Adverse event costs of systemic therapies for metastatic colorectal cancer previously treated with fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy and biologics in the US
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The objective of this study was to compare adverse event (AE) management costs for fruquintinib, regorafenib, trifluridine/tipiracil (T/T) and trifluridine/tipiracil+bevacizumab (T/T+bev) for patients with metastatic colorectal cancer (mCRC) previously treated with at least two prior lines of therapy from the US commercial and Medicare payer perspectives. Materials & methods: A cost-consequence model was developed to calculate the per-patient and per-patient-per-month (PPPM) AE costs using rates of grade 3/4 AEs with incidence ≥5% in clinical trials, event-specific management costs and duration treatment. Anchored comparisons of AE costs were calculated using a difference-in-differences approach with best supportive care (BSC) as a common reference. AE rates and treatment duration were obtained from clinical trials: FRESCO and FRESCO-2 (fruquintinib), RECOURSE (T/T), CORRECT (regorafenib) and SUNLIGHT (T/T, T/T+bev). AE management costs for the commercial and Medicare perspectives were obtained from publicly available sources. Results: From the commercial perspective, the AE costs (presented as per-patient, PPPM) were: $4015, $1091 for fruquintinib (FRESCO); $4253, $1390 for fruquintinib (FRESCO-2); $17,110, $11,104 for T/T (RECOURSE); $9851, $4691 for T/T (SUNLIGHT); $8199, $4823 for regorafenib; and $11,620, $2324 for T/T+bev. These results were consistent in anchored comparisons: the difference-in-difference for fruquintinib based on FRESCO was -$1929 versus regorafenib and -$11,427 versus T/T; for fruquintinib based on FRESCO-2 was -$2257 versus regorafenib and -$11,756 versus T/T. Across all analyses, results were consistent from the Medicare perspective. Conclusion: Fruquintinib was associated with lower AE management costs compared with regorafenib, T/T and T/T+bev for patients with previously treated mCRC. This evidence has direct implications for treatment, formulary and pathways decision-making in this patient population.
Plain language summary
What is this article about?
Fruquintinib, regorafenib, trifluridine/tipiracil (T/T) and trifluridine/tipiracil plus bevacizumab (T/T+bev) have demonstrated survival benefits versus best supportive care for the treatment of metastatic colorectal cancer (mCRC) that has progressed following prior lines of therapy. However, there is limited evidence on their relative safety profiles and respective adverse event (AE)-related cost burden. This study estimates the costs of grade 3/4 AEs related to these therapies based on clinical trial data.
What were the results?
The analysis found that fruquintinib was associated with a lower cost of managing AEs compared with the other therapies in previously treated patients with mCRC. A key cost-driver is the management of grade 3/4 hematologic AEs, which had the highest reported rates with T/T and T/T+bev compared with regorafenib or fruquintinib.
What do the results mean?
The cost implications of AEs associated with different treatments should be considered during treatment selection and formulary decision-making.
Colorectal cancer (CRC) is the fourth most common cancer type and the second leading cause of cancer deaths in the US, accounting for more than 153,000 cases and 56,000 deaths in 2023 [1,2]. CRC is often diagnosed at an advanced stage, with 21–23% of patients in the US diagnosed with metastatic CRC (mCRC) [2,3]. Additionally, up to half of patients with localized disease eventually develop metastases [4]. The prognosis for patients with mCRC is very poor, with the Surveillance, Epidemiology and End Results Program and Centers for Disease Control and Prevention reporting a 5-year relative survival rate in the US of <16% for patients with distant metastases, compared with 5-year survival rates ranging from 71 to 91% in patients with localized and regional CRC [2,5].
The burden associated with mCRC necessitates an effective treatment that prolongs survival while maintaining quality of life [6,7]. However, as mCRC is a heterogeneous disease with multiple pathogenic origins and various disease characteristics, multiple treatment options are needed in the mCRC treatment armamentarium to address individual patient needs [8,9]. Other factors, such as patient age and fitness, comorbidities and drug toxicity, must also be considered in treatment selection and may limit treatment options for certain patients [10].
First-line treatment of mCRC typically consists of a chemotherapy regimen based on fluoropyrimidine, oxaliplatin and/or irinotecan, with or without therapies targeting vascular endothelial growth factor receptors (VEGFRs) or epidermal growth factor receptors (EGFRs) [11–14]. However, most patients will progress following first-line treatment [11]. The presence of various biological determinants in some patients, including rat sarcoma proto-oncogene (RAS) mutations or deficient mismatch repair/microsatellite instability mutational status, may additionally influence treatment strategy [11].
Patients with mCRC are exposed to numerous cytotoxic agents during their lines of therapy, which often have substantial treatment-related toxicities [12,13,15–18]. Until recently, patients who have been previously treated with chemotherapy, anti-VEGF therapy, and/or anti-EGFR therapy (if RAS wild type) had only regorafenib and trifluridine/tipiracil (T/T) ± bevacizumab as recommended treatment options [13,14]. Safety concerns have been associated with each of these treatments. Regorafenib has a boxed warning for severe hepatoxicity in the US FDA Prescribing Information, and hand-foot skin reaction has been a frequently reported treatment-related and high-grade adverse event (AE) in clinical trials [17,19,20]. T/T is associated with high rates of myelosuppression, which can be severe and potentially life-threatening [18,21,22]. T/T + bevacizumab (T/T+bev) led to higher rates of grade ≥3 neutropenia than T/T alone, and almost a third of patients required treatment with granulocyte-colony stimulating factor in the SUNLIGHT phase III trial [23]. Furthermore, bevacizumab must be administered via an intravenous (IV) infusion over 30 to 90 min and is associated with infusion-related reactions [24].
Fruquintinib was recently approved by the US FDA (8 November 2023) for adult patients with mCRC who received prior fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy, an anti-VEGF therapy, and, if RAS wild-type and medically appropriate, an anti-EGFR therapy [25]. The most common grade 3/4 AE was hypertension [26,27], and most common AEs (incidence >20%) were hypertension, palmar-plantar erythrodysesthesia, proteinuria, dysphonia, abdominal pain, diarrhea and asthenia [25].
Despite the widely varying AE profiles of the treatment options available for patients with previously treated mCRC, there is limited evidence on the relative safety profiles and AE-related cost burden associated with these treatments. A recent study by Howe et al. comparing randomized trials of patients with mCRC previously treated with at least two prior lines of therapy showed lower treatment exposure-adjusted AE rates associated with grade 3/4 AEs with fruquintinib treatment compared with other treatment options [28]. This study aimed to evaluate the costs associated with managing grade 3/4 AEs related to systemic therapies in this patient population.
Methods
Overall approach
The costs of AE management were estimated from a third-party payer perspective using the rates of grade 3/4 AEs occurring in ≥5% of participants as reported in international phase III randomized clinical trials of fruquintinib, regorafenib, T/T, T/T+bev and best supportive care (BSC) and the respective AE management costs from public databases. For each AE, the cost was estimated as the AE rate multiplied by the corresponding cost of AE management. The AE cost per patient was estimated over the course of treatment for each therapy as the sum over all AEs included for cost estimation, as follows:
Because AEs occurred throughout the treatment course and the duration of treatment (DOT) was different for each therapy, per-patient-per-month (PPPM) AE costs were also calculated as the per-patient AE costs divided by the median DOT (in months) of the corresponding treatment.
In addition, anchored comparisons on AE costs were calculated between the different systemic therapies using a difference-in-differences approach with BSC as a common reference group. First, the incremental AE management costs for each systemic therapy versus BSC from the same clinical trial were calculated as mean per-patient AE costs of systemic treatment – mean per-patient AE costs of BSC. Anchored comparisons for fruquintinib versus each comparator were calculated as: (Incremental AE management cost of fruquintinib) – (Incremental AE management cost of comparator). Because there was no BSC arm in the SUNLIGHT trial, the AE burden for T/T+bev cannot be anchored to BSC.
Inputs & data sources
AE Rates & DOT
AE rates and DOT were obtained from international phase III randomized clinical trials. Specifically, data from the following trials were used as these are the clinical studies included in the US FDA Prescribing Information for each treatment: fruquintinib, FRESCO (NCT02314819) and FRESCO-2 (NCT04322539); T/T, RECOURSE (NCT01607957) and SUNLIGHT (NCT04737187); regorafenib, CORRECT (NCT01103323); T/T+bev, SUNLIGHT (NCT04737187) [19,22,25]. The treatments included fruquintinib (5 mg once daily [QD], orally [PO], 3 weeks on/1 week off) in FRESCO (n = 278) and FRESCO-2 (n = 456), T/T (35 mg/m2 twice daily [BID], PO, days 1–5 and 8–12) in RECOURSE (n = 533) and SUNLIGHT (n = 246) [18,23], regorafenib (160 mg QD, PO, 3 weeks on/1 week off) in CORRECT (n = 500) [17] and with T/T+bev (T/T 35 mg/m2 BID, PO, days 1–5 and 8–12 + bev 5 m/kg QD, IV, days 1 and 15) in SUNLIGHT (n = 246) [23]. For all aforementioned trials, except SUNLIGHT, both treatment or placebo were given in combination with BSC [19,22,25]. An overview of the clinical trials included is presented in Table 1; more detailed study characteristics and baseline characteristics for each trial can be found in Supplementary Table 1 and 2.
| Trial | Treatment | n | Median DoT (months) | Median follow-up (months) | Ref. |
|---|---|---|---|---|---|
| FRESCO | Fruquintinib + BSC | 278 | 3.7 | 13.3 | [26,29–31] |
| Placebo + BSC | 138 | 1.8 | 13.2 | ||
| FRESCO-2 | Fruquintinib + BSC | 461 | 3.1 | 11.3 | [32] |
| Placebo + BSC | 230 | 1.8 | 11.2 | ||
| CORRECT | Regorafenib + BSC | 505 | 1.7 | NR | [17] |
| Placebo + BSC | 255 | 1.6 | NR | ||
| RECOURSE | T/T + BSC | 534 | 1.54 | NR | [18,33–36] |
| Placebo + BSC | 266 | 1.31 | NR | ||
| SUNLIGHT | T/T | 246 | 2.1 | 13.6 | [23,37] |
| T/T+bev | 246 | 5.0 | 14.2 |
BSC: Supportive care; DoT: Duration of treatment; NR: Not reported; RAS: Rat sarcoma proto-oncogene; T/T: Trifluridine/tipiracil; T/T + bev: Trifluridine/tipiracil + bevacizumab; VEGF: Vascular endothelial growth factor.
AE reporting procedures were largely consistent across the phase III randomized clinical trials included in the analysis [17,18,23,26,38]. AEs were categorized using the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0, and AE rates were estimated as the proportion of patients in a treatment arm who experienced at least one event of the AE during the study period. Across all treatments, grade 3/4 AEs occurring in ≥5% for any treatment included: anemia, asthenia, diarrhea, fatigue, hand foot syndrome, hypertension, leukopenia, neutropenia, rash, thrombocytopenia and laboratory abnormalities (increased alanine aminotransferase, alkaline phosphatase, aspartate aminotransferase and total bilirubin). The most frequently reported grade 3/4 AEs (>15%) with fruquintinib were hypertension (16.5%) and with regorafenib were hand foot syndrome/palmar-plantar erythrodysesthesia (16.6%) and fatigue (15.4%). Both T/T and T/T+bev had high rates of hematologic grade 3/4 AEs, most notably neutropenia (43.1 and 36.0%, respectively); grade 3/4 anemia (15.9%) and leukopenia (14.6%) were also reported with T/T. Rates of grade 3/4 AEs that occurred in ≥5% of patients treated with fruquintinib (FRESCO and FRESCO-2), regorafenib (CORRECT), T/T (RECOURSE and SUNLIGHT) or T/T+bev (SUNLIGHT) are presented in Figure 1.
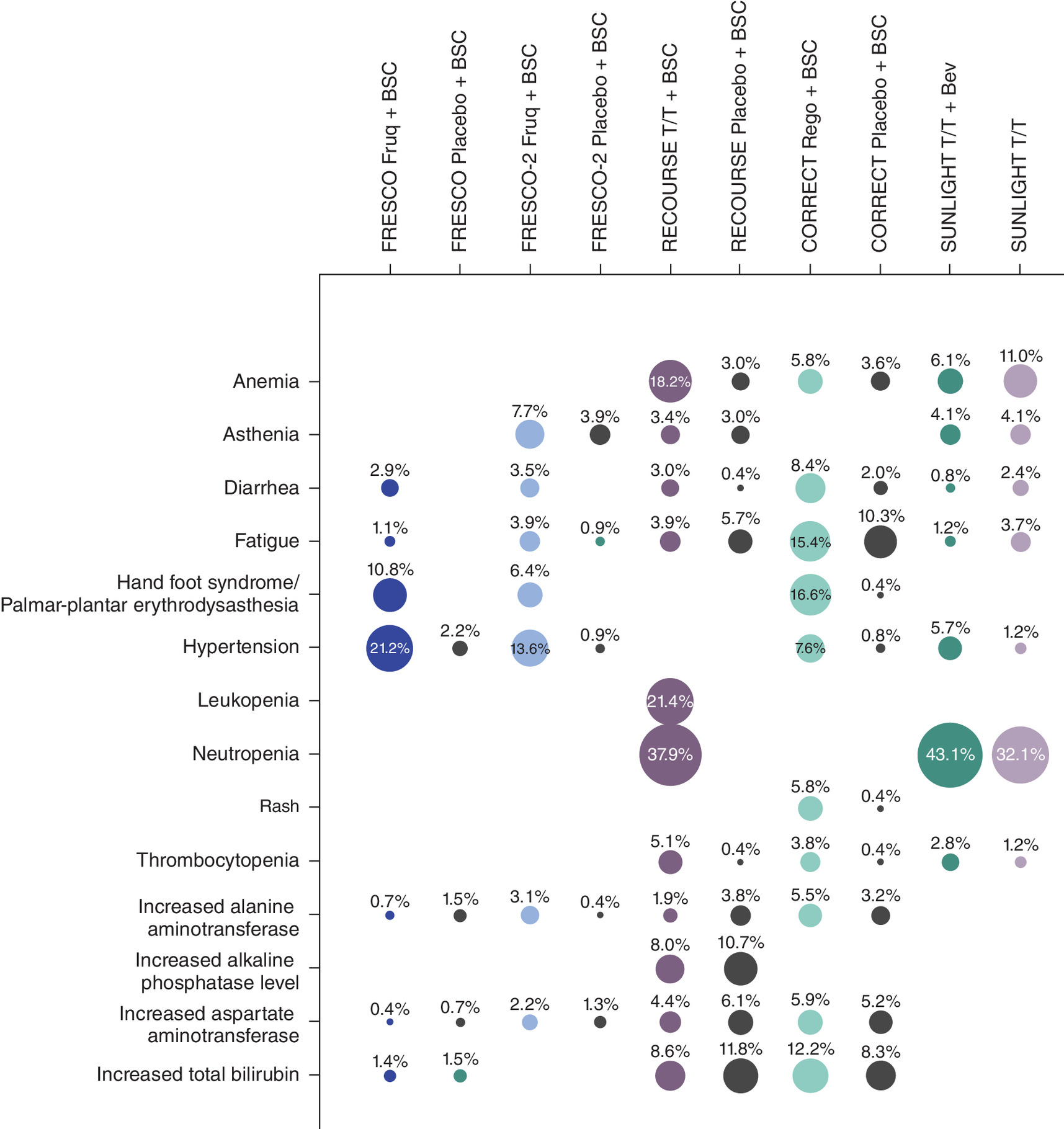
Figure 1. Rate of grade 3/4 adverse events occurring in ≥5% of patients in FRESCO-2, FRESCO, RECOURSE, CORRECT and SUNLIGHT.
AE: Adverse event; BSC: Best supportive care; Fruq: Fruquintinib; Rego: Regorafenib; T/T: Trifluridine/tipiracil; T/T + Bev: trifluridine/tipiracil + bevacizumab.
DOT was based on the reported median treatment duration for every treatment and BSC in each trial (Table 1) [17,18,23,26,38]. The reported median treatment duration was selected instead of the mean treatment duration, as only the median was reported for all the treatments; the mean treatment duration was not reported for T/T and T/T+bev in the SUNLIGHT trial [37].
Unit Cost of AEs
For laboratory abnormalities, for both the Medicare and commercial perspectives, the cost of a specialist visit was used based on a medical oncologist outpatient follow-up consultation for the evaluation and management of an established patient and moderate level of medical decision making (Table 2) [39,40]. The unit costs of management for the other AEs were obtained from the 2020 Healthcare Cost and Utilization Project for the commercial perspective and the FY2023 Medicare Acute Inpatient Prospective Payment System Fee Schedule for the Medicare perspective, based on the associated average hospital charged amount identified based on inpatient management diagnosis-related group codes (Table 2) [39,40]. The costs of AE management for the commercial perspective were inflated from 2020 to 2023 US dollars using a factor of 1.059 from the medical care component of the Consumer Price Index [41]. Additional details on how the management cost for each event was derived for both the commercial and Medicare perspectives is provided in Supplementary Table 3 and 4.
| Medicare [39] | Commercial [40]§ | |||
|---|---|---|---|---|
| DRG code | Mean cost | CCSR code | Mean cost | |
| Anemia | 811–812 | $7571.50 | BLD003 | $14,587.64 |
| Asthenia | 947–948 | $6109.69 | SYM007 | $14,586.58 |
| Diarrhea | 391–392 | $6319.82 | SYM006 | $9286.89 |
| Fatigue† | 947–948 | $6109.69 | SYM007 | $14,586.58 |
| Hand foot syndrome/palmar-plantar erythrodysesthesia | 606–607 | $7231.39 | SKN002 | $13,658.63 |
| Hypertension | 304–305 | $6000.46 | CIR008 | $9925.65 |
| Leukopenia | 814–816 | $9135.48 | BLD007 | $20,350.23 |
| Neutropenia | 808–810 | $10,779.63 | BLD007 | $20,350.23 |
| Rash | 606–607 | $7231.39 | SYM014 | $8829.28 |
| Thrombocytopenia | 813 | $10,735.85 | BLD006 | $19,497.50 |
| HCPCS code [42] | Mean cost | HCPCS code [43] | Mean cost | |
|---|---|---|---|---|
| Increased alanine aminotransferase‡ | 99214 | $128.43 | 99214 | $221.00 |
| Increased alkaline phosphatase level‡ | 99214 | $128.43 | 99214 | $221.00 |
| Increased aspartate aminotransferase‡ | 99214 | $128.43 | 99214 | $221.00 |
| Increased total bilirubin‡ | 99214 | $128.43 | 99214 | $221.00 |
†
The management cost associated with fatigue was assumed to be the same as asthenia due to lack of data for fatigue.
‡
The HCPCS Code 99214: Medical Oncologist Outpatient consultation – follow-up; office or other outpatient visit for the evaluation and management of an established patient, moderate level of medical decision making. 30–39 min of total time is spent on the date of the encounter.
§
Costs of AE management for the commercial perspective were inflated from 2020 to 2023 US dollars using a factor of 1.059 from the medical care component of the Consumer Price Index [41].
AE: Adverse event; CCSR: Clinical classifications software refined; DRG: Diagnosis related group; HCPCS: Healthcare common procedure coding system.
Results
AE management costs are shown in Table 3. The estimated management costs of grade 3/4 AEs of fruquintinib were lower compared with regorafenib, T/T and TT+bev, when considering costs either per-patient over the course of treatment or PPPM adjusted for median DOT, as shown in Figure 2A & B. From the commercial perspective, the lowest per-patient (and PPPM) AE management costs were for fruquintinib, at $4015 ($1091) based on AE rates in the FRESCO trial and $4253 ($1,390) in the FRESCO-2 trial. The highest AE management costs were associated with T/T, at $17,110 ($11,104) based on the RECOURSE trial and $9851 ($4691) based on the SUNLIGHT trial. Regorafenib and TT+bev had AE management costs between the AE management costs of T/T based on SUNLIGHT and RECOURSE. From the Medicare perspective, results were generally consistent. Per-patient (and PPPM) AE management costs for fruquintinib were $2307 ($627) based on FRESCO and $2216 ($724) based on FRESCO-2. Regorafenib-related AE management costs were $4425 ($2603). Finally, T/T per-patient and (PPPM) AE management costs were $8630 ($5601) based on RECOURSE and $5122 ($2439) based on SUNLIGHT, while costs for T/T+bev were $6125 ($1225).
| FRESCO | FRESCO-2 | RECOURSE | CORRECT | SUNLIGHT | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Fruq + BSC | Placebo + BSC | Fruq + BSC | Placebo + BSC | T/T + BSC | Placebo + BSC | Rego + BSC | Placebo + BSC | T/T+ Bev | T/T | |
| Per-patient over the course of treatment | ||||||||||
| Commercial | $4015 | $227 | $4253 | $793 | $17,110 | $1894 | $8199 | $2483 | $11,620 | $9851 |
| Medicare | $2307 | $137 | $2216 | $349 | $8630 | $868 | $4425 | $1191 | $6125 | $5122 |
| PPPM, adjusted for median DOT | ||||||||||
| Commercial | $1091 | $123 | $1390 | $431 | $11,104 | $1445 | $4823 | $1552 | $2324 | $4691 |
| Medicare | $627 | $74 | $724 | $190 | $5601 | $662 | $2603 | $744 | $1225 | $2439 |
BSC: Best supportive care; DOT: Duration of treatment; Fruq: Fruquintinib; PPPM: Per patient per month; Rego: Regorafenib; T/T: Trifluridine/tipiracil; T/T + bev: Trifluridine/tipiracil + bevacizumab.
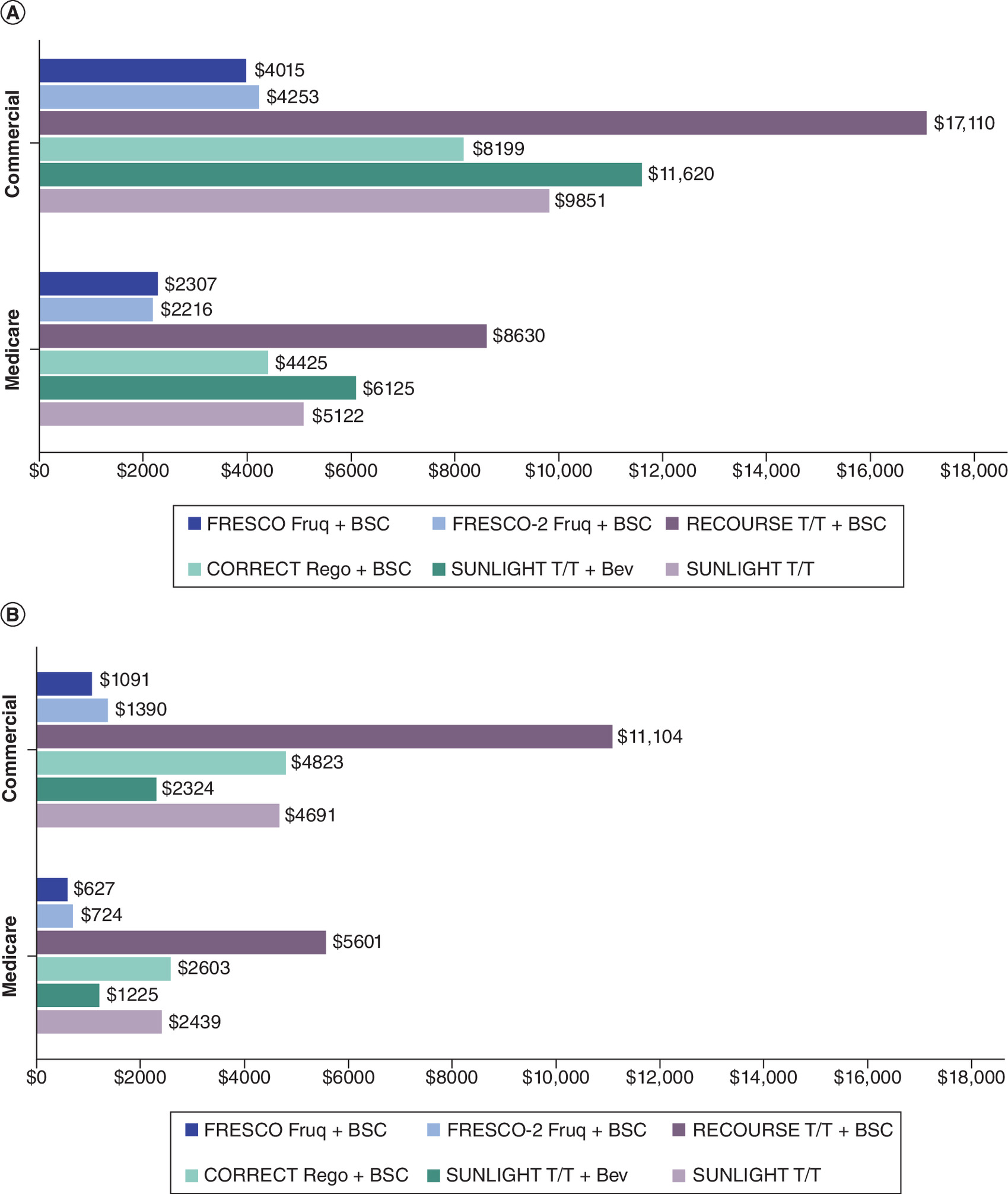
Figure 2. Commercial and Medicare per-patient adverse event management costs and per patient per month for grade 3/4 adverse events in FRESCO, FRESCO-2, RECOURSE, CORRECT and SUNLIGHT.
(A) Per-patient over the course of treatment. (B) PPPM adjusted for median DOT.
AE: Adverse event; DOT: Duration of treatment; Fruq: Fruquintinib; PPPM: Per patient per month; Rego: Regorafenib; T/T: Trifluridine/tipiracil; T/T + bev: Trifluridine/tipiracil + bevacizumab.
These results were also consistent in anchored comparisons using placebo + BSC as a common comparator. Using the difference-in-differences method, we quantified the difference between the incremental AE management cost of fruquintinib versus the incremental AE management cost of regorafenib and of T/T in RECOURSE (Table 4). Fruquintinib had the lowest incremental cost of AE management compared with regorafenib and T/T in RECOURSE. T/T+bev was not included in this analysis due to the absence of a placebo + BSC arm in the SUNLIGHT trial. From a commercial perspective, AE cost differences for fruquintinib (FRESCO) versus the other therapies were estimated at -$1929 versus regorafenib and -$11,427 versus T/T. Using AE rates in FRESCO-2, cost differences for fruquintinib versus the other therapies were estimated at -$2257 versus regorafenib and -$11,756 versus T/T. From the Medicare perspective, cost differences for fruquintinib based on FRESCO were estimated at -$1065 versus regorafenib and -$5592 versus T/T. Against FRESCO-2 fruquintinib AEs, cost differences were -$1368 versus regorafenib and -$5896 versus T/T.
| Fruquintinib + BSC (FRESCO) | Fruquintinib + BSC (FRESCO-2) | T/T + BSC (RECOURSE) | Regorafenib + BSC (CORRECT) | |
|---|---|---|---|---|
| Difference vs placebo + BSC | ||||
| Commercial | $3788 | $3460 | $15,216 | $5717 |
| Medicare | $2170 | $1866 | $7762 | $3235 |
| Difference-in-differences (based on FRESCO for fruquintinib + BSC) | ||||
| Commercial | -$11,427 | -$1929 | ||
| Medicare | -$5592 | -$1065 | ||
| Difference-in-differences (based on FRESCO-2 for fruquintinib + BSC) | ||||
| Commercial | -$11,756 | -$2257 | ||
| Medicare | -$5896 | -$1368 | ||
AE: Adverse event; BSC: Best supportive care; T/T: Trifluridine/tipiracil.
Discussion
This study compared the US costs of grade 3/4 AE management associated with fruquintinib, regorafenib, T/T and T/T+bev, using data from pivotal clinical trials. AE management costs were estimated using AE rates observed in the treatments' clinical studies included in their US FDA Prescribing Information and the costs of AE management in the US. The results indicate that fruquintinib was associated with lower AE management costs from both a Commercial and Medicare perspective. These findings suggest that the AE profile of fruquintinib translates to a lower AE management cost burden compared with regorafenib, T/T and T/T+bev.
In the RECOURSE and SUNLIGHT studies, T/T was associated with high rates of myelosuppression, which can be severe and potentially life-threatening [18,21,22]. AE costs were higher for T/T in RECOURSE than in SUNLIGHT given higher rates of AEs for T/T in RECOURSE. This may be due to RECOURSE and SUNLIGHT being conducted and published at least 8 years apart; thus, prior to the SUNLIGHT trial clinicians had real-world experience with T/T which could have led to improved management of T/T and its associated AEs. Compared with T/T and T/T+bev, the lower overall AE costs of fruquintinib are mainly attributable to the lower rate of hematological AEs. No hematologic AEs of grade 3/4 were reported with fruquintinib in the FRESCO or FRESCO-2 studies [26,27]. Targeted inhibition of VEGFRs with limited off-target activity with fruquintinib has demonstrated a well-tolerated safety profile characterized by manageable AEs [26,38]: in clinical trials, fruquintinib treatment was associated with low rates of grade ≥3 AEs for hepatotoxicity, myelosuppression, gastrointestinal hemorrhage or perforation, or neutropenia, compared with higher rates for treatment with regorafenib, T/T and T/T+bev [21–23].
DOT to calculate the PPPM AE costs was based on the reported median treatment duration for every treatment and BSC in each trial [17,18,23,26,38]. This was because only the median was reported for all the treatments and the mean treatment duration was not reported for T/T and T/T+bev in the SUNLIGHT trial. The reported mean DOT in months were: 4.93 and 4.04 for fruquintinib in FRESCO and FRESCO-2, respectively [26,38]; 2.80 for regorafenib in CORRECT [17]; and 2.92 for T/T in RECOURSE [18]. Using the mean DOT to adjust the per-patient AE costs, the PPPM AE costs remained lower for fruquintinib versus regorafenib and T/T from the commercial and Medicare perspectives. From the commercial perspective, PPPM AE costs, adjusted for mean DOT were $814 and $1053 for fruquintinib based on FRESCO and FRESCO-2, respectively, $2928 for regorafenib and $5858 for T/T based on RECOURSE. From the Medicare perspective, PPPM AE costs adjusted for mean DOT were $468 and $548 for fruquintinib based on FRESCO and FRESCO-2, respectively, $1580 for regorafenib and $2955 for T/T based on RECOURSE.
The anchored comparisons on AE costs used a difference-in-differences approach with placebo + BSC as a common reference group. FRESCO, FRESCO-2, RECOURSE and CORRECT used placebo + BSC as the control arm which was typically defined in the protocol as care required to manage symptoms such as pain, infection, and/or gastrointestinal events (Table 1) [17,18,26,38]. Based on the definitions of supportive care in the trial protocols, there was no information to indicate that BSC differed substantially across trials supporting the anchored comparisons of this study.
Limitations
With the exception of laboratory abnormalities, AE management costs were estimated based on inpatient costs for grade 3 and 4 AEs. It should be noted that costs associated with grade 3 or 4 AEs which occurred at an incidence of <5%, costs associated with grade 1 or 2 AEs, and costs incurred in outpatient settings were not considered in the AE cost estimation. However, this approach is supported by the fact that inpatient costs are the main driver of AE management and that grade 3/4 AEs commonly require treatments/procedures in the inpatient setting.
Additionally, this study evaluated the AE burden of treatments based on the AE rates reported in randomized clinical trials. Cross-trial comparisons may be potentially confounded by different trial designs and the nuances of the various study populations. In particular, FRESCO-2 was conducted during the global COVID-19 pandemic, and had a more heavily pretreated population relative to the other trials included in this study [17,18,26,38]. Furthermore, patient characteristics and AEs reported in clinical trials may differ from real-world clinical practice, which may limit the generalizability of this study. As real-world use of fruquintinib develops, these analyses should be revisited in the future to confirm the findings.
Conclusion
This study was conducted to better understand the relative safety profiles and AE-related cost burden associated with systemic therapies approved for the treatment of mCRC previously treated with fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy, an anti-VEGF biological therapy and if RAS wild-type, an anti-EGFR therapy. This study demonstrates that fruquintinib has a lower costs associated with the management of grade 3/4 AEs versus regorafenib, T/T and T/T+bev for the treatment of mCRC previously treated with fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy, an anti-VEGF therapy and if RAS wild-type, an anti-EGFR therapy in the US, both from a commercial and Medicare perspective. The observed AE management cost benefits for fruquintinib are driven by the lower rates of grade 3/4 AEs compared with regorafenib, T/T and T/T+bev. A key cost-driver is the management of grade 3/4 hematologic AEs, which had the highest reported rates with T/T and T/T+bev compared with regorafenib or fruquintinib. Fruquintinib had no reported grade 3/4 hematologic AEs in FRESCO or FRESCO-2. The cost implications of AEs associated with different treatments should be considered during treatment selection and formulary decision-making.
Summary points
•
Systemic therapies such as fruquintinib, regorafenib, trifluridine/tipiracil (T/T) and trifluridine/tipiracil+bevacizumab (T/T+bev) have demonstrated survival benefits versus best supportive care (BSC) in patients with metastatic colorectal cancer (mCRC) previously treated with at least two prior lines of systemic therapy, but there is limited evidence on their relative safety profiles and adverse event (AE)-related cost burden.
•
A cost-consequence model was developed to calculate the per-patient and per-patient-per-month (PPPM) AE costs using rates of grade 3/4 AEs with incidence ≥5% in clinical trials, the corresponding costs of AE management and the duration of each treatment.
•
The estimated management costs of grade 3/4 AEs of fruquintinib were lower compared with regorafenib, T/T and TT+bev, when considering costs either per-patient over the course of treatment or PPPM adjusted for median DOT.
•
These findings were consistent across the commercial and Medicare perspectives.
•
These results were also consistent in anchored comparisons using placebo + BSC as a common comparator with fruquintinib having the lowest incremental cost of AE management over placebo + BSC compared with regorafenib and T/T.
•
The observed AE management cost benefits for fruquintinib are driven by the lower rates of grade 3/4 AEs compared with regorafenib, T/T and T/T+bev.
•
A key cost-driver is the management of grade 3/4 hematologic AEs, which had the highest reported rates with T/T and T/T+bev compared with regorafenib or fruquintinib.
•
The cost implications of AEs associated with different treatments should be considered during treatment selection and formulary decision-making.
Author contributions
VF Paly and L Hernandez made substantial contributions to the conception and design of the work, as well as data analysis. All authors made substantial contributions to the interpretation of the data for the work. All authors also had final approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
Some of the findings of this study were presented in a poster format at the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) 2023 Europe scientific conference held 12–15 November 2023 (https://www.ispor.org/conferences-education/conferences/upcoming-conferences/ispor-europe-2023) and at the Academy of Managed Care Pharmacy (AMCP) 2024 conference to be held 15–18 April 2024 (https://amcpannual.org/about/about-amcp-2024).
Financial disclosure
This study was funded by Takeda Pharmaceuticals America, Inc., Lexington, MA, USA. VF Paly, T Padukkavidana and L Hernandez are employees of and own stock of Takeda. A Dasari reports advisory council or committee positions for HutchMed, Illumina, Personalis, Takeda and Sirtex as well as grants or funds from HutchMed, Guardant, Natera, Eisai and Enterome. J Hubbard has been on the advisory council or committee for Bayer and Taiho. T Bekaii-Saab reports research funding (to institution) from Agios, Arys, Arcus, Atreca, Boston Biomedical, Bayer, Eisai, Celgene, Lilly, Ipsen, Clovis, Seattle Genetics, Genentech, Novartis, Mirati, Merus, Abgenomics, Incyte, Pfizer and BMS; consulting (to institution) from Servier, Ipsen, Arcus, Pfizer, Seattle Genetics, Bayer, Genentech, Incyte, Eisai, Merus, Merck KGaA and Merck; consulting (to self) from Stemline, AbbVie, Blueprint Medicines, Boehringer Ingelheim, Janssen, Daiichi Sankyo, Natera, TreosBio, Celularity, Caladrius Biosciences, Exact Science, Sobi, Beigene, Kanaph, Astra Zeneca, Deciphera, Zai Labs, Exelixis, MJH Life Sciences, Aptitude Health, Illumina, Foundation Medicine, Sanofi, Glaxo SmithKline and Xilio; IDMC/DSMB with The Valley Hospital, Fibrogen, Suzhou Kintor, Astra Zeneca, Exelixis, Merck/Eisai, PanCan and 1Globe; scientific advisory board positions with Imugene, Immuneering, Xilis, Replimune, Artiva and Sun Biopharma; as well as the following inventions/patents: WO/2018/183488: Human PD1 peptide vaccines and uses thereof – licensed to Imugene, WO/2019/055687: Methods and compositions for the treatment of cancer cachexia – licensed to Recursion. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
The authors thank Evidera, Inc. for their review and editorial support on the manuscript. The authors also thank L Masten of Evidera, Inc. for her review and editorial support on the manuscript, which was funded by Takeda Pharmaceuticals America, Inc., Lexington, MA, USA. Editorial support for the development of this manuscript, under the direction of the authors, was also provided by C Jones of Ashfield MedComms, an Inizio Company, funded by Takeda Pharmaceuticals USA, Inc., Lexington, MA and complied with the Good Publication Practice (GPP) guidelines.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 87.52 KB
References
Papers of special note have been highlighted as: • of interest
1.
National Cancer Institute. Cancer Stat Facts: Common Cancer Sites. (2023). https://seer.cancer.gov/statfacts/html/common.html
2.
National Cancer Institute. Cancer Stat Facts: Colorectal Cancer. (2022). https://seer.cancer.gov/statfacts/html/colorect.html
3.
Centers for Disease Control and Prevention. Basic information about colorectal cancer. (2023). https://www.cdc.gov/cancer/colorectal/basic_info/
4.
Ciardiello F, Ciardiello D, Martini G et al. Clinical management of metastatic colorectal cancer in the era of precision medicine. CA Cancer J. Clin. 72(4), 372–401 (2022).
5.
Centers for Disease Control and Prevention. United States cancer statistics: data visualizations survival by stage. (2022). https://gis.cdc.gov/Cancer/USCS/#/SurvivalbyStage/
6.
Bekaii-Saab TS. Identifying disease progression in patients with metastatic colorectal cancer: when to initiate third-line therapy. Clin. Adv. Hematol. Oncol. 18(1 Suppl. 2), 2–7 (2020).
7.
Bekaii-Saab T, Kim R, Kim TW et al. Third- or Later-line Therapy for Metastatic Colorectal Cancer: Reviewing Best Practice. Clin Colorectal Cancer 18(1), e117–e129 (2019).
• Discusses and highlights the importance of managing adverse events to maintain quality of life as best practice for patients in third-line or later treatment of mCRC.
8.
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet 394(10207), 1467–1480 (2019).
9.
Prager G, Köhne CH, O'Connor JM et al. The Screening and COnsensus based on Practices and Evidence (SCOPE) program – results of a survey on daily practice patterns for patients with mCRC. Curr. Oncol. 28(3), 2097–2106 (2021).
10.
Sánchez-Gundín J, Fernández-Carballido AM, Martínez-Valdivieso L, Barreda-Hernández D, Torres-Suárez AI. New trends in the therapeutic approach to metastatic colorectal cancer. Int. J. Med. Sci. 15(7), 659–665 (2018).
11.
Grothey A, Marshall JL, Bekaii-Saab T. Sequencing beyond the second-line setting in metastatic colorectal cancer. Clin. Adv. Hematol. Oncol. 17 Suppl. 7(3), 1–19 (2019).
12.
Cervantes A, Adam R, Roselló S et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 34(1), 10–32 (2023).
13.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Colon Cancer. (2023). Version 4.2023.
14.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Rectal Cancer. (2023). Version 6.2023.
15.
Souglakos J, Androulakis N, Syrigos K et al. FOLFOXIRI (folinic acid, 5-fluorouracil, oxaliplatin and irinotecan) vs FOLFIRI (folinic acid, 5-fluorouracil and irinotecan) as first-line treatment in metastatic colorectal cancer (MCC): a multicentre randomised phase III trial from the Hellenic Oncology Research Group (HORG). Br. J. Cancer 94(6), 798–805 (2006).
16.
Guo Y, Xiong BH, Zhang T, Cheng Y, Ma L. XELOX vs. FOLFOX in metastatic colorectal cancer: an updated meta-analysis. Cancer Invest. 34(2), 94–104 (2016).
17.
Grothey A, Van Cutsem E, Sobrero A et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase III trial. Lancet 381(9863), 303–312 (2013).
• Global phase III trial of regorafenib versus placebo and reports relevant data on adverse event rates and duration of treatment used in this article.
18.
Mayer RJ, Van Cutsem E, Falcone A et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N. Engl. J. Med. 372(20), 1909–1919 (2015).
• Global phase III trial of trifluridine/tipriacil versus placebo and reports relevant data on adverse event rates and duration of treatment used in this article.
19.
STIVARGA (regorafenib) [package insert]. [Bayer HealthCare Pharmaceuticals Inc, Whippany, NJ (2012). https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/203085s007lbl.pdf
20.
Li J, Qin S, Xu R et al. Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): a randomised, double-blind, placebo-controlled, phase III trial. Lancet Oncol. 16(6), 619–629 (2015).
21.
European Medicines Agency. Lonsurf: summary of product characteristics. (2023). https://www.ema.europa.eu/en/documents/product-information/lonsurf-epar-product-information_en.pdf
22.
LONSURF (trifluridine and tipiracil) [package insert]. [Taiho Pharmaceutical Co Ltd, Princeton, NJ (September 22, 2023). https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/207981s012lbl.pdf
23.
Prager GW, Taieb J, Fakih M et al. Trifluridine-Tipiracil and Bevacizumab in Refractory Metastatic Colorectal Cancer. N. Engl. J. Med. 388(18), 1657–1667 (2023).
• Global phase III trial of trifluridine/tirpiracil+bevacizumab versus trifluridine/tirpiracil monotherapy and reports relevant data on adverse event rates and duration of treatment used in this article.
24.
AVASTIN (bevacizumab) [package insert]. [Genentech, Inc, San Fransisco, CA (2004). https://www.gene.com/download/pdf/avastin_prescribing.pdf
25.
FRUZAQLA (fruquintinib) [Package insert]. [Takeda Pharmaceuticals America, Inc, Lexington, MA (2023). https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217564s000lbl.pdf
26.
Li J, Qin S, Xu RH et al. Effect of Fruquintinib vs Placebo on Overall Survival in Patients With Previously Treated Metastatic Colorectal Cancer: The FRESCO Randomized Clinical Trial. JAMA 319(24), 2486–2496 (2018).
• Phase III trial of fruquintinib versus placebo conducted in China and reports relevant data on adverse event rates and duration of treatment used in this article.
27.
Dasari A, Sobrero A, Yao J et al. FRESCO-2: a global phase III study investigating the efficacy and safety of fruquintinib in metastatic colorectal cancer. Future Oncol. 17(24), 3151–3162 (2021).
28.
Howe A, Hernandez LG, Paly VF et al. Treatment exposure-adjusted event rates (EAERs) for grade 3/4 AEs associated with emerging and existing systemic therapies for mCRC with at least 2 prior lines of therapy: informing payer and pathway formulary decision making. Value Health 26(11), S2 (2023).
29.
Li J, Guo W, Bai Y et al. Safety profile and adverse events of special interest for fruquintinib in Chinese Patients with previously treated metastatic colorectal cancer: analysis of the phase III FRESCO trial. Adv. Ther. 37(11), 4585–4598 (2020).
30.
Qin S, Xu RH, Shen L et al. Subgroup analysis by liver metastasis in the Fresco trial comparing fruquintinib versus placebo plus best supportive care in chinese patients with metastatic colorectal cancer. Onco. Targets Ther. 14, 4439–4450 (2021).
31.
Xu R, Qin S, Guo W et al. Subgroup analysis by prior anti-VEGF or anti-EGFR target therapy in FRESCO, a randomized, double-blind, phase III trial. Future Oncol. 17(11), 1339–1350 (2021).
32.
Dasari NA, Lonardi S, Garcia-Carbonero R et al. LBA25 FRESCO-2: a global phase III multiregional clinical trial (MRCT) evaluating the efficacy and safety of fruquintinib in patients with refractory metastatic colorectal cancer. Ann. Oncol. 33, S1391–S1392 (2022).
33.
Longo-Muñoz F, Argiles G, Tabernero J et al. Efficacy of trifluridine and tipiracil (TAS-102) versus placebo, with supportive care, in a randomized, controlled trial of patients with metastatic colorectal cancer from Spain: results of a subgroup analysis of the phase III RECOURSE trial. Clin. Transl. Oncol. 19(2), 227–235 (2017).
34.
Tabernero J, Argiles G, Sobrero AF et al. Effect of trifluridine/tipiracil in patients treated in RECOURSE by prognostic factors at baseline: an exploratory analysis. ESMO Open 5(4), e000752 (2020).
35.
Van Cutsem E, Mayer RJ, Laurent S et al. The subgroups of the phase III RECOURSE trial of trifluridine/tipiracil (TAS-102) versus placebo with best supportive care in patients with metastatic colorectal cancer. Eur. J. Cancer 90, 63–72 (2018).
36.
Yoshino T, Cleary JM, Van Cutsem E et al. Neutropenia and survival outcomes in metastatic colorectal cancer patients treated with trifluridine/tipiracil in the RECOURSE and J003 trials. Ann. Oncol. 31(1), 88–95 (2020).
37.
Tabernero J, Prager GW, Fakih M et al. Trifluridine/tipiracil plus bevacizumab for third-line treatment of refractory metastatic colorectal cancer: the phase III randomized SUNLIGHT study. J. Clin. Oncol. 41(Suppl. 4), 4–4 (2023).
38.
Dasari A, Lonardi S, Garcia-Carbonero R et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): an international, multicentre, randomised, double-blind, phase III study. Lancet 402(10395), 41–53 (2023).
• Global phase III trial of fruquintinib versus placebo and reports relevant data on adverse event rates and duration of treatment used in this article.
39.
US Centers for Medicare & Medicaid Services. FY 2023 IPPS Final Rule Home Page. (2023). https://www.cms.gov/medicare/payment/prospective-payment-systems/acute-inpatient-pps/fy-2023-ipps-final-rule-home-page
40.
Agency for Healthcare Research and Quality. Clinical Classifications Software Refined (CCSR) for ICD-10-CM Diagnoses. Healthcare Cost and Utilization Project (HCUP). (2022). http://www.hcup-us.ahrq.gov/toolssoftware/ccsr/dxccsr.jsp
41.
Bureau of Labor Statistics UDoL. Consumer Price Index. (2023). https://www.bls.gov/news.release/archives/cpi_01182017.pdf
42.
Centers for Medicare and Medicaid Services. Medicare Physician Fee Schedule Look-Up Tool: 2023 National Payment Amount by HCPCS Code. (2023). https://www.cms.gov/medicare/physician-fee-schedule/search/overview
43.
Practice Management Information Corporation. Medical Fees Directory 2023 - eBook. Usual, Customary and Reasonable (UCR) Fees. (2023).
Information & Authors
Information
Published In
Copyright
© 2024 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 May 2024
Accepted: 19 June 2024
Published online: 8 July 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Adverse event costs of systemic therapies for metastatic colorectal cancer previously treated with fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy and biologics in the US. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0084
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Per Pfeiffer, Chiara Cremolini, Michel Ducreux, Pia Osterlund, Sarah Ronnebaum, Morodoluwa Akin-Fajiye, Victoria Paly, Luis Hernandez, Elena Elez, Survival benefit of oral systemic monotherapy in previously treated metastatic colorectal cancer: a meta-analysis, The Oncologist, 10.1093/oncolo/oyag175, 31, 7, (2026).
- Ana Fernández, Beatriz González Astorga, Nuria Rodríguez, María José Safont, Paula Castro Albarrán, María Mareque, Itziar Oyagüez, A Cost Analysis of Adverse Event Management of Systemic Therapies for Metastatic Colorectal Cancer on Patients with at Least Two Previous Lines of Treatment in Spain, ClinicoEconomics and Outcomes Research, 10.2147/CEOR.S586388, Volume 18, (1-13), (2026).
- Christopher Cann, Sophia Zhao, Nadeem Khan, Malinda O’Donnell, Melina Taylor, Tehseen Salimi, Third-line treatment decision-making for metastatic colorectal cancer: a cross-sectional survey of US community physicians, The Oncologist, 10.1093/oncolo/oyag018, 31, 3, (2026).
- Nuoya Wang, Jiachun Hu, Lili Jin, Shuangqing Wang, Bowen Zeng, Yanhong Liu, Aihua Jin, Jianyu Piao, Liqing Chen, Wei Huang, Zhonggao Gao, Yan Wang, Wenxiang Cui, Mingji Jin, Inulin and hyaluronic acid-based oral liposome for enhanced photo-chemotherapy against orthotopic colon cancer and its reversal effects on tumor hypoxia and intestinal microbiota, International Journal of Biological Macromolecules, 10.1016/j.ijbiomac.2025.140996, 304, (140996), (2025).
- Xin Wang, Zhigang Bai, Wei Deng, Xinfeng Wang, Efficacy and safety of fruquintinib plus capecitabine as first-line treatment in patients with metastatic colorectal cancer ineligible for intravenous chemotherapy: a two-stage, single-armed, phase II study, Investigational New Drugs, 10.1007/s10637-025-01510-1, 43, 2, (214-222), (2025).