Evaluation of inpatient and emergency department healthcare resource utilization and costs pre- and post-nusinersen for the treatment of spinal muscular atrophy using United States claims
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Nusinersen, administered by intrathecal injection at a dose of 12 mg, is indicated across all ages for the treatment of spinal muscular atrophy (SMA). Evidence on real-world healthcare resource use (HRU) and costs among patients taking nusinersen remains limited. This study aimed to evaluate real-world HRU and costs associated with nusinersen use through US claims databases. Patients & methods: Using the Merative™ MarketScan® Research Databases, patients with SMA receiving nusinersen were identified from commercial (January 2017 to June 2020) and Medicaid claims (January 2017 to December 2019). Those likely to have complete information on the date of nusinersen initiation and continuous enrollment 12 months pre- and post-index (first record of nusinersen treatment) were retained. Number and costs (US$ 2020) of inpatient admissions and emergency department (ED) visits, unrelated to nusinersen administration, were evaluated for 12 months pre- and post-nusinersen initiation and stratified by age: pediatric (<18 years) and adult (≥18 years). Results: Overall, 103 individuals treated with nusinersen were retained: 59 were pediatric (mean age [range]: 9 [1–17] years), and 44 were adults (30 [18–63] years). Inpatient admissions decreased by 41% for pediatrics and 67% for adults in the 12 months post-treatment versus the 12 months pre-treatment. Average inpatient admission costs per patient for the pediatric cohort decreased by 63% ($22,903 vs $8466) and by 79% ($13,997 vs $2899) for the adult cohort when comparing the 12 months pre-index with the 12 months post-index period. Total ED visits and ED visit costs decreased by 8% and 35%, respectively, for the overall cohort over the 12-month period pre- and post-index. Conclusion: Using US claims databases, nusinersen treatment in pediatric and adult patients was associated with reductions in HRU and costs over a 12-month period post-treatment initiation relative to the pre-treatment period.
Plain language summary
What is this article about/what is the aim of the research?
Spinal muscular atrophy (SMA) is an inherited disease affecting mainly infants and children, but it can also present in adults. This condition damages nerve cells and muscles that control key activities, such as sitting, walking, speaking, swallowing and breathing. Nusinersen was the first drug approved in the US to help manage SMA. It is administered by injection with a thin needle into a space in the lower back, below the end of the spinal cord, through a medical procedure known as a “lumbar puncture”. There is very little information on the medical management for people with SMA receiving nusinersen. Using insurance claims processed in the US, this study assessed trends in hospital stays, in emergency department (ED) visits and in related medical costs before and after nusinersen use.
What were the results?
Comparing the 12 months before nusinersen treatment with the 12 months following treatment, the number of hospital stays was 41% lower for children and 67% lower for adults after treatment. The average cost per person associated with hospital stays was 63% lower for children and 79% lower for adults. The number of days spent at the hospital was also reduced for all ages following nusinersen treatment. The number of ED visits and the resulting costs were 8% and 35% lower, respectively, for the overall cohort.
What do these results mean?
Overall, nusinersen treatment lessens the burden of disease among people with SMA in the US by lowering the rate of hospital stays and ED visits, and by reducing associated costs.
Spinal muscular atrophy (SMA) is an autosomal recessive neuromuscular disease characterized by the degeneration of brain stem and spinal cord motor neurons, which is caused by mutations or deletions of the survival motor neuron 1 (SMN1) gene [1–3]. Individuals with SMA display progressive muscular atrophy and weakness, with most patients experiencing significant motor impairment and related comorbidities, including difficulties with breathing and feeding [4]. Nusinersen (SPINRAZA®) is a modified antisense oligonucleotide that was the first approved drug for all SMA types [5,6] in the United States (US) and European Union [7,8] and is indicated across all ages. Nusinersen promotes the expression of functional survival motor neuron (SMN) protein from the paralogous SMN2 gene, which produces mostly truncated, inactive SMN protein [9,10], and has improved survival and motor function in patients of all ages and SMA types across multiple clinical trials and real-world studies [9,11–21]. Administration of nusinersen (12 mg) is by intrathecal injection, including four loading doses followed by maintenance dosing every 4 months [7,8].
The economic burden of SMA has been shown to be substantial. It is characterized by high healthcare costs and increased healthcare resource use (HRU) across the SMA patient population and is greatest among those with early-onset and severe disease [22–26]. The improvement of patient health outcomes associated with nusinersen treatment can be reflected in a lower overall burden on the healthcare system. A study using US administrative claims data from 23 December 2016 to 31 August 2018 showed that patients with SMA aged <2 years treated with nusinersen had fewer inpatient stays and lower inpatient costs when compared with similarly aged untreated patients with SMA; however, this study had a very limited median follow-up time of 7.6 months and only evaluated those patients <2 years of age [25]. Studies conducted outside the US have begun to demonstrate that nusinersen is associated with reductions in HRU and, consequently, financial burden over a longer time period; for example, fewer inpatient admissions between the first and second year of treatment among patients with infantile-onset SMA [27,28]. However, limited longitudinal evidence exists on real-world HRU and cost outcomes among patients of all ages receiving nusinersen treatment, especially in the US. The objective of this study was to evaluate real-world HRU and cost patterns pre- and post-nusinersen initiation through US claims databases using a retrospective study design to determine the economic impact of nusinersen treatment across all ages.
Patients & methods
Study design & data source
This retrospective cohort research study used administrative claims data from Merative™ MarketScan® Research Databases, formerly owned by IBM® (hereafter identified as MarketScan®). Data from MarketScan® represent de-identified, longitudinal, patient-level claims comprising more than 273 million unique patients [29].
Study period & cohort selection
Patients with SMA initiating nusinersen were identified from MarketScan® during the period from 1 January 2017 to 30 June 2019 for commercial insurance claims and from 1 January 2017 to 31 December 2018 for Medicaid claims. Patients with one or more codes for nusinersen treatment during the study period were identified using Healthcare Common Procedure Coding System codes (C9489 and J2326) and National Drug Codes (64406-0058-01, 64406-058-01). Patients were additionally required to have one or more International Classification of Diseases, 10th Revision (ICD-10) diagnosis codes for SMA (G12.0, G12.1, G12.8, G12.9) during the same period. Patients in the MarketScan® database were additionally required to have at least 12 months of continuous enrollment pre- and post-index (first record of nusinersen treatment). As a result, the entire study period included data from 1 January 2016 to 30 June 2020 for commercial insurance claims and 1 January 2016 to 31 December 2019 for Medicaid claims to allow for 12 months pre- and 12 months post-evaluation of nusinersen use. The first record of nusinersen use indicated the index date. Nusinersen index dates were limited to 1 January 2017 through 30 June 2019 (commercial) and 1 January 2017 through 31 December 2018 (Medicaid) (Figure 1A).
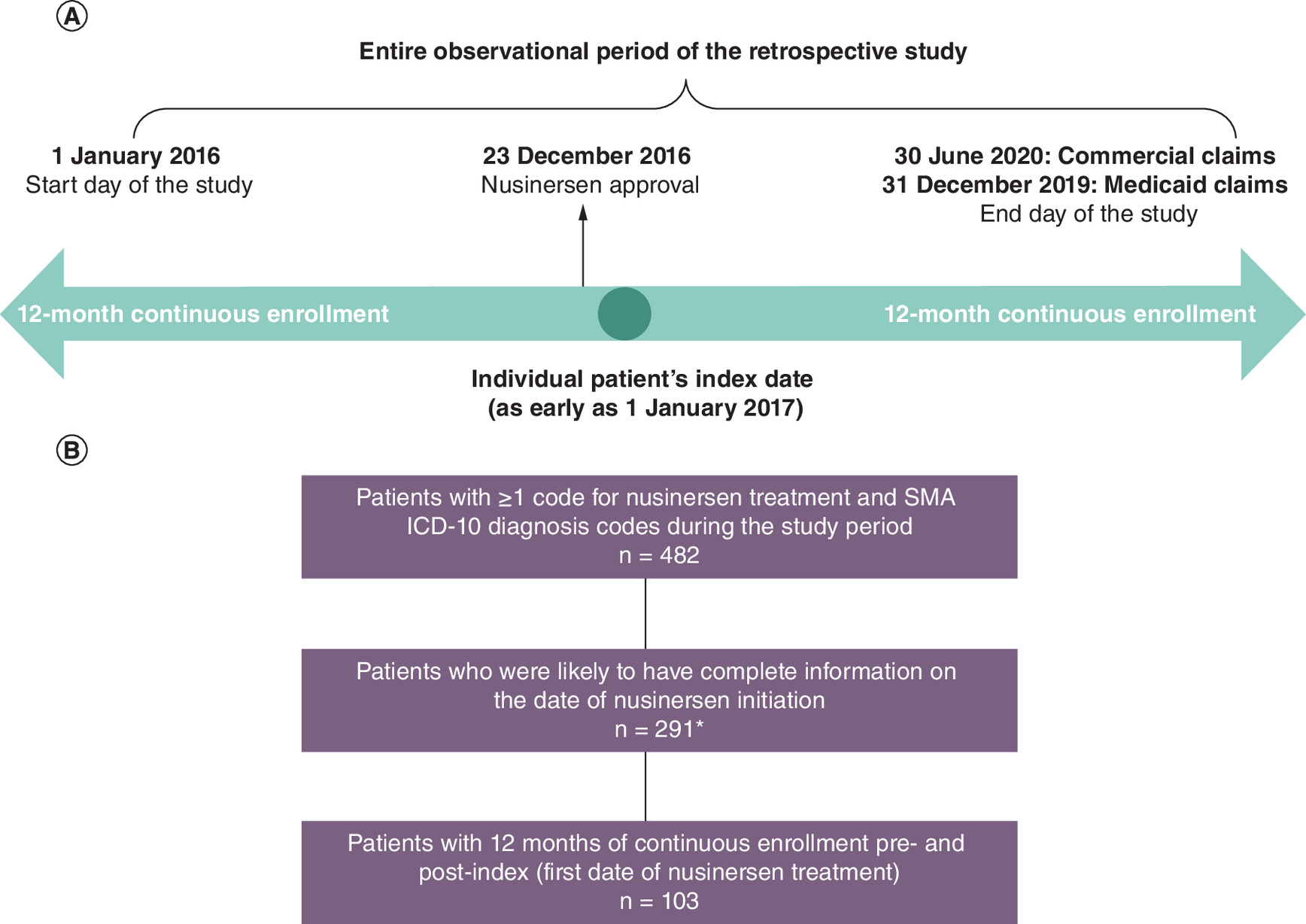
Figure 1. Study design and patient selection using Merative MarketScan® data.
(A) Study design. (B) Patient selection.
The retrospective study started on 1 January 2016 to allow for the analysis of 12-month pre-treatment period before nusinersen was approved on 23 December 2016. The index date is the first date of nusinersen treatment.
*Patients who received any of the first four recorded nusinersen doses in intervals of 120 days or greater (which would indicate maintenance doses and not loading doses per US label) were excluded. Patients with ≤4 doses were retained, as long as the inter-dose intervals for each of the first four recorded doses were within 120 days, respectively.
ICD-10: International Classification of Diseases, 10th Revision; SMA: Spinal muscular atrophy.
To compare HRU and cost 12 months before and after nusinersen initiation, patients who were likely to have complete information on the date of treatment initiation in the MarketScan® database (i.e., incident users or those newly treated with nusinersen) were selected. As described previously [30], to exclude patients with incomplete dosing history in administrative claims from the study cohort, patients who received any of the first four recorded doses in the databases with an inter-dose interval of 120 days or greater (i.e., an interval indicating a potential maintenance dose, not a potential loading dose per US label) were removed. No exclusion was made based on the total duration of an individual's loading dose phase or the total number of doses received. Patients with four or fewer doses were retained as long as the inter-dose intervals for each of the first four recorded doses were within 120 days.
As this study design included pre- and post-nusinersen data, patients who met the inclusion criteria served as their own controls. Infants with SMA that were 0–1 year of age and those identified via newborn screening were excluded from the analysis as they did not meet the 12-month pre-continuous enrollment requirement. Institutional review board oversight was not required for this study because the data utilized from both databases were de-identified.
Study variables & data analysis
Baseline patient demographics were summarized, including age, sex, region, race/ethnic group and percentage of patients selected in each claims database (e.g., commercial or Medicaid). Data for region were only available for patients identified in commercial claims, while data for race were only available for those identified in Medicaid claims.
The total number and costs (US$ 2020) of inpatient admissions, the length of stay for inpatient admissions, and the number and costs (US$ 2020) of emergency department (ED) visits were evaluated over 12 months pre- and post-nusinersen initiation (first record of nusinersen treatment). Mean values with standard deviation (SD) were also calculated at the patient level (e.g., mean number of admissions or costs per patient). Inpatient admissions and ED visits that were specific for nusinersen administration were excluded to focus on the HRU and costs related to the general medical management of patients with SMA. The percentage of patients who had ≥1 inpatient admission or ED visit was also reported, including the percentage with documented common comorbidities related to SMA disease: respiratory problems, gastrointestinal complications, musculoskeletal problems, scoliosis surgery and SMA diagnosis [31].
Total inpatient admission costs reflected services provided throughout the hospital stay. Of the total inpatient admission costs, those classified as respiratory costs included costs related to pneumonia, ventilation support and other respiratory illness, symptoms, or insufficiencies [31]. Because of the small number of patients with SMA, and that a majority of patients did not experience inpatient admissions or ED visits during the study period, descriptive analyses were presented for HRU and costs without statistical testing. Results were age-stratified as either pediatric (<18 years old) or adult (≥18 years old) based on age at index.
Additional analyses
A sensitivity analysis was conducted to compare the baseline characteristics of patients excluded based on the cohort selection criteria (patients with ≥1 code for nusinersen treatment and SMA ICD-10 diagnosis codes during the study period, those likely to have complete information on the index date, and those with 12 months of continuous enrollment pre- and post-index) with those being included in the final study cohort. The percentage of patients who transitioned from an ED visit to an inpatient admission within 10 days was also explored and reported as an additional analysis.
Results
Baseline demographics
Based on the inclusion criteria, 103 patients treated with nusinersen were included in the study (Figure 1B). Of the 103 patients retained, 59 were pediatric (including 50.9% female) and 44 were adult (including 31.8% female) (Table 1). The mean (range) age at nusinersen index date was 18 (1–63) years overall, 9 (1–17) years in the pediatric group and 30 (18–63) years in adults. Of the study sample, 18.5% were from the Northeast, 12.6% were from North central, 13.6% were from South, 12.6% were from West and 42.7% were unknown since data for region were only available for patients identified in the commercial database. Among the study sample, 30.1% were classified as White, 3.9% Black, 2.9% Hispanic and 63.1% were other/unknown, as data for race/ethnicity were only available for those identified in the Medicaid claims. Similar percentages were observed across the age cohorts for region and race/ethnicity, with the exception that more adults were from the South and fewer were from North central. In the MarketScan® database, 57.3% patients were identified from the commercial database and 42.7% patients were from the Medicaid database (Table 1).
| Total (n = 103) | Pediatric (<18 years) (n = 59) | Adult (≥18 years) (n = 44) | |
|---|---|---|---|
| Percentage of total study population | 100% | 57% | 43% |
| Mean age (range) at index date of nusinersen, years | 18 (1–63) | 9 (1–17) | 30 (18–63) |
| Female, n (%) | 44 (42.7%) | 30 (50.9%) | 14 (31.8%) |
| US region, n (%)† | |||
| Northeast | 19 (18.5%) | 11 (18.6%) | 8 (18.2%) |
| North central | 13 (12.6%) | 10 (17.0%) | 3 (6.9%) |
| South | 14 (13.6%) | 4 (6.8%) | 10 (22.7%) |
| West | 13 (12.6%) | 7 (11.9%) | 6 (13.6%) |
| Other/unknown | 44 (42.7%) | 27 (45.8%) | 17 (38.6%) |
| Race/ethnic group, n (%)† | |||
| White | 31 (30.1%) | 19 (32.2%) | 12 (27.3%) |
| Black | 4 (3.9%) | 3 (5.1%) | 1 (2.3%) |
| Hispanic | 3 (2.9%) | 2 (3.4%) | 1 (2.3%) |
| Other/unknown | 65 (63.1%) | 35 (59.3%) | 30 (68.2%) |
| Database, n (%) | |||
| Commercial | 59 (57.3%) | 32 (54.2%) | 27 (61.4%) |
| Medicaid | 44 (42.7%) | 27 (45.8%) | 17 (38.6%) |
†
Data for region were only available for patients in the commercial claims dataset, whereas data for race were only available for those in the Medicaid claims dataset.
Inpatient admissions & days spent in inpatient admissions
Of 103 patients treated with nusinersen, 25 (24.3%) had an inpatient admission during the 12 months pre-index, with 17 (28.8%) in the pediatric group and eight (18.2%) in the adult group. During the 12 months post-index, 19 (18.4%) patients had inpatient admissions, with 15 (25.4%) in the pediatric group and four (9.1%) in the adult group (Table 2). The percentage of patients with inpatient admissions decreased post-index, with corresponding reductions seen in inpatient admissions related to SMA or its common comorbidities (Table 2). The total number of inpatient admissions was reduced in the overall study cohort by 47%, from 49 during the 12 months pre-index to 26 during the 12 months post-index. In pediatric patients, the total number of inpatient admissions was reduced by 41%, from 37 pre-index to 22 post-index, and was reduced by 67% from 12 to four in adults (Figure 2A). Among all patients, the total length of stay for inpatient admissions was reduced by 11% from 318 days pre-index to 282 days post-index (by 10% from 229 days to 205 days in pediatric patients and by 13% from 89 days to 77 days in adult patients) (Figure 2B). The mean (SD) number of inpatient admissions and days spent in inpatient admissions per patient was reduced for all ages (Supplementary Figure 1).
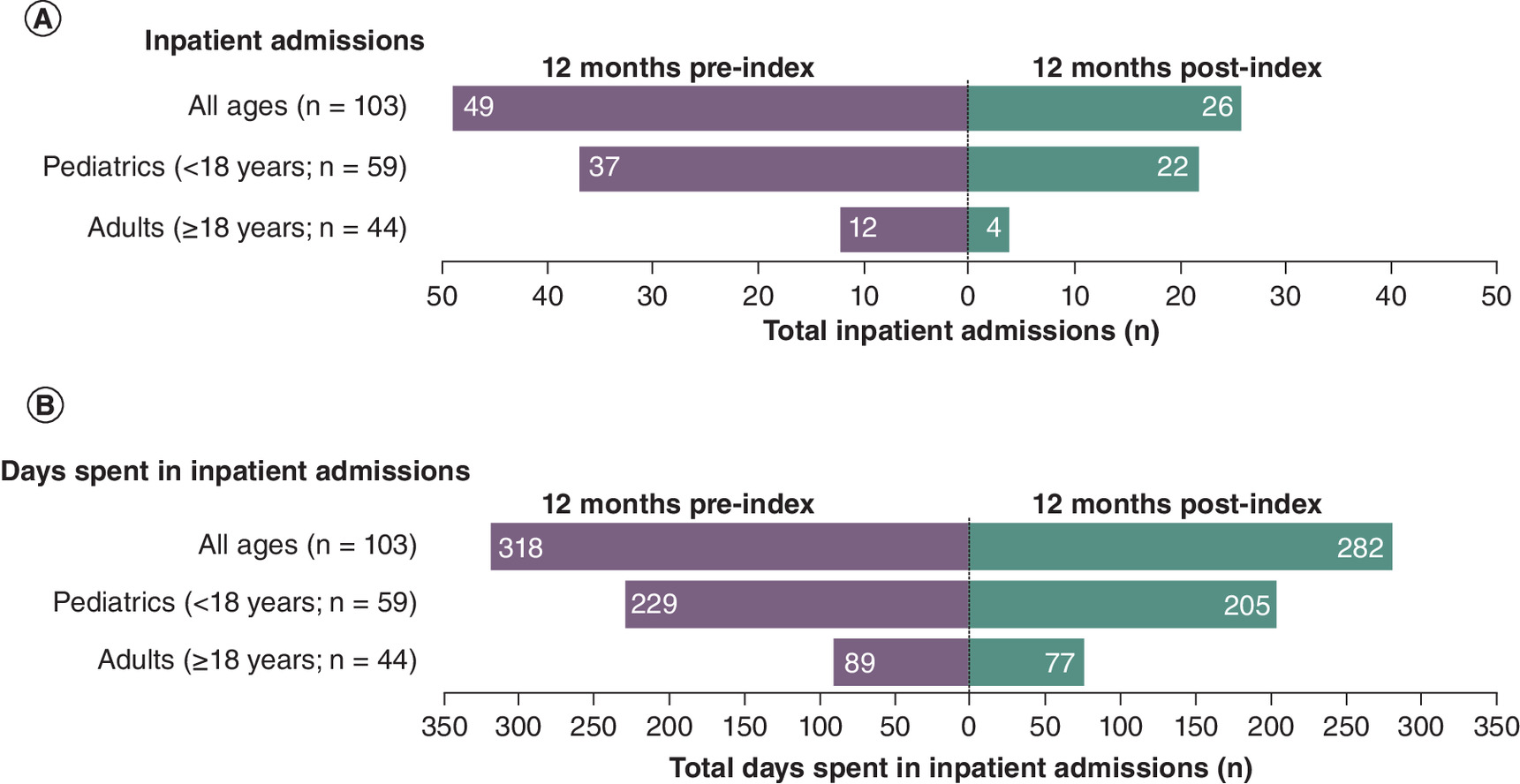
Figure 2. Total number of inpatient admissions and days spent in hospital in individuals with SMA in the 12 months before and after nusinersen treatment.
(A) Inpatient admissions. (B) Days spent in inpatient admissions.
SMA: Spinal muscular atrophy.
| Total (n = 103) | Pediatric (<18 years) (n = 59) | Adult (≥18 years) (n = 44) | ||||
|---|---|---|---|---|---|---|
| 12 months pre-index | 12 months post-index | 12 months pre-index | 12 months post-index | 12 months pre-index | 12 months post-index | |
| Patients with ≥1 inpatient admission, n (%) | 25 (24.3) | 19 (18.4) | 17 (28.8) | 15 (25.4) | 8 (18.2) | 4 (9.1) |
| Respiratory problems | 19 (18.4) | 16 (15.5) | 14 (23.7) | 14 (23.7) | 5 (11.4) | 2 (4.5) |
| Gastrointestinal complications | 1 (1.0) | 1 (1.0) | 1 (1.7) | 1 (1.7) | 0 (0.0) | 0 (0.0) |
| Musculoskeletal problems | 5 (4.9) | 1 (1.0) | 3 (5.1) | 1 (1.7) | 2 (4.5) | 0 (0.0) |
| Orthopedic (scoliosis) surgery | 4 (3.9) | 1 (1.0) | 3 (5.1) | 1 (1.7) | 1 (2.3) | 0 (0.0) |
| SMA diagnosis | 11 (10.7) | 3 (2.9) | 6 (10.2) | 3 (5.1) | 5 (11.4) | 0 (0.0) |
| Patients with ≥1 ED visits, n (%) | 41 (39.8) | 43 (41.7) | 29 (49.2) | 26 (44.1) | 12 (27.3) | 17 (38.6) |
| Respiratory problems | 24 (23.3) | 21 (20.4) | 19 (32.2) | 16 (27.1) | 5 (11.4) | 5 (11.4) |
| Gastrointestinal complications | 5 (4.9) | 3 (2.9) | 3 (5.1) | 1 (1.7) | 2 (4.5) | 2 (4.5) |
| Musculoskeletal problems | 4 (3.9) | 6 (5.8) | 4 (6.8) | 3 (5.1) | 0 (0.0) | 3 (6.8) |
| Orthopedic (scoliosis) surgery | 1 (1.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.3) | 0 (0.0) |
| SMA diagnosis | 4 (3.9) | 3 (2.9) | 4 (6.8) | 3 (5.1) | 0 (0.0) | 0 (0.0) |
ED: Emergency department; SMA: Spinal muscular atrophy.
Inpatient admission costs
The total costs of inpatient admissions decreased in patients of all ages by 68% from 12 months pre-index to 12 months post-index, from $1,967,121 to $627,063, with a 45% decrease in respiratory-related costs from $746,248 to $409,043. In pediatric patients, the total costs of inpatient admissions decreased by 63% from $1,351,259 pre-index to $499,506 post-index, with a 42% decrease in respiratory-related costs from $690,538 to $399,457. In adult patients, the total costs of inpatient admissions decreased pre- to post-index by 79% from $615,862 to $127,557, with an 83% decrease in respiratory-related costs from $55,710 to $9587 (Figure 3A).
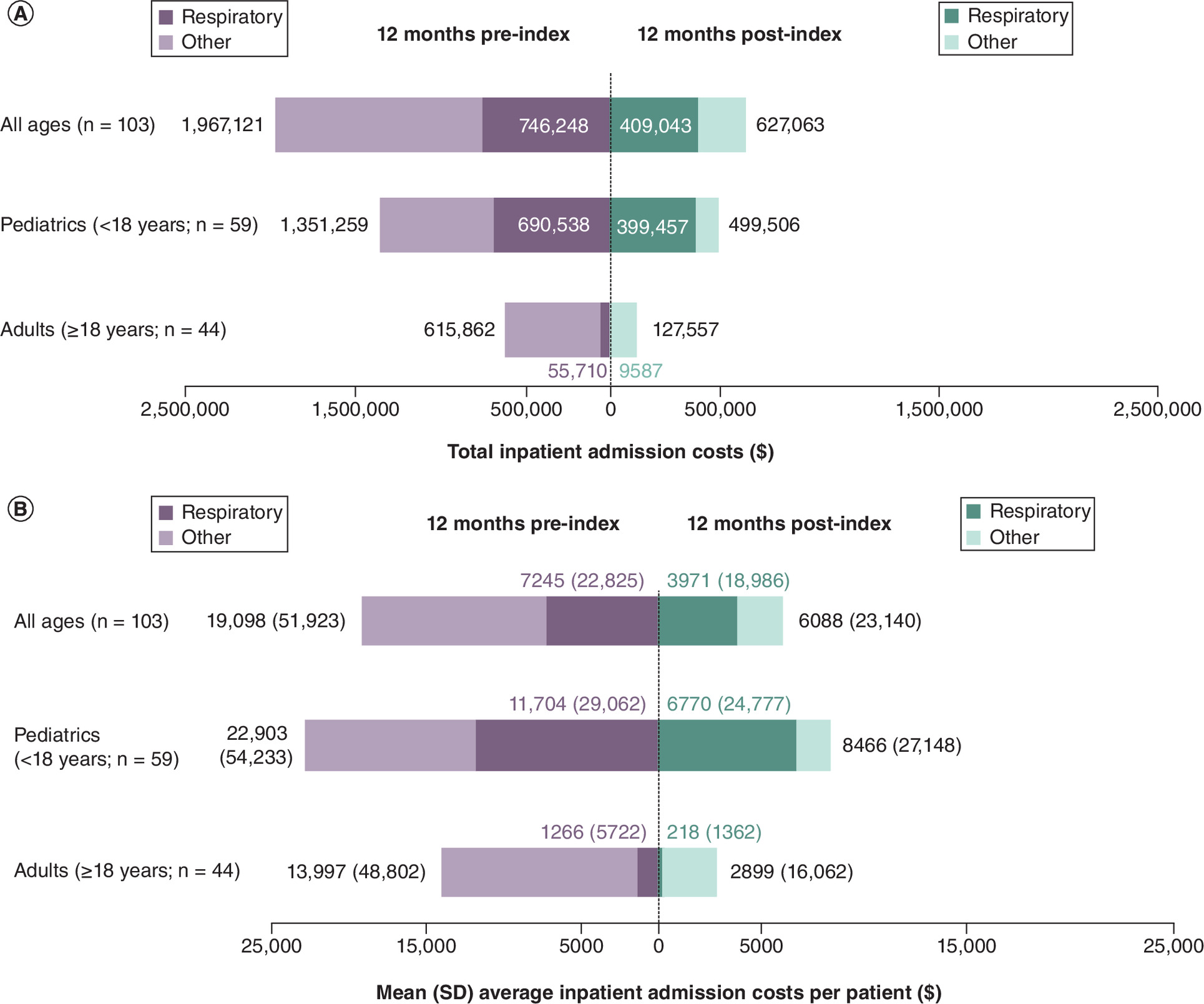
Figure 3. Total and average costs of inpatient admissions in individuals with spinal muscular atrophy in the 12 months before and after nusinersen treatment.
(A) *Total costs. (B) **Average costs.
*No SDs were available for total costs. Total overall costs shown at end of bars were reflective of services charged through hospital stay; respiratory-related referred to pneumonia, ventilation support and other respiratory illness, symptom or insufficiency.
**Cost values presented at the end of the bars represent average overall costs.
SD: Standard deviation; SMA: Spinal muscular atrophy.
The mean (SD) inpatient admission costs per patient were also reduced from 12 months pre-index to 12 months post-index in patients of all ages by 68% from $19,098 ($51,923) to $6088 ($23,140), with a 45% decrease in mean (SD) respiratory-related costs from $7245 ($22,825) to $3971 ($18,986). In pediatric patients, the mean (SD) inpatient admission costs per patient were reduced from pre- to post-index by 63% from $22,903 ($54,233) to $8466 ($27,146), with a 42% decrease in mean (SD) respiratory-related costs from $11,704 ($29,062) to $6770 ($24,777). In adult patients, the mean (SD) inpatient admission costs per patient were reduced from pre- to post-index by 79% from $13,997 ($48,802) to $2899 ($16,062), with an 83% decrease in mean (SD) respiratory-related costs from $1266 ($5722) to $218 ($1362) (Figure 3B).
ED visits & costs
Of the 103 patients identified, 41 (39.8%) had at least one ED visit in the 12 months pre-index (29 or 49.2% of patients in the pediatric group; 12 or 27.3% in the adult group) versus 43 (41.7%) in the 12 months post-index (26 or 44.1% patients in the pediatric group; 17 or 38.6% in the adult group) (Table 2). The total number of ED visits was reduced by 8% in the overall group from 92 pre-index to 85 post-index (by 21% in the pediatric group from 73 pre-index to 58 post-index) (Figure 4A), with the mean (SD) number of ED visits per patient following this trend (Supplementary Figure 2A). The total number of ED visits in the adult group increased by 47% from 19 pre-index to 28 post-index. The increase in ED visits post-index in the adult cohort was likely largely due to reasons not related to SMA; the percentage of patients with ED visits related to SMA or its common comorbidities were low and only increased slightly for musculoskeletal problems post-index (Table 2).
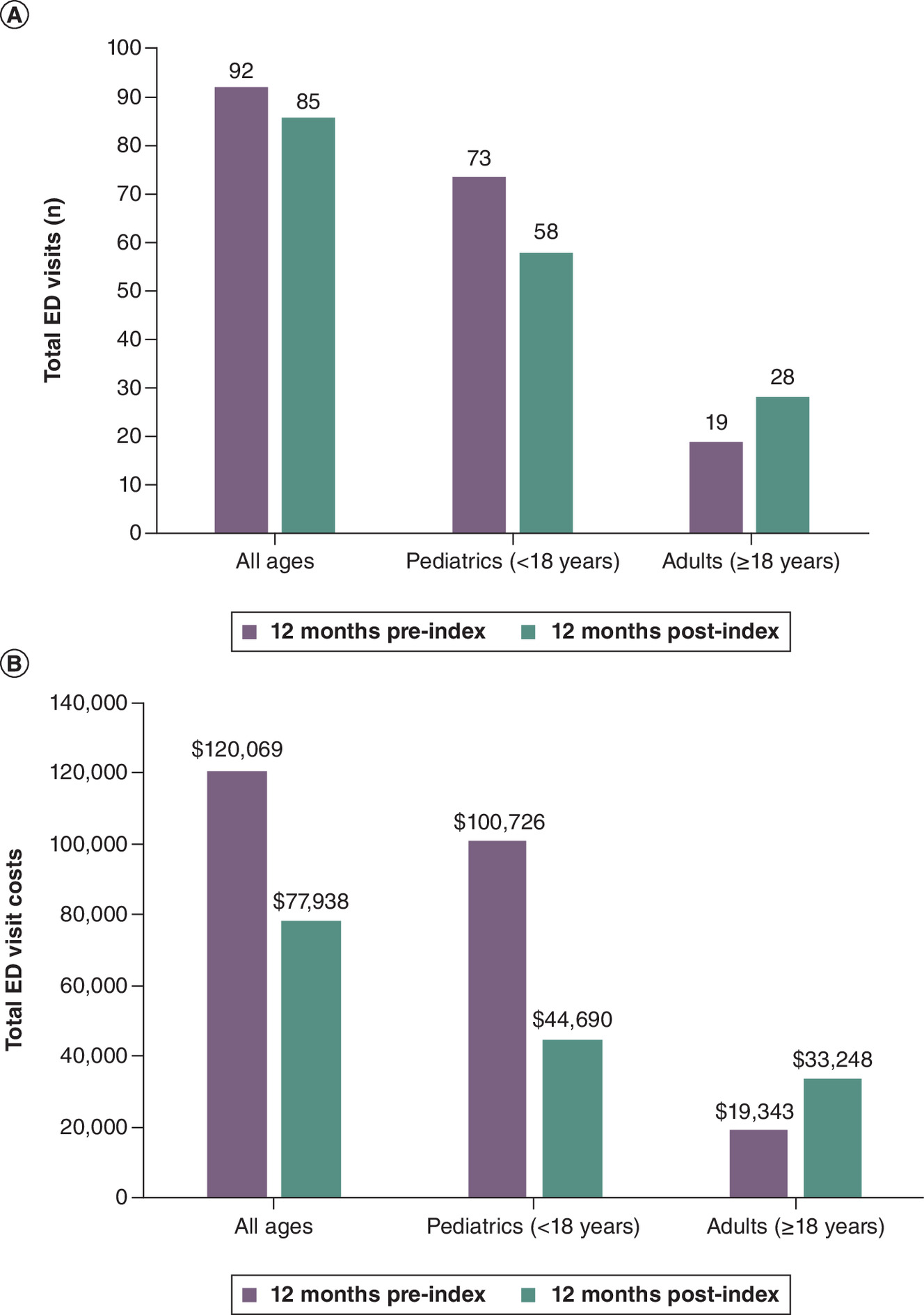
Figure 4. Total number of ED visits (A) and costs (B) in individuals with SMA in the 12 months before and after nusinersen treatment.
ED: Emergency department; SMA: Spinal muscular atrophy.
Total ED visit costs decreased from the 12 months pre-index to the 12 months post-index by 35% from $120,069 to $77,938 in the overall group and by 56% from $100,726 to $44,690 in the pediatric group, but increased by 72% from $19,343 to $33,248 in adults coinciding with the observed increase in ED visits (Figure 4B). Mean average (SD) ED costs per patient showed a similar trend (Supplementary Figure 2B).
Additional analyses
As part of the sensitivity analyses, the baseline demographics of those patients who were excluded from this study based on the cohort selection criteria were similar to those of the final study cohort (Supplementary Table 1). This additional analysis demonstrated that the cohort selection criteria did not result in identifiable selection bias.
Additionally, a substantial proportion of total ED visits (33%) resulted in an inpatient admission within a 10-day window, and most on the same day. The vast majority of these transitions (90%) were related to respiratory conditions. A decreasing number of transitions from ED visit to inpatient admission was observed post-nusinersen treatment (28%) compared with pre-nusinersen treatment (38%).
Discussion
This retrospective cohort research study using large US administrative claims showed that the total number of inpatient admissions was reduced by nearly 50% and total number of ED visits was reduced by nearly 10% for the overall cohort of patients treated with nusinersen in the 12 months post-nusinersen compared with the 12 months pre-nusinersen treatment. Similar reductions of the total inpatient admissions were observed for the age cohorts: 41% for pediatrics and 67% for adults. The total number of days spent in inpatient admissions was reduced by approximately 11% for patients of all ages treated with nusinersen in the post-12 months versus pre-12 months period. These HRU reductions in individuals with SMA after nusinersen treatment are aligned with previous studies occurring outside the US that have shown decreases in hospital admissions and emergency presentations from the first to second year of nusinersen treatment among patients with infantile-onset SMA [27,28]. The results of this study are also aligned with the findings of the previous US retrospective study but demonstrate more robust findings over a 12-month post-treatment period across a broader patient population [25].
In addition to HRU, reductions in inpatient admission and ED costs were also observed in this retrospective administrative claims study. The average cost of inpatient admissions was reduced from the 12 months pre-index to the 12 months post-index by 68% ($19,098 to $6088) in the overall group, with a 63% ($22,903 to $8466) reduction seen in the pediatric group and a 79% ($13,997 to $2899) reduction seen in adults. As expected, a large percentage of the total costs of inpatient admissions in the overall cohort was related to respiratory problems, which are an important comorbidity of SMA and part of disease management [32]. The average cost of respiratory-related services during inpatient admissions was reduced from the pre- to post-index period by 45% ($7245 to $3971) in the overall group, with a 42% ($11,704 to $6770) reduction in the pediatric group and an 83% ($1266 to $218) reduction seen in adults. Total ED visit costs decreased by 56% ($100,726 to $44,690) for the pediatric cohort and over the period of 12 months pre- and post-index. Although total ED visits and ED costs increased for the adult cohort over the same period, the increased ED visits were mostly unrelated to common SMA comorbidities and only increased slightly for musculoskeletal problems.
Nusinersen has been shown to improve motor function and other respiratory clinical outcomes, such as reduction of permanent ventilation and reduction of respiratory intervention or invasive ventilation in clinical trials and real-world studies [11,15,18,33]. The results in this study demonstrate nusinersen is likely to reduce the overall burden of SMA, including respiratory-related care administered in the inpatient setting in terms of frequency of admissions, time spent in the hospital and associated costs to the healthcare system. Despite the increase in ED visits observed for the adult cohort, it is noteworthy that there was a reduction in ED visits among the pediatric cohort with generally more severe diseases. As expected, the pediatric cohort had more ED visits throughout the study than adults. Additional analyses also revealed a decrease in the number of transitions from ED visits to inpatient admissions. These findings suggest potential reductions in both disease burden and financial burden for patients with SMA and their caregivers, which could have a meaningful impact on their daily lives.
There are several limitations to this study. While this study did utilize a robust pre/post analysis design over a 12-month period, descriptive analyses were only presented for HRU and costs due to the small number of patients with SMA, and because the majority of patients analyzed (>60%) did not have an event of interest (e.g., inpatient admission, or ED visits) during the study period. Also, these data and findings did not include infants with SMA aged 0–1 year because of the 12-month pre-index continuous enrollment requirement. Finding comparable untreated patients of those aged 0–1 year instead of using pre- and post-design has significant challenges, as those who have not received nusinersen or other disease-modifying treatment since 2017 are likely to be significantly different from those who have been treated, especially in the absence of disease severity information in administrative claims datasets. Infants aged 0–1 year are likely to have more severe symptoms and events of interest (e.g., inpatient admissions, ED visits) pre-treatment and would likely see larger reductions in number and costs of inpatient admissions and ED visits post-nusinersen treatment. This study also did not include those identified by newborn screening, who were treated with nusinersen before the presence of symptoms. Consequently, this study likely underestimated the HRU and cost reductions in inpatient admissions and ED visits associated with the medical management of patients with SMA, especially in the pediatric cohort. Despite applying rigorous inclusion/exclusion criteria, some patients may still have inaccuracies with regard to the initiation date of nusinersen in administrative claims [30]. Furthermore, we cannot ascertain disease severity in the MarketScan® database, similar to all administrative claims datasets and age was used as a proxy. An additional study limitation is that the results reported only represent two 12-month periods and cannot be extrapolated over the lifetime of patients. Finally, further stratification by age in the pediatric cohort was not performed as the patterns in smaller subgroups may not be reliable due to limited sample size and small number of events of interest. While our analysis does not offer age-specific estimates, the analysis based on a large commercial and Medicaid claims dataset in the US can contribute to understanding the overall impact of nusinersen on patients with SMA, which may be of great importance to payers and policy makers.
Conclusion
This study demonstrates that nusinersen treatment was associated with reductions in number and costs of inpatient admissions across pediatric and adult patients, and reductions in number and costs of ED visits among the pediatric cohort, over a period of 12-month post-treatment initiation compared with a 12-month pre-treatment period using US claims databases.
Summary points
•
The total number of inpatient admissions and days spent in the hospital decreased post-nusinersen treatment in pediatric and adult age cohorts.
•
The average days spent in the hospital per patient decreased post-nusinersen treatment in pediatric and adult age cohorts.
•
The total costs of inpatient admissions and average costs per patient for inpatient admissions decreased post-nusinersen treatment in pediatric and adult age cohorts.
•
The total and average costs per patient of respiratory-related inpatient admissions, as defined as pneumonia, ventilation support and other respiratory illness, symptoms or insufficiencies, also decreased post-nusinersen treatment in the pediatric and adult age cohorts.
•
The total number of ED visits and costs of ED visits decreased in the overall and pediatric cohorts post-nusinersen treatment but increased in the adult age cohort, an increase likely attributable to reasons unrelated to SMA and disease management.
•
The trends shown in this study suggest nusinersen is associated with additional benefits, such as reduced time in the hospital, and are relevant to patients and their families, providers and payers.
Author contributions
C Zhu, B Youn, AD Paradis, S Raynaud, BA Neville and NB Johnson participated in the design of the analyses; C Zhu and BA Neville conducted the statistical analyses. All authors participated in the analysis and interpretation of data and in drafting and critically revising the manuscript. The authors had full editorial control of the manuscript and provided their final approval of all content.
Financial disclosure
This study was funded by Biogen (Cambridge, MA, USA). C Zhu and BA Neville were employees of Biogen and may have owned stock in the company at the time of study. C Zaidman received research support from Biogen and Novartis and received speaking fees and/or served on advisory boards for Sarepta and Chugai. B Youn, AD Paradis, S Raynaud, and NB Johnson are employees of Biogen and may own stock in the company. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
Biogen (Cambridge, MA, USA) provided funding for medical writing support in the development of this paper. J Druso and V Ducas (Excel Scientific Communications, Fairfield, CT, USA) wrote the first draft of the manuscript based on input from authors, and C Farrell (Excel Scientific Communications, Fairfield, CT, USA) copyedited and styled the manuscript per journal requirements.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 128.80 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Mercuri E, Sumner CJ, Muntoni F, Darras BT, Finkel RS. Spinal muscular atrophy. Nat. Rev. Dis. Primers 8(1), 52 (2022).
2.
Darras BT, Monani UR, De Vivo DC. Genetic disorders affecting the motor neuron: spinal muscular atrophy. In: Swaiman's Pediatric Neurology (6th Edition). Swaiman KF, Ashwal S, Ferriero DMet al. et al. (Eds). Elsevier, The Netherlands, 1057–1064 (2017).
3.
Talbot K, Tizzano EF. The clinical landscape for SMA in a new therapeutic era. Gene Ther. 24(9), 529–533 (2017).
4.
Finkel RS, McDermott MP, Kaufmann P et al. Observational study of spinal muscular atrophy type I and implications for clinical trials. Neurology 83(9), 810–817 (2014).
5.
Hoy SM. Nusinersen: first global approval. Drugs 77(4), 473–479 (2017).
6.
Parente V, Corti S. Advances in spinal muscular atrophy therapeutics. Ther. Adv. Neurol. Disord. 11, 1756285618754501 (2018).
7.
Food and Drug Administration. Spinraza prescribing information. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/209531s011lbl.pdf (Accessed: 8 August 2023).
8.
European Medicines Agency. Spinraza summary of product characteristics. Available at: https://www.medicines.org.uk/emc/product/2715/smpc (Accessed: 8 August 2023).
9.
Chiriboga CA, Swoboda KJ, Darras BT et al. Results from a phase 1 study of nusinersen (ISIS-SMN(Rx)) in children with spinal muscular atrophy. Neurology 86(10), 890–897 (2016).
10.
Finkel RS, Chiriboga CA, Vajsar J et al. Treatment of infantile-onset spinal muscular atrophy with nusinersen: a Phase II, open-label, dose-escalation study. Lancet 388(10063), 3017–3026 (2016).
11.
Finkel RS, Mercuri E, Darras BT et al. Nusinersen versus sham control in infantile-onset spinal muscular atrophy. N. Engl. J. Med. 377(18), 1723–1732 (2017).
12.
De Vivo DC, Bertini E, Swoboda KJ et al. Nusinersen initiated in infants during the presymptomatic stage of spinal muscular atrophy: interim efficacy and safety results from the Phase II NURTURE study. Neuromuscul. Disord. 29(11), 842–856 (2019).
13.
Hagenacker T, Wurster CD, Gunther R et al. Nusinersen in adults with 5q spinal muscular atrophy: a non-interventional, multicentre, observational cohort study. Lancet Neurol. 19(4), 317–325 (2020).
14.
Mercuri E, Darras BT, Chiriboga CA et al. Nusinersen versus sham control in later-onset spinal muscular atrophy. N. Engl. J. Med. 378(7), 625–635 (2018).
15.
Crawford TO, Swoboda KJ, De Vivo DC et al. Continued benefit of nusinersen initiated in the presymptomatic stage of spinal muscular atrophy: 5-year update of the NURTURE study. Muscle Nerve 68(2), 157–170 (2023).
16.
Darras BT, Chiriboga CA, Iannaccone ST et al. Nusinersen in later-onset spinal muscular atrophy: long-term results from the phase 1/2 studies. Neurology 92(21), e2492–e2506 (2019).
17.
Maggi L, Bello L, Bonanno S et al. Nusinersen safety and effects on motor function in adult spinal muscular atrophy type 2 and 3. J. Neurol. Neurosurg. Psychiatry 91(11), 1166–1174 (2020).
18.
Coratti G, Cutrona C, Pera MC et al. Motor function in type 2 and 3 SMA patients treated with Nusinersen: a critical review and meta-analysis. Orphanet J. Rare Dis. 16(1), 430 (2021).
19.
Duong T, Wolford C, McDermott MP et al. Nusinersen treatment in adults with spinal muscular atrophy. Neurol. Clin. Pract. 11(3), e317–e327 (2021).
20.
Elsheikh B, Severyn S, Zhao S et al. Safety, tolerability, and effect of nusinersen treatment in ambulatory adults with 5q-SMA. Front. Neurol. 12, 650535 (2021).
21.
Elsheikh B, Severyn S, Zhao S et al. Safety, tolerability, and effect of nusinersen in non-ambulatory adults with spinal muscular atrophy. Front. Neurol. 12, 650532 (2021).
22.
Armstrong EP, Malone DC, Yeh WS, Dahl GJ, Lee RL, Sicignano N. The economic burden of spinal muscular atrophy. J. Med. Econ. 19(8), 822–826 (2016).
• Patients with SMA were found to have significantly higher hospitalizations and medical costs than matched comparators using a retrospective study design of administrative claims data in the US.
23.
Tan H, Gu T, Chen E, Punekar R, Shieh PB. Healthcare utilization, costs of care, and mortality among patients with spinal muscular atrophy. J. Health Econ. Outcomes Res. 6(3), 185–195 (2019).
• Relative to the general population, healthcare utilization and costs were higher for SMA patients in the US using a retrospective cohort study design of administrative claims.
24.
Belter L, Cruz R, Kulas S, McGinnis E, Dabbous O, Jarecki J. Economic burden of spinal muscular atrophy: an analysis of claims data. J. Mark Access Health Policy 8(1), 1843277 (2020).
• Direct inpatient and outpatient costs for untreated SMA patients was significantly higher relative to the general population in the US using administrative claims data.
25.
Droege M, Sproule D, Arjunji R, Gauthier-Loiselle M, Cloutier M, Dabbous O. Economic burden of spinal muscular atrophy in the United States: a contemporary assessment. J. Med. Econ. 23(1), 70–79 (2020).
•• Study showed nusinersen had fewer inpatient stays and lower inpatient costs when compared with similarly aged (<2 years) untreated patients with SMA in the US using administrative claims data.
26.
Lee M Jr, Franca UL, Graham RJ, McManus ML. Pre-nusinersen hospitalization costs of children with spinal muscular atrophy. Pediatr. Neurol. 92, 3–5 (2019).
27.
Menard J, Seferian AM, Fleurence E et al. Respiratory management of spinal muscular atrophy type 1 patients treated with Nusinersen. Pediatr. Pulmonol. 57(6), 1505–1512 (2022).
•• This retrospective multicenter study in France found a significant decrease in total number of inpatient admissions between the first and second year in SMA patients treated with nusinersen with SMA Type I.
28.
Chen KA, Widger J, Teng A, Fitzgerald DA, D'Silva A, Farrar M. Real-world respiratory and bulbar comorbidities of SMA type 1 children treated with nusinersen: 2-year single centre Australian experience. Paediatr. Respir. Rev. 39, 54–60 (2021).
•• This single center observational cohort study of patients with SMA Type I treated with nusinersen in Australia found the total number of hospitalizations was 50% lower in the second year of nusinersen treatment relative to the first year.
29.
Merative. Merative Marketscan Research Databases Explainer. Available at: https://www.merative.com/content/dam/merative/documents/brief/marketscan-explainer-general.pdf (Accessed: 28 November 2023).
30.
Youn B, Proud CM, Wang N et al. Examining real-world adherence to nusinersen for the treatment of spinal muscular atrophy using two large US data sources. Adv. Ther. 40(3), 1129–1140 (2023).
• This analysis highlighted important study methodology and inclusion/exclusion criteria when using real-world administrative databases in the US for evaluation of nusinersen treatment patterns.
31.
Johnson NB, Proud C, Wassel CL, Dreyfus J, Cochrane T, Paradis AD. Characterization of adult patients with SMA treated in US hospital settings: a natural history study in the premier healthcare database. J Neuromuscul Dis. 8(4), 569–578 (2021).
• This publication previously evaluated and characterized common comorbidities related to SMA disease using real-world administrative claims data and codes in the US.
32.
Finkel RS, Mercuri E, Meyer OH et al. Diagnosis and management of spinal muscular atrophy: Part 2: Pulmonary and acute care; medications, supplements and immunizations; other organ systems; and ethics. Neuromuscul. Disord. 28(3), 197–207 (2018).
33.
Sansone VA, Pirola A, Albamonte E et al. Respiratory needs in patients with Type 1 spinal muscular atrophy treated with nusinersen. J. Pediatr. 219, 223–228.e4 (2020).
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 16 December 2023
Accepted: 3 June 2024
Published online: 4 July 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Evaluation of inpatient and emergency department healthcare resource utilization and costs pre- and post-nusinersen for the treatment of spinal muscular atrophy using United States claims. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0187
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Neli Boseva-Stoyanova, Teodora Chamova, Guenka Petrova, Alexandra Savova, Real-world effectiveness and economic evaluations of EMA-approved orphan medicines for spinal muscular atrophy: a systematic literature review, Pharmacia, 10.3897/pharmacia.73.e195536, 73, (2026).
- Sandra Castellar-Leones, Edicson Ruiz-Ospina, Cristian Correa-Arrieta, Fernando Ortiz-Corredor, Perceived Impact on the Daily Lives of Patients With Spinal Muscular Atrophy Treated With Nusinersen, American Journal of Physical Medicine & Rehabilitation, 10.1097/PHM.0000000000002979, 105, 7, (597-602), (2026).
- Susan E Matesanz, Richard S Finkel, Real-world evidence on nusinersen treatment of persons with SMA: a focused review, Journal of Neuromuscular Diseases, 10.1177/22143602251385045, 13, 2, (190-206), (2025).
- Olga Khorkova, Claes Wahlestedt, The long-awaited solution for personalized medicine, Frontiers in Science, 10.3389/fsci.2025.1629021, 3, (2025).