Healthcare utilization and costs among patients with acromegaly in the United States
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Recent evidence regarding the healthcare resource utilization (HCRU) and associated costs of acromegaly is limited. Materials & methods: This retrospective, cross-sectional administrative claims analysis (IQVIA Pharmetrics Plus®) identified patients (≥18 years) with acromegaly between 1 January 2017 and 30 June 2022. HCRU and costs over 1 year were compared in patients with acromegaly and matched patients without acromegaly (age, sex, insurance type, year). Among patients with acromegaly, annual total healthcare costs of comorbidities and procedures consistent with high-risk comorbidities were reported. Costs were adjusted to 2023 USD. Results: Among 2289 patients with acromegaly and 2289 matched patients without acromegaly, mean age was 49.8 years and 51.6% were female. Patients with acromegaly had a significantly (p < 0.001) higher comorbidity burden than patients without acromegaly. A significantly (p < 0.001) greater proportion of patients with acromegaly versus patients without acromegaly had inpatient hospitalizations (20.1 vs 4.9%) and emergency department visits (23.9 vs 15.7%). Total mean healthcare costs were also significantly higher for patients with acromegaly than patients without acromegaly ($51,888 vs $10,601). The majority of acromegaly-related healthcare costs ($30,985) were attributable to acromegaly therapy ($25,895). Hypertension (42.8%) was the most common high-risk comorbidity associated with acromegaly. The costliest high-risk comorbidity was congestive heart failure, with a mean cost difference of $38,123 (p < 0.05) between patients with acromegaly with and without hypertension. Conclusion: Patients with acromegaly had higher HCRU and costs than matched patients without acromegaly, and the presence of acromegaly with high-risk comorbidities was associated with a substantial HCRU and cost burden. This high burden of illness may be alleviated with better disease control.
Plain language summary: Healthcare burden & costs in acromegaly
What is this article about?
Acromegaly is a rare hormonal disease that leads to poor health outcomes without effective treatment. This study examined healthcare use and cost among patients with and without acromegaly, along with acromegaly-specific services and costs.
What were the results?
In this retrospective cohort study, patients with acromegaly used more healthcare services than those without acromegaly. Twenty percent of patients with acromegaly were hospitalized during the 1-year study period compared with 5% of patients without acromegaly. Average total healthcare costs were almost fivefold higher for patients with acromegaly compared with those without acromegaly ($51,888 vs $10,601). Among patients with acromegaly, those with associated medical conditions and surgeries had the highest healthcare costs.
What do the results mean?
Acromegaly – and acromegaly with high-risk comorbidities – was associated with a substantial healthcare burden, indicating that an unmet need remains for affected patients.
Acromegaly is a rare disease that results from excessive growth hormone (GH) production, typically from a pituitary adenoma. Excess GH stimulates hepatic secretion of insulin-like growth factor-1 (IGF-1), leading to excessive acral and soft tissue growth [1]. Patients with acromegaly often experience abnormal growth of hands and feet, alteration of facial features and thickening of tissue leading to uncontrolled disease. Patients with uncontrolled acromegaly are at risk of developing multiple comorbidities, including diabetes mellitus, hypertension, cardiomyopathy, sleep apnea and colon polyps, at rates much higher than the nonacromegaly population [2,3]. The risk of development and progression of these conditions generally increases with prolonged exposure to elevated GH levels [2,3]. If left untreated, patients with acromegaly have a twofold higher mortality rate than the general population [4,5]. Clinical diagnosis is often delayed because the signs of acromegaly progress slowly over a period of many years [6–8]. The goal of acromegaly management is to reduce GH and/or IGF-1 levels to normal or near normal levels [9]. Initial treatment usually consists of surgery to remove the tumor, but about half of patients require additional treatment [10]. First-line pharmacologic treatment for patients with persistent, significant disease often consists of a somatostatin receptor ligand (SRL) (i.e., octreotide or lanreotide), which inhibits GH secretion, or a GH receptor antagonist (i.e., pegvisomant). The efficacy of SRL therapy varies greatly, with an average biochemical response rate of approximately 55% across most large studies. Among drug-naive patients, an even larger proportion (46–83%) may fail to have their disease controlled by their initial treatment [11,12]. These patients may require further treatment including adding dopamine agonists or pegvisomant, additional surgery or radiotherapy [13].
There is limited recent real-world data on the overall disease burden of acromegaly, particularly on the group of patients with evidence of poor disease control. In a study assessing claims data, commercially covered patients with acromegaly had increased healthcare utilization associated with comorbidities; however, healthcare costs were not reported [14]. Two prior studies that utilized administrative claims data to examine healthcare costs among patients with acromegaly predate the US FDA approval of oral octreotide in 2020 [15–17]. One reported higher healthcare utilization and costs in patients with acromegaly compared with matched controls [17]. The second found that hospitalizations and pharmacotherapy were the largest drivers of acromegaly-related costs, possibly because of severe comorbidities [18]. Given the changing treatment landscape of acromegaly, and the dearth of evidence on the impact of high-risk comorbidities associated with uncontrolled disease, we aimed to provide estimates for healthcare utilization and costs for acromegaly in a commercially insured population.
Materials & methods
Study design & data source
This retrospective cross-sectional cohort analyzed adults in the US with acromegaly from the IQVIA Pharmetrics Plus® Database of adjudicated medical and pharmacy claims, including patient enrollment and benefit data. This database includes a nationally representative sample of more than 210 million enrollees since 2006 and contains demographic and enrollment characteristics, diagnoses and procedures, inpatient hospitalizations, outpatient primary and specialty visits, outpatient prescriptions and costs. The database is a Health Insurance Portability and Accountability Act compliant administrative claims database.
These claims data provide an opportunity to examine acromegaly, a rare disease, because they provide a sufficiently large patient population. This study uses the most recent 5 years of available data, from 1 January 2017 to 30 June 2023, to investigate healthcare resource utilization (HCRU) and costs among adult patients with acromegaly compared with patients without acromegaly, and, in a secondary analysis, to analyze patients with acromegaly and high-risk comorbidities.
Claims data are well-suited for measuring burden of illness, HCRU and costs in patients with rare diseases; their large sample size, relatively long follow-up period, and detailed capture of healthcare encounters, diagnoses and billing allow researchers to evaluate real-world health outcomes and economic impact of acromegaly [19]. However, claims data are administrative data for which the primary purpose is to facilitate reimbursement and all results should be interpreted with this in mind [20]. Other limitations of claims data have been explored and include missing data, duplicate records, upcoding, high rates of disenrollment and general lack laboratory test results [20,21].
Patient identification
This study included adults (aged ≥ 18 years) with acromegaly during the identification (ID) period (1 January 2017 to 30 June 2022), identified by at least two medical claims with acromegaly (International Classification of Diseases, 10th Revision, Clinical Modification [ICD-10-CM] diagnosis code: E22.0) in any diagnosis field or at least one medical claim with an acromegaly diagnosis code in combination with one other claim for a pituitary tumor (ICD-10-CM: D35.2, D44.3), pituitary surgery (hypophysectomy), or cranial stereotactic radiosurgery (a full list of diagnosis and procedure codes is provided in Supplementary Table 1). A randomly selected claim with an acromegaly diagnosis was the index date. A random claim, rather than the first claim, was selected to include both individuals with existing and newly diagnosed acromegaly. All patients were followed for 1 year from the index date (observation period). Patients were excluded if they were not continuously enrolled in the database for the 1-year observation period. From a 5% random sample of enrollees in the database, a reference group of patients without acromegaly was selected by matching them with patients with acromegaly on a 1:1 ratio by age, sex, US geographic region and insurance type. The patients in this reference group were assigned the same index date as the matched acromegaly cases and met the same enrollment criteria.
In a secondary analysis, acromegaly with high-risk comorbidities was defined by the presence of one or more comorbidities of interest (i.e., osteoarthritis, hypertension, cardiomyopathy, congestive heart failure, valvular heart disease, sleep apnea, psychosis and depression) and procedures that are known to be associated with inadequately controlled disease.
Study measures
We reported baseline age, gender, insurance type and US geographic region at index date. During the observation period, we measured and compared disease burden between patients with and without acromegaly by analyzing comorbidities (a full list of diagnosis and procedure codes is provided in Supplementary Table 2), all-cause HCRU and costs. Comorbidity burden was measured by the Charlson Comorbidity Index (CCI) and specific comorbidities of interest. All-cause healthcare utilization included inpatient admissions, emergency department (ED) visits and outpatient visits. Costs included total healthcare costs and medical costs for inpatient hospitalizations, ED services and non-ED outpatient service costs.
For patients with acromegaly, we reported use of laboratory and imaging tests (i.e., IGF-1, glucose tolerance, GH, pituitary MRI), use of therapies (i.e., somatostatin analogs, dopamine receptor agonists, GH receptor antagonists, pituitary surgery, radiation therapy [a full list of diagnosis and procedure codes is provided in Supplementary Table 3]) and treatment costs. Acromegaly-related medical healthcare use and costs were estimated based on medical claims with acromegaly as any diagnosis. Costs were adjusted to 2023 US dollars using the medical component of the Consumer Price Index [22].
Statistical analysis
Descriptive statistics including mean, standard deviation (SD), and relative frequencies and percentages for continuous and categorical data, respectively, were reported. We used t-tests for continuous variables and Chi-squared tests for binary or categorical variables. All tests were two-sided. All data transformations and statistical analyses were performed using SAS© version 9.4.
Results
Patient identification & demographics
We identified 5578 patients with existing or newly diagnosed acromegaly during the ID period (1 January 2017 to 30 June 2022). After excluding patients without medical and pharmacy coverage around the index date (a randomly selected claim with an acromegaly diagnosis) or without continuous enrollment in a health plan during the 1-year observation period, 2404 patients remained. Among these patients, 2289 were at least 18 years old (Figure 1). The final sample consisted of 2289 patients with acromegaly and 2289 patients without acromegaly.
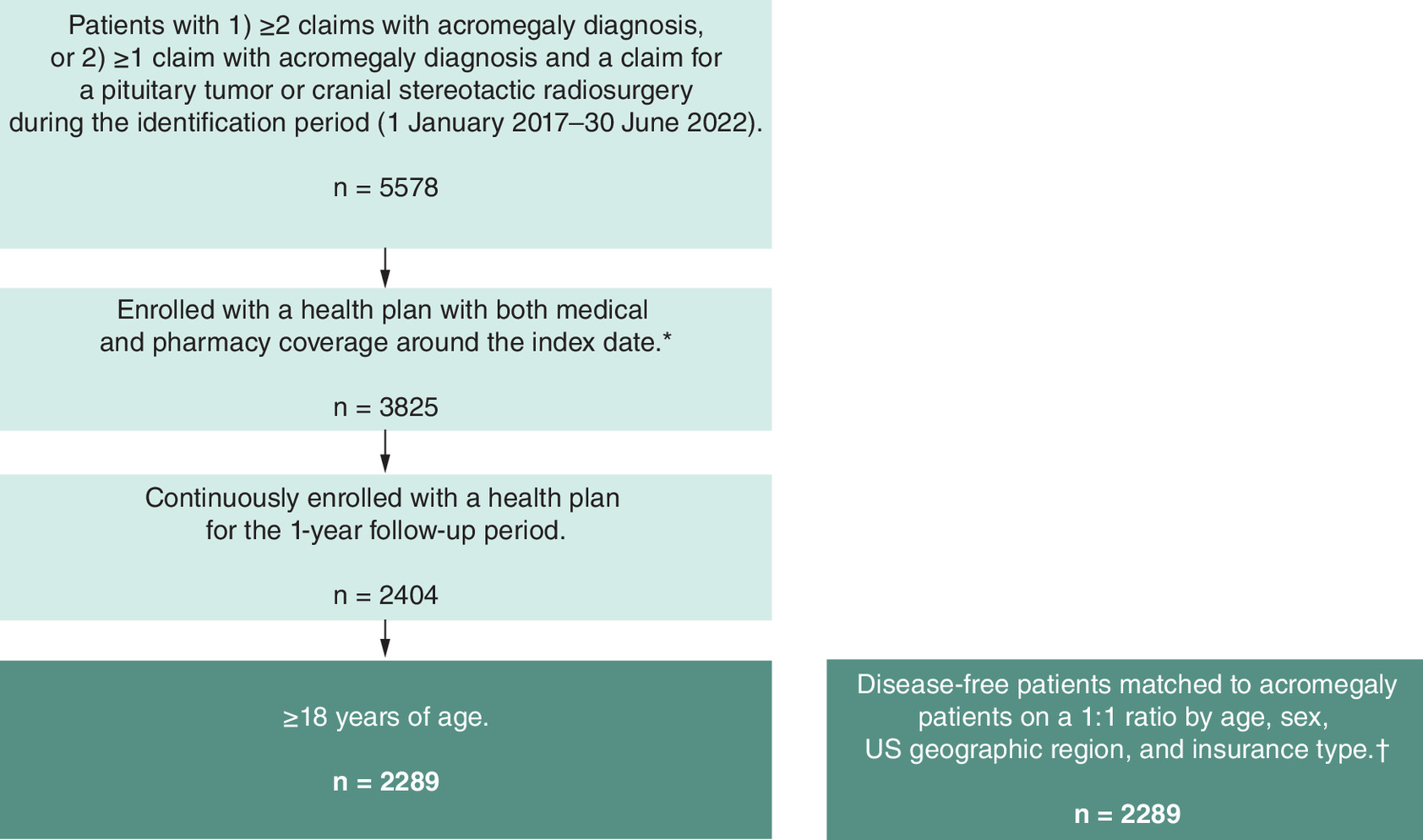
Figure 1. Patient attrition.
*A randomly selected claim with acromegaly diagnosis was the index date.
†Drawn from a 5% sample of the IQVIA Pharmetrics Plus® database. Assigned the same index date as the matched acromegaly cases and met the same enrollment criteria.
Across patients with and without acromegaly, the mean (SD) age was 49.8 (14.0) years. More patients were female (51.6%), from the South (38.6%), and had commercial insurance (64.2%). Patients with acromegaly had a higher comorbidity burden compared with patients without acromegaly (mean CCI score: 1.3 vs 0.6, p < 0.001), including greater proportions of patients with musculoskeletal (25.0 vs 12.1%), cardiovascular (49.2 vs 30.7%) and endocrine/metabolic (68.0 vs 34.5%) comorbidities of interest (p < 0.001 for all) (Table 1).
| Acromegaly patients (n = 2289) | Matched patients without acromegaly† (n = 2289) | All (n = 4578) | p-value | |
|---|---|---|---|---|
| Age, mean (SD) | 49.8 (14.0) | 49.8 (14.0) | 49.8 (14.0) | |
| Female, n (%) | 1180 (51.6) | 1180 (51.6) | 2360 (51.6) | |
| Geographic region, n (%) | ||||
| Midwest | 603 (26.3) | 603 (26.3) | 1206 (26.3) | |
| Northeast | 406 (17.7) | 406 (17.7) | 812 (17.7) | |
| South | 884 (38.6) | 884 (38.6) | 1768 (38.6) | |
| West | 396 (17.3) | 396 (17.3) | 792 (17.3) | |
| Insurance type, n (%) | ||||
| Commercial | 1469 (64.2) | 1469 (64.2) | 2938 (64.2) | |
| Medicare | 188 (8.2) | 188 (8.2) | 376 (8.2) | |
| Other | 632 (27.6) | 632 (27.6) | 1264 (27.6) | |
| Charlson Comorbidity Index (CCI), mean (SD) | 1.3 (2.0) | 0.6 (1.5) | 0.9 (1.8) | <0.001 |
| Comorbidities, n (%) | ||||
| Musculoskeletal | 573 (25.0) | 278 (12.1) | 851 (18.6) | <0.001 |
| Osteoarthritis | 350 (15.3) | 157 (6.9) | 507 (11.1) | <0.001 |
| Arthropathy/arthralgia/synovitis | 107 (4.7) | 43 (1.9) | 150 (3.3) | <0.001 |
| Kryphosis and scoliosis | 15 (0.7) | 7 (0.3) | 22 (0.5) | 0.087 |
| Vertebral fracture | 10 (0.4) | 5 (0.2) | 15 (0.3) | 0.196 |
| Carpal tunnel syndrome | 48 (2.1) | 32 (1.4) | 80 (1.7) | 0.017 |
| Myopathy/myalgia | 176 (7.7) | 86 (3.8) | 262 (5.7) | <0.001 |
| Cardiovascular | 1127 (49.2) | 702 (30.7) | 1829 (40.0) | <0.001 |
| Hypertension | 980 (42.8) | 662 (28.9) | 1642 (35.9) | <0.001 |
| Cardiomyopathy | 66 (2.9) | 21 (0.9) | 87 (1.9) | <0.001 |
| Cardiac hypertrophy | 83 (3.6) | 30 (1.3) | 113 (2.5) | <0.001 |
| Congestive heart failure | 81 (3.5) | 48 (2.1) | 129 (2.8) | 0.003 |
| Valvular heart disease | 171 (7.5) | 74 (3.2) | 245 (5.4) | <0.001 |
| Cardiac dysrhythmia/arrhythmia | 269 (11.8) | 108 (4.7) | 377 (8.2) | <0.001 |
| Endocrine/metabolic | 1557 (68.0) | 789 (34.5) | 2346 (51.2) | <0.001 |
| Diabetes (including impaired glucose tolerance) | 640 (28.0) | 278 (12.1) | 918 (20.1) | <0.001 |
| Obesity | 661 (28.9) | 371 (16.2) | 1032 (22.5) | <0.001 |
| Galactorrhea | 17 (0.7) | 0 (0.0) | 17 (0.4) | <0.001 |
| Menstrual abnormalities | 189 (8.3) | 85 (3.7) | 274 (6.0) | <0.001 |
| Impaired libido/impotence | 200 (8.7) | 106 (4.6) | 306 (6.7) | <0.001 |
| Hypothyroidism | 693 (30.3) | 200 (8.7) | 893 (19.5) | <0.001 |
| Chronic obstructive pulmonary disease | 86 (3.8) | 64 (2.8) | 150 (3.3) | 0.068 |
| Sleep apnea (obstructive and central) | 557 (24.3) | 175 (7.6) | 732 (16.0) | <0.001 |
| Solid tumor without metastasis | 1557 (68.0) | 340 (14.9) | 1897 (41.4) | <0.001 |
| Deficiency anemias | 189 (8.3) | 77 (3.4) | 266 (5.8) | <0.001 |
| Psychoses | 5 (0.2) | 3 (0.1) | 8 (0.2) | 0.726 |
| Depression | 388 (17.0) | 227 (9.9) | 615 (13.4) | <0.001 |
†
Disease-free beneficiaries were drawn from a 5% random sample of enrollees in the IQVIA Pharmetrics Plus® Database and matched to acromegaly beneficiaries on a 1:1 ratio by age, gender, insurance type and US geographic region. The disease-free controls were assigned with the same index date as the matched acromegaly cases and met the same enrollment criteria.
Healthcare utilization & costs
All-cause HCRU & costs
Patients with acromegaly had higher HCRU than patients without acromegaly, including a greater proportion of patients with an inpatient hospitalization (20.1 vs 4.9%) and ED visit (23.9 vs 15.7%), and a higher number of mean office visits (15.7 vs 10.9) and non-ED/non-office visits (11.5 vs 4.4) (p < 0.001 for all) (Table 2). Healthcare costs were higher among patients with acromegaly than patients without acromegaly, including total costs ($51,888 vs $10,601), medical (nonoutpatient pharmacy) costs ($32,095 vs $8101) and outpatient pharmacy costs ($19,794 vs $2500) (p < 0.001 for all) (Figure 2A). For patients with acromegaly, inpatient hospitalization was the largest single contributor ($9400) to medical costs (Figure 2B).
| Acromegaly patients (n = 2289) | Matched patients without acromegaly† (n = 2289) | All (n = 4578) | p-value | |
|---|---|---|---|---|
| Had an inpatient hospitalization, n (%) | 460 (20.1) | 113 (4.9) | 573 (12.5) | <0.001 |
| Length of stay (days) among utilizers, mean (SD) | 6.0 (9.9) | 8.2 (17.0) | 6.4 (11.7) | 0.176 |
| Inpatient hospitalizations, n (%) | <0.001 | |||
| 0 | 1829 (79.9) | 2176 (95.1) | 4005 (87.5) | |
| 1 | 353 (15.4) | 90 (3.9) | 443 (9.7) | |
| 2+ | 107 (4.7) | 23 (1.0) | 130 (2.8) | |
| Had an ED service, n (%) | 546 (23.9) | 360 (15.7) | 906 (19.8) | <0.001 |
| ED services, n (%) | <0.001 | |||
| 0 | 1743 (76.1) | 1929 (84.3) | 3672 (80.2) | |
| 1 | 338 (14.8) | 233 (10.2) | 571 (12.5) | |
| 2 | 113 (4.9) | 61 (2.7) | 174 (3.8) | |
| 3+ | 95 (4.2) | 66 (2.9) | 161 (3.5) | |
| Office visits, mean (SD) | 15.7 (15.5) | 7.5 (10.9) | 11.6 (14.0) | <0.001 |
| Other outpatient services (non-ED/non-office), mean (SD) | 11.5 (15.9) | 4.4 (11.5) | 8.0 (4.3) | <0.001 |
†
Disease-free beneficiaries were drawn from a 5% random sample of enrollees in the IQVIA Pharmetrics Plus® Database and matched to acromegaly beneficiaries on a 1:1 ratio by age, gender, insurance type and US geographic region. The disease-free controls were assigned with the same index date as the matched acromegaly cases and met the same enrollment criteria.
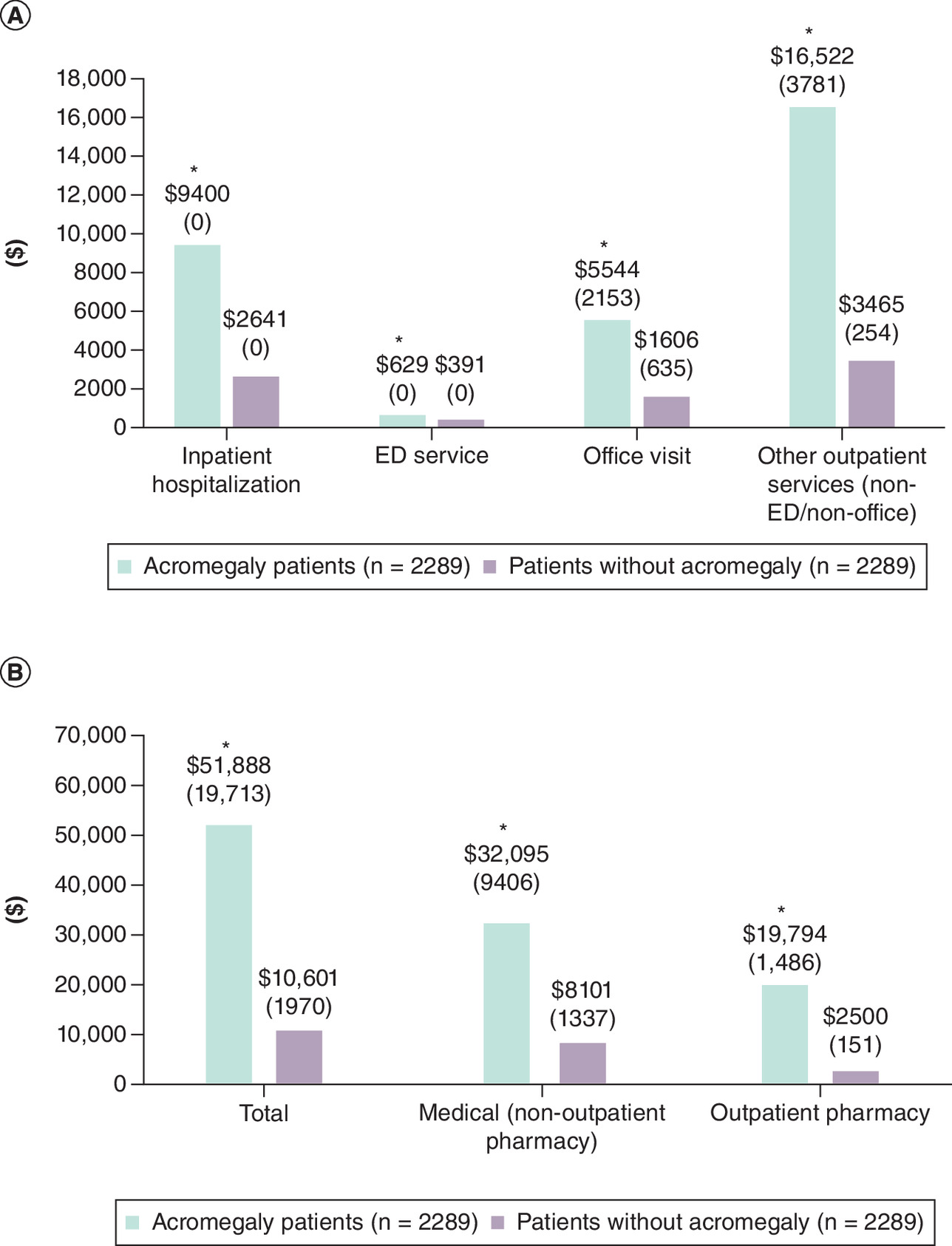
Figure 2. Matched cohort healthcare costs.
(A) Mean (median) healthcare services costs and (B) Mean (median) total, medical, and outpatient pharmacy costs for patients with acromegaly and patients without acromegaly. Medical healthcare costs were the combined costs of inpatient hospitalization, emergency department services, office visits and non-emergency department/non-office costs other than outpatient pharmacy.
*p < 0.001 versus patients without acromegaly.
Acromegaly-related HCRU & costs
The majority (59%) of patients with acromegaly did not have evidence of acromegaly therapy (medical, pituitary surgery or radiation therapy). Of the 41% of patients who received therapy, somatostatin analogs (octreotide, lanreotide and pasireotide) were the most observed therapies (48.9%), followed by dopamine receptor agonists (35.3%). Pituitary surgery (21.9%) and radiation therapy (2.7%) were the least common therapy modalities (Table 3). Acromegaly-related inpatient hospitalization and ED visits were observed in 12.2 and 2.7% of patients, respectively. Patients had a mean (SD) of 1.7 (2.5) endocrinologist office visits (Table 3). Acromegaly therapy costs ($25,895) accounted for the majority of the mean total acromegaly-related healthcare costs ($30,985). Therapy costs ranged from $141 for dopamine receptor agonists to $13,270 for somatostatin analogs (Table 4).
| Acromegaly patients (n = 2289) | |
|---|---|
| Laboratory or imaging test, n (%) | 1924 (84.1) |
| IGF-1 test | 1646 (71.9) |
| Glucose tolerance test | 335 (14.6) |
| Growth hormone test | 901 (39.4) |
| Pituitary MRI | 1033 (45.1) |
| Acromegaly therapy (medical, pituitary surgery and radiation therapy, n (%) | 938 (41.0) |
| Somatostatin analogs (octreotide, lanreotide, pasireotide) | 459 (20.1) |
| Dopamine receptor agonists (cabergoline, bromocriptine) | 331 (14.5) |
| GH receptor antagonist (pegvisomant) | 164 (7.2) |
| Pituitary surgery (hypophysectomy) | 205 (9.0) |
| Radiation therapy | 25 (1.1) |
| Had an acromegaly-related inpatient hospitalization, n (%) | 280 (12.2) |
| Length of stay (days) among utilizers, mean (SD) | 4.1 (6.2) |
| Acromegaly-related† inpatient hospitalizations, n (%) | |
| 0 | 2009 (87.8) |
| 1 | 246 (10.7) |
| 2+ | 34 (1.5) |
| Had an acromegaly-related † ED service, n (%) | 62 (2.7) |
| Acromegaly-related†office visits, mean (SD) | 2.4 (3.5) |
| Endocrinologist office visits, mean (SD) | 1.7 (2.5) |
| Acromegaly-related†other outpatient services (non-ED/non-office), mean (SD) | 2.7 (3.6) |
†
Medical claims with acromegaly as any diagnosis.
ED: Emergency department; GH: Growth hormone; IGF-1: Insulin-like growth factor 1.
| Acromegaly patients (n = 2289) | ||
|---|---|---|
| Total acromegaly-related†healthcare costs | Mean | $30,985 |
| SD | 59,856.7 | |
| Median | 1772 | |
| Costs of acromegaly-related † nontherapy claims | Mean | $5090 |
| SD | 16,967.4 | |
| Median | 869 | |
| Acromegaly-related † inpatient hospitalization costs | Mean | $1,896 |
| SD | 13,099.6 | |
| Median | 0 | |
| Acromegaly-related † ED service costs | Mean | $58 |
| SD | 545.5 | |
| Median | 0 | |
| Acromegaly-related † office visit costs | Mean | $689 |
| SD | 3123.2 | |
| Median | 242 | |
| Acromegaly-related † other outpatient services (non-ED/non-office) costs | Mean | $2446 |
| SD | 9076.6 | |
| Median | 284 | |
| Acromegaly therapy costs | Mean | $25,895 |
| SD | 55,549.4 | |
| Median | 0 | |
| Somatostatin analog costs | Mean | $13,270 |
| SD | 35,325.8 | |
| Median | 0 | |
| Dopamine receptor agonist costs | Mean | $141 |
| SD | 614.3 | |
| Median | 0 | |
| GH receptor antagonist costs | Mean | $7886 |
| SD | 36,069.5 | |
| Median | 0 | |
| Pituitary surgery costs | Mean | $4184 |
| SD | 15,843.8 | |
| Median | 0 | |
| Radiation therapy costs | Mean | $413 |
| SD | 5539.2 | |
| Median | 0 |
†
Medical claims with acromegaly as any diagnosis.
ED: Emergency department; GH: Growth hormone; IGF-1: Insulin-like growth factor 1.
High-risk comorbidity-related HCRU & costs in acromegaly
The most common high-risk comorbidities in patients with acromegaly were hypertension (42.8%), sleep apnea (24.3%), depression (17%) and osteoarthritis (15.3%). Among patients with acromegaly, the largest statistically significant mean cost difference between those with and without high-risk comorbidities was observed for congestive heart failure ($38,123), followed by osteoarthritis ($28,486), valvular heart disease ($25,543) and sleep apnea ($21,634) (p < 0.001 for all comparisons) (Figure 3).
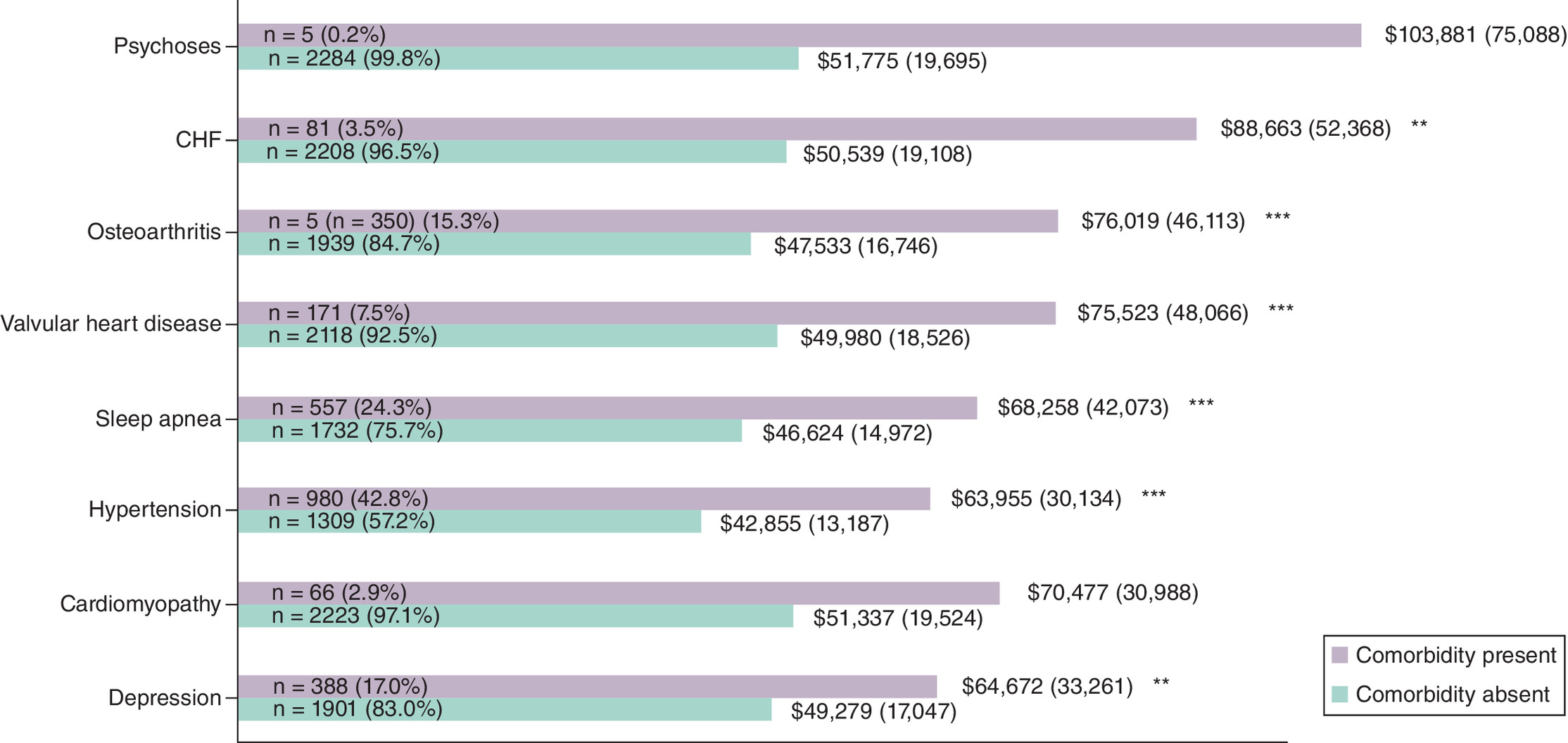
Figure 3. Total healthcare costs stratified by selected comorbidities among acromegaly patents.
Mean (median) total healthcare costs stratified by selected comorbidities among patients with acromegaly. Total healthcare costs included costs of medical claims (inpatient hospitalization, emergency department services, office visits, other outpatient non-emergency department/non-office services) and outpatient pharmacy claims.
**p < 0.01; ***p < 0.001 versus patients without acromegaly without comorbidities.
Colonoscopies and colonic procedures for polyps/tumors were the most frequent surgery (12.6% of cases) with a mean cost per surgery of $2179. The costliest surgeries were lumbar and cervical spinal fusions and laminectomies ($60,760; 0.8% of patients) (Table 5).
| Patients with surgery/event, n (%)† | Surgeries during observation period, n | Mean [median] costs per surgery‡ | |
|---|---|---|---|
| Surgery of interest | |||
| Total or partial hip replacements | 36 (1.57) | 41 | $23,196 [22,511] |
| Total or partial knee replacements | 30 (1.31) | 32 | $16,244 [11,128] |
| Lumbar and cervical spinal fusions, laminectomies | 18 (0.79) | 19 | $60,760 [43,931] |
| Other orthopedic surgeries for arthritis§ | 13 (0.57) | 15 | $21,043 [14,019] |
| Carpal tunnel release (bilateral) | 9 (0.39) | 9 | $2572 [1,736] |
| Uvulopalatopharyngoplasty and other sleep apnea procedures | 50 (2.18) | 65 | $31,375 [27,394] |
| Colonoscopies and colonic procedures for polyps/tumors | 288 (12.58) | 300 | $2179 [1,463] |
| Frontal protrusion corrected by osteotomy | 2 (0.09) | 2 | $42,864 [42,864] |
| Vertical and anteroposterior facial disproportion by bimaxillary procedures | 2 (0.09) | 2 | $42,864 [42,864] |
| Nasal deformity by rhinoplasty or skull bone grafting | 47 (2.05) | 51 | $34,708 [27,720] |
| Macroglossia by tongue resection | 0 (0) | 0 | N/A [N/A] |
†
Among 2289 acromegaly patients.
‡
Total admission costs of inpatient or outpatient surgeries, including costs of other surgeries or services done during the same admission.
§
Arthroplasty (complete and partial), arthrodesis and osteotomy, focusing on specific joints – hip, knee, shoulder, hand and foot.
Discussion
Patients with acromegaly use substantially more healthcare services and have higher costs than patients without acromegaly. Hospitalization is four-times more common among acromegaly patients than among those without acromegaly. Mean total healthcare costs are over fourfold higher for patients with acromegaly than patients without acromegaly. Mean total healthcare costs are over fourfold higher for patients with acromegaly than patients without. Among patients with acromegaly, high-risk comorbidities and procedures are associated with even higher costs.
No published studies have examined healthcare costs among patients with acromegaly in administrative claims data since the FDA approval of oral octreotide in 2020, and recent data on HCRU associated with acromegaly is limited [15]. Consistent with the current work, older studies reported a range of inpatient hospitalization rates (22–34.6%) and ED visits (20.2–28.3%) among patients with acromegaly [15–17], as well as a multifold higher hospitalization rate than matched controls [16]. The current study’s total costs (all-cause and acromegaly-related) were higher than those published in previous studies using older administrative claims data (all costs adjusted to 2023 USD) [16–18,23–25]. Placzek and colleagues reported acromegaly-related costs (medical and pharmacy) of $19,324, which is lower than the $30,985 (both adjusted to 2023 USD) in our study [17]. The main driver of the difference between these acromegaly-related costs appears to be related to therapy costs. Placzek and colleagues reported prescription (pharmacy) costs of $10,895 compared with the $25,895 we found (both inflation-adjusted to 2023 USD) [17]. In our study, total healthcare costs were highest for patients with acromegaly and high-risk comorbidities or procedures. Thus, despite the introduction of a new SRL, the humanistic and HCRU burden among patients with acromegaly remains high, with 20% of patients having at least one inpatient hospitalization in a year.
We reported higher rates of patients using acromegaly medical therapy compared with an older 2015 study that also used a prevalent acromegaly cohort [25]. This is an expected result, given that the proportion of patients receiving acromegaly medical therapy has increased over time [26,27]. However, the use of medical therapy in our cohort was somewhat lower than the 43–60% of patients with persistent or recurrent acromegaly [28–30]. This suggests that there is a portion of patients with persistent acromegaly who remain untreated and represents a significant unmet need in disease management for patients with high-risk comorbidities. Studies that assessed acromegaly therapy during earlier stages of the disease course found higher proportions of cabergoline and bromocriptine [18,25]. Over time, patients treated with cabergoline tend to discontinue, switch to a different therapy, or add-on an additional therapy [14]. This study was designed as a prevalent cohort to represent the full spectrum of the disease impact from initial diagnosis and treatment to the long-term impacts of well-controlled disease and acromegaly with high-risk comorbidities. The differences in the patients represented in each study explains why the current study’s proportion of patients on cabergoline is relatively low. While treatment switching may signal that patients are progressing to therapies that are more effective over time, it also raises questions about whether patients have access to the newer, more effective, treatment options soon after their initial diagnoses. Addressing these gaps in treatment utilization is essential for improving patient outcomes and reducing disease burden. This study’s design also explains why the current study’s proportion of patients who underwent pituitary surgery is low (9.0%) compared with other studies that report whether patients with acromegaly had ever received pituitary surgery (96.3%); this analysis only captured procedures documented during the 1-year observation period [31].
This was a retrospective cross-sectional study using claims data from a large, longitudinal health plan database that was conducted over several years. The primary purpose of administrative claims data is to support reimbursement; thus, the identification of patients with acromegaly with and without high-risk comorbidities based on diagnosis and procedure codes has not been validated and may be inaccurate. The following claims-based studies use the same, or similar, definition for identifying acromegaly in claims data [14,16–18,23–25,32,33]. Undiagnosed patients or those not seeking acromegaly-related care would not have been captured in this study. Also, results may not be generalizable to patients with incident cases of acromegaly, as our study cohort included patients at varying stages of disease. We identified patients diagnosed with high-risk conditions, rather than with laboratory testing, as the claims database used for this study had no information on test results. Commercial claims databases have limited coverage of patients aged 65 years or older, so data reported here may not be generalizable to the older population or to uninsured populations.
Conclusion
Despite the introduction of new medical therapies, patients with acromegaly still have substantial HCRU and costs compared with those without acromegaly. These costs are primarily driven by inpatient hospitalizations, other outpatient services (non-ED/non-office), and outpatient pharmacy. Patients with acromegaly who have high-risk comorbidities or procedures incur the highest costs and unmet need. New treatments that can provide better disease control could lead to lower HCRU, costs and symptom burden.
Summary points
•
No published studies have examined healthcare costs among patients with acromegaly in administrative claims data since the US FDA approval of oral octreotide in 2020, and recent data on healthcare resource utilization (HCRU) associated with acromegaly are limited. Prolonged exposure to elevated growth hormone levels increases the risk of comorbidities and mortality for patients with acromegaly.
•
This retrospective cohort study used 2017–2022 administrative claims data (IQVIA Pharmetrics Plus®) to compare HCRU and costs between patients with acromegaly and a reference group of patients without acromegaly, and, in a secondary analysis, analyzed patients with acromegaly who also have high-risk comorbidities and procedures.
•
Patients with acromegaly have a higher comorbidity burden than the matched reference group without acromegaly (Charlson Comorbidity Index: 1.3 vs 0.6, p < 0.001).
•
A fourfold greater proportion of patients with acromegaly have an inpatient hospitalization than the matched reference group without acromegaly.
•
Mean total healthcare costs are higher for patients with acromegaly than for the matched reference group ($51,888 vs $10,601).
•
Among patients with acromegaly, acromegaly therapy costs ($25,895) account for the majority of mean total acromegaly-related healthcare costs ($30,985); however, only 41% of patients with acromegaly have evidence of acromegaly therapy.
•
Mean all-cause healthcare costs are higher for patients with each comorbidity of interest than those without, with the largest mean cost difference seen for osteoarthritis ($28,486; p < 0.001).
•
The most frequent surgeries associated with acromegaly with high-risk comorbidities are colonoscopies and colonic procedures for polyps/tumors (12.6% of cases), and the costliest surgeries are lumbar and cervical spine fusions and laminectomies ($60,760; 0.8% of patients).
•
An unmet need remains for patients with acromegaly, especially those with high-risk comorbidities. Better disease control among patients with acromegaly could lead to lower HCRU, costs and symptom burden.
Author contributions
TP Quock, SK Rattana and IE Paulson: acquisition of data; design of the work; interpretation of data; revising the work for important intellectual content; final approval. E Chang, AK Das, A Speller, MH Tarbox, ML Rossi and MS Broder: design of the work; analysis of data; interpretation of data; drafting and revising the work for important intellectual content; final approval.
Financial disclosure
Funding for this study and publication-related fees were received from Crinetics Pharmaceuticals, Inc.
Competing interests disclosure
TP Quock, SK Rattana and IE Paulson are employees of, and hold stock in Crinetics Pharmaceuticals, Inc. at the time of this study. E Chang, AK Das, MH Tarbox and MS Broder were employees of Partnership for Health Analytic Research, LLC (now ADVI Health), which received funding from Crinetics to conduct the research described in this manuscript. PHAR also discloses financial relationships with the following commercial entities outside of the submitted work: Abbvie, Akcea, Amgen, Astellas, AstraZeneca, Delfi Diagnostics, Dompe, Exact Sciences Corporation, Genentech, Gilead, GRAIL, Ionis, Janssen, Nobelpharma, Novartis, Pfizer, Recordati, Regeneron and Sanofi US Services. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 44.14 KB
References
Papers of special note have been highlighted as: • of interest
1.
Holdaway IM, Rajasoorya C. Epidemiology of acromegaly. Pituitary 2(1), 29–41 (1999).
2.
Carmichael JD, Broder MS, Cherepanov D et al. The association between biochemical control and cardiovascular risk factors in acromegaly. BMC Endocr. Disord. 17(1), (2017).
• This prospective cohort study of a single-center acromegaly registry investigated the comorbidity burden among patients with acromegaly and highlighted the challenge of achieving disease control for those with uncontrolled disease.
3.
Colao A, Ferone D, Marzullo P, Lombardi G. Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr. Rev. 25(1), 102–152 (2004).
4.
Carroll PV, Joshi MN. Acromegaly. In: Endotext. Feingold KR, Ahmed SF, Anawalt Bet al. et al. (Eds)., MDText.com, Inc, MA, USA (2000).
5.
Orme SM, McNally RJ, Cartwright RA, Belchetz PE. Mortality and cancer incidence in acromegaly: a retrospective cohort study. United Kingdom Acromegaly Study Group. J. Clin. Endocrinol. Metab. 83(8), 2730–2734 (1998).
6.
Chanson P, Salenave S. Acromegaly. Orphanet. J. Rare Dis. 3(1), 17 (2008).
7.
Chanson P, Salenave S, Kamenicky P, Cazabat L, Young J. Acromegaly. Best Pract. Res. Clin. Endocrinol. Metab. 23(5), 555–574 (2009).
8.
Melmed S. Acromegaly. N. Engl. J. Med. 355(24), 2558–2573 (2006).
9.
Melmed S, Bronstein MD, Chanson P et al. A consensus statement on acromegaly therapeutic outcomes. Nature Rev. Endocrinol. 14(9), 552–561 (2018).
• In this consensus statement, experts reviewed current literature on acromegaly treatments and patient outcomes. They highlighted variable response rates to somatostatin receptor ligands, cabergoline and pegvisomant, along with high rates of cardiovascular, musculoskeletal, metabolic complications among patients with acromegaly.
10.
Ezzat S, Serri O, Chik CL et al. Canadian consensus guidelines for the diagnosis and management of acromegaly. Clin. Invest. Med. 29(1), 29–39 (2006).
11.
Carmichael JD, Bonert VS, Nuño M, Ly D, Melmed S. Acromegaly clinical trial methodology impact on reported biochemical efficacy rates of somatostatin receptor ligand treatments: a meta-analysis. J. Clin. Endocrinol. Metab. 99(5), 1825–1833 (2014).
12.
Colao A, Auriemma RS, Pivonello R, Kasuki L, Gadelha MR. Interpreting biochemical control response rates with first-generation somatostatin analogues in acromegaly. Pituitary 19(3), 235–247 (2016).
13.
Giustina A, Chanson P, Kleinberg D et al. Expert consensus document: a consensus on the medical treatment of acromegaly. Nat. Rev. Endocrinol. 10(4), 243–248 (2014).
14.
Fleseriu M, Barkan A, Brue T et al. Treatment patterns, adherence, persistence, and health care resource utilization in acromegaly: a real-world analysis. J. Endocrine Soc. 7(10), bvad104 (2023).
• This retrospective study used data from a large US commercial claims database to investigate health care utilization, disease burden and treatment patterns among acromegaly patients. The authors found higher healthcare utilization rates among patients with comorbidities, which may have been due to an increased disease burden.
15.
Daniel CP, Wagner MJ, Borne GE et al. Acromegaly: pathophysiological considerations and treatment options including the evolving role of oral somatostatin analogs. Pathophysiology 30(3), 377–388 (2023).
16.
Ribeiro-Oliveira A, Brook RA, Munoz KA et al. Burden of acromegaly in the United States: increased health services utilization, location of care, and costs of care. J. Med. Econ. 24(1), 432–439 (2021).
• This retrospective study used administrative claims data from a US employer database and reported higher healthcare utilization rates and healthcare costs among patients with acromegaly compared with matched controls.
17.
Placzek H, Xu Y, Mu Y, Begelman SM, Fisher M. Clinical and economic burden of commercially insured patients with acromegaly in the United States: a retrospective analysis. J. Manag. Care Spec. Pharm. 21(12), 1106–1112 (2015).
• This retrospective study used administrative claims data from a commercially insured US population to assess the disease burden among patients with acromegaly. The authors highlighted the need for improved disease management strategies due to high acromegaly-related healthcare costs.
18.
Burton T, Le Nestour E, Bancroft T, Neary M. Real-world comorbidities and treatment patterns of patients with acromegaly in two large US health plan databases. Pituitary 16(3), 354–362 (2013).
• This retrospective study used administrative claims data from two US commercial health plan databases and emphasized the high incidence of comorbidities associated with acromegaly, especially among patients who received acromegaly-related treatment. This finding may reflect insufficient disease management and poor disease control.
19.
Liu J, Barrett JS, Leonardi ET et al. Natural history and real-world data in rare diseases: applications, limitations, and future perspectives. J. Clin. Pharmacol. 62(Suppl. 2), S38–S55 (2022).
20.
Konrad R, Zhang W, Bjarndóttir M, Proaño R. Key considerations when using health insurance claims data in advanced data analyses: an experience report. Health Syst. (Basingstoke) 9(4), 317–325 (2019).
21.
Behrendt C-A, Debus ES, Mani K, Sedrakyan A. The strengths and limitations of claims based research in countries with fee for service reimbursement. Eur. J. Vasc. Endovasc. Surg. 56(5), 615–616 (2018).
22.
Bureau of Labor Statistics. Consumer price index, medical care, 2014–2024 (2024). Available at: https://data.bls.gov/timeseries/CUUR0000SAM?output_view=data
23.
Broder MS, Neary MP, Chang E, Cherepanov D, Katznelson L. Treatments, complications, and healthcare utilization associated with acromegaly: a study in two large United States databases. Pituitary 17(4), 333–341 (2014).
• This retrospective study used administrative claims data from two US databases and found that complications were common among patients with acromegaly patients, leading to increased healthcare utilization. The authors postulated that improved disease management might reduce healthcare utilization and costs.
24.
Yuen KCJ, Munoz KA, Brook RA et al. Health benefit costs and absenteeism among employed patients with acromegaly. Endocr. Pract. 27(10), 1034–1039 (2021).
25.
Chuang C-C, Bhurke S, Chen S-Y, Dinet J, Brulais S, Gabriel S. Treatment patterns and economic burden in patients treated for acromegaly in the USA. Drugs – Real World Outcomes 2(3), 299–309 (2015).
26.
Aagaard C, Christophersen AS, Finnerup S et al. The prevalence of acromegaly is higher than previously reported: changes over a three-decade period. Clin. Endocrinol. 97(6), 773–782 (2022).
27.
Karapanou O, Tzanela M, Christoforaki M et al. Therapeutic trends and outcome of acromegaly: a single center experience over a 40-year period. Hormones 15(3), 368–376 (2016).
• This retrospective single-center study in Greece evaluated acromegaly treatment trends and outcomes over a 40-year period and reported higher rates of medical treatment over time. Although the authors found improvements in acromegaly outcomes in the last 20 years, they highlighted that many patients still experience uncontrolled disease.
28.
Cremaschi A, Sala E, Lavezzi E et al. Recurrence in acromegaly: two tertiary centers experience and review of the literature. J. Endocrinol. Invest. 47(9), 2269–2277 (2024).
29.
Del Porto LA, Liubinas SV, Kaye AH. Treatment of persistent and recurrent acromegaly. J. Clin. Neurosci. 18(2), 181–190 (2011).
30.
Kyriakakis N, Seejore K, Hanafy A, Murray RD. Management of persistent acromegaly following primary therapy: the current landscape in the UK. Endocrinol. Diabetes Metab. 3(3), e00158 (2020).
31.
Donegan DM, Iñiguez-Ariza N, Sharma A et al. Necessity of multimodal treatment of acromegaly and outcomes. Endocr. Pract. 24(7), 668–676 (2018).
32.
Burton T, Le Nestour E, Neary M, Ludlam WH. Incidence and prevalence of acromegaly in a large US health plan database. Pituitary 19(3), 262–267 (2016).
33.
Broder MS, Chang E, Cherepanov D, Neary MP, Ludlam WH. Incidence and prevalence of acromegaly in the United States: a claims-based analysis. Endocr. Pract. 22(11), 1327–1335 (2016).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 May 2025
Accepted: 26 June 2025
Published online: 8 July 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Healthcare utilization and costs among patients with acromegaly in the United States. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0069
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Miranda Perez, William Zeng, Ishan Shah, David Gomez, Apurva Prasad, David J. Cote, Robert Grady Briggs, Jonathan Sisti, John D. Carmichael, Gabriel Zada, Outcomes Following Endoscopic Transsphenoidal Reoperation for Residual or Recurrent Growth-Hormone Secreting Pituitary Adenomas Causing Acromegaly, Journal of Neurological Surgery Part B: Skull Base, 10.1055/a-2872-1335, (2026).
- Eliza B Geer, Jill Sisco, The acromegaly patient experience: burden of treatment and quality of life, The Journal of Clinical Endocrinology & Metabolism, 10.1210/clinem/dgag122, 111, Supplement_1, (S123-S145), (2026).
- Hayri Bostan, Iris C. M. Pelsma, Nienke R. Biermasz, Sex-related differences in healthcare utilization and costs among patients with pituitary adenomas, Pituitary, 10.1007/s11102-026-01638-0, 29, 1, (2026).
- Maxwell Koobatian, Jill Sisco, Janetricks C. Okeyo, Alan Krasner, Tiffany P. Quock, Real-world burden of disease, treatment, and healthcare resource utilization in acromegaly: a quantitative survey of patient experiences, Journal of Patient-Reported Outcomes, 10.1186/s41687-025-00965-3, 9, 1, (2025).