Cost–effectiveness of obinutuzumab plus bendamustine in Chinese patients with relapse and refractory follicular lymphoma
Publication: Journal of Comparative Effectiveness Research
Abstract
A decision analytic model was constructed to assess the cost–effectiveness of obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy (O-B-O) in Chinese patients with relapsed and refractory follicular lymphoma (rrFL). O-B-O was associated with a dominant or more favorable cost–effectiveness than the conventional therapies. Survival outcomes, quality of life of progression-free survival, and subsequent treatment costs for progressive disease were the main drivers of the cost–effectiveness of O-B-O. The cost–effectiveness proportions of O-B-O relative to conventional therapies under the recommended cost–effectiveness threshold ranged from 61.0% to 99.9%. Thus, O-B-O was highly cost-effective for treating patients with rrFL in China compared with conventional therapies.
Plain language summary
In this study, researchers used a decision-making model to figure out if a treatment called obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy (O-B-O) is a good value for money for Chinese patients with a certain type of lymphoma (follicular lymphoma) that has come back or doesn't respond well to previous treatment (relapsed and refractory follicular lymphoma, rrFL). They found that O-B-O is a better choice in terms of cost–effectiveness compared with traditional treatments for Chinese patients with rrFL. Factors like how long patients live, their quality of life without the disease getting worse, and the costs of subsequent treatments if the disease comes back were the main things that influenced this result.
Follicular lymphoma (FL) is an indolent B-cell lymphoma originating from the germinal center. It is a malignant lymphoproliferative disorder characterized by the partial follicular growth pattern of follicular centrocytes and centroblasts. FL progresses slowly, and about 2–3% of the patients each year may progress to an advanced stage that requires medical interventions [1]. Immunochemotherapy is the main treatment for FL patients. Patients with FL often experience multiple relapses due to the long disease course. With the increase of the number of relapses, the likelihood of its progression into a refractory disease also increases whereas the treatment effect and survival prognosis decrease significantly. Relative to treatment-naive patients, patients with three relapses had the treatment remission rate decreased by 20% (68 vs 88%), the median duration of remission reduced by 25 months (6 months vs 31 months), and the median survival time shortened by 8 years (1.2 years vs 9.2 years) [2]. As illustrated, the disease burden of FL is mainly driven by patients with relapsed and refractory FL (rrFL).
Obinutuzumab is the first humanized glycosylation-modified type II anti-CD20 monoclonal antibody. Compared with rituximab, obinutuzumab has greater specificity and cytotoxicity to tumoral B cells. The superior effectiveness of obinutuzumab plus chemotherapy to rituximab plus chemotherapy in treatment-naive patients with FL has been well-established in phase III study settings. Another Phase III study demonstrated that obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy (O-B-O) was associated with a significantly longer progression-free survival (PFS) than bendamustine monotherapy (hazard ratio: 0.55, p < 0.001) in patients with rrFL [3]. Obinutuzumab was listed for reimbursement in treatment-naive FL patients shortly after its introduction in China. To address the limited evidence regarding the clinical utility of obinutuzumab for rrFL in Chinese patients, we conducted this cost–effectiveness study assessing the impact of O-B-O in comparison to conventional therapies on long-term health outcomes and medical costs in Chinese patients with rrFL.
Methods
This study was designed to conduct a cost–effectiveness analysis that compares O-B-O with conventional therapies used for rrFL in Chinese patients, from the perspective of healthcare payers. A decision analytic model was constructed to simulate the health outcomes and medical costs associated with O-B-O and conventional therapies, including bendamustine monotherapy (B-mono), bendamustine plus rituximab (BR), lenalidomide plus rituximab followed by lenalidomide maintenance therapy (R2), rituximab monotherapy as both induction and maintenance therapy (R-mono), lenalidomide monotherapy as both induction and maintenance therapy (L-mono), and the combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) as induction therapy, in rrFL patients over a lifetime horizon. To ensure the generalizability of the cost–effectiveness analysis, this study systematically searched for sources of data on Chinese patients with rrFL to estimate the model variables.
Model structure
The model cohort in this cost–effectiveness analysis was defined as Chinese patients with rrFL. The decision analytic model was constructed using the Markov framework with three health states, including PFS, post-progression survival (PPS), and death. The model simulated the cohort under treatments with O-B-O and the selected conventional therapies. The simulation time horizon was set to a lifetime, with each simulation cycle set to one month. The model outputs, including life years, quality-adjusted life years (QALY), and medical costs, were discounted at 5% per year. The structure of the constructed cost–effectiveness model is illustrated in Figure 1.

Figure 1. The structure of the constructed cost–effectiveness model assessing obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy relative to the conventional treatment regimens for relapsed and refractory follicular lymphoma in Chinese patients.
rrFL: Relapse and refractory follicular lymphoma; PFS: Progression-free survival; PPS: Post-progression survival; O-B-O: Obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy.
Estimating model inputs
The constructed cost–effectiveness model was used to guide the search for appropriate evidence to estimate the model inputs. However, obinutuzumab is a relatively new treatment, and there are limited clinical studies directly comparing O-B-O with the conventional therapies examined in our study for clinical effectiveness and toxicity. As a result, this study was unable to estimate the differences in effectiveness and toxicity between O-B-O and the conventional therapies used for rrFL [4]. To address this limitation, we conducted a systematic literature search of clinical studies published in English or Chinese from 2011 to 2021 that assessed O-B-O and/or any of the six conventional therapies examined in this study. Subsequently, a single-arm meta-analysis was conducted to synthesize the reported PFS, overall survival (OS), and serious adverse events of the treatment methods from the identified studies [5–10]. To better simulate the survival outcomes associated with O-B-O and the six reference treatments in the model, this study used the plotted Kaplan–Meier (KM) survival curves for PFS from the phase III clinical trial (GADOLIN) comparing O-B-O with B-mono in patients with rrFL to identify the most appropriate survival function from six survival functions (Exponential distribution, Weibull distribution, log-logistic distribution, log-normal distribution, generalized gamma distribution, and Gompertz distribution). Based on the Akaike Information Criterion (AIC), the predicted average PFS over lifetime simulation, and the 10-year PFS rate, Weibull distribution was likely to be the most appropriate survival function to fit the observed PFS associated with O-B-O and B-mono. Thus, Weibull distribution was selected to simulate PFS associated with O-B-O and B-mono in the model. Exponential distribution was used to simulate PFS associated with other reference treatments and OS associated with all treatments in the model due to the lack of plotted KM survival curves in the identified clinical trials.
The data source for the utility values of the three health states in the cost–effectiveness model was another study assessing the cost–effectiveness of O-B-O relative to B-mono in Norwegian patients with rrFL [11]. However, because the GADOLIN trial contained data mainly from European countries and didn't assess the impact of age and gender on quality of life, the quality of life data of the Chinese population by age and gender was applied in the model to adjust utility associated with health states over lifetime simulation according to the demographics of the model cohort [12].
The data sources for cost inputs in the model included the latest drug reimbursement bidding prices, patient survey (for administration costs of induction therapy for rrFL in the hospital setting, medical costs per outpatient visit, outpatient visit frequency, and average hospital costs per admission for progressive disease), and physician survey (for hospital admissions in the last year prior to death and health resource utilization associated with managing the reported serious adverse events by treatments). These data sources were used to estimate the average medical costs associated with health states for each model cycle over lifetime simulation. The treatment costs included the drug acquisition costs based on treatment dosage, treatment administration frequency, and treatment cycles or duration, treatment administration costs, and adverse events management costs based on the risk of adverse events by types and medical costs managing each type adverse event. Disease management costs were estimated according to the health resources utilization and unit costs of utilized health resources for PFS and post-progression survival (PPS), respectively. The estimations of the model inputs are summarized in Table 1.
| Variables | Baseline | 95%CI | |
|---|---|---|---|
| Lower limit | Upper limit | ||
| Demographics | |||
| Age (years) | 50.5 | 46.1 | 55 |
| Male (%) | 60.6% | 43.4% | 75.6% |
| Body weight (kg) | 68.8 | 64.3 | 73.2 |
| Body surface area (m2) | 1.8 | 1.7 | 1.9 |
| Treatment cycles | |||
|---|---|---|---|
| O-B-O (induction) | 6 | ||
| O-B-O (maintenance) | 12 | ||
| R-mono (induction) | 1 | ||
| R-mono (maintenance) | 4 | ||
| L-mono | Until disease progression | ||
| R2 (induction) | 1 | ||
| R2 (maintenance) | Until disease progression | ||
| B-mono (induction) | 6 | ||
| BR (induction) | 6 | ||
| R-CHOP (induction) | 6 | ||
| Treatment efficacy | |||
|---|---|---|---|
| Median PFS (months) | |||
| O-B-O | 25.3 | 17.4 | 36 |
| R-mono | 10.4 | 4.4 | 15.9 |
| L-mono | 13.2 | 8.5 | 19.5 |
| R2 | 24 | 15.5 | 35.3 |
| B-mono | 14 | 11.3 | 15.3 |
| BR | 17.7 | 11 | 26.9 |
| R-CHOP | 22.8 | 18.8 | 27.4 |
| Median OS (months) | |||
| O-B-O | 77.3 | 65.1 | 90.9 |
| R-mono | 62.4 | 52.6 | 73.4 |
| L-mono | 65.2 | 54.9 | 76.7 |
| R2 | 76 | 64 | 89.4 |
| B-mono | 46.1 | 39.9 | 53 |
| BR | 49.9 | 43.1 | 57.3 |
| R-CHOP | 54.9 | 47.5 | 63.1 |
| Quality of life (utility) | |||
| PFS: on treatment | 0.807 | 0.784 | 0.831 |
| PFS: off treatment | 0.822 | 0.802 | 0.842 |
| PPS | 0.758 | 0.738 | 0.778 |
| Medical costs | |||
|---|---|---|---|
| Monthly medical care costs | |||
| Induction | ¥2051 | ||
| Maintenance | ¥2310 | ||
| Follow-up: off-treatment (≤2 years) | ¥757 | ||
| Follow-up: off-treatment (>2 years) | ¥378 | ||
| Adverse events management costs | |||
| Anemia | ¥272 | ||
| Decreased appetite | ¥315 | ||
| Diarrhea | ¥57 | ||
| Edema | ¥17 | ||
| Fatigue | ¥558 | ||
| Febrile neutropenia | ¥1386 | ||
| Hepatic function abnormal | ¥626 | ||
| Infusion related reaction | ¥21 | ||
| Leukopenia | ¥1566 | ||
| Lymphopenia | ¥1566 | ||
| Nausea | ¥239 | ||
| Neutropenia | ¥1386 | ||
| Pneumonia | ¥1479 | ||
| Rash generalized | ¥24 | ||
| Thrombocytopenia | ¥2208 | ||
| Vomiting | ¥239 | ||
| Obstipation | ¥135 | ||
| Alopecia | ¥1063 | ||
| Stomatitis | ¥183 | ||
| Allergic reaction | ¥77 | ||
| Cardiac disorder | ¥1032 | ||
| Monthly average medical costs during induction treatment | |||
| O-B-O | ¥24,169 | ||
| R-mono | ¥83,083 | ||
| L-mono | ¥17,577 | ||
| R2 | ¥94,103 | ||
| B-mono | ¥14,027 | ||
| BR | ¥25,250 | ||
| R-CHOP | ¥36,407 | ||
| Monthly average medical costs during maintenance treatment | |||
| O-B-O | ¥7939 | ||
| R-mono | ¥9437 | ||
| L-mono | ¥17,577 | ||
| R2 | ¥17,639 | ||
| End-of-life care costs | |||
| Terminal care costs | ¥127,625 | ||
B-mono: Bendamustine monotherapy; BR: Bendamustine plus rituximab; L-mono: Lenalidomide monotherapy as both induction and maintenance therapy; O-B-O: Obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy; PFS: Progression-free survival; PPS: Post-progression survival; R-CHOP: Rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone; R2: Rituximab plus lenalidomide and followed by lenalidomide maintenance therapy; R-mono: Rituximab monotherapy as both induction and maintenance therapy.
Model assumptions
To adhere to clinical guidelines and practices, we constructed a cost–effectiveness model based on the following assumptions. Firstly, the model assumed that maintenance therapy associated with the treatment scenarios of interest would continue until the disease progressed. Secondly, we assumed that maintenance therapy requiring intravenous administration would be administered in a day ward, which is widely implemented in tier III hospitals across China to facilitate cancer treatment and reduce medical costs. Additionally, the cost–effectiveness model only considered the medical costs resulting from the management of serious adverse events, as mild or moderate adverse events usually do not require medical attention in real-world settings.
Since the patients in the clinical studies referenced by our study received subsequent treatments after disease progression, the cost–effectiveness model assumed that the survival outcomes of subsequent treatments for progressive disease were accounted for in the post-progression survival estimated in these clinical studies. Therefore, our cost–effectiveness model did not separately simulate survival outcomes but included the medical costs associated with subsequent treatments in patients with progressive disease under the treatment scenarios.
Data analysis
The constructed decision analytic model was used to assess the cost–effectiveness of O-B-O relative to conventional therapies for rrFL in Chinese patients. The cost–effectiveness analyses included a base case analysis, one-way sensitivity analysis (OWSA), and probabilistic sensitivity analysis (PSA). The base case analysis used the model inputs' baseline values to estimate the incremental cost–effectiveness ratio per gained QALY (ICER). Two treatment regimens, BR and R2, were selected to conduct OWSA and PSA to assess the uncertainty of O-B-O's cost–effectiveness. OWSA was conducted by varying the model inputs within the 95% confidence interval (CI) or the range of +/-25% of the baseline value if a 95% CI was lacking. PSA was performed using the decision analytic model with the distributions of the selected model inputs with a 95% CI. Ten thousand Monte Carlo simulations were performed to plot the distribution of the generated ICER and calculate the median and 95% credible intervals of the ICER for O-B-O relative to BR and R2. cost–effectiveness acceptability curves were plotted for O-B-O relative to the selected treatment regimens under varying willingness-to-pay to gain one additional QALY. To aid in interpreting the results of the cost–effectiveness analysis under the recommended cost–effectiveness threshold in China (triple the 2022 China gross domestic products per capita [GDPPC]), all ICER results were converted to a ratio to the 2022 China GDPPC (¥85,698 or US$12,743 based on the 2022 average exchange rate [$1: ¥6.725]). The statistical software R (v 4.1.0) was used for common evidence synthesis methods to estimate model variables. Microsoft Excel (version 16.63) was used to construct the decision analytic model and perform the cost–effectiveness analyses, including base case analyses, OWSA, and PSA.
Results
The decision analytic model simulated survival outcomes, QALY, and the lifetime direct medical costs associated with O-B-O and the conventional treatment regimens in Chinese patients with rrFL. In addition, the model outputs were further used to calculate the point estimation of ICER from base case analysis and explore the uncertainty of ICER through OWSA and PSA.
Model simulations for discounted survival outcomes, QALY, & lifetime direct medical costs associated with O-B-O & the conventional treatment regimens
According to the simulation, O-B-O was associated with the longest PFS (2.965 years) and the fourth-longest PPS (3.450 years) among the included treatment regimens, just after R-mono (4.358 years), Lenalidomide (4.228 years), and R2 (3.758 years). The simulation of OS indicated that O-B-O could add the most years to a patient's OS (6.415 years), and B-mono could add the least duration to a patient's OS (4.454 years) among the treatment regimens. The simulated QALY associated with the treatment regimens in the model displayed a similar trend as the simulated survival outcomes. Of the included treatment regimens, O-B-O was associated with the most QALY derived from PFS (2.471 QALY) and the most QALY gained (5.100 QALY). The QALY gained associated with B-mono (3.535 QALY) was ranked the lowest among the included treatment regimens. The lifetime direct medical costs simulated in the model were classified by PFS and PPS. O-B-O was ranked third for the cumulative direct medical costs associated with PFS (¥252,684) but in the bottom for the cumulative direct medical costs associated with PPS (¥288,495). O-B-O was ranked fourth for the overall lifetime direct medical costs among the included treatment regimens in the model. The survival outcomes, QALY, and lifetime direct medical costs associated with the included treatment regimens simulated by the model are summarized in Table 2.
| Model outputs | O-B-O | B-mono | BR | R2 | R-mono | L-mono | R-CHOP | |
|---|---|---|---|---|---|---|---|---|
| OS (years) | Total | 6.415 | 4.454 | 4.729 | 6.346 | 5.562 | 5.733 | 5.080 |
| PFS | 2.965 | 1.557 | 1.977 | 2.588 | 1.204 | 1.506 | 2.474 | |
| PPS | 3.450 | 2.897 | 2.752 | 3.758 | 4.358 | 4.228 | 2.606 | |
| QALY | Total | 5.100 | 3.535 | 3.770 | 5.005 | 4.350 | 4.486 | 4.071 |
| PFS | 2.471 | 1.311 | 1.661 | 2.139 | 1.008 | 1.248 | 2.077 | |
| PPS | 2.629 | 2.224 | 2.110 | 2.866 | 3.342 | 3.238 | 1.994 | |
| Cumulative direct medical costs associated with PFS | Total | ¥252,684 | ¥80,838 | ¥150,492 | ¥459,738 | ¥137,694 | ¥272,395 | ¥154,561 |
| Drug acquisition costs | ¥131,511 | ¥20,815 | ¥84,520 | ¥351,476 | ¥80,897 | ¥227,312 | ¥85,483 | |
| Administration costs | ¥63,978 | ¥39,394 | ¥43,083 | ¥30,756 | ¥34,015 | ¥0 | ¥44,293 | |
| Management of serious adverse events | ¥839 | ¥213 | ¥462 | ¥1,094 | ¥58 | ¥386 | ¥303 | |
| Follow-up costs | ¥56,356 | ¥20,416 | ¥22,426 | ¥76,413 | ¥22,725 | ¥44,697 | ¥24,482 | |
| Cumulative direct medical costs associated with PPS | ¥288,495 | ¥340,053 | ¥339,716 | ¥303,656 | ¥337,746 | ¥327,752 | ¥330,575 | |
| Total lifetime direct medical costs | ¥541,179 | ¥420,891 | ¥490,208 | ¥763,394 | ¥475,440 | ¥600,147 | ¥485,136 | |
B-mono: Bendamustine monotherapy; BR: Bendamustine plus rituximab; L-mono: Lenalidomide monotherapy as both induction and maintenance therapy; O-B-O: Obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy; PFS: Progression-free survival; PPS: Post-progression survival; R-CHOP: Rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone; R2: Rituximab plus lenalidomide and followed by lenalidomide maintenance therapy; R-mono: Rituximab monotherapy as both induction and maintenance therapy.
Point estimation of ICER associated with O-B-O
The base case analyses indicated that O-B-O was superior in cost–effectiveness over R2 and L-mono by producing more QALY gained but costing less for Chinese patients with rrFL. In addition, O-B-O indicated highly attractive cost–effectiveness over the other four treatment regimens (B-mono: ¥76,859 or 0.897 GDPPC; BR: ¥38,331 or 0.447 GDDPC; R-mono: ¥87,620 or 1.022 GDPPC; R-CHOP: ¥54,463 or 0.636 GDPPC) with an ICER under 2 GDPPC. The results of the base case analyses are illustrated in Figure 2.
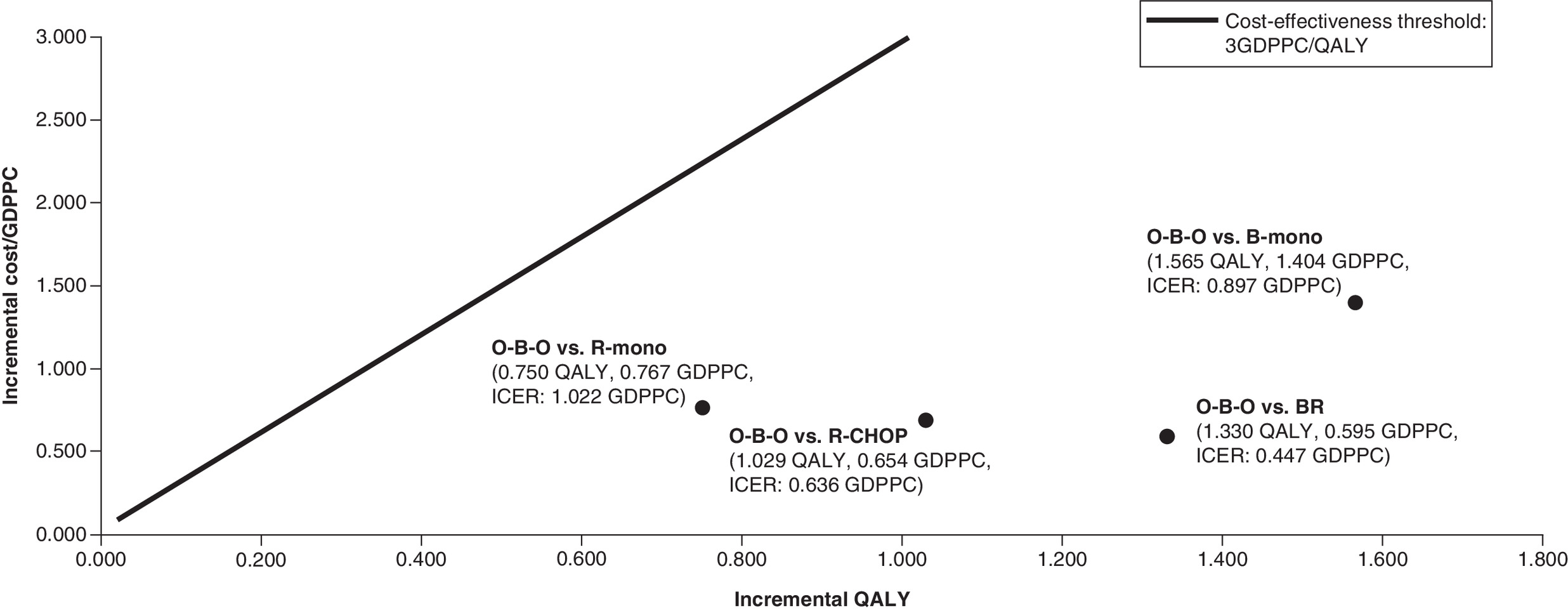
Figure 2. The results of the base case cost–effectiveness analyses for obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy relative to conventional treatment regimens for rrFL in Chinese patients.
O-B-O: Obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy; R-mono: Rituximab monotherapy as both induction and maintenance therapy; R-CHOP: Rituximab plus cyclophosphamide; doxorubicin; vincristine and prednisone; B-mono: Bendamustine monotherapy; BR: Bendamustine plus rituximab; GDPPC: 2022 China gross domestic products per capita; QALY: Quality-adjusted life years.
Uncertainty of ICER associated with O-B-O in OWSA
The ICER of O-B-O, compared with the six conventional therapies in OWSA, varied substantially. The cost–effectiveness of O-B-O relative to BR was driven by key model inputs, including subsequent treatment acquisition costs associated with progressive disease (ICER varied from -¥6676 to ¥83,338), the median OS associated with O-B-O (ICER varied from ¥24,210 to ¥71,566), and the subsequent treatment rate for progressive disease (ICER varied from ¥22,611 to ¥65,193) (Figure 3A). For the cost–effectiveness of O-B-O relative to R2, only median PFS associated with R2 (ICER varied from -¥5,969,345 to ¥1,187,554), median OS associated with O-B-O (ICER varied from -¥381,641 to ¥507,718), and median OS associated with R2 (ICER varied from -¥374,533 to ¥526,159) could drive the ICER above $0 (Figure 3B). Median OS associated with O-B-O (ICER varied from ¥47,166 to ¥314,826) and R-mono (ICER varied from ¥46,710 to ¥281,472) were the key model inputs driving the cost–effectiveness of O-B-O relative to R-mono (Figure 3C). Only median PFS associated with L-mono could drive the ICER of O-B-O relative to L-mono above ¥0 (ICER varied from -¥193,361 to ¥2189) (Figure 3D). The cost–effectiveness of O-B-O relative to B-mono was driven by median OS associated with O-B-O (ICER varied from ¥54,956 to ¥121,739) and subsequent treatment acquisition costs associated with B-mono (ICER varied from ¥39,613 to ¥114,105) and O-B-O (ICER varied from ¥44,312 to ¥109,406) (Figure 3E). Similarly, the cost–effectiveness of O-B-O relative to R-CHOP was driven by median OS associated with O-B-O (ICER varied from ¥32,267 to ¥123,722) and subsequent treatment acquisition costs associated with R-CHOP (ICER varied from -¥3431 to ¥112,357) and O-B-O (ICER varied from ¥4962 to ¥103,964) (Figure 3F).

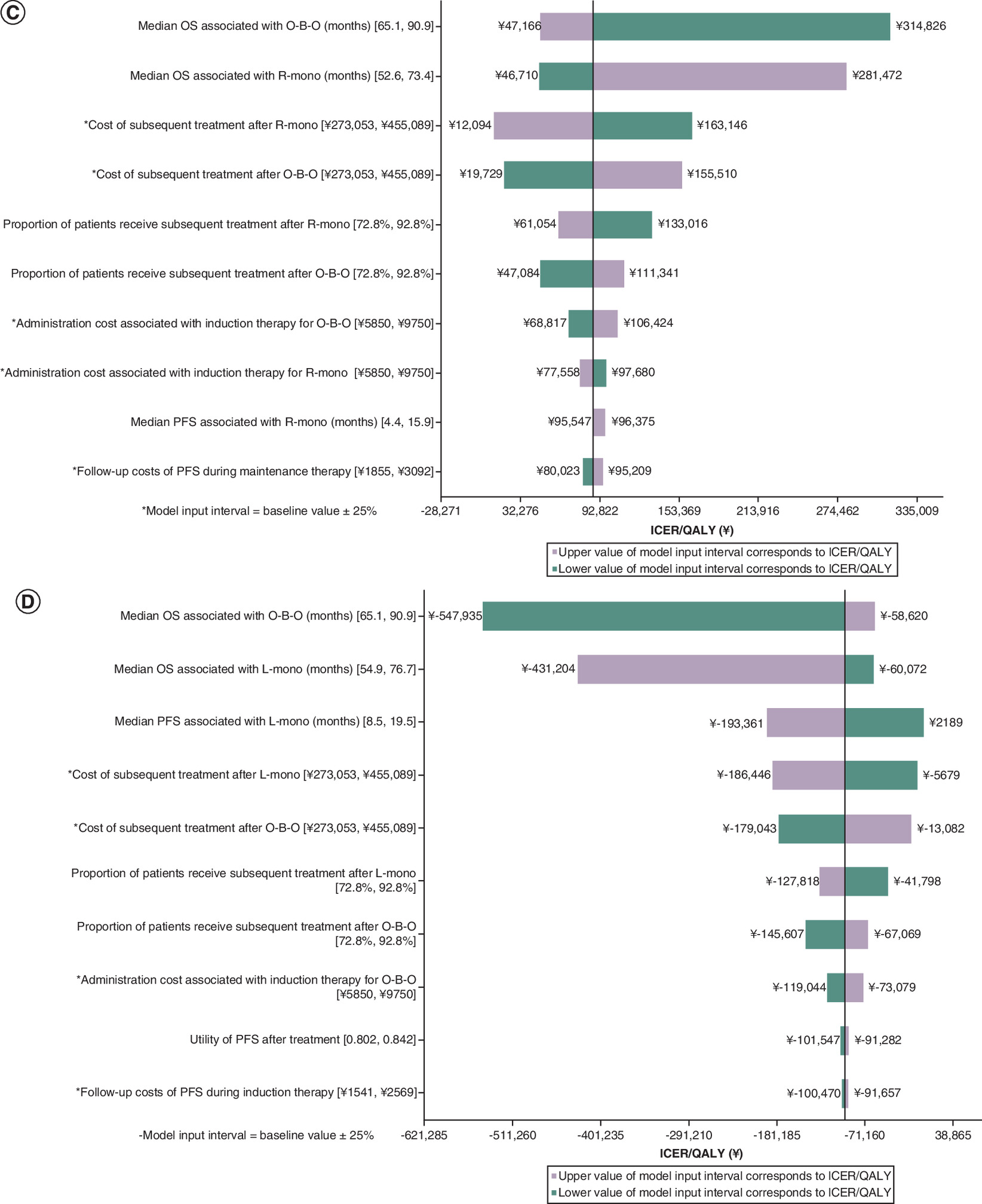
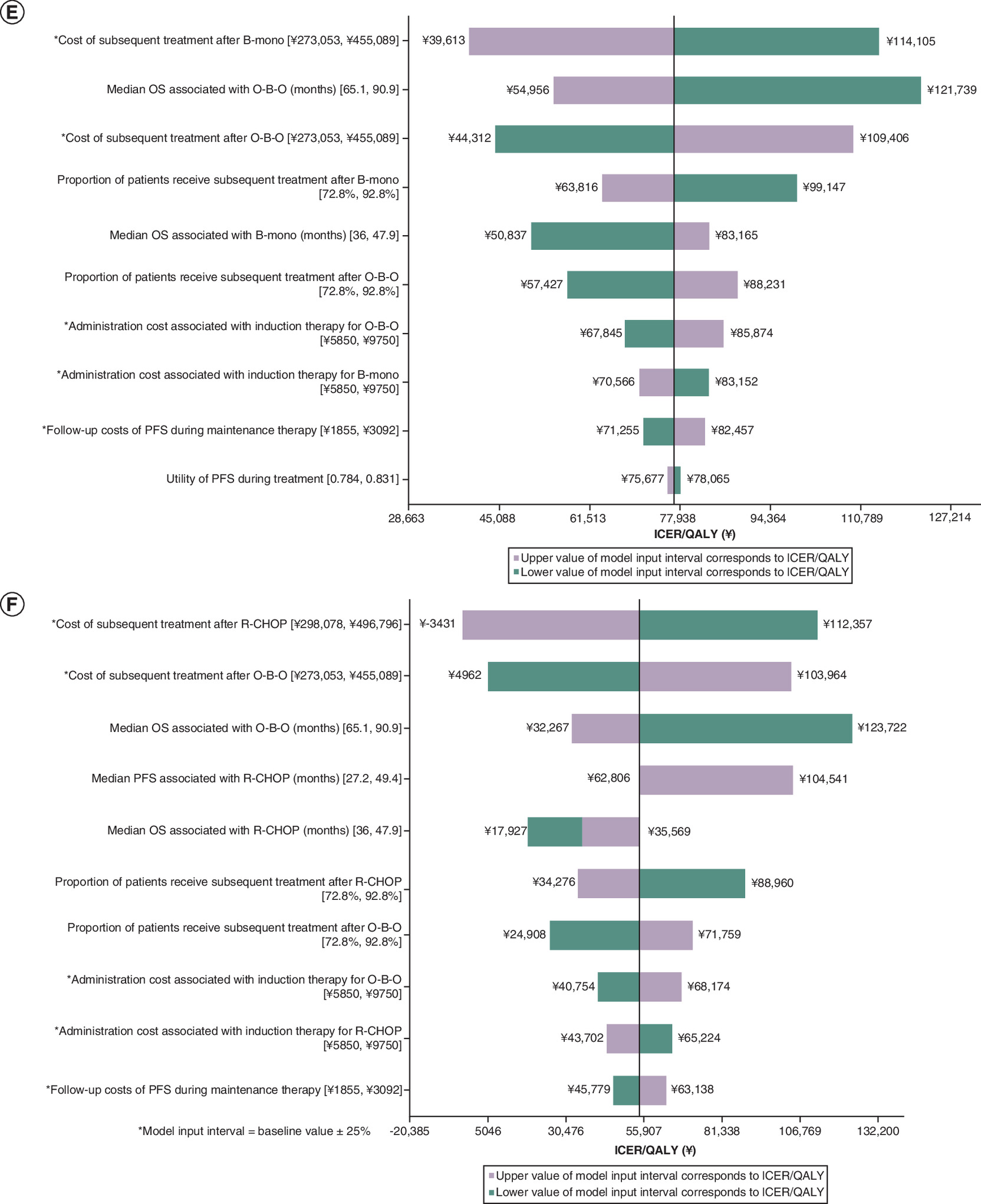
Figure 3. The results of the one-way sensitivity analysis for the cost–effectiveness of obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy relative to conventional treatment regimens for relapsed and refractory follicular lymphoma in Chinese patients.
(A) O-B-O versus BR. (B) O-B-O versus R2. (C) O-B-O versus R-mono. (D) O-B-O versus L-mono. (E) O-B-O versus B-mono. (F) O-B-O versus R-CHOP.
O-B-O: Obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy; BR: Bendamustine plus rituximab; OS: Overall survival; PFS: Progression-free survival; PPS: Post-progression survival; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life years.
Overall uncertainty of ICER associated with O-B-O in PSA
The 10,000 Monte Carlo simulations for the cost–effectiveness of O-B-O relative to the six conventional therapies for rrFL were used to identify median and 95% credible intervals of ICER and the cost–effectiveness proportions under the cost–effectiveness thresholds as of 1, 2, and three-times of GDPPC (Table 3). Based on these PSA, the cost–effectiveness proportions of O-B-O relative to all six included conventional therapies were above 50% under the guideline recommended cost–effectiveness threshold (3 GDPPC). When the cost–effectiveness threshold reduced to 1 GDPPC, the cost–effectiveness proportions of O-B-O still remained above 50% for the comparisons with BR (93.7%), R2 (59.9%), L-mono (94.7%), B-mono (61.7%) and R-CHOP (79.0%).
| Comparison | ICER | Cost–effectiveness proportion | ||||
|---|---|---|---|---|---|---|
| Median | 95% credible Interval | 1 GDPPC | 2 GDPPC | 3 GDPPC | ||
| O-B-O vs BR | ¥39,285 | ¥7303 | ¥109,812 | 93.7% | 99.5% | 99.9% |
| O-B-O vs R2 | ¥-369,272 | ¥-8,969,604 | ¥9,001,526 | 59.9% | 60.0% | 61.0% |
| O-B-O vs R-mono | ¥88,480 | ¥-186,554 | ¥629,127 | 48.2% | 81.6% | 90.7% |
| O-B-O vs L-mono | ¥-83,729 | ¥-709,901 | ¥431,604 | 94.7% | 95.8% | 96.4% |
| O-B-O vs B-mono | ¥78,231 | ¥44,123 | ¥152,493 | 61.7% | 98.8% | 99.8% |
| O-B-O vs R-CHOP | ¥54,766 | ¥13,057 | ¥200,994 | 79.0% | 96.1% | 98.5% |
B-mono: Bendamustine monotherapy; BR: Bendamustine plus rituximab; GDPPC: Gross domestic products per capita; L-mono: Lenalidomide monotherapy as both induction and maintenance therapy; O-B-O: Obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy; PFS: Progression-free survival; PPS: Post-progression survival; R-CHOP: Rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone; R2: Rituximab plus lenalidomide and followed by lenalidomide maintenance therapy; R-mono: Rituximab monotherapy as both induction and maintenance therapy.
Discussion
The high expression of the B-cell surface antigen CD20 in patients with chronic lymphocytic leukemia led to the development of monoclonal antibodies for immunotherapies. Obinutuzumab is a type II anti-CD20 monoclonal antibody, which binds to CD20 in a different orientation than type I anti-CD20 monoclonal antibodies such as rituximab. When compared with type I anti-CD20 monoclonal antibodies, type II anti-CD20 monoclonal antibodies generate stronger homotypic adhesion, cause more direct cell death via actin-dependent enhancement of cell-to-cell contact, induce more lysosome rupture, and generate more reactive oxygen species [13]. With increased affinity to FcγRIIIa through glycoengineered technology, obinutuzumab enhances the activity of antibody-dependent cellular cytotoxicity and becomes more clinically effective than type I antibodies. Existing clinical evidence has proven the superior treatment efficacy of obinutuzumab in combination with bendamustine over B-mono in treatment-naive and previously treated patients with indolent non-Hodgkin lymphoma, which includes FL [14]. As a relatively new treatment, obinutuzumab-containing therapies have not been widely studied in comparison with other recommended therapies in patients with rrFL. Although it may be challenging to conduct adjusted comparisons of the reported efficacies associated with treatments for rrFL in trial settings, the comparable patient characteristics of rrFL patients in these trials could support the development of a robust cost–effectiveness model to simulate survival outcomes associated with O-B-O and common treatment regimens for rrFL in Chinese patients. Using a comprehensive pool of data, our cost–effectiveness analysis confirmed that O-B-O could be highly cost-effective for rrFL in Chinese patients by engendering more health benefits with saving or a limited increase in direct medical costs.
Because FL is an indolent form of lymphoma and it can be challenging to enroll a sufficient number of patients with rrFL in clinical trials, there are very few studies assessing treatments for this condition. Our study identified only six studies with sufficient treatment outcome information following a thorough search of both major English and Chinese bibliographic databases. An examination of the survival outcomes reported from these trials indicated that O-B-O was associated with longer median PFS and median OS than type I anti-CD20 monoclonal antibody-containing immunotherapies (BR, R2, R-mono, R-CHOP) and an immunomodulatory treatment, L-mono. Since PFS is associated with a much higher quality of life than living with a progressive disease [11], O-B-O was expected to produce more health benefits, measured as QALYs gained in the cost–effectiveness model, than all other treatment regimens studied in the cost–effectiveness analyses. Based on the simulated survival outcomes associated with the treatment regimens in our study, both R-mono and L-mono were associated with much longer PPS than other treatments. For hematologic malignancies, the treatment effects and disease prognosis are mainly reflected by PFS and PPS. After reviewing the distribution of Follicular Lymphoma International Prognostic Index (FLIPI) scores of the patients in the clinical trials used as data sources in our model, we found that the patients who received R-mono and L-mono had a much lower proportion of high-risk FLIPI that could be correlated with poorer survival prognosis [15]. Thus, the health benefits associated with R-mono and L-mono could be overestimated in the cost–effectiveness analysis. Future studies are needed to directly compare the treatment regimens in rrFL patients with comparable characteristics to control the confounding effects associated with the survival outcomes.
There are additional factors that influence the medical costs associated with the studied treatments in the model. For example, the gains in PFS associated with the treatment regimens increased follow-up outpatient costs. However, this had only a modest economic impact because regular follow-up outpatient visits by patients with PFS did not cost much. The simulation of medical costs in the base case analyses revealed that treatment regimens that include maintenance therapy added substantially to the medical costs with accumulated drug acquisition costs and treatment administration costs (except for lenalidomide, which is administered orally) over a longer treatment duration. Since treatment regimens that include maintenance therapy usually had better survival outcomes [16], it is much more difficult to predict the cost–effectiveness without a comprehensive analysis of all health benefits and direct medical costs over the time horizon of the model. Another significant contributor of medical costs in the model was progressive disease, which could result in a significant consumption of health resources through continued treatments, disease management for symptoms caused by advanced diseases, and pre-death management [17]. Therefore, the aforementioned confounding in PFS could substantially confound the medical costs as well in the model and bias the cost–effectiveness analysis.
The base case analyses suggested that O-B-O had dominant cost–effectiveness over R2 and L-mono in Chinese patients with rrFL. According to the distributions of the simulated health benefits and medical costs associated with the four treatment regimens, the superior cost–effectiveness of O-B-O over R2 and L-mono was largely due to the accumulated drug acquisition costs of lenalidomide, which was administered until disease progressed in the model. In comparison to the other four treatment regimens (B-mono, BR, R-mono and R-CHOP), O-B-O was associated with greater lifetime medical costs mainly due to its much higher drug acquisition costs. However, O-B-O showed more favorable cost–effectiveness over these treatment regimens by gaining more QALYs. The OWSA performed in this study suggested that the impact of the model inputs on the cost–effectiveness of O-B-O varied by the treatment in comparison. The medical costs and treatment rate of subsequent treatments for progressive diseases had a predominant impact on the cost–effectiveness of O-B-O over BR but not R2, which persistently treated patients with lenalidomide until disease progressed. In comparison to R2, this made the substantial accumulation of drug acquisition costs of lenalidomide the key influence on the cost–effectiveness of O-B-O. Thus, the results of OWSA should be carefully reviewed for each treatment examined and inform the optimization strategies for the cost–effectiveness of O-B-O for rrFL. Similarly, the results of PSA should be interpreted separately by each treatment. The PSA only included a limited number of model inputs due to the lack of supporting data to construct the distributions of model inputs. The model inputs in the PSA had wide distributions due to small sample sizes in the studies used as data sources. Therefore, future studies are needed to fill the gap in supporting data and diminish the uncertainty of model inputs.
The main limitation in this cost–effectiveness analysis was the lack of clinical evidence used for the adjusted comparisons of survival outcomes between O-B-O and other common treatment regimens for rrFL in Chinese patients. Using unadjusted survival outcomes from the clinical trials and the assumptions on the survival distribution due to insufficient information would have inevitably biased the PPS measurement and the cost–effectiveness assessment. In addition, the epidemiology of and health resources utilization for rrFL in China were based on a limited number of patients and healthcare providers that may not be representative. Consequently, the findings in this study should be interpreted with caution. Future real-world studies for rrFL in China are strongly encouraged to address these limitations and improve the robustness of the cost–effectiveness assessment for O-B-O.
Conclusion
In summary, this study constructed a cost–effectiveness model using all existing evidence to explore the cost–effectiveness of O-B-O relative to the approved treatment regimens for rrFL in Chinese patients. The cost–effectiveness analysis confirmed that O-B-O could generate more health benefits, primarily from gains in PFS, and would be more cost-effective than the other treatment regimens by saving medical costs or minimizing the increase of medical costs from drug acquisition. The sensitivity analyses suggested that the uncertainty of the cost–effectiveness of O-B-O varied depending on the treatment regimen it was compared against. Despite the great uncertainty associated with model inputs, our study found that O-B-O would likely be the most cost-effective treatment option for rrFL in Chinese patients.
Executive summary
•
Obinutuzumab plus bendamustine followed by obinutuzumab maintenance therapy (O-B-O) could generate more health benefits which stem mostly from gains in progression-free survival and be more cost-effective than the existing treatment regimens by saving medical costs or minimizing the increase of medical costs.
•
O-B-O had a dominant cost–effectiveness over R2 and L-mono in Chinese patients with relapsed and refractory follicular lymphoma (rrFL), largely due to the accumulated drug acquisition costs of lenalidomide, which was administered until disease progressed in the model.
•
In comparison to B-mono, BR, R-mono, and R-CHOP, O-B-O was associated with greater lifetime medical costs mainly due to its much higher drug acquisition costs but showed a more favourable cost–effectiveness over these treatment regimens by gaining more QALY.
•
Even though the cost–effectiveness of O-B-O varied depending on the treatment regimen that it was compared against, O-B-O would likely be the most cost-effective treatment option for rrFL in Chinese patients.
•
The cost–effectiveness of O-B-O relative to existing treatment regimens was mainly driven by survival outcomes of treatments, subsequent treatment for the progressive disease, and drug acquisition costs of O-B-O.
•
Future real-world studies for rrFL in China are strongly encouraged to address the limitations for the lack of clinical evidence directly comparing O-B-O and the existing treatment regiments for rrFL.
Author contributions
J Ma and W Chen formulated research idea and developed the study protocol. J Ma, D Zhao, B Zhen, W Chen, Qi Gong developed the cost–effectiveness model structure. W Chen and Q Gong constructed the cost–effectiveness model and searched the literatures to identify appropriate evidence for the estimation of model inputs. All authors were fully involved with the development of this manuscript. All authors critically reviewed the manuscript and approved the submission of this manuscript.
Financial disclosure
This study was funded by Shanghai Roche Pharmaceuticals Ltd, Shanghai, China. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interest disclosure
Q Gong and W Chen are the employees of Normin Health, a consulting firm receiving industry to conduct health economic and outcome research. B Zhen and Y Xia are the employees of Roche. The authors have no other competing interests or relevant affiliations with any organization/entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Link BK. Transformation of follicular lymphoma – why does it happen and can it be prevented? Best Pract. Res. Clin. Haematol. 31(1), 49–56 (2018).
2.
Johnson PW, Rohatiner AZ, Whelan JS et al. Patterns of survival in patients with recurrent follicular lymphoma: a 20-year study from a single center. J. Clin. Oncol. 13(1), 140–147 (1995).
3.
Cheson BD, Trněný M, Bouabdallah K et al. Obinutuzumab plus bendamustine followed by obinutuzumab maintenance prolongs overall survival compared with bendamustine alone in patients with rituximab-refractory indolent non-Hodgkin lymphoma: updated results of the GADOLIN study. Blood 128(22), 615 (2016).
4.
Sehn LH, Trněný M, Bouabdallah K et al. Sustained overall survival benefit of obinutuzumab plus bendamustine followed by obinutuzumab maintenance compared with bendamustine alone in patients with rituximab-refractory indolent non-hodgkin lymphoma: final results of the Gadolin Study. Blood 134(Suppl. 1), 2822 (2019).
•• Main data source for clinical outcomes used in the cost–effectiveness model.
5.
Matsumoto K, Takayama N, Aisa Y et al. A Phase II study of bendamustine plus rituximab in Japanese patients with relapsed or refractory indolent B-cell non-Hodgkin lymphoma and mantle cell lymphoma previously treated with rituximab: BRB study. Int. J. Hematol. 101(6), 554–562 (2015).
6.
Leonard JP, Jung SH, Johnson J et al. Randomized trial of lenalidomide alone versus lenalidomide plus rituximab in patients with recurrent follicular lymphoma: CALGB 50401 (Alliance). J. Clin. Oncol. 33(31), 3635–3640 (2015).
•• Main data source for clinical outcomes used in the cost–effectiveness model.
7.
Hainsworth JD, Greco FA, Raefsky EL et al. Rituximab with or without bevacizumab for the treatment of patients with relapsed follicular lymphoma. Clin. Lymphoma Myeloma Leuk. 14(4), 277–283 (2014).
•• Main data source for clinical outcomes used in the cost–effectiveness model.
8.
Muntañola A, Baumann T, Caballero AC et al. Results of R-ESHAP as salvage therapy in refractory/relapsed follicular lymphoma: a real-world experience on behalf of GELCAB group. Ann. Hematol. 99(7), 1627–1634 (2020).
•• Main data source for clinical outcomes used in the cost–effectiveness model.
9.
Zinzani PL, Khuageva NK, Wang H et al. Bortezomib plus rituximab versus rituximab in patients with high-risk, relapsed, rituximab-naïve or rituximab-sensitive follicular lymphoma: subgroup analysis of a randomized phase 3 trial. J Hematol Oncol. 5, 67 (2012).
•• Main data source for clinical outcomes used in the cost–effectiveness model.
10.
van Oers MH, Van Glabbeke M, Giurgea L et al. Rituximab maintenance treatment of relapsed/resistant follicular non-Hodgkin's lymphoma: long-term outcome of the EORTC 20981 phase III randomized intergroup study. J. Clin. Oncol. 28(17), 2853–2858 (2010).
•• Main data source for utility values used in the cost–effectiveness model.
11.
Haukaas FS, Ohna A, Krivasi T. Cost–effectiveness of obinutuzumab in combination with bendamustine followed by obinutuzumab maintenance versus bendamustine alone in treatment of patients with rituximab-refractory follicular lymphoma in Norway. Appl. Health Econ. Health Policy 16(4), 569–577 (2018).
• Supporting the treatment benefits of obinutuzumab in patients with follicular lymphoma.
12.
Szende A, Janssen B, Cabases J. (Eds). Self-reported population health: an international perspective based on EQ-5D. Springer, Dordrecht, Netherlands (2014).
•• Data sources used to adjust utility by age and gender in the cost–effectiveness model.
13.
Alduaij W, Ivanov A, Honeychurch J et al. Novel type II anti-CD20 monoclonal antibody (GA101) evokes homotypic adhesion and actin-dependent, lysosome-mediated cell death in B-cell malignancies. Blood 117(17), 4519–4529 (2011).
14.
Davies A, Kater AP, Sharman JP et al. Obinutuzumab in the treatment of B-cell malignancies: a comprehensive review. Future Oncology. 18(26), 2943–2966 (2022).
15.
Muntañola A, Mozas P, Mercadal S et al. Early progression in follicular lymphoma in the absence of histological transformation or high-risk Follicular Lymphoma International Prognostic Index still has a favourable outcome. Br. J. Haematol. 200(3), 306–314 (2023).
16.
Bachy E, Seymour JF, Feugier P et al. Sustained progression-free survival benefit of rituximab maintenance in patients with follicular lymphoma: long-term results of the PRIMA study. J. Clin. Oncol. 37(31), 2815 (2019).
17.
Kuruvilla J, Ewara EM, Elia-Pacitti J et al. Estimating the Burden of Illness of Relapsed Follicular Lymphoma and Marginal Zone Lymphoma in Ontario, Canada. Current Oncology. 30(5), 4663–4676 (2023).
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 11 May 2023
Accepted: 20 October 2023
Published online: 2 November 2023
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of obinutuzumab plus bendamustine in Chinese patients with relapse and refractory follicular lymphoma. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0073
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Shen Lin, Xiangzhen Wang, Lijing Yang, Shaohong Luo, Xiaoting Huang, Xiuhua Weng, Xiongwei Xu, The pricing barrier: cost-effectiveness of Glofitamab for relapsed/refractory DLBCL in China beyond threshold and value-based pricing strategy considerations, Expert Review of Anticancer Therapy, 10.1080/14737140.2026.2630025, (1-8), (2026).
- Mengya Li, Qian Li, Yinhui Zhang, Changjing Xu, Zhu Chen, Yilan Huang, Longyang Jiang, Cost-effectiveness of polatuzumab vedotin plus chemoimmunotherapy for untreated diffuse large B-cell lymphoma in China, Scientific Reports, 10.1038/s41598-025-15477-9, 15, 1, (2025).
- Bijal Shah, Mei Xue, Wesley Furnback, Erlene K. Seymour, Jin Kim, Po-Ya Chuang, Madeline Dec, Keri Yang, A Systematic Literature Review of the Economic and Healthcare Resource Utilization Burden of Relapsed/Refractory Follicular Lymphoma, PharmacoEconomics - Open, 10.1007/s41669-025-00577-z, 9, 4, (541-570), (2025).
- Liangliang Dong, Wanfu Zhong, Ting Chen, Qiuling Zhao, Wenbin Liu, Xiuliang Qiu, Ruyi Huang, Shengqiang Huang, Ruixiang Xie, Lin Yang, Is first-line treatment with polatuzumab vedotin–rituximab–cyclophosphamide, doxorubicin and prednisone (pola-R-CHP) for previously untreated diffuse large B-cell lymphoma cost-effective in China? A cost-effectiveness analysis using a Markov model, BMJ Open, 10.1136/bmjopen-2024-086251, 15, 1, (e086251), (2025).
- Chao Wang, Yunzhuo Dong, Peng Men, Ruixia Zhang, Ying Xiao, Yishan Bu, Yinpeng Qin, Xinran Zhang, Qianqian Dou, Yiheng Yang, Huier Gao, Yi Zhang, Efficacy, safety and cost-effectiveness of obinutuzumab in patients with follicular lymphoma: a rapid review, Frontiers in Pharmacology, 10.3389/fphar.2024.1426772, 15, (2025).