Six-minute walk test as clinical end point in cardiomyopathy clinical trials, including ATTR-CM: a systematic literature review
Publication: Journal of Comparative Effectiveness Research
Abstract
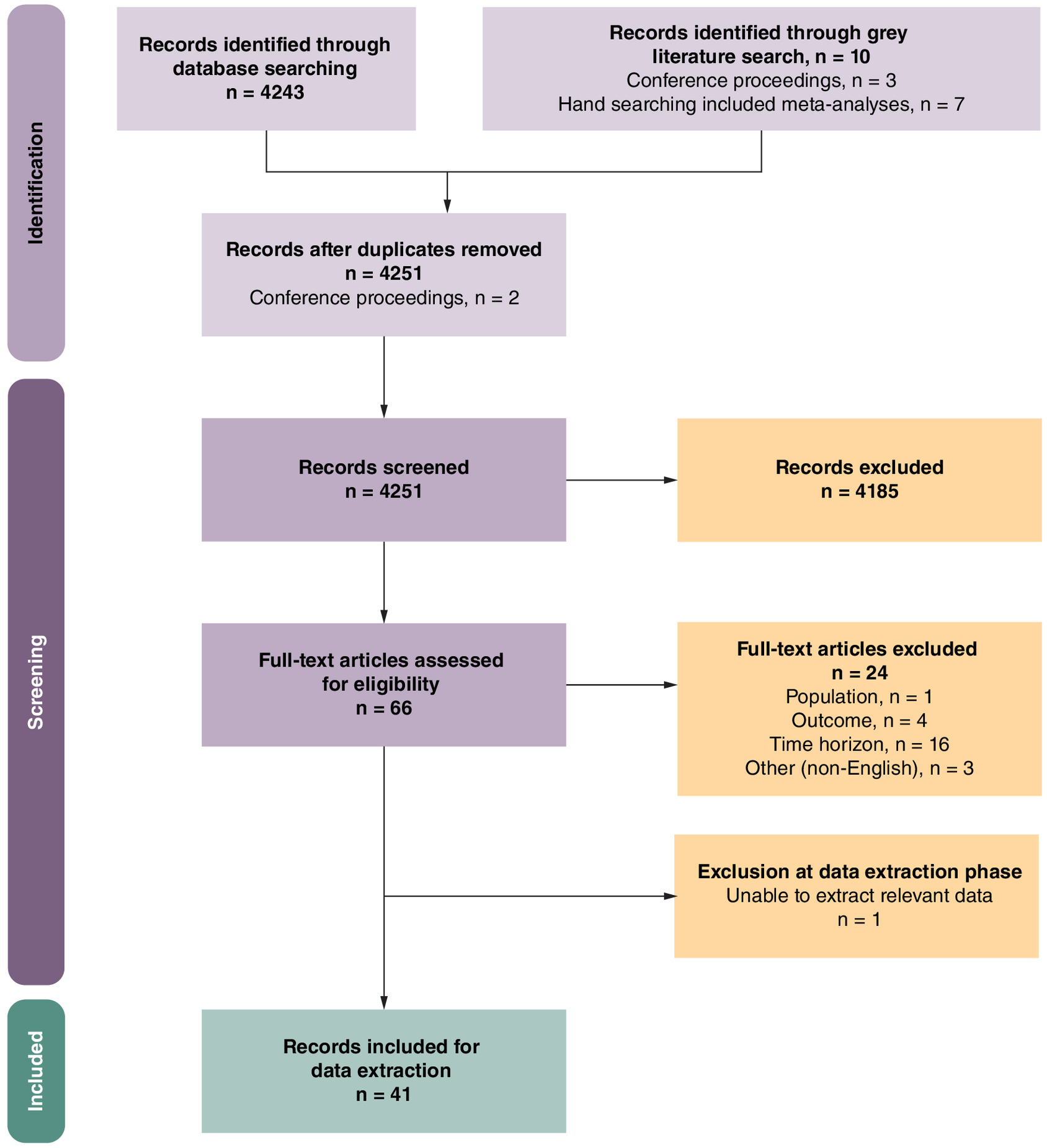
Aim: The six-minute walk test (6MWT) is a common measure of functional capacity in patients with heart failure (HF). Primary clinical study end points in cardiomyopathy (CM) trials, including transthyretin-mediated amyloidosis with CM (ATTR-CM), are often limited to hospitalization and mortality. Objective: To investigate the relationship between the 6MWT and hospitalization or mortality in CM, including ATTR-CM. Method: A PRISMA-guided systematic literature review was conducted using search terms for CM, 6MWT, hospitalization and mortality. Results: Forty-one studies were identified that reported 6MWT data and hospitalization or mortality data for patients with CM. The data suggest that a greater 6MWT distance is associated with a reduced risk of hospitalization or mortality in CM. Conclusion: The 6MWT is an accepted alternative end point in CM trials, including ATTR-CM.
Plain language summary
What is this study about?
This study looked at people with cardiomyopathy, a disease in which the heart loses its ability to pump blood effectively around the body. Some cases of cardiomyopathy are caused by problems with a protein called transthyretin. In clinical trials for cardiomyopathy, doctors often use the number of hospitalizations or deaths to assess a drug's effectiveness. However, this may not tell the whole story. The six-minute walk test (6MWT) is another way of assessing the severity of cardiomyopathy. It measures how far a person can walk on flat ground in 6 min, which can be important to people with heart conditions as it affects whether they can perform normal daily activities. Using the 6MWT in clinical trials may make it easier to assess new drugs and give a more holistic view of a drug's effects. Our study explored the link between the 6MWT and the risk of death or hospitalization in people with cardiomyopathy.
What were the results?
We analyzed 41 studies that measured 6MWT and rates of hospitalization and/or death in people with cardiomyopathy. The results showed that those who could walk further during the 6MWT were less likely to die or be hospitalized than those who could walk a shorter distance. Similar findings were seen in people with cardiomyopathy caused by transthyretin.
What do the results mean?
Our results suggest that the 6MWT is a valid and meaningful measure of the severity of cardiomyopathy, supporting its use as a key assessment in cardiomyopathy clinical trials.
Cardiomyopathies (CMs) encompass diverse causes of structurally or functionally impaired heart muscle, but commonly share a phenotype in which a decline in functional capacity precedes and coincides with rising morbidity and mortality [1–3]. Clinical trials tend to focus on hospitalization and mortality, which necessitates long and large studies to demonstrate the efficacy of a treatment. The strict focus can, however, limit insight into the benefits of a therapy on functional capacity [4,5]. Furthermore, a strong preference for hospitalization and mortality outcomes as the primary end point to demonstrate efficacy might limit the development of therapeutics that could have a positive impact on functional capacity. Prioritizing functional capacity as an end point has thus been recognized as important and relevant to the daily lives of older adults with cardiovascular (CV) disease [6]. Furthermore, health authorities have stated that demonstration of a benefit on functional capacity may be acceptable for approval of drugs for heart failure (HF) in conditions with a high unmet, need even if a benefit on hospitalization or mortality has not been established [7,8].
Transthyretin-mediated (ATTR) cardiac amyloidosis is an example of a CM typically affecting older adults where there is a high unmet need for treatment options. ATTR amyloidosis is a rapidly progressive, debilitating and fatal disease caused by misfolding and deposition of the transthyretin (TTR) protein (initially synthesized in the liver) and accumulation of toxic TTR amyloid fibrils in multiple organs and tissues [9]. There are two types of ATTR amyloidosis: hereditary (ATTRv) amyloidosis, in which variants in the TTR gene result in misfolded TTR protein, and wild-type (wtATTR) amyloidosis, in which wild-type TTR protein misfolds without a variant in the gene but through aging-linked processes [9]. Awareness of ATTR amyloidosis is gradually increasing as new treatment options are available and, based on the projected aging of the worldwide population, wtATTR amyloidosis is predicted to become the most common form of cardiac amyloidosis [10,11]. Recognizing the initial symptoms of ATTRv, also known as variant, and wtATTR amyloidosis is critical to diagnosing and treating the disease as early as possible [12–20].
Progressive CMs, including ATTR amyloidosis with CM (ATTR-CM), are associated with worsening CV function, and there is a need for a short-term and practical functional capacity end point to measure the efficacy of clinical treatments in attenuating disease progression. Currently, cardiopulmonary exercise testing is regarded as the gold standard for assessing exercise capacity; however, the requirement for specialized equipment and trained personnel limits its practicability for many hospital settings [21]. The six-minute walk test (6MWT) is a practical assessment that measures the distance that a patient can walk on a flat, hard surface in a period of 6 min and therefore can be feasibly implemented in both trial and real-world clinical settings [22].
The 6MWT is accepted as a prognostic indicator in both HF and pulmonary arterial hypertension [21–25] and is reported to be a valuable measure of functional capacity in patients with primary light-chain amyloidosis [26,27]. In the case of HF, the 6MWT has been recommended as a clinically meaningful end point for use in HF clinical trials when assessed in combination with N-terminal pro-brain natriuretic peptide levels and quality of life scores [28]. There is also a benefit for using the 6MWT as a prognostic indicator in CM and its subtypes, including ATTR-CM. According to recent guidelines on ATTRv amyloidosis, the 6MWT holds relevance for monitoring disease progression and response to therapy in patients with ATTRv-CM [29,30], and is currently used in the real-world setting [31,32]. Functional capacity is recognized by the US FDA as an acceptable efficacy end point in HF studies that would be able to establish effectiveness and support the approval of drugs to treat HF [33].
Nevertheless, an understanding of the relationship between functional capacity and clinical outcomes would be relevant to interpret trials that employ the 6MWT end point. This systematic literature review (SLR) thus aims to determine the relationship in CM clinical trials between 6MWT performance and two commonly used primary end points: hospitalization and/or mortality for patients with various CM subtypes, including ATTR-CM. The analysis supports a connection between 6MWT performance and prognosis of ATTR-CM. Thus, 6MWT may be used not only to measure the impact of a treatment on functional capacity but also to suggest the potential impact on clinical outcomes.
Materials & methods
This SLR was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [34] and the Cochrane handbook for systematic reviews [35].
The literature included in the SLR is from the Embase and Medline databases using the Ovid® platform (11 February 2022 and 14 February 2022, respectively). The searched terms included the subject headings and keywords relating to 6MWT, mortality, hospitalization, as well as CM. The searches were limited to 2012 to present. In addition to the database searches, a gray literature review, involving hand-searching relevant meta-analyses for additional key texts and a review of conference proceedings from 2020 to present, was conducted to identify evidence not reported in the published literature. The full search strategies and details of the conferences searched are provided in the Supplementary material.
Two independent reviewers screened titles, abstracts and full text publications, with a consensus reached over any disagreements. The following inclusion criteria were used for the review: any study investigating patients with CM, and recording the 6MWT and mortality and/or hospitalization outcomes. The full Population, Intervention, Comparison, Outcome, Time and Study design (PICOTS) criteria are provided in Table 1. Finally, this SLR excluded records that were not published in English.
| Topic | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Population | Patients with HF including: > Patients with CM > Patients with PAH | Patients with no recorded HF, CM or PAH |
| Interventions/ comparators | NA | NA |
| Outcomes | Recorded 6MWT AND Mortality AND/OR Hospitalization | No reported outcomes of interest |
| Time | 2012 to current date for journal articles ≥2020 to current date for conference publications | <2012 for journal articles <2020 for conference publications |
| Study design | Cross-sectional, retrospective and prospective cohorts, case-control and randomized controlled trials | Animal and in vitro studies, letters and editorials |
| Other | NA | Non-English language publications |
6MWT: Six-minute walk test; CM: Cardiomyopathy; HF: Heart failure; NA: Not applicable; PAH: Pulmonary arterial hypertension; PICOTS: Population, Intervention, Comparison, Outcome, Time and Study design
Data were extracted from the included publications and qualitatively synthesized to summarize the key themes reported by the publications captured in this literature review. Publications were grouped by key outcomes with respect to those investigating an association between the 6MWT and hospitalization or mortality, and to those reporting 6MWT independent of hospitalization or mortality data. These latter publications were also subgrouped by key outcome (hospitalization, mortality and major adverse CV events [MACE]).
Included records were subjected to a quality assessment to determine the strength and applicability of their findings. The critical appraisal tools published in the Joanna Briggs Institute handbook for evidence synthesis were used [36].
Results
A total of 41 publications (Figure 1) relating to 30 empirical studies and six meta-analyses were identified, of which 15 were randomized controlled trials (RCTs), 10 were cohort studies and five were cross-sectional studies. Of these publications, six reported the association between 6MWT and either hospitalization, mortality or a combination of these events in patients with CM, while 15 reported separate 6MWT and hospitalization data and 27 reported 6MWT and mortality data (Figure 1). The greatest number of identified studies, for which there were multiple publications, were conducted over a multinational geography (n = 5), Slovenia (n = 4) and the US (n = 4). The characteristics of these included studies are presented in Supplementary Table 7.
The quality of the included studies varied, and the full quality assessment report is provided in the Supplementary material. Thirteen studies were judged to be at a low risk of bias [12,37–48], while eight publications were judged to be at a high risk of bias [14,49–55]. Nine were considered to be of an unclear risk of bias due to insufficient provision of information [56–64]. The most common reason for poor quality regarding RCTs was failure to conceal the allocation of groups to participants and/or clinicians, whereas for cohort or cross-sectional studies, the publications did not provide sufficient information for how they had adjusted their results to address confounding factors.
Data from the included publications were grouped by key outcomes in terms of association between the 6MWT and hospitalization or mortality, and to publications not investigating an association. These latter publications were also subgrouped by key outcome (hospitalization, mortality and MACE), with the identified meta-analyses reported as a stand-alone section.
Association between 6MWT & hospitalization &/or mortality &/or MACE
Hospitalization
Two publications reported an association between the 6MWT distance and hospitalization (Table 2) [58,65]. Bieleck-Dabrowa et al. investigated the prognostic value of the 6MWT for predicting HF-related hospitalization in patients with dilated CM (DCM), reporting that 6MWT distance was a significant predictor over five years of follow-up (odds ratio [OR]: 0.99; p = 0.001) [58]. Vong et al. investigated the association between baseline 6MWT distance and improvement in CV-related hospitalization with a 30-month follow-up [65]. Using a repeated time-to-event model showing the percentage change in risk of death with covariates in the 25th and 75th percentiles, Vong et al. reported that patients with ATTR-CM with a 6MWT distance of 445 meters, 75th percentile, experienced a 15% reduction in CV-related hospitalization, while a 6MWT distance of 269 meters, 25th percentile, was associated with a 20% increase in CV-related hospitalization. In the repeated time-to-event model, the 75th and 25th percentiles were compared with the median value to determine the percentage change in risk of hospitalization [65]. In the available literature, for patients with chronic HF with New York Heart Association (NYHA) class I–IV and mean left ventricular ejection fraction (LVEF) range of 20% to 40%, 6MWT cut-off values range from 300–490 meters, meaning that if a patient walks a distance equal to or less than 300–490 meters, the 6MWT remains a strong prognostic predictor [66].
| Study (year), country | Patient population | Intervention | Follow-up period | Association investigated | Outcome | Statistical test | p-value | Association found with 6MWT | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| Hospitalization | |||||||||
| Bielecka-Dabrowa et al. (2013a), Poland | DCM | Atorvastatin (n = 22); standard care (n = 23) | 5 years | 6MWT distance as a predictor of HF-related re-hospitalization | OR: 0.99 | Multivariate logistic regression | 0.001 |  | [58] |
| ATTR-ACT Vong et al. (2021), Belgium, Brazil, Canada, Czech Republic, France, Germany, Italy, Japan, Netherlands, Spain, Sweden, UK, US | ATTR-CM | Tafamidis or placebo (n = 441) | 30 months | 6MWT distance as a predictor of CV-related hospitalization | 6MWT distance associated with 15% risk reduction: 445 m 6MWT distance associated with 20% risk increase: 269 m | Repeated time-to-event model | NR | | [65] |
| Mortality | |||||||||
| Den Boer et al. (2017), Netherlands | DCM | No intervention (n = 49) | Median (IQR):P | Percent predicted 6MWT† distance as a predictor of death (or heart transplant | HR: 0.95 (95% CI: 0.91–0.99) | Univariate Cox regression | 0.006 | | [39] |
| Lane et al. (2019), UK | ATTR-CM | No intervention (n = 1034) | 100 months | Risk of death per 50 m increase in baseline 6MWT distance | HR: 0.88 (95% CI: 0.832–0.933) | Multivariate Cox proportional hazards model | <0.001 | | [14] |
| Van der Meulen et al. (2020), Netherlands | DCM | No intervention (n = 57) | Median (IQR): 3 years (1.5–5.1) | Percent predicted 6MWT† ≤63% risk of death (or heart transplant) relative to % predicted 6MWT† ≥63% | HR: 10.8 (95%CI: 2.4–49) | Log-rank test | 0.002 | | [48] |
| ATTR-ACT Vong et al. (2021), Belgium, Brazil, Canada, Czech Republic, France, Germany, Italy, Japan, Netherlands, Spain, Sweden, UK, US | ATTR-CM | Tafamidis or placebo (n = 441) | 30 months | 6MWT distance as a predictor of risk of death | 6MWT distance associated with 40% risk reduction: 445 m 6MWT distance associated with 57% risk increase: 269 m | Time-to-event model | NR | | [65] |
| Cardiac event | |||||||||
| Toledo et al. (2021), Brazil | ICM; NICM | No intervention (n = 178) | Median (range): 516 days (39–1340) | Association of 6MWT distance with a cardiac event‡ | HR: 0.99 (95% CI: 0.993–0.999) (G2 value: 6.30) | Likelihood-ratio chi-square (G2) test | 0.01 | | [47] |
†
% Predicted 6MWT adjusts for factors such as age, height and weight, which may impact the 6MWT distance.
‡
Defined as cardiac-related death, HF-related hospitalization and heart transplant.
6MWT: Six-minute walk test; ATTR-CM: Transthyretin-mediated amyloidosis with cardiomyopathy; CI: Confidence interval; CV: Cardiovascular; DCM: Dilated cardiomyopathy; HF: Heart failure; HR: Hazard ratio; ICM: Ischemic cardiomyopathy; IQR: Interquartile range; NICM: Non-ischemic cardiomyopathy; NR: Not reported; OR: Odds ratio.
These data show that an increase in 6MWT distance is associated with a reduction in CV-related hospitalization for patients with DCM or ATTR-CM.
Mortality
In four publications, the association between 6MWT and mortality outcomes was investigated and a trend of a greater 6MWT distance corresponding to an improved outcome was observed (Table 2) [14,39,48,65]. Two publications reported the association between the 6MWT and mortality in patients with ATTR-CM and found that a greater 6MWT distance at baseline was associated with a reduction in the risk of death [14,65]. Lane et al. investigated the association between 6MWT distance and patient survival, reporting that for each 50-meter increase in 6MWT at the time of ATTR-CM diagnosis, there was an estimated 12% reduction in the risk of death (hazard ratio [HR)]: 0.88, 95% confidence interval [CI]): 0.832–0.933; p < 0.001) [14]. A publication by Vong et al. investigated the association between baseline 6MWT distance and improvement in risk of death with a 30-month follow-up [65]. Using a time-to-event model, Vong et al. reported that the risk of death substantially increased to 57% in patients with a 6MWT distance of less than 269 meters, while patients with a 6MWT distance greater than 445 meters experienced a 40% reduction in the risk of death [65].
Two further publications reported the relationship between the 6MWT and mortality in pediatric patients with DCM [39,47], of which one investigated the use of 6MWT as a prognostic marker for death [39]. Den Boer et al. found that after adjusting for factors that may impact the 6MWT distance, such as age, height and weight, the percentage predicted 6MWT distance remained a significant predictor of death (or heart transplant) [39,67]. Additionally, Van der Muelen et al. reported that pediatric patients who recorded a 6MWT distance less than 63% of the predicted distance (the expected distance a patient of that gender, height and age would record in the 6MWT) had a significantly higher risk of death or heart transplant than patients with a 6MWT distance above 63% of the predicted distance (HR: 10.8; 95% CI: 2.4–49; p = 0.001) [48]. These studies demonstrated that the 6MWT was a feasible functional parameter for use in a pediatric population with DCM and could be beneficial as a risk-predicting tool [39,48].
Together, these data show that the 6MWT is a predictor of mortality, and a greater 6MWT distance is associated with a reduction in the risk of mortality for patients with ATTR-CM and patients with DCM.
Major adverse cardiac events
One publication identified an association between 6MWT distance and MACE, with the 6MWT distance again demonstrating prognostic value (Table 2) [47]. Toledo et al. reported that 6MWT distance was significantly associated with subsequent cardiac events (including cardiac hospitalization, cardiac-related death or heart transplant) (HR: 0.99; 95% CI: 0.993–0.999; G2 = 6.30; p = 0.01) in patients with either ischemic CM (ICM) or non-ischemic CM (NICM) [47]. This publication investigated the prognostic value of serum potassium levels in HF, because they are frequently associated with adverse outcomes in patients with HF. Interestingly, the authors reported that incorporating serum potassium levels into prognostic models may improve the predictive value of the 6MWT in this patient population [47].
Within the six publications that investigated the association between 6MWT and the outcomes of interest, the data collectively show that 6MWT distance is associated with hospitalization, mortality and MACE outcomes in patients with CM.
6MWT & hospitalization, mortality or MACE reported independently
The SLR identified several publications reporting 6MWT data and hospitalization (n = 15) (Supplementary Table 8), mortality (n = 27) (Supplementary Table 9) or MACE (n = 4) (Table 3) outcomes independently. While no direct association was investigated, these data collectively show that both a greater 6MWT distance and a greater improvement in 6MWT distance may be associated with improved outcomes. Nine publications reported that a greater 6MWT at baseline, or a smaller decrease in 6MWT distance from baseline, corresponds with a reduced rate of hospitalization in patients with CM [12,41,45,56,59,62,65,68,69]. A further 17 publications reported that patients with CM with a greater 6MWT distance corresponded to improved mortality or survival [12,37,40,44–46,49,50,52–54,56,58,61,68–70] and, finally, three publications reported data that show that a greater 6MWT distance corresponds with a reduced risk of MACE [40,44,61].
| Author (year), country | Intervention(s) | Subgroup | Time point | 6MWT distance (m) | MACE/combined cardiac events (n [%]) | Ref. |
|---|---|---|---|---|---|---|
| Henry et al. (2014), US | Ixmyelocel-T; control, standard care | Ixmyelocel-T (ischemic) (n = 21) | Baseline | Mean: 357.7 | NR | [51] |
| 12 months | Mean change from baseline: 49.89 (95% CI: 25.67–73.74) | MACE: n = 3 (14%) | ||||
| Ixmyelocel-T (non-ischemic) (n = 18) | Baseline | Mean: 379.1 m | NR | |||
| 12 months | Mean change from baseline: 39.10 (95% CI: 11.32–66.17) | MACE: n = 8 (44%) | ||||
| Control (ischemic) (n = 9) | Baseline | Mean: 386.3 | NR | |||
| 12 months | Mean change from baseline: -102.66 (95% CI: -75.29 to -130.40) | MACE: n = 3 (27%) | ||||
| Control (non-ischemic) (n = 9) | Baseline | Mean: 375.5 m | NR | |||
| 12 months | Mean change from baseline: 74.36 (95% CI: 23.08–NR) | MACE: n = 5 (56%) | ||||
| Leyva et al. (2016), UK | Cardiac resynchronization therapy | Idiopathic DCM (n = 165) | Baseline | Mean ± SD: 232.9 ± 121.4 | NR | [61] |
| Median 4.52 years | Mean ± SD: 305.0 ± 132.0 | Mortality or MACE-free survival: 32.9% | ||||
| ICM (n = 353) | Baseline | Mean ± SD: 206.3 ± 109.1 | NR | |||
| Median 4.52 years | Mean ± SD: 288.8 ± 120.3 | Mortality or MACE-free survival: 9.1% | ||||
| ATTR-ACT Maurer et al. (2018), Belgium, Brazil, Canada, Czech Republic, France, Germany, Italy, Japan, Netherlands, Spain, Sweden, UK, US | Tafamidis (20 mg and 80 mg); placebo | Quartile 1 (baseline 6MWT <269 m) | 30 months | Least-squares mean decline in 6MWT from placebo: 73.4 (95% CI: 23.9–122.9) | Improvement in primary outcome (hierarchical combination of all-cause mortality and CV hospitalization frequency) win ratio: 1.15 (95% CI: 0.71–1.87) | [45] |
| Quartile 2 (baseline 6MWT ≥269 m to 351 m) | 30 months | Least-squares mean decline in 6MWT from placebo (win ratio): 58.3 (95% CI:0.4–116.2) | Improvement in primary outcome (hierarchical combination of all-cause mortality and CV hospitalization frequency) win ratio: 1.48 (95% CI: 0.88–2.49) | |||
| Quartile 3 (baseline 6MWT ≥351 m to 445 m) | 30 months | Least-squares mean decline in six-minute walk distance (6MWD) from placebo (win ratio): 78.2 (95% CI: 41.2–115.2) | Improvement in primary outcome (hierarchical combination of all-cause mortality and CV hospitalization frequency) win ratio: 1.78 (95% CI: 0.95–3.31) | |||
| Quartile 4 (baseline 6MWT ≥445 m) | 30 months | Least-squares mean decline in 6MWT from placebo (win ratio): 92.0 (95% CI: 49.2–134.8) | Improvement in primary outcome (hierarchical combination of all-cause mortality and CV hospitalization frequency) win ratio: 2.56 (95% CI: 1.36–4.84) | |||
| Domae et al. (2021), Japan | Autologous stem cell-patch implantation | Responder (n = 13) | Baseline | Mean: 471 (95% CI: 379–540) | NR | [40] |
| 6 months | Mean: 527 | NR | ||||
| 12 months | Mean: 525 | MACE-free survival: 100% | ||||
| 36 months | NR | MACE-free survival: 100% | ||||
| Non-responder (n = 11) | Baseline | Mean: 454 (95% CI: 367.5–491.5) | NR | |||
| 6 months | Mean: 472 | NR | ||||
| 12 months | Mean: 457 | MACE-free survival: 63.4% | ||||
| 36 months | NR | MACE-free survival: 9.1% |
6MWT: Six-minute walk test; CI: Confidence interval; CV: Cardiovascular; DCM: Dilated cardiomyopathy; ICM: Ischemic cardiomyopathy; MACE: Major adverse cardiovascular events; NR: Not reported; SD: Standard deviation; UK: United Kingdom; US: United States.
ATTR-ACT study
Five publications were identified where the 6MWT was investigated in post-hoc analyses of the ATTR-ACT study, in which patients with ATTR-CM were assigned to receive tafamidis or placebo over a 30-month period [65,68–71]. These data suggested that, regardless of intervention, patients with ATTR-CM who have a greater baseline 6MWT distance or experience a smaller decrease in 6MWT distance over time are at a reduced risk of CV-related hospitalization and mortality. Two post-hoc analyses of the ATTR-ACT study reported the data separately by wtATTR and ATTRv amyloidosis [69,70]. Rapezzi et al. reported that patients with ATTRv amyloidosis experienced a least-squares mean decrease in 6MWT distance from baseline of 80.2 meters with tafamidis and 160.0 meters with placebo and reported an all-cause mortality rate of 46.0% and 62.8%, respectively [70]. Patients with wtATTR amyloidosis experienced a least-squares mean decrease in 6MWT distance from baseline of 43.1 meters with tafamidis and 121.5 meters with placebo, and an all-cause mortality rate of 24.3% and 35.8%, respectively [70]. These results highlight the correlation between a reduction in the decline of 6MWT distance from baseline to a reduced risk of mortality for both subgroups of ATTR amyloidosis.
Meta-analyses
The six meta-analyses identified as part of the SLR did not directly measure the associations between 6MWT and hospitalization or mortality. However, the results reported do highlight that patients with CM who had an improved 6MWT distance also had a measurable reduction in risk of re-hospitalization, reduced risk of mortality or heart transplant and a reduced risk of MACE (Table 4) [72–77].
| Publication (year) | Patient population | Subgroups | Effect measured | Follow-up | Summary results | p-value | Level of heterogeneity (%) | Ref. |
|---|---|---|---|---|---|---|---|---|
| Lu et al. (2016) | NIDCM | 1. Intracoronary treatment with BMMC or CD34+ cells 2. Control, no cell therapy | Impact of cell therapy on 6MWT result | Up to 6 months | Studies n = 4 Mean difference increase of 39.89 m (95% CI: -50.22 to 129.99) | 0.39 | 88 | [74] |
| More than 12 months | Studies n = 5 Mean difference increase of 51.56 m (95% CI: -24.09 to 127.20) | 0.18 | 95 | |||||
| Impact of cell therapy on mortality | 12–60 months | Studies n = 6 Risk difference reduction by 0.08 (95% CI: -0.16 to 0.00) | 0.04 | 52 | ||||
| Xia et al. (2020) | NICM | 1. Autologous stem cell therapy 2. Control | Impact of cell therapy on 6MWT result | 3–60 months | Studies n = 7 Mean difference increase of 101.46 m (95% CI: 45.62–157.35) | <0.01 | 94 | [76] |
| Impact of cell therapy on all-cause mortality | 3–60 months | Studies n = 12 RR: 0.78 (95% CI: 0.55–1.11) | 0.17 | 0 | ||||
| Impact of cell therapy on mortality or heart transplant | 3–60 months | Studies n = 12 RR: 0.78 (95% CI: 0.57–1.07) | 0.13 | 14 | ||||
| Impact of cell therapy on mortality or heart transplant (excluding studies with intramyocardial injection) | 3–60 months | Studies n = 10 RR: 0.73 (95% CI: 0.52–1.00) | 0.05 | 15 | ||||
| Wang et al. (2019) | CM | 1. Bone marrow-derived cell therapy 2. Control, no cell therapy | Effect of cell therapy on 6MWT result | 3–60 months | Studies n = 9 Mean difference increase of 53.13 m (95% CI: 25.47–81.10) | 0.0002 | NR | [75] |
| 3 months | Studies n = 6 Mean difference increase of 47.92 m (95% CI: 7.95–87.89) | 0.02 | NR | |||||
| 6 months | Studies n = 8 Mean difference increase of 49.68 m (95% CI: 3.34–96.01) | 0.04 | NR | |||||
| ≥12 months | Studies n = 6 Mean difference increase of 63.91 m (95% CI: 0.06–127.76) | 0.05 | NR | |||||
| Effect of cell therapy on MACE | 3–60 months | Studies n = 6 RR: 0.79 (95% CI: 0.60–1.04) | 0.09 | NR | ||||
| Effect of cell therapy on all-cause mortality | 3–60 months | Studies n = 17 RR: 0.74 (95% CI: 0.56–0.98) | 0.04 | NR | ||||
| Effect of cell therapy on cardiac-related death | 3–60 months | Studies n = 8 RR: 0.65 (95% CI: 0.29–1.46) | 0.29 | NR | ||||
| Effect of cell therapy on re-hospitalization | 3–60 months | Studies n = 5 RR: 0.71 (95% CI: 0.49–1.04) | 0.08 | NR | ||||
| Effect of cell therapy on quality of life (MLHFQ score) | 3–60 months | Studies n = 4 Mean difference reduction of 18.41 (95% CI:-29.90 to -6.92) | 0.02 | NR | ||||
| Jiao et al. (2014) | DCM | 1. Cell therapy (CD34+ stem cell therapy, BMMC or BMSC and mononuclear cells) 2. Control, no cell therapy | Effect of cell therapy on 6MWT result | Mean: 19.8 months | Studies n = 5 Mean difference increase of 132.12 m (95% CI: 88.15–176.09) | <0.01 | 89 | [73] |
| Effect of cell therapy on mortality or heart transplant | Mean: 19.8 months | Studies n = 7 OR: 0.48 (95% CI: 0.29–0.80) | <0.01 | 0 | ||||
| Diaz-Navarro et al. (2021) | NIDCM | 1. Stem cell therapy (any type) 2. Control, no intervention/no sham intervention | Effect of cell therapy on 6MWT result | 6 months to 5 years | Studies n = 5 Mean difference increase of 70.12 m (95% CI: -5.28 to 145.51) | 0.07 | 87 | [72] |
| Effect of cell therapy on all-cause mortality | 6 months to 5 years | Studies n = 7 RR: 0.84 (95% CI: 0.54–1.31) | 0.44 | 0 | ||||
| Effect of cell therapy on quality of life | 6 months to 5 years | Studies n = 5 Standard mean difference of 0.62 (95% CI: 0.01–1.31) | 0.05 | 80 | ||||
| 1. Stem cell therapy (any type) 2. Control, peripheral therapy with granulocyte colony-stimulating factor | Effect of cell therapy on 6MWT result | 6 months to 5 years | Studies n = 2 Mean difference increase of 140.14 m (95% CI: 119.51–160.77) | <0.01 | 0 | |||
| Effect of cell therapy on all-cause mortality | 6 months to 5 years | Studies n = 3 RR: 0.46 (95% CI: 0.16–1.31) | 0.15 | 39 | ||||
| Effect of cell therapy on quality of life | 6 months to 5 years | Studies n = 1 Standard mean difference: 4.61 (95% CI: -5.62 to 14.83) | 0.38 | NR | ||||
| Rong et al. (2020) | DCM | 1. Stem cell therapy (any type) 2. Control, no cell therapy | Effect of stem cell therapy on 6MWT result | 12 to 60 months | Studies n = 5 Weighted mean difference increase of 51.52 m (95% CI: -24.21 to 127.55) | NR | 94.8 | [77] |
| Effect of stem cell therapy on mortality | 12 to 60 months | Studies n = 8 RR: 0.72 (95% CI: 0.50–1.02) | NR | 30.2 |
6MWT: Six-minute walk test; BMMC: Bone marrow mononuclear cell; BMSC: Bone marrow mesenchymal cell; CI: Confidence interval; CM: Cardiomyopathy; DCM: Dilated cardiomyopathy; MACE: Major adverse cardiovascular events; MLHFQ: Minnesota Living with Heart Failure Questionnaire; NICM: Non-ischemic cardiomyopathy; NIDCM: Non-ischemic dilated cardiomyopathy; NR: Not reported; OR: Odds ratio; RR: Risk ratio.
Discussion
The clinical studies in this SLR included measured 6MWT and outcomes from diverse forms of CM across a broad age range from pediatric patients to older adult patients. In addition, the clinical studies measuring 6MWT and outcomes also report diverse causes of CM, including genetic, idiopathic, peripartum and both ischemic and non-ischemic causes. Despite major differences in patient characteristics and disease courses, the association of 6MWT with outcomes appears to hold even if the actual numbers (baseline or change from baseline) cannot be compared between types of CM or studies with different patient populations.
The application of the 6MWT in clinical studies highlights how diverse pathophysiological mechanisms and disease severity can impact functional capacity. Collectively, the publications which investigated the association between the 6MWT and hospitalization or mortality show that an increase in 6MWT result (or at least a smaller decrease compared with the control group) is a prognostic indicator of a reduced risk of hospitalization or mortality for patients with CM overall [14,39,47,48,58,65].
Specifically, for ATTR-CM, a low 6MWT was reported to be a predictor of CV-related hospitalization [65]. Similarly, in this patient population, the 6MWT was found to be a predictor of mortality for patients with ATTR-CM, with a greater 6MWT distance at baseline reported to be associated with a reduction in risk of mortality in these patient populations [14,65]. Vong et al. reported that a 6MWT distance of 445 meters was associated both with a 15% reduction in risk of CV-related hospitalization and a 40% reduction in risk of death compared with a 6MWT of 351 meters [65]. This implies that a greater 6MWT distance is associated with a greater reduction in the risk of death relative to the reduction in the risk of CV-related hospitalization in patients with ATTR-CM.
The 6MWT was also reported to be significantly associated with hospitalization and mortality in patients with DCM [39,48,58], as well as subsequent cardiac events in patients with either ICM or NICM [47].
Due to inconsistencies in the reporting of 6MWT data between studies, it would be inappropriate to draw comparative conclusions between the predictive potential of the 6MWT in different subtypes of CM. However, collectively, the publications identified within this SLR do suggest an association between 6MWT and the outcomes of interest across subtypes of CM, including ATTR-CM (both ATTRv-CM and wtATTR-CM), DCM, ICM and NICM.
The 6MWT has been used as a clinical end point in recent and ongoing clinical trials investigating novel therapeutic interventions for patients with ATTR-CM [45,78,79]. Recent guidelines published on ATTRv amyloidosis have supported the use of the 6MWT, alongside other measures, for monitoring disease progression and response to therapy in patients with ATTRv-CM [29,30,80]. Guidelines support a decline in 6MWT as being reflective of disease progression [28]. This SLR identified four separate studies investigating therapeutic interventions in patients with ATTR-CM, including the ATTR-ACT study [12,14,45,56]. These studies reported 6MWT distances for patients with ATTR-CM (260–400 m) that largely lie within the accepted range for being a strong prognostic indicator for patients with HF (300–490 m) [66].
Despite reports that the rate of 6MWT decline is similar between untreated patients with wtATTR and ATTRv amyloidosis [69], differences between the ATTR-CM subpopulations of wtATTR and ATTRv amyloidosis need to be considered when interpreting the relevance of 6MWT for predicting hospitalization or mortality. One such difference is that patients with wtATTR amyloidosis have typically been diagnosed later in life relative to ATTRv amyloidosis, with the average age of wtATTR diagnosis being 77 years of age compared with 71.2 years and 65 years for ATTRv-V122I and ATTRv-T60A, respectively [80]. Adjusting for these differences using measures such as the percentage of predicted 6MWT could be beneficial for facilitating comparisons and meaningful interpretations within the ATTR-CM population [81]. Future ATTR-CM clinical trials may present different 6MWT results to those identified as part of this review due to populations receiving improved medical management or earlier diagnosis of ATTR-CM. However, it is expected that the association between 6MWT and mortality would remain the same.
The studies that independently reported 6MWT data and hospitalization or mortality outcomes also show that improvements in 6MWT distance were associated with reduced hospitalization and mortality for patients with CM; although, some studies were not consistent with this finding. Speculative explanations as to why these contradicting studies did not support the expected trend include heterogeneity in comorbidities between patient groups, limited sample sizes and a potentially confounding influence of therapeutic intervention on the outcomes of interest [42,43,59,61,63,64].
The relationship between the 6MWT and patient quality of life was not the primary focus for this review; however, the importance of patient quality of life is becoming increasingly realized [82]. Based on the publications included in this review, a greater 6MWT distance may be associated with a better quality of life. The two main quality of life measures employed by the identified publications included the Kansas City Cardiomyopathy Questionnaire (n = 9) [12,14,45,56,57,68–71], and the Minnesota Living with Heart Failure Questionnaire assessment (n = 7) [42,44,51,57,60,63,75]. An assessment of which quality of life measure is the most appropriate in this population, and the consistency in which quality of life measures are used between studies, will facilitate any future work in investigating the relationship between 6MWT and patient quality of life.
In this review, there was a large degree of heterogeneity among the included publications in terms of the number and range of comorbidities, interventions, patient age and study design. Several publications were for studies of observational design, thus lacking the methodological rigor required for external validity, and cannot be considered generalizable. Most publications were not intended to investigate the specific objective of this review, typically reporting 6MWT data alongside hospitalization or mortality data. Consequently, there were often differences in 6MWT approaches and reporting of 6MWT data. In addition, the 6MWT result can be impacted by factors independent to cardiopulmonary health, including, age, sex, body mass index, or methodological factors such as the length of test track used and patient encouragement [22,83,84]. It has been demonstrated that these factors are independently associated with the 6MWT distance, likely a result of a decline in musculoskeletal strength, which is typically associated with aging, and a greater burden of age-related comorbidities [5]. Therefore, the heterogeneity of the disease introduces difficulties for combining and comparing the reported 6MWT between these studies and should also be taken into consideration when interpreting the findings of this review. Many studies were aimed to primarily investigate the impact of therapeutic intervention. However, the change in 6MWT distance following therapeutic intervention can be differentially effective for predicting outcomes depending on the patient population [83] and is another area that requires further research in specific CM populations, including ATTR-CM. Finally, improvements in non-invasive diagnostic tools present an opportunity for systematic screening of high-risk populations and earlier ATTR-CM diagnosis in the real-world setting [85,86]. It should be noted that patients with an earlier ATTR-CM diagnosis may not have severe CV impairment, and thus the prognostic value of the 6MWT may be reduced in this population. To support future use of the 6MWT as a prognostic indicator in the clinic, it may be more appropriate to combine the 6MWT with other surrogate end points, a practice considered suitable for use in HF clinical trials [28], for the generation of a singular, more sensitive composite score.
The 6MWT is an established measure of functional capacity and accepted as a predictor of hospital readmission and mortality, and the findings of this review are largely consistent with observations found in the broader population of patients with HF [3,66,87]. While several studies collecting 6MWT data and hospitalization or mortality measures have established the 6MWT as a measure of functional capacity for HF populations, there is a need to conduct studies that directly investigate the relationship between these outcomes in patients with CM, and additional high-quality and population-specific research is also required in patients with CM and its subtypes, such as ATTR-CM. A more standardized approach across the field for collecting, reporting and analyzing 6MWT data would be beneficial for forming relevant conclusions. Considering the sensitivity of the 6MWT to confounding factors [22], the reporting of adjusted 6MWT data, such as the percentage of predicted 6MWT, would facilitate the drawing of more definitive conclusions [81]. Standardizing the methodology for reporting 6MWT could lead to better support for the use of the 6MWT as a meaningful clinical end point for patients with CM and ATTR-CM, as it is currently for patients with HF.
Conclusion
The publications identified as part of this SLR highlight that patients with CM, including subtypes such as ATTR-CM, who have a greater distance at baseline or a smaller decline in 6MWT, are likely to report a reduced risk of hospitalization and mortality. The independent collection of 6MWT data alongside hospitalization or mortality outcomes appears to be commonplace for studies in patients with CM. Wider acceptance of 6MWT as an end point in CM studies could accelerate the development of new treatments that improve the lives of patients provided that the study reasonably excludes the possibility of harm. The association of 6MWT with outcomes bolsters confidence in this approach. An efficient approach to trial design is especially important for CMs like ATTR-CM that have a high unmet need.
Summary points
•
Restricting primary end points in clinical trials to hospitalizations and mortality alone limits insight into the impact of a clinical intervention on a patient's functional capacity.
•
The six-minute walk test (6MWT) is a practical assessment with proven relevance as a clinical measure in some cardiovascular populations and has benefit as a prognostic indicator in cardiomyopathy and its subtypes, including transthyretin-mediated amyloidosis with cardiomyopathy.
•
The 6MWT is utilized as a measure of functional capacity and end point in cardiomyopathy clinical trials.
•
The publications identified as part of this systematic review show that patients with cardiomyopathy who have a greater distance at baseline or a smaller decline in six-minute walk test are likely to report a reduced risk of hospitalization and mortality.
•
Studies that use the 6MWT as an end point while collecting adequate safety data would bring new therapies sooner to improve patient lives.
•
The association of 6MWT with outcomes further bolsters confidence in more efficient study designs, especially when there is a high unmet need.
Author contributions
A Yilmaz, J Nativi-Nicolau, N Dasgupta and R Zolty provided expert guidance including conceptualization and review of the protocol, results and interpretation. C Summers and J Luth provided conceptualization and review of the protocol, results and interpretation. R Macey, J Cochrane and J Peatman conducted the review of the literature, developed the protocol and drafted the manuscript. All authors were involved in the review process and signed off on the manuscript content.
Acknowledgments
The authors would like to thank and acknowledge P Lavelle, L Heron and F Howells from Adelphi Values PROVE™ for their support in conducting the literature review and drafting and revising content.
Financial disclosure
This study was funded by Alnylam Pharmaceuticals. Adelphi Values PROVE™ received funding from Alnylam Pharmaceuticals for the conduct of the review, from development of the systematic review methodology through to overseeing the final formatting and manuscript submission processes. A Yilmaz has participated in advisory boards for Alnylam Pharmaceuticals, BridgeBio, GE and Pfizer, and has research collaborations with Circle Imaging and Phillips. J Nativi-Nicolau institutions have received research funding from Alnylam Pharmaceuticals, Ionis/Akcea and Pfizer, and has participated in advisory boards for Alnylam Pharmaceuticals, Ionis/Akcea and Pfizer. N Dasgupta has participated in advisory boards for Eidos, Intellia, Ionis/Akcea and Pfizer, and has been a speaker for Alnylam Pharmaceuticals and Pfizer. R Zolty has participated in advisory boards for Alnylam Pharmaceuticals, Bayer, Johnson & Johnson and United Therapeutics. C Summers and J Luth are employees of Alnylam Pharmaceuticals. R Macey, J Cochrane and J Peatman are employees of Adelphi Values PROVE™. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Data sharing statement
Data for this manuscript were from published studies, all of which have been cited appropriately in text and tables.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 152.60 KB
References
Papers of special note have been highlighted as: • of interest
1.
Bittner V, Weiner DH, Yusuf S et al. Prediction of mortality and morbidity with a 6-minute walk test in patients with left ventricular dysfunction. JAMA 270(14), 1702–1707 (1993).
2.
Casanova C, Celli BR, Barria P et al. The 6-min walk distance in healthy subjects: reference standards from seven countries. Eur. Respir. J. 37(1), 150–156 (2011).
3.
McCabe N, Butler J, Dunbar SB, Higgins M, Reilly C. Six-minute walk distance predicts 30-day readmission after acute heart failure hospitalization. Heart Lung 46(4), 287–292 (2017).
4.
Spertus JA, Jones PG, Sandhu AT, Arnold SV. Interpreting the Kansas City Cardiomyopathy Questionnaire in clinical trials and clinical care: JACC state-of-the-art review. J. Am. Coll. Cardiol. 76(20), 2379–2390 (2020).
5.
Enright PL, Sherrill DL. Reference equations for the six-minute walk in healthy adults. Am. J. Respir. Crit. Care Med. 158(5), 1384–1387 (1998).
6.
Forman DE, Arena R, Boxer R et al. Functional capacity as a principal end point for therapies oriented to older adults with cardiovascular disease: a scientific statement for healthcare professionals from the American Heart Association. Circulation 135(16), e894–e918 (2017).
7.
Fiuzat M, Lowy N, Stockbridge N et al. Endpoints in heart failure drug development: history and future. JACC. Heart. Fail. 8(6), 429–440 (2020).
8.
European Medicines Agency. Guideline on clinical investigation of medicinal products for the treatment of chronic heart failure (2017). https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-chronic-heart-failure-revision-2_en.pdf (Accessed: 16 April 2023).
9.
Ruberg FL, Grogan M, Hanna M, Kelly JW, Maurer MS. Transthyretin amyloid cardiomyopathy: JACC state-of-the-art review. J. Am. Coll. Cardiol. 73(22), 2872–2891 (2019).
10.
Ruberg FL, Berk JL. Transthyretin (TTR) cardiac amyloidosis. Circulation 126(10), 1286–1300 (2012).
11.
Narotsky DL, Castano A, Weinsaft JW, Bokhari S, Maurer MS. Wild-type transthyretin cardiac amyloidosis: novel insights from advanced imaging. Can. J. Cardiol. 32(9), 1166.e1–1166.e10 (2016).
12.
Ruberg FL, Maurer MS, Judge DP et al. Prospective evaluation of the morbidity and mortality of wild-type and V122I mutant transthyretin amyloid cardiomyopathy: the Transthyretin Amyloidosis Cardiac Study (TRACS). Am. Heart J. 164(2), 222–228.e1 (2012).
13.
Connors LH, Sam F, Skinner M et al. Heart failure resulting from age-related cardiac amyloid disease associated with wild-type transthyretin: a prospective, observational cohort study. Circulation 133(3), 282–290 (2016).
14.
Lane T, Fontana M, Martinez-Naharro A et al. Natural history, quality of life, and outcome in cardiac transthyretin amyloidosis. Circulation 140(1), 16–26 (2019).
• Association between six-minute walk test (6MWT) and mortality reported.
15.
Pinney JH, Whelan CJ, Petrie A et al. Senile systemic amyloidosis: clinical features at presentation and outcome. J. Am. Heart. Assoc. 2(2), e000098 (2013).
16.
Sattianayagam PT, Hahn AF, Whelan CJ et al. Cardiac phenotype and clinical outcome of familial amyloid polyneuropathy associated with transthyretin alanine 60 variant. Eur. Heart J. 33(9), 1120–1127 (2012).
17.
Grogan M, Scott CG, Kyle RA et al. Natural history of wild-type transthyretin cardiac amyloidosis and risk stratification using a novel staging system. J. Am. Coll. Cardiol. 68(10), 1014–1020 (2016).
18.
Aus dem Siepen F, Bauer R, Voss A et al. Predictors of survival stratification in patients with wild-type cardiac amyloidosis. Clin. Res. Cardiol. 107(2), 158–169 (2018).
19.
Givens RC, Russo C, Green P et al. Comparison of cardiac amyloidosis due to wild-type and V122I transthyretin in older adults referred to an academic medical center. Aging Health 9(2), 229–235 (2013).
20.
Gillmore JD, Damy T, Fontana M et al. A new staging system for cardiac transthyretin amyloidosis. Eur. Heart J. 39(30), 2799–2806 (2018).
21.
Heidenreich PA, Bozkurt B, Aguilar D et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 79(17), e263–e421 (2022).
22.
ATS Board Of Directors. ATS statement: guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 166(1), 111–117 (2002).
23.
Ingle L, Cleland JG, Clark AL. The long-term prognostic significance of 6-minute walk test distance in patients with chronic heart failure. BioMed. Res. Int. 505969 (2014).
24.
Kamiya K, Hamazaki N, Matsue Y et al. Gait speed has comparable prognostic capability to six-minute walk distance in older patients with cardiovascular disease. Eur. J. Prev. Cardiol. 25(2), 212–219 (2018).
25.
Wegrzynowska-Teodorczyk K, Rudzinska E, Lazorczyk M et al. Distance covered during a six-minute walk test predicts long-term cardiovascular mortality and hospitalisation rates in men with systolic heart failure: an observational study. J. Physiother. 59(3), 177–187 (2013).
26.
Cohen OC, Sathyanath A, Ravichandran S et al. The prognostic importance of the 6-minute walk test in AL amyloidosis. Blood 136, 16–17 (2020).
27.
Pulido V, Doros G, Berk JL, Sanchorawala V. The six-minute walk test in patients with AL amyloidosis: a single centre case series. Br. J. Haematol. 177(3), 388–394 (2017).
28.
Ferreira JP, Duarte K, Graves TL et al. Natriuretic peptides, 6-min walk test, and quality-of-life questionnaires as clinically meaningful endpoints in HF trials. J. Am. Coll. Cardiol. 68(24), 2690–2707 (2016).
• 6MWT recommended as a clinically meaningful end point for use in HF clinical trials in combination with other measures.
29.
Ando Y, Adams D, Benson MD et al. Guidelines and new directions in the therapy and monitoring of ATTRv amyloidosis. Amyloid 29(3), 143–155 (2022).
• Supports the use of 6MWT in ATTRv-CM.
30.
Garcia-Pavia P, Bengel F, Brito D et al. Expert consensus on the monitoring of transthyretin amyloid cardiomyopathy. Eur. J. Heart. Fail. 23(6), 895–905 (2021).
31.
Oginezawa S, Ishihara T, Iwafuchi Y, Hatano Y, Kashimura K, Onodera O. ATTRv amyloidosis with early improvement demonstrated by the 6-minute walk test following Patisiran therapy: a case report. Clin. Neurol. 62(5), 375–379 (2022).
32.
Yungher FW, Kim A, Boehme A et al. Peripheral neuropathy symptoms in wild type transthyretin amyloidosis. J. Peripher. Nerv. Syst. 25(3), 265–272 (2020).
33.
Food and Drug Administration. Treatment for heart failure: endpoints for drug development guidance for industry (2019). https://www.fda.gov/regulatory-information/search-fda-guidance-documents/treatment-heart-failure-endpoints-drug-development-guidance-industry (Accessed: 16 April 2024).
34.
Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
35.
Akl E, Altman DG, Aluko P et al. Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons, NJ, USA (2019).
36.
Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. Based. Healthc. 13(3), 147–153 (2015).
37.
Ambrosy AP, Stevens SR, Al-Khalidi HR et al. Burden of medical co-morbidities and benefit from surgical revascularization in patients with ischaemic cardiomyopathy. Eur. J. Heart. Fail. 21(3), 373–381 (2019).
38.
Bielecka-Dabrowa A, von Haehling S, Aronow WS, Ahmed MI, Rysz J, Banach M. Heart failure biomarkers in patients with dilated cardiomyopathy. Int. J. Cardiol. 168(3), 2404–2410 (2013).
39.
den Boer SL, Flipse DHK, van der Meulen MH et al. Six-minute walk test as a predictor for outcome in children with dilated cardiomyopathy and chronic stable heart failure. Pediatr. Cardiol. 38(3), 465–471 (2017).
40.
Domae K, Miyagawa S, Yoshikawa Y et al. Clinical outcomes of autologous stem cell-patch implantation for patients with heart failure with nonischemic dilated cardiomyopathy. J. Am. Heart. Assoc. 10(13), e008649 (2021).
41.
Hajahmadi M, Shemshadi S, Khalilipur E et al. Muscle wasting in young patients with dilated cardiomyopathy. J. Cachexia Sarcopenia Muscle 8(4), 542–548 (2017).
42.
Heldman AW, DiFede DL, Fishman JE et al. Transendocardial mesenchymal stem cells and mononuclear bone marrow cells for ischemic cardiomyopathy: the TAC-HFT randomized trial. JAMA 311(1), 62–73 (2014).
43.
Kainuma S, Miyagawa S, Toda K et al. Long-term outcomes of autologous skeletal myoblast cell-sheet transplantation for end-stage ischemic cardiomyopathy. Mol. Ther. 29(4), 1425–1438 (2021).
44.
Martino H, Brofman P, Greco O et al. Multicentre, randomized, double-blind trial of intracoronary autologous mononuclear bone marrow cell injection in non-ischaemic dilated cardiomyopathy (the dilated cardiomyopathy arm of the MiHeart study). Eur. Heart J. 36(42), 2898–2904 (2015).
45.
Maurer MS, Schwartz JH, Gundapaneni B et al. Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N. Engl. J. Med. 379(11), 1007–1016 (2018).
46.
Miyagawa S, Domae K, Yoshikawa Y et al. Phase I clinical trial of autologous stem cell-sheet transplantation therapy for treating cardiomyopathy. J. Am. Heart. Assoc. 6(4), e003918 (2017).
47.
Toledo CC, Schwartzmann PV, Silva LM et al. Serum potassium levels provide prognostic information in symptomatic heart failure beyond traditional clinical variables. ESC. Heart. Fail. 8(3), 2133–2143 (2021).
• Association between 6MWT and MACE reported.
48.
van der Meulen MH, den Boer S, du Marchie Sarvaas GJ et al. Does repeated measurement of a 6-min walk test contribute to risk prediction in children with dilated cardiomyopathy? Pediatr. Cardiol. 41(2), 223–229 (2020).
• Association between 6MWT and mortality reported.
49.
Godino C, Scotti A, Taramasso M et al. Two-year cardiac mortality after MitraClip treatment of functional mitral regurgitation in ischemic and non-ischemic dilated cardiomyopathy. Int. J. Cardiol. 269, 33–39 (2018).
50.
Hare JM, DiFede DL, Rieger AC et al. Randomized comparison of allogeneic versus autologous mesenchymal stem cells for nonischemic dilated cardiomyopathy: POSEIDON-DCM trial. J. Am. Coll. Cardiol. 69(5), 526–537 (2017).
51.
Henry TD, Traverse JH, Hammon BL et al. Safety and efficacy of ixmyelocel-T: an expanded, autologous multi-cellular therapy, in dilated cardiomyopathy. Circ. Res. 115(8), 730–737 (2014).
52.
Trifunovic Z, Obradovic S, Balint B et al. Functional recovery of patients with ischemic cardiomyopathy treated with coronary artery bypass surgery and concomitant intramyocardial bone marrow mononuclear cell implantation—a long-term follow-up study. Vojnosanit. Pregl. 72(3), 225–232 (2015).
53.
Vrtovec B, Poglajen G, Lezaic L et al. Effects of intracoronary CD34+ stem cell transplantation in nonischemic dilated cardiomyopathy patients: 5-year follow-up. Circ. Res. 112(1), 165–173 (2013).
54.
Vrtovec B, Sever M, Domanovic D et al. Long-term effects of stem cell transplantation in heart failure. Zdrav. Vestn. 81, 373–383 (2012).
55.
Xiao W, Guo S, Gao C et al. A randomized comparative study on the efficacy of intracoronary infusion of autologous bone marrow mononuclear cells and mesenchymal stem cells in patients with dilated cardiomyopathy. Int. Heart J. 58(2), 238–244 (2017).
56.
Judge DP, Kristen AV, Grogan M et al. Phase III multicenter study of Revusiran in patients with hereditary transthyretin-mediated (hATTR) amyloidosis with cardiomyopathy (ENDEAVOUR). Cardiovasc. Drugs Ther. 34(3), 357–370 (2020).
57.
Abraham WT, Aggarwal S, Prabhu SD et al. Ambulatory extra-aortic counterpulsation in patients with moderate to severe chronic heart failure. JACC. Heart Fail. 2(5), 526–533 (2014).
58.
Bielecka-Dabrowa A, Mikhailidis DP, Rizzo M, von Haehling S, Rysz J, Banach M. The influence of atorvastatin on parameters of inflammation left ventricular function, hospitalizations and mortality in patients with dilated cardiomyopathy – 5-year follow-up. Lipids Health Dis. 12, 47 (2013).
• Association between 6MWT and hospitalization reported.
59.
Frljak S, Jaklic M, Zemljic G, Cerar A, Poglajen G, Vrtovec B. CD34(+) cell transplantation improves right ventricular function in patients with nonischemic dilated cardiomyopathy. Stem Cells Transl. Med. 7(2), 168–172 (2018).
60.
Kuschyk J, Nagele H, Heinz-Kuck K et al. Cardiac contractility modulation treatment in patients with symptomatic heart failure despite optimal medical therapy and cardiac resynchronization therapy (CRT). Int. J. Cardiol. 277, 173–177 (2019).
61.
Leyva F, Umar F, Taylor RJ, Steeds RP, Frenneaux MP. The clinical outcome of cardiac resynchronization therapy in post-surgical valvular cardiomyopathy. Europace 18(5), 732–738 (2016).
62.
Ma G, Chen L, Yue Y et al. Impact of autoantibodies against the M2-muscarinic acetylcholine receptor on clinical outcomes in peripartum cardiomyopathy patients with standard treatment. BMC Cardiovasc. Disord. 21(1), 619 (2021).
63.
Sant'Anna RT, Fracasso J, Valle FH et al. Direct intramyocardial transthoracic transplantation of bone marrow mononuclear cells for non-ischemic dilated cardiomyopathy: INTRACELL, a prospective randomized controlled trial. Rev. Bras. Cir. Cardiovasc. 29(3), 437–447 (2014).
64.
Vrtovec B, Poglajen G, Sever M et al. Effects of repetitive transendocardial CD34(+) cell transplantation in patients with nonischemic dilated cardiomyopathy. Circ. Res. 123(3), 389–396 (2018).
65.
Vong C, Boucher M, Riley S et al. Modeling of survival and frequency of cardiovascular-related hospitalization in patients with transthyretin amyloid cardiomyopathy treated with Tafamidis. Am. J. Cardiovasc. Drugs. 21(5), 535–543 (2021).
• Association between 6MWT and hospitalization and mortality reported.
66.
Pollentier B, Irons SL, Benedetto CM et al. Examination of the six minute walk test to determine functional capacity in people with chronic heart failure: a systematic review. Cardiopulm. Phys. Ther. J. 21(1), 13–21 (2010).
67.
Henricson E, Abresch R, Han JJ et al. Percent-predicted 6-minute walk distance in Duchenne muscular dystrophy to account for maturational influences. PloS Curr. 4, RRN1297 (2012).
68.
Rapezzi C, Kristen AV, Gundapaneni B, Sultan MB, Hanna M. Benefits of tafamidis in patients with advanced transthyretin amyloid cardiomyopathy. Eur. Heart J. 41, ehaa946.2115 (2020).
69.
Nativi-Nicolau J, Judge DP, Hoffman JE et al. Natural history and progression of transthyretin amyloid cardiomyopathy: insights from ATTR-ACT. ESC Heart Fail. 8(5), 3875–3884 (2021).
70.
Rapezzi C, Elliott P, Damy T et al. Efficacy of tafamidis in patients with hereditary and wild-type transthyretin amyloid cardiomyopathy: further analyses from ATTR-ACT. JACC Heart Fail. 9(2), 115–123 (2021).
71.
Maurer MS, Adler E, Gundapaneni B, Sultan MB, Rapezzi C. Efficacy of tafamidis by baseline 6-minute walk test distance in the tafamidis in transthyretin cardiomyopathy clinical trial (ATTR-ACT). J. Card. Fail. 26(10), S10 (2020).
72.
Diaz-Navarro R, Urrutia G, Cleland J Gf et al. Stem cell therapy for dilated cardiomyopathy. Cochrane Database Syst. Rev. 7(7), CD013433 (2021).
73.
Jiao R, Liu Y, Yang W-J, Zhu X-Y, Li J, Tang Q-Z. Effects of stem cell therapy on dilated cardiomyopathy. Saudi. Medical J. 35(12), 1463–1468 (2014).
74.
Lu Y, Wang Y, Lin M et al. A systematic review of randomised controlled trials examining the therapeutic effects of adult bone marrow-derived stem cells for non-ischaemic dilated cardiomyopathy. Stem Cell Res. Ther. 7(1), 186 (2016).
75.
Wang C, Li J, Zhang B, Li Y. Safety and efficacy of bone marrow-derived cells therapy on cardiomyopathy: a meta-analysis. Stem Cell Res. Ther. 10(1), 137 (2019).
76.
Xia L, Zeng L, Pan J, Ding Y. Effects of stem cells on non-ischemic cardiomyopathy: a systematic review and meta-analysis of randomized controlled trials. Cytotherapy 22(12), 699–711 (2020).
77.
Rong S-L, Wang Z-K, Zhou X-D, Wang X-L, Yang Z-M, Li B. Efficacy and safety of stem cell therapy in patients with dilated cardiomyopathy: a systematic appraisal and meta-analysis. J. Transl. Med. 17, 221 (2019).
78.
Benson MD, Dasgupta NR, Rissing SM, Smith J, Feigenbaum H. Safety and efficacy of a TTR specific antisense oligonucleotide in patients with transthyretin amyloid cardiomyopathy. Amyloid 24(4), 217–223 (2017).
79.
ClinicalTrials.gov. APOLLO-B: a study to evaluate patisiran in participants with transthyretin amyloidosis with cardiomyopathy (ATTR amyloidosis with cardiomyopathy) (2022). https://www.clinicaltrials.gov/ct2/show/NCT03997383 (Accessed: 16 April 2024).
80.
Goyal A, Lahan S, Dalia T et al. Clinical comparison of V122I genotypic variant of transthyretin amyloid cardiomyopathy with wild-type and other hereditary variants: a systematic review. Heart. Fail. Rev. 27(3), 849–856 (2022).
81.
Lee W-TN, Peacock AJ, Johnson MK. The role of per cent predicted 6-min walk distance in pulmonary arterial hypertension. Eur. Respir. J. 36(6), 1294–1301 (2010).
82.
Hamo CE, Gheorghiade M, Butler J. Novel endpoints for heart failure clinical trials. Curr. Heart. Fail. Rep. 14(4), 210–216 (2017).
83.
Heresi GA, Dweik RA. Strengths and limitations of the six-minute-walk test: a model biomarker study in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 183(9), 1122–1124 (2011).
84.
Klein SR, Gulart AA, Venancio RS et al. Performance difference on the six-minute walk test on tracks of 20 and 30 meters for patients with chronic obstructive pulmonary disease: validity and reliability. Braz. J. Phys. Ther. 25(1), 40–47 (2021).
85.
Porcari A, Merlo M, Rapezzi C, Singara G. Transthyretin amyloid cardiomyopathy: an uncharted territory awaiting discovery. Eur. J. Intern. Med. 82, 7–15 (2020).
86.
Witteles RM, Bokhari S, Damy T et al. Screening for transthyretin amyloid cardiomyopathy in everyday practice. JACC Heart Fail. 7(8), 709–716 (2019).
87.
Grundtvig M, Eriksen-Volnes T, Orn S, Slind EK, Gullestad L. 6 min walk test is a strong independent predictor of death in outpatients with heart failure. ESC Heart Fail. 7(5), 2904–2911 (2020).
Information & Authors
Information
Published In
Copyright
© 2024 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 19 October 2023
Accepted: 20 May 2024
Published online: 13 June 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Six-minute walk test as clinical end point in cardiomyopathy clinical trials, including ATTR-CM: a systematic literature review. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0158
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ahmad Masri, Francesco Cappelli, Margot K. Davis, Marianna Fontana, Pablo Garcia-Pavia, Julian D. Gillmore, Mazen Hanna, Laura Obici, Scott D. Solomon, Brett W. Sperry, Nobuhiro Tahara, Márcia Waddington-Cruz, Arnt V. Kristen, Rodney H. Falk, Sanjiv J. Shah, Jose Nativi-Nicolau, Nicholas J. Viney, Qingqing Yang, Jersey Chen, Sotirios Tsimikas, Mathew S. Maurer, Rationale and Design of CARDIO-TTRansform, a Phase 3 Trial of Eplontersen in Transthyretin Amyloid Cardiomyopathy, Circulation: Heart Failure, 10.1161/CIRCHEARTFAILURE.126.014205, 19, 6, (2026).
- Qiuqi Zhang, Jinhe Zhao, Li Ma, Haizhen Jia, Jie Zhen, Research on the effect of augmented reality based sensory interaction device in rehabilitation training of patients with chronic heart failure, BMC Cardiovascular Disorders, 10.1186/s12872-026-05625-y, 26, 1, (2026).
- Yen-Hung Lin, Hsu-Wen Chou, Sarah Tsai, Roy Gomez, Real-World Characteristics and Treatment Patterns of Patients With Transthyretin Amyloid Cardiomyopathy: Protocol for a Multicountry Disease Registry Study, JMIR Research Protocols, 10.2196/71314, 14, (e71314), (2025).
- Farooq H. Sheikh, Gilbert Habib, W.H. Wilson Tang, Julian D. Gillmore, Ugochukwu O. Egolum, Simone Longhi, Chongshu Chen, Emre Aldinc, Marianna Fontana, Impact of Vutrisiran on Functional Capacity and Quality of Life in Transthyretin Amyloidosis With Cardiomyopathy, Journal of the American College of Cardiology, 10.1016/j.jacc.2025.03.454, 85, 20, (1943-1955), (2025).
- Isabel Carvajal, Luis Caballero Hortiales, Valeria Rojo Galicia, Denka Durán Aguilar, Erick Alexanderson, Six-Minute Walk Test in Patients with Cardiac Amyloidosis: Does it mean anything?, International Journal of Cardiovascular Sciences, 10.36660/ijcs.20240205, 38, (2025).