Gastrointestinal adverse effects associated with the use of intravenous oliceridine compared with intravenous hydromorphone or fentanyl in acute pain management utilizing adjusted indirect treatment comparison methods
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: In the absence of head-to-head comparative data from randomized controlled trials, indirect treatment comparisons (ITCs) may be used to compare the relative effects of treatments versus a common comparator (either placebo or active treatment). For acute pain management, the effects of oliceridine have been compared in clinical trials to morphine but not to fentanyl or hydromorphone. Aim: To assess the comparative safety (specifically differences in the incidence of nausea, vomiting and opioid-induced respiratory depression [OIRD]) between oliceridine and relevant comparators (fentanyl and hydromorphone) through ITC analysis. Methods: A systematic literature review identified randomized clinical trials with oliceridine versus morphine and morphine versus fentanyl or hydromorphone. The ITC utilized the common active comparator, morphine, for the analysis. Results: A total of six randomized controlled trials (oliceridine – 2; hydromorphone – 3; fentanyl – 1) were identified for data to be used in the ITC analyses. The oliceridine data were reported in two studies (plastic surgery and orthopedic surgery) and were also reported in a pooled analysis. The ITC focused on nausea and vomiting due to limited data for OIRD. When oliceridine was compared with hydromorphone in the ITC analysis, oliceridine significantly reduced the incidence of nausea and/or vomiting requiring antiemetics compared with hydromorphone (both orthopedic surgery and pooled data), while results in plastic surgery were not statistically significant. When oliceridine was compared with hydromorphone utilizing data from Hong, the ITC only showed a trend toward reduced risk of nausea and vomiting with oliceridine that was not statistically significant across all three comparisons (orthopedic surgery, plastic surgery and combined). An ITC comparing oliceridine with a study of fentanyl utilizing the oliceridine orthopedic surgery data and combined orthopedic and plastic surgery data showed a trend toward reduced risk that was not statistically significant. Conclusion: In ITC analyses, oliceridine significantly reduced the incidence of nausea and/or vomiting or the need for antiemetics in orthopedic surgery compared with hydromorphone and a non-significant trend toward reduced risk versus fentanyl.
Tweetable abstract
An indirect treatment comparison, used when head-to-head comparative data are lacking, showed that oliceridine reduced nausea/vomiting and antiemetic use in acute pain management for orthopedic surgery more than hydromorphone.
Plain language summary
Why are indirect treatment comparisons used?
When making treatment decisions, providers and payers often require data that compares the effectiveness of two or more treatments. However, there is often a lack of head-to-head comparative effectiveness data between the treatments, especially since the randomized controlled trials required for drug approval often compare a single treatment to a placebo instead of to other existing treatments. To compensate for this lack of head-to-head data, indirect treatment comparisons (ITCs) may be used if the two treatments being compared were both evaluated in clinical trials against a placebo or against the same comparison treatment.
How did this study use indirect treatment comparisons?
In acute pain management, the effects and adverse effects of three drugs – oliceridine, fentanyl and hydromorphone – have all been directly compared in clinical trials to morphine. However, no head-to-head trials have been conducted between oliceridine and the other two comparators (fentanyl and hydromorphone). Therefore, since all three drugs were compared with morphine, ITCs were conducted using the three drugs' clinical trial data in order to compare their adverse effects of nausea and/or vomiting.
What did the indirect treatment comparisons reveal?
The ITC analyses found that oliceridine significantly reduced the incidence of nausea and/or vomiting or the need for antiemetics in orthopedic surgery when compared with hydromorphone. Results of the drugs' use in plastic surgery were not significantly different.
Indirect treatment comparisons (ITCs) are used to compare treatments when there is no evidence or insufficient evidence from head-to-head clinical trials, or when more than two treatments are of interest. ITCs may use the relative effects of the treatments versus their common comparator, often a placebo, to assess the head-to-head comparison of interest. ITCs may be unbiased if specific assumptions are met: homogeneity, similarity of studies and consistency of evidence [1]. ISPOR, the International Society for Pharmacoeconomics and Outcomes Research, published a best practices report focused on interpreting indirect treatment comparisons and network meta-analyses [1].
For acute pain management, especially in postoperative pain, treatment commonly includes opioids such as morphine, hydromorphone and fentanyl [2]. In late 2020, oliceridine was approved for use in the treatment of severe pain. Adverse effects (AEs) of these medications can include nausea and/or vomiting, among others [2].
The effects and adverse effects of oliceridine have been directly compared in clinical trials to morphine [3,4]. Similarly, fentanyl [5,6] and hydromorphone [7–9] have both been compared with morphine in clinical trials. However, no clinical trials have directly compared oliceridine to fentanyl or hydromorphone.
Because all three medications have been compared with morphine, an ITC may be useful to comparatively assess their adverse effects despite the lack of head-to-head clinical trials. Therefore, the goal of this study was to conduct an adjusted ITC analysis of oliceridine compared with hydromorphone and to fentanyl. The primary method considered for the adjusted ITC was Bucher's anchor-based indirect comparison method [10]. Bucher's anchor-based indirect comparison method uses the relative effects to compare treatments (i.e., it subtracts out the common comparator effect, morphine). When there are significant differences in the populations from various studies, the matching-adjusted indirect comparison (MAIC) [11] may be appropriate. MAIC is a novel technique allowing for a robust comparison by re-weighting individual patient data (IPD) from one study to the baseline summary statistics of another, to provide greater adjustment for observed trial differences compared with conventional meta-analytic methods. The Bucher method was chosen because individual patient data were not available.
Objectives
The primary objective of this study was to assess the comparative safety between oliceridine, fentanyl and hydromorphone in randomized controlled trials (RCTs) where morphine was the common comparator and the analgesic effect was shown to be statistically similar to morphine. Specifically, the incidence of nausea and/or vomiting and opioid-induced respiratory depression (ORID) were compared where sufficient data existed to allow for the analysis.
Methods
To identify randomized clinical trials with oliceridine versus morphine and clinical trials of morphine versus comparators fentanyl and hydromorphone to be used in the ITC, literature searches were conducted using PubMed, focusing on papers published in English from 1995 to 2022.
A pilot literature review was conducted in February 2022 identifying potential articles to consider for an adjusted ITC analysis regarding opioid-related adverse events (AEs). The articles identified were screened independently by two reviewers and any disagreements were referred to a third reviewer for resolution. Screened articles were included in evidence tables if they included information about adverse events (nausea, vomiting, respiratory depression, somnolence and sedation, constipation and pruritus) or the outcome measure SPID (sum of pain intensity differences).
The articles in the evidence tables were then reviewed to determine if they contained data that would be useful for conducting an adjusted ITC analysis. In addition, the references from the articles were also screened and reviewed if there was any indication that they contained additional data of use for the ITC analysis.
Separate literature searches were then performed for oliceridine versus morphine, and for morphine versus fentanyl and hydromorphone. The search strategy was modified based on the results of the search. Additional search terms were added if needed to identify potential studies to include.
Articles were filtered for clinical trial, phase II; or clinical trial, phase III; or clinical trial phase IV; or clinical trial; or randomized controlled trial. The pain type was MESH heading acute pain/drug therapy. Drugs of interest were oliceridine versus morphine, fentanyl (with MESH headings ‘administration & dosage’, ‘adverse effects’ and ‘therapeutic use’), hydromorphone (with MESH headings ‘administration & dosage’, ‘adverse effects’ and ‘therapeutic use’), route of administration (with MESH heading ‘administration, intravenous’) and type of use (with MESH heading ‘surgical procedures, operative’).
Adjusted ITC analysis
Pooled data for oliceridine were obtained from two phase III randomized placebo and active controlled trials (APOLLO-1 [orthopedic surgery] [3] and APOLLO-2 [plastic surgery] [4]) in postsurgical adult patients (18–75 years) with moderate-to-severe pain. Patients receiving demand doses administered by patient-controlled analgesia (PCA) of either 0.35 mg oliceridine, 0.5 mg oliceridine or 1.0 mg morphine were included in the analysis. The dosing for oliceridine and morphine in the two phase III trials is shown in Table 1.
| Treatment regimens | Clinician administered loading dose (mg) | Demand dose via PCA (mg) | Clinician-administered supplemental dose (mg) |
|---|---|---|---|
| Placebo | Volume matched | Volume matched | Volume matched |
| Oliceridine 0.1 mg | 1.5 | 0.1 | 0.75 |
| Oliceridine 0.35 mg | 1.5 | 0.35 | 0.75 |
| Oliceridine 0.5 mg | 1.5 | 0.5 | 0.75 |
| Morphine | 4 | 1 | 2 |
For each regimen, a clinician-administered fixed IV loading dose was followed by demand doses administered PRN via a PCA device. Thus, each dose regimen included a range of actual cumulative drug exposures over the course of the study. The PCA doses were allowed from 10 min after the loading dose and were limited by a 6-min lockout interval. Clinician-administered IV supplemental PRN doses were permitted from 1 h after the loading dose and then as often as hourly. The dosing limit for all groups was three PCA syringes or six clinician-administered supplemental PRN doses within the first 12 h (60 mg for oliceridine), after which patients were discontinued and managed conventionally.
Aggregate data for hydromorphone were obtained from three randomized, double-blind clinical trials comparing intravenous (IV) hydromorphone to IV morphine in adults presenting to the emergency department (ED) of an academic medical center with acute severe pain [7], or adults having elective day surgeries with a potential to cause moderate-to-severe pain at three hospitals affiliated with a medical school [8], or general or gynecological adult surgery patients at an academic medical center [6]. Aggregate data for fentanyl were obtained from a randomized study in adult patients (aged 18–65 years) comparing the use of IV morphine and fentanyl after painful ambulatory procedures [5].
Baseline demographics and clinical characteristics of the populations for the ITC analyses were compared.
A Bucher anchor-based indirect comparison was conducted to indirectly compare oliceridine to hydromorphone and oliceridine to fentanyl. The Bucher method is an adjusted indirect comparison [12] that uses the magnitude of the effect measure reported in studies that compared the treatments (i.e., oliceridine, hydromorphone and fentanyl) to a common comparator (i.e., morphine). The indirect comparison of oliceridine and hydromorphone as well as oliceridine and fentanyl can be estimated as a function of the direct comparisons of oliceridine versus morphine and of either hydromorphone versus morphine or fentanyl versus morphine. The strengths of this approach are that it partially maintains the strength of randomization and it can be applied with minimal information regarding the common indirect treatment comparison.
For this adjusted ITC, the difference in risk differences (RD) for both oliceridine versus hydromorphone and oliceridine versus fentanyl were calculated, where the RD is the measure of the difference between the proportions of achievers of complete GI response within the populations. For oliceridine, achievers of complete GI response were compared with no antiemetic use in both hydromorphone and fentanyl since complete GI response was not reported in the hydromorphone and fentanyl studies. RD was selected as the effect measure because it can be readily translated into number needed to treat (NNT). The difference in RD was calculated for oliceridine versus hydromorphone as shown in the formula (same formula was used for fentanyl):
The binary achiever outcome was modeled using either multivariable log-binomial, Poisson or logistic regression. In this model, the binary outcome variable was achiever of complete GI response (oliceridine) or no antiemetic use (hydromorphone and fentanyl). The binary predictor variables were study, drug and study x drug interaction. The incidence proportions of achiever (risk), risk differences (RD) and difference of RD were obtained by marginal estimation and tested for significance using a Wald post test. This was done using the Stata-16.1 statistical software [13].
Results
Search results
The pilot search with filters described above yielded 387 articles for fentanyl AND surgical procedures, operative AND administration, intravenous as well as 24 articles for hydromorphone AND surgical procedures, operative AND administration, intravenous.
Data for opioid-induced respiratory depression (OIRD) were very limited; low prevalence of OIRD was reported and no differences were seen between the opioids, which is consistent with literature on OIRD [11]. Additionally, there was lack of agreement in the literature regarding which end points would constitute an episode of OIRD.
Therefore, nausea and/or vomiting was selected as the adverse effect of interest for the ITC.
The clinical end point for oliceridine was complete gastrointestinal (GI) response (no vomiting and not requiring use of rescue antiemetics), while the end point for the opioid comparators was the use of rescue antiemetics. Of the studies identified for the comparators, some reported the incidence of nausea and vomiting; however, the use of rescue antiemetics was reported in all the studies for the comparators. For example, in the Chang study there were 35 patients out of 97 total in the hydromorphone arm that experienced nausea and vomiting but only 20 patients received antiemetics. For the ITC comparison, the lower incidence of nausea and vomiting based on use of antiemetics was used. Additionally, only the data for oliceridine 0.35 and 0.5 mg were used in the analysis, as these were the doses found to be equipotent to morphine [10].
Table 2 shows the baseline demographics and clinical characteristics of the populations used in the ITC analysis.
| Oliceridine | Morphine | ||
|---|---|---|---|
| 0.35 mg | 0.5 mg | 1.0 mg | |
| Plastic surgery (Singla, 2019) [4] | n = 80 | n = 80 | n = 83 |
|---|---|---|---|
| Mean age, years (SD) | 42.0 (10.0) | 40.4 (10.0) | 40.4 (10.4) |
| Female, n (%) | 80 (100.0) | 80 (100.0) | 81 (97.6) |
| Mean baseline pain score (SD) | 7.4 (1.6) | 7.5 (1.6) | 7.3 (1.5) |
| Pain responder rates 48 h post surgery† | 76.3% | 70.0% | 78.3% |
| Orthopedic surgery (Viscusi, 2019) [3] | n = 79 | n = 79 | n = 76 |
|---|---|---|---|
| Mean age, years (SD) | 43.6 (13.9) | 46.9 (13.8) | 43.3 (14.1) |
| Female, n (%) | 65 (82.3) | 66 (83.5) | 65 (85.5) |
| Mean baseline pain score (SD) | 6.6 (1.9) | 6.5 (1.7) | 6.7 (1.6) |
| Pain responder rates 48 h post surgery† | 62.0% | 65.8% | 71.1% |
| Acute pain in ED (Chang, 2006) [7] | Hydromorphone | Morphine | |
|---|---|---|---|
| n = 97 | n = 94 | ||
| Mean age (years) | 42 | 41 | |
| Female, n (%) | 62 (54) | 61 (65) | |
| Baseline pain score, n (%) | |||
| 6 | 5 (5) | 6 (6) | |
| 7 | 2 (2) | 10 (11) | |
| 8 | 13 (13) | 14 (15) | |
| 9 | 6 (6) | 14 (15) | |
| 10 | 71 (73) | 50 (53) | |
| Pain location, n (%) | |||
| Abdomen/pelvis | 66 (68) | 68 (74) | |
| Mean change pain score baseline – 2h‡ | -5.4 | -4.5 |
| Elective day surgery (Shanthanna, 2019) [8] | Hydromorphone | Morphine | |
|---|---|---|---|
| n = 203 | n = 199 | ||
| Mean age, years (SD) | 47.1 (14.0) | 46.1 (13.8) | |
| Female, n (%) | 126 (62) | 132 (66) | |
| Preoperative pain in the operative area, n (%) | 83 (41) | 83 (42) | |
| Type of surgery, n (%) | |||
| Laparoscopic | 185 (91) | 194 (97) | |
| Mean pain score 24 h post surgery (SD)‡ | 4.3 (2.2) | 4.1 (2.2) |
| General and gynecological surgery (Hong, 2008) [6] | Hydromorphone | Morphine | |
|---|---|---|---|
| n = 25 | n = 25 | ||
| Age (years), mean (SD)‡ | 44 (8) | 42 (12) | |
| Female, n (%)‡ | 22 (88%) | 23 (92%) | |
| Surgery type, n (open)‡ | 17 | 17 | |
| Duration of surgery (min), mean (SD)‡ | 203 (66) | 214 (87) | |
| Mean postoperative (8 h), pain (NRS; SD)‡ | 4.0 (2.5) | 3.5 (2.0) |
| Painful ambulatory surgery (Claxton, 1997) [5] | Fentanyl | Morphine | |
|---|---|---|---|
| n = 29 | n = 29 | ||
| Mean age, years (SD) | 34 (10) | 37 (11) | |
| Female, n (%) | 14 (48.3) | 8 (27.6) | |
| Type of surgery, n (%) | |||
| Arthroscopy | 22 (75.9) | 23 (79.3) | |
| Pain scores 24 h post surgery, n (%) | |||
| Mild | 4 (14) | 5 (17) | |
| Moderate | 22 (76) | 15 (52) | |
| Severe | 3 (10) | 9 (31) |
†
Equianalgesic to morphine using a noninferiority analysis.
‡
Not statistically significant.
ED: Emergency department; SD: Standard deviation.
Upon review of the literature search results, the only adverse event data sufficient for ITC analysis were for nausea and/or vomiting. Data for OIRD were reported in two studies (Chang 2006 [7] and Shanthanna 2019 [8]). Chang [7] utilized the outcomes of respiratory rate (RR <12 breaths/min) and O2 saturation (<90% as indicator for respiratory depression), while the Shanthanna study [8] defined respiratory depression as the number of patients needing treatment with naloxone. The lack of a common end point for respiratory depression and the very low incidence of OIRD [6–8] (consistent with previously reported literature [11]) precluded the ability to conduct an ITC analysis. The other end points of interest (somnolence, sedation, pruritus, constipation and SPID) were either not reported (SPID, constipation and somnolence) or occurred with very low incidence (sedation and pruritus) [6–8], precluding the ability to conduct an ITC analysis.
Articles for adjusted ITC between oliceridine & hydromorphone for rescue antiemetics
Six articles were identified for adjusted ITC between oliceridine and hydromorphone for rescue antiemetics. The Chang 2006 study reported the total number of patients experiencing nausea or vomiting, as well as the number of patients receiving antiemetics [7]. For the ITC analysis, the data for the number of patients receiving antiemetics were used for comparison. The Shanthanna 2019 study reported the number of patients with vomiting severe enough to need treatment and the number of patients with nausea severe enough to need treatment, separately [8]. The Hong 2006 study reported the number of patients with nausea and vomiting receiving treatment [6]. For the ITC analyses, the clinical end point used was the number of patients requiring treatment for nausea and/or vomiting from these three studies.
There were three articles describing the oliceridine data from two studies that were used in the ITC analysis: the Viscusi 2019 study (orthopedic surgery) [3], the Singla 2019 study (plastic surgery) [4] and the Beard 2021 article (combined orthopedic and plastic surgery data) [10]. In contrast to the hydromorphone studies, the oliceridine studies reported the number of patients with a complete GI response defined as no vomiting and not requiring antiemetic use. This was the clinical end point used for comparison in the ITC analyses. Also, only the data for oliceridine 0.35 and 0.5 mg (pooled) were used in the ITC analysis, since these dose regimens were found to be equianalgesic to morphine using a noninferiority analysis.
The Liu 2018 study reported the numbers of patients with the combined end point of postoperative nausea and vomiting (PONV) by grades (I–IV). There was no mention of antiemetic usage, and all patients in both arms had PONV [9]. A decision was made to not utilize the Liu study, although patients with grade III or IV nausea and/or vomiting could be used in an ITC analysis with the assumption that grade III or IV nausea and/or vomiting is severe enough to require antiemetics.
Articles for adjusted ITC between oliceridine & fentanyl for rescue antiemetics
Three studies were identified for adjusted ITC between oliceridine and fentanyl for rescue antiemetics. In addition to the two oliceridine studies (described above), the Claxton 1997 study reported on the number of patients who experienced nausea and vomiting in the hospital and after discharge as well as the number of patients that received an antiemetic [5]. For the ITC analysis, the data for the number of patients who received an antiemetic were used for comparison to the oliceridine data on the number of patients with a complete GI response as described above.
Table 3 shows the results of the ITC analysis.
| Difference in risk difference | 95% CI | p-value | Needed to treat (n) | 95% CI | p-value | Ref. | |
|---|---|---|---|---|---|---|---|
| Oliceridine vs hydromorphone | |||||||
| Orthopedic surgery vs Chang (2006) | 23.03% | 5.95%; 40.12% | 0.008 | 4.34 | 2.49; 16.82 | 0.008 | [7] |
| Plastic surgery vs Chang (2006) | 9.98% | -6.49%; 26.45% | 0.235 | [7] | |||
| Combined vs Chang (2006) | 16.55% | 2.36%; 30.74% | 0.022 | 6.04 | 3.25; 41.84 | 0.022 | [7] |
| Orthopedic surgery vs Shanthanna (2019) (vomiting) | 22.10% | 8.18%; 36.03% | 0.002 | 4.52 | 2.77; 12.22 | 0.002 | [8] |
| Plastic surgery vs Shanthanna (2019) (vomiting) | 9.05% | -4.11%; 22.21% | 0.178 | [8] | |||
| Combined vs Shanthanna (2019) (vomiting) | 15.62% | 5.47%; 25.77% | 0.003 | 6.40 | 3.88; 18.28 | 0.003 | [8] |
| Orthopedic surgery vs Shanthanna (2019) (nausea) | 20.43% | 5.72%; 35.14% | 0.006 | 4.89 | 2.85; 17.48 | 0.006 | [8] |
| Plastic surgery vs Shanthanna (2019) (nausea) | 7.38% | -6.60%; 21.37% | 0.301 | [8] | |||
| Combined vs Shanthanna (2019) (nausea) | 13.95% | 2.75%; 25.16% | 0.015 | 7.17 | 3.97; 36.36 | 0.015 | [8] |
| Orthopedic surgery vs Hong (2008) | 18.37% | -10.63%; 47.37% | 0.214 | ||||
| Plastic surgery vs Hong (2008) | 5.32% | -23.32%; 33.96% | 0.716 | ||||
| Combined vs Hong (2008) | 11.89% | -14.50%; 39.28% | 0.395 | ||||
| Oliceridine vs fentanyl | |||||||
|---|---|---|---|---|---|---|---|
| Orthopedic surgery vs Claxton (1997) | 8.03% | -15.90%; 31.95% | 0.511 | [5] | |||
| Plastic surgery vs Claxton (1997) | -5.02% | -28.55%; 18.51% | 0.676 | [5] | |||
| Combined vs Claxton (1997) | 1.54% | -20.43%; 23.51% | 0.890 | [5] | |||
CI: Confidence interval.
ITC: Oliceridine versus hydromorphone
The Chang study was a prospective, randomized, double-blind clinical trial comparing hydromorphone to morphine analgesia, conducted in the emergency department (ED) of an academic medical center [7]. The mean age of patients in the study was 42 years and 64% were females. The majority of patients presented with abdomen/pelvis pain. Baseline pain scores were not similar between the hydromorphone and morphine cohorts, with 79% of hydromorphone patients experiencing pain scores ≥9 compared with 68% of morphine patients. There was no statistically significant difference in changes in pain score from baseline to 2-h post-baseline. The mean age of patients in the oliceridine studies was 41 years (plastic surgery) and 45 years (orthopedic surgery). There were 99% females in the plastic surgery study and 84% females in the orthopedic surgery study. Baseline pain scores and pain responder rates were similar in both of the oliceridine studies. It should be noted that the Chang study is in an ED population, while the oliceridine studies evaluate pain management post surgery.
Three separate ITC analyses were conducted: oliceridine orthopedic surgery versus hydromorphone, oliceridine plastic surgery versus hydromorphone and oliceridine pooled versus hydromorphone (See Figure 1). Utilizing the total number of hydromorphone patients requiring antiemetics at any time in the ITC analysis versus oliceridine, oliceridine [both orthopedic surgery (RD: 23.03%; 95% CI: 5.95%; 40.12%; p = 0.008) and pooled data (RD: 16.55%; 95% CI: 2.36%; 30.74%; p = 0.022)] was found to significantly reduce the incidence of nausea and/or vomiting requiring antiemetics compared with hydromorphone. The ITC results for oliceridine plastic surgery versus hydromorphone were not statistically significant (RD: 9.98%; 95% CI: -6.49%; 26.45%; p = 0.235). The oliceridine number needed to treat (NNT) to achieve one more patient with a complete GI response was 6 (based on the pooled data).
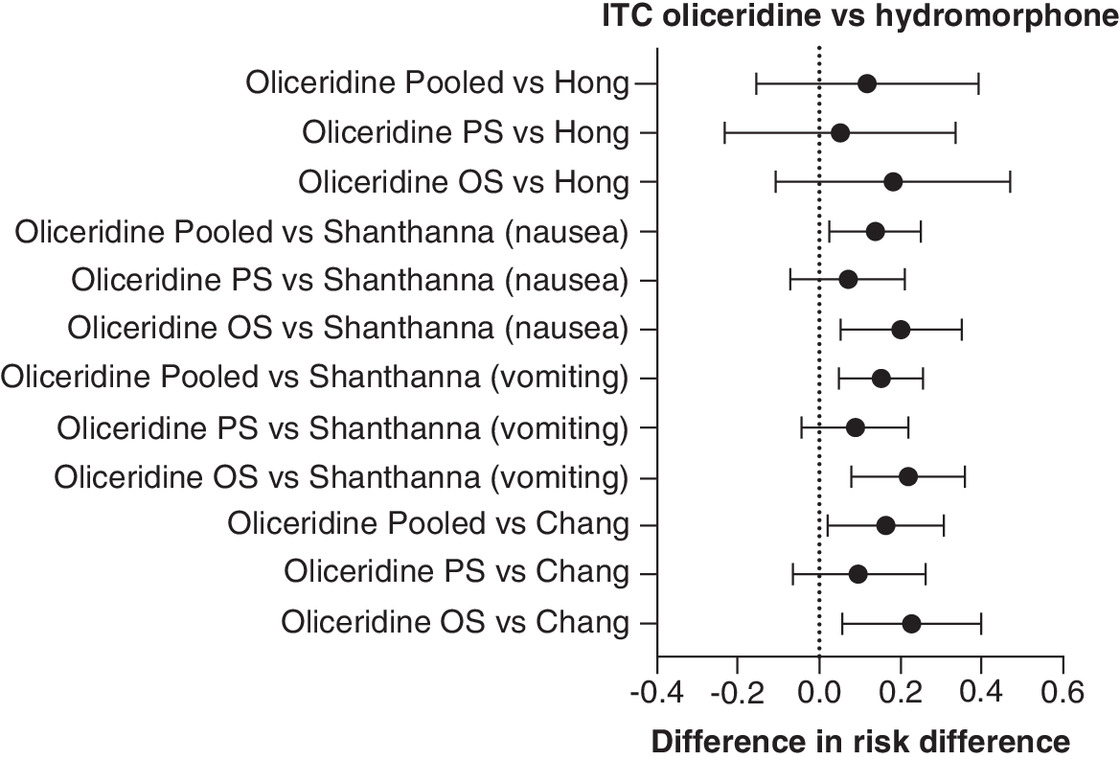
Figure 1. Indirect treatment comparison, oliceridine vs hydromorphone.
ITC: Indirect treatment comparison; OS: Orthopedic surgery; PS: Plastic surgery.
The Shanthanna study was an RCT comparing the use of morphine versus hydromorphone in ambulatory surgery patients. The mean age of these patients was approximately 46 years and 64% were females. The majority of these patients (94%) underwent laparoscopic surgery. There were no statistically significant differences in mean pain score at 24 h post surgery [8]. Utilizing the data from Shanthanna for both nausea severe enough to need treatment and vomiting severe enough to need treatment, the findings were similar to those seen in the ITC versus the Chang study. Oliceridine orthopedic surgery (vomiting: RD: 22.10%; 95% CI: 8.18%; 36.03%; p = 0.002 and nausea: RD: 20.43%; 95% CI: 5.72%; 35.14%; p = 0.006) and pooled (vomiting: RD: 15.62%; 95% CI: 5.47%; 25.77%; p = 0.003 and nausea: RD: 13.95%; 95% CI: 2.75%; 25.16%; p = 0.015) were found to significantly reduce the incidence of nausea or vomiting compared with hydromorphone. The ITC results for oliceridine plastic surgery (vomiting: RD: 9.05%; 95% CI: -4.11%; 22.21%; p = 0.178 and nausea: RD: 7.38%; 95% CI: -6.60%; 21.37%; p = 0.301) were not statistically significant.
The Hong study was an RCT comparing the use of morphine versus hydromorphone in general and gynecological surgery patients at an academic medical center. There were only 25 patients in each group. The mean age of these patients was 43 years and 90% were females. The majority of patients (68%) underwent open surgery. There were no statistically significant differences in mean pain scores at 8 h post surgery. The proportion of patients needing treatment for nausea and vomiting was not different in the two groups. The ITC analysis compared oliceridine (orthopedic surgery, plastic surgery and combined) versus treatment for nausea and vomiting in the Hong study and found that the RD was not statistically significant in any comparison (Table 3).
ITC: Oliceridine versus fentanyl
The Claxton study [5] was an RCT comparing postoperative analgesia among patients undergoing an ambulatory surgical procedure. The study only included 58 patients (29 in each group). The mean age of patients was approximately 35 years and only 38% of patients were females. The majority of patients experienced an arthroscopic procedure (shoulder, elbow, knee or ankle) and were given equal doses of morphine and fentanyl [5]. In-hospital side effects were similar in both groups, and time-to-recovery milestones were also similar. The proportion of patients needing antiemetics was not different in the two groups. The ITC analysis compared oliceridine (orthopedic surgery, plastic surgery and combined) versus antiemetic use in the Claxton study and the RD was not statistically significant in any comparison (Table 3 & Figure 2).
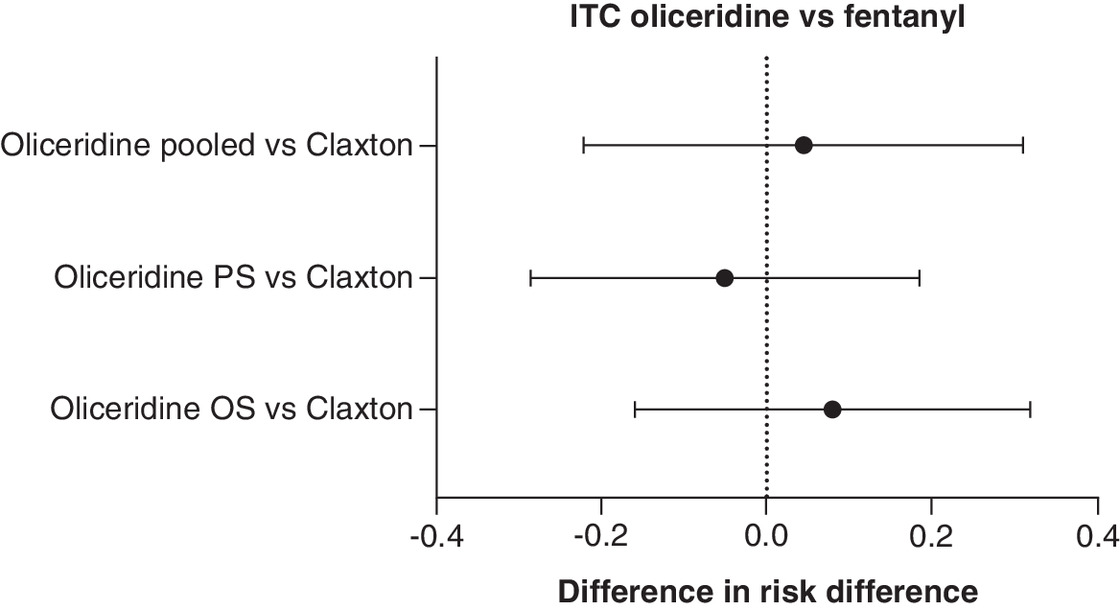
Figure 2. Indirect treatment comparisons, oliceridine vs fentanyl.
ITC: Indirect treatment comparison; OS: Orthopedic surgery; PS: Plastic surgery.
Discussion
This study used an indirect treatment comparison (ITC) methodology, a technique to provide a comparison between similar drugs for an indication where no head-to-head clinical trials exist [1]. The ITC method uses results from different clinical trials where there are common comparators and outcomes to make an indirect comparison and also assumes the comparability of the trials (i.e., similar design, setting, population and outcomes).
ITCs can provide useful information to supplement RCTs, which focus on demonstrating the safety and efficacy of a product for registration. In particular, an ITC can provide additional information on treatment outcomes for a drug that has been recently approved by the US FDA and for which no direct head-to-head comparisons against other available treatments yet exist. The primary outcome for this study was a comparison of rates of AEs, such as nausea and vomiting, between oliceridine and a common comparator.
Our ITC analyses found that patients treated with oliceridine were less likely to develop nausea and vomiting than patients treated with hydromorphone (2 of the 3 studies) but not with fentanyl. The exploratory analysis from two phase III trials conducted by Beard (2021) found that at equivalent analgesic effects, the odds of achieving complete GI response was two- to three-times higher with oliceridine than with morphine [10]. All of the studies used in these ITC analyses found no difference in nausea and vomiting between morphine and hydromorphone or morphine and fentanyl. Further, a meta-analysis comparing the clinical effects of hydromorphone and morphine (Felden 2011), found no difference in nausea and vomiting as well [14]. Given the consistent lack of difference in the incidence of nausea and vomiting between morphine and hydromorphone or fentanyl, and the two clinical trials for oliceridine versus morphine that show a difference in the incidence of nausea and vomiting favoring oliceridine, the results of the ITC analysis appear consistent with published studies.
The observed lack of statistical difference in postoperative nausea and vomiting (PONV) with oliceridine versus hydromorphone and/or fentanyl in patients undergoing plastic surgery procedures may be an artifact due to the high incidence of nausea and vomiting observed in these patients. The overall incidence of PONV in plastic surgery is estimated to be around 35%. The plastic surgery procedure associated with the greatest risk of PONV is breast augmentation. The incidence of PONV for breast augmentation is eight- to ten-times higher than for other types of plastic surgery [15]. Therefore the higher incidence of PONV in this population may affect the outcome of smaller studies. Much larger studies would be needed to compare the PONV rate among various opioids.
An important consideration in evaluating the likelihood an opioid will produce nausea and vomiting is the dose of the opioid administered. Doses used in the clinical trials included in the ITC were similar in terms of morphine-equivalent dosing. When comparing oliceridine to placebo, all doses of oliceridine were found to be superior to placebo in a 24- or 48-h time period utilizing a treatment responder composite end point [3,4]. Oliceridine dosing regimens utilized in phase II and phase III studies were previously found to be relatively equianalgesic to morphine [16–18]. In an exploratory analysis, oliceridine demand doses of 0.35 and 0.5 mg were found to be noninferior to morphine [4]. Therefore utilizing these studies in the ITC of morphine compared with oliceridine provided equianalgesic doses from which to directly compare morphine to fentanyl and hydromorphone and indirectly compare oliceridine to fentanyl and hydromorphone. In an exploratory analysis, when controlled for analgesic effect, oliceridine-treated patients exhibited statistically significant higher gastrointestinal response (no vomiting and no use of rescue antiemetics) compared with morphine-treated patients [10]. Our current ITC analysis confirms that oliceridine is less likely to cause vomiting than other opioids.
Limitations
Data comparing oliceridine in plastic surgery patients did not show a statistically significant difference versus hydromorphone in the ITC analyses. Patients in the Chang study had predominantly abdominal/pelvic pain [7], but it is not clear if this was soft tissue versus bone pain. Patients in the Shanthanna study underwent mainly laparoscopic surgeries, suggesting mostly soft tissue pain [8]. The population within the oliceridine plastic surgical procedures comparative group was 100% females. The results in this comparison may not be generalizable.
ITC analysis versus the Claxton data and the Hong data failed to show a benefit for oliceridine. This could be related to the small number of patients in these two studies.
Additional limitations include limited data availability for the ITC, differences in study populations and the fact that only GI adverse effects were analyzed. Additionally, differences in GI outcome definitions can limit the generalizability of these study findings.
The patient populations in these ITC analyses were seen in different clinical settings and experienced different types of pain. The Chang study looked at pain in patients presenting in an ED while the other studies examined postoperative pain. Among the postoperative pain population, there was variability as well. The oliceridine studies looked at postoperative pain present in patients following either abdominoplasty (plastic surgery) or bunionectomy (orthopedic surgery). The Hong study looked at postoperative pain in general and gynecological surgery patients similar to the Shanthanna study of postoperative pain in patients undergoing laparoscopic surgery. The Claxton study was predominantly postoperative pain in orthopedic surgery patients (93%), but there were also patients receiving breast augmentation surgery (plastic surgery). There were no statistically significant differences seen in any of the studies with regard to pain analgesia.
The GI clinical end point compared in these ITC analyses was also defined differently. The oliceridine studies used the end point of complete GI response defined as no vomiting or use of antiemetics, while all the other studies used the end point of nausea and vomiting requiring antiemetics. Some of these studies may have had patients with nausea and vomiting that did not require treatment, but that was not reported in any of the published studies, except for Chang. Since complete GI response is more stringent than end point than nausea and vomiting requiring antiemetics, the ITC analyses may underestimate the benefit of oliceridine.
Since the level of evidence provided by this ITC is low and no clinical trials or real-world head-to-head evidence exists comparing the three medications, clinical trials comparing oliceridine to hydromorphone and/or fentanyl are needed to confirm the results of these analyses.
Conclusion
In these ITC analyses, oliceridine use was shown to have statistically significant lower rates of nausea and vomiting compared with hydromorphone but not fentanyl use. The NNT analysis, comparing oliceridine to hydromorphone, showed a low number (<10), indicating a favorable GI tolerability profile of oliceridine versus hydromorphone.
Despite their limitations, ITCs can provide useful information to healthcare decision makers. Providers can use the information from this ITC to support the use of oliceridine in patients that may be at high risk of nausea and vomiting. Payers may consider this ITC comparison for reimbursement and benefit design between similar drugs in a class with oliceridine showing a lower incidence of nausea and vomiting in some surgeries. Additionally, the NNT results may be particularly relevant in a busy operation room setting where vomiting episodes can cause disruption to the healthcare team as well as be mentally and physically detrimental for the patient. Since the level of evidence provided by this ITC is low and no clinical trials or real-world head-to-head evidence exists comparing the three medications, clinical trials comparing oliceridine to hydromorphone and/or fentanyl are needed to confirm the results of these analyses.
Summary points
•
In the absence of head-to-head comparative effectiveness data between the treatments, indirect treatment comparisons (ITCs) may be used if the treatments being compared were evaluated in clinical trials against the same placebo or a common comparison treatment.
•
In acute pain management, the effects and adverse effects of oliceridine, fentanyl and hydromorphone have all been directly compared in clinical trials to morphine, but oliceridine has not been compared directly to fentanyl or hydromorphone.
•
Since all three drugs have been compared directly to morphine in clinical trials, ITCs were conducted using the three drugs' clinical trial data to compare their adverse effects of nausea and/or vomiting.
•
In an ITC comparing oliceridine study results with hydromorphone study results, oliceridine was found to significantly reduce the incidence of nausea and/or vomiting requiring antiemetics compared with hydromorphone (both orthopedic surgery and pooled data), while ITC results for oliceridine versus hydromorphone in plastic surgery were not statistically significant.
•
In an ITC comparing oliceridine to a fentanyl study of fentanyl usage in orthopedic surgery, comparisons showed no statistically significant difference in risk difference, so further ITC analyses were not conducted.
•
In conclusion, in ITC analyses, oliceridine was found to significantly reduce the incidence of nausea and/or vomiting or the need for antiemetics in orthopedic surgery compared with hydromorphone, while results in plastic surgery were not significantly different.
•
Since the level of evidence provided by this ITC is low and no clinical trials or real-world head-to-head evidence exists comparing the three medications, clinical trials comparing oliceridine to hydromorphone and/or fentanyl are needed to confirm the results of these analyses.
Author contributions
Authors J Biskupiak, G Oderda and D Brixner were responsible for the conception and design of the work; the acquisition, analysis and interpretation of data for the work; and for drafting and revising the work. TL Wandstrat was responsible for the conception and design of the work and for drafting and revising the work. All authors gave final approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors thank D Whiteman (of Syneos Health) for his editorial assistance and medical writer KJP Lindberg (of Blue Raven Services, Inc.) for her editing assistance.
Financial disclosure
This work was supported by a grant from Trevena, Inc. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interest disclosure
Todd L Wandstrat is an employee of Trevena and owns Trevena stock. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing and editorial support were provided by KJP Lindberg of Blue Raven Services, Inc., and were funded by Trevena, Inc.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/40.0/
References
Papers of special note have been highlighted as: • of interest
1.
Hoaglin DC, Hawkins N, Jansen JP et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 2. Value Health 14(4), 429–437 (2011).
2.
Garimella V, Cellini C. Postoperative pain control. Clin. Colon Rectal Surg. 26(3), 191–196 (2013).
3.
Viscusi ER, Skobieranda F, Soergel DG, Cook E, Burt DA, Singla N. APOLLO-1: a randomized placebo and active-controlled phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the micro-opioid receptor, for management of moderate-to-severe acute pain following bunionectomy. J. Pain Res. 12, 927–943 (2019).
• In the APOLLO-1 study, a phase III, double-blind randomized controlled trial (RCT) in patients with acute pain following bunionectomy, oliceridine was found to be an effective IV analgesic for pain relief and showed a favorable safety and tolerability profile compared to morphine.
4.
Singla NK, Skobieranda F, Soergel DG et al. APOLLO-2: a randomized, placebo and active-controlled phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the mu-opioid receptor, for management of moderate to severe acute pain following abdominoplasty. Pain Pract. 19(7), 715–731 (2019).
• The APOLLO-2 study, a phase III, double-blind RCT in patients with moderate-to-severe pain following bunionectomy, concluded that oliceridine in 0.35 mg and 0.5 mg doses was an effective IV analgesic for pain relief and had a favorable safety and tolerability profile compared to morphine.
5.
Claxton AR, McGuire G, Chung F, Cruise C. Evaluation of morphine versus fentanyl for postoperative analgesia after ambulatory surgical procedures. Anesth. Analg. 84(3), 509–514 (1997).
• This article describes a study comparing IV morphine and fentanyl use after painful ambulatory procedures with respect to analgesic efficacy, the incidence of side effects, and impact on the patient's readiness for discharge. Morphine produced a better quality of analgesia but was associated with an increased incidence of nausea and vomiting, the majority of which occurred after discharge.
6.
Hong D, Flood P, Diaz G. The side effects of morphine and hydromorphone patient-controlled analgesia. Anesth. Analg. 107, 1384–1389 (2008).
• In this prospective, randomized, double-blind trial of 50 general and gynecological surgery patients comparing the safety profiles of hydromorphone and morphine, the study found no systematic difference between morphine and hydromorphone in opioid-related side effects.
7.
Chang AK, Bijur PE, Meyer RH, Kenny MK, Solorzano C, Gallagher EJ. Safety and efficacy of hydromorphone as an analgesic alternative to morphine in acute pain: a randomized clinical trial. Ann. Emerg. Med. 48(2), 164–172 (2006).
• In this prospective, randomized, double-blind clinical trial of 198 adult patients comparing the use of intravenous hydromorphone and intravenous fentanyl for acute pain management in an ED, intravenous hydromorphone (0.015 mg/kg) was shown to be a feasible alternative to intravenous morphine (0.1 mg/kg).
8.
Shanthanna H, Paul J, Lovrics P et al. Satisfactory analgesia with minimal emesis in day surgeries: a randomised controlled trial of morphine versus hydromorphone. Br. J. Anaesth. 122(6), e107–e113 (2019).
• This multicenter study of 402 patients having ambulatory surgery, randomized to receive either morphine or hydromorphone, found no significant differences between the two drugs regarding analgesia and common side effects.
9.
Liu Y, Yang L, Tao SJ. Effects of hydromorphone and morphine intravenous analgesia on plasma motilin and postoperative nausea and vomiting in patients undergoing total hysterectomy. Eur. Rev. Med. Pharmacol. Sci. 22(17), 5697–5703 (2018).
10.
Beard TL, Michalsky C, Candiotti KA et al. Oliceridine is associated with reduced risk of vomiting and need for rescue antiemetics compared to morphine: exploratory analysis from two Phase III randomized placebo and active controlled trials. Pain Ther. 10(1), 401–413 (2021).
• This exploratory analysis analyzing two phase III studies to assess gastrointestinal tolerability found that when controlled for analgesic effects (constant SPID-48/24), the odds ratio for complete GI response was higher with oliceridine than morphine, suggesting better GI tolerability with oliceridine.
11.
Dahan A, Aarts L, Smith TW. Incidence, reversal, and prevention of opioid-induced respiratory depression. Anesthesiology 112(1), 226–238 (2010).
12.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 50(6), 683–691 (1997).
• Describes the Bucher's anchor-based indirect comparison method.
13.
Greenland S. Model-based estimation of relative risks and other epidemiologic measures in studies of common outcomes and in case-control studies. Am. J. Epidemiol. 160(4), 301–305 (2004).
14.
Felden L, Walter C, Harder S et al. Comparative clinical effects of hydromorphone and morphine: a meta-analysis. Br. J. Anaesth. 107(3), 319–328 (2011).
15.
Keramidas E, Vasileiou I, Pascovitis A et al. Breast augmentation: reducing postoperative nausea and vomiting. A prospective study. J. Anesth. Crit. Care Open Access 7, 00285 (2017).
16.
Soergel DG, Subach RA, Burnham N et al. Biased agonism of the mu-opioid receptor by TRV130 increases analgesia and reduces on-target adverse effects versus morphine: a randomized, double-blind, placebo-controlled, crossover study in healthy volunteers. Pain 155(9), 1829–1835 (2014).
17.
Viscusi ER, Webster L, Kuss M et al. A randomized, phase II study investigating TRV130, a biased ligand of the mu-opioid receptor, for the intravenous treatment of acute pain. Pain 157(1), 264–272 (2016).
18.
Singla N, Minkowitz HS, Soergel DG et al. A randomized, phase IIb study investigating oliceridine (TRV130), a novel micro-receptor G-protein pathway selective (mu-GPS) modulator, for the management of moderate to severe acute pain following abdominoplasty. J. Pain Res. 10, 2413–2424 (2017).
Information & Authors
Information
Published In
Copyright
© 2024 Trevena, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 24 March 2023
Accepted: 21 February 2024
Published online: 18 March 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Gastrointestinal adverse effects associated with the use of intravenous oliceridine compared with intravenous hydromorphone or fentanyl in acute pain management utilizing adjusted indirect treatment comparison methods. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0041
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Li-Hao Rao, Ze-Xue Yang, Lun Huang, Li-Dong Zheng, The Effect of Oliceridine Versus Sufentanil on the Quality of Postoperative Recovery in Patients Undergoing Laparoscopic Cholecystectomy, Journal of Pain Research, 10.2147/JPR.S591720, Volume 19, (1-10), (2026).
- Ye Liu, Mingshu Tao, Biran Dai, Xia Yin, Xinyu Gu, Jie Xiao, Jun-Li Cao, Weifeng Yu, Liqun Yang, Song Zhang, Effect of oliceridine on hypoxia during sedated hysteroscopy: a Phase 4 randomized clinical trial, Communications Medicine, 10.1038/s43856-026-01562-1, 6, 1, (2026).
- Na Hu, Chong Wang, Qi-Qi Zhang, Zhong-Jun Zhang, Xian Ding, Yu Zhang, Oliceridine versus Sufentanil for Postoperative Recovery and Opioid-Related Adverse Events in Patients Undergoing Thoracoscopic Lobectomy: A Randomized Double-Blind Controlled Trial, Drug Design, Development and Therapy, 10.2147/DDDT.S582482, Volume 20, (1-12), (2026).
- Jinfeng Cao, Xiaoyu Gu, Xinyang Zhang, Yao Cheng, Liuqin Jiang, Determination of the effective dose of oliceridine combined with propofol using the modified Dixon’s up-and-down method in painless gastroscopy, Frontiers in Pharmacology, 10.3389/fphar.2025.1620158, 16, (2025).
- Yuxiang Meng, Sumin Yuan, Hengrui Zhang, Zijie Ling, Chenyang Shi, Yang Niu, Li Zhang, Zhibiao Xu, Yujun Liu, Kang Zhou, Su Liu, Linlin Zhao, Comparison of oliceridine and sufentanil in patient - controlled intravenous analgesia for post - thoracoscopic nausea and vomiting: a prospective, double - blind, randomized controlled trial, Frontiers in Pharmacology, 10.3389/fphar.2025.1576154, 16, (2025).
- Dongxue Wu, Yeqing Liao, Yanlin Qin, Yafeng Wang, Bing Xu, Qiuling Chen, Xianting Wang, Xiaoshan Wu, Yalan Li, Xuehai Guan, Estimation of ED50 and ED95 of Oliceridine Required to Suppress the Bronchoscopy Response in Patients Undergoing Fiberoptic Bronchoscopy Under Sedation with Cipepofol: An Up-and-Down Sequential Allocation Trial, Drug Design, Development and Therapy, 10.2147/DDDT.S535435, Volume 19, (8879-8889), (2025).
- Chengya Huang, Biying Liu, Shouyu Xie, Yunyun Zhang, Kun Liu, Yuwei Qiu, Jingxiang Wu, Evaluating the Opioid-Related Adverse Events of Oliceridine Versus Conventional Opioids in Patient-Controlled Analgesia After Thoracoscopic Lung Resection: A Retrospective Cohort Study, Drug Design, Development and Therapy, 10.2147/DDDT.S532778, Volume 19, (5929-5939), (2025).
- Kun Yi, Wenjie Sun, Wen Yu, Shibiao Chen, Overview and Prospects of the Clinical Application of Oliceridine, Drug Design, Development and Therapy, 10.2147/DDDT.S525471, Volume 19, (5415-5430), (2025).
- Zhiyong Tang, Guangfen Yin, Yaohan Yu, Yinghong Luo, Shuqin Tian, Qingdong Zhang, Yanwei Fang, Qinghang Xuan, Determination of ED90 and ED99 of Oliceridine combined with Propofol in inhibiting responses to gastroscope insertion: a biased coin up-and-down design, BMC Anesthesiology, 10.1186/s12871-025-03052-8, 25, 1, (2025).
- Yulin Liu, Ying Zhu, Hong Fu, Tolerability of different doses of oliceridine versus traditional opioids in acute pain management: a systematic review and meta-analysis, Scientific Reports, 10.1038/s41598-025-95978-9, 15, 1, (2025).
- See more