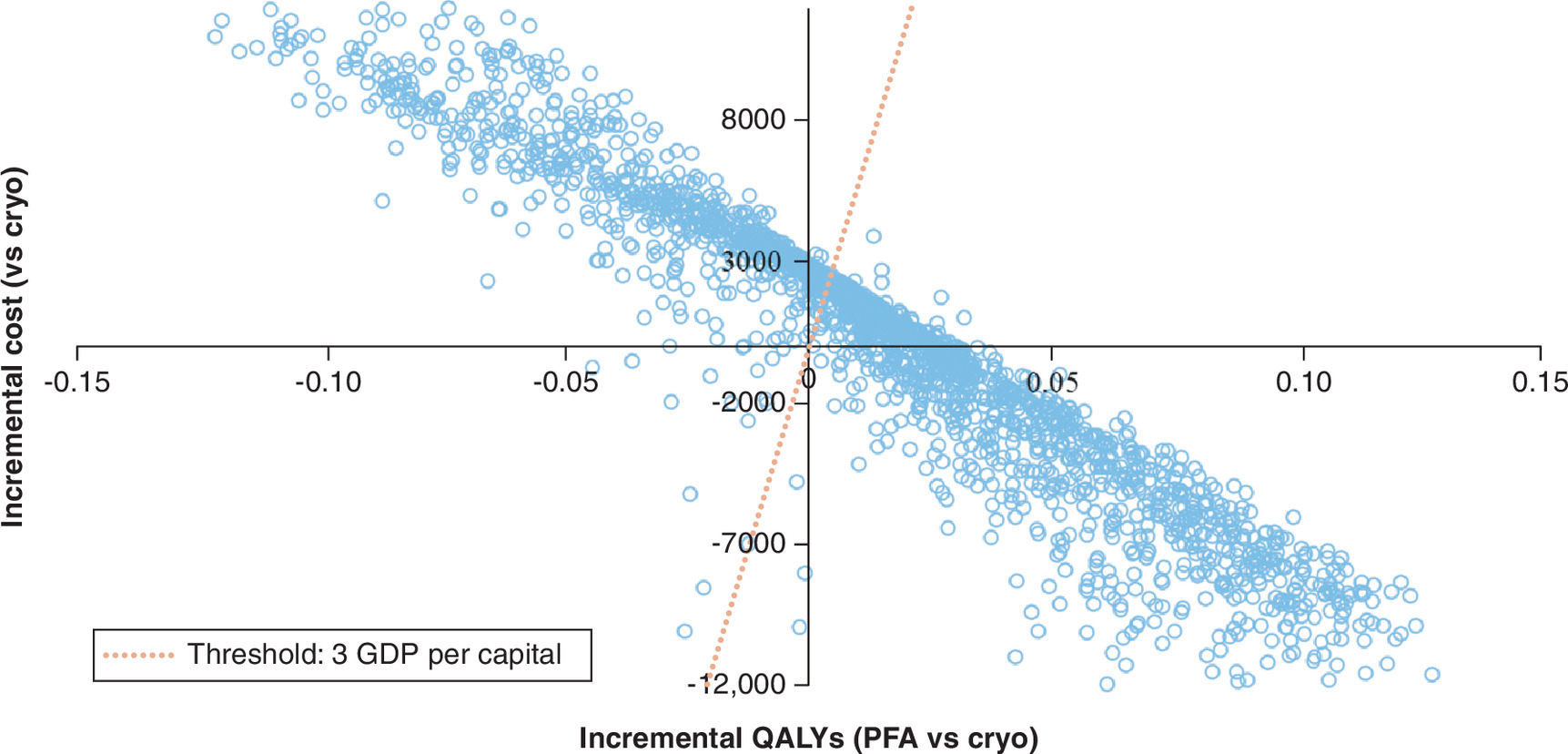
Figure 5. Incremental cost–effectiveness scatter plot for probabilistic sensitivity analysis (pulsed field ablation vs cryoablation).
Cryo: Cryoablation; PFA: Pulsed field ablation; QALY: Quality-adjusted life year.
ROI analysis
PFA generated the highest net monetary benefit (NMB = ¥19,387 per patient per ablation procedure), exceeding cryoablation (¥18,395) and RFA (¥17,000), despite higher upfront procedure costs (¥62,000 vs ¥59,000 for both comparators). This cost was more than offset by superior revenue generation (¥81,387 vs ¥76,000 and ¥77,395, respectively), yielding the highest ROI ratio of 31.27%, compared with 31.18% for cryoablation and 28.81% for RFA.
Discussion
This study employed a decision tree model from the perspective of the Chinese healthcare system to conduct a cost–effectiveness analysis of PFA, RFA and cryoablation as first-line treatments for patients with PAF. Our findings demonstrate that PFA is a highly cost-effective and financially viable alternative. Beyond these clinical and economic outcomes, these results carry significant practical relevance within the strategic framework of China’s ongoing medical service pricing reform. Under this initiative, the government is actively prioritizing the incorporation of innovative technologies into the ‘New Medical Service Price Items’ catalog to accelerate their clinical adoption. Currently, in many Chinese provinces, dedicated medical service pricing entries exist only for radiofrequency and cryoablation, while a specific billing code for PFA has yet to be established. This gap in the pricing catalog underscores the need for evidence-based data to justify PFA's clinical and economic value. By quantifying the long-term systemic savings and institutional benefits of PFA, our study provides a timely foundation for health security bureaus to justify the creation of an independent pricing entry. Such a value-based pricing strategy is essential to distinguish PFA from conventional methods, ensuring that its innovation-driven advantages are appropriately recognized and compensated within the evolving national healthcare landscape.
Our results demonstrate that PFA is more cost-effective than both RFA and cryoablation under the three-times China’s per capita GDP threshold. Although PFA incurred higher upfront procedural costs, its cost–effectiveness advantage is primarily attributed to its lower rates of post-procedure complications, decreased need for redo ablation and reduced incidence of nonfatal strokes. These factors contribute to offsetting savings in healthcare expenditures related to complication management, re-interventions and post-stroke care. In terms of health outcomes, PFA resulted in higher QALYs, primarily due to reduced disutility associated with redo ablation and stroke, as well as a higher proportion of patients reaching the optimal health state (<0.1% AA burden). While the ICERs indicate that PFA is not dominantly cost-effective, a recent clinical study demonstrates that even when clinical outcomes are evaluated without stratification by AA burden, PFA shows lower recurrence rates and improved quality of life outcomes [19]. Therefore, our economic evaluation model, which incorporated detailed AA burden stratification in assessing clinical outcomes, likely provides conservative estimates of PFA’s cost–effectiveness.
Key model parameters included redo ablation rates, the distribution of patients across different AA burden statuses following each ablation, and stroke incidence rates. A recent meta-analysis [20] demonstrated that PFA is associated with a 45% relative risk reduction in stroke compared with conventional thermal ablation. A retrospective study including over 17,000 cases reported a stroke incidence of 0.12% in patients with paroxysmal AF treated with PFA [5], and the CABANA trial [21] reported a post-ablation stroke rate of 0.3% following conventional thermal ablation. These findings are generally consistent with the relative risk assumptions for post-ablation stroke incidence across the three ablation methods used in our model.
Model results showed that the QALY differences between PFA and both RF and cryoablation were small. Also, the sensitivity analysis suggested that the utilities of different AA burden states were the main contributors to model sensitivity. This relatively small △QALY is expected, as the actual differences in quality-of-life improvements across ablation strategies appear to be limited. Consistent with this, the ADVENT trial [3] reported comparable quality-of-life improvements across the three ablation methods within each AA burden level, with AFEQT score differences within 5 points (out of a total of 100).
The efficacy end point in the model was based on AA burden rather than the traditional 30-second recurrence of AA. Studies have shown that the traditional gold standard for determining AF recurrence relies on intermittent monitoring, which can result in a recurrence rate error of 20–25% [22]. Additionally, several clinical trials [23,24] have demonstrated that continuous monitoring in catheter ablation allows AA burden to more comprehensively and objectively reflect treatment outcomes, correlating directly with healthcare resource utilization and quality of life. Therefore, the inclusion of AA burden in our model enables a more accurate calculation of both the cost and effectiveness of ablation in AF patients.
We also evaluated the ROI of PFA compared with RFA and cryoablation for a single ablation procedure in Chinese hospitals, demonstrating that PFA offers a superior financial return from a hospital perspective. With an ROI ratio of 0.313 and a NMB of ¥19,387 per patient per ablation procedure, PFA outperformed RFA (ROI: 0.288, NMB: ¥17,000) and cryoablation (ROI: 0.312, NMB: ¥18,395). The higher revenue (¥81,387 for PFA vs ¥76,000 for RFA and ¥77,395 for cryoablation) drove PFA’s economic advantage. These findings align with emerging evidence suggesting PFA’s efficiency in atrial fibrillation management, particularly in reducing procedural complications and subsequent healthcare utilization. The incremental NMB of ¥2387 for PFA over RFA reflects its potential to enhance hospital financial sustainability under Diagnosis-Related Groups reimbursement systems, a critical consideration in China’s healthcare reform context. Compared with prior studies, our results are consistent with analyses reporting PFA’s cost–effectiveness due to shorter procedure times and fewer adverse events, though most focus on payer or societal perspectives rather than hospital revenue.
There are also some limitations to this study that should be acknowledged. First, the cost–utility model simulated only one redo ablation within a 1-year time frame, which may lead to a conservative estimate of PFA’s incremental cost–effectiveness. The ADVENT study [3] demonstrated that the proportion of patients requiring redo ablation within 1 year is lower for PFA compared with thermal ablation. If this advantage of lower redo ablation rates for PFA compared with thermal ablation persists beyond the first year, and considering that the ablation procedure constitutes the majority of costs, the overall cost advantage of PFA would likely be even more pronounced. Therefore, by limiting the analysis to a single redo ablation, our model may actually underestimate the true cost–effectiveness of PFA. Second, due to the 1-year simulation period, the study does not capture costs and outcomes resulting from recurrence beyond 1 year post-ablation. This limitation was accepted after careful consideration. Most published studies about ablation follow patients for only 1 year. Beyond the first year, differences in outcomes between ablation techniques gradually diminish, as long-term results become more influenced by patient factors such as age, underlying cardiac conditions, comorbidities and medication adherence rather than the initial ablation method chosen. By limiting the model to 1 year, we reduce the uncertainty associated with long-term predictions.
Conclusion
From the perspective of the Chinese healthcare system, PFA demonstrates superior cost–effectiveness compared with RFA and cryoablation as first-line treatment for PAF. PFA is associated with fewer post-procedural complication expenses, reduced redo ablation costs, decreased nonfatal stroke management expenses and lower annual medication costs. PFA yielded an incremental 0.016 QALYs compared with RFA, and maintained comparable QALYs to cryoablation (slightly higher, 0.006). Sensitivity analyses confirmed the robustness of these findings. These results suggest PFA represents an economic first-line treatment option for PAF in China. Future research incorporating multi-year modeling and validation through long-term real-world clinical data will be essential to further substantiate these findings and evaluate the sustained economic impact of PFA over a patient's lifetime.
Summary points
•
Objective: First health economic evaluation in China comparing pulsed field ablation (PFA) against radiofrequency (RFA) and cryoablation (Cryo) for paroxysmal atrial fibrillation (PAF).
•
Method: A 1-year decision-tree model from the healthcare system perspective, simulating clinical pathways based on post-ablation atrial arrhythmia burden (AA burden) states.
•
Key results versus RFA: PFA gained 0.016 more uality-adjusted life years (QALYs) (0.859 vs 0.842) with an incremental cost–effectiveness ratio of ¥37,000/QALY – well below the cost–effectiveness threshold (¥287,247).
•
Key results versus Cryo: PFA gained 0.006 more QALYs (0.859 vs 0.852) with an incremental cost–effectiveness ratio of ¥231,167/QALY, also below the threshold.
•
Cost savings: PFA reduced redo ablation costs (¥1558 saved vs RFA; ¥1300 vs Cryo) and long-term medication costs (¥506 saved vs RFA; ¥133 vs Cryo).
•
Sensitivity analysis: Results were robust in probabilistic sensitivity analysis; PFA was cost-effective in 80% of simulations versus Cryo and dominant over RFA.
•
ROI outcome: From a hospital perspective, PFA had the highest return on investment (ROI = 0.313) and net monetary benefit (¥19,387 per procedure).
•
Conclusion: PFA is a cost-effective first-line treatment for PAF in China, offering better outcomes, lower complication-related costs and higher hospital returns.
Author contributions
J Ye, Y Fan and Y Wang were responsible for study conception and providing clinical data as clinical experts; Y Jian and Y Gao were responsible for study conception and design; Y Jian, Y Gao and S Chen were responsible for acquisition of data, model building and drafting and revision of the manuscript; J Xuan and H Hu were responsible for supervision of the project.
Acknowledgments
This work has been previously presented as two posters at: ISPOR 2025, Virtual, 13–16 May 2025; EE420, Y Fan, Y Wang, Y Gao, Y Jian, S Chen, J Xuan, H Hu. Compare the return on investment of pulsed field ablation with conventional thermal ablation for treatment of atrial fibrillation in China; and EE103, Y Fan, Y Wang, Y Gao, Y Jian, S Chen, J Xuan, H Hu. Cost–effectiveness analysis of pulsed field ablation versus RFA and cryoablation for PAF in China.
Financial disclosure
The authors have received no financial or material support for this research or the creation of this work.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
The authors have received no medical writing and editorial support or AI-assisted technologies for this research or the creation of this work.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Gao MY, He L, Du X et al. Epidemiology of atrial fibrillation in China: 20-year trends. Chin. J. Cardiol. 52(2), 220–226 (2024).
2.
Reddy VY, Gerstenfeld EP, Natale A et al. Pulsed field or conventional thermal ablation for paroxysmal atrial fibrillation. N. Engl. J. Med. 389(18), 1660–1671 (2023).
•• This randomized trial establishes that pulsed-field ablation is noninferior to thermal ablation for treating paroxysmal atrial fibrillation (PAF) and has a superior safety profile.
3.
Reddy VY, Mansour M, Calkins H et al. Pulsed field vs conventional thermal ablation for paroxysmal atrial fibrillation: recurrent atrial arrhythmia burden. J. Am. Coll. Cardiol. 84(1), 61–74 (2024).
•• This analysis shows that pulsed-field ablation significantly reduced the burden of recurrent atrial arrhythmias (AA) compared to conventional thermal ablation.
4.
China NBoSo. Major Figures on 2020 Population Census of China. China Statistics Press (2021).
5.
Ekanem E, Neuzil P, Reichlin T et al. Safety of pulsed field ablation in more than 17,000 patients with atrial fibrillation in the MANIFEST-17K study. Nat. Med. 30(7), 2020–2029 (2024).
• This large-scale real-world study of over 17,000 patients established the safety of pulsed-field ablation for atrial fibrillation (AF), demonstrates a very low rate of major complications.
6.
Go AS, Reynolds K, Yang J et al. Association of burden of atrial fibrillation with risk of ischemic stroke in adults with paroxysmal atrial fibrillation: the KP-RHYTHM Study. JAMA Cardiol. 3(7), 601–608 (2018).
7.
Wang Z, Tang M, Reddy VY et al. Efficacy and safety of a novel hexaspline pulsed field ablation system in patients with paroxysmal atrial fibrillation: the PLEASE-AF study. Europace 26(7), euae174 (2024).
8.
Ming J, Wei Y, Sun H et al. Cost-effectiveness of cryoballoon ablation versus radiofrequency ablation for paroxysmal atrial fibrillation in China: results based on real-world data. Value Health 22(8), 863–870 (2019).
9.
Sun XR, He SN, Lin ZY et al. Radiofrequency catheter ablation versus cryoballoon ablation in the treatment of paroxysmal atrial fibrillation: a cost-effectiveness analysis in China. Clin. Ther. 41(1), 78–91 (2019).
10.
Fortuni F, Casula M, Sanzo A et al. Meta-analysis comparing cryoballoon versus radiofrequency as first ablation procedure for atrial fibrillation. Am. J. Cardiol. 125(8), 1170–1179 (2020).
11.
Darvishi A, Sadeghipour P, Darrudi A et al. Cost-utility analysis of Cryoballoon ablation versus Radiofrequency ablation in the treatment of paroxysmal atrial fibrillation in Iran. PLoS One 17(7), e0270642 (2022).
12.
Punekar YS, Shukla A, Mullerova H. COPD management costs according to the frequency of COPD exacerbations in UK primary care. Int. J. Chron. Obstruct. Pulmon. Dis. 9, 65–73 (2014).
13.
Du X, He X, Jia Y et al. A long-term cost-effectiveness analysis comparing radiofrequency catheter ablation with antiarrhythmic drugs in treatment of Chinese patients with atrial fibrillation. Am. J. Cardiovasc. Drugs 19(6), 569–577 (2019).
14.
Lee HY, Hwang JS, Jeng JS et al. Quality-adjusted life expectancy (QALE) and loss of QALE for patients with ischemic stroke and intracerebral hemorrhage: a 13-year follow-up. Stroke 41(4), 739–744 (2010).
15.
Sawyer LM, Witte KK, Reynolds MR et al. Cost-effectiveness of an insertable cardiac monitor to detect atrial fibrillation in patients with cryptogenic stroke. J. Comp. Eff. Res. 10(2), 127–141 (2021).
16.
Reynolds MR, Zimetbaum P, Josephson ME et al. Cost-effectiveness of radiofrequency catheter ablation compared with antiarrhythmic drug therapy for paroxysmal atrial fibrillation. Circ. Arrhythm Electrophysiol. 2(4), 362–369 (2009).
17.
Aronsson M, Walfridsson H, Janzon M et al. The cost-effectiveness of radiofrequency catheter ablation as first-line treatment for paroxysmal atrial fibrillation: results from a MANTRA-PAF substudy. Europace 17(1), 48–55 (2015).
18.
Lau D, Sandhu RK, Andrade JG et al. Cost-utility of catheter ablation for atrial fibrillation in patients with heart failure: an economic evaluation. J. Am. Heart Assoc. 10(14), e019599 (2021).
19.
Reichlin T, Kueffer T, Badertscher P et al. Pulsed field or cryoballoon ablation for paroxysmal atrial fibrillation. N. Engl. J. Med. 392(15), 1497–1507 (2025).
•• Pulsed-field ablation was noninferior to cryoballoon ablation in efficacy for PAF and proved safer.
20.
Amin AM, Nazir A, Abuelazm MT et al. Efficacy and safety of pulsed-field versus conventional thermal ablation for atrial fibrillation: a systematic review and meta-analysis. J. Arrhythm. 40(5), 1059–1074 (2024).
•• This systematic review and meta-analysis found pulsed-field ablation to be as effective as, but safer than, conventional thermal ablation in treating AF.
21.
Packer DL, Mark DB, Robb RA et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA 321(13), 1261–1274 (2019).
22.
Verma A, Haines DE, Boersma LV et al. Influence of monitoring and atrial arrhythmia burden on quality of life and health care utilization in patients undergoing pulsed field ablation: a secondary analysis of the PULSED AF trial. Heart Rhythm 20(9), 1238–1245 (2023).
• The secondary analysis found that symptoms were a poor indicator of actual AA burden after pulsed-field ablation, highlighting the limitation of symptom-based follow-up.
23.
Terricabras M, Mantovan R, Jiang CY et al. Association between quality of life and procedural outcome after catheter ablation for atrial fibrillation: a secondary analysis of a randomized clinical trial. JAMA Netw. Open. 3(12), e2025473 (2020).
• This analysis shows that improved quality of life after AF ablation was linked to a reduction in symptom burden, rather than procedural success alone.
24.
Andrade JG, Deyell MW, Macle L et al. Healthcare utilization and quality of life for atrial fibrillation burden: the CIRCA-DOSE study. Eur. Heart J. 44(9), 765–776 (2023).
• This analysis found a direct relationship between AF burden and both increased use of healthcare resources and worse patient-reported quality of life.
Information & Authors
Information
Published In
Copyright
© 2026 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 25 September 2025
Accepted: 26 March 2026
Published online: 29 April 2026
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Health economic analysis of pulsed field ablation compared to conventional thermal ablation for patients with paroxysmal atrial fibrillation in China. (2026) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0153
Export citation
Select the citation format you wish to export for this article or chapter.