Assessing healthcare resource utilization burden and unmet treatment needs in patients with Parkinson’s disease: results from a real-world study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Current Parkinson’s disease (PD) research evaluates patients with early and severe PD, but often overlooks patients with intermediate PD. This study aims to quantify unmet treatment needs, disease burden and healthcare resource utilization among patients with PD within different Hoehn and Yahr stage groups in the US. Materials & methods: Data were drawn from the Adelphi Parkinson’s Disease Specific Programme™, a cross-sectional survey of physicians and their patients in the US from September 2021 to April 2022. Patients were staged as early (Hoehn and Yahr stage 1–2), intermediate (stage 2.5–3) or severe (stage 4–5) PD. Analyses compared PD stages, focusing on the intermediate group. Results: Ninety-five physicians provided data for 1251 patients; 47.4%, 40.4%, and 12.2% were early-, intermediate-, and severe-stage PD, respectively. Mean age was 65.1, 71.8, and 77.8 years and mean time since diagnosis was 2.5, 5.1, and 7.7 years (p < 0.001) across early, intermediate, and severe groups, respectively. The mean number of products used in current regimen was 1.1 for early, 1.9 for intermediate and 2.4 for severe groups. The intermediate versus early group had a significantly greater proportion of patients with unmet treatment needs (p < 0.001), e.g., slowing disease progression, providing neuroprotection. Incidence rate ratios were increased for the intermediate versus early group for number (in previous 12 months) of healthcare professionals involved in patients’ PD management (incidence rate ratios 1.1), healthcare professional consultations (1.4), emergency room visits (3.8) and rehabilitation admissions (6.8). Patient-reported quality of life was significantly poorer in the intermediate versus early group. Conclusion: This real-world analysis found significant increases in disease burden and healthcare resource utilization for patients with intermediate versus early PD. More effective intervention of patients at intermediate-stage PD may improve symptom control and decrease the PD burden for patients and the healthcare system.
Plain language summary: A survey of patients with Parkinson’s disease to assess use of healthcare resources & current treatment needs
What is this article about?
This study looked at the burden of Parkinson’s disease (PD) on patients and the healthcare system in the US. Early, intermediate and severe stages of the disease were compared.
What were the results?
There were significant increases in disease burden and healthcare resource use for patients with intermediate PD compared with patients with early PD.
What do the results mean?
More effective intervention of patients at intermediate-stage PD may delay the transition to severe PD, improve symptom control and decrease the PD burden for patients and the healthcare system.
Parkinson’s disease (PD) is a progressive and complex neurodegenerative disorder characterized by motor symptoms associated with the loss of dopaminergic neurons in the substantia nigra [1,2]. However, pathologic neurodegeneration, with its protein aggregate hallmarks, also extends to cells in other regions of the neural network and to neurotransmitters [1,2]. With a prevalence of over 8.5 million people in 2019, PD is the second most common neurodegenerative disease globally [3]. In 2019, in North America, the age-standardized incidence and prevalence rates were 25.1 and 107.7 per 100,000 people, respectively [3].
The prevalence of PD is increasing in the US, with the 0.55 million cases in 2017 representing an 89.9% increase from 1990 [4], and with the age-standardized prevalence increasing to 97.0 per 100,000 in 2017, representing a 16.2% increase from 1990 [4]. Disease management has a substantial impact on patients and on the economy [5,6]. Moreover, the patient burden of PD is increasing, with a 24.8% increase in the rate of US age-standardized disability-adjusted life-years over the ∼30 years prior to 2017 [4]. In 2019, an estimated 5.8 million lost disability-adjusted life-years were attributable to PD [7]. Estimates suggested that the total economic disease burden was $51.9 billion in the US in 2017, with direct medical costs amounting to $25.4 billion, and indirect costs, such as lost wages, missed work and family/caregiver time, making up $26.5 billion [6].
The clinical features of PD are heterogeneous. However, typical motor symptoms include tremor, rigidity and bradykinesia, with postural instability developing with disease progression [1,2,8]. PD is also associated with nonmotor symptoms, including hyposmia, urinary dysfunction, constipation, orthostatic hypotension, memory loss, depression, pain and rapid eye movement sleep disorders, with these symptoms often appearing years before motor symptoms [2,9]. Current diagnostic criteria are based on the presence of two of the four motor symptoms, including tremor, rigidity, bradykinesia and postural instability [2]. Revised criteria that exclude postural instability, include both motor and nonmotor signs, and utilize exclusion criteria and red flags, have gained increasing attention and have been suggested to improve accuracy [9–11]. However, a definitive diagnosis is still made by histopathological assessment confirming substantia nigra neuronal loss [2,9]. Diagnosing PD remains a challenge as clinical disease characteristics overlap with other neurodegenerative conditions, and diagnostic tests or biomarkers do not enable a definitive diagnosis in the early stages [9]. This often results in detection of PD in the later disease stages when neurons have degenerated [12].
Current treatment of PD is well documented [13,14], although many unmet needs remain [15]. While levodopa remains the mainstay of PD treatment [16], there are no disease-modifying drugs currently available for PD, nor treatments that slow the neurodegenerative process [1,13]. To improve treatment outcomes, alternative levodopa and other dopamine agonist formulations have been developed, including extended-release oral drugs, intestinal gel infusion, subcutaneous and inhaled formulations, and combinations with other agents, such as catechol-O-methyltransferase (COMT) inhibitors and monoamine oxidase-B (MAO-B) inhibitors [14], at low doses. Additionally, clinical experience is being gained for use of other advanced treatments, such as N-methyl-D-aspartate (NMDA) antagonists [17,18]. Management strategies are also shifting toward earlier treatment combined with lower drug doses than those traditionally used [16]. Benefits of earlier treatment, before major neurological damage occurs and substantial motor symptoms appear, may include fewer symptoms and delayed levodopa initiation, as well as the possibility of slowed disease progression, improved quality of life (QoL) and lower medical costs [19].
Clinical trials have failed to conclusively demonstrate that early treatment slows PD progression [19]. A key factor has been the difficulty in distinguishing between a treatment’s ability to reduce symptoms versus reducing ‘real’ disease progression. This was the case with prasinezumab, where no significant difference was found in terms of disease progression between treatment and placebo groups over a 1-year period, although the drug was associated with some symptomatic improvements [20]. Evidence for early treatment is provided by a pilot clinical trial suggesting that subthalamic nucleus deep brain stimulation plus optimal drug therapy applied in early-stage PD could reduce the risk of developing or worsening dyskinesia [21]. Patients with PD experience significant worsening in outcomes when progressing from both early to intermediate and intermediate to severe stage of the disease, suggesting that more assertive and proactive treatment beyond early-stage PD would help to smooth out the steep declines currently seen when sparing treatment options until a last resort. However, the lack of conclusive evidence highlights the need for further research on targeted treatment approaches.
Recent estimates of the economic burden of PD on the US healthcare system underscore the need for treatments that reduce the impact and prevalence of PD [5,6]. There are many unmet needs in the treatment and management of PD, including an improved understanding of PD pathophysiology to create multiple-target strategies, earlier detection of PD using genetic, biochemical, and imaging biomarkers and improved diagnostic and PD assessment measures. There is also an emphasis on moving treatment focus from motor symptom relief to the development of neuroprotective therapies through improved understanding of the multi-neurotransmitter cell processes involved in PD pathology [22].
The Hoehn and Yahr (H&Y) staging scale is widely used for the classification of PD severity and level of disability [23,24]. The original five-stage scale has been modified to include two 0.5-point increments to allow for midline involvement with unilateral signs, and very mild postural impairment [23]. The impact of PD has been well documented for patients with early and severe disease. However, research is currently lacking on the particular impact of intermediate stage on patients and the healthcare system, and how this impact changes between H&Y stages as disease severity increases. The aim of this analysis was to quantify unmet treatment needs and disease burden in patients with PD, as well as the burden on the healthcare system, across different H&Y stage groups in the US. To our knowledge, this is the first study of intermediate-stage PD and disease burden, and its comparison of intermediate-stage patients with early- and severe-stage patients makes it unique.
Materials & methods
Survey design
Data were drawn from the Adelphi Real World Disease Specific Programme (DSP)™, a cross-sectional survey with elements of retrospective data collection of physicians and their consulting patients with PD conducted in the US from September 2021 to April 2022. The DSP, conducted in routine clinical practice, provides real-world data on patient demographics and clinical characteristics, disease management (including treatment history), the burden and impact of PD and any associated treatment effects from the perspective of both patient and physician. The DSP methodology has been utilized across various disease areas and has been previously described [25,26], validated [27], and demonstrated to be representative and consistent over time [28]. The DSP includes a physician survey to determine/screen for eligibility, physician-completed patient record forms, patient self-completion forms and caregiver self-completion forms.
Participant selection
Physicians (neurologists) were eligible to participate in the survey if they were personally responsible for the management and treatment of patients with PD and had a clinical workload of at least three patients with PD in a typical week.
Patients were eligible for inclusion if they were aged 18 years or older, had a physician-confirmed diagnosis of PD, and were not involved in a clinical trial at the time of data collection.
Data collection
Physicians were recruited by a local fieldwork agency and screened using the above predefined selection criteria. A geographically representative sample of physicians who were involved in the management and treatment of patients, and who met the inclusion criteria and agreed to participate, were recruited into the study.
Half of all participating physicians were instructed to complete patient record forms for their next 12 consecutively consulting patients meeting the patient eligibility criteria. The other half of physicians completed patient record forms for their next six consecutively consulting patients meeting the patient eligibility criteria, followed by seven patients who met further criteria: one patient who had been prescribed five or more doses of oral levodopa per day; one patient who had two or more hours of ‘OFF-time’ per day; one patient who had severe PD; two patients who had a modified H&Y stage of 2.5; and two patients who had a modified H&Y stage of 3.0. Physicians were allocated to a quota group at random, but neither they nor the patients were designated into study arms. The number of patients sampled was calculated to ensure sufficient analysis power for each group, based upon each patient’s representation within random sample data collection in prior waves of the Parkinson’s disease DSP in the US.
Physicians reported data on patient demographics, clinical characteristics, current treatment, unmet needs of current treatment and general patient management in terms of healthcare resource utilization (HCRU). Physicians completed the survey using both patient clinical records and their own judgment and diagnostic skills.
Each patient for whom the physician completed a patient record form was invited to fill out a patient self-completion form. The patient self-completion form included detailed questions on their current condition, including symptoms, level of satisfaction with their treatment and QoL tools. The QoL tools were the Parkinson’s Disease Questionnaire (PDQ-39) [29], EQ-5D-5L health utility index, EQ visual analogue scale (EQ VAS, US value sets) [30,31] and the Work Productivity and Activity Impairment (WPAI) questionnaire [32].
For each patient for whom the physician completed a patient record form and a caregiver was present, the caregiver was invited to complete a caregiver self-completion form based on their own perspective. The caregiver self-completion form included questions on demographics, relationship to patient, care provided, patient treatment and symptoms and QoL tools, including the Zarit Burden Interview [33], EQ-5D-5L and EQ VAS (US value sets) [30,31].
The patient self-completion form and the caregiver self-completion form were completed independently of their physician immediately after the consultation and returned in a sealed envelope.
Survey measures
Treatment satisfaction was reported on a 7-point scale, from 1 (very unsatisfied) to 7 (very satisfied); 4 = neither unsatisfied nor satisfied.
The PDQ-39 is a PD-specific health status and QoL questionnaire comprising 39 items [29]. For each question item, patients were requested to select one of five responses (never, occasionally, sometimes, often, always) according to how often they have experienced the problem during the last month due to their PD. Items were grouped into eight scales, and item scores were summed and expressed as a percentage score ranging from 0 to 100, with a higher score indicating more health problems.
The EQ-5D-5L measures participants’ general health status on five dimensions. Empirically derived weights were applied to an individual’s responses to the EQ-5D-5L descriptive system to generate an EQ-5D health utility index. The US weighting algorithm was applied to all patients for all analyses. An EQ-5D-5L health utility index score of 1 is perfect health, with lower scores indicating worse health.
The EQ VAS records the patient’s self-rated health on a 100-mm vertical VAS, ranging from 0 (worst imaginable health) to 100 (best imaginable health) [31].
The patient-reported WPAI measures included time missed from work (absenteeism), impairment ineffectiveness at work (presenteeism), overall work productivity loss (overall work impairment) and nonwork related activity impairment (total activity impairment) due to their PD [32]. Higher values indicated more PD-related impairment, with WPAI component scores reported as percentage impairment.
The caregiver-completed Zarit Burden Interview 22-item questionnaire [33] comprises statements centered around emotional well-being, social and family life, finances and impact on relationship with the patient. The caregiver was asked to indicate how often they feel burdened by caring for the patient using a 5-point scale (never, rarely, sometimes, frequently, nearly always).
Patient satisfaction was rated on a 7-point scale, where 1 = very unsatisfied, 2 = unsatisfied, 3 = fairly unsatisfied, 4 = neither unsatisfied nor satisfied, 5 = fairly satisfied, 6 = satisfied and 7 = very satisfied.
Ethics & consent
This study was granted ethical exemption by the Pearl Institutional Review Board, approval number AG9140.
Using a checkbox, patients provided informed consent to take part in the survey. Data were collected in such a way that patients and physicians could not be identified directly. Data were aggregated before being shared with the subscriber and/or for publication. Data collection was undertaken in line with European Pharmaceutical Marketing Research Association guidelines [34] and as such did not require ethics committee approval. Each survey was performed in full accordance with relevant legislation at the time of data collection, including the US Health Insurance Portability and Accountability Act 1996 [35] and Health Information Technology for Economic and Clinical Health Act legislation [36]. Fieldwork partners adhered to national data collection regulations in the US.
Data analysis
Physicians staged each patient using the modified H&Y scale [23]. For this analysis, patients were categorized as ‘early stage’ (H&Y stage 1.0–2.0), ‘intermediate stage’ (H&Y stage 2.5–3.0) or ‘severe stage’ (H&Y stage 4.0–5.0; Supplementary Table 1). ‘OFF time’ refers to periods when the motor/nonmotor symptoms of PD reappear or worsen as the effects of symptomatic treatment ‘wear off’.
Regarding the lines of therapy, line 1 was the initial treatment regimen for PD and line 2 was the following treatment regimen, that being one that has at least one change in treatment composition, not just a dose titration.
Means and standard deviations (SD) were calculated for continuous variables, and frequency and percentages were calculated for categorical variables. Missing data were not imputed, and therefore the number of patients for analysis could vary from variable to variable. Where, due to missing data, patient numbers differ from the total population for the group, the number of patients is reported.
Bivariate and pairwise analyses compared outcomes between patients at the three H&Y stages. For the bivariate analyses, ANOVA was used for continuous outcome variables, Kruskal–Wallis for ordered categorical variables and Chi-squared otherwise. For the pairwise analyses, t-test was used for continuous variables, Mann–Whitney U test for ordinal variables, Fisher’s exact test for dichotomous variables and Chi-square test otherwise. For all tests in the pairwise analysis, p-values were Bonferroni corrected. Logistic regression and negative binomial regression analyses were conducted with H&Y stage being used as the main predictor variable. Regression analyses were adjusted for patient age, sex and body mass index. Odds ratios (OR) and incidence rate ratios (IRR), with 95% confidence intervals (CI) and p-values, were presented. A p-value of 0.05 or less was statistically significant for all analyses.
This analysis compared the H&Y groups in outcomes, including prescribed treatment and HCRU (i.e., numbers of consultations and hospitalizations in the last 12 months). All analyses were generated using the statistical software package STATA® Version 17 or later (StataCorp 2021, USA StataCorp LLC, TX, USA).
Results
Patient demographics & clinical characteristics
Patient demographics and clinical characteristics are shown in Table 1 & Supplementary Table 2. A total of 95 physicians provided data on 1251 patients with PD, of which 47.4% were classed as early stage (n = 593), 40.4% as intermediate stage (n = 505) and 12.2% as severe stage (n = 153). Overall, 243 patients completed patient self-completion forms, and 57 caregivers completed caregiver self-completion forms. The overall mean age (SD) was 69.4 (10.3) years, with a significant difference in age between disease stages (overall p < 0.001), and 60.9% were male. Three-quarters (75.5%) of all patients were White/Caucasian. There was a significant difference in employment status between disease severity stages (overall p < 0.001; Table 1).
| Variable | Overall (n = 1251) | H&Y stage† | p-value (test) | ||
|---|---|---|---|---|---|
| Early (n = 593) | Intermediate (n = 505) | Severe (n = 153) | |||
| Demographics | |||||
| Age, years | <0.001 (ANOVA) | ||||
| Mean (SD) | 69.4 (10.3) | 65.1 (10.6) | 71.8 (8.1) | 77.8 (7.1) | |
| Age, years, n (%) | <0.001 (CH) | ||||
| ≤90 | 1231 (98.4) | 589 (99.3) | 499 (98.8) | 143 (93.5) | |
| >90 | 20 (1.6) | 4 (0.7) | 6 (1.2) | 10 (6.5) | |
| Sex, n (%) | 0.057 (CH) | ||||
| Male | 762 (60.9) | 367 (61.9) | 291 (57.6) | 104 (68.0) | |
| BMI, mean (SD) | 26.4 (4.6) | 25.4 (3.7) | 27.2 (5.0) | 27.4 (5.7) | <0.001 (ANOVA) |
| Ethnicity, n (%) | 0.060 (CH) | ||||
| White/Caucasian | 944 (75.5) | 427 (72.0) | 401 (79.4) | 116 (75.8) | |
| African–American | 120 (9.6) | 68 (11.5) | 37 (7.3) | 15 (9.8) | |
| Native American | 1 (0.1) | 1 (0.2) | 0 (0.0) | 0 (0.0) | |
| Asian (Indian subcontinent) | 21 (1.7) | 13 (2.2) | 6 (1.2) | 2 (1.3) | |
| Asian (other) | 21 (1.7) | 16 (2.7) | 4 (0.8) | 1 (0.7) | |
| Hispanic/Latino | 71 (5.7) | 26 (4.4) | 33 (6.5) | 12 (7.8) | |
| Middle Eastern | 17 (1.4) | 10 (1.7) | 4 (0.8) | 3 (2.0) | |
| Mixed race | 30 (2.4) | 16 (2.7) | 12 (2.4) | 2 (1.3) | |
| South-East Asian | 26 (2.1) | 16 (2.7) | 8 (1.6) | 2 (1.3) | |
| Employment status, n (%) | <0.001 (CH) | ||||
| Working full-time | 204 (16.3) | 183 (30.9) | 21 (4.2) | 0 (0.0) | |
| Working part-time | 106 (8.5) | 68 (11.5) | 37 (7.3) | 1 (0.7) | |
| Student | 1 (0.1) | 1 (0.2) | 0 (0.0) | 0 (0.0) | |
| Unemployed | 55 (4.4) | 26 (4.4) | 25 (5.0) | 4 (2.6) | |
| Retired | 802 (64.1) | 265 (44.7) | 394 (78.0) | 143 (93.5) | |
| Homemaker | 73 (5.8) | 45 (7.6) | 24 (4.8) | 4 (2.6) | |
| Clinical characteristics | |||||
| Time since diagnosis, years | |||||
| n | 984 | 475 | 399 | 110 | |
| Mean (SD) | 4.1 (4.2) | 2.5 (2.7) | 5.1 (4.3) | 7.7 (5.8) | <0.001 (ANOVA) |
| Current symptoms | |||||
| n | 1238 | 584 | 501 | 153 | |
| Motor symptoms, n (%) | 1231 (99.4) | 578 (99.0) | 500 (99.8) | 153 (100.0) | 0.118 (CH) |
| Nonmotor symptoms, n (%) | 758 (61.2) | 289 (49.5) | 340 (67.9) | 129 (84.3) | <0.001 (CH) |
| Current symptoms (10 most reported), n (%) | |||||
| Tremor at rest | 877 (70.1) | 414 (69.8) | 365 (72.3) | 98 (64.1) | 0.147 (CH) |
| Bradykinesia | 651 (52.0) | 262 (44.2) | 294 (58.2) | 95 (62.1) | <0.001 (CH) |
| Shuffling walk | 646 (51.6) | 199 (33.6) | 334 (66.1) | 113 (73.9) | <0.001 (CH) |
| Rigidity | 597 (47.7) | 203 (34.2) | 297 (58.8) | 97 (63.4) | <0.001 (CH) |
| Falling/imbalance | 488 (39.0) | 115 (19.4) | 264 (52.3) | 109 (71.2) | <0.001 (CH) |
| Lack of arm swing | 443 (35.4) | 161 (27.2) | 216 (42.8) | 66 (43.1) | <0.001 (CH) |
| Lack of facial expression | 317 (25.3) | 72 (12.1) | 177 (35.1) | 68 (44.4) | <0.001 (CH) |
| Micrographia | 298 (23.8) | 90 (15.2) | 153 (30.3) | 55 (36.0) | <0.001 (CH) |
| Freezing of gait | 282 (22.5) | 42 (7.1) | 161 (31.9) | 79 (51.6) | <0.001 (CH) |
| Physical fatigue/low energy | 234 (18.7) | 87 (14.7) | 98 (19.4) | 49 (32.0) | <0.001 (CH) |
| Caregiver status | |||||
| Caregiver responsible for patients’ daily needs, n (%) | <0.001 (CH) | ||||
| Patients, n | 1158 | 543 | 467 | 148 | |
| No caregiver | 742 (64.1) | 465 (85.6) | 262 (56.1) | 15 (10.1) | |
| Caregiver | 416 (35.9) | 78 (14.4) | 205 (43.9) | 133 (89.9) | |
| Total caregiver hours per week, mean (SD) | <0.001 (ANOVA) | ||||
| Patients, n | 1153 | 541 | 464 | 148 | |
| Caregiver hours | 17.8 (40.4) | 4.3 (19.0) | 20.9 (43.5) | 57.3 (57.0) | |
†
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
Patient numbers shown only where some patients are missing.
Proportions may not equal 100% due to rounding.
ANOVA: Analysis of variance; CH: Chi-square test; H&Y: Hoehn and Yahr; SD: Standard deviation.
There was a significant difference in time from symptom onset to PD diagnosis between severity groups, from a mean (SD) of 2.5 (2.7) years for the early group to 5.1 (4.3) years and 7.7 (5.8) years for the intermediate and severe groups, respectively (p < 0.001 across groups).
Regardless of PD severity, 99.4% of patients experienced at least one motor symptom. Overall, 61.2% of patients experienced nonmotor symptoms, and there was a significant difference between disease stages of PD (p < 0.001; Table 1). The most common motor symptoms were tremor at rest (70.1%), bradykinesia (52.0%), shuffling walk (51.6%) and rigidity (47.7%). The most common nonmotor symptoms were falling/imbalance (39.0%) and physical fatigue/low energy (18.7%). Each of the top ten most reported symptoms differed significantly across disease stages (p < 0.001; Table 1), excluding tremor at rest where there was no significant difference.
For each of the top ten common symptoms, there was a significant difference in patients’ symptom severity (i.e., mild, moderate or severe) between disease stages (i.e., early, intermediate or severe; p < 0.001; Supplementary Table 2). Significance was observed from the early group to the intermediate group and to the severe group, as well as from the intermediate group to the severe group. The four most common symptoms, tremor at rest, bradykinesia, shuffling walk and rigidity, were present in 72.3, 58.2, 66.1 and 58.8% of patients, respectively, in the intermediate group. These symptoms were mild or moderate in severity for 92.0, 95.6, 94.0 and 98.6% of patients, respectively. There was a significant difference in the control of symptoms (Supplementary Table 2) across disease stages (p < 0.001) in all but physical fatigue/low energy. Less than 20% of the intermediate group achieved full control of tremor at rest, bradykinesia, shuffling walk and rigidity (Supplementary Table 2).
There was a significant difference in the percentage of patients experiencing nonmotor symptoms across disease stages. Nonmotor symptoms were reported in 49.5, 67.9 and 84.3% of patients in the early, intermediate and severe groups, respectively (Table 1).
Caregivers were responsible for the daily needs of 14.4% of early stage, 43.9% of intermediate stage and 89.9% of severe-stage patients. Each patient needed 4.3, 20.9 and 57.3 h of care per week, respectively (Table 1).
Physician-reported treatment
Treatment patterns
The mean (SD) number of lines of treatment was 1.2 (0.4), 1.8 (0.9) and 2.1 (1.0) for the early-, intermediate- and severe-stage patients, respectively (p < 0.001; Table 2). The mean (SD) number of drugs used as part of the current regimen was 1.1 (0.8), 1.9 (1.2) and 2.4 (1.4) for the early-, intermediate- and severe-stage patients, respectively (p < 0.001).
| Variable | Overall (n = 1251) | H&Y stage† | p-value (test) | ||
|---|---|---|---|---|---|
| Early (n = 593) | Intermediate (n = 505) | Severe (n = 153) | |||
| Lines of treatment | |||||
| n | 933 | 442 | 382 | 109 | |
| Mean (SD) | 1.5 (0.8) | 1.2 (0.4) | 1.8 (0.9) | 2.1 (1.0) | <0.001 (ANOVA) |
| Current regimen | |||||
| Drugs taken as part of current treatment regimen, n | |||||
| Mean (SD) | 1.6 (1.2) | 1.1 (0.8) | 1.9 (1.2) | 2.4 (1.4) | <0.001 (ANOVA) |
| Current treatment class, n (%) | |||||
| Levodopa | 828 (66.2) | 277 (46.7)‡,§ | 421 (83.4) | 130 (85.0) | <0.001 (CH) |
| Dopamine agonist, 1st generation | 419 (33.5) | 190 (32.0) | 172 (34.1) | 57 (37.3) | 0.448 (CH) |
| MAO-B inhibitor | 221 (17.7) | 99 (16.7) | 92 (18.2) | 30 (19.6) | 0.642 (CH) |
| NMDA antagonist | 192 (15.4) | 50 (8.4)‡,§ | 91 (18.0)¶ | 51 (33.3) | <0.001 (CH) |
| COMT inhibitor | 79 (6.3) | 7 (1.2)‡,§ | 49 (9.7) | 23 (15.0) | <0.001 (CH) |
| Dopamine agonist, 2nd generation | 5 (0.4) | 1 (0.2) | 4 (0.8) | 0 (0.0) | 0.186 (CH) |
| Other | 98 (7.8) | 16 (2.7)‡,§ | 56 (11.1) | 26 (17.0) | <0.001 (CH) |
| Current advanced treatment, n (%) | |||||
| Apomorphine injection (APO-go® PEN) | 14 (1.1) | 1 (0.2) | 2 (0.4) | 11 (7.2) | <0.001 (CH) |
| Apomorphine sublingual film (KYNMOBI®) | 23 (1.8) | 4 (0.7) | 11 (2.2) | 8 (5.2) | <0.001 (CH) |
| Deep brain stimulation | 17 (1.4) | 3 (0.5) | 9 (1.8) | 5 (3.3) | 0.018 (CH) |
| Duopa (levodopa and carbidopa intestinal infusion gel) and pump | 7 (0.6) | 0 (0.0) | 3 (0.6) | 4 (2.6) | <0.001 (CH) |
| Apomorphine injection (APO-go® pump) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Lecigon (carbidopa and entacapone intestinal infusion gel) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Other | 3 (0.2) | 0 (0.0) | 3 (0.6) | 0 (0.0) | 0.108 (CH) |
†
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
Pairwise comparison:
‡
p < 0.050 Early stage vs intermediate stage.
§
p < 0.050 Early stage vs severe stage.
¶
p < 0.050 Intermediate stage vs severe stage.
Patient numbers shown only where some patients are missing.
Patients may be using >1 treatment.
ANOVA: Analysis of variance; CH: Chi-square test; COMT: Catechol-O-methyl transferase; H&Y: Hoehn and Yahr; MAO-B: Monoamine oxidase B; NMDA: N-methyl-D-aspartate; SD: Standard deviation.
Levodopa was the most used current treatment class, reported for 66.2% of all patients (early, 46.7%; intermediate, 83.4%; severe, 85.0%), with significant differences between the early group and both the intermediate and the severe groups (Table 2 & Figure 1). The likelihood of a levodopa prescription significantly increased from early- to intermediate-stage PD (OR: 5.6; p < 0.001), and from early- to severe-stage PD (OR: 4.6; p < 0.001; Table 3 & Figure 1). A treatment for severe PD was currently prescribed for 1.3% of the early group, 5.5% of the intermediate group and 18.3% of the severe group (Table 2).
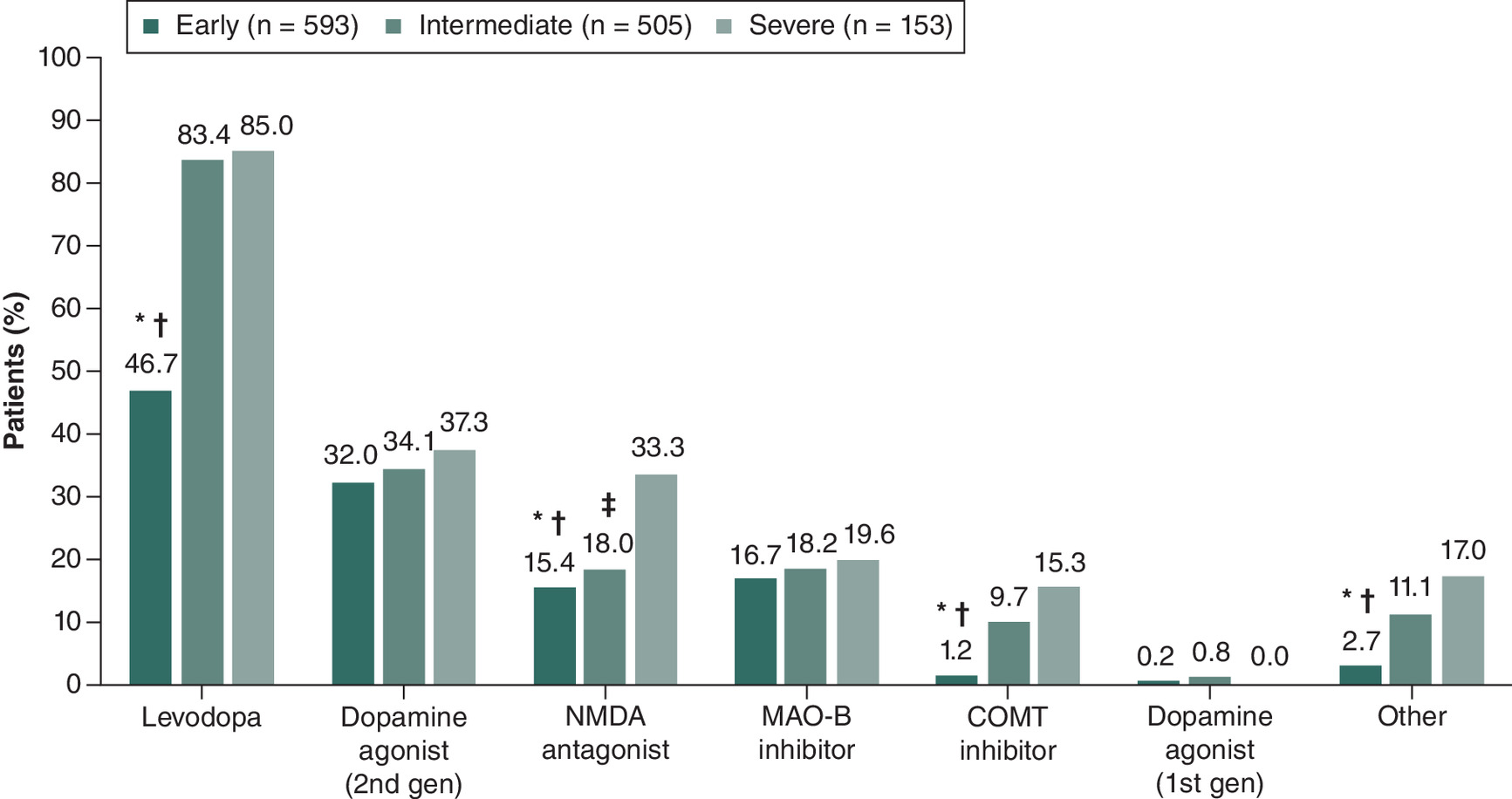
Figure 1. Physician-reported current treatment class of patients with Parkinson’s disease according to Hoehn and Yahr stage.
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
Pairwise comparison:
*p < 0.050 Early stage versus intermediate stage.
†p < 0.050 Early stage versus severe stage.
‡p < 0.050 Intermediate stage versus severe stage.
COMT: Catechol-O-methyl transferase; Gen: Generation; H&Y: Hoehn and Yahr; MAO-B: Monoamine oxidase-B; NMDA: N-methyl-D-aspartate.
| Variable | H&Y stage† | ||
|---|---|---|---|
| Early (n = 593) | Intermediate (n = 505) | Severe (n = 153) | |
| Odds ratio (95% CI) | |||
| Levodopa | 1 | 5.6 (3.7, 8.5)§ | 4.6 (2.5, 8.5)§ |
| Dopamine agonist, 2nd generation | 1 | 1.3 (0.9, 1.9) | 1.7 (1.0, 2.8)‡ |
| MAO-B inhibitor | 1 | 1.2 (0.8, 1.8) | 1.3 (0.7, 2.4) |
| NMDA antagonist | 1 | 2.5 (1.5, 4.1)§ | 6.0 (3.1, 11.7)§ |
| COMT inhibitor | 1 | 9.2 (4.0, 21.6)§ | 13.9 (4.0, 47.9)§ |
| Other | 1 | 4.2 (2.4, 7.6)§ | 6.1 (3.0, 12.4)§ |
†
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
‡
‘Early’ H&Y stage is the reference value; p < 0.050 for early stage vs severe stage.
§
‘Early’ H&Y stage is the reference value; p < 0.050 for early stage vs intermediate stage and early stage vs severe stage.
CI: Confidence interval; COMT: Catechol-O-methyl transferase; H&Y: Hoehn and Yahr; MAO-B: Monoamine oxidase B; NMDA: N-methyl-D-aspartate.
The likelihood of a prescription for an NMDA antagonist (OR: 2.5; p < 0.001) or a COMT inhibitor (OR: 9.2; p < 0.001) also significantly increased from early- to intermediate-stage PD (Table 3 & Figure 1). Similarly, the likelihood of a prescription for an NMDA antagonist (OR: 6.0; p < 0.001) or a COMT inhibitor (OR: 13.9; p < 0.001) also significantly increased from early- to severe-stage PD (Table 3 & Figure 1). However, for second-generation dopamine agonists, the likelihood of a prescription significantly increased from early- to severe-stage PD (OR: 1.7; p = 0.045), but not from early- to intermediate-stage PD (OR: 1.3; p = 0.248; Table 3 & Figure 1).
Treatment with levodopa predominated across all previous lines of therapy, with significant differences across the severity groups for levodopa at lines 1 (p < 0.001) and 2 (p = 0.040; Table 4). There were also significant differences across the severity groups for COMT inhibitors at line 1 (p = 0.019) and NMDA antagonists at line 2 (p < 0.001). For the intermediate and severe groups, respectively, use of levodopa was 70.3% and 69.4% at line 1, and 87.9% and 86.1% at line 2. At line 1, 1.3% of patients in the intermediate group received a COMT inhibitor compared with 3.7% of patients in the severe group. At line 2, 19.4% of patients in the intermediate group received an NMDA antagonist compared with 39.2% of patients in the severe group.
| Variable | Overall (n = 1251) | H&Y stage† | p-value (test) | ||
|---|---|---|---|---|---|
| Early (n = 593) | Intermediate (n = 505) | Severe (n = 153) | |||
| Previous treatment class line 1, n (%) | |||||
| n | 931 | 442 | 381 | 108 | |
| Dopamine agonist, 2nd generation | 343 (36.8) | 168 (38.0) | 134 (35.2) | 41 (38.0) | 0.679 (CH) |
| Dopamine agonist, 1st generation | 4 (0.4) | 1 (0.2) | 3 (0.8) | 0 (0.0) | 0.362 (CH) |
| Levodopa | 555 (59.6) | 212 (48.0) | 268 (70.3) | 75 (69.4) | <0.001 (CH) |
| MAO-B inhibitor | 167 (17.9) | 80 (18.1) | 72 (18.9) | 15 (13.9) | 0.485 (CH) |
| COMT inhibitor | 11 (1.2) | 2 (0.5) | 5 (1.3) | 4 (3.7) | 0.019 (CH) |
| NMDA antagonist | 115 (12.4) | 46 (10.4) | 52 (13.6) | 17 (15.7) | 0.194 (CH) |
| Other | 25 (2.7) | 9 (2.0) | 13 (3.4) | 3 (2.8) | 0.476 (CH) |
| Previous treatment class line 2, n (%) | |||||
| n | 364 | 79 | 206 | 79 | |
| Dopamine agonist, 2nd generation | 168 (46.2) | 30 (38.0) | 99 (48.1) | 39 (49.4) | 0.252 (CH) |
| Dopamine agonist, 1st generation | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Levodopa | 309 (84.9) | 60 (75.9) | 181 (87.9) | 68 (86.1) | 0.040 (CH) |
| MAO-B inhibitor | 90 (24.7) | 24 (30.4) | 48 (23.3) | 18 (22.8) | 0.419 (CH) |
| COMT inhibitor | 39 (10.7) | 5 (6.3) | 21 (10.2) | 13 (16.5) | 0.113 (CH) |
| NMDA antagonist | 78 (21.4) | 7 (8.9) | 40 (19.4) | 31 (39.2) | <0.001 (CH) |
| Other | 41 (11.3) | 6 (7.6) | 23 (11.2) | 12 (15.2) | 0.319 (CH) |
| Previous treatment class line 3, n (%) | |||||
| n | 96 | 3 | 70 | 23 | |
| Dopamine agonist, 2nd generation | 54 (56.3) | 2 (66.7) | 37 (52.9) | 15 (65.2) | 0.546 (CH) |
| Dopamine agonist, 1st generation | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Levodopa | 94 (97.9) | 3 (100.0) | 68 (97.1) | 23 (100.0) | 0.684 (CH) |
| MAO-B inhibitor | 32 (33.3) | 2 (66.7) | 25 (35.7) | 5 (21.7) | 0.215 (CH) |
| COMT inhibitor | 22 (22.9) | 0 (0.0) | 17 (24.3) | 5 (21.7) | 0.611 (CH) |
| NMDA antagonist | 27 (28.1) | 0 (0.0) | 19 (27.1) | 8 (34.8) | 0.425 (CH) |
| Other | 17 (17.7) | 0 (0.0) | 12 (17.1) | 5 (21.7) | 0.632 (CH) |
| Previous treatment class line 4, n (%) | |||||
| n | 32 | 1 | 20 | 11 | |
| Dopamine agonist, 2nd generation | 18 (56.3) | 1 (100.0) | 11 (55.0) | 6 (54.5) | 0.669 (CH) |
| Dopamine agonist, 1st generation | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 (CH) |
| Levodopa | 31 (96.9) | 1 (100.0) | 20 (100.0) | 10 (90.9) | 0.373 (CH) |
| MAO-B inhibitor | 11 (34.4) | 0 (0.0) | 9 (45.0) | 2 (18.2) | 0.246 (CH) |
| COMT inhibitor | 9 (28.1) | 0 (0.0) | 8 (40.0) | 1 (9.1) | 0.153 (CH) |
| NMDA antagonist | 14 (43.8) | 0 (0.0) | 10 (50.0) | 4 (36.4) | 0.512 (CH) |
| Other | 11 (34.4) | 0 (0.0) | 6 (30.0) | 5 (45.5) | 0.524 (CH) |
| Previous treatment class line 5, n (%) | |||||
| n | 11 | 0 | 6 | 5 | |
| Dopamine agonist, 2nd generation | 8 (72.7) | 0 (0.0) | 4 (66.7) | 4 (80.0) | 1.000 (FE) |
| Dopamine agonist, 1st generation | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Levodopa | 11 (100.0) | 0 (0.0) | 6 (100.0) | 5 (100.0) | 1.000 |
| MAO-B inhibitor | 3 (27.3) | 0 (0.0) | 2 (33.3) | 1 (20.0) | 1.000 (FE) |
| COMT inhibitor | 3 (27.3) | 0 (0.0) | 3 (50.0) | 0 (0.0) | 0.182 (FE) |
| NMDA antagonist | 6 (54.5) | 0 (0.0) | 3 (50.0) | 3 (60.0) | 1.000 (FE) |
| Other | 5 (45.5) | 0 (0.0) | 2 (33.3) | 3 (60.0) | 0.567 (FE) |
| Previous treatment class line 6, n (%) | |||||
| n | 2 | 0 | 1 | 1 | |
| Dopamine agonist, 2nd generation | 1 (50.0) | 0 (0.0) | 1 (100.0) | 0 (0.0) | 1.000 (FE) |
| Dopamine agonist, 1st generation | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Levodopa | 2 (100.0) | 0 (0.0) | 1 (100.0) | 1 (100.0) | 1.000 |
| MAO-B inhibitor | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| COMT inhibitor | 1 (50.0) | 0 (0.0) | 1 (100.0) | 0 (0.0) | 1.000 (FE) |
| NMDA antagonist | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Other | 1 (50.0) | 0 (0.0) | 0 (0.0) | 1 (100.0) | 1.000 (FE) |
†
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
Patients may be using >1 treatment.
CH: Chi-square test; COMT: Catechol-O-methyl transferase; FE: Fisher exact test; H&Y: Hoehn and Yahr; MAO-B: Monoamine oxidase B; NMDA: N-methyl-D-aspartate.
Unmet treatment needs
Pairwise comparisons showed that physicians reported greater treatment related unmet needs for intermediate-stage patients than early-stage patients’ needs in relation to: slowing disease progression, disease modification, providing neuroprotection, maintaining QoL, long-term efficacy, reducing rigidity, cost effectiveness, reducing bradykinesia, availability of different formulations, enabling levodopa dose limitation/reduction, preventing dystonia, lack of interactions with other drugs, treating bladder/bowel problems, good clinical trial evidence and suitability for add-on therapy (all p <0.001; Figure 2). The need to reduce tremor was also reported for a greater proportion of the intermediate versus early groups (p = 0.002). ‘Slowing disease progression’, ‘disease modification’ and ‘providing neuroprotection’ were the most frequently reported needs. Among the three PD groups, the reporting of these unmet needs was often highest for intermediate-stage patients (p < 0.001 for the early group vs intermediate group).
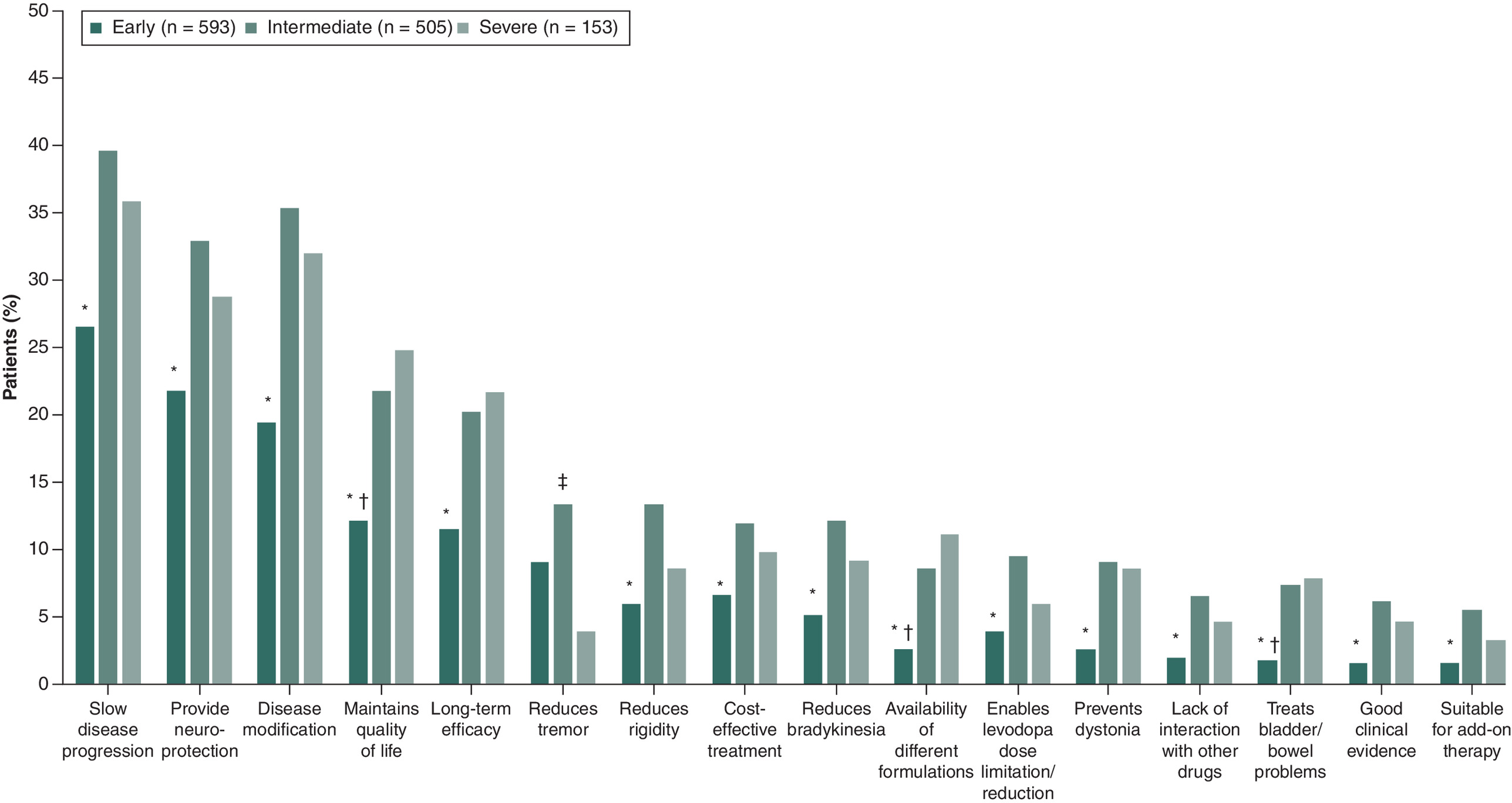
Figure 2. Physician-reported unmet treatment needs of patients with Parkinson’s disease according to Hoehn and Yahr stage.
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
Pairwise comparison:
*p < 0.050 Early stage versus intermediate stage.
†p < 0.050 Early stage versus severe stage.
‡p < 0.050 Intermediate stage versus severe stage.
H&Y: Hoehn and Yahr.
Pairwise comparisons showed that physicians reported greater treatment related unmet needs for severe-stage patients than early-stage patients’ needs in relation to: disease modification (p < 0.05), maintaining QoL (p < 0.001), long-term efficacy (p < 0.05), preventing dystonia (p < 0.05), treating bladder/bowel problems (p = 0.001) and availability of different formulations (p < 0.001; Figure 2), as well as increasing amount of ‘ON time’ (p = 0.002), increasing ‘ON time’ without dyskinesia (p < 0.001), treating symptoms of psychosis (p < 0.05) and suitability in cognitively impaired patients (p < 0.05).
‘Reducing tremor’ was reported as an unmet need for 10.2% of patients overall; and for 9.1, 13.3 and 3.9% of the early, intermediate and severe groups, respectively. The difference between the intermediate group and severe group was significant (p = 0.0018) (Figure 2).
Patient-reported treatment satisfaction
There was a significant difference in patients’ treatment satisfaction across disease stages. The mean (SD) satisfaction score was 5.6 (1.2) for early (n = 119), 5.1 (1.1) for intermediate (n = 89) and 4.4 (1.3) for severe groups (n = 22; (p < 0.001; Figure 3). 75.3% patients in the intermediate group rated their satisfaction as 5 (‘fairly satisfied’, 32.6%) or 6 (‘satisfied’, 42.7%) out of a total of 7 points.
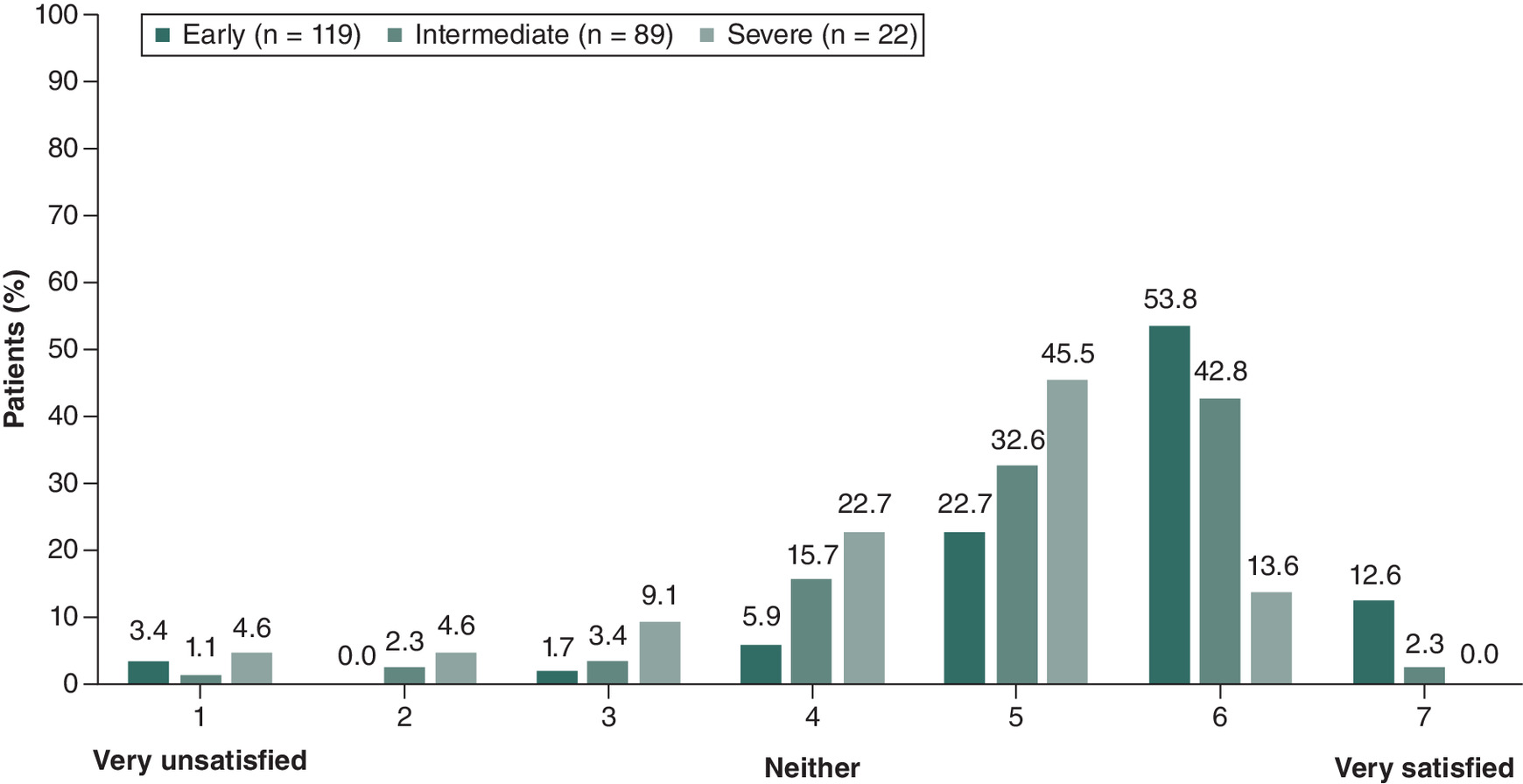
Figure 3. Patient-reported treatment satisfaction of patients with Parkinson’s disease according to Hoehn and Yahr stage.
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
p < 0.050 for the distribution across groups.
H&Y: Hoehn and Yahr.
Patient-reported QoL
There was a significant difference in patient-reported QoL across disease stages, as reported by EQ-5D-5L and EQ VAS (Figure 4A & B). For the early, intermediate and severe groups, mean (SD) EQ-5D-5L scores were 0.8 (0.2), 0.6 (0.3) and 0.2 (0.4), respectively (p < 0.001). Mean (SD) EQ VAS scores were 79.3 (12.1), 68.6 (16.8) and 42.9 (19.9; p < 0.001). Pairwise comparisons for the EQ-5D-5L and EQ VAS scores showed that the intermediate group reported a significantly worse QoL compared with the early group (p < 0.001), although QoL for the intermediate group was significantly better than for the severe group (p < 0.001). The EQ-5D-5L and EQ VAS scores showed that the severe group also reported a significantly worse QoL compared with the early group (p < 0.001).
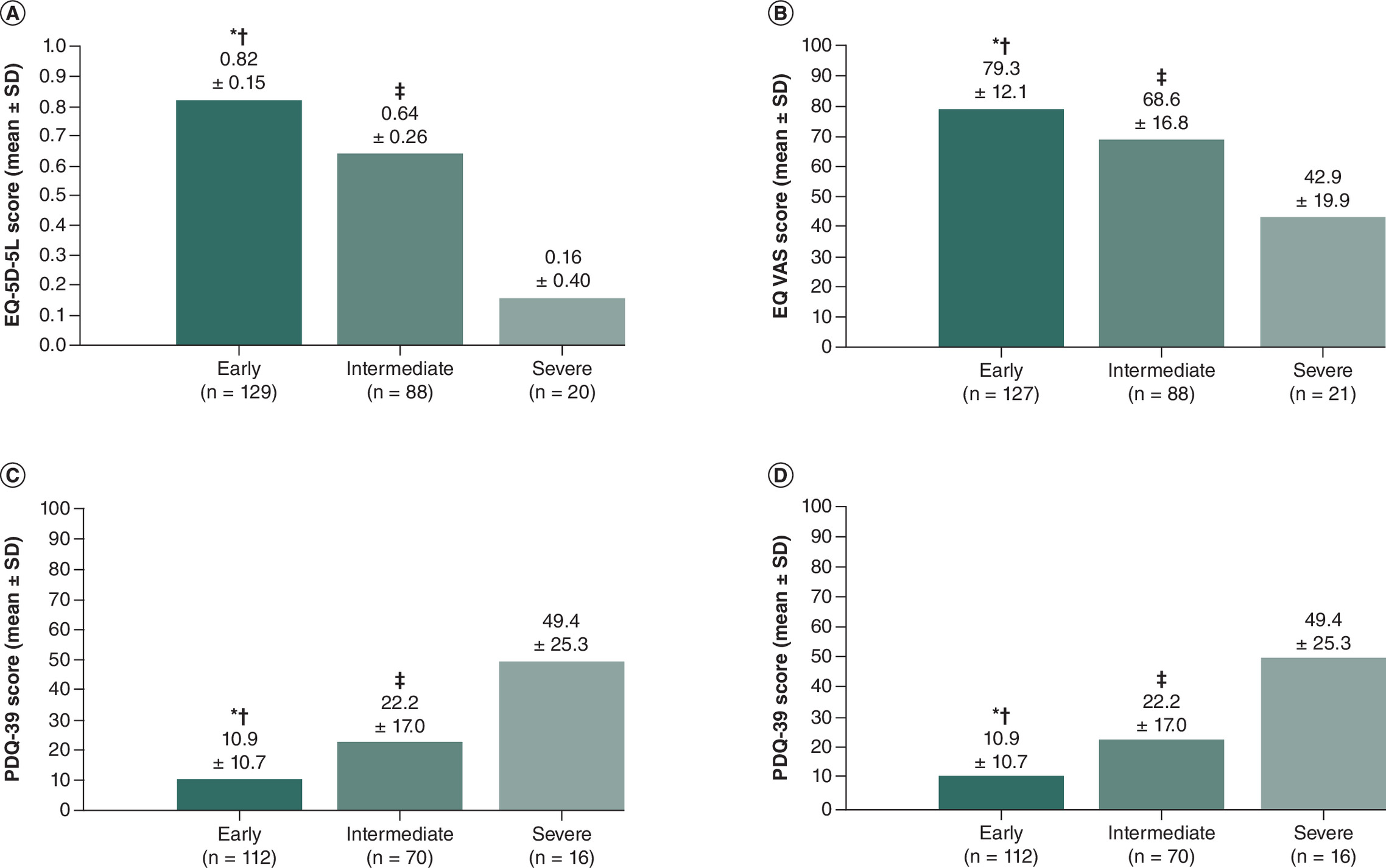
Figure 4. Patient-reported quality of life of patients with Parkinson’s disease according to Hoehn and Yahr stage:
(A) EQ-5D5L (US) scores, (B) EQ VAS scores, (C) PDQ-39 scores and (D) WPAI percent activity impairment due to problem.
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
For all four measures shown, p < 0.001 across groups.
Pairwise comparison:
*p < 0.050 Early stage versus intermediate stage.
†p < 0.050 Early stage versus severe stage.
‡p < 0.050 Intermediate stage versus severe stage.
EQ VAS: EQ visual analogue scale; H&Y: Hoehn and Yahr; PDQ-39: Parkinson’s Disease Questionnaire-39 questions; WPAI: Work Productivity and Activity Impairment.
As reported by patients using the PDQ-39 and WPAI, there was a significant difference in health problems and impairments in activity due to PD across disease stages (Figure 4C & D). For the early, intermediate and severe groups, respectively, mean (SD) PDQ-39 scores were 10.1 (10.7), 22.2 (17.0) and 49.4 (25.3; p < 0.001). There was a significant difference (p < 0.001) across the groups for all eight scales of the PDQ-39. Mean (SD) WPAI percent activity impairment due to PD was 28.2% (22.0%), 44.2% (22.4%) and 67.9% (21.8%) for the early, intermediate and severe groups, respectively. Patient numbers reporting work time missed, impairment while working and overall work impairment due to PD were too low for meaningful comparisons in the intermediate (n = 9) and severe (n = 1) groups. Pairwise comparisons for the PDQ-39 scores and WPAI showed that the intermediate group reported a significantly worse health status and activity compared with the early group (p < 0.001), although they were significantly better than the severe group (p < 0.001). The PDQ-39 scores showed that the severe group also reported a significantly worse health status compared with the early group (p < 0.001).
Healthcare resource utilization
Overall, there was a significant difference in HCRU across disease stages (all comparisons p < 0.001).
Patients in the intermediate and severe groups had a higher likelihood of being managed by more healthcare professionals (HCPs) in the previous 12 months compared with patients in the early group (early vs intermediate: p < 0.050; early vs severe: p < 0.050; Table 5). Over a third of patients in the intermediate (36.2%) and severe (41.5%) groups had visited an HCP four of more times in the previous 12 months (Table 5).
| Variable | Overall (n = 1251) | H&Y stage† | p-value (test) | ||
|---|---|---|---|---|---|
| Early (n = 593) | Intermediate (n = 505) | Severe (n = 153) | |||
| HCPs involved in the patients' PD management in the previous 12 months | <0.001 (KW) | ||||
| n | 1251 | 593 | 505 | 153 | |
| Mean (SD) | 1.2 (0.7) | 1.1 (0.6) | 1.3 (0.7) | 1.3 (0.8) | |
| Median (min, max) | 1.0 (0.0, 11.0) | 1.0 (0.0, 11.0) | 1.0 (0.0, 6.0) | 1.0 (0.0, 5.0) | |
| HCP consultations in previous 12 months | <0.001 (KW) | ||||
| n | 1128 | 527 | 459 | 142 | |
| Times seen by HCP, n (%) | |||||
| 0 | 19 (1.7) | 8 (1.5) | 9 (2.0) | 2 (1.4) | |
| 1 | 167 (14.8) | 83 (15.7) | 67 (14.6) | 17 (12.0) | |
| 2 | 396 (35.1) | 247 (46.9) | 119 (25.9) | 30 (21.1) | |
| 3 | 225 (19.9) | 93 (17.6) | 98 (21.4) | 34 (23.9) | |
| 4 | 176 (15.6) | 59 (11.2) | 90 (19.6) | 27 (19.0) | |
| 5–6 | 93 (8.2) | 25 (4.7) | 51 (11.1) | 17 (12.0) | |
| ≥7 | 52 (4.6) | 12 (2.3) | 25 (5.4) | 15 (10.6) | |
| Emergency room visits in the previous 12 months | <0.001 (KW) | ||||
| n | 993 | 465 | 403 | 125 | |
| Mean (SD) | 0.2 (0.7) | 0.0 (0.2) | 0.3 (0.6) | 0.9 (1.3) | |
| Median (min, max) | 0.0 (0.0, 9.0) | 0.0 (0.0, 2.0) | 0.0 (0.0, 4.0) | 0.0 (0.0, 9.0) | |
| Admissions to a rehabilitation center in the previous 12 months | <0.001 (KW) | ||||
| n | 997 | 471 | 401 | 125 | |
| Mean (SD) | 0.0 (0.2) | 0.0 (0.1) | 0.0 (0.2) | 0.1 (0.4) | |
| Median (min, max) | 0.0 (0.0, 2.0) | 0.0 (0.0, 1.0) | 0.0 (0.0, 2.0) | 0.0 (0.0, 2.0) | |
†
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
Proportions may not equal 100% due to rounding.
H&Y: Hoehn and Yahr; HCP: Healthcare professional; KW: Kruskal–Wallis test; PD: Parkinson’s disease; SD: Standard deviation.
The number of consultations with any HCP in the previous 12 months was significantly greater for patients in the intermediate group versus early group (IRR: 1.4; 95% CI: 1.2, 1.7; p < 0.050; Table 6). In the previous 12 months, patients in the intermediate group had a higher likelihood of more consultations with psycho-geriatricians (IRR: 45.8; 95% CI: 11.0, 190.5; p < 0.050), PD nurses (IRR: 23.6; 95% CI: 13.9, 39.8; p < 0.050), gastroenterologists (IRR: 13.9; 95% CI: 1.2, 162.7; p < 0.050) and social workers (IRR: 6.3; 95% CI: 4.7, 8.6; p < 0.050) when compared with patients in the early group. IRRs for PD nurses and gastroenterologists were higher for the intermediate group than the severe group (severe group: PD nurses: IRR: 7.5; 95% CI: 3.3, 16.8; gastroenterologists: IRR: 1.6e–06; 95% CI: 1.5e–07, 1.8e–05).
The number of consultations with any HCP in the previous 12 months was also notably greater for patients in the severe group compared with the early group (IRR: 1.6; 95% CI: 1.3, 1.9; p < 0.001; Table 6). In the previous 12 months, patients in the severe group had a higher likelihood of more consultations with movement disorder specialists (IRR: 844.7; 95% CI: 68.0, 10488.2; p < 0.001), psycho-geriatricians (IRR: 60.3; 95% CI: 18.0, 202.0; p < 0.001), PD nurses (IRR: 7.5; 95% CI: 3.3, 16.8; p < 0.001), gastroenterologists (IRR: 1.6e–06; 95% CI: 1.5e–07, 0.00002; p < 0.001) and social workers (IRR: 21.0; 95% CI: 3.0, 149.0; p = 0.002) when compared with patients in the early group.
Patients in the intermediate group were more likely to have a higher number of emergency room (ER) visits in the previous 12 months compared with patients in the early group (IRR: 3.8; 95% CI: 2.3, 6.4; p < 0.001; Table 6). Patients in the intermediate group were also more likely to have admissions to rehabilitation centers compared with patients in the early group (IRR: 6.8; 95% CI: 1.4, 34.1; p < 0.050; Table 6).
Similarly, patients in the severe group were more likely to have a higher number of ER visits in the previous 12 months compared with patients in the early group (IRR: 10.5; 95% CI: 5.3, 20.7; p < 0.001; Table 6). Patients in the severe group were also more likely to have admissions to rehabilitation centers compared with patients in the early group (IRR: 8.3; 95% CI: 1.7, 40.1; p < 0.050; Table 6).
Discussion
Current Parkinson’s research often overlooks patients with intermediate-stage PD, opting to compare disease burden and HCRU between early- and severe-stage PD. Our analysis is unique in that it evaluated the impact of intermediate-stage PD on patients and HCRU in the US to elucidate clinical characteristics, treatment patterns and patient-reported outcomes among these patients and compare them to their early and severe PD counterparts. Our findings identified differences across early, intermediate and severe PD, highlighting the significant increase in both disease burden and HCRU for patients with intermediate PD compared with patients with early PD.
| Variable | H&Y stage† | ||
|---|---|---|---|
| Early (n = 593) | Intermediate (n = 505) | Severe (n = 153) | |
| Incidence rate ratio (95% CI) | |||
| HCPs involved in patients PD management in the previous 12 months, n | 1 | 1.14 (1.0, 1.3)§ | 1.20 (1.0, 1.4)§ |
| Times seen by HCP, n | 1 | 1.38 (1.2, 1.7)‡ | 1.61 (1.3, 1.9)‡ |
| Emergency room visits in the last 12 months, n | 1 | 3.80 (2.3, 6.4)‡ | 10.49 (5.3, 20.7)‡ |
| Admissions to a rehabilitation center in the previous 12 months, n | 1 | 6.8 (1.4, 34.1)‡ | 8.30 (1.7, 40.1)‡ |
†
H&Y stage: early, H&Y stage 1.0–2.0; intermediate, H&Y stage 2.5–3.0; severe, H&Y stage 4.0–5.0.
‡
‘Early’ H&Y stage is the reference value; p < 0.050 for early stage vs severe stage.
§
‘Early’ H&Y stage is the reference value; p < 0.050 for early stage vs intermediate stage, and early stage vs severe stage.
CI: Confidence interval; HCP: Healthcare professional; H&Y: Hoehn and Yahr; IRR: Incidence rate ratio; PD: Parkinson’s disease.
Defined by the emergence of postural instability (which is absent in early stage) while remaining physically independent (which is lost due to severe disability at severe stage), the intermediate stage of PD is a critical point in disease progression from early- to severe-stage PD [23]. This fact highlights the need for a better understanding of the intermediate stage, its characterization in real-world settings, and its inclusion within PD clinical trials to improve patient QoL.
Possibly to address increasing levels of disease burden, physician prescribing of levodopa significantly increased from early PD to intermediate PD, and the proportions of patients receiving levodopa were similar between the intermediate and severe groups. The analysis indicated that use of levodopa predominates in the treatment of motor symptoms. However, there is evidence that combination therapy was used in some patients, likely to prevent the frequent complication of shortening therapeutic response with recurrence of motor and nonmotor symptoms during the period known as ‘wearing-off’ when levodopa does not provide an adequate dopaminergic effect [37]. These data support existing evidence suggesting that levodopa remains key to antiparkinsonian therapy, is favored as the initial treatment for patients with PD, and may be best used in combination therapy [16].
Dopamine agonists were currently used approximately by a third of patients across all groups, supporting the view that they remain a popular choice for augmentation of levodopa [38] despite their potential to increase the severity of levodopa-induced dyskinesia [39]. While COMT inhibitors are commonly used alongside levodopa to avoid the troughs in levodopa plasma concentration associated with motor fluctuations [40], we found that few patients overall used COMT inhibitors. However, their use significantly increased among patients in the intermediate group compared with the early group. Moreover, among the intermediate group, use of NMDA antagonists significantly increased versus the early group but was significantly less than in the severe group where they were used by a third of patients. Furthermore, while there was limited prescribing of advanced therapies, only a third as many patients in the intermediate group versus the severe group were prescribed such therapies.
Data concerning previous lines of therapy suggested that the use of levodopa at lines 1 and 2 was similarly high when the patients’ disease stage was intermediate or severe. However, use of NMDA antagonists and COMT inhibitors was at least twice as high in patients in the severe group versus the intermediate group. Low use of NMDA antagonists and COMT inhibitors at the early stage, alongside findings of increased disease burden and HCRU burden at the intermediate stage, suggests that use of more effective treatments in the early and intermediate stages may help to reduce the overall burden of PD.
Despite disease stage, the intermediate group had many unmet treatment needs, which were often present in similar proportions to those of patients in the severe group. ‘Reducing tremor’ was a need reported for few patients, but it was threefold greater in the intermediate versus severe group. ‘Slowing disease progression’ and ‘disease modification’ were in the top three unmet needs reported across severity stages. While there are no available disease-modifying drugs or neuroprotective treatments [1,13], a few patients only received therapies for severe PD. Whether due to the reluctance to prescribe or lack of awareness of these therapies, this suggests a need for more efficacious drugs.
Several promising advancements in levodopa formulation and delivery have been made, including extended-release oral drugs, continuous subcutaneous infusions, intravenous infusions and administration by intestinal and inhalation routes [16]. However, it has been suggested that failing to properly recognize the disease stage of the patient, and thus failing to treat appropriately, may be one reason PD treatments fail to limit disease progression [41]; this may be particularly relevant to patients with intermediate-stage PD.
Most patients with intermediate PD reported that they were satisfied with their treatment (scoring 5 or 6 out of 7). Contrary to physician reports of unmet treatment needs, this finding suggests that patients consider their current treatment to be achieving the best possible disease control. US and European surveys of early- and advanced-stage patients with PD found that patients rated their treatment as 6.6 points (6.7 and 6.6 out of 10 for early- and advanced-stage, respectively) [42]. Additionally, we found that satisfaction was lower among patients with more severe disease, and that these patients also had reduced QoL, increased health problems, worsened activity impairment and increased unmet needs, potentially indicating an association between these factors.
We found that there were significant differences in symptom prevalence, severity and control across disease stages for motor symptoms such as bradykinesia, shuffling walk, falling/imbalance, rigidity and freezing of gait. These motor symptoms are known to reappear between medication doses when treatment regimens are not adequately optimized, leading to periods of time when symptoms are poorly managed [43]. As a result, patients can experience an increased risk of falls and injuries, primarily driven by tremor, slow movement, impaired gait and rigidity. While we did not observe any significant difference between disease stages in terms of tremor at rest, this was expected as this hallmark symptom of PD often appears before other symptoms and persists as the disease progresses [2]. PD-associated motor symptoms not only impact QoL, but also pose a risk to the safety of the patient. When symptoms are not well controlled, patients are also more likely to require medical attention, leading to increased hospitalizations and associated healthcare costs. Therefore, these findings underscore the importance of optimizing dosage and treatment to ensure continuous and effective symptom management for patients at all disease stages.
For all patient-reported QoL measures, intermediate-stage PD patients reported significantly worse QoL compared with early-stage patients, and severe-stage patients reported significantly worse QoL than intermediate-stage patients. In the intermediate stage of PD, patients continue to strive to maintain independence while they still retain sufficient physical and mental function. As the disease progresses to severe stage, independence and mobility are further reduced, leading to a reduced QoL and greater dependence on caregivers for help with daily activities [44]. A previous study demonstrated that patients with PD had lower QoL scores when compared with healthy controls, especially in physical function and mental health domains [45]. We found that physicians reported a significantly greater unmet need among intermediate-stage PD patients compared with early-stage patients, but not between the intermediate and severe stages. This suggests that during the intermediate stage of PD, there is a window of time during which addressing unmet needs is crucial, particularly as patients strive to maintain independence and mobility. However, once the disease progresses, the focus shifts from maintaining mobility to managing more advanced symptoms. We observed no significant differences in physician-reported unmet needs between intermediate- and severe-stage patients, indicating that offering disease-modifying treatments, maintaining QoL, ensuring long-term efficacy and reducing bradykinesia/rigidity are not realistic considerations. These findings highlight the complexity of managing PD as it progresses and underscore the importance of timely intervention during the intermediate stage to potentially mitigate the decline in QoL.
Our analysis found that there was a significant difference in HCRU across disease stages, and patients with intermediate-stage PD utilized significantly more healthcare resources than patients with early-stage disease. Compared with beneficiaries without PD, patients with PD have been found to have higher rates of HCRU, including a more than fivefold increase in neurologist visits and a twofold increase in skilled nursing facility admissions [46]. A Medicare claims database study found that severe PD was associated with a larger economic burden than mild/moderate PD in elderly US beneficiaries [5]. Additionally, higher total annual direct costs are reported for patients experiencing treatment ‘OFF’ episodes due to the resulting HCP consultations, hospitalizations and ER visits [47], with significant increases in PD-related ER visits and hospitalizations associated with patients experiencing ‘OFF’ episodes for longer time periods (≥2 years vs <2 years) [48]. These findings suggest that optimizing the pharmacological symptomatic treatment of patients before they reach more severe stages may incur savings. Thus, with 40% of patients in the intermediate stage of PD and the 2017 US total annual medical cost attributable to PD at $51.9 billion (including consultations, hospital outpatient visits and hospitalizations) [6], the potential economic burden associated with intermediate-stage PD in the US is considerable.
In managing PD, treatment strategies should be tailored to the individual and their disease stage in order to optimize patient outcomes. In the early stage, symptomatic treatment using oral medications, particularly before introducing levodopa, helps to maintain QoL. This approach is effective as long as the therapeutic window remains open, i.e., until ‘OFF’ episodes become an issue. For intermediate-stage patients who aspire to maintain independence but may experience ‘OFF’ episodes and injuries, introducing continuous levodopa at lower doses could help to avoid peaks and troughs in its bioavailability and the subsequent fluctuations in symptom control. In severe PD, continuous delivery of high-dose levodopa, along with other advanced device-aided therapies, is accepted due to the increased severity of symptoms. Therefore, by commencing continuous levodopa dosing at an earlier disease stage, dosing could be gradually optimized over time, potentially slowing the decline in QoL, rather than patients experiencing the sudden and significant decline we observed between the intermediate and severe stages.
The findings of this analysis suggest that further research into patients that fall into the intermediate H&Y disease stages (2.5–3.0) is warranted. Such data may allow the opportunity for more effective intervention and help to decrease the burden of PD for patients and the healthcare system by delaying the transition to the severe stages of PD. Furthermore, a more targeted approach to treatment for patients with intermediate-stage PD is required, along with new methods of drug delivery, to address the unmet needs that are prominent in this patient group.
Limitations
While identification of statistically significant associations is possible, the cross-sectional design of the DSP prevents any conclusions about causal relationships. Patients participating in the surveys may not reflect the general PD population, as patients who are visiting their physician are necessarily those who visit more frequently. High rates of patients in the intermediate and severe groups were retired and therefore their work productivity could not be assessed, restricting the findings of the WPAI to activity impairment.
Although minimal inclusion criteria governed the selection of participating physicians, only those willing to complete the survey were included. Thus, bias is possible since participating physicians may not be representative of the overall population of physicians treating PD.
A strength of this study is that it uses real-world data collected from the Adelphi PD DSP, which utilizes standardized methodology and is well validated and published. Nevertheless, our findings on intermediate PD should be considered with regard to the limitations of the DSP survey.
Conclusion
This real-world analysis demonstrated significant increases in both disease burden and HCRU for patients with intermediate PD compared with patients with early PD. It also indicated that among all people diagnosed with PD at any given time, a large proportion of these patients may be in the intermediate stage. This PD stage is crucial since it is when postural instability emerges, and because it immediately precedes the advanced/severe stages. Our data support more effective intervention, specifically at the intermediate stage of the disease, to help decrease the burden of PD for patients and the healthcare system. They also suggest the need for the development of more targeted treatment interventions directed at the intermediate disease stage to reduce such burden. This analysis provides a better understanding of patients with intermediate-stage PD, and highlights the need for this disease stage to be further characterized and included in real-world studies and clinical trials to improve patient QoL.
Summary points
•
Current Parkinson’s disease (PD) research evaluates patients with early and severe PD but often overlooks patients with intermediate PD, despite the increasing burden on patients and healthcare resource utilization.
•
This study quantified the unmet treatment needs and disease burden in patients with PD, as well as the burden on the healthcare system, across different Hoehn and Yahr (H&Y) stage groups in the US.
•
US data were drawn from the Adelphi PD Disease Specific Programme™. Using H&Y stages, patients were categorized as early (stage 1.0–2.0), intermediate (stage 2.5–3.0) or severe (stage 4.0–5.0).
•
The number of drugs in the current treatment regimen and use of levodopa were each significantly different across disease stages (p < 0.001).
•
Odds ratios were significantly increased for the intermediate group using levodopa (OR 5.6) and other treatment classes versus the early group.
•
The proportion of the intermediate group with unmet treatment needs was significantly greater than the early group (all comparisons, p < 0.001, except ‘reduces tremor,’ p = 0.002).
•
Incidence rate ratios (IRR) were increased for the intermediate group versus the early group for numbers (in previous 12 months) of healthcare professionals involved in patient’s PD management (IRR 1.1), healthcare professionals consultations (IRR 1.4), emergency room visits (IRR 3.8) and rehabilitation admissions (IRR 6.8).
•
Patient-reported quality of life was significantly poorer in the intermediate group versus the early group (p < 0.001).
•
This real-world analysis found significant increases in disease burden and healthcare resource utilization for patients with intermediate PD versus patients with early PD.
•
More effective intervention of patients at intermediate-stage PD may delay the transition to severe PD and decrease the burden of PD for both patients and the healthcare system.
Author contributions
M Ciepielewska was responsible for clinical oversight and guidance as lead author. All authors were involved in conception or design, or analysis and interpretation of data; drafting and revising the article; providing intellectual content of critical importance to the work described and final approval of the version to be published, and therefore meet the criteria for authorship in accordance with the International Committee of Medical Journal Editors (ICMJE) guidelines. In addition, all named authors take responsibility for the integrity of the work as a whole and have given their approval for this version to be published. All named authors meet the ICMJE criteria for authorship of this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Acknowledgments
This work has been previously presented as a poster at: AMCP Nexus 2022, National Harbor, MD, USA, 11–14 October 2022; Abstract G3: M Ciepielewska, M Hagan, E Jones, A Gillespie, C Walker, L Le Brocq. Assessing the clinical and economic burden experienced by patients with intermediate Parkinson’s disease: results from a real-world study; and at ISPOR Europe 2022, Virtual, 6–9 November 2022; PCR187: M Ciepielewska, M Hagan, E Jones, A Gillespie, C Walker, L Le Brocq. Assessing treatment needs and outcomes in patients with Parkinson's disease: results from a real-world study.
Financial disclosure
Data collection was undertaken by Adelphi Real World as part of an independent survey entitled, Adelphi Real World Parkinson’s Disease DSP. The DSP is a wholly owned Adelphi Real World product. Mitsubishi Tanabe Pharma America, Inc., New Jersey, is one of multiple subscribers to the DSP. Mitsubishi Tanabe Pharma America, Inc., New Jersey, USA, did not influence the original survey through either contribution to the design of questionnaires or data collection. Publication of survey results was not contingent on the subscriber’s approval or censorship of the publication. No funding or sponsorship was received by Adelphi Real World for this study or publication of this article.
Competing interests disclosure
M Ciepielewska is an employee of Mitsubishi Tanabe Pharma America, Inc., and has stocks/shares in Mitsubishi Tanabe Pharma America. E Jones, A Gillespie, C Walker, L LeBrocq and S Weatherby are employees of Adelphi Real World. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing support under the guidance of the authors was provided by S Libretto of Sue Libretto Publications Consultant Ltd, on behalf of Adelphi Real World in accordance with Good Publication Practice (GPP 2022) Guidelines. Editorial support was also provided by p-value communications, Cedar Knolls, NJ, USA. This support was funded by Mitsubishi Tanabe Pharma America, Inc., Jersey City, NJ, USA, in accordance with Good Publication Practice Guidelines 2022 [49].
Informed consent disclosure
A survey number was assigned to all participating physicians and patients to enable anonymous data collection and data linkage during data collection and analysis, enabling physician-patient data matching. Using a checkbox, patients provided informed consent to take part in the survey. Data were collected in such a way that patients and physicians could not be identified directly. Data were aggregated before being shared with the subscriber and/or for publication. Data collection was undertaken in line with European Pharmaceutical Marketing Research Association guidelines [34] and as such did not require ethics committee approval. Each survey was performed in full accordance with relevant legislation at the time of data collection, including the US Health Insurance Portability and Accountability Act 1996 [35] and Health Information Technology for Economic and Clinical Health Act legislation [36]. Fieldwork partners adhered to national data collection regulations in the USA.
Data sharing statement
All data, i.e., methodology, materials, data and data analysis, that support the findings of this survey are the intellectual property of Adelphi Real World. All requests for access should be addressed directly to Chloe Walker at [email protected]. C Walker is an employee of Adelphi Real World.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Kalia LV, Lang AE. Parkinson's disease. Lancet 386(9996), 896–912 (2015).
2.
Kouli A, Torsney KM, Kuan WL. Chapter 1: Parkinson's disease: etiology, neuropathology, and pathogenesis. In: Parkinson's Disease: Pathogenesis and Clinical Aspects. Stoker TB, Greenland JC (Eds). Codon Publications, Australia (2018).
3.
Ou Z, Pan J, Tang S et al. Global trends in the incidence, prevalence, and years lived with disability of Parkinson's disease in 204 countries/territories from 1990 to 2019. Front. Public Health 9, 776847 (2021).
4.
US Neurological Disorders Collaborators; Feigin VL, Vos T, Alahdab F et al. Burden of neurological disorders across the US from 1990–2017: a Global Burden of Disease study. JAMA Neurol. 78(2), 165–176 (2021).
5.
Dahodwala N, Li P, Jahnke J et al. Burden of Parkinson's disease by severity: health care costs in the U.S. medicare population. Mov. Disord. 36(1), 133–142 (2021).
6.
Yang W, Hamilton JL, Kopil C et al. Current and projected future economic burden of Parkinson's disease in the U.S. NPJ. Parkinsons Dis. 6, 15 (2020).
• Analyzes the economic burdens of Parkinson’s disease in the US (2017) and projections for the next two decades, with findings underscoring the substantial burden of PD to society, payers, patients and caregivers.
7.
World Health Organization. Parkinson disease. A public health approach. Technical brief. World Health Organization, Switzerland (2022).
8.
Balestrino R, Schapira AHV. Parkinson disease. Eur. J. Neurol. 27(1), 27–42 (2020).
9.
Tolosa E, Garrido A, Scholz SW, Poewe W. Challenges in the diagnosis of Parkinson's disease. Lancet Neurol. 20(5), 385–397 (2021).
10.
Postuma RB, Berg D, Adler CH et al. The new definition and diagnostic criteria of Parkinson's disease. Lancet Neurol. 15(6), 546–548 (2016).
11.
Tysnes OB, Storstein A. Epidemiology of Parkinson's disease. J. Neural. Transm. (Vienna) 124(8), 901–905 (2017).
12.
Lotankar S, Prabhavalkar KS, Bhatt LK. Biomarkers for Parkinson's disease: recent advancement. Neurosci. Bull. 33(5), 585–597 (2017).
13.
Zahoor I, Shafi A, Haq E. Chapter 7: pharmacological treatment of Parkinson's disease. In: Parkinson's Disease: Pathogenesis and Clinical Aspects. Stoker TB, Greenland JC (Eds). Codon Publications, Australia (2018).
14.
Halli-Tierney AD, Luker J, Carroll DG. Parkinson disease. Am. Fam. Physician 102(11), 679–691 (2020).
• Provides a comprehensive overview of PD and its treatment.
15.
LeWitt PA, Chaudhuri KR. Unmet needs in Parkinson disease: motor and non-motor. Parkinsonism Relat. Disord. 80(Suppl. 1), S7–S12 (2020).
16.
Lees A, Tolosa E, Stocchi F et al. Optimizing levodopa therapy, when and how? Perspectives on the importance of delivery and the potential for an early combination approach. Expert Rev. Neurother. 23(1), 15–24 (2023).
• Discusses the evidence for current levodopa optimization strategies during early disease and once motor complications have started. It reaffirms levodopa as the cornerstone of antiparkinsonian therapy and suggests patients would benefit from earlier use of low doses of several agents.
17.
Vanle B, Olcott W, Jimenez J et al. NMDA antagonists for treating the non-motor symptoms in Parkinson's disease. Transl. Psychiatry 8(1), 117 (2018).
18.
Cenci MA, Skovgård K, Odin P. Non-dopaminergic approaches to the treatment of motor complications in Parkinson's disease. Neuropharmacology 210, 109027 (2022).
19.
van den Heuvel L, Evers LJW, Meinders MJ et al. Estimating the effect of early treatment initiation in Parkinson's disease using observational data. Mov. Disord. 36, 407–414 (2021).
20.
Pagano G, Taylor KI, Anzures-Cabrera J et al. Trial of prasinezumab in early-stage Parkinson's disease. N. Engl. J. Med. 387(5), 421–432 (2022).
21.
Hacker ML, Turchan M, Heusinkveld LE et al. Deep brain stimulation in early-stage Parkinson disease: five-year outcomes. Neurology 95(4), e393–e401 (2020).
22.
Chaudhuri KR, Titova N. Societal burden and persisting unmet needs of Parkinson's disease. Eur. Neurol. Rev. 14(1), 28–35 (2019).
• Presents the current and future societal burden of PD and the unmet needs in PD, and the efforts and progress made to resolve them.
23.
Goetz CG, Poewe W, Rascol O et al. Movement disorder society task force on rating scales for Parkinson's Disease. Movement disorder society task force report on the Hoehn and Yahr staging scale: status and recommendations. Mov. Disord. 19(9), 1020–1028 (2004).
24.
Bhidayasiri R, Tarsy D. Parkinson's disease: Hoehn and Yahr scale. In: Movement Disorders: A Video Atlas. Humana Totowa, USA, p4–5 (2012).
25.
Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: disease-specific programmes – a means to understand. Curr. Med. Res. Opin. 24(11), 3063–3072 (2008).
26.
Anderson P, Higgins V, Courcy J et al. Real-world evidence generation from patients, their caregivers and physicians supporting clinical, regulatory and guideline decisions: an update on Disease Specific Programmes. Curr. Med. Res. Opin. 39(12), 1707–1715 (2023).
27.
Babineaux SM, Curtis B, Holbrook T, Milligan G, Piercy J. Evidence for validity of a national physician and patient-reported, cross-sectional survey in China and UK: the disease specific programme. BMJ Open 6(8), e010352 (2016).
28.
Higgins V, Piercy J, Roughley A et al. Trends in medication use in patients with Type 2 diabetes mellitus: a long-term view of real-world treatment between 2000 and 2015. Diabetes Metab. Syndr. Obes. 9, 371–380 (2016).
29.
Peto V, Jenkinson C, Fitzpatrick R, Greenhall R. The development and validation of a short measure of functioning and well being for individuals with Parkinson's disease. Qual. Life Res. 4(3), 241–248 (1995).
30.
EuroQol Group. EuroQol—a new facility for the measurement of health-related quality of life. Health Policy 16(3), 199–208 (1990).
31.
EuroQol Research Foundation. EQ-5D-5L User Guide.v3 2019. EuroQol Research Foundation, Rotterdam, The Netherlands (2021).Available from: https://euroqol.org/publications/user-guides/
32.
Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a Work Productivity and Activity Impairment instrument. Pharmacoeconomics 4(5), 353–365 (1993).
33.
Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist 20(6), 649–655 (1980).
34.
European Pharmaceutical Market Research Association (EPHMRA). Code of Conduct. (2020). Available from: https://www.ephmra.org/media/4857/ephmra-2020-code-of-conduct-final.pdf
35.
US Department of Health and Human Services. Summary of the HIPAA Privacy Rule. (2003). Available from: http://www.hhs.gov/sites/default/files/privacysummary.pdf
36.
Health Information Technology (HITECH). Health Information Technology Act. (2009). Available from: https://www.healthit.gov/sites/default/files/hitech_act_excerpt_from_arra_with_index.pdf
37.
Stocchi F, Antonini A, Barone P et al. Early detection of wearing off in Parkinson disease: the DEEP study. Parkinsonism Relat. Disord. 20(2), 204–211 (2014).
38.
Crispo JA, Fortin Y, Thibault DP et al. Trends in inpatient antiparkinson drug use in the USA, 2001–2012. Eur. J. Clin. Pharmacol. 71(8), 1011–1019 (2015).
39.
Brodsky MA, Park BS, Nutt JG. Effects of a dopamine agonist on the pharmacodynamics of levodopa in Parkinson disease. Arch. Neurol. 67(1), 27–32 (2010).
40.
Müller T. Catechol-O-methyltransferase inhibitors in Parkinson's disease. Drugs 75(2), 157–174 (2015).
41.
Zhang Z, Zhang S, Fu P et al. Roles of glutamate receptors in Parkinson's disease. Int. J. Mol. Sci. 20(18), 4391 (2019).
42.
Fargel M, Grobe B, Oesterle E, Hastedt C, Rupp M. Treatment of Parkinson's disease: a survey of patients and neurologists. Clin. Drug Investig. 27(3), 207–218 (2007).
43.
Freitas ME, Hess CW, Fox SH. Motor complications of dopaminergic medications in Parkinson's disease. Semin. Neurol. 37(2), 147–157 (2017).
44.
Rosqvist K, Schrag A, Odin P. The CLaSP Consortium. Caregiver burden and quality of life in late stage Parkinson's disease. Brain Sci. 12(1), 111 (2022).
45.
Zhao N, Yang Y, Zhang L et al. Quality of life in Parkinson's disease: a systematic review and meta-analysis of comparative studies. CNS Neurosci. Ther. 27(3), 270–279 (2021).
46.
Gandhi AB, Onukwugha E, Albarmawi H et al. Health care resource utilization associated with Parkinson disease among Medicare beneficiaries. Neurology 97(6), e597–e607 (2021).
47.
Thach A, Jones E, Pappert E, Pike J, Wright J, Gillespie A. Real-world assessment of “OFF” episode-related healthcare resource utilization among patients with Parkinson's disease in the United States. J. Med. Econ. 24(1), 540–549 (2021).
48.
Serbin M, Odak S, Macahilig C et al. Real-world healthcare resource utilization in patients with Parkinson's disease and motor fluctuations. Mov. Disord. 35(Suppl.1), S142 (2022). Available at: https://www.mdsabstracts.org/abstract/real-world-healthcare-resource-utilization-in-patients-with-parkinsons-disease-and-motor-fluctuations/
49.
DeTora LM, Toroser D, Sykes A et al. Good Publication Practice (GPP) guidelines for company-sponsored biomedical research: 2022 update. Ann. Intern. Med. 175(9), 1298–1304 (2022).
Information & Authors
Information
Published In
Copyright
© 2025 Mitsubishi Tanabe Pharma America, Inc., Jersey City, NJ, USA. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 3 October 2024
Accepted: 13 August 2025
Published online: 23 September 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Assessing healthcare resource utilization burden and unmet treatment needs in patients with Parkinson’s disease: results from a real-world study. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0186
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yongxin Xu, Chenhao Yang, Yichao Du, Xiaonan Shen, Tingting Li, Yufeng Zhang, Zijun Lu, Jie Zhuang, Nan Chen, Yulian Zhu, Chencheng Zhang, Jiaojiao Lü, Lingyan Huang, Lu Li, Jianqiang Lü, Zhenyu Qian, Zhen Wang, Jian Zhang, Junhong Zhou, Yu Liu, Temporal Interference Stimulation Modulates Resting State Functional Connectivity of Motor Circuit in Parkinson's Disease, Movement Disorders, 10.1002/mds.70321, (2026).