Long-term efficacy and safety of lorlatinib versus alectinib in anaplastic lymphoma kinase-positive advanced/metastatic non-small cell lung cancer: matching-adjusted indirect comparison
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Lorlatinib demonstrated superior efficacy over alectinib as a first-line treatment for ALK-positive (ALK+) advanced/metastatic non-small cell lung cancer in a matching-adjusted indirect comparison (MAIC) using 3-year follow-up data from CROWN (lorlatinib). This study aimed to update these findings using the latest extended 5-year follow-up data from CROWN. Materials & methods: We conducted an anchored MAIC using data from CROWN and ALEX (alectinib). Patients were matched based on prespecified effect modifiers. We compared progression-free survival (PFS) using hazard ratios (HRs), restricted mean survival time and PFS probabilities and adverse events (AEs) using rate ratios and rate differences. PFS was analyzed in subgroups with and without baseline brain/CNS metastases. Results: Lorlatinib demonstrated superior PFS over alectinib, reducing the risk of progression or death by 45% (HR: 0.55, 95% CI: 0.34, 0.88). Lorlatinib extended restricted mean survival time by 8.5 months up to 4 years and 11.2 months up to 5.5 years, with generally higher annual PFS probabilities across years 1–5. While lorlatinib was associated with a higher incidence of grade ≥3 AEs, the rates of AEs leading to treatment discontinuation, dose interruption and dose reduction were similar between the treatments. In patients with baseline brain/CNS metastases, lorlatinib showed a numerical PFS benefit, with significant improvement at year 1. In patients without brain/CNS metastases, lorlatinib significantly improved PFS, with significant increases at years 2–4. Conclusion: This extended analysis reaffirms lorlatinib’s superior efficacy over alectinib in prolonging PFS. Despite the higher grade ≥3 AE incidence, similar rates of dose reduction, interruption, or discontinuation suggest these AEs are manageable. Lorlatinib remains a first-line treatment option for ALK+ metastatic non-small cell lung cancer, offering meaningful benefits to appropriate patients.
Plain language summary: Long-term efficacy & safety of lorlatinib versus alectinib in anaplastic lymphoma kinase-positive advanced/metastatic non-small cell lung cancer: matching-adjusted indirect comparison
What is already known about this subject?
Lorlatinib and alectinib are both recommended first-line treatment options for anaplastic lymphoma kinase (ALK+) metastatic non-small cell lung cancer. In the absence of a head-to-head randomized clinical trial directly comparing the efficacy and safety of these two treatments, indirect treatment comparisons, such as matching-adjusted indirect comparisons (MAIC), can help inform healthcare decision-making.
In a previous MAIC using 3-year follow-up data from the CROWN trial, lorlatinib outperformed alectinib in progression-free survival (PFS) for ALK+ metastatic non-small cell lung cancer.
What are the new findings?
Our updated MAIC based on extended follow-up data from the CROWN trial confirms lorlatinib’s PFS superiority over alectinib, showing a 45% reduction in the risk of progression or death.
Lorlatinib extended the restricted mean survival time by up to 11.2 months and maintained higher annual PFS probabilities over 5 years.
Lorlatinib significantly improved PFS in patients without baseline brain/CNS metastases and showed a numerical PFS benefit in those with baseline brain/CNS metastases, with significant improvement at year 1.
While lorlatinib had a higher incidence of grade ≥3 adverse events (AEs), rates of AEs leading to dose reduction, interruption or discontinuation were similar to alectinib.
How might it impact clinical practice in the foreseeable future?
The updated findings support lorlatinib as an effective first-line treatment option for ALK+ advanced/metastatic NSCLC, offering significant improvements in PFS and manageable AEs compared with alectinib.
Over the past decade, anaplastic lymphoma kinase tyrosine kinase inhibitors (ALK TKIs) have become the recognized standard of care for the first-line treatment of ALK-positive (ALK+) advanced or metastatic non-small cell lung cancer (mNSCLC) [1]. Crizotinib, a first-generation ALK TKI, was the first ALK TKI approved for this indication [2]. While crizotinib demonstrated efficacy in targeting ALK+ tumors compared with chemotherapy, it was eventually surpassed by next-generation treatments, including second-generation (e.g., alectinib [3–6] and brigatinib [7,8]) and third-generation (e.g., lorlatinib [9,10]) ALK TKIs. These next-generation ALK TKIs, which have demonstrated superiority over crizotinib as a first-line treatment for patients with ALK+ mNSCLC, are recommended as preferred first-line treatment options [1,3–8].
In the phase III CROWN trial, lorlatinib demonstrated superiority over crizotinib, with longer progression-free survival (PFS) and higher response rates. However, lorlatinib was associated with more grade ≥3 adverse events (AEs) [9,10]. Similarly, in the phase III ALEX trial, alectinib was superior to crizotinib in prolonging PFS, with fewer grade ≥3 AEs [3]. However, to date, no clinical trials have directly compared lorlatinib to alectinib as first-line treatments for ALK+ mNSCLC. Existing indirect treatment comparisons (ITCs) are outdated, based on earlier clinical trial data cuts, or do not adjust for differences in baseline characteristics [11–18]. These previous studies using unadjusted ITCs [11] or network meta-analyses [12,13,15] have shown that lorlatinib offers superior PFS and CNS progression benefits compared with other ALK inhibitors, but with higher toxicity, while alectinib provides a favorable safety profile. However, these studies lack direct comparison and adjustment for baseline differences, limiting their applicability. Therefore, robust comparative effectiveness studies are needed to generate relative efficacy and safety data on these next-generation medications to aid in physician prescribing, patient preference and payer reimbursement decisions. A previous matching-adjusted indirect comparison (MAIC) derived comparative estimates for lorlatinib versus alectinib in ALK+ mNSCLC using 3-year follow-up data from the CROWN trial (data cuts: 20 March 2020 and 20 September 2021) and ALEX (data cuts: 30 November 2018 and 29 November 2019) trial. The analysis demonstrated superior efficacy outcomes for lorlatinib compared with alectinib, which showed a significant benefit in PFS and numerically improved time to progression in the central nervous system (TTP-CNS) over alectinib, although lorlatinib was associated with a higher rate of grade ≥3 AEs [18]. However, given the recent availability of 5-year follow-up data from the CROWN trial, there is a need to reassess the comparative efficacy and safety of lorlatinib and alectinib using these extended follow-up data. These updated results with approximately 2 years of additional follow-up provide more reliable estimates of the long-term efficacy and safety of lorlatinib versus alectinib.
This study aimed to address this gap by updating the findings of the previous MAIC analysis using 5-year follow-up data from the latest CROWN data cut (released 31 October 2023). Specifically, this study aimed to compare lorlatinib to alectinib in terms of PFS over the extended follow-up period and assess differences in safety profiles between lorlatinib and alectinib in both the global population and subpopulations of patients with and without baseline brain/CNS metastases.
Materials & methods
This MAIC compared the efficacy and safety of lorlatinib versus alectinib following the methodology outlined in Garcia et al. [18]. A summary of the data sources used, populations/subpopulations considered, and outcomes assessed is presented in Table 1. Additional details regarding the methodology are presented in the Supplementary Material.
| Data cuts | Population/subgroup | Outcomes (relative effect measures) |
|---|---|---|
| Efficacy outcomes | ||
| CROWN: 31 October 2023† ALEX: 30 November 2018‡ | ITT: CROWN: lorlatinib [n = 139]; crizotinib [n = 137] ALEX: alectinib [n = 152]; crizotinib [n = 151] | Efficacy: PFS-INV (HR; RR/RD of PFS probabilities at years 1–5; ratio/difference of RMST PFS time up to year 4; ratio/difference of RMST PFS time up to maximum follow-up of CROWN) |
| Brain metastases subgroup: CROWN: lorlatinib [n = 35]; crizotinib [n = 37] ALEX: alectinib [n = 64]; crizotinib [n = 58] | Efficacy: PFS-INV (HR; RR/RD in PFS probabilities at years 1–4) | |
| No brain metastases subgroup: CROWN: lorlatinib [n = 104]; crizotinib [n = 100] ALEX: alectinib [n = 88]; crizotinib [n = 93] | ||
| Safety outcomes | ||
| CROWN: 31 October 2023† ALEX: 29 November 2019§ | ITT: CROWN: lorlatinib [n = 139]; crizotinib [n = 132] ALEX: ITT alectinib [n = 152]; crizotinib [n = 151] | Safety: Grade ≥3 AEs, AEs leading to discontinuation/dose reduction/dose interruption (RR/RD) |
†
The data cut-off date for the CROWN trial was 31 October 2023, with a median follow-up period for PFS of 60.2 months for patients treated with lorlatinib and 55.1 months for those treated with crizotinib.
‡
The data cut-off date for the ALEX trial was 30 November 2018, with a median follow-up period for PFS of 37.8 months for patients treated with alectinib and 23.0 months for those treated with crizotinib.
§
The data cut-off date for the ALEX trial was 29 November 2019, with a median follow-up period for OS of 48.2 months for patients treated with alectinib and 23.3 months for those treated with crizotinib.
AE: Adverse event; HR: Hazard ratio; ITT: Intention to treat; OS: Overall survival; PFS-INV: Progression-free survival assessed by investigator; PFS: Progression-free survival; RD: Rate difference; RMST: Restricted mean survival time; RR: Rate ratio.
Analysis population & subgroups
The ALEX trial [6] was selected to provide long-term efficacy and safety data for alectinib, while individual patient level data (IPD) for lorlatinib were sourced from the CROWN trial [9,10]. The analyses considered both the intention-to-treat (ITT) population and subpopulations with and without baseline brain/CNS metastases. The subgroup analysis of patients with baseline brain/CNS metastases was planned and conducted as an exploratory analysis due to the relatively small sample size in the CROWN trial. Data from CROWN patients enrolled at Chinese sites (n = 20, 6.8%) were excluded from the MAIC due to country-specific privacy restrictions.
Variable matching
IPD from the CROWN trial were re-weighted such that the summary statistics of the baseline characteristics of patients in the lorlatinib arm matched those in the alectinib arm of the ALEX trial and the baseline characteristics of patients in the crizotinib arm in the CROWN trial matched those in the crizotinib arm in the ALEX trial. A single matching set was used based on the primary matching set from Garcia et al. [18], which included the most clinically important effect modifiers (EMs), as determined by a targeted literature review, assessment of quantitative evidence and consultation with clinical experts. These EMs included Eastern Cooperative Oncology Group Performance Score of 0 versus 1+, presence of brain/CNS metastases at baseline per independent review committee, and race (Asian vs non-Asian). In the CROWN trial, ethnicity was used as a proxy for missing race data. Only Asian versus non-Asian categories were considered.
Statistical analysis
We updated the MAIC with the aim to generate robust long-term comparative data and explore new effect measures with clinically meaningful interpretations. In addition to quantifying the effect of treatment in terms of the hazard ratio (HR) for PFS assessed by investigator (INV), the differences and ratios in restricted mean survival time (RMST) up to a prespecified timepoint and annual probabilities were considered to relax the proportional hazards assumption and provide additional comparative evidence that is more easily understood than the HR. AEs were compared based on rate ratios (RRs) and rate differences (RDs).
In the MAICs comparing PFS, observed Kaplan–Meier (KM) data were used where possible. PFS-INV with alectinib in ALEX was extrapolated to facilitate an MAIC using 5-year PFS data. The last observed PFS probability at year 4 (and its associated standard error [SE]) with alectinib was conservatively assumed to be constant until year 5 given the observed plateau in the KM curve. Parametric survival models were required to extrapolate PFS from years 2–4 for crizotinib (CROWN) in the brain metastases subgroup, as the observed KM curve reached 0% at approximately 22 months. Seven parametric distributions commonly recommended by health technology assessment bodies, including the National Institute for Health and Care Excellence (NICE) [19] and the Canadian Agency for Drugs and Technologies in Health (CADTH) [20] (i.e., exponential, Weibull, Gompertz, log-normal, log-logistic, gamma and generalized gamma) were tested as candidate models. The parametric model that predicted year 2–4 PFS probabilities closest to zero (without truly reaching zero) was selected for the primary analysis.
Results
The adjusted results of the MAIC are presented in the following sections, and unadjusted results are presented alongside the adjusted results in Figures 1–3.
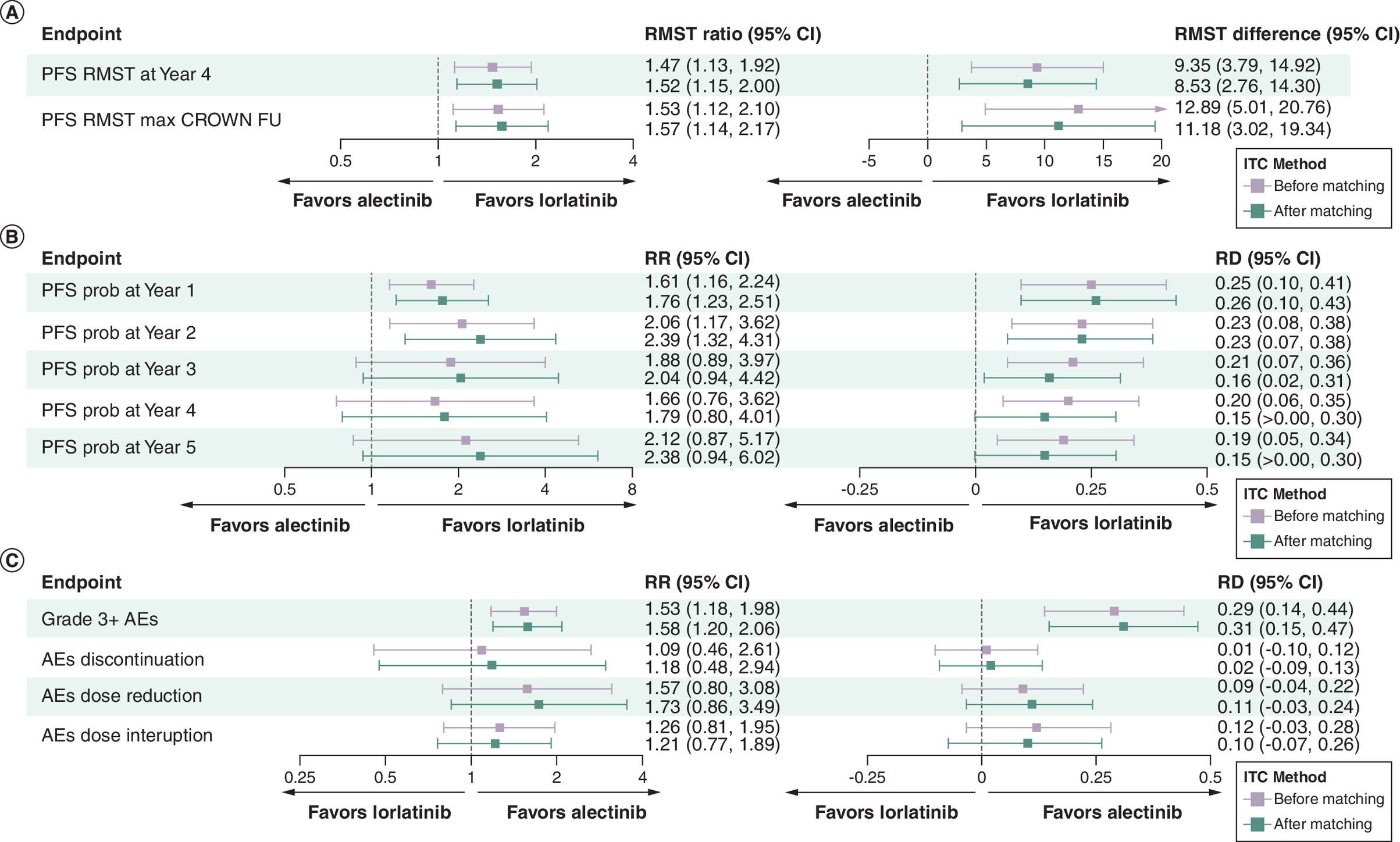
Figure 1. Matching-adjusted indirect comparison results: lorlatinib (CROWN) versus alectinib (ALEX) in the intention-to-treat population.
(A) PFS RMST. (B) PFS probabilities. (C) Safety endpoints. The difference in RMST is presented in months. RMST up to max CROWN follow-up: PFS-INV for alectinib and crizotinib (ALEX) was extrapolated to facilitate an MAIC on 66-month PFS data (i.e., minimum of maximum follow-up in CROWN). The last observed PFS probability at approx. year 4 (and its associated SE) for alectinib and crizotinib was conservatively assumed constant until month 66, given the observed plateau in the KM curve. PFS probability at year 5: PFS-INV for alectinib and crizotinib (ALEX) was extrapolated to facilitate an MAIC on 5-year PFS data. The last observed PFS probability at year 4 (and its associated SE) for alectinib and crizotinib (ALEX) was conservatively assumed constant until year 5, given the observed plateau in the KM curve.
AE: Adverse event; CI: Confidence interval; FU: Follow-up; ITC: Indirect treatment comparison; KM: Kaplan–Meier; MAIC: Matching-adjusted indirect comparisons; PFS-INV: Progression-free survival assessed by investigator; PFS: Progression-free survival; Prob: Probability; RD: Rate difference; RMST: Restricted mean survival time; RR: Rate ratio.
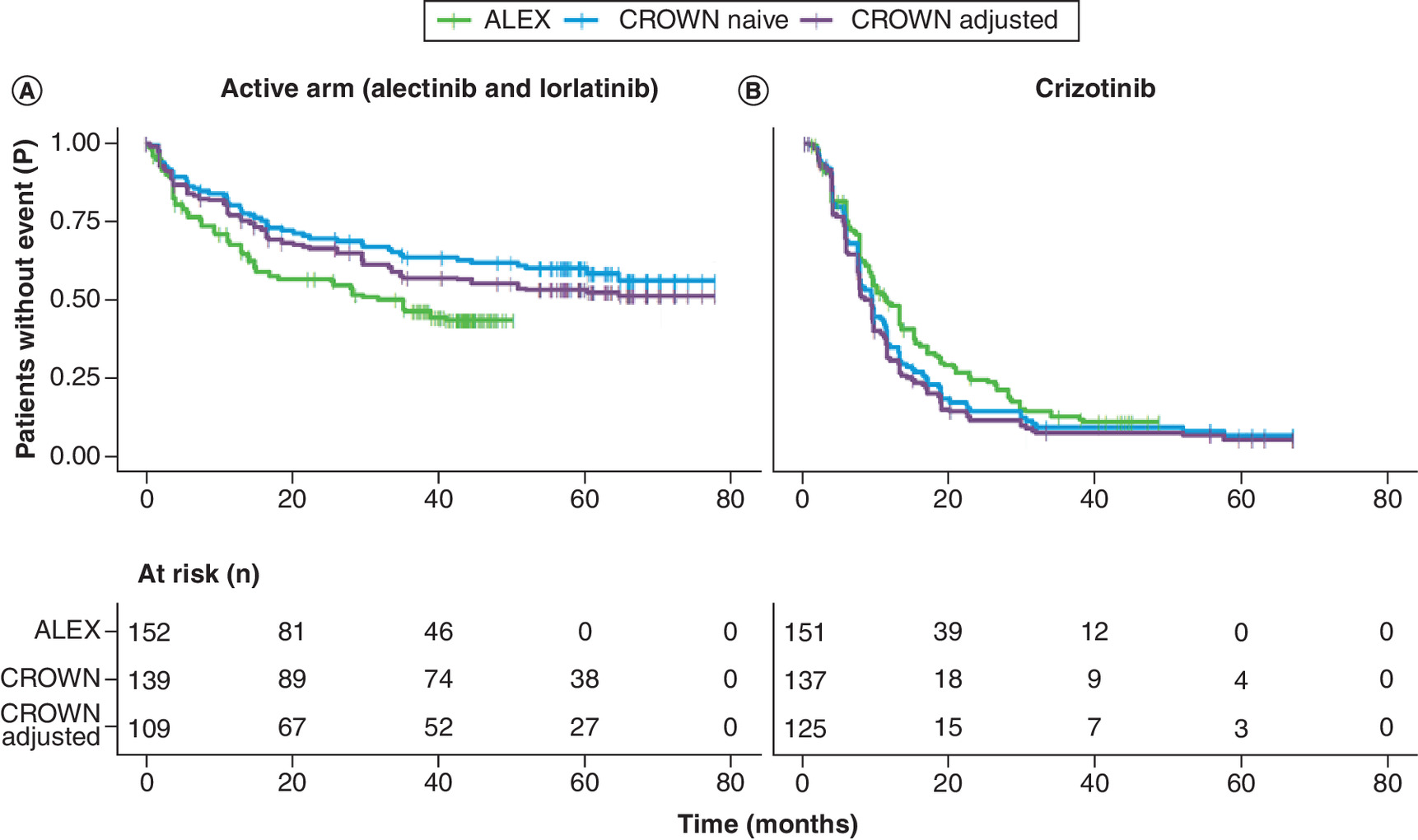
Figure 2. Kaplan–Meier curves for progression-free survival assessed by investigator before (naive) and after adjustment.
(A) Active arm (alectinib and lorlatinib). (B) Crizotinib.
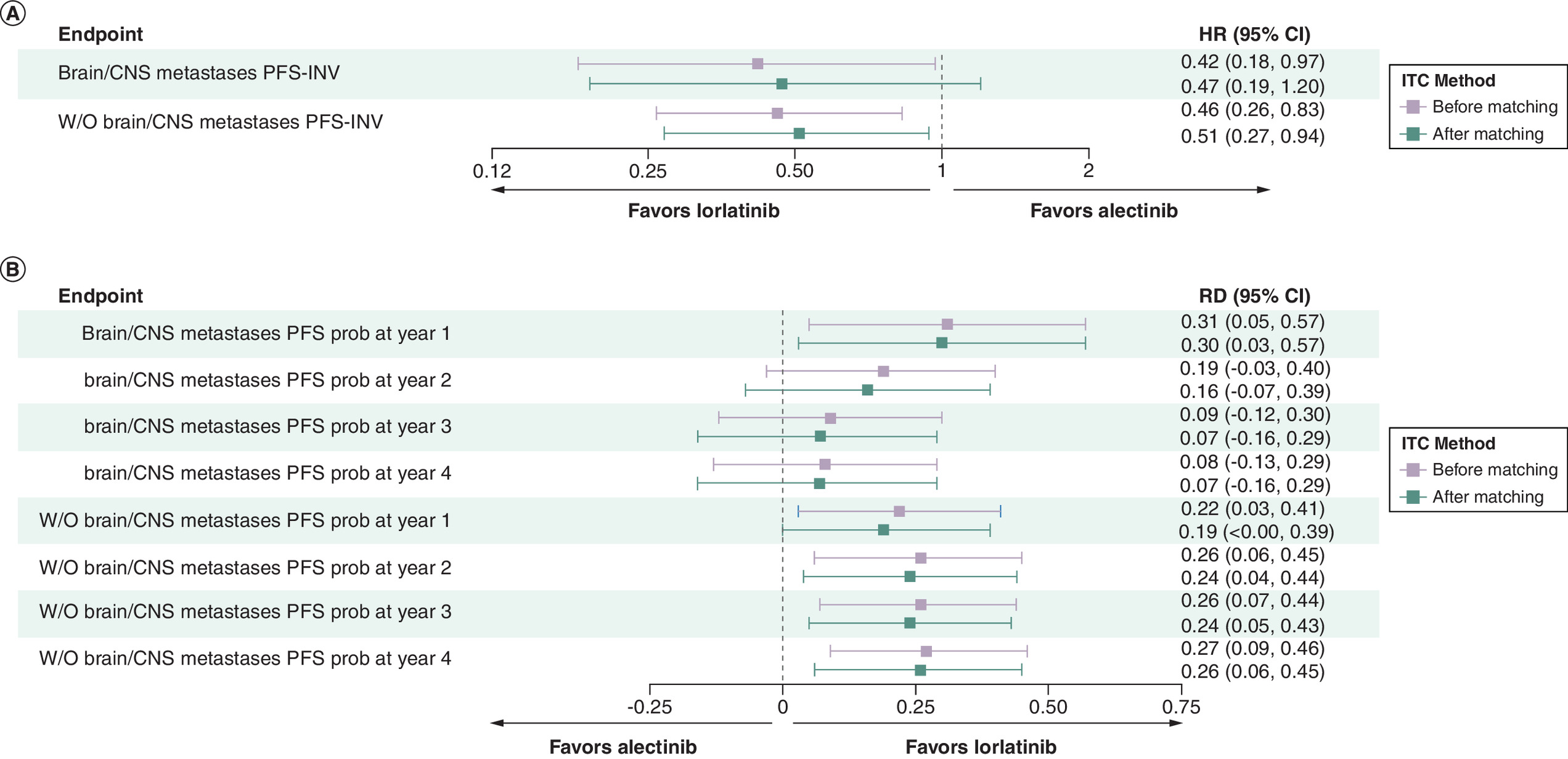
Figure 3. Matching-adjusted indirect comparison results: Lorlatinib (CROWN) versus alectinib (ALEX) in subpopulations with and without baseline brain/CNS metastases.
(A) PFS-INV. (B) PFS probabilities. PFS-INV for crizotinib (ALEX trial) was extrapolated to facilitate an MAIC on 4-year PFS data. The last observed PFS probability at year 3 (and its associated SE) for crizotinib was conservatively assumed constant until year 4, given the observed plateau in the KM curve. Parametric Weibull curves were fitted for crizotinib (CROWN) so that PFS probabilities at years 2–4 could be extrapolated and compared in the MAIC.
CI: Confidence interval; CNS: Central nervous system; HR: Hazard ratio; ITC: Indirect treatment comparison; KM: Kaplan–Meier; MAIC: Matching-adjusted indirect comparisons; PFS-INV: Progression-free survival assessed by investigator; PFS: Progression-free survival; Prob: Probability; RD: Rate difference; RR: Rate ratio; W/O: Without.
Population matching
Population matching was successful, and additional results, including the baseline characteristics and sample sizes before and after matching, are presented by Garcia et al. The effective sample sizes (ESS) after matching on EMs across studies were 108.62 (of n = 139 [78%]) and 125.46 (of n = 137 [92%]) for lorlatinib and crizotinib, respectively.
Efficacy
Lorlatinib demonstrated superior PFS-INV compared with alectinib (HR: 0.55, 95% CI: 0.34, 0.88), with a reduction in the risk of progression or death of 45%. Additionally, the mean PFS time (RMST up to 4 and 5.5 years [66 months]) in the lorlatinib arm was statistically superior to that in the alectinib arm. The difference in the RMST ranged from 8.5 months (RMST up to 4 years) to 11.2 months (RMST up to 5.5 years), resulting in an RMST approximately 1.5–1.6-times higher with lorlatinib compared with alectinib. Specifically, lorlatinib extended the mean PFS time by 8.5 months up to year 4 (RMST difference: 8.53, 95% CI: 2.76, 14.30; RMST ratio: 1.52, 95% CI: 1.15, 2.00) and by an even greater margin by year 5 (RMST difference: 11.18, 95% CI: 3.02, 19.34; RMST ratio: 1.57, 95% CI: 1.14, 2.17) compared with alectinib (Figure 1A). Furthermore, the PFS probabilities at years 1–5 were also significantly improved in terms of RDs with lorlatinib versus alectinib, ranging from 0.15 to 0.26 increases in annual PFS probabilities. The greatest difference in the annual PFS probability was observed at year 1 (0.26 [0.10, 0.43]), and by years 4–5, the estimated annual difference in PFS was 0.15 (>0.00, 0.30) (Figure 1B). The KM curves for PFS-INV before and after adjustment are presented in Figure 2A & B. The PFS-INV curve for lorlatinib was higher (i.e., more favorable) than that of alectinib both before and after the population adjustment, although KM curve for lorlatinib was higher before the adjustment compared with after the adjustment.
Safety
Lorlatinib had a higher rate of grade ≥3 AEs (RD: 0.31, 95% CI: 0.15, 0.47; RR: 1.58, 95% CI: 1.20, 2.06) compared with alectinib. However, the rates of AEs leading to treatment discontinuation (RD: 0.02, 95% CI: -0.09, 0.13; RR: 1.18, 95% CI: 0.48, 2.94), dose interruption (RD: 0.10, 95% CI: -0.07, 0.26; RR: 1.21, 95% CI: 0.77, 1.89), and dose reduction (RD: 0.11, 95% CI: -0.03, 0.24; RR: 1.73, 95% CI: 0.86, 3.49) were similar between the two treatments (Figure 1C).
Brain/CNS metastases subgroup analysis
Among patients with baseline brain/CNS metastases (ESS = 64.41 of n = 72), lorlatinib demonstrated a benefit in PFS-INV compared with alectinib (HR: 0.47, 95% CI: 0.19, 1.20), although this result was not statistically significant given the small sample size in this cohort. Among patients without baseline brain/CNS metastases (ESS = 195.19 of n = 204), lorlatinib demonstrated superior PFS-INV compared with alectinib (HR: 0.51, 95% CI: 0.27, 0.94) (Figure 3A).
Among patients with baseline brain/CNS metastases, at year 1, lorlatinib significantly improved PFS (RD: 0.30, 95% CI: 0.03, 0.57). A numerical benefit in the annual PFS probability was observed in the remaining time periods, although these results were not statistically significant, presumably due to the small sample sizes and event counts. Meanwhile, among patients without baseline brain/CNS metastases, at year 1, lorlatinib was associated with a higher PFS compared with alectinib (RD: 0.19, 95% CI: -0.003, 0.39), although this result was not statistically significant. Over time, lorlatinib continued to show a consistent improvement in PFS, maintaining its advantage over alectinib and demonstrating a significant increase in PFS probabilities at years 2–4 (year 4 difference: 0.26, 95% CI: 0.06, 0.45) (Figure 3B).
Discussion
This study sought to determine whether lorlatinib demonstrates superior PFS compared with alectinib over an extended follow-up period and to assess differences in the safety profiles between lorlatinib and alectinib in both the global population and subpopulations of patients with and without baseline brain/CNS metastases. The findings show that lorlatinib demonstrated superior PFS compared with alectinib, as evidenced by the significant reduction in the hazard of progression or death (measured by the PFS-INV HR) and further supported by the significant results in favor of lorlatinib across the RMST and annual PFS probability estimates. In the overall population, lorlatinib demonstrated superior PFS compared with alectinib, with an advantage observed at each time point examined. In patients with baseline brain/CNS metastases, lorlatinib showed a benefit in PFS, which was significant at year 1 only, despite these comparisons likely being underpowered due to the small sample sizes. In patients without baseline brain/CNS metastases, lorlatinib demonstrated improvement in PFS, with significant improvements observed at years 2–4, compared with alectinib.
In the phase III CROWN trial, despite the higher incidence of grade ≥3 AEs with lorlatinib, patients experienced significant improvements in quality of life and functioning scores compared with baseline. Most AEs were manageable through dose modifications and medications, allowing the clinical benefits of lorlatinib to outweigh the negative impact of these AEs. Furthermore, these improvements were sustained throughout the study period, indicating durable benefits despite grade ≥3 AEs [21].
In our analysis, while lorlatinib was associated with a higher incidence of grade ≥3 AEs compared with alectinib, no statistically significant differences were observed in other safety end points, such as AEs leading to treatment discontinuation, dose reduction, and dose interruption. The lack of increased discontinuations or dose reductions suggests that, despite the higher rate of grade ≥3 AEs, these AEs are manageable. According to guidelines, lorlatinib-associated AEs can be effectively controlled through dose modifications or the use of additional therapies [22,23]. Specifically, lipid-lowering therapy can be used to manage hyperlipidemia (the most common AE associated with lorlatinib), dose modifications can be applied to manage CNS effects, and standard of care or dose modifications can be used for the management of other AEs, which tend to be mild to moderate [22–24].
Overall, the findings of this long-term MAIC were consistent with the results reported by Garcia et al. [18]. This updated MAIC analysis, using the latest CROWN data cut, further bolsters the totality of evidence on the comparative efficacy and safety of lorlatinib as a first-line treatment for ALK+ mNSCLC versus alectinib. The consistent findings across different measures in the ITT and subgroups reinforce the robustness of lorlatinib's clinical benefits in the entire population of patients with ALK+ mNSCLC regardless of the presence of brain/CNS metastases at baseline. Particularly for PFS, the HRs, RMST and annual PFS probabilities consistently favored lorlatinib over alectinib, indicating lorlatinib’s superiority across multiple, complementary metrics. Interpreting different estimates for PFS, such as HRs and RMST, provides a more holistic understanding of treatment efficacy as HRs offer insight into the relative risk of progression or death, while RMSTs provide absolute measures of time patients remain progression-free, enhancing the clinical relevance of the findings.
Given the high prevalence of brain metastases among ALK+ mNSCLC patients, these results are particularly noteworthy. Patients with ALK+ mNSCLC frequently present with brain metastases, with nearly a third of cases diagnosed at this advanced stage and face a significant risk of developing brain metastases [25]. Lorlatinib has proven effective in improving treatment responses in patients with brain metastases, including extending the TTP-CNS [26]. The results of this updated analysis suggest a trend toward improved efficacy of lorlatinib in this subpopulation, demonstrating supportive evidence of improvements in PFS-INV. Furthermore, lorlatinib had superior PFS-INV compared with alectinib in the subgroup of patients without baseline brain/CNS metastases, and these improvements in PFS-INV were sustained over the entire follow-up period of 4 years. This highlights the utility of lorlatinib as a first-line treatment in the overall population of patients with ALK+ mNSCLC.
Overall, the results were largely expected given the known efficacy of lorlatinib in targeting ALK+ tumors and the findings of the previous MAIC analysis by Garcia et al. [18]. The superiority of next-generation ALK TKIs over crizotinib, as established in various clinical trials, supports these findings [1,3–8]. The efficacy results are further supported by previous unadjusted ITCs [11] and network meta-analyses [12,13,15]. The significant benefit observed in patients with baseline brain/CNS metastases at year 1 was particularly noteworthy, as this subgroup often presents a more challenging treatment scenario [25,26]. The observation that lorlatinib's benefit in this subgroup was significant only at year 1 was an unexpected finding but is likely due to the small sample size of patients with baseline brain/CNS metastases in the CROWN trial, which could have limited the statistical power to detect significant differences beyond the first year. In terms of safety, our study confirms that lorlatinib is associated with a higher incidence of grade ≥3 AEs compared with alectinib [11,12,15]. However, we found no statistically significant differences in other safety end points, such as treatment discontinuation, dose reduction and dose interruption, suggesting that these AEs are manageable. Our analysis supports previous findings and provides a more comprehensive and updated evaluation using the latest CROWN data cut, reinforcing the robustness of lorlatinib’s clinical benefits and highlighting its potential as a first-line treatment for ALK+ mNSCLC.
Future research
As the treatment landscape continues to evolve, future research exploring the biological mechanisms underlying the efficacy of ALK+ mNSCLC treatments has the potential to provide a more comprehensive understanding of how these mechanisms influence clinical outcomes and help refine treatment strategies. Further research with larger sample sizes of patients with baseline brain/CNS metastases and longer follow-up periods is needed to confirm the long-term benefits of lorlatinib in this specific subgroup and to better understand the dynamics of its efficacy over time.Our study primarily focused on PFS and did not consider overall survival (OS) because at the time of the analysis, the required number of OS events per the protocol-specified second interim analysis in the CROWN trial had not been reached. OS follow-up research is ongoing, and additional OS analyses are planned. Future research should continue to monitor OS to provide a more complete picture of the long-term benefits of ALK+ mNSCLC treatments and to validate these findings. This ongoing OS analysis will be crucial for understanding the full impact of these treatments on patient survival and guiding future treatment protocols.
Additionally, understanding economic implications is crucial for optimizing treatment decisions and ensuring that advancements in clinical efficacy are accessible and sustainable for healthcare systems globally. The literature on the cost-effectiveness of ALK+ mNSCLC treatments reveals significant variability in outcomes across different countries due to differences in model assumptions, pricing and willingness-to-pay thresholds [27–29], emphasizing the need for ongoing research to inform personalized and cost-effective treatment strategies [30,31].
Strengths & limitations
The results of this analysis should be interpreted in the context of the study limitations. First, while MAICs provide valuable insights, they cannot fully replace head-to-head RCTs, which offer a more robust direct comparison of treatments under controlled conditions. The robustness of anchored MAICs relies on the successful adjustment for differences in the distribution of all treatment EMs between trials. Our MAIC adjusted for imbalances in all suspected EMs according to clinical experts and the literature, minimizing potential bias. However, although the analysis attempted to adjust for all identified EMs, which were selected based on the literature and clinical expert recommendations, other differences that are not reported in the trials may exist, potentially leading to residual confounding. Second, the study relied on data from different trials (CROWN vs ALEX) with potentially heterogeneous patient populations, treatment protocols, and follow-up procedures. Despite matching, these differences may have impacted the comparability of the PFS and AE rates. Third, Chinese patients from the CROWN trial were not included in the MAIC analyses because of country-specific privacy restrictions. Given the small proportion of excluded patients (n = 20, 6.8%), the exclusion of these patients is unlikely to significantly impact the results’ generalizability. Fourth, the MAIC analyses of the subgroup of patients with baseline brain/CNS metastasis are limited by the relatively small sample size in the CROWN trial (n = 72) and are likely underpowered. This subgroup was investigated as an exploratory analysis and should be interpreted with caution. Fifth, although the outcome definitions were generally similar between the trials, the AE severity grading was conducted according to different versions of National Cancer Institute criteria. Since the comparisons were anchored, these differences are not expected to introduce significant bias. Sixth, the MAIC analysis adjusted for only four baseline variables, which were selected based on the literature and clinical expert recommendations. Other important prognostic factors affecting survival may have been overlooked, potentially leading to residual confounding and unaddressed differences between the study groups, affecting the comparability of the results. The crizotinib survival curves still appear different across studies because not all prognostic factors may be captured; however, this should not impact the findings from the anchored ITC, which only requires adjustment for EMs. Finally, the generalizability of these results to other diseases using targeted therapies in first-line therapy is unclear. Lorlatinib is approved specifically for ALK-positive NSCLC, and therefore, it is uncertain whether these findings can be applied more broadly, which may limit their applicability beyond ALK-positive NSCLC.
Despite these limitations, the analysis also has several notable strengths. The use of long-term data offered a more comprehensive understanding of lorlatinib’s relative efficacy and safety, which is crucial for making informed treatment decisions over both short-term and extended periods. The robust adjustment for EMs ensured a balanced and fair comparison between lorlatinib and alectinib, addressing potential population imbalances that could have otherwise distorted the results. Furthermore, the use of an anchored approach enhances the reliability and validity of the findings by leveraging indirect comparisons through a common comparator. These strengths collectively provided a solid foundation for supporting lorlatinib as an effective first-line treatment option for patients with ALK+ mNSCLC, offering both short-term and long-term benefits.
Conclusion
This analysis using long-term data demonstrates lorlatinib’s superior efficacy in extending PFS compared with alectinib and its manageable AE profile. These results strongly support lorlatinib as an effective and viable first-line treatment option for patients with ALK+ mNSCLC.
Summary points
•
In a previous matching-adjusted indirect comparison, lorlatinib had shown superior efficacy over alectinib for ALK+ advanced/metastatic non-small cell lung cancer.
•
This study updated those findings with extended follow-up data (median follow-up of 5 years) to estimate the long-term efficacy and safety of lorlatinib versus alectinib.
•
Indirect comparisons were conducted in the overall population and subgroups of patients with and without brain/CNS metastases at baseline.
•
In the overall population, the matching-adjusted indirect comparisons revealed superior progression-free survival (PFS) for patients treated with lorlatinib, reducing the risk of progression or death by 45% versus alectinib.
•
Lorlatinib extended the mean PFS time, with generally higher annual PFS probabilities across years 1–5.
•
Subgroup analyses confirm a consistent PFS benefit for lorlatinib.
•
Despite higher rates of grade ≥3 adverse events, lorlatinib consistently showed a benefit over alectinib, regardless of the presence of brain/CNS metastases at baseline.
•
These results reaffirm lorlatinib as a robust first-line treatment option for ALK+ metastatic non-small cell lung cancer.
CRediT authorship contribution statement
T Bauer: Conceptualization, formal analysis, investigation, methodology, supervision, validation, visualization, writing – original draft, writing – review and editing; D Abrahami: Conceptualization, formal analysis, funding acquisition, investigation, methodology, supervision, project administration, resources, supervision, validation, visualization, writing – original draft, writing – review and editing; A Polli: Conceptualization, data curation, formal analysis, investigation, methodology, validation, visualization, writing – original draft, writing – review and editing; H Chu: Conceptualization, formal analysis, investigation, methodology, visualization, writing – original draft, writing – review and editing; P Ramachandran: Conceptualization, formal analysis, investigation, methodology, visualization, writing – original draft, writing – review and editing; C Chandler: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing – original draft, writing – review and editing; M Tan: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing – original draft, writing – review and editing; J Truscott: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing – original draft, writing – review and editing; J Mazieres: Conceptualization, formal analysis, investigation, methodology, visualization, writing – original draft, writing – review and editing; CA Garcia: Conceptualization, formal analysis, investigation, methodology, visualization, writing – original draft, writing – review and editing.
Financial disclosure
This study was sponsored by Pfizer.
Competing interests disclosure
D Abrahami, A Polli, H Chu and P Ramachandran are employees of Pfizer and have stock ownership in Pfizer. T Bauer receives consulting fees from and is an ad board member of Pfizer, Bayer and Lilly. J Mazieres reports personal fees from Roche, Astra Zeneca, Pierre Fabre, Takeda, BMS, MSD, Pfizer, Jiangsu Hengruii, Blueprint, Daiichi, Novartis, Amgen and -grants from Roche, Astra Zeneca, Pierre Fabre, BMS, Illumina. CA Garcia receives consulting fees from Pfizer, Regeneron, Johnson and Johnson. Thermo Fisher Scientific received financial support from Pfizer in connection with the study and the development of this manuscript. C Chandler, M Tan and J Truscott are employees of Thermo Fisher Scientific, which was a paid consultant for Pfizer in connection with the study and the development of this manuscript. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support was provided by Dr Ruth Sharf (Thermo Fisher Scientific) and was funded by Pfizer, Inc.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 35.99 KB
References
Papers of special note have been highlighted as: • of interest
1.
Ettinger DS, Wood DE, Aisner DL et al. Non–small cell lung cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J. Natl Compr. Canc. Netw. 20(5), 497–530 (2022).
2.
Solomon BJ, Kim D-W, Wu Y-L et al. Final overall survival analysis from a study comparing first-line crizotinib versus chemotherapy in ALK-mutation-positive non–small-cell lung cancer. J. Clin. Oncol. 36(22), 2251–2258 (2018).
3.
Peters S, Camidge DR, Shaw AT et al. Alectinib versus crizotinib in untreated ALK-positive non–small-cell lung cancer. N. Engl. J. Med. 377(9), 829–838 (2017).
4.
Zhou C, Kim SW, Reungwetwattana T et al. Alectinib versus crizotinib in untreated Asian patients with anaplastic lymphoma kinase-positive non-small-cell lung cancer (ALESIA): a randomised phase III study. Lancet Respir. Med. 7(5), 437–446 (2019).
5.
Zhou C, Lu Y, Kim S et al. LBA11 alectinib (ALC) vs crizotinib (CRZ) in Asian patients (pts) with treatment-naïve advanced ALK+ non-small cell lung cancer (NSCLC): 5-year update from the phase III ALESIA study. Ann. Oncol. 33, S1563 (2022).
6.
Mok T, Camidge D, Gadgeel S et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Ann. Oncol. 31(8), 1056–1064 (2020).
• Reports the final overall survival (OS) and progression-free survival (PFS) results and other relevant data from ALEX, a pivotal phase III trial comparing alectinib versus crizotinib, which were analyzed in the matching-adjusted indirect comparison (MAIC).
7.
Ahn MJ, Kim HR, Yang JC et al. Efficacy and safety of brigatinib compared with crizotinib in Asian vs. non-Asian patients with locally advanced or metastatic ALK–inhibitor-naive ALK+ non–small cell lung cancer: final results from the phase III ALTA-1L study. Clin. Lung Cancer 23(8), 720–730 (2022).
8.
Camidge DR, Kim HR, Ahn M-J et al. Brigatinib versus crizotinib in ALK inhibitor–naive advanced ALK-positive NSCLC: final results of phase III ALTA-1L trial. J. Thorac. Oncol. 16(12), 2091–2108 (2021).
• Reports the final OS and PFS results and other relevant data from ALTA-1L, a pivotal phase III trial comparing brigatinib versus crizotinib, which were analyzed in the MAIC.
9.
Solomon BJ, Liu G, Felip E et al. Lorlatinib versus crizotinib in patients with advanced ALK-positive non–small cell lung cancer: 5-year outcomes from the phase III CROWN study. J. Clin. Oncol. 42(29), 3400–3409 (2024).
• Presents the latest trial publication for CROWN, summarizing the long-term (5 year) outcomes that were analyzed in this MAIC.
10.
Shaw AT, Bauer TM, de Marinis F et al. First-line lorlatinib or crizotinib in advanced ALK-positive lung cancer. N. Engl. J. Med. 383(21), 2018–2029 (2020).
11.
Ando K, Manabe R, Kishino Y et al. Comparative efficacy and safety of lorlatinib and alectinib for ALK-rearrangement positive advanced non-small cell lung cancer in Asian and non-Asian patients: a systematic review and network meta-analysis. Cancers 13(15), 3704 (2021).
12.
Chuang C-H, Chen H-L, Chang H-M et al. Systematic review and network meta-analysis of anaplastic lymphoma kinase (ALK) inhibitors for treatment-naïve ALK-positive lung cancer. Cancers 13(8), 1966 (2021).
13.
Jiang J, Zhao C, Zhang F et al. ALK inhibitors in ALK-rearranged non-small cell lung cancer with and without brain metastases: systematic review and network meta-analysis. BMJ Open 12(9), e060782 (2022).
14.
Naik J, Beavers N, Nilsson FOL, Iadeluca L, Lowry C. Cost-effectiveness of lorlatinib in first-line treatment of adult patients with anaplastic lymphoma kinase (ALK)-positive non-small-cell lung cancer in Sweden. Appl. Health Econ. Health Policy 21(4), 661–672 (2023).
15.
Peng L, Lu D, Xia Y et al. Efficacy and safety of first-line treatment strategies for anaplastic lymphoma kinase-positive non-small cell lung cancer: a Bayesian network meta-analysis. Front. Oncol. 11, 754768 (2021).
16.
Camidge DR, Kim HR, Ahn MJ et al. Brigatinib versus crizotinib in ALK-positive non-small-cell lung cancer. N. Engl. J. Med. 379(21), 2027–2039 (2018).
17.
Reckamp KL, Lin HM, Cranmer H et al. Indirect comparisons of brigatinib and alectinib for front-line ALK-positive non-small-cell lung cancer. Future Oncol. 18(20), 2499–2510 (2022).
• Presents a previously published matching-adjusted indirect comparison of PFS for brigatinib and alectinib, but not lorlatinib.
18.
Garcia C, Abrahami D, Polli A et al. Comparative efficacy and safety of lorlatinib versus alectinib and lorlatinib versus brigatinib for ALK-positive advanced/metastatic NSCLC: matching-adjusted indirect comparisons. Clin. Lung Cancer 25(7), 634–642 (2024).
• The updated MAIC presented in this paper compared the efficacy and safety of lorlatinib versus alectinib following the methodology outlined in Garcia et al., which was conducted using an older data cut for CROWN.
19.
Latimer N. National Institute for Health and Care Excellence. NICE DSU technical support document 14: survival analysis for economic evaluations alongside clinical trials - extrapolation with patient-level data [cited January 2025]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK395885/pdf/Bookshelf_NBK395885.pdf
20.
Canada's Drug Agency. Procedures for reimbursement reviews [January 2025]. Available from: https://www.cda-amc.ca/sites/default/files/Drug_Review_Process/Drug_Reimbursement_Review_Procedures.pdf
21.
Mazieres J, Iadeluca L, Shaw AT et al. Patient-reported outcomes from the randomized phase III CROWN study of first-line lorlatinib versus crizotinib in advanced ALK-positive non-small cell lung cancer. Lung Cancer 174, 146–156 (2022).
22.
Liu G, Mazieres J, Stratmann J et al. A pragmatic guide for management of adverse events associated with lorlatinib. Lung Cancer 191, 107535 (2024).
23.
Bauer TM, Felip E, Solomon BJ et al. Clinical management of adverse events associated with lorlatinib. Oncologist 24(8), 1103–1110 (2019).
24.
John A, McMahon DJ, Chauhan D et al. Lorlatinib-associated weight gain and dyslipidaemia: a retrospective analysis and implications for future care. Lung Cancer 198, 108034 (2024).
25.
Johung KL, Yeh N, Desai NB et al. Extended survival and prognostic factors for patients with ALK-rearranged non–small-cell lung cancer and brain metastasis. J. Clin. Oncol. 34(2), 123 (2016).
26.
Solomon BJ, Bauer TM, Mok TSK et al. Efficacy and safety of first-line lorlatinib versus crizotinib in patients with advanced, ALK-positive non-small-cell lung cancer: updated analysis of data from the phase III, randomised, open-label CROWN study. Lancet Respir. Med. 11(4), 354–366 (2023).
• This study is a trial publication on the 3-year data cut for CROWN, which was used to inform the prior MAIC by Garcia et al.
27.
Byun J-Y, Park S-K, Ng BP, Liu Y-S, Kim C-R, Park C. A systematic review of economic evaluations of tyrosine kinase inhibitors for non-small cell lung cancer (NSCLC). Expert Opin. Pharmacother. 23(11), 1247–1257 (2022).
28.
Luo X, Zhou Z, Zeng X, Peng L, Liu Q. Cost-effectiveness of ensartinib, crizotinib, ceritinib, alectinib, brigatinib and lorlatinib in patients with anaplastic lymphoma kinase-positive non-small cell lung cancer in China. Front. Public Health 10, 985834 (2022).
29.
Zhang M, Zheng B, Yang W et al. Cost-effectiveness analysis of 6 tyrosine kinase inhibitors as first-line treatment for ALK-positive NSCLC in China. Clin. Med. Insights Oncol. 18, 11795549241257234 (2024).
30.
Chayab L, Konstantelos N, Leighl NB, Tadrous M, Wong WW. A systematic review of the cost-effectiveness analyses of Anaplastic lymphoma kinase (ALK) inhibitors in patients with locally advanced or metastatic non-small cell lung cancer (NSCLC). Pharmacoeconomics 41(8), 945–980 (2023).
31.
Mudumba R, Liu X, Davis I, Romley JA, Nieva JJ. Real-world costs, treatment patterns, and clinical outcomes associated with treatments for advanced anaplastic lymphoma kinase–positive non–small cell lung cancer. J. Manag. Care Spec. Pharm. 31(9), 890–899 (2025).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 17 July 2025
Accepted: 3 December 2025
Published online: 15 December 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Long-term efficacy and safety of lorlatinib versus alectinib in anaplastic lymphoma kinase-positive advanced/metastatic non-small cell lung cancer: matching-adjusted indirect comparison. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0117
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Melek Özdemir, Gamze Gököz Doğu, Burcu Yapar Taşköylü, Arzu Yaren, Serkan Değirmencioğlu, Atike Gökçen Demiray, Ferda Bir, Bensu Selbest Altay, Burçin Çakan Demirel, Tolga Doğan, Semra Taş, Taliha Güçlü Kantar, Ömer Acar, Differential Metastatic Patterns and Prognostic Value of Systemic Inflammation Scores in Anaplastic Lymphoma Kinase Rearranged Versus Anaplastic Lymphoma Kinase Negative Non-Small Cell Lung Cancer, Cancers, 10.3390/cancers18030501, 18, 3, (501), (2026).