Serious treatment-emergent adverse events in chronic low back pain patients treated with buprenorphine or oral opioids: a retrospective commercial claims analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Explore the safety of Belbuca® (buprenorphine buccal film), buprenorphine transdermal patches and oral opioids for chronic low back pain (cLBP) treatment. Methods: The retrospective analysis of the MarketScan Commercial database (2018–2021) included treatment-naive cLBP adults. The first date of buprenorphine (Belbuca and transdermal patch) or opioid prescription was index date. Cohorts were defined based on the index medication. Observation included a 6-month pre-index period, while post-index lasted until the end of continuous insurance coverage. There were 44 relevant treatment-emergent adverse events (TEAEs) identified in the literature. Incidence rate ratio (IRR) and incidence rate difference (IRD) were used to compare serious TEAE rates (in 1000 person-years) between cohorts. Propensity-score matching minimized the selection bias. Results: Buprenorphine had lower rates of 15 serious TEAEs than oral opioids (all p ≤ 0.037), while higher rates only for serious dizziness (IRR 2.44, p = 0.011; driven by Belbuca), opioid abuse/dependence (IRR 3.13, p = 0.004; driven by patches) and cholecystitis (IRD 20.25, p = 0.044; an outlier). Additionally, a comparison between Belbuca and oral opioids showed lower rates of 13 serious TEAEs (all p ≤ 0.024) and a higher serious dizziness rate (IRR 3.17, p = 0.024). Although the rates of serious opioid abuse/dependence were similar (24.60 vs 26.93, p = 0.921), all Belbuca patients and none of the opioid patients had a positive history of these events. Belbuca also had lower rates of five serious TEAEs than transdermal patches (all p ≤ 0.018), including a serious opioid abuse/dependence (IRR 0.04, p < 0.001), but higher rates of serious cholecystitis (IRD 52.17, p = 0.035; an outlier) and suicidal ideation (IRD 156.50, p < 0.001; an outlier). Conclusion: Buprenorphine had a better safety profile than oral opioids in cLBP treatment. Belbuca showed a more favorable TEAE profile than buprenorphine transdermal patches and oral opioids.
Shareable abstract
#Belbuca (#buprenorphine buccal film) used for chronic #lowbackpain showed a better #safety profile than buprenorphine transdermal patches or oral #opioids. Also, buprenorphine (Belbuca and transdermal patch) was associated with fewer serious #adverseevents than oral opioids.
Plain language summary
Serious harmful effects of treatment for long-lasting low back pain
What is this article about?
This study explored how safe is to use the drugs prescribed for chronic low back pain – buprenorphine and opioids. Researchers analyzed insurance data of patients with long-lasting low back pain and explored the occurrence of serious medical problems that may be caused by the treatment they take. Buprenorphine was compared with opioids and also different forms of buprenorphine were compared with each other – the patch that adheres to the skin versus the film that sticks to the inner cheek (buccal film).
What were the results?
We laid out 44 different types of harmful effects while taking the drugs and tracked their frequency in the patient insurance records. The most relevant results were:
•
Fifteen out of the 44 medical problems occurred less often when taking buprenorphine than opioids. Only three illnesses were more frequent with buprenorphine
•
Patients with buccal films felt serious dizziness more commonly than those with opioids but they less often experienced 13 other illnesses
•
Five serious harmful effects were observed less frequently in the buccal film than in skin patches
•
Two harmful effects were more common when using the buccal film than the skin patch. These effects were not related to the treatment but rather to the patient's disease history.
What do the results mean?
Buprenorphine treatment for long-lasting low back pain may be a safer option than opioids. Also, patients had fewer serious harmful treatment effects when using buccal film than skin patches and opioids.
Chronic low back pain (cLBP) is a disabling condition that affects millions of people worldwide. In the US, cLBP is the leading cause of disability and one of the most frequent reasons for seeking healthcare services resulting in very high expenditures [1,2]. The National Health Interview Survey data reported a 3-month cLBP occurrence among US adults of approximately 39% in 2019, with higher rates among the elderly, females, non-Hispanic Whites and low-income subpopulations [3]. cLBP can have significant impacts on physical, psychological, social and economic aspects of life, reducing health-related quality of life and overall productivity while increasing healthcare costs [1]. The treatment options for cLBP vary depending on the cause, severity, duration and impact of pain and may include pharmacological, non-pharmacological and surgical interventions [4].
Opioids are commonly prescribed medications for cLBP, especially for moderate-to-severe pain that does not respond to other analgesics. However, opioid use has been associated with serious risks and limitations, such as addiction, overdose, tolerance, dependence, withdrawal and various adverse effects and drug interactions. Many of these events are dose-dependent and require thorough treatment planning and close patient monitoring [5–7]. Center for Disease Control and Prevention has developed the opioid use guideline, opioid-prescribing checklist and many additional tools with the initiative to ensure effective communication between patients and clinicians, improve treatment-related and patient-reported outcomes and reduce the risks of long-term opioid use [7].
Buprenorphine is an atypical opioid medication that has unique characteristics and some advantages over other analgesics in cLBP management. Buprenorphine is a partial agonist at μ-opioid receptors, which diminishes opioid-rewarding effects and euphoria, but also limits the risk of life-threatening serious adverse events such as respiratory depression and opioid overdose [8,9]. Due to a moderate to low potential for physical and psychological dependence, Drug Enforcement Administration classified buprenorphine as a schedule III (CIII) substance, while nearly all other opioids are in schedule II (CII) category [10]. Additionally, the administration of buprenorphine transdermal patch and buccal film formulations produced effective pain relief and improved the quality of life of cLBP patients in clinical trials [11–13]. Therefore, buprenorphine may be preferred by some patients who have contraindications for the use of CII opioids or want to reduce/avoid their utilization. However, buprenorphine is not without challenges, such as titration protocols, diversion potential and regulatory barriers and should be used as part of a comprehensive and individualized treatment plan that includes psychosocial support and monitoring [8,14]. Risk-benefit determination for initiating and continuing long-term use of opioids should also be part of best clinical practices.
The study objective was to assess and compare the safety profiles of CIII buprenorphine (Belbuca® and buprenorphine patch) and CII oral opioids (short-acting opioids [SAOs] and long-acting opioids [LAOs]) among CIII buprenorphine- and CII opioid-naive cLBP patients. Additional sub-analyses investigated safety outcomes more granularly between Belbuca (buprenorphine buccal film) and either oral CII opioids or the buprenorphine patch.
Patients & methods
The research was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) cohort studies recommendations [15].
Data source
This retrospective cohort study was conducted using US insurance claims data from the Merative MarketScan® Commercial Claims Database. This database consists of medical and drug data for over 215 million individuals, encompassing employees and their spouses and dependents covered by employer-sponsored private health insurance in the US [16]. The study was performed on the insurance data claims captured in a period from 1 January 2018 to 31 December 2021.
Study population
The study population was identified based on pre-defined inclusion/exclusion criteria to ensure a homogenous pool of treatment-naive cLBP patients prescribed CIII buprenorphine (Belbuca or buprenorphine patch) or oral CII opioid (SAO or LAO) medications.
Inclusion criteria
•
Patients prescribed CIII buprenorphine (Belbuca or buprenorphine patch) or oral CII opioids
•
Adult patients (≥18 years of age on index date)
•
At least two claims with a diagnosis of low back pain based on the International Classification of Diseases – Clinical Modification (ICD-10-CM) codes (Appendix, Supplementary Table 1) in the 6-month pre-index period
•
Treatment-naive patients – no oral CII opioid, buprenorphine buccal film, or buprenorphine patch prescriptions in the 6-month pre-index period
Exclusion criteria
•
A gap in the health plan or pharmaceutical coverage during the observational period
•
Patients prescribed buprenorphine buccal film or buprenorphine patch treatment within the CII opioid cohort
To avoid an overlap between study cohorts, CIII buprenorphine patients (Belbuca and buprenorphine patch) were allowed to have concomitant oral CII opioids during the treatment period, while CII opioid patients that received buprenorphine buccal film or buprenorphine patch prescriptions in the post-index period were excluded from the cohort. Therefore, the adverse event rates in buprenorphine-treated patients could be influenced by CII opioid utilization and potentially be slightly overestimated.
Study design
Patients diagnosed with cLBP and treated with CIII buprenorphine (Belbuca and buprenorphine patch) or oral CII opioids (SAO and LAO) were captured in the database based on the relevant National Drug Code (NDC) (Appendix, Supplementary Table 2). The first date of buprenorphine or oral opioid prescription was assigned as the index date. The observational period consisted of a 6-month pre-index and the post-index period was defined by the final day of continuous healthcare and pharmaceutical coverage. The study included only cLBP treatment-naive patients identified as cases without buprenorphine buccal film, buprenorphine patch, or oral CII opioid prescriptions in the pre-index period. Demographic characteristics of the study sample were assessed on the index date, while clinical characteristics were evaluated during the 6-month pre-index period. Based on the prescribed product type on the index date, patients were stratified in two separate cohorts – CIII buprenorphine (prescribed Belbuca or buprenorphine patch) and oral CII opioid patients (SAO or LAO). For sub-analyses, the CIII buprenorphine cohort was further stratified by the type of index buprenorphine prescription, either Belbuca or buprenorphine patch. The study design is presented on Figure 1.
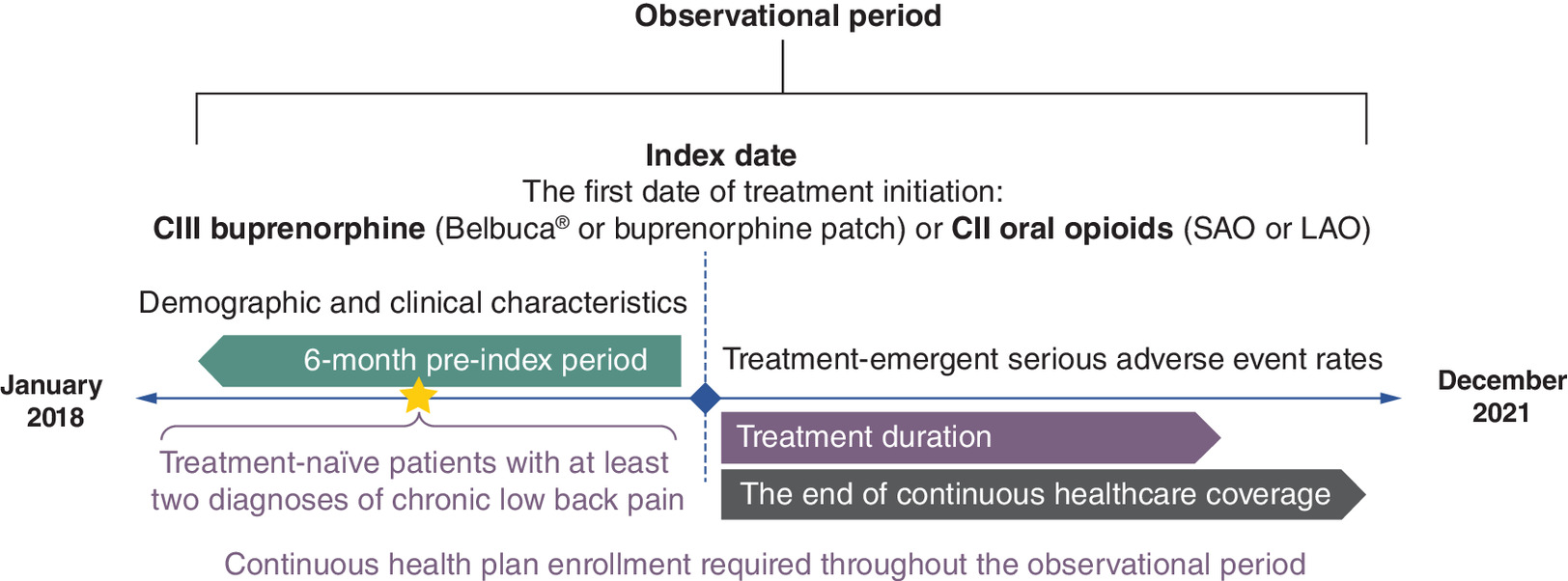
Figure 1. Study design.
CII: Schedule II; CIII: Schedule III; LAO: Long-acting opioid; SAO: Short-acting opioid.
Outcome measures
The main study outcomes were serious treatment-emergent adverse event (TEAE) rates. Based on the most relevant available buprenorphine or opioid evidence, the most common adverse events (≥5% rate), serious adverse events, adverse events leading to treatment discontinuation and opioid-related adverse events were selected as TEAEs of interest for this analysis [17–26]. In total, there were 44 relevant serious TEAEs identified, stratified into the following organ system categories:
•
Cardiovascular: QT prolongation, hypotension, atrial fibrillation, coronary artery disease, hypertension
•
Central nervous system (CNS): dizziness, somnolence, confusion, seizures, syncope, cerebrovascular accident, nervousness, visual discomfort, suicidal ideation, sleep disturbances
•
OUD: opioid abuse/dependence (OAD), opioid poisoning
•
Hormonal: adrenal insufficiency
•
Musculoskeletal: bone fractures, osteoarthritis
•
Respiratory: respiratory depression, pneumonia
•
General: headache, fatigue, allergic reactions, dehydration, dry mouth, xerostomia, sweating, hot flushes, sinusitis
•
Gastrointestinal (GIT): nausea/vomiting, constipation, hepatotoxicity, cholecystitis, abdominal pain, diarrhea, anorexia/loss of appetite
•
Skin toxicities: cellulitis, pruritus, erythema, rash, skin irritation
•
Urinary: urinary discomfort
Serious TEAEs were defined as TEAE events claimed in inpatient or emergency department (ED) settings and were captured in the database via ICD-10-CM codes (Appendix, Supplementary Table 3). Only events that occurred during the treatment period with index medication (CIII buprenorphine or oral CII opioids) were considered to be associated with the prescribed product. The treatment period was defined as the sum of all periods during which patients were supplied with index medication, calculated using prescription date and days of supply for each claim, excluding gaps in the index treatment and accounting for prescription overlaps. Although CIII buprenorphine patients (Belbuca and buprenorphine patch) were allowed to have concomitant oral CII opioid use (SAO and LAO), only buprenorphine prescription claims were included in defining treatment period. As the post-index period duration differed between patients, TEAE rates were reported per 1000 person-years and compared between study cohorts using absolute incidence rate difference (IRD) and incidence rate ratio (IRR) as outcome measures. The IRD represents the crude difference of the incidence rates observed among study cohorts (i.e., incidence rate in cohort 1 minus the incidence rate in cohort 2), while IRR is defined as relative difference measure used to compare the incidence rates of adverse events (i.e., by dividing the incidence rate in cohort 1 with incidence rate in cohort 2).
The primary analysis compared safety outcomes between CIII buprenorphine (Belbuca and buprenorphine patch) versus oral CII opioid (SAO and LAO) cohorts. Sub-analyses aimed to assess the outcomes in more granularly stratified populations (Belbuca vs CII oral opioid and Belbuca vs buprenorphine patch cohorts).
Statistical analysis
Continuous variables were summarized as means and standard deviations, while categorical variables were reported as numbers and proportions of the sample. Independent t-test (continuous variables) and chi-square test of independence (categorical variables) were performed to test the difference between the comparable cohorts. P-values lower than 0.05 implied statistical significance between the cohorts.
All TEAE rates and IRD values were reported per 1000 person-years, while IRR was reported as a rate ratio with 95% confidence intervals (95% CI). The incidence rate ratio test computed IRD and IRR and explored the statistical significance of TEAE rate differences between study cohorts. P-values referred to IRDs in case TEAEs occurred in only one cohort, while significance related to IRRs was used if the event was captured in both compared cohorts. Negative IRD values and IRRs less than 1 imply that the TEAE rate was lower in the referent cohort (CIII buprenorphine in primary analysis and Belbuca® in sub-analyses).
Propensity-score matching (PSM) analysis with the nearest-neighbor matching algorithm was performed to minimize the selection bias. The demographic characteristics of patients observed on the index date and clinical characteristics observed throughout the pre-index period were used as a basis for the matching process.
All statistical analyses were performed using the IBM Statistical Package for the Social Sciences (SPSS®), Statistical Analysis System (SAS®) and MedCalc® statistical software.
Results
Out of 1,706,386 patients prescribed CIII buprenorphine (Belbuca or buprenorphine patch) or oral CII opioids, 213,195 patients have been identified in a final non-matched sample (781 in the CIII buprenorphine and 212,414 in the CII opioid cohorts) after applying inclusion/exclusion criteria. More granularly, 380 patients within the CIII buprenorphine cohort were treated with Belbuca and 401 patients with buprenorphine patch. After PSM, the primary analysis final sample consisted of 2737 patients (711 patients in the CIII buprenorphine cohort matched to 2020 patients in the CII opioid cohort). Additionally, the final samples in the subgroup analyses consisted of 1982 patients (352 Belbuca matched to 1630 CII opioid) and 478 patients (239 Belbuca matched to 239 buprenorphine patch). The patient selection flow diagram is presented in Figure 2.
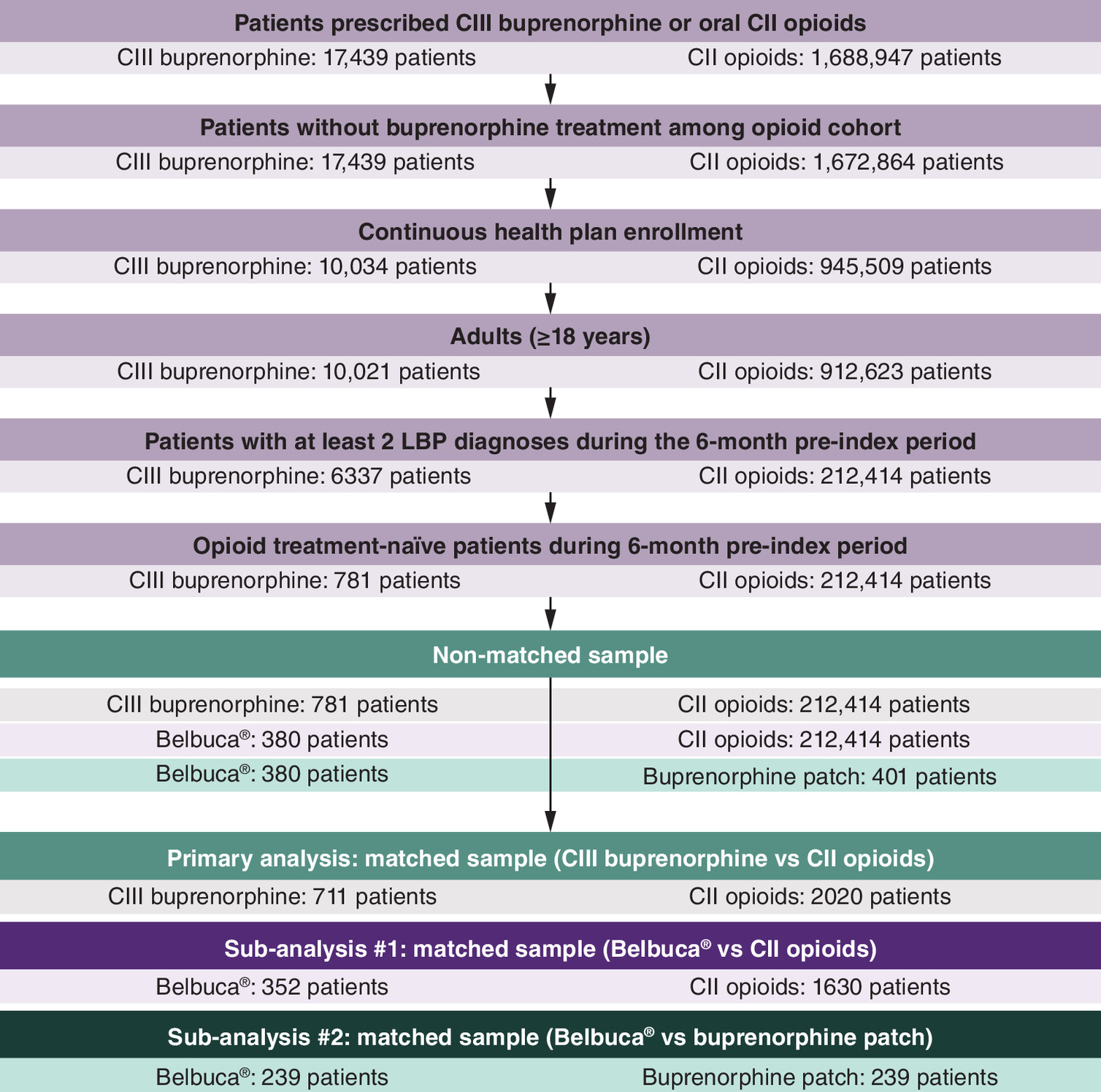
Figure 2. Patient selection flow diagram.
CII: Schedule II; CIII: Schedule III; LBP: Low back pain.
Non-matched population
Primary analysis: CIII buprenorphine versus CII opioids
A total non-matched sample consisted of 213,195 patients with 781 patients initially prescribed CIII buprenorphine and 212,414 patients initially prescribed oral CII opioids.
Demographic characteristics of the non-matched sample of patients treated with CIII buprenorphine and CII opioids are presented in Supplementary Table 4. Patients in the CIII buprenorphine cohort were significantly older with an average age of 49.3 years than patients in the CII opioid cohort (46.7 years). A higher proportion of males was denoted among CII opioid patients (34.1 vs 40.4%, p < 0.001). Regarding healthcare insurance, the only difference was noted in the proportion of patients covered by the comprehensive health plan (4.4 vs 2.2%, p < 0.001). CII opioid-treated patients mostly resided in North East, North Central and West regions, while the majority of CIII buprenorphine patients were located in the South region (p < 0.001, respectively).
In general, CIII buprenorphine patients had greater Charlson Comorbidity Index (CCI) than CII opioid patients (0.9 vs 0.5, p < 0.001), with a significantly higher proportion of patients in all CCI categories (CCI 1–4+, p < 0.001) except CCI 0 category (59.2% vs 72.0%, p < 0.001). Significantly higher proportions of patients with a majority of CCI components were shown in the CIII buprenorphine cohort, including cerebrovascular disease, dementia, chronic pulmonary disease, rheumatic disease, peptic ulcer disease, mild, moderate, or severe liver diseases, diabetes mellitus with and without chronic complications and renal disease (all p < 0.05). Regarding mental health comorbidities, significantly higher proportions of patients were reported in the CIII buprenorphine cohort (all p < 0.001). Higher proportions of patients diagnosed with other chronic pain comorbidities (except spine disorders) were observed among CIII buprenorphine-treated versus CII opioid patients (all p < 0.05). The full list of clinical characteristics is presented in Supplementary Table 5.
Sub-analysis #1: Belbuca versus CII opioids
A total non-matched sample consisted of 212,794 patients with 380 patients initially prescribed Belbuca and 212,414 patients initially prescribed oral CII opioids.
There was a significant difference in mean age (48.9 vs 46.7 years, p < 0.001) and gender distribution (31.8% vs 40.4% were males, p = 0.001) between sub-analysis #1 cohorts. Higher rate of Belbuca patients was covered by consumer-driven health plan (16.6% vs 12.3%, p = 0.011) and resided in South region (68.9% vs 47.1%, p < 0.001), while CIII opioid patients were more common in North East (7.6% vs 12.5%, p = 0.004), North Central (13.2% vs 23.9%, p < 0.001) and West (10.0% vs 16.4%, p = 0.001) regions. All demographic characteristics of the non-matched sub-analysis #1 sample are listed in Supplementary Table 6.
The Belbuca cohort had slightly but statistically higher CCI (0.7 vs 0.5, p = 0.003), with a higher proportion of patients in CCI groups 1 (23.4% vs 16.3%, p < 0.001) and 3 (4.7% vs 2.8%, p = 0.019). A higher rate of CII opioid patients did not have any CCI comorbidities in the pre-index period (60.3% vs 72.0%, p < 0.001). Specific comorbidities with the highest rates across Belbuca and CII oral opioids cohorts were chronic pulmonary disease (13.7% vs 8.8%, p = 0.001) and diabetes without chronic complications (13.2% vs 9.6%, p = 0.018) among CCI items, anxiety (31.6% vs 16.5%, p < 0.001) and depression (30.8% vs 12.1%, p < 0.001) among mental health disorders and spine disorders (99.7% vs 99.8%, p = 0.591) and musculoskeletal disorders (75.8% vs 57.4%, p < 0.001) among other chronic pain conditions. There were no identified comorbidities with a significantly higher rate in CII opioid patients. The list of all clinical characteristics in a non-matched sub-analysis #1 sample is reported in Supplementary Table 7.
Sub-analysis #2: Belbuca versus buprenorphine patch
A total non-matched sample consisted of 781 patients with 380 patients initially prescribed Belbuca and 401 patients initially prescribed buprenorphine patch.
There were no statistical differences observed in age and gender distribution characteristics between cohorts. Buprenorphine buccal film patients were more commonly covered by consumer-driven health plan (16.6% vs 8.5%, p = 0.001) and resided in the South region (68.9% vs 56.1%, p < 0.001), while buprenorphine patch patients were more frequent in North Central area (13.2% vs 21.9%, p = 0.001). All demographic characteristics of sub-analysis #2 non-matched sample are shown in Supplementary Table 8.
Buprenorphine patch patients had significantly higher CCI (0.7 vs 1.0, p = 0.025) and higher rates of mild liver disease (3.7% vs 8.2%, p = 0.008) and psychoses (0.8% vs 3.2%, p = 0.021). All other CCI components, mental disorders and chronic pain comorbidities had similar distribution between the cohorts. The list of all clinical characteristics among sub-analysis #2 non-matched sample is reported in Supplementary Table 9.
Matched population
Primary analysis: CIII buprenorphine versus CII opioids
A total number of 2737 patients were identified in the final matched sample (711 patients in the CIII buprenorphine and 2020 patients in the CII opioid cohorts). Patients were well-balanced between the study cohorts and there were no differences in demographic and clinical characteristics that could impact study outcome measures (Appendix, Supplementary Tables 10 and 11).
Only one significant difference was noted among serious cardiac-related TEAEs, the rate of serious coronary artery disease with a lower in the CIII buprenorphine cohort compared with the CII opioid cohort (IRR 0.05, p < 0.001). From all investigated serious CNS-related TEAEs, the rate of dizziness was significantly higher among CIII buprenorphine patients (IRR 2.44, p = 0.011) which could be a potential signal of cardiac arrhythmias, although there were no differences in QT prolongation between the cohorts. The rates of sleep disturbances and seizures were higher among CII opioid-treated patients (IRR 0.34 and IRD -39.88 per 1000 person-years, p < 0.05). The rate of serious OAD was significantly higher in CIII buprenorphine patients (IRR 3.13, p = 0.004), while the rate of serious opioid poisoning was significantly higher in CII opioid patients (IRD -29.91 per 1000 person-years, p = 0.007). Serious dehydration and hot flushes were more frequent among CII opioid patients compared with the CIII buprenorphine cohort (IRR 0.37 and IRD -34.89 per 1000 person-years, p < 0.05). Within the group of GIT-related TEAEs, only serious cholecystitis was more prevalent among CIII buprenorphine patients (IRD 20.25 per 1000 person-years, p = 0.044), while the rates of serious constipation, abdominal pain and nausea/vomiting were significantly higher among CII opioid patients (IRR 0.35, 0.45 and 0.57, respectively, all p < 0.05). Serious osteoarthritis was the musculoskeletal TEAE that occurred more commonly in oral CII opioid-treated patients, with an IRR of 0.05 (p < 0.001). The rates of serious respiratory depression and pneumonia appeared to be significantly higher among CII opioid cohort (IRR 0.18 and 0.32, respectively, p < 0.05), as well as the rates of serious skin-related TEAEs, pruritus and rash (both IRD -19.94 per 1000 person-years, p = 0.027). The rate of serious urinary discomfort was also significantly higher in CII opioid patients (IRR 0.08, p < 0.001). All serious TEAE rates for primary analysis are reported in Table 1.
| CIII buprenorphine (n = 711) | CII opioids (n = 2,020) | Incidence rate difference (95% CI) | Incidence rate ratio (95% CI) | p-value† | |
|---|---|---|---|---|---|
| Cardiac adverse events | |||||
| QT prolongation | 40.49 | 14.95 | 25.54 (-6.21–57.29) | 2.71 (0.70–15.31) | 0.123 |
| Hypotension | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Atrial fibrillation | 64.79 | 44.86 | 19.93 (-24.10–63.96) | 1.44 (0.60–3.71) | 0.386 |
| Coronary artery disease | 4.05 | 89.72 | -85.67 (-124.05–(-47.29)) | 0.05 (0.00–0.29) | <0.001 |
| Hypertension | 32.40 | 14.95 | 17.45 (-11.76–46.65) | 2.17 (0.52–12.68) | 0.261 |
| Central nervous system-related adverse events | |||||
|---|---|---|---|---|---|
| Dizziness | 121.48 | 49.84 | 71.64 (15.95–127.33) | 2.44 (1.16–5.59) | 0.011 |
| Somnolence | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Confusion | 32.40 | 29.91 | 2.49 (-30.46–35.44) | 1.08 (0.33–3.79) | 0.894 |
| Seizures | 0.00 | 39.88 | -39.88 (-64.78–(-14.97)) | 0.00 (0.00–0.48) | 0.002 |
| Syncope | 24.30 | 54.83 | -30.53 (-66.84–5.77) | 0.44 (0.13–1.31) | 0.110 |
| Cerebrovascular accident | 72.89 | 39.88 | 33.01 (-11.89–77.91) | 1.83 (0.76–4.86) | 0.154 |
| Nervousness | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Visual discomfort | 24.30 | 19.94 | 4.36 (-23.49–32.20) | 1.22 (0.29–5.87) | 0.779 |
| Suicidal ideation | 4.05 | 0.00 | 4.05 (-4.76–12.86) | - | 0.367 |
| Sleep disturbances | 20.25 | 59.81 | -39.57 (-75.87–(-3.26)) | 0.34 (0.09–1.03) | 0.037 |
| OUD-related adverse events | |||||
|---|---|---|---|---|---|
| OAD | 109.34 | 34.89 | 74.45 (23.10–125.79) | 3.13 (1.33–8.52) | 0.004 |
| Opioid poisoning | 0.00 | 29.91 | -29.91 (-51.48–(-8.34)) | 0.00 (0.00–0.69) | 0.007 |
| General adverse events | |||||
|---|---|---|---|---|---|
| Headache | 89.09 | 94.70 | -5.61 (-62.00–50.76) | 0.94 (0.49–1.84) | 0.843 |
| Fatigue | 52.64 | 94.70 | -42.06 (-91.88–7.75) | 0.56 (0.25–1.19) | 0.104 |
| Allergic reactions | 0.00 | 14.95 | -14.95 (-30.21–0.30) | 0.00 (0.00–1.97) | 0.055 |
| Dehydration | 48.59 | 129.60 | -81.01 (-135.29–(-26.72)) | 0.37 (0.17–0.77) | 0.004 |
| Dry mouth | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Xerostomia | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Sweating | 16.20 | 0.00 | 16.20 (-1.41–33.81) | - | 0.071 |
| Hot flushes | 0.00 | 34.89 | -34.89 (-58.19–(-11.59)) | 0.00 (0.00–0.56) | 0.003 |
| Sinusitis | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Gastrointestinal adverse events | |||||
|---|---|---|---|---|---|
| Nausea and vomiting | 218.67 | 383.80 | -165.13 (-265.90–(-64.40)) | 0.57 (0.39–0.82) | 0.001 |
| Constipation | 40.49 | 114.64 | -74.15 (-124.73–(-23.57)) | 0.35 (0.15–0.77) | 0.005 |
| Hepatotoxicity | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Cholecystitis | 20.25 | 0.00 | 20.25 (0.56–39.94) | - | 0.044 |
| Abdominal pain | 287.51 | 633.02 | -345.51 (-469.40–(-221.60)) | 0.45 (0.33–0.61) | <0.001 |
| Diarrhea | 24.30 | 49.84 | -25.54 (-60.77–9.67) | 0.49 (0.15–1.48) | 0.168 |
| Anorexia/loss of appetite | 0.00 | 14.95 | -14.95 (-30.21–0.30) | 0.00 (0.00–1.97) | 0.055 |
| Hormonal adverse events | |||||
|---|---|---|---|---|---|
| Adrenal insufficiency | 8.10 | 4.98 | 3.12 (-12.14–18.37) | 1.62 (0.08–95.86) | 0.745 |
| Musculoskeletal adverse events | |||||
|---|---|---|---|---|---|
| Bone fractures | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Osteoarthritis | 4.05 | 89.72 | -85.67 (-124.05–(-47.29)) | 0.05 (0.00–0.29) | <0.001 |
| Respiratory adverse events | |||||
|---|---|---|---|---|---|
| Respiratory depression | 20.25 | 109.66 | -89.41 (-135.14–(-43.66)) | 0.18 (0.05–0.50) | <0.001 |
| Pneumonia | 28.35 | 89.72 | -61.37 (-105.40– (17.35)) | 0.32 (0.11–0.79) | 0.007 |
| Skin-related adverse events | |||||
|---|---|---|---|---|---|
| Cellulitis | 89.09 | 69.78 | 19.31 (-33.53–72.14) | 1.28 (0.62–2.70) | 0.482 |
| Pruritus | 0.00 | 19.94 | -19.94 (-37.55–(-2.33)) | 0.00 (0.00–1.23) | 0.027 |
| Erythema | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Rash | 0.00 | 19.94 | -19.94 (-37.55–(-2.33)) | 0.00 (0.00–1.23) | 0.027 |
| Skin irritation | 4.05 | 0.00 | 4.05 (-4.76–12.86) | - | 0.367 |
| Urinary adverse events | |||||
|---|---|---|---|---|---|
| Urinary discomfort | 8.10 | 99.69 | -91.59 (-132.89–(-50.29)) | 0.08 (0.01–0.33) | <0.001 |
†
Incidence rate ratio test was performed to assess statistical differences between study cohorts. If the rate of adverse event was zero in one of the cohorts, p-value reflects the difference between study cohorts in the absolute incidence rate difference.
CII: Schedule II; CIII: Schedule III; CI: Confidence interval; OAD: Opioid abuse/dependence; OUD: Opioid use disorder.
Sub-analysis #1: Belbuca versus CII opioids
A total number of 1982 patients were identified in the final sample of matched patients (352 patients in the Belbuca and 1630 patients in the CII opioid cohorts). Patients were well-balanced between the study cohorts and there were no differences in patients' characteristics that could impact study outcome measures. As the demographic and clinical characteristics were used as a basis for PSM analysis, there were no statistical differences in these outcomes implying the cohorts were well-balanced. The list of demographic characteristics is shown in Appendix Supplementary Table 12, while clinical characteristics are reported in Appendix Supplementary Table 13.
Belbuca had a lower rate of 13/44 serious TEAEs with only a higher rate of serious dizziness (IRR 3.17, p = 0.024) compared with CII opioid patients. Serious TEAEs with higher rates among CII oral opioid patients were respiratory depression (IRD -134.63 per 1000 person-years, p < 0.001), atrial fibrillation (IRD -87.51 per 1000 person-years, p = 0.001), osteoarthritis (-74.05 per 1000 person-years, p = 0.003), seizures (IRD -60.59 per 1000 person-years, p = 0.007), sleep disturbances (IRD -53.85 per 1000 person-years, p = 0.010), urinary discomfort (IRD -47.12 per 1000 person-years, p = 0.017), syncope (IRR 0.12, p = 0.015), pneumonia (IRR 0.20, p = 0.020), nausea/vomiting (IRR 0.29, p < 0.001), constipation (IRR 0.32, p = 0.007), abdominal pain (IRR 0.32, p < 0.001), fatigue (IRR 0.34, p = 0.024) and dehydration (IRR 0.35, p = 0.016). Although the rates of serious OAD were similar between study cohorts (24.60 vs 26.93 per 1000 person-years, IRR 0.91, p = 0.921), all Belbuca patients had positive OAD history while all CII opioid patients obtained the diagnosis after treatment initiation. All serious TEAE rates among sub-analysis #1 matched sample are listed in Table 2.
| Belbuca® (n = 352) | CII opioids (n = 1630) | Incidence rate difference (95% CI) | Incidence rate ratio (95% CI) | p-value† | |
|---|---|---|---|---|---|
| Cardiac adverse events | |||||
| QT prolongation | 0.00 | 6.73 | -6.73 (-21.29–7.83) | 0.00 (0.00–47.50) | 0.365 |
| Hypotension | 0.00 | 20.20 | -20.20 (-45.42–5.02) | 0.00 (0.00–2.95) | 0.117 |
| Atrial fibrillation | 0.00 | 87.51 | -87.51 (-140.01–(-35.01)) | 0.00 (0.00–0.40) | 0.001 |
| Coronary artery disease | 0.00 | 6.73 | -6.73 (-21.29–7.83) | 0.00 (0.00–47.50) | 0.365 |
| Hypertension | 0.00 | 13.46 | -13.46 (-34.06–7.13) | 0.00 (0.00–6.48) | 0.200 |
| Central nervous system-related adverse events | |||||
|---|---|---|---|---|---|
| Dizziness | 106.58 | 33.66 | 72.92 (11.15–134.7) | 3.17 (1.06–11.35) | 0.024 |
| Somnolence | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Confusion | 57.39 | 74.05 | -16.66 (-78.43–45.12) | 0.748 (025–2.19) | 0.612 |
| Seizures | 0.00 | 60.59 | -60.59 (-104.27–(-16.90) | 0.00 (0.00–0.62) | 0.007 |
| Syncope | 8.20 | 67.32 | -59.12 (-107.41–(-10.83)) | 0.12 (0.00–0.86) | 0.015 |
| Cerebrovascular accident | 24.60 | 53.85 | -29.26 (-77.55–19.04) | 0.46 (0.08–1.90) | 0.254 |
| Nervousness | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Visual discomfort | 0.00 | 20.20 | -20.20 (-45.42–5.02) | 0.00 (0.00–2.95) | 0.117 |
| Suicidal ideation | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Sleep disturbances | 0.00 | 53.85 | -53.85 (-95.04–(-12.67)) | 0.00 (0.00–0.71) | 0.010 |
| OUD-related adverse events | |||||
|---|---|---|---|---|---|
| OAD | 24.60 | 26.93 | -2.33 (-40.86–36.19) | 0.91 (0.13–5.40) | 0.921 |
| Opioid poisoning | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| General adverse events | |||||
|---|---|---|---|---|---|
| Headache | 90.20 | 114.44 | -24.25 (-101.30–52.80) | 0.79 (0.33–1.78) | 0.548 |
| Fatigue | 40.99 | 121.17 | -80.18 (-150.01–(-10.35)) | 0.34 (0.10–0.95) | 0.024 |
| Allergic reactions | 0.00 | 13.46 | -13.46 (-34.06–7.13) | 0.00 (0.00–6.48) | 0.200 |
| Dehydration | 49.19 | 141.37 | -92.17 (-167.83–(-16.51)) | 0.35 (0.11–0.89) | 0.016 |
| Dry mouth | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Xerostomia | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Sweating | 0.00 | 13.46 | -13.46 (-34.06–7.13) | 0.00 (0.00–6.48) | 0.200 |
| Hot flushes | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Sinusitis | 0.00 | 6.73 | -6.73 (-21.29–7.83) | 0.00 (0.00–47.50) | 0.365 |
| Gastrointestinal adverse events | |||||
|---|---|---|---|---|---|
| Nausea and Vomiting | 131.18 | 451.03 | -319.80 (-452.50–(-187.20)) | 0.29 (0.16–0.51) | <0.001 |
| Constipation | 49.19 | 154.83 | -105.60 (-184.00– (-27.20)) | 0.32 (0.11–0.80) | 0.007 |
| Hepatotoxicity | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Cholecystitis | 40.99 | 40.39 | -0.60 (-47.69–48.90) | 1.01 (0.25–3.99) | 0.974 |
| Abdominal Pain | 270.56 | 841.47 | -570.90 (-753.90–(-387.90)) | 0.32 (0.21–0.48) | <0.001 |
| Diarrhea | 57.39 | 47.12 | 10.27 (-44.21–64.75) | 1.22 (0.36–4.07) | 0.717 |
| Anorexia/loss of appetite | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Hormonal adverse events | |||||
|---|---|---|---|---|---|
| Adrenal insufficiency | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Musculoskeletal adverse events | |||||
|---|---|---|---|---|---|
| Bone fractures | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Osteoarthritis | 0.00 | 74.05 | -74.05 (-122.34–(-25.76)) | 0.00 (0.00–0.49) | 0.003 |
| Respiratory adverse events | |||||
|---|---|---|---|---|---|
| Respiratory depression | 0.00 | 134.63 | -134.63 (-199.80– (-69.50)) | 0.00 (0.00–0.25) | <0.001 |
| Pneumonia | 16.40 | 80.78 | -64.38 (-118.86–(-9.90)) | 0.20 (0.02–0.91) | 0.020 |
| Skin-related adverse events | |||||
|---|---|---|---|---|---|
| Cellulitis | 90.19 | 94.24 | -4.06 (-76.86–68.75) | 0.96 (0.39–2.27) | 0.920 |
| Pruritus | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Erythema | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Rash | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Skin irritation | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Urinary adverse events | |||||
|---|---|---|---|---|---|
| Urinary discomfort | 0.00 | 47.12 | -47.12 (-85.65–(-8.60)) | 0.00 (0.00–0.85) | 0.017 |
†
Incidence rate ratio test was performed to assess statistical differences between study cohorts. If the rate of adverse event was zero in one of the cohorts, p-value reflects the difference between study cohorts in the absolute incidence rate difference.
CII: Schedule II; CI: Confidence interval; OAD: Opioid abuse/dependence; OUD: Opioid use disorder.
Sub-analysis #2: Belbuca versus buprenorphine patch
A total number of 478 patients were identified in the final sample of matched patients (239 patients in both cohorts). Patients were well-balanced between the study cohorts and there were no differences in patients' characteristics that could impact study outcome measures. There were no statistical differences between cohorts in demographic and clinical characteristics as they were used to match patients in PSM analysis. The demographic and clinical characteristics in sub-analysis #2 matched sample are shown in Appendix Supplementary Tables 14 and 15.
Serious suicidal ideation and cholecystitis occurred only in the Belbuca cohort (IRDs 156.50 [p < 0.001] and 52.17 [p = 0.035], respectively). However, the rates of serious atrial fibrillation (IRD -163.86 per 1000 person-years, p < 0.001), QT prolongation (IRD -117.04 per 1000 person-years, p = 0.001), respiratory depression (-58.52 per 1000 person-years, p = 0.018), OAD (IRR 0.04, p < 0.001) and dizziness (IRR 0.04, p < 0.001) were higher in the buprenorphine patch cohort. All serious TEAE rates in sub-analysis #2 matched sample are reported in Table 3.
| Belbuca® (n = 239) | Bup. patch (n = 239) | Incidence rate difference (95% CI) | Incidence rate ratio (95% CI) | p-value† | |
|---|---|---|---|---|---|
| Cardiac adverse events | |||||
| QT prolongation | 0.00 | 117.04 | -117.04 (-185.50–(-48.60)) | 0.00 (0.00–0.40) | 0.001 |
| Hypotension | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Atrial fibrillation | 0.00 | 163.86 | -163.86 (-244.90–(-82.80)) | 0.00 (0.00–0.27) | <0.001 |
| Coronary artery disease | 0.00 | 11.70 | -11.70 (-33.36–9.95) | 0.00 (0.00–34.76) | 0.290 |
| Hypertension | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Central nervous system-related adverse events | |||||
|---|---|---|---|---|---|
| Dizziness | 10.43 | 234.08 | -223.60 (-322.90–(-124.40)) | 0.04 (0.00–0.28) | <0.001 |
| Somnolence | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Confusion | 52.17 | 11.70 | 40.46 (-12.59–93.51) | 4.46 (0.50–210.80) | 0.161 |
| Seizures | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Syncope | 20.87 | 58.52 | -37.65 (-94.96–19.65) | 0.36 (0.03–2.18) | 0.228 |
| Cerebrovascular accident | 31.30 | 58.52 | -27.22 (-88.48–34.04) | 0.53 (0.08–2.75) | 0.413 |
| Nervousness | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Visual discomfort | 0.00 | 35.11 | -35.11 (-72.63–2.40) | 0.00 (0.00–2.16) | 0.067 |
| Suicidal ideation‡ | 156.50 | 0.00 | 156.50 (72.6–240.40) | - | <0.001 |
| Sleep disturbances | 0.00 | 23.41 | -23.41 (-54.04–7.22) | 0.00 (0.00–4.75) | 0.134 |
| OUD-related adverse events | |||||
|---|---|---|---|---|---|
| OAD | 10.43 | 269.19 | -258.80 (-364.90–(-152.70)) | 0.04 (0.00–0.24) | <0.001 |
| Opioid poisoning | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| General adverse events | |||||
|---|---|---|---|---|---|
| Headache | 73.03 | 140.45 | -67.42 (-161.82–26.99) | 0.52 (0.17 -1.43) | 0.172 |
| Fatigue | 52.17 | 58.52 | -6.36 (-74.85–62.13) | 0.89 (0.21–3.87) | 0.859 |
| Allergic reactions | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Dehydration | 31.30 | 46.82 | -15.52 (-72.82–41.78) | 0.67 (0.10–3.95) | 0.620 |
| Dry mouth | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Xerostomia | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Sweating | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Hot flushes | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Sinusitis | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Gastrointestinal adverse events | |||||
|---|---|---|---|---|---|
| Nausea and vomiting | 52.17 | 81.93 | -29.76 (-104.79–45.26) | 0.64 (0.16–2.33) | 0.455 |
| Constipation | 52.17 | 105.34 | -53.17 (-134.21–27.87) | 0.50 (0.13–1.65) | 0.214 |
| Hepatotoxicity | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Cholecystitis‡ | 52.17 | 0.00 | 52.17 (3.74–100.59) | - | 0.035 |
| Abdominal pain | 198.23 | 187.27 | 10.96 (-117.17–139.09) | 1.06 (0.52–2.20) | 0.871 |
| Diarrhea | 41.73 | 0.00 | 41.73 (-1.58–85.05) | - | 0.059 |
| Anorexia/loss of appetite | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Hormonal adverse events | |||||
|---|---|---|---|---|---|
| Adrenal insufficiency | 0.00 | 23.41 | -23.41 (-54.04–7.22) | 0.00 (0.00–4.75) | 0.134 |
| Musculoskeletal adverse events | |||||
|---|---|---|---|---|---|
| Bone fractures | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Osteoarthritis | 0.00 | 11.70 | -11.70 (-33.36–9.95) | 0.00 (0.00–34.76) | 0.290 |
| Respiratory adverse events | |||||
|---|---|---|---|---|---|
| Respiratory depression | 0.00 | 58.52 | -58.52 (-106.95–(-10.09)) | 0.00 (0.00–0.97) | 0.018 |
| Pneumonia | 41.73 | 58.52 | -16.79 (-81.76–48.19) | 0.71 (0.14–3.31) | 0.630 |
| Skin-related adverse events | |||||
|---|---|---|---|---|---|
| Cellulitis | 114.77 | 128.75 | -13.95 (-115.57–87.6) | 0.89 (0.35–2.27) | 0.790 |
| Pruritus | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Erythema | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Rash | 0.00 | 0.00 | 0.00 (0.00–0.00) | - | - |
| Skin irritation | 0.00 | 11.70 | -11.70 (-33.36–9.95) | 0.00 (0.00–34.76) | 0.290 |
| Urinary adverse events | |||||
|---|---|---|---|---|---|
| Urinary discomfort | 0.00 | 11.70 | -11.70 (-33.36–9.95) | 0.00 (0.00–34.76) | 0.290 |
†
Incidence rate ratio test was performed to assess statistical differences between study cohorts. If the rate of adverse event was zero in one of the cohorts, p-value reflects the difference between study cohorts in the absolute incidence rate difference.
‡
represents one outlier patient with AE relating to comorbidities.
CI: Confidence interval; Bup.: Buprenorphine; OAD: Opioid abuse/dependence; OUD: Opioid use disorder.
Discussion
This study showed a more favorable safety and tolerability profile in cLBP patients treated with CIII buprenorphine than oral CII opioids. Out of 44 relevant serious TEAEs that were followed during the treatment, CIII buprenorphine had significantly lower rates in 15 events. Among these 15 events, serious opioid poisoning, seizures, rash, pruritus and hot flushes occurred only in oral CII opioid patients. On the other hand, higher rates of serious dizziness, cholecystitis and OAD were reported in the CIII buprenorphine cohort. However, exploratory analysis revealed that the high serious cholecystitis rate in the CIII buprenorphine cohort (20.25 per 1000 person-years) originated from a single patient. This patient had 5 cholecystitis episodes during a 6-day hospital stay with claimed acute kidney failure, unspecified jaundice and bacteremia. Therefore, serious cholecystitis was considered an outlier and not related to cLBP treatment but most likely to other comorbid conditions. Deep data mining also examined the background of the high serious OAD rate in the CIII buprenorphine cohort (109.34 per 1000 person-years). It was established that the reported rate was not impacted by the positive OAD history during the 6-month pre-index period. After excluding patients with OAD diagnosis in the pre-index, serious OAD rates during the follow-up were still higher in CIII buprenorphine than in CII opioid patients (115.2 vs 35.54 per 1000 person-years, respectively; p = 0.004). However, it was denoted that all serious OAD events occurred in buprenorphine patch- and none in Belbuca-treated patients (215.07 and 0.00 per 1000 person-years, respectively; p < 0.001). Thus, high serious OAD rate in CIII buprenorphine cohort was not associated with Belbuca treatment but was mainly driven by buprenorphine transdermal patches. Greater rates of OAD events in the buprenorphine patch cohort may be the consequence of lower and insufficient doses of buprenorphine with this formulation. To provide pain relief, the patients may reach for the opioid overtreatment. Still, this is only a hypothetical explanation that may not be confirmed in retrospective claims.
In general, long-term opioid treatment is associated with a greater risk of adverse events compared with other non-opioid medications. A comprehensive Cochrane review with meta-analysis by Jackson et al. [24] pointed out that opioid treatment in non-cancer chronic pain conditions has to clearly demonstrate clinical benefits before considering long-term use due to a great risk of adverse events. Comparisons between opioids and placebo or non-opioid analgesics yielded significantly higher risk ratios for adverse events (1.42 and 1.21, respectively; both p < 0.001). Opioid-treated patients also had a 2.75-times higher risk of experiencing serious adverse events compared with placebo (p < 0.001) [24]. However, buprenorphine's partial μ opioid receptor activity distinguishes it from standard CII opioids. In a randomized trial by Choudhury et al. [27], the efficacy and safety characteristics of transdermal buprenorphine patches and oral morphine were directly compared. Besides similar pain relief outcomes, buprenorphine yielded a better safety profile and treatment compliance [27]. In summary the main findings in our study are in accordance with the available evidence on CIII buprenorphine versus CII opioids safety differences.
The safety of different buprenorphine formulations was also examined and showed favorable characteristics in the published research. Yoon et al. [28] observed clinical benefits of buprenorphine transdermal patches titrated up to 40 mcg/h in patients with moderate to severe cLBP. Although 78.1% of the study population experienced an adverse event, 96.5% of events were of mild to moderate intensity and only 36.0% required medications for their prevention or management [28]. However, the maximal approved dose of buprenorphine patch formulations in the US is 20 mcg/h. Studies using buprenorphine buccal film reported numerically lower adverse event rates with 41.0% and 49.2% rates in opioid-naive and opioid-experienced patients [11,29]. Also, the long-term use of buccal film in Hale et al. [30] yielded 22.9% rates of treatment-related adverse events in the titration phase and 14.0% in long-term phase. However, direct comparison of safety characteristics between buprenorphine buccal film and CII opioids or buprenorphine transdermal patches is still missing. This study addresses this unmet need and explores safety outcomes more granularly among these subpopulations.
The results of sub-analysis #1 that compared serious TEAE rates between matched Belbuca and oral CII opioid cohorts provided more benefits than the comparison of all buprenorphine products versus CII opioids. Buprenorphine buccal film showed significantly lower rates of 13 out of 44 serious TEAEs with respiratory depression, seizures, osteoarthritis, atrial fibrillation, sleep disturbance and urinary discomfort events occurring only in the oral CII opioid cohort. Dizziness was the only serious TEAE with a higher rate in Belbuca patients. Although the frequency of serious OAD was similar between the cohorts (IRR 0.91, p = 0.921), it was observed that these events were not related to buprenorphine buccal film treatment as all cases had positive OAD history prior to initiating buprenorphine. On the other hand, all patients with OAD in the oral CII opioid cohort were diagnosed after starting opioid medications for cLBP.
In matched sub-analysis #2, safety outcomes were compared between different buprenorphine formulations – buccal film (Belbuca) and transdermal patches. Most results were similar between the cohorts, but Belbuca patients yielded a slightly better safety profile with a significantly lower rate in 5 of 44 serious TEAEs. Serious respiratory depression, QT prolongation and atrial fibrillation occurred only in the buprenorphine patch cohort. In addition, there were no patients that obtained serious OAD diagnosis during the index treatment period in the Belbuca cohort. After excluding patients with positive OAD history, the rates of serious OAD were significantly higher among buprenorphine patch- than Belbuca-treated patients (302.90 and 0.00 per 1000 person-years, respectively; p < 0.001). This finding supports the results of exploratory data mining within the primary analysis, concluding that high serious OAD rate in the CIII buprenorphine cohort was a result of the higher rates observed in the transdermal patch group. On the other hand, suicidal ideation and cholecystitis were serious TEAEs with higher rates in the Belbuca cohort. However, an unexpectedly high rate of serious suicidal ideation among Belbuca patients (156.50 per 1000 person-years) was due to occurrence in one patient with 15 episodes during a 23-day stay in a psychiatric facility. This patient was diagnosed with severe major depression comorbid with stiff-man syndrome and had a personal history of other mental and behavioral disorders. Also, a higher rate of serious cholecystitis (52.17 per 1000 person-years) was influenced by occurrence in one inpatient with 5 episodes during a 6-day hospital stay due to acute kidney failure comorbid with jaundice and bacteremia. Therefore, it was likely these patients should be considered as outliers since the serious suicidal ideation and cholecystitis events were probably not associated with buprenorphine buccal film treatment for cLBP but with other underlying severe conditions.
Strengths & limitations
This is the first retrospective real-world evidence study in the US healthcare setting that captured a wide range of serious TEAEs and compared their rates in cLBP patients treated with CIII buprenorphine and oral CII opioids. The comprehensive analysis was extended by exploring safety outcomes in more granularly classified populations, Belbuca versus oral CII opioids and Belbuca versus buprenorphine transdermal patches. Patients were required to have continuous insurance coverage during the pre- and post-index periods which established a trustworthy longitudinal observation. The PSM was employed to provide a valid between-group comparison by ensuring a homogenous pool of cLBP patients regarding their demographic and clinical characteristics and to avoid the impact of patients' comorbidities on the safety outcomes. Additionally, patients were required to be treatment-naive during the pre-index period to minimize the long-term effects of investigated treatments on the outcomes during the follow-up period.
However, the study limitations should be noted prior to the interpretation of the results. First, the main limitation is related to the restrictions of coding systems due to the nature and characteristics of real-world insurance claims. This data is primarily collected for billing purposes, henceforth, many data entry errors may have occurred (miscoding, duplicate claims, or negative-input claims). The influence of this limitation has been reduced to a minimum by performing thorough data cleaning, a careful patient selection process and bias-controlling methods such as PSM. Second, the chronicity of low back pain could not be determined in the database. Chronicity was assumed in patients that had low back pain claimed at least two-times during the pre-index period. The third limitation is related to the study findings' generalizability. This retrospective analysis was performed on a commercially-insured population and results may not be applicable to patients with other types of insurance. Furthermore, the sub-analysis that compared the occurrence of AEs within Belbuca- and buprenorphine patch-treated patients yielded statistical significance between cohorts, but it was conducted on a small sample of cLBP patients (239 in each cohort) and the findings should be carefully interpreted. Fourth, the treatment-naive inclusion criterion was defined as an absence of oral CII opioid, Belbuca, or buprenorphine patch claims during the 6-month pre-index period. This was performed by selecting the first CIII buprenorphine or oral CII opioid prescription as the index date. However, authors are unaware if patients received treatment outside the database period (i.e., prior to January 01, 2018). The fifth limitation is associated with the underlying causes of serious TEAEs. Although the connection between index treatment and TEAEs should be secured by capturing only events that occurred during the treatment period, there were still some cases that were not related to CIII buprenorphine and oral CII opioids (e.g., serious cholecystitis and suicidal ideation in Belbuca). Since buprenorphine patients were allowed to have concomitant CII opioid treatment, there is a possibility that some of serious TEAEs were caused by CII opioids in buprenorphine cohort. However, there was no other way to precisely explore TEAE causality in the insurance claims database. In addition, the impact of average daily doses between CII opioids and CIII buprenorphine cohorts could not be considered since buprenorphine has no MME conversion factor value.
Conclusion
In this retrospective real-world evidence study, buprenorphine showed a better safety and tolerability profile than oral CII opioid medications in cLBP patients, with lower rates of many serious TEAEs commonly occurring during the treatment. Serious dizziness and OAD were the only events with higher TEAE rates related to buprenorphine treatment. However, high rate of serious OAD was mainly driven by buprenorphine transdermal patch use. Serious cholecystitis had a higher rate in the buprenorphine cohort but was associated with other comorbid conditions and not index medication.
After further stratification in this study, Belbuca had a more favorable treatment option regarding patients' safety compared with oral CII opioids and buprenorphine patches. Dizziness was the only serious TEAE found to be significantly higher in the buprenorphine buccal film cohort relative to both the CII and patch groups. Multiple episodes of serious cholecystitis and suicidal ideation occurred in a single patient each but were associated with severe underlying conditions and not Belbuca administration. Unlike buprenorphine patches and oral CII opioids, Belbuca was not associated with developing incident diagnosis of serious OAD during treatment. Buprenorphine buccal film also had lower rates of numerous serious TEAEs than comparator cohorts. The rates of serious atrial fibrillation and respiratory depression were consistently lower among Belbuca patients in both sub-analyses.
Summary points
•
This was a retrospective commercial claims analysis (2018–2021) including buprenorphine- and opioid-naive chronic low back pain (cLBP) patients prescribed Belbuca®, buprenorphine transdermal patch, or oral schedule II (CII) opioids.
•
The main study outcome was the occurrence of 44 serious treatment-emergent adverse events related to opioid and buprenorphine use (identified in the published literature) captured during the treatment period with index medication.
•
Oral CII opioids had higher rates of 15 serious adverse events than buprenorphine treatment for cLBP (coronary artery disease, dehydration, hot flushes, nausea and vomiting, constipation, abdominal pain, seizures, sleep disturbances, pruritus, opioid poisoning, osteoarthritis, respiratory depression, pneumonia, rash and urinary discomfort).
•
Buprenorphine treatment for cLBP had higher rates of serious dizziness (driven by Belbuca), opioid abuse/dependence (driven by the patch) and cholecystitis (an outlier) compared with oral CII opioids.
•
Belbuca had lower rates of 13 serious adverse events than oral CII opioids (atrial fibrillation, seizures, syncope, sleep disturbances, osteoarthritis, respiratory depression, pneumonia, fatigue, dehydration, nausea and vomiting, constipation, abdominal pain and urinary discomfort).
•
Only a higher rate of serious dizziness was reported among Belbuca patients compared with the oral CII opioid cohort.
•
The rates of serious QT prolongation, atrial fibrillation, dizziness, opioid abuse/dependence and respiratory depression were higher among buprenorphine patch than Belbuca patients.
•
Although the rates of serious suicidal ideation and cholecystitis were higher in Belbuca than in the buprenorphine patch cohort, it was likely these results originated from outlier cases with a low probability that were associated with the index treatment.
•
Buprenorphine showed better safety than oral CII opioids.
•
Belbuca had a better safety profile than oral CII opioids and buprenorphine transdermal patches.
Author contributions
F Stanicic, D Grbic, D Vukicevic and V Zah equally contributed to this research. All authors were responsible for the conception and design of the work, the acquisition, analysis and interpretation of data for the work, drafting the work and revising it critically for important intellectual content, providing the final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
All steps in conducting this research were supervised and critically reviewed by experts from Collegium Pharmaceutical, Inc.
Financial disclosure
This study was funded by Collegium Pharmaceutical, Inc. ZRx Outcomes Research Inc. received financial support for conducting the research. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary data.docx)
- Download
- 94.31 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Hartvigsen J, Hancock MJ, Kongsted A et al. What low back pain is and why we need to pay attention. Lancet 391(10137), 2356–2367 (2018).
2.
Dieleman JL, Cao J, Chapin A et al. US health care spending by payer and health condition, 1996–2016. JAMA 323(9), 863–884 (2020).
3.
Lucas JW, Connor EM, Bose J. Back, lower limb, and upper limb pain among U.S. adults, 2019. NCHS Data Brief (415), 1–8 (2021).
4.
Qaseem A, Wilt TJ, Mclean RM et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann. Intern. Med. 166(7), 514–530 (2017).
5.
Chou R, Deyo R, Devine B et al. The effectiveness and risks of long-term opioid treatment of chronic pain. Evid. Rep. Technol. Assess. (Full Rep.) 218, 1–219 (2014).
6.
Krebs EE, Gravely A, Nugent S et al. Effect of opioid vs nonopioid medications on pain-related function in patients with chronic back pain or hip or knee osteoarthritis pain: the SPACE randomized clinical trial. JAMA 319(9), 872–882 (2018).
7.
Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain – United States, 2016. MMWR Recomm. Rep. 65(1), 1–49 (2016).
• Points out the significance of controlled opioid usage in long-term treatment due to their safety concerns. It focuses on the opioid use treatment guidelines and other supporting tools developed by the Center for Disease Control and Prevention.
8.
Drug Enforcement Administration - Diversion Control Division - Drug & Chemical Evaluation Section. Buprenorphine (2022). https://www.deadiversion.usdoj.gov/drug_chem_info/buprenorphine.pdf
9.
Gudin J, Fudin J. A narrative pharmacological review of buprenorphine: a unique opioid for the treatment of chronic pain. Pain Ther. 9(1), 41–54 (2020).
10.
Drug Enforcement Administration - Department of Justice. Schedules of controlled substances: rescheduling of buprenorphine from Schedule V to Schedule III (2002). https://www.federalregister.gov/documents/2002/10/07/02-25293/schedules-of-controlled-substances-rescheduling-of-buprenorphine-from-schedule-v-to-schedule-iii
• Drug Enforcement Administration recognized the safety advantages of buprenorphine over other opioids and classified it as a Schedule III drug.
11.
Rauck RL, Potts J, Xiang Q, Tzanis E, Finn A. Efficacy and tolerability of buccal buprenorphine in opioid-naive patients with moderate to severe chronic low back pain. Postgrad. Med. 128(1), 1–11 (2016).
12.
Gordon A, Rashiq S, Moulin DE et al. Buprenorphine transdermal system for opioid therapy in patients with chronic low back pain. Pain Res. Manag. 15(3), 169–178 (2010).
13.
Miller K, Yarlas A, Wen W et al. Buprenorphine transdermal system and quality of life in opioid-experienced patients with chronic low back pain. Expert Opin. Pharmacother. 14(3), 269–277 (2013).
14.
Daitch D, Daitch J, Novinson D, Frey M, Mitnick C, Pergolizzi J Jr. Conversion from high-dose full-opioid agonists to sublingual buprenorphine reduces pain scores and improves quality of life for chronic pain patients. Pain Med. 15(12), 2087–2094 (2014).
•• The authors reported a significant reduction in pain scores and an increase in quality of life after converting patients from high-dose opioid treatments for chronic pain conditions to sublingual buprenorphine.
15.
Cuschieri S. The STROBE guidelines. Saudi J. Anaesth. 13(Suppl. 1), S31–S34 (2019).
16.
Merative. IBM MarketScan Research Databases is now Merative™ MarketScan® Research Databases (2023). https://www.merative.com/real-world-evidence
17.
Papaleontiou M, Henderson CR Jr, Turner BJ et al. Outcomes associated with opioid use in the treatment of chronic noncancer pain in older adults: a systematic review and meta-analysis. J. Am. Geriatr. Soc. 58(7), 1353–1369 (2010).
18.
Oosten AW, Oldenmenger WH, Mathijssen RH, Van Der Rijt CC. A systematic review of prospective studies reporting adverse events of commonly used opioids for cancer-related pain: a call for the use of standardized outcome measures. J. Pain 16(10), 935–946 (2015).
19.
Moore RA, Mcquay HJ. Prevalence of opioid adverse events in chronic non-malignant pain: systematic review of randomised trials of oral opioids. Arthritis Res. Ther. 7(5), R1046 (2005).
20.
Furlan AD, Sandoval JA, Mailis-Gagnon A, Tunks E. Opioids for chronic noncancer pain: a meta-analysis of effectiveness and side effects. CMAJ 174(11), 1589–1594 (2006).
21.
Food and Drug Administration. FDA label: belbuca® (buprenorphine buccal film), CIII (2019). https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/207932s012lbl.pdf
22.
Food and Drug Administration. FDA label: butrans® (buprenorphine transdermal system) CIII (2019). https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/021306s035lbl.pdf
23.
Food and Drug Administration. FDA Adverse Event Reporting System (FAERS) public dashboard (2021). https://www.fda.gov/drugs/questions-and-answers-fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard
24.
Els C, Jackson TD, Kunyk D et al. Adverse events associated with medium- and long-term use of opioids for chronic non-cancer pain: an overview of Cochrane Reviews. Cochrane Database Syst. Rev. 10(10), Cd012509 (2017).
25.
Eisenberg E, Mcnicol ED, Carr DB. Efficacy and safety of opioid agonists in the treatment of neuropathic pain of nonmalignant origin: systematic review and meta-analysis of randomized controlled trials. JAMA 293(24), 3043–3052 (2005).
26.
Busse JW, Wang L, Kamaleldin M et al. Opioids for chronic noncancer pain: a systematic review and meta-analysis. JAMA 320(23), 2448–2460 (2018).
27.
Choudhury K, Dasgupta P, Paul N, Choudhury KB, Roy B, Maity S. A comparative study of transdermal buprenorphine and oral morphine in the treatment of chronic pain of malignant origin. Indian J. Palliat. Care 24(4), 500–504 (2018).
•• This study directly compared buprenorphine transdermal patches and morphine (medium- and long-term use) in non-cancer chronic pain patients. The results showed similar pain score changes with better safety and treatment compliance in the buprenorphine patch arm.
28.
Yoon DH, Bin SI, Chan SK et al. Effectiveness and tolerability of transdermal buprenorphine patches: a multicenter, prospective, open-label study in Asian patients with moderate to severe chronic musculoskeletal pain. BMC Musculoskelet. Disord. 18(1), 337 (2017).
• High-dose buprenorphine transdermal patch treatment was associated with frequent adverse events but with mild-to-moderate severity in most cases that did not require medication prevention or management.
29.
Gimbel J, Spierings ELH, Katz N, Xiang Q, Tzanis E, Finn A. Efficacy and tolerability of buccal buprenorphine in opioid-experienced patients with moderate to severe chronic low back pain: results of a Phase III, enriched enrollment, randomized withdrawal study. Pain 157(11), 2517–2526 (2016).
30.
Hale M, Urdaneta V, Kirby MT, Xiang Q, Rauck R. Long-term safety and analgesic efficacy of buprenorphine buccal film in patients with moderate-to-severe chronic pain requiring around-the-clock opioids. J. Pain Res. 10, 233–240 (2017).
•• The researchers observed much lower rates of treatment-related adverse events among buprenorphine buccal film-treated patients with moderate-to-severe chronic pain than other publications. The results were even better in the long-term treatment phase.
Information & Authors
Information
Published In
Copyright
© 2024 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 December 2023
Accepted: 27 June 2024
Published online: 16 July 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Serious treatment-emergent adverse events in chronic low back pain patients treated with buprenorphine or oral opioids: a retrospective commercial claims analysis. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0183
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Vladimir Zah, Dimitrije Grbic, Filip Stanicic, Treatment characteristics and safety profiles of Belbuca®, buprenorphine patch, and oral schedule II opioids among chronic low back pain patients without a positive history of opioid-use disorder: a retrospective US commercial claims analysis, Frontiers in Pain Research, 10.3389/fpain.2026.1764842, 7, (2026).