Real-world assessment of treatment inertia in the management of patients treated for major depressive disorder in the USA
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Major depressive disorder (MDD) is a debilitating illness in which depressive symptoms may persist after treatment. Treatment inertia is the continued use of the same pharmacotherapy regimen when treatment goals are not met. This study assessed the frequency of treatment inertia among adult patients with MDD treated in a real-world setting. Patients & methods: This was a retrospective, observational study of patients with MDD identified in the Decision Resources Group Real World Evidence US Data Repository from January 2014 to June 2018. Patients (≥18 years) had an elevated Patient Health Questionnaire-9 (PHQ-9) score (≥5) following 8 weeks of stable baseline antidepressant use with/without mental-health outpatient therapy. Treatment inertia, modification and discontinuation were evaluated over a 16-week follow-up period (timeline based on the APA Practice Guidelines). The primary outcome was the proportion of MDD patients experiencing treatment inertia. Results: 2850 patients (median age, 55 years; 74% female) met the study criteria. Of these patients, 834 (29%) had study-defined treatment inertia, 1534 (54%) received treatment modification and 482 (17%) discontinued treatment. Use of mirtazapine (Odd ratio [OR]: 0.63; 95% confidence interval [CI]: 0.50–0.79), selective serotonin reuptake inhibitors (OR: 0.64; 95% CI: 0.54–0.75) or bupropion (OR: 0.71; 95% CI: 0.60–0.84) in the baseline period was associated with an increased likelihood of treatment modification versus not receiving treatment with these medications. Frequency of treatment inertia may differ among those who do not have a documented PHQ-9 score. Conclusion: Effective symptom management is critical for optimal outcomes in MDD. Results demonstrate that treatment inertia is common in MDD despite guidelines recommending treatment modification in patients not reaching remission.
Tweetable abstract
This real-world, observational study showed that treatment inertia (continued use of the same treatment when remission goals are not met) is common in major depressive disorder, occurring in about 1 in 3 patients with unresolved symptoms.
Plain language summary
Major depressive disorder (MDD) is a mental illness. Treatment for MDD typically involves medications. Some people do not respond to initial treatment but continue to use the same medication. This is called treatment inertia. We assessed the real-world frequency of treatment inertia among patients with MDD. Despite treatment modification guidance, treatment inertia is common in MDD, affecting 29% of patients surveyed.
Implications of managed care
This real-world study assessed the frequency of treatment inertia in the management of adult patients with MDD and compared the characteristics of those patients with others whose treatment was modified. A large proportion of patients in this analysis did not change treatment or discontinued the treatment altogether, despite guidelines recommending treatment modification in patients not reaching remission. These results illuminate significant inefficiencies in the treatment management of many patients with MDD.
Introduction
Major depressive disorder (MDD) is a debilitating mental health (MH) illness affecting approximately 17.3 million adults in the USA [1]. Patients with MDD experience a loss of interest or pleasure and/or depressed mood for ≥2 weeks, in addition to other burdensome symptoms such as sleep disturbance, psychomotor retardation or agitation, fatigue or loss of energy, excessive/inappropriate guilt or feelings of worthlessness, indecisiveness or diminished ability to concentrate or think, and recurrent thoughts of death or suicidal ideation [2]. Depression is the leading cause of disability globally [3], resulting in almost 400 million disability days per year in the US, substantially more than most other physical and mental conditions [4].
Patients with MDD experience impairments in physical, occupational and social functioning [2,5]. Ongoing functional impairment may interfere with work and other daily activities, highlighting the importance of optimal management of MDD symptoms [6]. Delaying treatment may reduce the likelihood of both symptom remission and functional recovery [7–10]. This can lead to structural changes within the brain, which worsen with ongoing depressive episodes [11]. Following treatment, residual symptoms are a major predictor of relapse [12]. The importance of prompt and effective treatment of residual MDD symptoms is therefore key for achieving optimal clinical outcomes in patients with MDD [7–11,13].
Treatment guidelines recommend antidepressants (ADs) as the first line of treatment for patients with MDD [2,14]. However, approximately 40.0%–50.0% of patients with MDD do not respond to initial AD treatment, and therefore many patients need treatment modification to reach remission [15–17]. Treatment guidelines such as those of the American Psychiatric Association (APA), American College of Neuropsychopharmacology and Canadian Psychiatric Association Network for Mood and Anxiety Treatments recommend treatment modification for patients not in remission [2,18–20].
Treatment inertia, defined as not modifying treatment when treatment goals have not been met, is a term that has been used in relation to other medical disorders. For example, the prevalence of treatment inertia and associated negative consequences are established in other disease areas such as type II diabetes [21,22]; however, the concept of treatment inertia has not been studied in MDD.
Although treatment guidelines have included recommendations for management of MDD in the setting of non-response for decades, the real-world management of AD non-response in accordance with guidelines has not been explored. The objective of this study was to assess the frequency of treatment inertia in the management of adult patients with MDD treated in a real-world setting and compare the characteristics of those patients with others whose treatment was modified.
Methods
This was a retrospective observational study using real-world data from the Decision Resources Group (DRG) Real World Evidence US Data Repository (now Clarivate) [23]. The repository links medical and prescription claims from commercial and public (Medicare, Medicaid) plans with electronic health records (EHRs) to provide longitudinal patient-level data representative of more than 300 million patients in the US. Claims data are sourced directly from transactional clearing houses, and EHR data are sourced directly from EHR providers. Claims and EHR data are linked together by a Health Insurance Portability and Accountability Act-compliant encrypted patient key generated by a third party. Informed consent was not required because this was a retrospective observational study using records from an anonymized data repository.
Adult patients (aged ≥18 years) with MDD were identified from January 2014 to June 2018. Patients with MDD were identified as those with ≥2 encounters within the medical claims database with ≥1 MDD International Classification of Diseases, ninth revision (ICD-9) or ICD-10 diagnosis codes and an elevated Patient Health Questionnaire (PHQ-9) score from baseline at the most recent assessment (≥2 valid test score values needed) and who have received ADs specifically for the treatment of MDD and not for another disorder. The PHQ-9 is a self-administered diagnostic tool for assessing depression, and PHQ-9 scores categorize depression severity as minimal (0–4), mild (5–9), moderate (10–14), moderately severe (15–19) and severe (20–27) [24]. Patients without available PHQ-9 score data and patients with a diagnosis for a psychiatric comorbidity (not including anxiety or depression) were excluded. All patients were required to receive stable AD pharmacotherapy, with or without MH outpatient therapy during an 8-week pre-index period. Lack of remission was defined as a PHQ-9 score ≥5 following stable treatment over an 8-week follow-up period after the administration of the PHQ-9 because patients with a PHQ-9 score <5 are considered in remission, and the APA Practice Guidelines recommend treatment aimed toward inducing remission. Eight weeks was selected because the APA Practice Guidelines recommend 4–8 weeks of treatment before concluding a patient is partially or unresponsive to treatment [14]. The initial date of the elevated PHQ-9 score (≥5) served as the index date.
Three cohorts were formed based on evidence of treatment inertia, treatment modification and treatment discontinuation that occurred over a 16-week follow-up period. Sixteen weeks was selected because the APA Practice Guidelines recommend reappraisal of symptoms 4–8 weeks after treatment initiation and then a subsequent review after the reappraisal after 4–8 additional weeks. By selecting the maximum amount of time whenever the guidelines list a range and allowing for the reappraisal, this operational definition of treatment inertia allows the most generous amount of time recommended in the guidelines for treatment modification at all steps [2,14].
Treatment inertia was defined as continued use of the same pharmacotherapy regimen with no switching, augmentation or dose adjustment of pharmacotherapy and ≥1 of the following: average daily dose of most recent fill in the pre-index period (8 weeks before initial PHQ-9 score) equal to the average daily dose in the 8-week follow-up period; for patients receiving pharmacotherapy alone in the pre-index period, no MH outpatient therapy added to the treatment regimen in the follow-up period; among those receiving MH outpatient therapy in the follow-up period, no increase in the frequency of sessions from pre-index period to follow-up period. Patients receiving pharmacotherapy and MH outpatient therapy during the baseline period met study definition of treatment inertia criteria if pharmacotherapy remained unchanged and the frequency of MH outpatient therapy did not increase.
Treatment modification was defined as augmentation, switching to a new pharmacotherapy in the follow-up period, pharmacotherapy dose adjustment (defined as the continuation with the same pharmacotherapy regimen and ≥1 of the average daily dose in the pre-index date period that differs from average daily dose in the follow-up period [including a decrease in dose of pharmacotherapy]) or a higher number of MH outpatient therapy sessions in the follow-up period compared with the pre-index period (for those patients receiving MH outpatient therapy in the follow-up period).
Treatment discontinuation was defined among patients receiving AD pharmacotherapy with or without MH outpatient therapy, as no fills of AD pharmacotherapy in the follow-up period, patient reached end of days' supply of any medications received in the pre-index period and patient did not receive MH outpatient therapy in the follow-up period. Among those receiving baseline MH outpatient therapy only, treatment discontinuation was defined as no MH outpatient therapy in the follow-up period and patient did not initiate AD pharmacotherapy in the follow-up period.
Data analysis
A descriptive analysis by study cohort was conducted using univariate statistics for demographics, baseline clinical characteristics and the outcomes of interest. Frequencies and percentages were used for categorical variables, while means and standard deviations were used for continuous variables. Patients who discontinued therapy were defined for completeness but not included in the comparative analyses.
For median PHQ-9 scores, the paired Wilcoxon signed-ranked test was used. Odds ratios (ORs) were calculated using logistic regression (the binary outcome variable was categorized as treatment inertia compared with treatment modification as the baseline), with variables simultaneously modeled to create a comprehensive overview of the estimated likelihood of treatment inertia. T-tests (alpha 0.5 level of significance) were used to calculate significance.
Results
Among patients with MDD and ≥1 MDD prescription (n = 4,081,602), 0.9% had a documented PHQ-9 score (n = 35,883) (Figure 1A). Of those patients with a documented PHQ-9 score and on stable treatment, 36.2% had an elevated PHQ-9 score at baseline. Overall, 2850 patients had an elevated PHQ-9 score (PHQ-9 ≥5) after ≥8 weeks of stable baseline treatment and 16 weeks of available follow-up data (Figure 1A). Of the 2850 patients, 74% were female and the median age of the cohort was 55 years (Table 1). Commonly prescribed medications among the patient cohort were selective serotonin reuptake inhibitors (SSRIs), serotonin modulators and serotonin norepinephrine reuptake inhibitors (SNRIs). Common comorbidities included anxiety, cardiovascular disease and hypertension (Table 1).
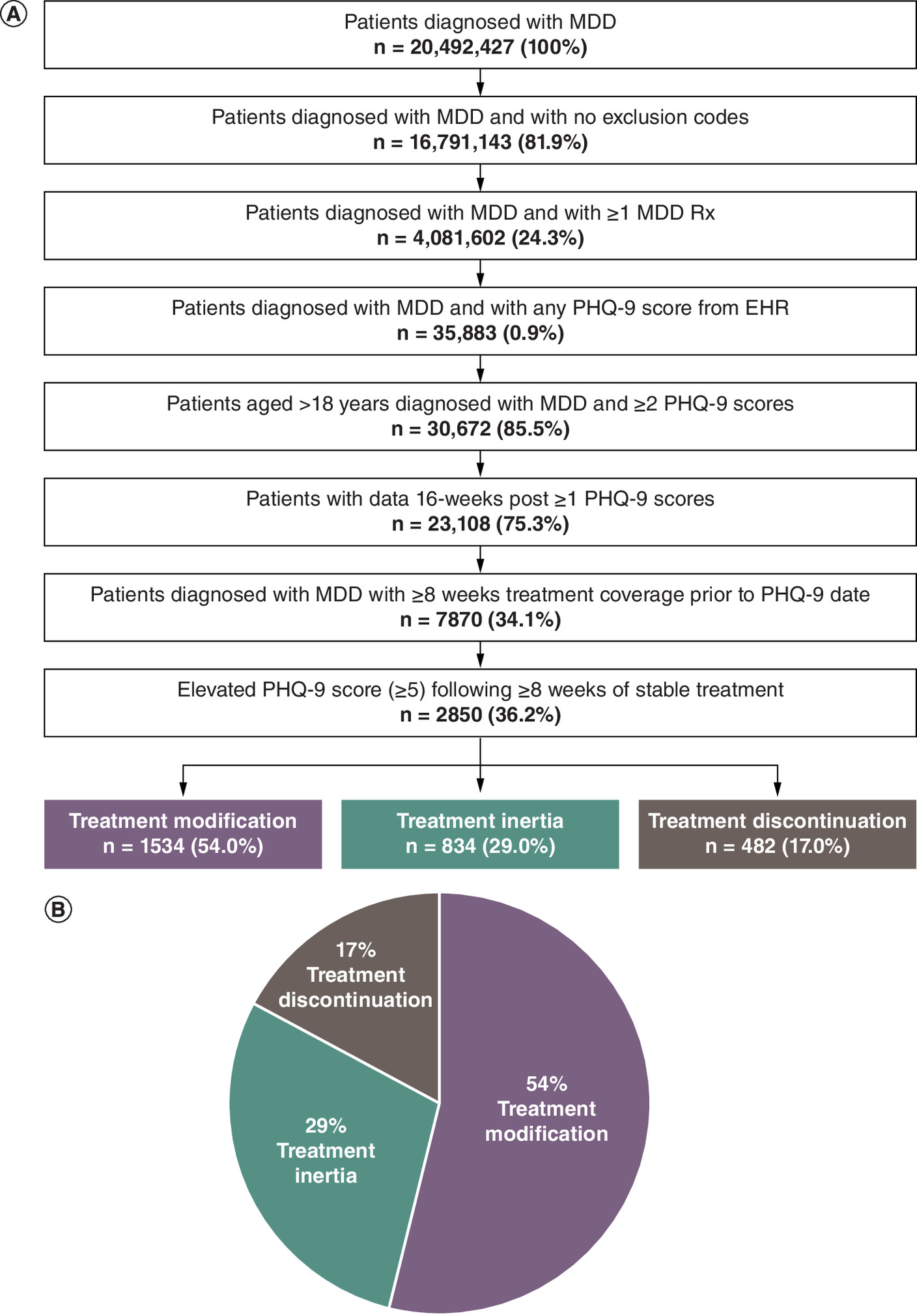
Figure 1. Inclusion criteria and treatment CONSORT diagram.
(A) Eligible patients meeting study inclusion and exclusion criteria matched on age and gender. Index date is the date of initial PHQ-9 score. Patients without available PHQ-9 score data and patients with a diagnosis for a psychiatric comorbidity (not including anxiety or depression) were excluded. (B) Treatment outcomes of patients with elevated PHQ-9 scores following ≥8 weeks of stable treatment.
AD: Antidepressant; EHR: Electronic health record; MDD: Major depressive disorder; PHQ-9: Patient Health Questionnaire-9.
| Characteristics | Patients with elevated PHQ-9 score | |
|---|---|---|
| Treatment inertia (n = 834) | Treatment modification (n = 1534) | |
| n (%) | n (%) | |
| Age, years | ||
| 18–24 | 42 (5.0) | 122 (8.0) |
| 25–34 | 92 (11.0) | 143 (9.3) |
| 35–44 | 88 (10.6) | 212 (13.8) |
| 45–54 | 141 (16.9) | 259 (16.9) |
| 55–64 | 228 (27.3) | 391 (25.5) |
| ≥65 | 245 (29.4) | 410 (26.7) |
| Sex | ||
| Female | 612 (73.4) | 1150 (75.0) |
| Male | 222 (26.6) | 384 (25.0) |
| CNS drug class (top 5 most common)† | ||
| SSRI | 535 (64.1) | 1,091 (71.1) |
| Serotonin modulator‡ | 356 (42.7) | 678 (44.2) |
| SNRI | 324 (38.8) | 616 (40.2) |
| AD other | 202 (24.2) | 475 (31.0) |
| Tricyclic agents | 156 (18.7) | 320 (20.9) |
| Common comorbidities§ | ||
| Anxiety | 677 (81.2) | 1237 (80.6) |
| Cardiovascular | 679 (81.4) | 1195 (77.9) |
| Hypertension | 504 (60.4) | 823 (53.7) |
†
Medications captured at any point during study period.
‡
Serotonin modulator: defined as a drug with a multimodal action specific to the serotonin neurotransmitter system and includes nefazodone, trazodone, vilazodone and vortioxetine [28].
§
Defined using ICD-9 and ICD-10 codes.
AD: Antidepressant; CNS: Central nervous system; PHQ-9: Patient Health Questionnaire-9; SNRI: Serotonin-norepinephrine reuptake inhibitor; SSRI: Selective serotonin reuptake inhibitor.
In total, 834 (29%) patients experienced treatment inertia, 1534 (54%) received treatment modification and 482 (17%) discontinued treatment (Figure 1B). The median index PHQ-9 score was 16, 18 and 15 for patients who experienced treatment inertia, treatment modification and treatment discontinuation, respectively. The median index PHQ-9 score was significantly higher in the treatment modification group versus patients with treatment inertia (p < 0.001), treatment inertia versus treatment discontinuation groups (p = 0.002) and treatment modification versus treatment discontinuation groups (p < 0.001).
Among the 1534 patients receiving treatment modification, the most common treatment modifications were changing AD pharmacotherapy (1228 [80%] patients) and a change in pharmacotherapy dose or MH-related outpatient visit frequency (306 [20%]) (Table 2). Among the 834 patients experiencing treatment inertia, most (90%) were not receiving MH-related outpatient therapy. Of those who were receiving MH therapy, 22 (3%) and 51 (6%) patients decreased and discontinued MH therapy, respectively, in the follow-up period. The most frequently switched to/added medication during the study period was an SSRI (Figure 2).
| Treatment modification in patients with an elevated PHQ-9 score (≥5), n = 1534 n (%) | |
|---|---|
| Continued with the same MDD medication | 306 (19.9) |
| Decreased Dosage† | 112 (7.3) |
| Increased Dosage | 192 (12.5) |
| No Change in Medication Dose, Increased MH visits | 2 (0.1) |
| Change in MDD medication‡ | 1228 (80.1) |
| Discontinued MDD medication, increased MH visits | 5 (0.3) |
†
Decreased dose could be attributed to reduction of current therapy with anticipation of switching Rx or potentially due to adverse events that could impact patient adherence.
‡
This could include switching to another MDD medication, addition of a second MDD medication or addition of an adjunct MDD medication.
MDD: Major depressive disorder; MH: Mental health; PHQ-9: Patient Health Questionnaire-9; Rx: Prescription.
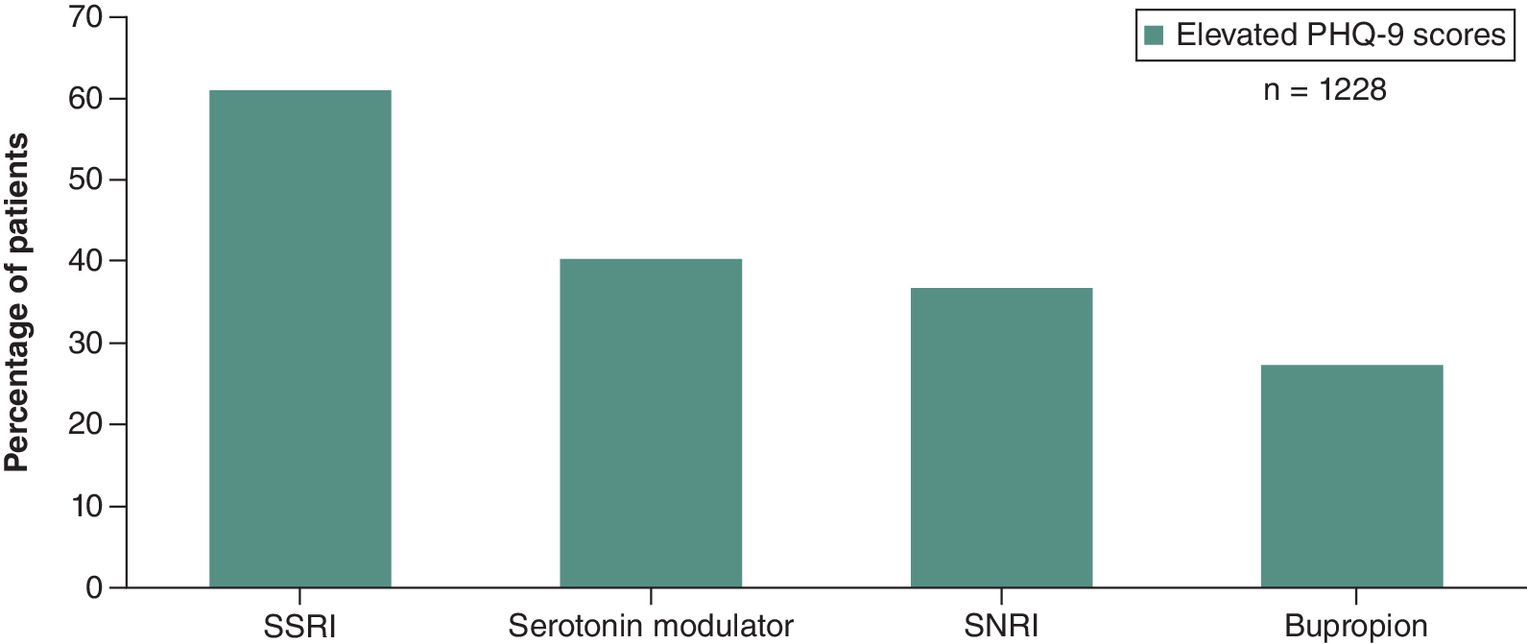
Figure 2. Medication prescribed 16 weeks post-index among patients who switched/added major depressive disorder Rx therapy.
Serotonin modulator: defined as a drug with a multimodal action specific to the serotonin neurotransmitter system and includes nefazodone, trazodone, vilazodone and vortioxetine [28]. Note: This is not a complete list of all drug classes investigated.
PHQ-9: Patient Health Questionnaire-9; Rx: Prescription; SNRI: Serotonin-norepinephrine reuptake inhibitor; SSRI: Selective serotonin reuptake inhibitor.
The likelihood of treatment inertia was higher among patients aged 25–34 (OR: 1.66; 95% confidence interval [CI]: 1.15–2.4: p = 0.006) compared with those aged 18–24 (Figure 3 & Supplementary Table 2). ORs also indicate that prescriptions for several medications during the baseline period were associated with a decreased likelihood of treatment inertia versus not receiving that particular medication (bupropion [OR: 0.71; 95% CI: 0.60–0.84; p = 0.001], SSRI [OR: 0.64; 95% CI: 0.54–0.75; p = 0.001], atypical antipsychotic [OR: 0.80; 95% CI: 0.67–0.96; p = 0.02] and mirtazapine [OR: 0.63; 95% CI: 0.50–0.79; p < 0.001]) (Figure 3 & Supplementary Table 2). Patients with a moderate PHQ-9 score (10–14) were more likely to experience treatment inertia (OR: 1.47; 95% CI: 1.10–1.98; p < 0.01) versus those with a mild PHQ-9 score (5–9). Patients with comorbidities such as anxiety (OR: 1.28; 95% CI: 1.08–1.52; p < 0.005) and hypertension (OR: 1.35; 95% CI: 1.14–1.63; p < 0.001) were more likely to experience treatment inertia compared with those without. Healthcare coverage provided by either Medicaid or Medicare did not significantly influence likelihood of treatment inertia versus a commercial payer source. Similarly, geographic region did not significantly impact the likelihood of experiencing treatment inertia (Figure 3 & Supplementary Table 2).
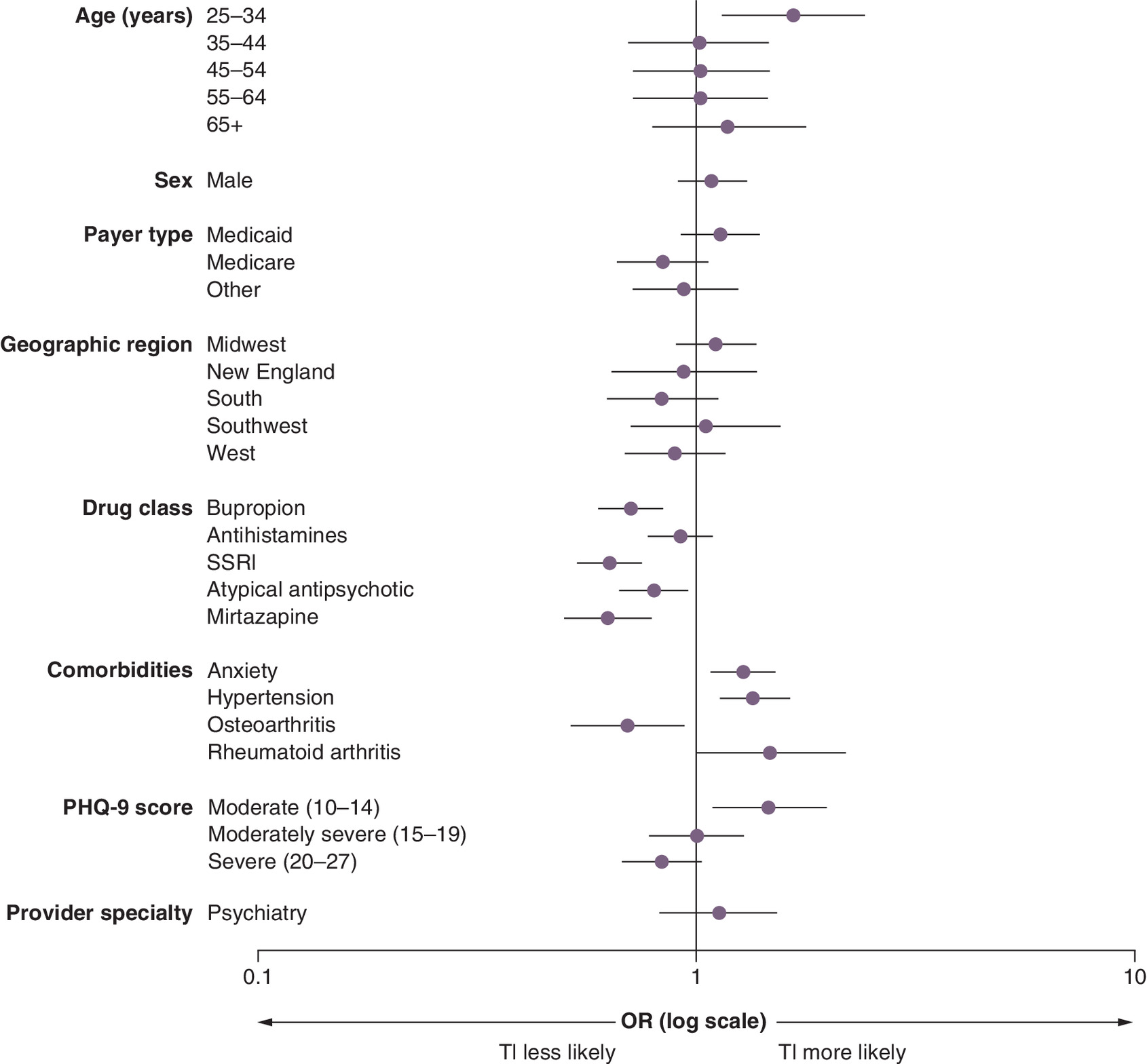
Figure 3. Odds ratios for treatment inertia in each category compared with reference.
Reference groups: age group, 18−24 years; sex, female; payer type, commercial; geographic region, mid-Atlantic; PHQ-9 score, mild (5–9); all other variables are ‘Yes/No’. See Supplementary Table 1 for exact odds ratios.
OR: Odds ratio; PHQ-9: Patient Health Questionnaire-9; SSRI: Selective serotonin reuptake inhibitor; TI: Treatment inertia.
Of the 2850 patients who received medication treatment for MDD, 306 (11%) were treated by a psychiatrist, 1073 (38%) by a primary care physician, and 1471 (52%) by another physician. Receiving treatment from a psychiatrist was not associated with a statistically significant difference in likelihood of treatment inertia compared with not receiving care from a psychiatrist (OR: 1.13; 95% CI: 0.85–1.51; p = 0.39) (Figure 3 & Supplementary Table 2). Receiving treatment from a psychiatrist compared with a non-mental healthcare provider did not change the intensity of follow-up (3.7 vs 4.0 visits, respectively).
Discussion
Using real-world data from the DRG Real World Evidence US Data Repository [23], this study highlights the prevalence of treatment inertia in MDD. In this analysis, a substantial proportion of patients with continued depression symptoms following 8 weeks of initial treatment did not receive treatment modification during a 16-week observation period despite treatment guideline recommendations for patients not in remission to adjust treatment within this timeframe.
Guidelines recommend treatment modification in patients with persistent depression symptoms after the initial course of therapy. Only about half (54.0%) of patients with MDD with PHQ-9 score ≥5 experienced treatment modification, while the remainder either did not modify treatment (29.0%) or discontinued all treatment (17.0%). As might be expected, clinicians were more likely to modify treatment in those patients with higher PHQ-9 scores; however, the median PHQ-9 score of the treatment inertia and treatment discontinuation groups still fell in the moderate-severe category, well above the PHQ-9 threshold for remission.
This analysis used a comprehensive definition of treatment modification. Treatment modification consisted of pharmacotherapy treatment switch, augmentation or dose adjustment using any AD and some non-AD medications (including dose decrease), as well as initiation or increased frequency of MH therapy. A stricter definition, for example using only switch or addition of ADs, would yield greater estimates of treatment inertia. Similarly, some treatment guidelines [18–20] and a recent naturalistic study [25] recommend applying shorter time frames (2–6 weeks) to detect non-response and trigger treatment modification than was used in this analysis, which would also classify more patients as experiencing treatment inertia compared with the findings of this study. Despite this generous definition of treatment modification, only slightly more than half of the patients had their treatment modified.
Factors that influence clinician likelihood of treatment inertia versus treatment modification were assessed. To understand treatment inertia related to clinician prescribing practices as opposed to that arising from patient or payer factors, treatment discontinuation was excluded from the modeling because treatment discontinuation may arise from patient choice or payer-driven economic barriers. It was assumed that patients who continued with treatment would have been amenable to clinician-initiated treatment modification. The model suggested key factors associated with treatment inertia that warrant further investigation: the likelihood of treatment inertia was highest in the age 25–34 years category, and patients with comorbid anxiety and hypertension were more likely to experience treatment inertia. Clinicians may interpret PHQ-9 scores differently among patients with comorbid anxiety and may more cautiously modify pharmacotherapy in patients with hypertension because of concerns about adverse events. It is interesting to note that receiving treatment from a psychiatrist was not associated with a significant difference in the likelihood of treatment inertia compared with not receiving care from a psychiatrist. Of note, patients receiving prescriptions for bupropion, an SSRI, an atypical antipsychotic, or mirtazapine were less likely to experience treatment inertia compared with those not receiving those particular medications. This could be due, in part, to selection of approved antidepressants for initial treatment rather than use of other agents (e.g., benzodiazepines, antihistamines) or use of medications as augmenting agents [17,26]. Both approaches may suggest the clinicians were more familiar with treatment guidelines.
Although no significant difference was found in treatment inertia between patients insured through Medicare or Medicaid and those insured through a commercial source, studies have shown that delays in treatment of MDD may significantly increase the cost of care [27]. Therefore, insurers should recognize that when patients attempt to fill a prescription for an antidepressant, they have already surmounted treatment barriers, including seeking care for an initial diagnosis, filling the initial prescription, visiting the clinician for follow-up, articulating lack of response to initial treatment, receiving a prescription for adjusted treatment and filling the prescription for adjusted treatment. Therefore, patients need readily available and easy access to antidepressants to reduce additional treatment barriers.
Limitations
This study has several limitations. Real-world data collected from routine clinical practice are subject to coding errors, variations in reporting across clinical practices and missing data. Due to the open network nature of the databases used in the current analysis, patients' continuous eligibility cannot be ascertained, and healthcare services provided by out-of-network providers may not be captured by the databases. However, this analysis included only patients who had at least one pharmacy fill (for any physical or MH condition) in the follow-up period, and any patients with missing pharmacy record data were excluded. This design choice helped minimize misclassification of patients as treatment inertia or treatment discontinuation because they filled their prescription at a pharmacy outside of the database. Despite these limitations, real-world data provide an advantage in this analysis of treatment inertia because clinician prescribing behavior may change in a research environment.
A large proportion of patients with MDD identified in the database did not have a PHQ-9 score and were excluded from the analysis; therefore, generalizability of these findings to patients without a documented PHQ-9 score cannot be ascertained. It is plausible that treatment inertia would be more common among patients with depression symptoms in the absence of a documented PHQ-9 score, as an elevated PHQ-9 score may prompt treatment modification. This result highlights that PHQ-9 score is rarely documented in clinical practice despite guideline recommendations to monitor patient response. Updated guidelines emphasizing more clearly how to incorporate measurement-based care into the treatment pathway may increase the use of evidence-based care in MDD.
Conclusion
Overall, treatment inertia is a relatively new concept in psychiatry, and these results indicate it is a common event, which has implications for clinical management of patients with MDD. Approximately half the patients in this analysis did not change treatment or discontinued treatment entirely, despite treatment guideline recommendations to modify treatment in patients not reaching remission and the importance of effective management of symptoms for optimal outcomes.
Summary points
•
Major depressive disorder (MDD) is a debilitating illness in which depressive symptoms may persist after treatment.
•
This retrospective, observational study of patients with MDD evaluated the frequency of treatment inertia in the management of adult patients with MDD treated in a real-world setting and compare the characteristics of those patients with others whose treatment was modified.
•
Treatment inertia (continued use of the same pharmacotherapy regimen when treatment goals are not met), modification and discontinuation were evaluated for patients with elevated PHQ-9 score (≥5) after ≥8 weeks of stable baseline treatment and 16 weeks of available follow-up data. This operational definition of treatment inertia is based on timelines from the APA Practice Guidelines.
•
A total of 29% of patients experienced treatment inertia, 54% received treatment modification and 17% discontinued treatment.
•
Use of mirtazapine, selective serotonin reuptake inhibitors, or bupropion in the baseline period was associated with an increased likelihood of treatment modification versus not receiving treatment with these medications.
•
Results demonstrate that treatment inertia is a common event in MDD despite guidelines recommending treatment modification in patients not reaching remission and the importance of effective management of symptoms for optimal outcomes.
•
PHQ-9 is underutilized in the real-world setting, as the study found at the end of treatment, PHQ-9 assessment was implemented and reported for only 1% of patients.
•
These results do not assess the frequency of treatment inertia in patients without a documented PHQ-9 score. To the extent documentation of unresolved depression symptoms spurs treatment modification, it can be inferred treatment inertia would be more common among those without PHQ-9 assessment.
Author contributions
All authors contributed to developing study concept, design, interpretation of results and drafting the manuscript. All authors have approved the final manuscript.
Financial disclosure
This study was conducted by the Decision Resources Group (DRG), and work by the DRG was funded by Janssen Scientific Affairs, LLC. Through co-authors JA Pesa, K Joshi and JJ Sheehan, the study sponsor was involved in study design, data interpretation and manuscript review/approval. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
C LaVallee, K Maughn and S Balakrishnan are employees of Decision Resources Group (DRG), a healthcare research and consulting company. JA Pesa, K Joshi and JJ Sheehan are employees of Janssen Scientific Affairs, LLC, and stockholders of Johnson & Johnson. JCN has served as an advisor or consultant to Astellas, Biohaven, Johnson & Johnson, Novartis, Otsuka and UpToDate. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing assistance was provided by A Newcombe and S Doran, employees of DRG (part of Clarivate), and by J Washington, PharmD, of Lumanity Communications, Inc. Work by DRG and Lumanity was funded by Janssen Scientific Affairs, LLC.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 31.59 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
National Institute of Mental Health. Major depression. National survey on drug use and health. www.nimh.nih.gov/health/statistics/major-depression.shtml
2.
American Psychiatric Association. Practice guidelines for the treatment of major depressive disorder. https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf
3.
GBD DALYs and Hale Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 390(10100), 1260–1344 (2017).
4.
Merikangas KR, Ames M, Cui L et al. The impact of comorbidity of mental and physical conditions on role disability in the US adult household population. Arch. Gen. Psychiatry 64(10), 1180–1188 (2007).
5.
Kessler RC, Berglund P, Demler O et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 289(23), 3095–3105 (2003).
•• Emphasizes the importance of adequate treatment in major depressive disorder.
6.
Oluboka OJ, Katzman MA, Habert J et al. Functional recovery in major depressive disorder: providing early optimal treatment for the individual patient. Int. J. Neuropsychopharmacol. 21(2), 128–144 (2018).
• Provides recommendations for early, optimal treatment of patients with major depressive disorder, highlighting that delays are associated with poorer outcomes.
7.
Ghio L, Gotelli S, Marcenaro M, Amore M, Natta W. Duration of untreated illness and outcomes in unipolar depression: a systematic review and meta-analysis. J. Affect. Disord. 152–154, 45–51 (2014).
• Highlights the importance of shorter no-treatment intervals patients with depression, which aligns with a strategy of overcoming treatment inertia.
8.
Bukh JD, Bock C, Vinberg M, Kessing LV. The effect of prolonged duration of untreated depression on antidepressant treatment outcome. J. Affect. Disord. 145(1), 42–48 (2013).
9.
Okuda A, Suzuki T, Kishi T et al. Duration of untreated illness and antidepressant fluvoxamine response in major depressive disorder. Psychiatry Clin. Neurosci. 64(3), 268–273 (2010).
10.
Gormley N, O'Leary D, Costello F. First admissions for depression: is the ‘no-treatment interval’ a critical predictor of time to remission? J. Affect. Disord. 54(1–2), 49–54 (1999).
11.
Moylan S, Maes M, Wray NR, Berk M. The neuroprogressive nature of major depressive disorder: pathways to disease evolution and resistance, and therapeutic implications. Mol. Psychiatry. 18(5), 595–606 (2013).
12.
Hiranyatheb T, Nakawiro D, Wongpakaran T et al. The impact of residual symptoms on relapse and quality of life among Thai depressive patients. Neuropsychiatr. Dis. Treat. 12, 3175–3181 (2016).
13.
Jackson WC, Papakostas GI, Rafeyan R, Trivedi MH. Recognizing inadequate response in patients with major depressive disorder. J. Clin. Psychiatry 81(3), OT19037BR2 (2020).
14.
American Psychiatric Association. Clinical Practice Guideline for the Treatment of Depression Across Three Age Cohorts. www.apa.org/depression-guideline/guideline.pdf
15.
Frodl T. Recent advances in predicting responses to antidepressant treatment. F1000Res. 6, 1–6 F1000 Faculty Rev-619 (2017).
16.
Nierenberg AA, Fava M, Trivedi MH et al. A comparison of lithium and T(3) augmentation following two failed medication treatments for depression: a STAR*D report. Am. J. Psychiatry 163(9), 1519–1530 (2006).
17.
Rush AJ, Trivedi MH, Wisniewski SR et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am. J. Psychiatry 163(11), 1905–1917 (2006).
•• Highlights the importance of treatment choice and sequencing, noting that patients with more treatment steps had a higher rate of relapse.
18.
Rush AJ, Kraemer HC, Sackeim HA et al. Report by the ACNP Task Force on response and remission in major depressive disorder. Neuropsychopharmacology 31(9), 1841–1853 (2006).
19.
US Department of Veterans Affairs. VA/DoD Clinical Practice Guidelines. www.healthquality.va.gov/guidelines/MH/mdd/
20.
Kennedy SH, Lam RW, McIntyre RS et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments. Can. J. Psychiatry 61(9), 540–560 (2016).
21.
Reach G, Pechtner V, Gentilella R, Corcos A, Ceriello A. Clinical inertia and its impact on treatment intensification in people with type 2 diabetes mellitus. Diabetes Metab. 43(6), 501–511 (2017).
22.
Khunti K, Wolden ML, Thorsted BL, Andersen M, Davies MJ. Clinical inertia in people with Type 2 diabetes: a retrospective cohort study of more than 80,000 people. Diabetes Care 36(11), 3411–3417 (2013).
23.
DRG. Research and data. https://decisionresourcesgroup.com/research-data/
24.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16(9), 606–613 (2001).
25.
Belanger HG, Lee C, Poliacoff Z, Gupta CT, Winsberg M. Early response to antidepressant medications in adults with major depressive disorder: a naturalistic study and odds of remission at 14 weeks. J. Clin. Psychopharmacol. 43(1), 46–54 (2023).
•• Has implications for treatment inertia as shorter time frames for detection of non-response would classify more patients as experiencing treatment inertia.
26.
Rafeyan R, Papakostas GI, Jackson WC, Trivedi MH. Inadequate response to treatment in major depressive disorder: augmentation and adjunctive strategies. J. Clin. Psychiatry 81(3), OT19037BR3 (2020).
27.
McIntyre RS, Prieto R, Schepman P et al. Healthcare resource use and cost associated with timing of pharmacological treatment for major depressive disorder in USA: a real-world study. Curr. Med. Res. Opin. 35(12), 2169–2177 (2019).
28.
University of Massachusetts Medical School. Therapeutic Class Overview. Serotonin modulators, www.medicaid.nv.gov/Downloads/provider/Serotonin_Modulators_2014-0213.pdf
Information & Authors
Information
Published In
Copyright
© 2023 Becaris Publishing Limited. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 8 June 2023
Accepted: 31 October 2023
Published online: 21 November 2023
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world assessment of treatment inertia in the management of patients treated for major depressive disorder in the USA. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0091
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Deni Rkman, René Ernst Nielsen, Rasmus W. Licht, Klaus Martiny, Philipp Ritter, Marton Asztalos, Algorithm-guided treatment for major depressive disorder versus treatment as usual: a systematic review, Frontiers in Psychiatry, 10.3389/fpsyt.2026.1765024, 17, (2026).
- Fernando Mora, Jose Antoni Ramos-Quiroga, Enrique Baca-García, José Manuel Crespo, Luis Gutiérrez-Rojas, Aránzazu Madrazo, Lucía Pérez Costillas, Pilar A. Saiz, Vicente Tordera, Eduard Vieta, Treatment-resistant depression and intranasal esketamine: Spanish consensus on theoretical aspects, Frontiers in Psychiatry, 10.3389/fpsyt.2025.1623659, 16, (2025).
- Ashlyn M. Kiebach, Tara E. McAlpine, Mitchell H. Cavanaugh, Jessica A. Benzer, Retrospective cohort study of ambulatory care pharmacist interventions’ impact on incidence of therapeutic response in anxiety and depression, JACCP: JOURNAL OF THE AMERICAN COLLEGE OF CLINICAL PHARMACY, 10.1002/jac5.2046, 7, 12, (1147-1153), (2024).
- Yusuf A. Rajabally, Young Gi Min, Kabir K. Nazeer, Christina Englezou, Treatment response amplitude and timing in chronic inflammatory demyelinating polyneuropathy with routine care: Study of a UK cohort, European Journal of Neurology, 10.1111/ene.16399, 31, 10, (2024).