Evaluation of the efficacy and cost-effectiveness of safinamide versus rasagiline: a systematic review
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This systematic review aimed to evaluate the comparative efficacy, safety and cost-effectiveness of safinamide (50/100 mg) versus rasagiline (1 mg) in managing Parkinson’s disease (PD). Materials & methods: Randomized clinical trials were identified through systematic searches of PubMed, Embase and Cochrane databases (last searched September 2023). Eligibility criteria included studies assessing Unified Parkinson’s Disease Rating Scale (UPDRS) scores, On/Off time and adverse events. Risk of bias was evaluated using funnel plots, and data synthesis employed odds ratios, number needed to treat (NNT) and incremental cost-effectiveness ratios, calculated using the current costs of safinamide and rasagiline in Spain. Results: Thirteen trials (n = 4157 participants) were included. Safinamide demonstrated greater efficacy (NNT-UPDRS: 6 vs 8) and safety (number needed to harm-serious adverse events: 135 vs 83) compared with rasagiline. The benefit-risk balance of safinamide was superior, as evidenced by higher likelihood of being helped over harmed ratios. Cost-effectiveness analysis revealed lower costs per NNT for On/Off time with safinamide. While rasagiline treated more patients within a fixed budget, safinamide achieved better responder-to-nonresponder ratios. Conclusion: Safinamide showed superior efficacy, safety and cost-efficiency compared with rasagiline, supporting its use as a preferred adjunct therapy for PD. Limitations include reliance on clinical trial data and Spanish cost models. Future research incorporating real-world evidence is warranted.
Plain language summary
What is this article about?
Parkinson’s disease (PD) is a condition that affects the brain and causes movement problems such as stiffness, shaking and difficulty with balance. As PD gets worse over time, people with the condition may also experience memory and thinking problems. To help manage these symptoms, doctors often use medicines that improve movement and reduce complications. Two such medicines are safinamide and rasagiline, which are used alongside another common treatment called levodopa.
This study compared safinamide and rasagiline to find out which one works better, is safer and is more cost-effective for treating people with PD. Researchers looked at results from 13 studies involving over 4000 people. They measured how well each medicine improved symptoms, how often they caused side effects and how much they cost.
What were the results?
The results showed that safinamide worked slightly better than rasagiline in improving symptoms and had fewer serious side effects. Safinamide also helped reduce the amount of time people spent in ‘Off’ periods (times when their usual medicine stops working well). Although rasagiline could treat more people for the same budget, safinamide was more effective in helping people improve their symptoms.
What do the results mean?
This study helps healthcare providers decide which medicine might be the best option for people with PD, considering both the benefits and the costs. However, the findings are based on clinical trial data and future research is needed to confirm these results in real-world settings.
Parkinson’s disease (PD) is a chronic and progressive neurodegenerative disorder that is clinically manifested by symptoms such as bradykinesia, tremor, rigidity and postural instability [1]. Additionally, a considerable proportion of individuals with PD eventually develop dementia, further complicating the management of the disease and exacerbating its impact on health systems and caregivers [1].
Although PD predominantly affects older adults, it is not exclusive to this age group as younger individuals may also develop the condition [2]. Epidemiological data indicate a higher prevalence of PD among males compared with females [2]. The etiology of PD remains elusive; however, genetic predispositions, and environmental factors, have been implicated in increasing the risk of developing PD [3].
Global statistics from 2019 report that more than 8.5 million individuals are living with PD [4]. Projections indicate a significant escalation in the burden of PD over the coming decades [5]. The burgeoning prevalence of PD imposes considerable challenges on societal structures, individual lives and healthcare systems [6].
Despite the growing impact of PD, health and welfare systems in many nations remain underprepared to handle the complications associated with an aging population [7]. Thus, there is a pressing need for effective management strategies and the development of innovative treatments to mitigate the progression of PD and alleviate its societal and economic burdens [7].
Since the introduction of levodopa, it has remained the cornerstone of PD treatment due to its effectiveness, tolerability and cost-effectiveness [8]. However, chronic use of levodopa often leads to motor complications as the disease progresses [8]. In response, adjunct therapy with monoamine oxidase B (MAO-B) inhibitors like safinamide and rasagiline, has become a validated strategy to mitigate these side effects after being approved by the EMA [9–11]. Numerous studies have affirmed the efficacy and safety of these MAO-B inhibitors when used in conjunction with levodopa [9].
In the current economically strained healthcare environment, assessing both the efficacy and the economic efficiency of new therapies is imperative [12]. Therefore, there is a critical need for studies that evaluate both the efficacy and safety of treatments in conjunction with their associated costs.
This study aims to assess the cost-effectiveness of the MAO-B inhibitor safinamide (50/100 mg) compared with rasagiline (1 mg) from an evidence-based medicine perspective. This evaluation will help determine which therapy offers the best value in health in managing PD within the constraints of current healthcare budgets.
Materials & methods
The present study adheres to established guidelines and has been structured in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement [13].
Literature search
We conducted searches of the PubMed, Embase and Cochrane Review databases up to September 2023. The search strategy used was: ((Parkinson disease[Title/Abstract]) AND (safinamide[Title/Abstract])) and ((Parkinson disease[Title/Abstract]) AND (rasagiline[Title/Abstract])).
Study selection
Titles and abstracts of all retrieved citations were independently screened by two reviewers to identify potentially relevant publications, extract the data and evaluate the bias risk.
Inclusion criteria were randomized controlled trials (RCTs), participants diagnosed with PD, comparison of safinamide and/or rasagiline with placebo, availability of quantitative outcomes including Unified Parkinson’s Disease Rating Scale (UPDRS), On/Off time or adverse events.
Exclusion criteria included nonhuman studies, reviews or meta-analyses, studies without extractable efficacy or safety data, duplicates or secondary analyses of previously published pivotal trials.
Data extraction
Data elements extracted from the studies included the size of the control group and intervention group, ‘Off time’, ‘On time’, change in the UPDRS score, number of patients achieving a change in UPDRS score of at least 30% above baseline (responder patients), number of patients with serious adverse events (SAE; a drug-related adverse event was defined as any unexpected or detrimental event in the participant related to the drug) and number of patients withdrawing the drug due to adverse events.
The minimum time horizon has been 24 weeks of treatment.
All calculations were weighted according to the size of the control group and intervention group.
Costs used in the pharmacoeconomic analysis
For the analysis, only the direct costs associated with the current medication at the ex-factory price in Spain were considered, and all costs are presented in Euros (€), as detailed in Supplementary Table 1.
Assessment of risk of bias in selected studies
Publication bias was evaluated using funnel plots. Subgroup analyses with direct comparisons for prespecified variables were also conducted. Additionally, sensitivity analyses were performed to assess the robustness of the results by repeating the analyses using a Bayesian hierarchical model and both a fixed-effect model and a random-effects model.
Data analysis & statistical methods
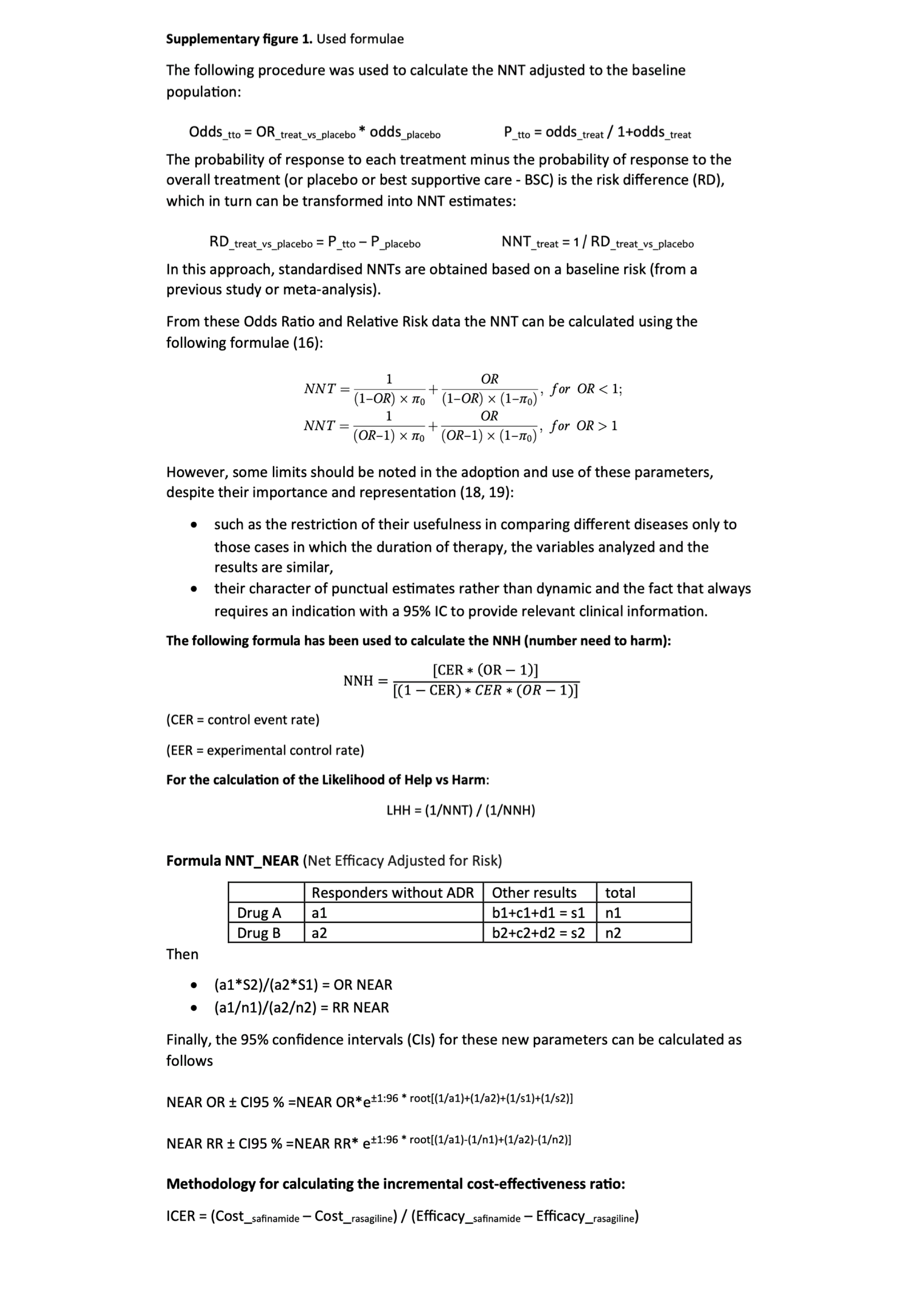
In this study, we employed several statistical metrics to assess the therapeutic efficacy and safety of the treatments under investigation, including the number needed to treat (NNT), number needed to harm (NNH), and the likelihood of being helped or harmed (LHH). Net efficacy adjusted for risk (NEAR) a simple quantitative indicator of risk: benefit developed by Boada JN et al. [14], was also used. For the combined analysis of quantitative data (number of hours in On time/Off time and UPDRS scale score), the difference-in-differences (Diff and Diff) analysis methodology was used.
In this study, a comprehensive pharmacoeconomic evaluation was conducted to determine the economic viability and potential healthcare impact of the investigated therapies. The pharmacoeconomic metrics used included cost-effectiveness analysis (CEA), incremental cost-effectiveness ratio (ICER) and a budget impact analysis using a fixed pharmacy budget of €100,000 per year.
All the formulas used are detailed in Supplementary Figure 1 [15].
Statistical analysis
Calculations were performed for the probabilities of improvement on the odds ratios (OR) with a 95% CI were calculated for dichotomous outcomes, and mean differences with a 95% CI were calculated for continuous outcomes. For dichotomous outcomes, absolute effects were also calculated based on the pooled ORs and the initial risk (the average incidence rate in the placebo group).
UPDRS, SAE and withdrawals analyses were conducted using IBM SPSS version 26 (IBM; Armonk, NY, USA). Data comparison from the various studies analyzed were processed with Meta-Essentials (Erasmus Research Institute of Management) [16], and a calculator for meta-analysis developed by J Primo, recommended by the GENESIS group of the SEFH, for obtaining data corresponding to the OR/risk ratio for two subgroups (e.g., drug vs placebo) [17].
Heterogeneity among trials within each comparison was assessed using the I2 statistic.
Results
Included studies
Figure 1 illustrates the flowchart of the search strategy employed in this study.
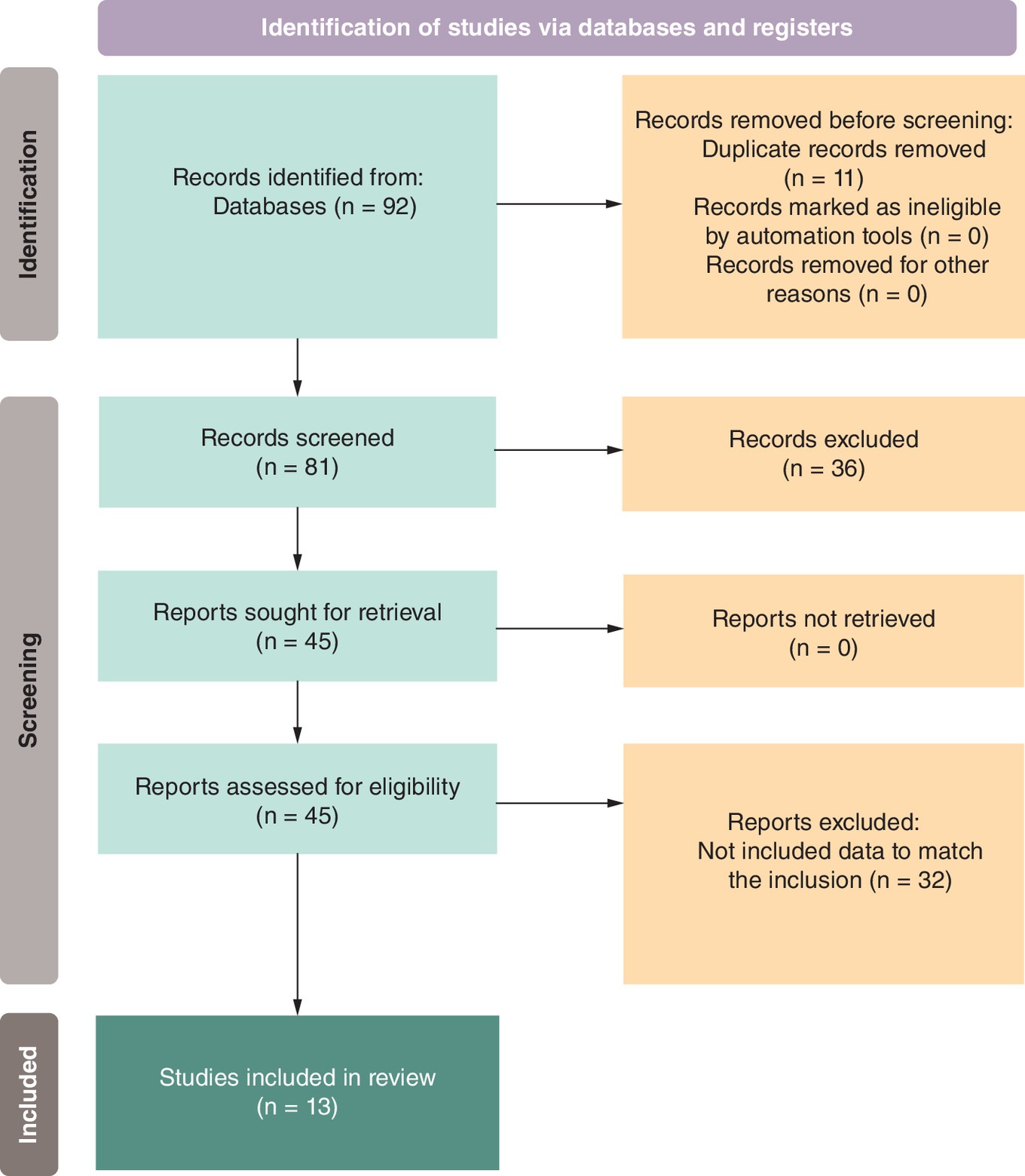
The search yielded 45 citations that included studies in English or Spanish that compared study drugs with placebo (controlled clinical trial or controlled study or meta-analysis or RCT or systematic review), analyzed the required variables and were free text.
After removing articles that did not meet the inclusion/exclusion criteria, 13 phase III RCTs, documented across 13 publications [18–30], were selected for analysis.
Treatment versus placebo
Treatment (combined data of safinamide and rasagiline) versus placebo analysis results are summarized in Table 1. The UPDRS analysis, incorporating data from 13 studies with 3713 patients, revealed a statistically significant (p < 0.0001) OR of 1.97 (95% CI: 1.75–2.22) when compared with placebo. Heterogeneity was moderate, indicated by an I2 of 46%, despite a Q of 22.19. For SAEs, the integration of data from 12 studies including 4061 patients demonstrated an OR of 1.06 (95% CI: 0.76–1.49), which was not statistically different from placebo. The heterogeneity for this metric was low, with an I2 of 22% and a Q of 11.10 (p = 0.43). In the case of withdrawals, pooling results from 15 studies with 4157 patients showed an OR of 0.96 (95% CI: 0.95–0.96), indicating no significant difference from comparators. This outcome displayed minimal heterogeneity, with an I2 of 0% and a Q of 7.94 (p = 0.89), suggesting a consistent effect across studies.
| Studies | Patients | Odds ratio (IC 95%) | p-value | Q | p-value | I2 (%) | |
|---|---|---|---|---|---|---|---|
| UPDRS | 13 | 3713 | 2.02 (1.65–2.47) | 0.00000 | 22.19 | 0.036 | 46 |
| SAEs | 12 | 4061 | 1.06 (0.76–1.49) | 0.89738 | 11.10 | 0.43 | 22 |
| Withdrawals | 15 | 4157 | 0.96 (0.95–0.96) | 0.70417 | 7.90 | 0.89 | 0 |
SAE: Serious adverse event; UPDRS: Unified Parkinson’s Disease Rating Scale.
Efficacy & safety of safinamide & rasagiline versus placebo
Number needed to treat
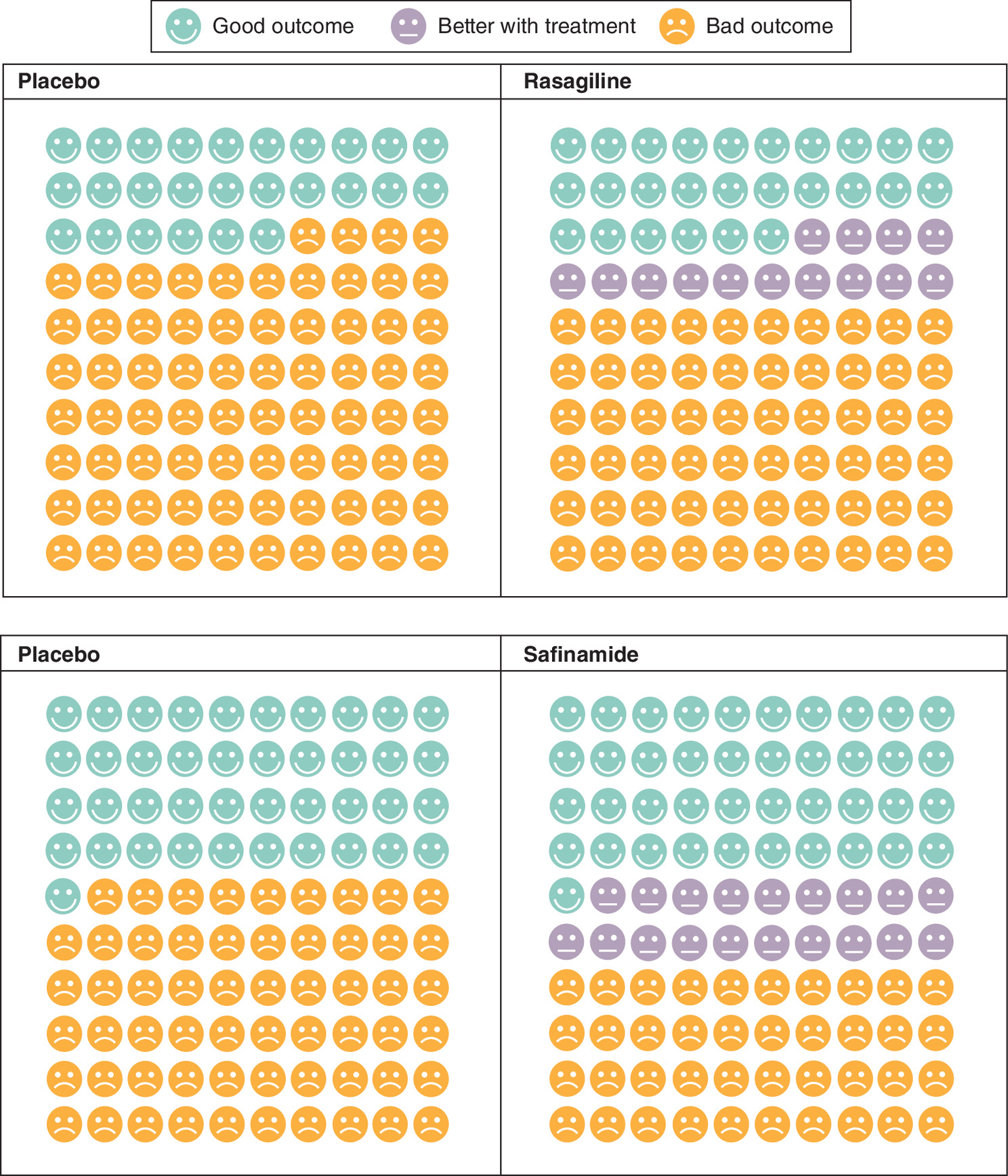
The study examined the effect of two treatments, rasagiline and safinamide, on the UPDRS (Table 2 and Figure 2). For rasagiline, data from eight studies involving 1742 patients showed an NNT-UPDRS of 8 with an OR of 1.91 (95% CI: 1.46–2.50). Safinamide was evaluated across five studies including 1971 patients, indicating an NNT-UPDRS of 6 with an OR of 2.17 (95% CI: 1.23–3.84), suggesting a higher efficacy.
| Treatment | Studies | Parameter | n | Odds ratio (IC 95%) | NNT or NNH |
|---|---|---|---|---|---|
| Rasagiline | 8 | UPDRS | 1742 | 1.91 (1.46–2.50) | 8 |
| Safinamide | 5 | 1971 | 2.17 (1.23–3.84) | 6 | |
| Rasagiline | 12 | SAEs | 1769 | 1.20 (0.83–1.74) | 83 |
| Safinamide | 6 | 2292 | 0.88 (0.53–1.47) | 135 | |
| Rasagiline | 12 | Withdrawals | 1865 | 0.96 (0.77–1.21) | 214 |
| Safinamide | 6 | 2292 | 0.96 (0.66–1.39) | 460 |
NNH: Number needed to harm; NNT: Number needed to treat; SAE: Serious adverse event; UPDRS: Unified Parkinson’s Disease Rating Scale.
Number needed to harm
NNH analysis of rasagiline and safinamide is presented in Table 2. SAE data for rasagiline was extracted from 12 studies including 1769 patients, and indicated an OR of 1.20 (95% CI: 0.83–1.74) with a NNH-SAE of 83. Safinamide was assessed in six studies with 2292 patients, showing an OR of 0.88 (95% CI: 0.53–1.47). The NNH-SAE for safinamide was determined to be 135, suggesting an even lower risk of causing harm compared with rasagiline. No statistically significant increase in withdrawal rates compared with the control were found in both cases.
Regarding the analysis of withdrawals, rasagiline was assessed across 12 studies involving 1865 patients. The OR for withdrawals was 0.96 (95% CI: 0.80–1.16). The NNH for treatment withdrawals was calculated to be 214, indicating that one additional patient would discontinue treatment for every 214 patients treated compared to the control. Safinamide was examined in six studies with a larger sample size of 2292 patients. The OR of 0.96 (95% CI: 0.66–1.39) also indicates no significant difference in withdrawal rates compared with the control, similar to rasagiline. However, the NNH- withdrawals for safinamide is substantially higher at 460, implying that withdrawals are even less frequent compared with rasagiline.
Likelihood of being helped over harmed
Results of LHH are presented in Supplementary Table 2. Higher LHH ratios for safinamide were found in both LHH-SAEs and LHH withdrawals when compared with rasagiline. The data suggests that safinamide offers a more favorable balance between effectiveness and safety.
NNT of drugs adjusted for risk of an adverse event
The NNT-NEAR results are systematically presented in Supplementary Table 3. For both SAEs and withdrawals, safinamide demonstrated a superior efficacy ratio when compared with rasagiline, adjusted for the risk of adverse events. The results brought by this efficacy ratio underscore the favorable balance between therapeutic benefits and safety risks associated with safinamide.
Diff & diff analysis
Results of the NNT diff and diff analysis are presented in Supplementary Table 4. Lower NNT values for safinamide were found across all efficacy parameters, including Off time, On time and UPDRS, when compared with rasagiline. The data suggests that safinamide is more effective in reducing Off time, increasing On time and improving UPDRS scores.
Pharmacoeconomy
Results from a comprehensive cost-effectiveness analysis are presented in Figure 3 and Supplementary Table 5. As can be inferred from the results, the differences between the two drugs are minimal in several parameters (NNT; NNT-NEAR-SAE; NNT-NEAR-Withdrawals; and NNT-UPDRS). However, safinamide showed to be more efficient when compared with rasagiline in the variables ‘NNT-On time’ and ‘NNT-Off time’.
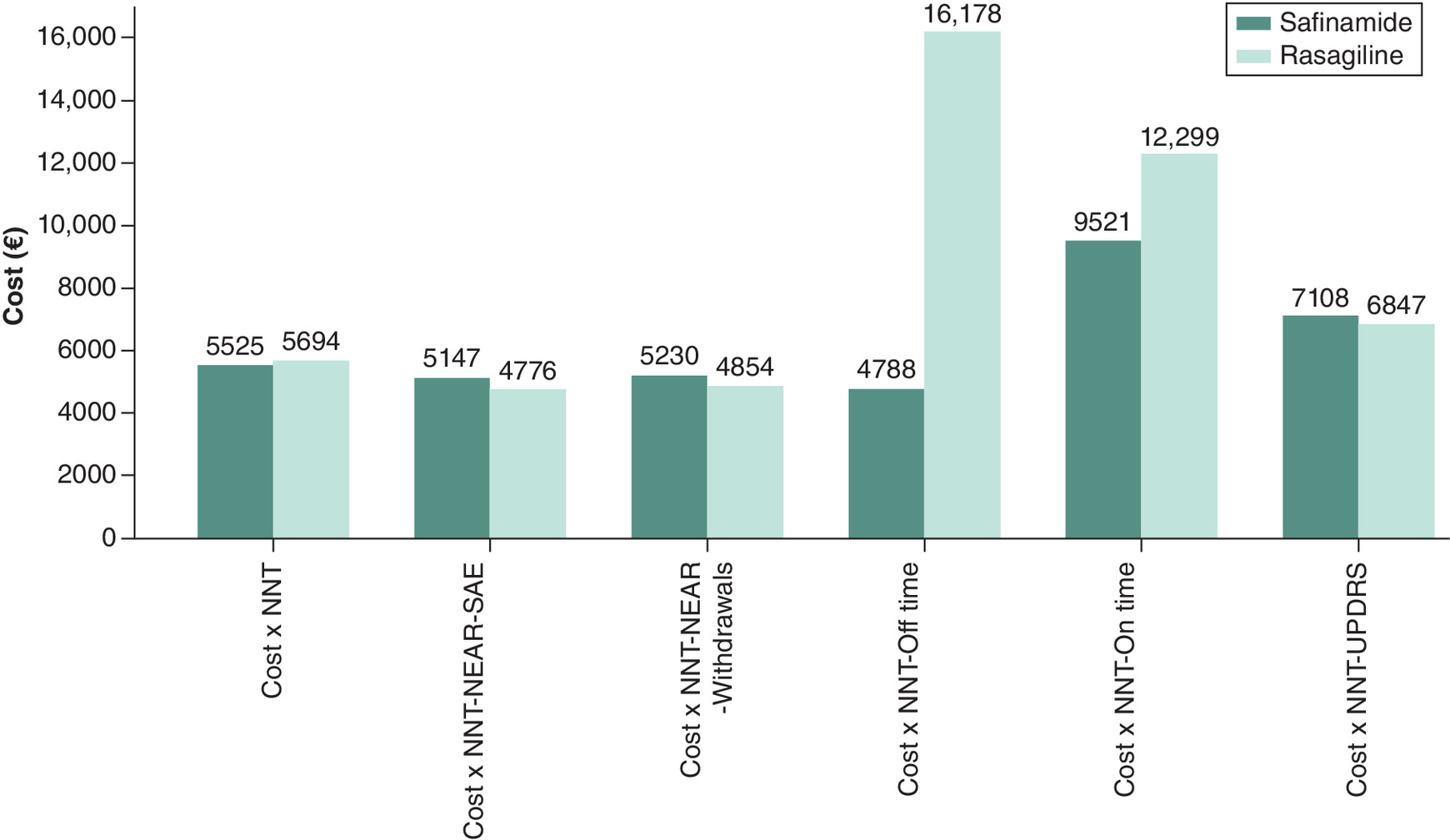
Figure 3. Cost-effectiveness comparison (per year).
ICER: Incremental cost-effectiveness ratio; NEAR: Net efficacy adjusted for risk; NNT: Number needed to treat; SAE: Serious adverse event; UPDRS: Unified Parkinson’s Disease Rating Scale.
Results from the ICER are summarized in Figure 4 and Supplementary Table 6. The cost of achieving greater efficacy with safinamide ranged from €1409.27 (NNT-Time Off) to €8171.36 (NNT-UPDRS).
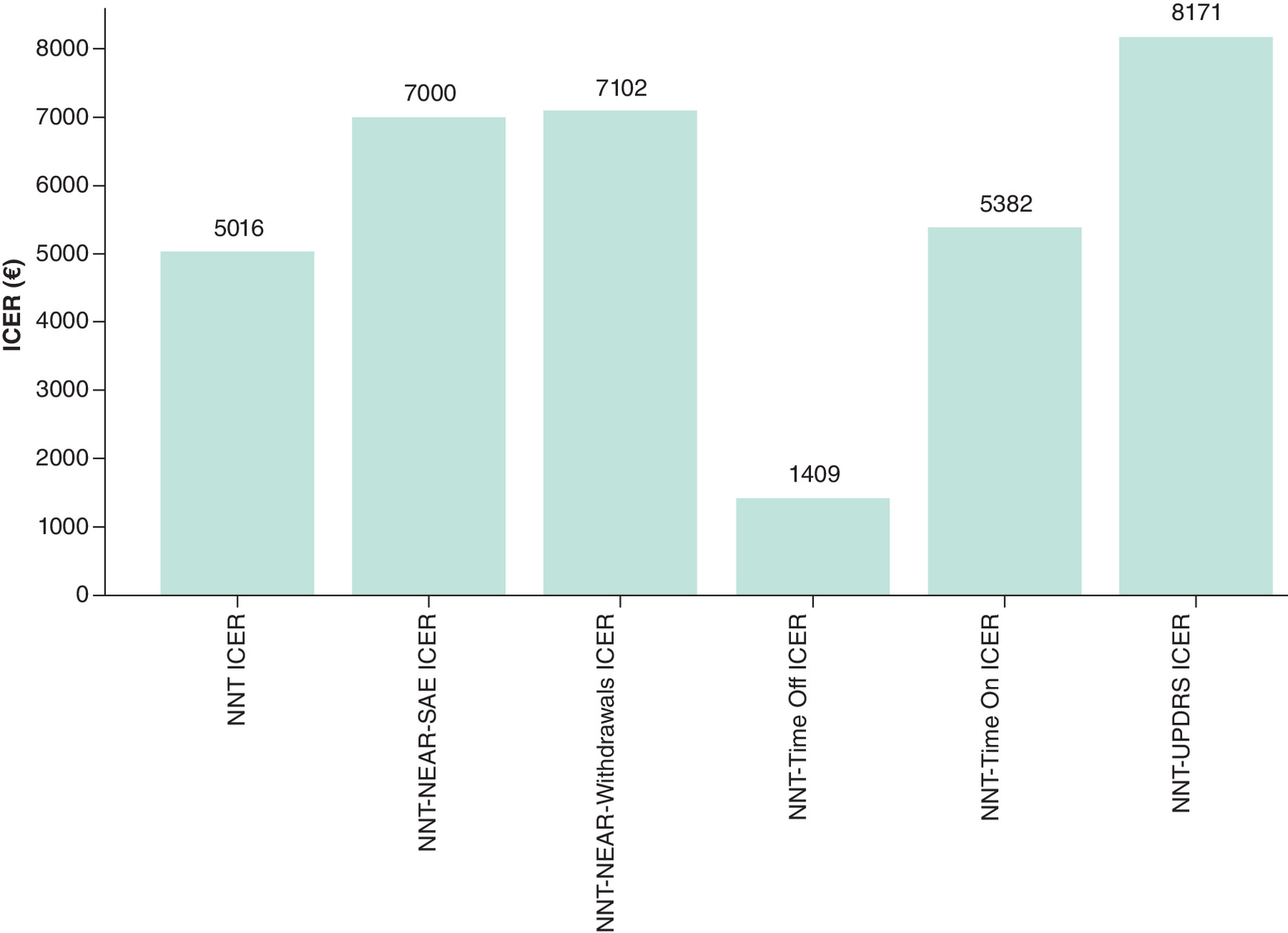
Figure 4. Incremental cost-effectiveness ratio.
ICER: Incremental cost-effectiveness ratio; NEAR: Net efficacy adjusted for risk; NNT: Number needed to treat; SAE: Serious adverse event; UPDRS: Unified Parkinson’s Disease Rating Scale.
Finally, the outcomes of a budget analysis conducted with a fixed pharmacy budget of €100,000/year are presented in Table 3. The OR figures indicate the number of times the responder/nonresponder ratio is better for safinamide versus rasagiline. As can be seen from the results presented, safinamide was superior to rasagiline in all cases.
| Treatment | Treated | R | NR | Ratio R/NR | OR | |
|---|---|---|---|---|---|---|
| NNT-UPDRS | Rasagiline | 140 | 17 | 124 | 0.14 | 1.40 |
| Safinamide | 109 | 17 | 91 | 0.19 | ||
| NNT-NEAR-SAE | Rasagiline | 140 | 21.07 | 119.42 | 0.18 | 1.24 |
| Safinamide | 109 | 20 | 89 | 0.22 | ||
| NNT-NEAR-WITHDRAWALS | Rasagiline | 140 | 20 | 120 | 0.17 | 1.21 |
| Safinamide | 109 | 18 | 90 | 0.20 | ||
| NNT-TIME Off | Rasagiline | 140 | 6 | 134 | 0.05 | 4.98 |
| Safinamide | 109 | 21 | 88 | 0.23 | ||
| NNT-TIME ON | Rasagiline | 140 | 9 | 132 | 0.06 | 1.54 |
| Safinamide | 109 | 10 | 99 | 0.10 | ||
| NNT-UPDRS | Rasagiline | 140 | 14.05 | 126.45 | 0.11 | 1.37 |
| Safinamide | 109 | 14 | 94 | 0.15 |
Ex-factory price costs used: rasagiline; €711.75/year; safinamide: €920.77/year.
NR: Nonresponder; NEAR: Net efficacy adjusted for risk; NNT: Number needed to treat; R: Responder ; SAE: Serious adverse event; UPDRS: Unified Parkinson’s Disease Rating Scale.
Discussion
To our knowledge, this is the first study that compares the efficacy, safety and costs of safinamide versus rasagiline for the treatment of PD, as no other meta-analyses or systematic reviews have been published on this subject. Taking into account the considered parameters, the analysis revealed that safinamide consistently surpassed rasagiline across efficacy and safety metrics, including NNT, NNH and the LHH. Moreover, when evaluating the combined measures of efficacy and safety (NNT-NEAR), safinamide also demonstrated superior performance. In terms of cost-efficacy, safinamide outperformed rasagiline with respect to both NNT and NNT-NEAR. Additionally, safinamide presented lower costs per NNT for both On time and Off time. Although rasagiline could potentially treat a larger number of patients within a predefined pharmacy budget, safinamide showcased a more favorable responder to nonresponder ratio in all evaluated scenarios, emphasizing its superior efficacy and cost-efficiency. This comprehensive analysis underscores safinamide as a potentially more advantageous choice for the management of PD, considering both clinical outcomes and economic feasibility.
Given the financial strain on many healthcare systems, there is a critical need for treatment decisions that consider not only efficacy and safety but also economic impact [31]. Comprehensive evaluations can support clinicians, pharmacists and health managers in selecting cost-effective options. This is especially vital in PD, where increasing prevalence and treatment costs heighten the need for strategic, evidence-based therapy choices [32,33].
Previous studies have explored the efficacy, safety and cost-effectiveness of MAO-B inhibitors for PD, though with differing methodologies. In contrast, our study applies a comprehensive framework using NNT, NNH, LHH and NEAR to evaluate clinical outcomes, alongside a robust pharmacoeconomic analysis incorporating CEA, ICER and budget impact. These metrics – particularly NNT and NNH – help balance benefit and risk, and are widely recognized, including by the Spanish Society of Hospital Pharmacy [34–37]. Favorable profile of safinamide is supported by its dual mechanism of action – enhancing dopaminergic transmission and modulating glutamate – along with its reversibility, selectivity and superior bioavailability, distinguishing it among MAO-B inhibitors [38,39].
In healthcare management, the efficacy and safety of a drug, while crucial, are insufficient in isolation and must be complemented by favorable pharmacoeconomics [40]. Consequently, we have incorporated several analyses including CEA, ICER and assessments of the number of patients treatable within a fixed pharmacy budget of €100,000/year. CEA is fundamental as it evaluates the economic value of a drug by comparing the costs incurred to achieve specified health outcomes, thereby aiding decisions on drug coverage and patient access [41]. ICER plays a pivotal role in this context by providing a ratio that juxtaposes the additional cost of a drug against its health benefits relative to alternatives [42]. At last, assessing how many patients can be treated within a predetermined budget provides a tangible measure of the financial implications of drug selection. Our findings indicate that safinamide is more cost-effective, particularly evident in the ‘Off time’ and ‘On time’ metrics, where it demonstrates lower NNTs and costs per NNT compared with rasagiline. Furthermore, safinamide tends to yield a more favorable response ratio under fixed budget constraints in critical treatment areas. Although the cost per NNT may be marginally higher in some instances, the overall advantages in terms of treatment outcomes and enhanced capability to manage severe symptoms could justify the additional expenditure. In this regard, it is also important to consider broader economic impacts and health service metrics when analyzing the cost and effectiveness of any drug. The quality-adjusted life year (QALY) has served as the benchmark metric in these analyses worldwide for more than three decades, offering a standardized measure to assess how various medical interventions extend and improve the quality of patient life [43]. Within the framework of the Spanish National Health Service, a comprehensive study utilizing data from 17 regional health services established that the average cost per QALY ranges between €22,000 and €25,000 [44,45]. In the present study, QALY was not calculated because current controversies regarding QALYs impede their application in clinical decision-making [46]. For this reason, NNT, a standard clinical decision-making metric, was used [47]. The data collected showed that the incremental cost of treating with safinamide over rasagiline ranges from €1409.27 to €8171.36 in the efficacy parameters studied. Therefore, all the metrics studied indicated that the cost of improving the efficacy of the treatment in a patient by changing from rasagiline to safinamide is at least two-times lower than the established QALY threshold in Spain. This data should be taken into consideration when underscoring the economic viability of opting for safinamide, given its higher cost-effectiveness.
Concerning the economic analysis, it is also to be highlighted that this study focused solely on the monetary value of each treatment, yet the full economic impact of PD encompasses a broader array of costs directly affecting patients, their families and caretakers. A recent multinational, real-world, cost-of-illness study reported that only 9–32% of the total expenditures related to PD management in European countries correspond to drug treatments [33]. In contrast, these costs reach up to 62% and 68% in Japan and the US, respectively [33]. Therefore, it is important to note that other costs should also be considered in the comprehensive picture of PD management. While the literature lacks comprehensive analyses of the impact of safinamide and rasagiline on the overall costs of managing PD patients, other general cost studies can be interpreted to hypothesize the potential economic costs. Research indicates that PD patients who are better controlled, as measured by the UPDRS and ‘Off time’, incur lower care costs [48,49]. These observation supports the hypothesis that more effective disease management could also reduce the indirect costs associated with PD. Because safinamide resulted in a treatment that induce a lower UPDRS and lower Off time over rasagiline it is possible to speculate that safinamide also provides a lower indirect cost in the management of PD patients. In this context, the direct economic advantages observed with safinamide over rasagiline in this study might represent only a fraction of the total economic benefits that safinamide treatment could offer. Future research is needed to explore this hypothesis.
The results of the present study should be interpreted taking into account several limitations. The comparative analysis of safinamide versus rasagiline was performed using a modeling methodology rather than a direct comparison, which could impact the applicability of the findings. Regarding the cost estimation, as mentioned, it is important to note that the present study only considered medication costs, which can significantly influence the total cost-effectiveness assessment. Moreover, the costs used reflect the current prices established in Spain, a condition that may differ from other countries or that may vary substantially in the future. Finally, the dataset is exclusively derived from clinical trials; therefore, for a comprehensive evaluation of these medications in routine practice settings, the incorporation of real-world data is essential. It is also important to note that while all trials included in this review evaluated safinamide or rasagiline as adjunctive treatments to levodopa, there may have been variations in the background therapies, baseline UPDRS scores, age and disease duration among the enrolled patients. These differences may introduce heterogeneity that could influence efficacy and safety outcomes. As individual patient-level data were not available for our analysis, we could not perform adjustments for baseline comparability. This limitation should be considered when interpreting the results, as it represents a potential source of indirect comparison bias. Future studies aiming to perform a similar comparison in this condition would benefit from addressing these limitations to better inform clinical and economic decision making. Despite these limitations, we consider this study to be both unique and significant. To the best of our knowledge, this is the first report on the comparative cost-effectiveness of safinamide and rasagiline in the treatment of PD.
Conclusion
In conclusion, notwithstanding its intrinsic limitations, the indirect comparative analysis performed in this study suggests that safinamide exhibits enhanced efficacy and safety profiles, both individually and when considering the combination of the selected variables, compared with rasagiline. From a cost-effectiveness perspective, safinamide outperformed rasagiline in terms of the NNT and the NNT-NEAR. In this sense, it is to note that although rasagiline allows for a higher number of patients to be treated within a fixed pharmacy budget, the responder/nonresponder ratio for safinamide was superior across all comparisons. In a landscape where healthcare systems are experiencing financial strain, the significance of these findings in informing clinical practice, pharmaceutical management and healthcare policy cannot be overstated. Substantiating these observations will require future research complemented by real-world data, which promises to provide valuable and robust insights for clinicians, hospital pharmacists and health administrators.
Summary points
•
Parkinson’s Disease (PD) overview: PD is a chronic, progressive neurodegenerative disorder characterized by symptoms like bradykinesia, tremor, rigidity and postural instability. It also leads to dementia in many patients, increasing the burden on healthcare systems and caregivers.
•
Treatment challenges: Levodopa remains the primary treatment for PD, but long-term use leads to motor complications. Adjunct therapies like MAO-B inhibitors (e.g., safinamide and rasagiline) are efficacious and safe and help mitigate these side effects.
•
Need of the study: In the current economically strained healthcare environment, assessing the efficacy and cost-effectiveness of new therapies is imperative. There is a critical need for studies that evaluate treatments’ efficacy, safety and associated costs.
•
Study objective: This study evaluates the cost-effectiveness of the MAO-B inhibitors safinamide versus rasagiline in managing PD, focusing on efficacy, safety and economic impact within healthcare budget constraints.
•
Methodology: The study followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, analyzing data from 13 randomized controlled trials to compare the efficacy, safety and pharmacoeconomic metrics of safinamide and rasagiline.
•
Key findings: Safinamide demonstrated superior efficacy and safety over rasagiline, with lower number needed to treat and higher likelihood of being helped over harmed ratios and better Unified Parkinson's Disease Rating Scale scores. It also showed better cost-effectiveness in reducing ‘Off time’ and improving ‘On time’ in PD patients. Moreover, safinamide showed a more favorable benefit-risk balance and lower likelihood of treatment withdrawals.
•
Pharmacoeconomic analysis: Safinamide was more cost-effective than rasagiline, with lower incremental costs for achieving clinical benefits. However, rasagiline could treat more patients within a fixed pharmacy budget, though safinamide had a better responder-to-nonresponder ratio.
•
Clinical relevance: The study highlights the need for data-driven treatment decisions in financially strained healthcare systems, prioritizing therapies that balance efficacy, safety and economic feasibility.
•
Limitations: The study relied on indirect comparisons and clinical trial data, excluding real-world evidence. Cost analyses were based on Spanish medication prices, which may not reflect global variations.
•
Conclusion: Safinamide offers a more favorable balance of efficacy, safety and cost-effectiveness compared with rasagiline, making it a potentially superior choice for PD management. Further research with real-world data is needed to validate these findings.
Financial disclosure
This manuscript has been funded by Zambon Spain.
Competing interests disclosure
MJG Heredia has received honorariums for presentations, advice and/or attendance at scientific meetings from ABBVIE, Bial, Italfarmaco, UCB, Zambon. FPE has received honorariums for presentations, advice and/or attendance at scientific meetings from ABBVIE, Alter, Bial, Esteve, Italfarmaco, TEVA, UCB, Zambon. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Writing and editorial assistance was provided by Content Ed Net (Madrid, Spain) with funding from Zambon Spain.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
{kind=link}
References
1.
DeMaagd G, Philip A. Parkinson's disease and its management: Part 1: disease entity, risk factors, pathophysiology, clinical presentation, and diagnosis. P.T. 40(8), 504–532 (2015).
2.
Collier TJ, Kanaan NM, Kordower JH. Aging and Parkinson's disease: different sides of the same coin? Mov. Disord. 32(7), 983–990 (2017).
3.
Ball N, Teo WP, Chandra S, Chapman J. Parkinson's disease and the environment. Front. Neurol. 10, 218 (2019).
4.
World Health Organization. Parkinson disease: a public health approach: technical brief (2022).
5.
Kowal SL, Dall TM, Chakrabarti R, Storm MV, Jain A. The current and projected economic burden of Parkinson's disease in the United States. Mov. Disord. 28(3), 311–318 (2013).
6.
Ou Z, Pan J, Tang S et al. Global trends in the incidence, prevalence, and years lived with disability of Parkinson's Disease in 204 countries/territories from 1990 to 2019. Front. Public Health 9, 776847 (2021).
7.
Dorsey ER, Sherer T, Okun MS, Bloem BR. The emerging evidence of the Parkinson pandemic. J. Parkinsons Dis. 8, S3–S8 (2018).
8.
di Biase L, Pecoraro PM, Carbone SP, Caminiti ML, Di Lazzaro V. Levodopa-induced dyskinesias in Parkinson's disease: an overview on pathophysiology, clinical manifestations, therapy management strategies and future directions. J. Clin. Med. 12, (2023).
9.
Tan YY, Jenner P, Chen SD. Monoamine oxidase-B inhibitors for the treatment of Parkinson's disease: past, present, and future. J. Parkinsons Dis. 12, 477–493 (2022).
10.
EMA. Rasagiline ratiopharm: EPAR summary for the public. EMA/723435/2014. Available at: https://www.ema.europa.eu/en/documents/overview/rasagiline-ratiopharm-epar-summary-public_en.pdf
11.
EMA. Xadago: EPAR – Summary for the public. EMA/181382/2015. Available at: https://www.ema.europa.eu/en/documents/overview/xadago-epar-summary-public_en.pdf
12.
Kim Y, Kim Y, Lee HJ et al. The primary process and key concepts of economic evaluation in healthcare. J. Prev. Med. Public Health 55, 415–423 (2022).
13.
Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6, e1000097 (2009).
14.
Boada JN, Boada C, García-Sáiz M, García M, Fernández E, Gómez E. Net efficacy adjusted for risk (NEAR): a simple procedure for measuring risk:benefit balance. PLoS ONE 3, e3580 (2008).
15.
Mendes D, Alves C, Batel-Marques F. Number needed to treat (NNT) in clinical literature: an appraisal. BMC Med. 15, 112 (2017).
16.
Suurmond R, van Rhee H, Hak T. Introduction, comparison, and validation of Meta-Essentials: a free and simple tool for meta-analysis. Res. Synth. Methods 8, 537–553 (2017).
17.
Sociedad Española de Farmacia Hospitaliria (SEFH). Calculadoras y herramientas sobre subgrupos. Available at: https://gruposdetrabajo.sefh.es/genesis/index.php?option=com_content&view=article&id=45&Itemid=41
18.
Rabey JM, Sagi I, Huberman M et al. Rasagiline mesylate, a new MAO-B inhibitor for the treatment of Parkinson's disease: a double-blind study as adjunctive therapy to levodopa. Clin. Neuropharmacol. 23, 324–330 (2000).
19.
Parkinson Study Group. A randomized placebo-controlled trial of rasagiline in levodopa-treated patients with Parkinson disease and motor fluctuations: the PRESTO study. Arch. Neurol. 62, 241–248 (2005).
20.
Rascol O, Brooks DJ, Melamed E et al. LARGO study group. Rasagiline as an adjunct to levodopa in patients with Parkinson's disease and motor fluctuations (LARGO, Lasting effect in Adjunct therapy with Rasagiline Given Once daily, study): a randomised, double-blind, parallel-group trial. Lancet 365, 947–954 (2005).
21.
Zhang L, Zhang Z, Chen Y et al. Efficacy and safety of rasagiline as an adjunct to levodopa treatment in Chinese patients with Parkinson's disease: a randomized, double-blind, parallel-controlled, multi-centre trial. Int. J. Neuropsychopharmacol. 16, 1529–1537 (2013).
22.
Hanagasi HA, Gurvit H, Unsalan P et al. The effects of rasagiline on cognitive deficits in Parkinson's disease patients without dementia: a randomized, double-blind, placebo-controlled, multicenter study. Mov. Disord. 26, 1851–1858 (2011).
23.
Frakey LL, Friedman JH. Cognitive effects of rasagiline in mild-to-moderate stage Parkinson's disease without dementia. J. Neuropsychiatry Clin. Neurosci. 29, 22–25 (2017).
24.
Lim TT, Kluger BM, Rodriguez RL et al. Rasagiline for the symptomatic treatment of fatigue in Parkinson's disease. Mov. Disord. 30, 1825–1830 (2015).
25.
Hauser RA, Silver D, Choudhry A, Eyal E, Isaacson S. ANDANTE study investigators. Randomized, controlled trial of rasagiline as an add-on to dopamine agonists in Parkinson's disease. Mov. Disord. 29, 1028–1034 (2014).
26.
Borgohain R, Szasz J, Stanzione P et al. Randomized trial of safinamide add-on to levodopa in Parkinson's disease with motor fluctuations. Mov. Disord. 29, 229–237 (2014).
27.
Schapira AH, Fox SH, Hauser RA et al. Assessment of safety and efficacy of safinamide as a levodopa adjunct in patients with Parkinson disease and motor fluctuations: a randomized clinical trial. JAMA Neurol. 74, 216–224 (2017).
28.
Hattori N, Tsuboi Y, Yamamoto A, Sasagawa Y, Nomoto M. ME2125-3 Study Group. Efficacy and safety of safinamide as an add-on therapy to L-DOPA for patients with Parkinson's disease: a randomized, double-blind, placebo-controlled, Phase II/III study. Parkinsonism Relat. Disord. 75, 17–23 (2020).
29.
Barone P, Santangelo G, Morgante L et al. A randomized clinical trial to evaluate the effects of rasagiline on depressive symptoms in non-demented Parkinson's disease patients. Eur. J. Neurol. 22, 1184–1191 (2015).
30.
Wei Q, Tan Y, Xu P et al. The XINDI Study: A randomized Phase III clinical trial evaluating the efficacy and safety of safinamide as add-on therapy to levodopa in Chinese patients with Parkinson's disease with motor fluctuations. CNS Drugs 36, 1217–1227 (2022).
31.
Recio RS, Pablo Alonso Pérez De Ágreda J, José Rabanaque M, Aguilar Palacio I. Understanding the effect of economic recession on healthcare services: a systematic review. Iran J. Public Health 51, 495–507 (2022).
32.
Kulkova J, Kulkov I, Rohrbeck R et al. Medicine of the future: how and who is going to treat us? Futures 146, 103097 (2023).
33.
Chaudhuri KR, Azulay JP, Odin P et al. Economic burden of Parkinson's disease: a multinational, real-world, cost-of-illness study. Drugs Real World Outcomes 11, 1–11 (2024).
34.
Laupacis A, Sackett DL, Roberts RS. An assessment of clinically useful measures of the consequences of treatment. N. Engl. J. Med. 318, 1728–1733 (1988).
35.
Eslava AO, Gil RM, Fuentes MDF, López-Briz E, Latorre FP. Guía de evaluación económica e impacto presupuestario en los informes de evaluación de medicamentos. (2017).
36.
Andrade C. The numbers needed to treat and harm (NNT, NNH) statistics: what they tell us and what they do not. J. Clin. Psychiatry 76, e330–333 (2015).
37.
Straus SE. Individualizing treatment decisions – the likelihood of being helped or harmed. Eval. Health Prof. 25, 210–224 (2002).
38.
Marzo A, Dal Bo L, Monti NC et al. Pharmacokinetics and pharmacodynamics of safinamide, a neuroprotectant with antiparkinsonian and anticonvulsant activity. Pharmacol. Res. 50, 77–85 (2004).
39.
Alborghetti M, Nicoletti F. Different generations of type-B monoamine oxidase inhibitors in Parkinson's disease: from bench to bedside. Curr. Neuropharmacol. 17, 861–873 (2019).
40.
Bodrogi J, Kaló Z. Principles of pharmacoeconomics and their impact on strategic imperatives of pharmaceutical research and development. Br. J. Pharmacol. 159, 1367–1373 (2010).
41.
Bang H, Zhao H. Cost-effectiveness analysis: a proposal of new reporting standards in statistical analysis. J. Biopharm. Stat. 24, 443–460 (2014).
42.
Simoens S. How to assess the value of medicines? Front. Pharmacol. 1, 115 (2010).
43.
Mahdiani H, Münch N, Paul NW. A QALY is [still] a QALY is [still] a QALY? BMC Medical Ethics 25, 35 (2024).
44.
Vallejo-Torres L, García-Lorenzo B, Serrano-Aguilar P. Estimating a cost-effectiveness threshold for the Spanish NHS. Health Econ. 27, 746–761 (2018).
45.
Sacristán JA, Oliva J, Campillo-Artero C et al. ¿Qué es una intervención sanitaria eficiente en España en 2020? [What is an efficient health intervention in Spain in 2020?]. Gac. Sanit. 34(2), 189–193 (2020).
46.
O'Day K, Campbell D. The expanded number needed to treat: applying the concept of NNT to continuous health economic outcomes. Value Health 18, A35 (2015).
47.
Nguyen C, Naunton M, Thomas J et al. Availability and use of number needed to treat (NNT) based decision aids for pharmaceutical interventions. Explor. Res. Clin. Soc. Pharm. 2, 100039 (2021).
48.
Abeynayake I, Tanner CM. The economic impact of OFF periods in Parkinson disease. Am. J. Manag. Care 26, S265–S269 (2020).
49.
Winter Y, Balzer-Geldsetzer M, Spottke A et al. Longitudinal study of the socioeconomic burden of Parkinson's disease in Germany. Eur. J. Neurol. 17, 1156–1163 (2010).
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 March 2025
Accepted: 2 July 2025
Published online: 14 August 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Evaluation of the efficacy and cost-effectiveness of safinamide versus rasagiline: a systematic review. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0031
Export citation
Select the citation format you wish to export for this article or chapter.