Comparative effectiveness of porcine placental extracellular matrix against other cellular, acellular and matrix-like products in diabetic foot ulcers from the Medicare database
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Diabetic foot ulcers (DFUs) are often hard to heal and may require advanced treatment with cellular, acellular and matrix-like products (CAMPs). This retrospective cohort study examines the Medicare fee-for-service population to compare clinical outcomes and health resources utilization in patients receiving porcine placental extracellular matrix (PPECM [InnovaMatrix® AC, Convatec Triad Life Sciences, LLC, TN, USA]) against other CAMPs. Materials & methods: The Center for Medicare & Medicaid Services 100% Research Identifiable Files database was searched for potentially eligible patients using relevant ICD-10 diagnosis codes between 1 January 2020 and 31 December 2023. Patients with confirmed diagnoses of DFU and non-pressure chronic ulcers were selected for further evaluation. Eligible patients were categorized into groups according to treatment received: PPECM, PPECM’s 510(k) predicate† (OASIS® Wound Matrix, Cook Biotech Inc., IN, USA), or other similar CAMPs (OSC [Marigen Shield and Omega3 (Kerecis, Ísafjörður, Iceland); Integra Dermal Regeneration Template and Primatrix (Integra LifeSciences, NJ, USA); GraftJacket (Stryker, MI, USA); Theraskin and Dermacell (LifeNet Health, VA, USA); FlexHD/AllopatchHD and Amnioband (MTF Biologics, NJ, USA); Grafix/Stravix (Smith + Nephew, MA, USA); Epicord and Epifix (MiMedx, GA, USA); Affinity, Apligraf and Dermagraft (Organogenesis, MA, USA)]). Patient demographics, comorbidities and ulcer location were assessed for cohort homogeneity and balanced via inverse probability of treatment weighting, to adjust for potential confounding factors when comparing health outcomes. Results: There were 940,910 patients with a DFU diagnosis; of these, 738,124 (78.4%) also had same-day diagnosis of a non-pressure chronic ulcer. After application of eligibility criteria, there were a total of 34,664 patients with DFUs with 37,380 episodes of care that included one of the CAMP treatments (PPECM: number of patients (n) = 186, number of episodes (e) = 186; PPECM’s 510(k) predicate: n = 369, e = 370; and OSC: n = 33,858, e = 36,559). In the inverse probability of treatment weighting-balanced model, patients with OSC episodes were 1.309-times more likely to undergo outpatient amputation than those with PPECM (95% CI: 1.251–1.371, p < 0.0001). Bacteremia was 2.75-times more likely in OSC episodes than in PPECM episodes (95% CI: 2.471–3.053, p < 0.0001). PPECM episodes had significantly fewer outpatient hospital visits compared with both OSC and PPECM’s 510(k) predicate (5.84, 8.79 and 10.24, respectively, p < 0.0001). There were no differences in physician office visits or hospital admissions. Conclusion: The findings suggest that PPECM performed clinically as well as or better than other well-established CAMPs. Notably, episodes of DFU care that involved PPECM were associated with significantly fewer outpatient amputations, fewer episodes of bacteremia, and fewer outpatient hospital visits. These data suggest that PPECM offers a clinically competitive treatment option for patients with DFUs.
Plain language summary
What is this article about?
Diabetic foot ulcers are wounds that are often difficult to heal and pose significant health risks to patients, including infection, amputation and hospitalization, as well as economic and societal costs.This study examines the comparative effectiveness of porcine placental extracellular matrix against other well-established cellular, acellular and matrix-like products in the management of diabetic foot ulcers within the Medicare fee-for-service patient population.
What were the results?
Patients with diabetic foot ulcers who received porcine placental extracellular matrix (PPECM) showed significantly lower relative risk for major and minor outpatient amputations and wound complications.Patients receiving PPECM also showed fewer outpatient hospital visits compared with similar cellular, acellular and matrix-like products and PPECM’s 510(k) predicate.
What do the results mean?
Porcine placental extracellular matrix demonstrated lower healthcare utilization across all settings and clinical performance that surpassed or was comparable to that of other cellular, acellular and matrix-like products (CAMPs). This study builds on previous CAMPs literature, supporting evidence that have shown CAMPs application is associated with lower rates of amputation, a direct predictor of mortality rates in diabetic foot ulcers patients.
Diabetic foot ulcers (DFUs) are a common yet serious complication of diabetes, affecting as many as a third of people with diabetes over their lifetime [1]. Analysis of real-world data from the US Wound Registry provides compelling evidence that most DFUs do not heal (55–70%) [2]. This may be a consequence of the significant morbidity and mortality associated with DFUs, with up to 60% becoming infected and nearly 20% of infections leading to lower-extremity amputation (LEA) [3]. Within 5 years of DFU diagnosis, the overall mortality rate approaches nearly 50%, primarily due to cardiovascular issues and infections [4]; but after a major amputation, the 5-year mortality rate increases significantly, as high as 90% by some estimates [5].
Although historical data from preceding decades has shown a significant decline in the rates of diabetes-related LEAs, more recent data signal a slowing or even a reversal of this trend. An analysis of surveillance data from the US National Inpatient sample from 2009 to 2015 suggests that the rate of LEAs has rebounded, with the largest increase observed in younger and middle-aged adults with diabetes [6]. The upward trend of LEA rates has also been identified for older adults in an analysis of US Medicare fee-for-service (FFS) data, though the increase is less severe than in other age groups [7].
Beyond the increased risk of morbidity and mortality, DFUs impose significant human costs by restricting an affected individual’s productivity and employment opportunities, often leading to economic stress and emotional suffering [8]. Furthermore, DFUs impose significant societal and economic burdens. In the US, treatment expenses for the most severe ulcers can reach upwards of $50,000 per wound episode [1], and when amputation is necessary, the costs are nearly double [9–12]. Since ulcer duration has been shown to be an independent risk factor for infection [13–15], as well as for LEA [16–18], there is significant human, clinical and economic value in products that may decrease the time-to-wound closure and/or increase the incidence of complete closure.
Cellular, acellular and matrix-like products, or CAMPs, constitute a diverse class of therapeutic options for wounds that do not improve despite application of standard treatment techniques. The precise mechanism of action for any given CAMP will vary according to the source material used in its production [19], which may include biomaterials derived from animal or human tissues, or biocompatible synthetic materials. Porcine placental extracellular matrix (PPECM, InnovaMatrix® AC) is the only CAMP on the market that is derived from porcine placenta and indicated for management of a wide array of challenging wound types, including DFUs.
As a class, CAMPs have been shown to be more effective than standard wound care alone in achieving complete wound closure in patients with DFUs [20,21]. For PPECM specifically, comparative studies of PPECM against standard of care (SOC) alone are in progress; however, a recent real-world study reported encouraging clinical performance of PPECM [22]. In this study PPECM was used in the treatment of 60 wounds, 52% of which were documented as limb/life threatening. PPECM showed encouraging results in this challenging population, achieving 53.3% wound closure at a median of 53 days.
There is a general absence of robust comparative evidence assessing different CAMPs in head-to-head randomized trials, cost–effectiveness analyses, and in real-world studies, all of which could aid decisions on which CAMP to use in clinical practice [21]. Regarding comparative health economics and outcomes research, the Medicare FFS claims database has been used previously to show that CAMPs were associated with significant reductions in major and minor amputation, emergency department visits and hospital readmissions as compared with the SOC cohort [23,24].
This study aims to assess the clinical outcomes associated with PPECM compared with other CAMPs on the market using the latest Medicare data, in an effort to close the gaps in comparative CAMPs evidence in the real-world treatment of DFUs.
Materials & methods
Data source & study design
This retrospective cohort study was conducted to examine the clinical outcomes and health resource utilization in patients receiving PPECM compared with other CAMPs. Data were obtained from the Center for Medicare & Medicaid Services (CMS) 100% Research Identifiable Files (RIFs) database. The dataset comprises administrative claims data from Medicare FFS beneficiaries enrolled in part A and part B coverage, including physician offices, outpatient hospitals, inpatient admissions, intensive care unit (ICU) visits, durable medical equipment (DME), home health, skilled nursing facilities and hospice care. The study utilized healthcare claims data from 1 January 2020 through 30 June 2024. The demographic characteristics of the study population were derived from the Master Beneficiary Summary File provided by the Chronic Conditions Data Warehouse. Patients with incomplete demographics or claims data were excluded from the study.
Patient population selection
Patients with diagnoses of DFU and non-pressure chronic ulcers with at least one medical claim in Medicare Parts A and B were selected from the index period between 1 April 2020 and 31 December 2023.The pre-index period covered 90 days prior to the first diagnosis date, with data available from as early as 1 January 2020. The post-index period extended through 30 June 2024, allowing up to 6 months of follow-up after the latest claim date. The International Statistical Classification of Disease and Related Health Problems (ICD-10-CM) codes were used to identify patients with study relevant diagnoses (Table 1).
| ICD-10-CM code | Diagnosis description |
|---|---|
| E08.621 | Diabetes mellitus due to underlying condition with foot ulcer |
| E08.622 | Diabetes mellitus due to underlying condition with other skin ulcer |
| E09.621 | Drug or chemical induced diabetes mellitus with foot ulcer |
| E09.622 | Drug or chemical induced diabetes mellitus with other skin ulcer |
| E10.621 | Type 1 diabetes mellitus with foot ulcer |
| E10.622 | Type 1 diabetes mellitus with other skin ulcer |
| E11.621 | Type 2 diabetes mellitus with foot ulcer |
| E11.622 | Type 2 diabetes mellitus with other skin ulcer |
| E13.621 | Other specified diabetes mellitus with foot ulcer |
| E13.622 | Other specified diabetes mellitus with other skin ulcer |
| L97.xxx | Non-pressure chronic ulcer of lower limb (including all child codes) |
For consideration of eligibility, patients were required to have at least one claim associated with a dual diagnosis of both diabetic foot ulcer and non-pressure chronic ulcer of lower limb.
There were no restrictions on code ordering (e.g., E08.621 + L97.103 is equivalent to L97.103 + E08.621).
Following their first diagnosis date, patients were evaluated for their receipt of CAMPs reported under relevant Current Procedural Terminology codes for the application of CAMPs (15271, 15272, 15275, 15276, C5271, C5272, C5275 and C5276) and product-specific Healthcare Common Coding System (HCPCS) Q or A codes (Table 2).
| Treatment group | Product name | HCPCS code |
|---|---|---|
| PPECM | InnovaMatrix AC | A2001 |
| PPECM’s 510(k) predicate | Oasis Wound Matrix | Q4102 |
| Oasis Tri-layer Wound Matrix | Q4124 | |
| OSC | Kerecis Marigen/Shield | A2019 |
| Apligraf | Q4101 | |
| Integra DRT | Q4105 | |
| Dermagraft | Q4106 | |
| Graftjacket | Q4107 | |
| Primatrix | Q4110 | |
| Theraskin | Q4121 | |
| Dermacell | Q4122 | |
| Flex HD/Allopatch HD | Q4128 | |
| Grafix/Stravix | Q4133 | |
| Amnioband | Q4151 | |
| Kerecis Omega3 | Q4158 | |
| Affinity | Q4159 | |
| Epifix | Q4186 | |
| Epicord | Q4187 | |
| Derma-Gide | Q4203 |
CAMP: Cellular, acellular and matrix-like products; HCPCS: Healthcare Common Coding System; OSC: Other similar CAMPs; PPECM: Porcine placental extracellular matrix.
A treatment episode included all relevant claims for CAMPs, spanning from the date of the first application to the date of the last treatment claim. A new episode was initiated if a gap of 90 days or more was observed between CAMPs. Episodes were included if they had at least one claim with the relevant HCPCS code (Table 2).
To ensure specificity in the care of the wounds and to guarantee a complete 6-month post-episode period, patients were excluded from the analysis if any of the following were present:
•
Claim of non-pressure chronic ulcer in the 90-day period prior to their first diagnosis date.
•
Claim of wound depth at the bone (ICD-10-CM: L97.xx4, L97.xx6).
•
Received multiple treatment types across episodes.
•
Treated with multiple CAMPs within an episode of care.
•
Episodes concluded after 31 December 2023.
•
Did not maintain continuous enrollment in Medicare Parts A, B and D from 90 days before their first diagnosis date to 6 months after their last episode date.
After inclusion and exclusion criteria were applied, patient episodes were divided into one of three treatment groups (Table 2).
Study measures
Baseline characteristics, including demographics and the Charlson Comorbidity Index (CCI) were assessed to understand the differences between the treatment groups. Patient demographics measured at the first diagnosis date included age, gender, race, dual enrollment in Medicare and Medicaid, current reason for Medicare entitlement, and comorbidities. The total CCI score was calculated by summing the values of the 19 CCI comorbidities. All covariates were evaluated for differences to ensure accurate comparisons between treatment groups. The covariates used for balancing treatment groups included age, race, dual eligibility in Medicare and Medicaid, current reason for enrollment and congestive heart failure.
Outcomes
The primary objective of this study was to comparatively evaluate the clinical effectiveness of CAMPs, by investigating rate of amputations, the use of adjunctive wound therapy and frequency of wound complications. The rate of amputations (in both inpatient and outpatient settings) and wound complications (such as bacteremia, cellulitis, lymphangitis, abscess, gangrene and sepsis) were assessed in the 6-month post-episode period. Episodes were also reviewed for adjunctive wound care treatments commonly used in the management of DFUs such as surgical (operating room) debridement, total contact casting, compression therapy, negative pressure wound therapy, hyperbaric oxygen therapy, MIST therapy and other adjunctive therapies. Healthcare resource utilization and Medicare reimbursement amounts were evaluated across various service sites, including physician offices, outpatient hospitals, inpatient admissions, ICU visits, DME, home health, skilled nursing facilities and hospice care.
Statistical analyses
Descriptive statistics were used to summarize the demographics and baseline characteristics of the study population. Categorical variables were reported using percentages and continuous variables were reported using mean and standard deviation. Comparisons were made of both categorical and continuous variables, using chi-square and t-test, respectively. Differences in treatment groups were presented in terms of p-values and standard mean differences (SMD). Due to the correlation between p-values and population size, the SMD was used to determine imbalance, with SMD ≥10 indicating an imbalanced variable between groups. Inverse probability of treatment weighting (IPTW) was performed to ensure balance in characteristics and control for differences between treatment groups. To assess differences between groups after IPTW, weighted chi-square tests were performed to assess categorical variables for independence. For continuous variables, weighted t-tests were employed to evaluate differences in means between the groups. Regression models were used to further evaluate outcomes and control data skewness. Poisson regression models were used for patient visits. IPTW-adjusted Kaplan–Meier and Cox-Hazard regression analysis was performed to assess amputation-free survival in the 6 months post-episode period. All analyses were completed using SAS software v.9.4 (SAS Institute Inc, NC, USA).
Results
From 2020 to 2023, a total of 940,910 patients in the Medicare FFS population had a confirmed diagnosis of a DFU. Of these, 738,124 patients (78.4%) had diagnoses of both a DFU and a non-pressure chronic ulcer on the same day. After inclusion and exclusion criteria were applied (Figure 1 for summary), the study dataset included 37,380 patient episodes; 186 episodes (0.5%) were treated with PPECM, 36,559 episodes received other similar CAMPs (OSC) (97.8%) and 379 episodes (1%) were treated with PPECM’s 510(k) predicate. Additionally, 256 episodes (0.7%) involved a combination of at least two treatment groups, and were excluded from the analysis.
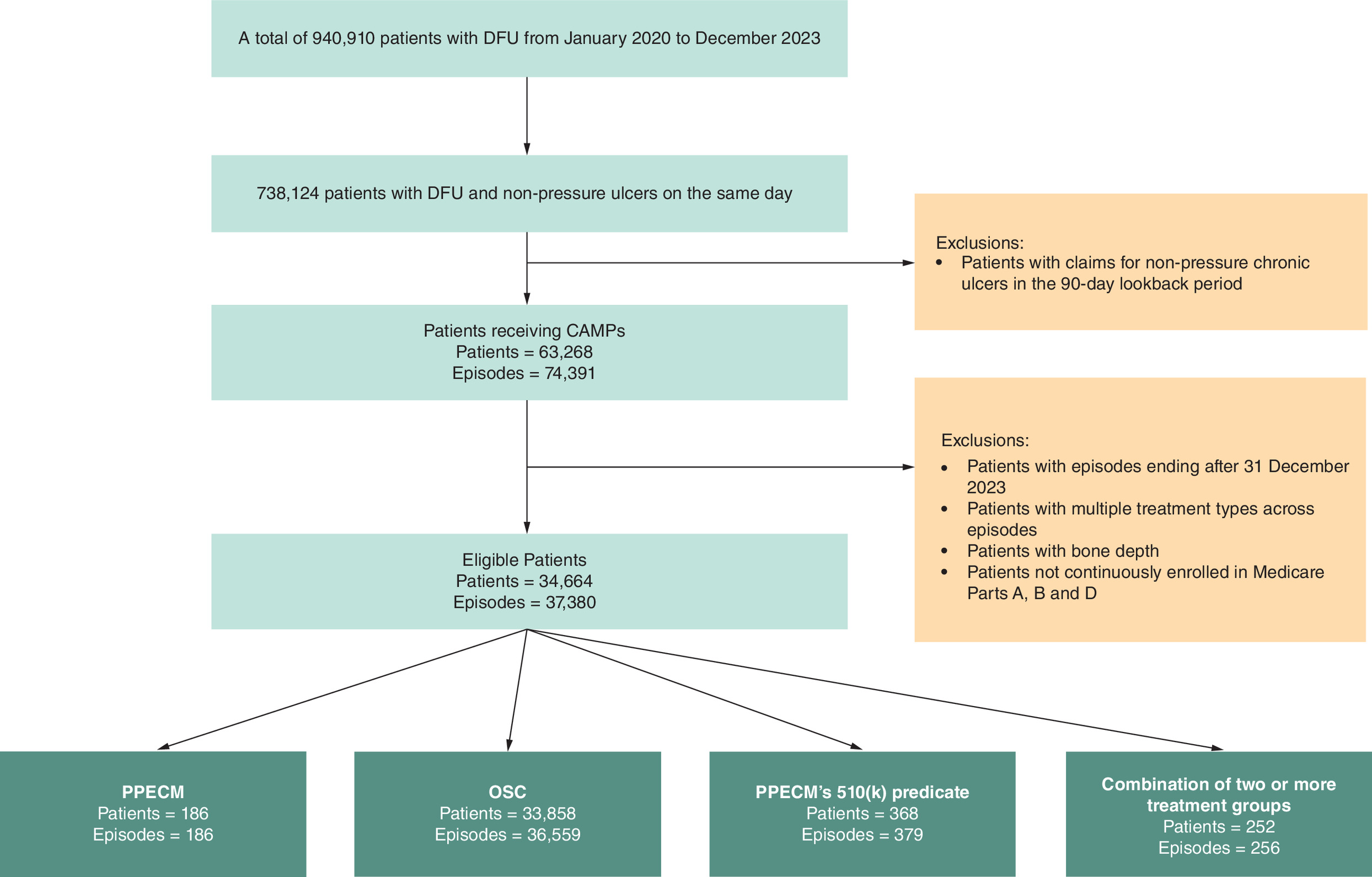
Figure 1. Stepwise attrition to identify eligible patients and episodes.
CAMP: Cellular, acellular and matrix-like products; DFU: Diabetic foot ulcer; OSC: Other similar CAMPs; PPECM: Porcine placental extracellular matrix.
Patient episode characteristics
The unweighted baseline demographic characteristics of the study population were striated for each treatment group (Table 3). Across the groups, the mean age ranged from 69.9 years in the OSC group to 72.1 years in the PPECM group. The distribution of age groups showed a similarly higher proportion of individuals aged 65–74 in all groups, with the OSC group having the highest percentage (41%) in this age bracket. The gender distribution across all treatment groups remained relatively consistent, with males accounting for 62–66% and females for 34–38%. The mean CCI ranged from 3.8 to 4.2 between the groups, with the OSC group having the highest CCI score (4.22, p = 0.001). The prevalence of peripheral vascular disease ranged from 56 to 62%, with the lowest proportion observed in the PPECM group and the highest in the OSC group. Diabetes without complications and diabetes with complications had similar presentations between the treatment groups. Nearly all patients (99–100%) had diabetes without complications; however, the prevalence of diabetes with complications ranged from 84 to 88% across groups. The proportion of renal disease was the same for the PPECM and the PPECM’s 510(k) predicate group (45%), with the OSC group having a slightly higher proportion (50%).
| Variable | Unweighted cohort | Weighted cohort | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PPECM n (%) | OSC n (%) | SMD between PPECM and OSC | PPECM’s 510(k) predicate | SMD between PPECM and PPECM’s 510(k) predicate | PPECM (%) | OSC (%) | SMD between PPECM and OSC | PPECM’s 510(k) predicate | SMD between PPECM and PPECM’s 510(k) predicate | |
| Age | ||||||||||
| Mean age, years (st. dev.) | 72.05 ± 11.28 | 69.94 ± 11.45 | 18.62 | 70.39 ± 11.77 | 14.45 | 70.03 | 69.96 | 0.08 | 70.05 | 0.02 |
| < Age 65 | 35 (19%) | 8,937 (24%) | 13.69 | 92 (24%) | 13.28 | 25% | 24% | 0.36 | 25% | 0.19 |
| Age 65–74 | 70 (38%) | 14,907 (41%) | 6.43 | 152 (40%) | 5.06 | 40% | 41% | 0.12 | 40% | 0.09 |
| Age 75–84 | 58 (31%) | 9,597 (26%) | 10.90 | 90 (24%) | 16.68 | 26% | 26% | 0.19 | 26% | 0.07 |
| Age >= 85 | 23 (12%) | 3,118 (9%) | 12.55 | 45 (12%) | 1.51 | 9% | 9% | 0.05 | 9% | 0.33 |
| Gender | ||||||||||
| Male | 121 (65%) | 24,137 (66%) | 2.04 | 235 (62%) | 6.32 | 66% | 66% | 0.15 | 62% | 0.89 |
| Female | 65 (35%) | 12,422 (34%) | 2.04 | 144 (38%) | 6.32 | 35% | 34% | 0.15 | 38% | 0.89 |
| Race | ||||||||||
| White | 141 (76%) | 28,834 (79%) | 7.31 | 297 (78%) | 6.08 | 81% | 79% | 0.59 | 78% | 0.72 |
| Black | 36 (19%) | 4,106 (11%) | 22.68 | 43 (11%) | 22.31 | 10% | 11% | 0.42 | 12% | 0.62 |
| Asian | 0 (0%) | 397 (1%) | * (*) | 0% | 1% | 1% | ||||
| Hispanic | * (*) | 1,654 (5%) | 16.93 | 18 (5%) | 17.91 | 5% | 5% | 0.22 | 5% | 0.19 |
| Other | * (*) | 1,568 (4%) | 5.59 | * (*) | 7.78 | 4% | 4% | 0.03 | 4% | 0.06 |
| Dual eligibility in Medicare and Medicaid | ||||||||||
| Dual | 44 (24%) | 14,122 (39%) | 32.72 | 134 (35%) | 25.82 | 39% | 39% | 0.14 | 38% | 0.15 |
| Not dual | 142 (76%) | 22,437 (61%) | 32.72 | 245 (65%) | 25.82 | 61% | 62% | 0.14 | 62% | 0.15 |
| Reason for Medicare enrollment | ||||||||||
| Aged | 148 (80%) | 27,451 (75%) | 10.71 | 286 (76%) | 9.83 | 73% | 75% | 0.65 | 75% | 0.49 |
| Disability | * (*) | 7,829 (21%) | 12.10 | * (*) | 14.54 | 23% | 21% | 0.59 | 23% | 0.10 |
| ESRD | * (*) | 1,279 (4%) | 1.42 | * (*) | 9.78 | 4% | 4% | 0.23 | 2% | 0.95 |
| Comorbidities | ||||||||||
| Mean CCI (st. dev.) | 3.81 ± 1.60 | 4.22 ± 1.70 | 24.45 | 4.15 ± 1.70 | 20.55 | 3.95 | 4.21 | 2.27 | 4.22 | 1.90 |
| Myocardial infarction | 22 (12%) | 4,828 (13%) | 4.16 | 48 (13%) | 2.55 | 14% | 13% | 0.21 | 13% | 0.16 |
| CHF | 60 (32%) | 13,738 (38%) | 11.16 | 150 (40%) | 15.27 | 35% | 38% | 0.76 | 40% | 1.25 |
| Peripheral vascular disease | 104 (56%) | 22,560 (62%) | 11.78 | 226 (60%) | 7.52 | 55% | 62% | 1.96 | 59% | 1.02 |
| Cerebrovascular | 26 (14%) | 5,512 (15%) | 3.11 | 54 (14%) | 0.77 | 15% | 15% | 0.03 | 14% | 0.27 |
| Dementia | * (*) | 2,220 (6%) | 7.99 | 26 (7%) | 11.15 | 3% | 6% | 2.13 | 6% | 1.67 |
| COPD | 21 (11%) | 8,591 (24%) | 32.60 | 91 (24%) | 33.78 | 13% | 24% | 4.78 | 25% | 3.95 |
| Connective tissue disease | * (*) | 1,903 (5%) | 4.25 | 14 (4%) | 3.09 | 5% | 5% | 0.54 | 4% | 0.44 |
| Peptic ulcer disease | 0 (0%) | 526 (1%) | n/a | * (*) | n/a | 0% | 1% | n/a | 2% | n/a |
| Liver disease | * (*) | 2,226 (6%) | 5.50 | 27 (7%) | 9.63 | 6% | 6% | 0.22 | 8% | 0.56 |
| Diabetes without complications | 186 (100%) | 36,437 (100%) | 8.18 | 377 (99%) | 10.29 | 100% | 100% | 11.98 | 100% | 1.50 |
| Diabetes with complications | 157 (84%) | 32,118 (88%) | 9.96 | 326 (86%) | 4.52 | 88% | 88% | 0.05 | 88% | 0.01 |
| Paraplegia and hemiplegia | * (*) | 1,001 (3%) | 0.31 | 13 (3%) | 4.30 | 2% | 3% | 0.65 | 3% | 0.75 |
| Renal disease | 83 (45%) | 18,141 (50%) | 10.01 | 169 (45%) | 0.07 | 48% | 50% | 0.47 | 49% | 0.35 |
| Cancer | 17 (9%) | 3,276 (9%) | 0.62 | 39 (10%) | 3.88 | 9% | 9% | 0.07 | 9% | 0.05 |
| Moderate or severe liver disease | * (*) | 306 (1%) | 3.62 | * (*) | 0.14 | 1% | 1% | 0.21 | 1% | 0.16 |
| Metastatic carcinoma | * (*) | 520 (1%) | 3.12 | * (*) | 9.94 | 1% | 1% | 0.00 | 1% | 0.46 |
| HIV/AIDS | 0 (0%) | 181 (1%) | n/a | * (*) | n/a | 0% | 1% | n/a | 1% | n/a |
*Given datapoint comprised fewer than 11 patients and has been obscured in accordance with Center for Medicare & Medicaid Services Data Use Agreement requirements.
Values are presented as mean ± standard deviation or number (%). SMD ≥10 indicates an unbalanced cohort.
CCI: Charlson comorbidity index; CHF: Congestive heart failure; COPD: Chronic obstructive pulmonary disease; ESRD: End-stage renal disease; OSC: Other similar CAMPs; PPECM: Porcine placental extracellular matrix; SMD: Standard mean difference; St. dev.: Standard deviation.
Rate of usage of adjunctive wound care treatments in combination with CAMPs during treatment episode
To evaluate treatment patterns during the episodes, the rate of adjunctive therapies was evaluated in Medicare Parts A and B (Figure 2). The rate of surgical (operating room) debridement use was lower in the PPECM group (36%, p = 0.034) compared with the OSC group (43%) and the rate of negative pressure wound therapy use was lower in the PPECM group (1%, p = 0.007) compared with the other treatment groups (5–6%). Other therapies were evaluated but did not show a significant difference in the usage rates across groups.
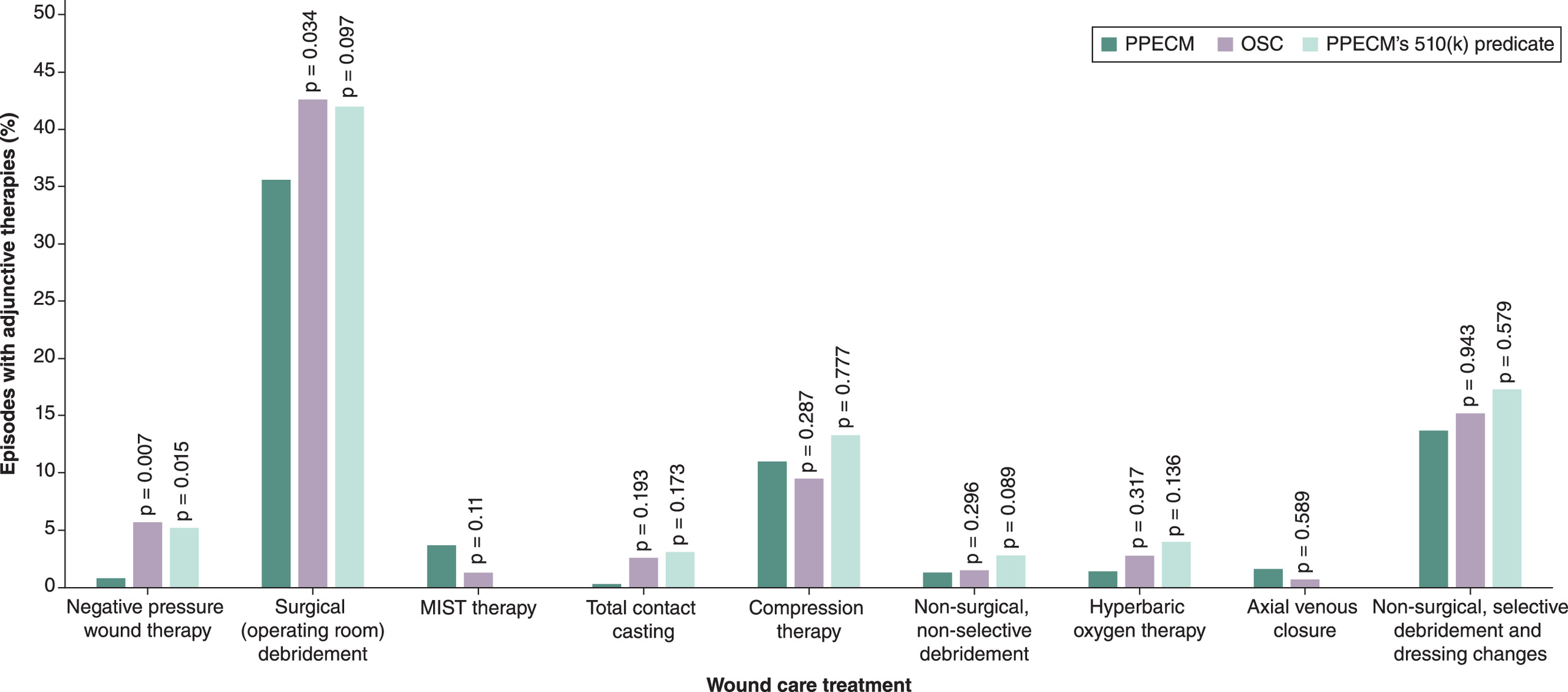
Figure 2. Rate of adjunctive therapies used in combination with cellular, acellular and matrix-like products during the patient episode.
A p-value less than <0.05 indicates statistical significance.
OSC: Other similar CAMPs; PPECM: Porcine placental extracellular matrix.
Wound complications in the 6-month post-episode period
The overall rate of wound complications was assessed in the post-episode period. No significant difference was observed in the total or individual wound complications rates when comparing PPECM to PPECM’s 510(k) predicate. However, significant differences were noted between the PPECM and OSC groups. Across all complications evaluated, the PPECM group (57%, p = 0.034) had a lower proportion of patients with wound complications compared with the OSC group (60%). Bacteremia was 2.75-times more likely in OSC group (95% CI: 2.471–3.053, p < 0.0001) and 1.99-times more likely in the PPECM’s 510(k) predicate group compared with PPECM. Abscess was more common in the PPECM group compared with OSC group (Figure 3).
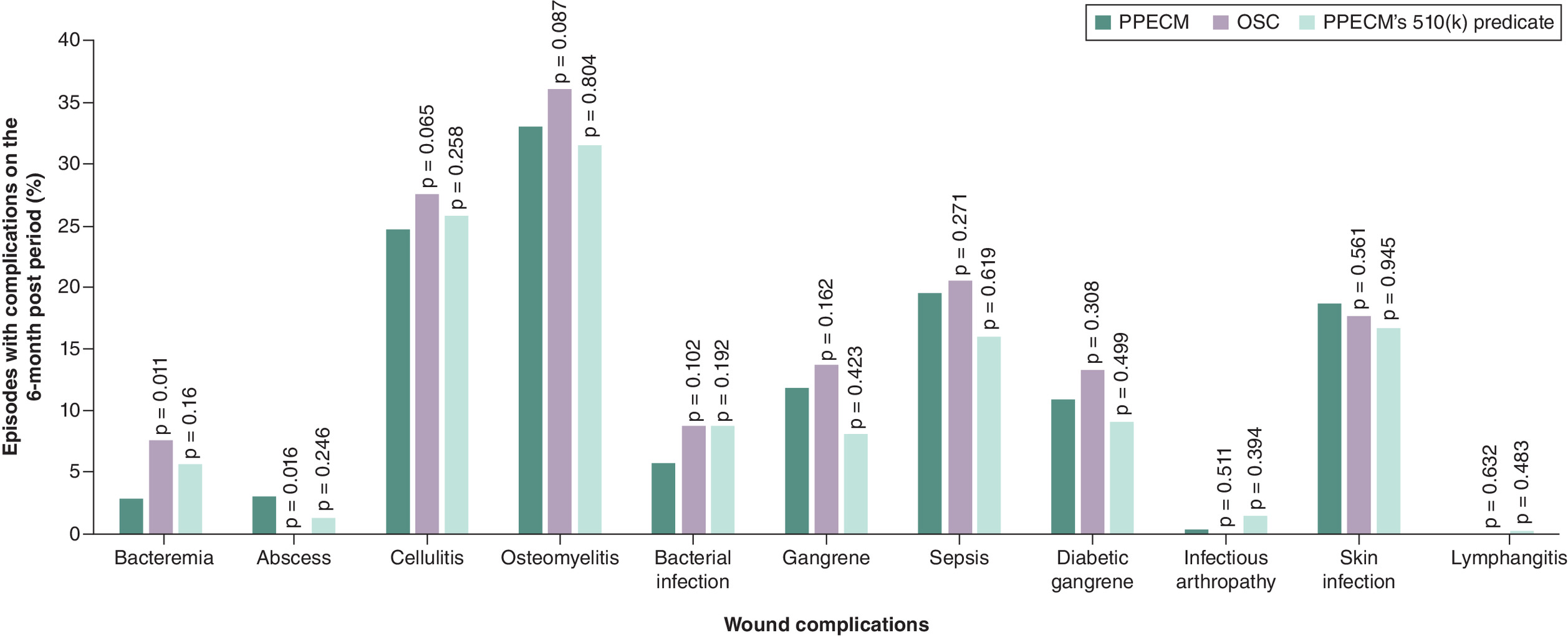
Figure 3. Wound complications in the 6-month post-episode period.
A p-value less than <0.05 indicates statistical significance.
OSC: Other similar CAMPs; PPECM: Porcine placental extracellular matrix.
Amputations in the 6-month post-episode period
The rate of major and minor amputations was assessed in inpatient, outpatient, and across both settings combined. It should be noted that patients receiving inpatient and outpatient amputations were not mutually exclusive groups, as a patient could have multiple amputations in the post-episode period. After application of IPTW, the PPECM group showed no significant differences with the PPECM’s 510(k) predicate groups in amputations. The overall and inpatient amputation rates did not significantly differ between PPECM and OSC; however, outpatient amputations were more frequent in the OSC group (35%) than in the PPECM group (29%) with a borderline significant difference (p = 0.058).
A logistic regression predicting outpatient amputation by treatment grouping was performed to examine the borderline results further. The analysis found that the OSC group was 30.9% more likely to have an outpatient amputation compared with the PPECM group (odds ratio [OR] = 1.309, CI: 1.251–1.371, p < 0.0001). Additionally, a Cox-hazard analysis on the time to first amputation in the 6-month post-episode period found a 5.8% higher relative risk of amputation for patients in the OSC group (HR: 1.058, CI: 1.022–1.095, p = 0.002) compared with those in the PPECM group. No significant differences were observed between the PPECM and the PPECM’s 510(k) predicate group (p = 0.176) (Figure 4).
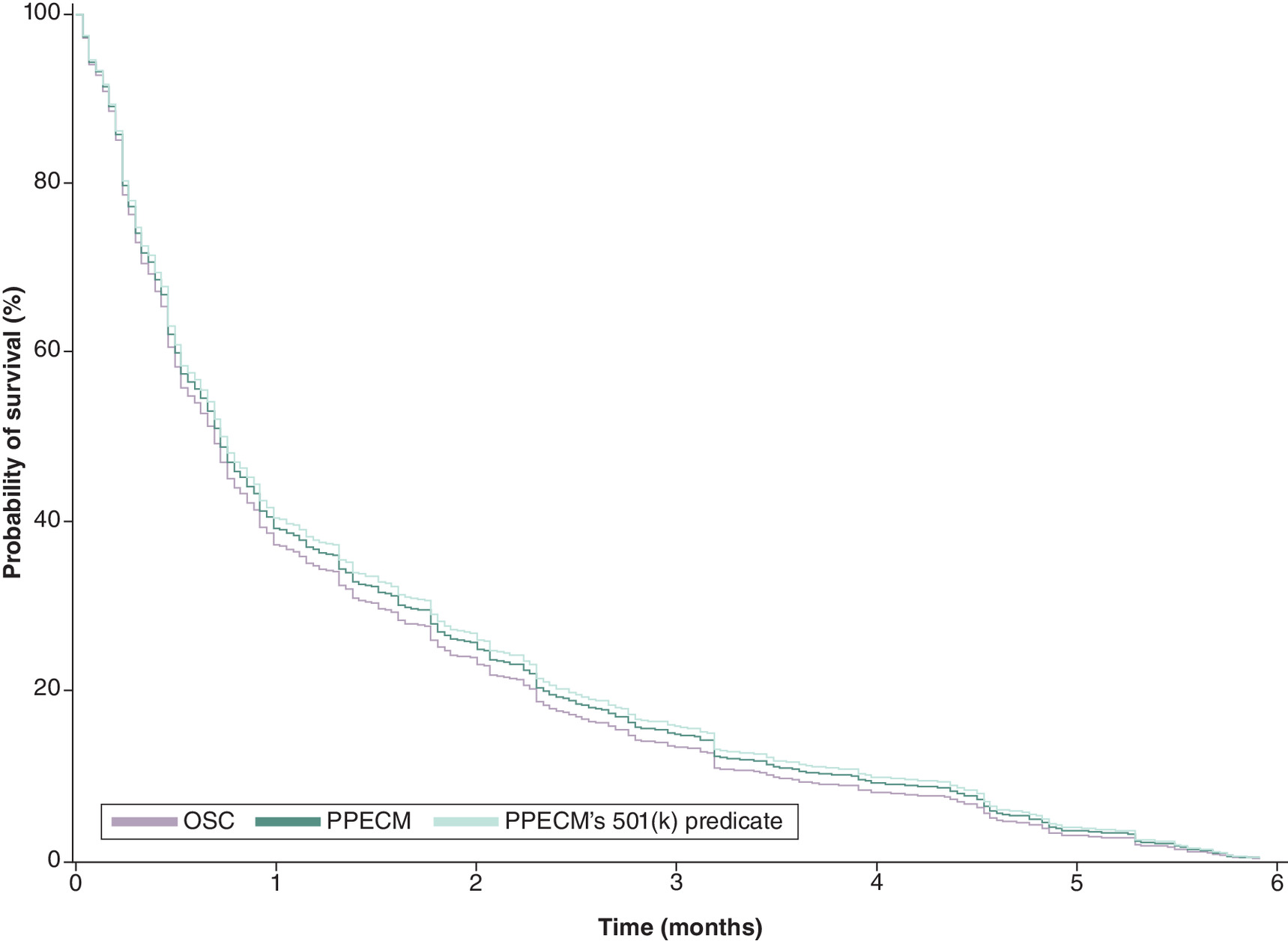
Figure 4. Inverse probability of treatment weighting-adjusted Kaplan–Meier curves for amputation-free survival for patients in the treatment groups over the 6-month post-episode period.
OSC: Other similar CAMPs; PPECM: Porcine placental extracellular matrix.
Healthcare resource utilization in the 6-month post-episode period
Patients were assessed in the subsequent 6 months for healthcare utilization in Medicare Parts A and B. The point estimates of the Poisson regression found significant differences in utilization between the three treatment groups (Figure 5). The PPECM compared with the OSC group had significantly less utilization across all care settings. PPECM compared with PPECM’s 510(k) predicate had significantly fewer visits in the physician’s office (27.52, CI: 27.45–27.60, p < 0.0001) and outpatient hospital (5.84, CI: 5.81–5.88, p < 0.0001). Additionally, across the less frequently utilized care sites, PPECM had significantly fewer visits for home health, ICU and DME compared with both comparator treatment groups.
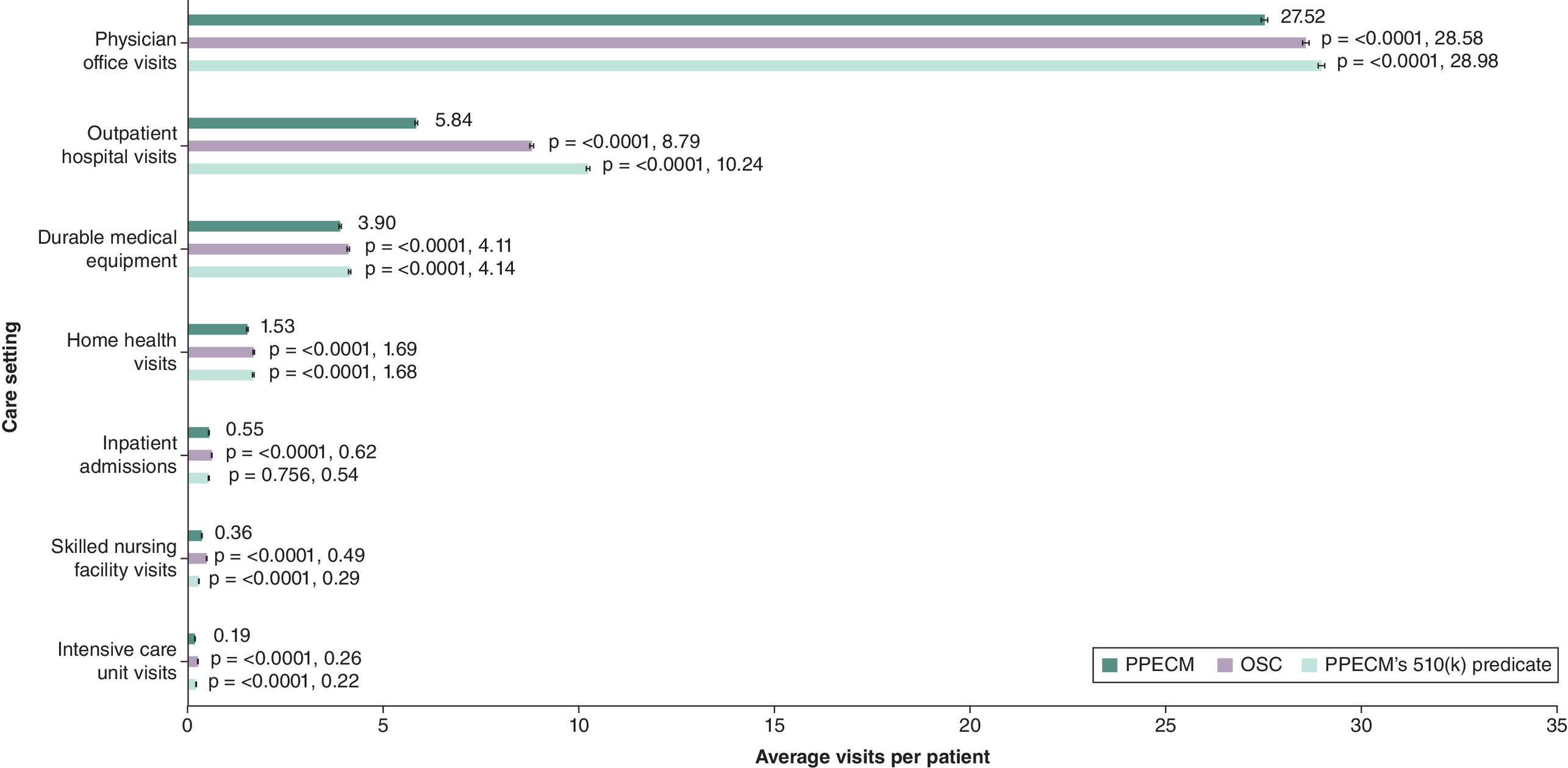
Figure 5. Average visits per patient in the 6-month post-episode period.
A p-value less than <0.05 indicates statistical significance.
OSC: Other similar CAMPs; PPECM: Porcine placental extracellular matrix.
Discussion
This analysis is among the first to evaluate PPECM compared with other well-established CAMPs in the Medicare population. The results demonstrated comparable outcomes between PPECM and the other treatment groups. After IPTW balancing observable differences between the cohorts, the analyses found a statistically significant lower relative risk of amputation and wound complications in episodes of DFU care that utilized PPECM. Specifically, PPECM episodes were associated with a 30.9% lower risk of outpatient amputation compared with the OSC group (OR: 1.309, p < 0.0001). This was supported by the Cox hazard analysis on the time to first amputation in the 6-month episode post period, which found that the relative risk of amputation was 5.8% higher in OSC episodes (HR: 1.058, CI: 1.022–1.095, p = 0.002) as compared with PPECM episodes. The lower relative risk of amputation could be related to a lower relative risk of potential wound complications such as bacteremia, which was 2.75-fold higher in the OSC group than in the PPECM group. However, given the retrospective nature of this claims data analysis, it is not possible to determine whether these are causally linked. In terms of healthcare utilization, the PPECM group had lower rates of inpatient and ICU visits compared with the OSC group. Utilization rates were similar for PPECM and PPECM’s 510(k) predicate.
The impact of including CAMPs in the treatment of lower extremity diabetic ulcers has been previously examined using CMS claims data by Armstrong et al. [23]. In their analysis of the Medicare Limited Data standard analytic hospital inpatient and outpatient department files from 2015 to 2018, the authors demonstrated superior outcomes for CAMPs over standard wound care. Notably, lower extremity diabetic ulcers managed with CAMPs had significant reductions in major and minor amputation rates, emergency visits and hospital readmissions, as compared with those managed with standard wound care. Though it is considered foundational to the current study, the previous examination is not without limitation. The Medicare Limited Dataset only includes claims from inpatient and outpatient settings and does not include claims from physician offices, or other data from Medicare Parts A, B and D. Additionally, propensity score matching was used to generate equivalent cohorts for comparison; while statistically robust, this technique typically results in significant attrition of the starting sample size. Of the nearly 55,000 patients eligible for inclusion in the previous analysis, fewer than half (∼25,000, 45%) were successfully matched and included in the final analysis.
The current study leverages more recent data (2020–2024) from the CMS 100% RIFs database, which encompasses all sites of care for Medicare Parts A and B. Furthermore, the IPTW approach used here allowed for all identified beneficiaries to be used in the analysis, thereby eliminating the potential for attrition seen with matching techniques. The IPTW methodology allows for balanced cohorts, and parallels the effect of randomization in interventional trials [25], which in turn ensures that the observed differences in outcomes have a more direct relationship to potential differences between CAMP treatments. However, additional prospective comparative research would be necessary to confirm these observations.
Limitations
The study examines source data from one payer (Medicare FFS) and the results of the analysis may not extend to other, younger populations. This study is a retrospective analysis of administrative claims which does not allow for consideration of clinical decisions or uniformity in quality of care by site, patient compliance to care or details that are incomplete from claims data.
Conclusion
This 4-year retrospective analysis of the Medicare Claims database found that patients treated with PPECM had similar or better clinical outcomes, with a potential reduction in healthcare utilization and fewer visits across all care settings compared with OSC. This evidence builds on prior literature that showed significantly reduced rates of amputations in patients with DFUs managed with a wide variety of CAMPs. These findings may help guide healthcare practitioners and payers in choosing an effective and efficient solution for their patient population.
Summary points
•
Diabetic foot ulcers (DFU) are often hard-to-heal and may require advanced treatment with cellular, acellular and matrix-like products (CAMPs).
•
The primary objective of this study was to comparatively evaluate the clinical effectiveness of CAMPs within the 100% Medicare Research Identifiable Files (January 2020 to June 2024).
•
Relevant outcomes of interest included rate of amputations, frequency of wound complications, as well as healthcare utilization.
•
Patients with diagnoses of DFU and non-pressure chronic ulcers with at least one medical claim in Medicare Parts A and B were selected from the period between 1 January 2020 and 31 December 2023.
•
Eligible patients were categorized into groups according to treatment received: porcine, placental extracellular matrix (PPECM), PPECM’s 510(k) predicate or other similar CAMPs (OSC).
•
A total of 34,664 patients with DFUs received a CAMP treatment (3.6% of all patients with DFUs).
•
Patient demographics, comorbidities and ulcer location were assessed for cohort homogeneity via inverse probability of treatment weighting, allowing for balanced comparison of health outcomes.
•
PPECM was associated with a 30.9% lower risk of outpatient amputation compared with the OSC group (OR: 1.309, p < 0.0001).
•
This was supported by the Cox-hazard analysis on the time to first amputation in the 6-month episode post period which found that the relative risk of amputation was 5.8% higher in the OSC group (HR: 1.058, CI: 1.022–1.095, p = 0.002) compared with the PPECM group.
•
This 4-year retrospective analysis of the Medicare Claims database found that patients treated with PPECM had similar or improved clinical outcomes with potential reduction in healthcare utilization and fewer visits across all care settings compared with OSC.
Author contributions
B Marcinek, J Levinson, S Nally, I Varghese, C Sheetz, P Kardel and C Taylor: Substantial contributions to the conception or design of the work; drafting the work or reviewing it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
J Maynard (ADVI Health) is thanked for his support in statistical analysis and data interpretation.
Financial disclosure
This research was funded by Convatec Ltd. The funder of this study played a role in the design of the study; in the interpretation of data; in the writing of the manuscript; and in the decision to publish the results.
Competing interests disclosure
B Marcinek: employee of Convatec and Convatec shareholder; J Levinson: employee of Convatec and Convatec shareholder; S Nally: employee of Convatec and Convatec shareholder; I Varghese: none to declare; C Sheetz: none to declare; P Kardel: none to declare; C Taylor: employee of Convatec and Convatec shareholder. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Institutional Review Board Statement: ADVI received IRB approval from Sterling IRB (https://www.sterlingirb.com/) to conduct retrospective claims-based analytics under ADVI’s data use agreement (DUA) with Center for Medicare and Medicaid Services (CMS). The current analysis falls within the research purposes outlined in the DUA, and specific IRB approval for this project was not obtained.
Informed consent statement: Patient informed consent was waived because secondary analysis of deidentified RIFs was considered exempt research, pursuant to HHS Protection of Human Subjects Regulations Title 45 CFR Part 46.
Data sharing statement
Secondary analysis of third-party data subject to restrictions. This study used third party data made available under license that the authors do not have permission to share. Data were obtained by ADVI Health, LLC under a DUA with CMS from the CMS Chronic Condition Warehouse. Requests to access the data should be directed to CMS at https://www2.ccwdata.org.
Open access
This work is licensed under the Creative Commons Attribution 4.0 License. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
McDermott K, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care 46(1), 209–221 (2023).
• Provides background context for the disease burden and socioeconomic impact of diabetic foot ulcers.
2.
Fife CE, Eckert KA, Carter MJ. Publicly reported wound healing rates: the fantasy and the reality. Adv. Wound Care 7(3), 77–94 (2018).
3.
Armstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic foot ulcers: a review. JAMA 330(1), 62–75 (2023).
• Provides background context for the underlying disease process, severity and risk factors associated with lower extremity amputation.
4.
Chen L, Sun S, Gao Y, Ran X. Global mortality of diabetic foot ulcer: a systematic review and meta-analysis of observational studies. Diabetes Obes. Metab. 25(1), 36–45 (2023).
5.
Vuorlaakso M, Kiiski J, Salonen T, Karppelin M, Helminen M, Kaartinen I. Major amputation profoundly increases mortality in patients with diabetic foot infection. Front. Surg. 8, 655902 (2021).
6.
Geiss LS, Li Y, Hora I, Albright A, Rolka D, Gregg EW. Resurgence of diabetes-related nontraumatic lower-extremity amputation in the young and middle-aged adult U.S. population. Diabetes Care 42(1), 50–54 (2019).
7.
Harding JL, Andes LJ, Rolka DB et al. National and state-level trends in nontraumatic lower-extremity amputation among U.S. Medicare beneficiaries with diabetes, 2000–2017. Diabetes Care 43(10), 2453–2459 (2020).
8.
Crocker RM, Palmer KNB, Marrero DG, Tan TW. Patient perspectives on the physical, psycho-social, and financial impacts of diabetic foot ulceration and amputation. J. Diabetes Complications 35(8), 107960 (2021).
• Highlights the significant psychological, financial and physical burdens experienced by patients with diabetic foot ulcers.
9.
Ollendorf DA, Kotsanos JG, Wishner WJ et al. Potential economic benefits of lower-extremity amputation prevention strategies in diabetes. Diabetes Care 21(8), 1240–1245 (1998).
10.
Tennvall RG, Apelqvist J. Health-economic consequences of diabetic foot lesions. Clin. Infect. Dis. 39(Suppl. 2), S132–S139 (2004).
11.
Hunt NA, Liu GT, Lavery LA. The economics of limb salvage in diabetes. Plast. Reconstr. Surg. 127(Suppl. 1), S289–S295 (2011).
12.
Skrepnek GH, Mills JL Sr, Armstrong DG. A Diabetic Emergency One Million Feet Long: Disparities and Burdens of Illness among Diabetic Foot Ulcer Cases within Emergency Departments in the United States, 2006–2010. PLOS ONE 10(8), e0134914 (2015).
13.
Margolis DJ, Allen-Taylor L, Hoffstad O, Berlin JA. Diabetic neuropathic foot ulcers: the association of wound size, wound duration, and wound grade on healing. Diabetes Care 25(10), 1835–1839 (2002).
14.
Lavery LA, Armstrong DG, Wunderlich RP, Mohler MJ, Wendel CS, Lipsky BA. Risk factors for foot infections in individuals with diabetes. Diabetes Care 29(6), 1288–1293 (2006).
15.
Jia L, Parker CN, Parker TJ et al. Incidence and risk factors for developing infection in patients presenting with uninfected diabetic foot ulcers. PLoS One 12(5), e0177916 (2017).
16.
Uysal S, Arda B, Taşbakan MI et al. Risk factors for amputation in patients with diabetic foot infection: a prospective study. Int. Wound J. 14(6), 1219–1224 (2017).
17.
Ugwu E, Adeleye O, Gezawa I, Okpe I, Enamino M, Ezeani I. Predictors of lower extremity amputation in patients with diabetic foot ulcer: findings from MEDFUN, a multi-center observational study. J. Foot Ankle Res. 12, 1–8 (2019).
• Highlights the predictive factors in diabetic foot ulcers that are associated with lower extremity amputation.
18.
Okur KT, Ozan F, Kahraman M, Melez M, Ünlü ÖC, Altun İ. Assessment of the risk factors determining the prognosis of major and minor limb amputations in patients with diabetic foot ulcers. Adv. Clin. Exp. Med. 33(1), 21–30 (2024).
19.
Wu S, Carter M, Cole W et al. Best practice for wound repair and regeneration use of cellular, acellular and matrix-like products (CAMPs). J. Wound Care. 32(Sup4b), S1–S31 (2023).
•• This consensus document provides significant context for the historic and current use of cellular, acellular and matrix-like products (CAMPs). It provides insights on how CAMPs are classified, their mechanism of action, indications for their use and an overview on the observed clinical benefits.
20.
Monami M, Scatena A, Ragghianti B et al. Effectiveness of most common adjuvant wound treatments (skin substitutes, negative pressure wound therapy, hyperbaric oxygen therapy, platelet-rich plasma/fibrin, and growth factors) for the management of hard-to-heal diabetic foot ulcers: a meta-analysis of randomized controlled trials for the development of the Italian Guidelines for the Treatment of Diabetic Foot Syndrome. Acta Diabetol. 1–15 (2024).
21.
Banerjee J, Lasiter A, Nherera L. Systematic Review of Cellular, Acellular, and Matrix-like Products and Indirect Treatment Comparison Between Cellular/Acellular and Amniotic/Nonamniotic Grafts in the Management of Diabetic Foot Ulcers. Adv. Wound Care 13(12), 639–651 (2024).
22.
Fife C, LeBoutillier B, Taylor C, Marcinek BT. Real-World Use and Outcomes of Hard-To-Heal Wounds Managed With Porcine Placental Extracellular Matrix. Cureus 16(12), e76262 (2024).
23.
Armstrong DG, Tettelbach WH, Chang TJ et al. Observed impact of skin substitutes in lower extremity diabetic ulcers: lessons from the Medicare Database (2015–2018). J. Wound Care 30(Sup7), S5–S16 (2021).
•• Demonstrates the benefits of CAMPs (skin substitutes) in lower extremity diabetic ulcers. The authors consider this reference foundational to the current article.
24.
Tettelbach WH, Driver V, Oropallo A et al. Treatment patterns and outcomes of Medicare enrolees who developed venous leg ulcers. J. Wound Care 32(11), 704–718 (2023).
25.
Chesnaye NC, Stel VS, Tripepi G et al. An introduction to inverse probability of treatment weighting in observational research. Clin. Kidney J. 15(1), 14–20 (2022).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Creative Commons Attribution 4.0 License
History
Received: 10 June 2025
Accepted: 30 June 2025
Published online: 25 July 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of porcine placental extracellular matrix against other cellular, acellular and matrix-like products in diabetic foot ulcers from the Medicare database. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0092
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Chengru Li, Kechao Wang, Shu Xia, Pengfei Hu, Huihui Liu, Chong Liu, Sijiong Wang, Mingjiang Xian, Hao Song, Application of Smart Hydrogels in Diabetic Wound Management: Microenvironment-Responsive Strategies and Clinical Translation Challenges, ACS Biomaterials Science & Engineering, 10.1021/acsbiomaterials.6c00731, (2026).
- Daniel Kapp, Angelina Ferguson, T Kent Denmark, Jonathan Johnson, Shawn Naqvi, Shaun Carpenter, Jordan Morrison, Efficacy of a dual-layer pre-hydrated amniotic membrane allograft in the treatment of hard-to-heal wounds, Journal of Wound Care, 10.12968/jowc.2025.0604, 35, 2, (150-161), (2026).
- Daniel Kapp, Shaun Carpenter, Angelina Ferguson, Kent Denmark, Eric Lullove, Michael Bain, Shawn Naqvi, Jordan Morrison, Garrett Johnson, Efficacy of a dehydrated porcine placental extracellular matrix for the treatment of multiple chronic wound types in a private practice model: a retrospective feasibility study, International Journal of Tissue Repair, 10.63676/1p43y632, 2, 1, (2026).
- Katherine W Freeland, Matt D Ramirez, Ashley M Wakelee, Use of Relese in the treatment of hard-to-heal ulcers: a retrospective, multicentre real-world study, Journal of Wound Care, 10.12968/jowc.2025.0499, 34, S11a, (S32-S40), (2025).
- Eddie Soong, Brad Marcinek, Cristin Taylor, Christopher Michaelis, Real-World Use of a Decellularized Porcine Placental Extracellular Matrix in Hard-to-Heal Wounds: A Retrospective, Single-Center Study, Journal of Clinical Medicine, 10.3390/jcm14196823, 14, 19, (6823), (2025).