Screening for diminished ovarian reserve in Portugal: a cost-saving answer to shorten the fertility journey
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Assess the budget impact of nationwide screening for diminished ovarian reserve (OR), via anti-Müllerian hormone (AMH) levels, to the Portugal National Health System (NHS). Patients & methods: The clinical journey was determined using literature and the family planning decision-making process/response using survey results. A panel of four local clinicians validated all assumptions/inputs. Results: Screening for OR led to an expected savings of € 9.4 million for the NHS, driven by a 24% reduction in medically assisted reproduction (MAR) use. When needed, referral for MAR was earlier and more women used first-line versus second-line techniques. The model estimated a 12% decrease in failure. Conclusion: This model shows AMH screening may allow more informed decisions, leading to a shorter fertility journey, more efficient use of treatments, and substantial cost-savings for the NHS.
Since 1960, the Portuguese national birth rate has been decreasing, reaching 8.2 children per 1000 habitants in 2020 [1], one of lowest rates in Europe [2]. This is correlated with a continuous decrease in total population, as there have been more deaths than births in Portugal for 12 consecutive years [3].
Furthermore, since 1982, the average age of women at birth of first child has increased from 25 to 30 years [1]. This is especially relevant since women experience continuous reproductive aging from birth until menopause, which leads to a continuous decrease in natural birth rates (Hansen et al.) and a consequent increase in the need for medically assisted reproduction (MAR) [4].
Infertility is a disease of the reproductive system, defined as the non-achievement of a clinical pregnancy after 12 months of regular, unprotected sexual intercourse, due to a physical or metabolic impairment of a person's capacity to reproduce. Several factors can influence fertility, from lifestyle to reproductive health, however, diminished ovarian reserve (OR) alone accounts for 30% of infertility cases among women [5–7].
According to national and international guidelines, if conception is not achieved after one year, it is recommended that the couple seeks medical advice with a general practitioner (GP) or an obstetrician-gynaecologist (Ob-Gyn), where they can be clinically evaluated for fertility issues [4]. In the event of an inconclusive evaluation, referral to a fertility expert should be considered for further analysis [8–10]. Once a clear diagnosis is established, treatment falls into three categories: medical management; surgical management; or medically assisted reproduction (MAR) [8,9]. Treatment selection is a shared decision between patient and physician, based on patient's medical history, physical examination, and diagnostic testing results [11]. Typically this process takes around 6–12 months from diagnosis until reaching a treatment decision [4].
Anti-Müllerian hormone (AMH) is a dimeric glycoprotein produced in females by the granulosa cells of pre-antral and small antral follicles during their maturation process [12,13]. The measurement of circulating AMH reflects the number of primordial follicles present in the ovaries. Additionally, it can also identify iatrogenic damage to the OR and predict the ovarian response to hyperstimulation for MAR [13,14]. Therefore, AMH is considered as an accurate biomarker for OR assessment.
Moreover, there is a correlation between AMH levels and reproductive aging [15–18]. Typically, a woman's AMH levels achieve its peak in her early twenties, after which they begin to decrease until menopause. Naturally and at any age, there may be significant variations in AMH levels among women [12,13,19], however the greatest variability is seen in women aged ∼25 years. There is also evidence sustaining that the AMH decrease may be associated with the quantity and/or quality of oocytes, mainly in women with ≥35 years of age [20].
Therefore, screening for diminished OR in young women could improve the outcome of family planning counselling by providing women with more information, giving them greater decision-making power in their fertility efforts. When women face a low AMH result, they may decide not to change their reproductive planning, or to instead expedite it, or even to consider oocyte cryopreservation – thinking about a future pregnancy. Expediting the reproductive plan, by attempting to conceive earlier, could improve pregnancy success rates, both naturally and with MAR if needed, as women would start at a younger age than previously planned. Additionally, this could potentially reduce costs associated with MAR procedures, while allowing for improvement of the birth rate.
Given this rationale, a budget impact model (BIM) was developed to evaluate the potential economic impact to the Portuguese National Health System (NHS) of implementing a nationwide screening program for diminished OR in women aged 25–30, through the assessment of serum AMH levels.
Patients & methods
To assess the potential budget impact of implementing a diminished OR screening with an AMH test, two scenarios were compared – the current practice, where no screening is performed, and a proposed scenario, where AMH test is offered at a family planning appointment with a GP or an Ob-Gyn. An individual patient-level Markov model was developed to simulate the family planning process, fertility projections, and reproductive care in the public setting.
The model's design was developed using two primary resources – (1) a nationwide survey to the target population, assessing women's willingness to perform the test and their hypothetical course of action afterward; and (2) assessing the current clinical practice in Portugal, achieved by gathering evidence from published literature related to resource consumption throughout the process, complemented and validated by local experts through a modified-Delphi panel.
The study was conducted in accordance with applicable regulations, including relevant European Union directives and regulations, and the principles of the Declaration of Helsinki. The model did not use any patient data from any institution and was based only on published data, expert's opinion, and (anonymous) aggregate summary results of a previously conducted, voluntary electronic survey performed for marketing purposes. According to local Portuguese Law No. 21/2014 of 16 April, the survey, whose results were used in this analysis, did not meet the criteria for a clinical study, and thus, no ethics committee vote was required.
Patient population
The target population, assumed to represent the population eligible for OR screening, was Portuguese women aged 25–30 years (n = 330,181 in 2019) [21] who have not previously been pregnant, nor attempted to become pregnant. Subsequent pregnancies were not considered due to the complexity and potential impact on success rates and fertility strategies, and the huge uncertainty and lack of data related to women's will to pursue a second child, as well as time-intervals between them.
The budget impact analysis was performed from the perspective of the Portuguese NHS, therefore all economic aspects consider the local legislation around MAR and related resources reimbursement, with costs reported in Euros (2020). A hypothetical population of 250,000 women were individually simulated through the model to estimate the average total cost for the NHS of each woman's reproductive journey. This average cost was then applied to the target population to estimate the total budget impact. A time horizon of 15 years was assumed as the necessary time-period to cover all attempts and pregnancy outcomes. However, one individual's flow would not be extended for more than 4 years. A discount rate was not applied in the base model, but multiple rates were tested in a deterministic sensitivity analysis.
The economic modelling was performed in TreeAge Pro Healthcare, Version 2021. The statistical significance of comparisons was assessed through a Q-square test.
Modeling the decision-making process to undergo & react to an AMH test
To model the decision-making process of a woman's willingness to undergo the AMH test, along with the potential impact that the results could have on fertility choices and family planning, the results of a market research survey conducted by Roche Diagnostics were utilized [22]. The anonymous voluntary survey was conducted independent of this study, with the data available on file.
As the marketing data have not been previously published, we will briefly describe the methods used. The survey featured a 16-item questionnaire performed through a CAWI (Computer Assisted Web Interviewing) system (Supplementary Appendix). The survey was conducted on 300 women aged 25–30 years, randomly selected from an online access panel that had previously been informed of the opportunity through an e-mail with related information. The exclusion criteria were women that had previously been pregnant, undergone fertility evaluation, or were diagnosed with a reproductive disorder. The survey questionnaire that was used is available in the Supplementary Materials.
The results of the survey, which were utilized in this economic analysis, showed that 73.3% of women were willing to have children, 6.72% planning it to the next 12 months, 53.42% to the following 1–3 years, 33.04% to the following 4–6 years, and 6.82% to ≥7 years. Overall, 80% of responders, including those not planning to have children, were interested in knowing their OR status, of which 88.3% would perform an AMH test knowing that it only takes a blood sample collection. Among the ones not interested in performing the test (11.7%), 48.5% were only concerned about its price. Other reasons included fear of feeling discomfort or pain (39.4%), trouble in having access to the test (21.2%) and fear of anguish/anxiety (12.1%) and unspecified reasons (6.1%) – multiple reasons could be reported.
Lastly, the survey showed that if women had diminished AMH levels, 83% would change their reproductive plans, with 35.9% considering accelerating their first pregnancy to the upcoming two years. A significant percentage would consider oocyte cryopreservation (27.5%), and the remaining would either consider alternative ways, such as adoption if unable to conceive, or not change their plans after getting the information.
Expert panel: fertility care pathway
A modified-Delphi panel was conducted to define the reproductive care clinical pathway in Portugal. First, 4 fertility experts answered an extensive questionnaire individually, second, they were engaged in a virtual interactive session to solidify data needed to build the model. It was consensual that, for women below 30 years of age, AMH levels are most likely a marker of oocyte quantity, rather than quality, and therefore would not affect pregnancy rates in the short-term. Although it isn't possible to establish an infertility diagnosis, nor a direct correlation with treatment success rates, based on AMH levels only, it was recognized that low/extremely low AMH could influence women's fertility planning, and when applicable and in association with the woman's age, the treatment of choice.
Given these findings, the BIM took a conservative approach, assuming low AMH had no direct impact on natural pregnancy rates, only affecting the decision on reproductive planning and choice of MAR, when applicable. However, as natural pregnancy and MAR success rates are impacted by age, there was indeed an indirect effect on the success rates, as 35.9% of women would accelerate their reproductive plans after a low AMH result, which leads to a higher probability of success simply by starting at a younger age [22].
Model costs
The simulated costs in this analysis are based on the reimbursement process for MAR in Portugal. Reimbursement is comprised of bundled payments, in which the NHS, based on hospitals' previous data, covers the average costs. Per definition, ovulation induction (OI) and intrauterine insemination (IUI) are considered first-line MAR options, while in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) are second-line options, although not necessarily applied in a sequential order. Following the legislation available at the time of this study, it was assumed that women could complete a maximum of 3 cycles of first-line treatments, if younger than 42 years at the admission, as well as 3 cycles of second-line treatments, up until 40 years of age [23]. One MAR cycle is composed of a follicle aspiration, which could result in the retrieval of several oocytes and generation of several embryos, with an average of 1–2 embryos being transferred. The remaining embryos cryopreserved for future transfers, if required, were considered to be included in the initial bundled cost [23]. The cost used in the model are shown in Table 1.
| Resource | Cost per cycle (SNS) | Source |
|---|---|---|
| AMH Test | 13.00 € | Roche internal data on file |
| Medical appointment (GP or gynaecologist / obstetrician) | 31.00 € | Informative deliberation no. 15/2019 /DPS/ ACSS, Code: 57710 |
| Fertility support appointment (initial) | 88.00 € | Informative deliberation no. 15/2019 /DPS/ ACSS, Code: 57720 |
| Ovarian Induction (OI) | 133.00 € | Informative deliberation no. 15/2019 /DPS/ ACSS, Code: 57730 |
| Intrauterine Insemination (IUI) | 335.00 € | Informative deliberation no. 15/2019 /DPS/ ACSS, Code: 57740 |
| In vitro fertilization (IVF) | 2,098.00 € | Informative deliberation no. 15/2019 /DPS/ ACSS, Code: 57750 |
| Intra-cytoplasmic sperm injection (ICSI) | 2,308.00 € | Ordinance no. 254/2018, Article no. 6 |
| Intra-cytoplasmic injection of surgically collected sperm (ICSI) | 2,937.00 € | Informative deliberation no. 15/2019 /DPS/ ACSS, Code: 57700 |
| Total | ||
|---|---|---|
| Current practice | Weighted by patients distributions among the correlated MAR lines | |
| 1st Line (OI & IUI) | 329.49€ | |
| 2nd Line (IVF & ICSI) | 2,508.25 € | |
| Proposed practice | Weighted by patient distributions among the correlated MAR lines and includes one AMH test and GP appointment extra of package | |
| Low AMH | ||
| 1st Line (OI & IUI) | 278.18 € | |
| 2nd Line (IVF & ICSI) | 2,267.15 € | |
| Extremely low AMH | ||
| 1st Line (OI & IUI) | 270.54 € | |
| 2nd Line (IVF & ICSI) | 2,215.90 € |
*According to the informative deliberation 15/2019 /DPS/ ACSS, it is assumed that the Specialist visit package already covers for the diagnosis resources, and ART lines packages covers patients monitoring resources, as well as any co-medicine prescribed in the scope of ART procedure.
AMH: Anti-Müllerian hormone; GP: General practitioner; OI: Ovarian induction; IUI: Intrauterine insemination; IVF: In vitro fertilization; ICSI: Intra-cytoplasmic sperm injection; MAR: Medically assisted reproduction; ACSS: Administração Central do Sistema de Saúde; DPS: Departamento de Gestão e Financiamento de Prestações de Saúde; SNS: Serviço Nacional de Saúde.
To estimate the cost of each MAR cycle, a weighted average of the treatment line was calculated based on the overall age-specific distribution of each technique in the clinical practice (Supplementary Materials & Supplementary Table 3). Therefore, the average cost of first-line MAR was estimated from the bundled cost of OI and IUI techniques, weighed by the proportion of women undergoing each technique. The same rationale was applied for second-line MAR, considering the proportion of women performing IVF versus ICSI.
The model only considers medical costs supported by the NHS, with cost data extracted from the official national fee schedules [24]. Costs were based on the bundled costs per MAR cycle, which includes diagnosis confirmation and monitoring resources, concomitant medicines, and related procedures. Costs related to preliminary procedures before infertility diagnosis, e.g., GP appointments and AMH test, are covered separately, applying an AMH average price of 13.00 €. Since the NHS does not cover alternative approaches such as oocyte cryopreservation or adoption, these are not explored in the analysis [24]. Additionally, the model did not incorporate costs related to the social and psychological impacts that may result from fertility issues.
Model structure & assumptions
Current practice (no screening)
To begin, the current practice arm estimated the distribution of theoretical ages at which the cohort of women would start trying to conceive, ranging from women 25–30 years old. This projection is based on the survey data [22], with the following possibilities: within the next 12 months, 1–3 years, 4–6 years, and >7 years. Within this timeframe, the probability is evenly distributed among the period (e.g., if 36% of women that are 25 years old wanted to have children within 1–3 years, 12% were assumed to be at age 26 (wait one year), 12% at age 27 (wait two years) and 12% at age 28 (wait three years). The maximum horizon was assumed as 10 years. Success or failure was estimated based on the average natural pregnancy rates between ages of 25–44 (Supplementary Materials & Supplementary Table 2). Moreover, the expert panel estimated that approximately 50% of women among the general population would seek a medical appointment and ultimately receive an infertility diagnosis after 1-year of failed attempts, and 44.3% would pursue to MAR. This is aligned with the estimates of the Conselho Nacional De Procriação Medicamente Assistida (CNPMA) [4].
To reflect the local practice, the experts validated the distribution among MAR techniques across age groups, and clinical pregnancy rates per MAR within the age ranges were publicly available [4]. Due to lack of specific data, pregnancy success rate per cycle was assumed to be the same for both first-line treatments, and the rate for second-line treatments was assumed as the average of IVF and ICSI pregnancy rates. The same success rate per line of MAR was applied for all three possible cycles. Final rates are shown in the Supplementary Materials (Supplementary Table 2).
It is important to note that the elapsed time within the model leads to an increment in the patient's age, which potentially negatively affects the pregnancy rate. Once referred to MAR, the time elapsed in the simulation included the time to treatment beginning, cycle duration (∼20 days), time until pregnancy confirmation and waiting time between re-trying cycles. When applicable, all three cycles of first-line treatments were assumed to be completed during a one-year period. It only extended beyond one year if the patient moved to second-line treatments, after failing first line. However, for second-line MAR, it was assumed that, due to the lack of human resources, equipment and logistics to meet NHS demand [25–27], there was an usual waiting period of 6–12 months to get the approval to start the treatment, with no more than one cycle per year. Therefore, if second-line treatments are recommended as the first approach, then the first cycle would occur at the end of the decision year, and the second and third cycles would increment one year of age each (Figure 1).
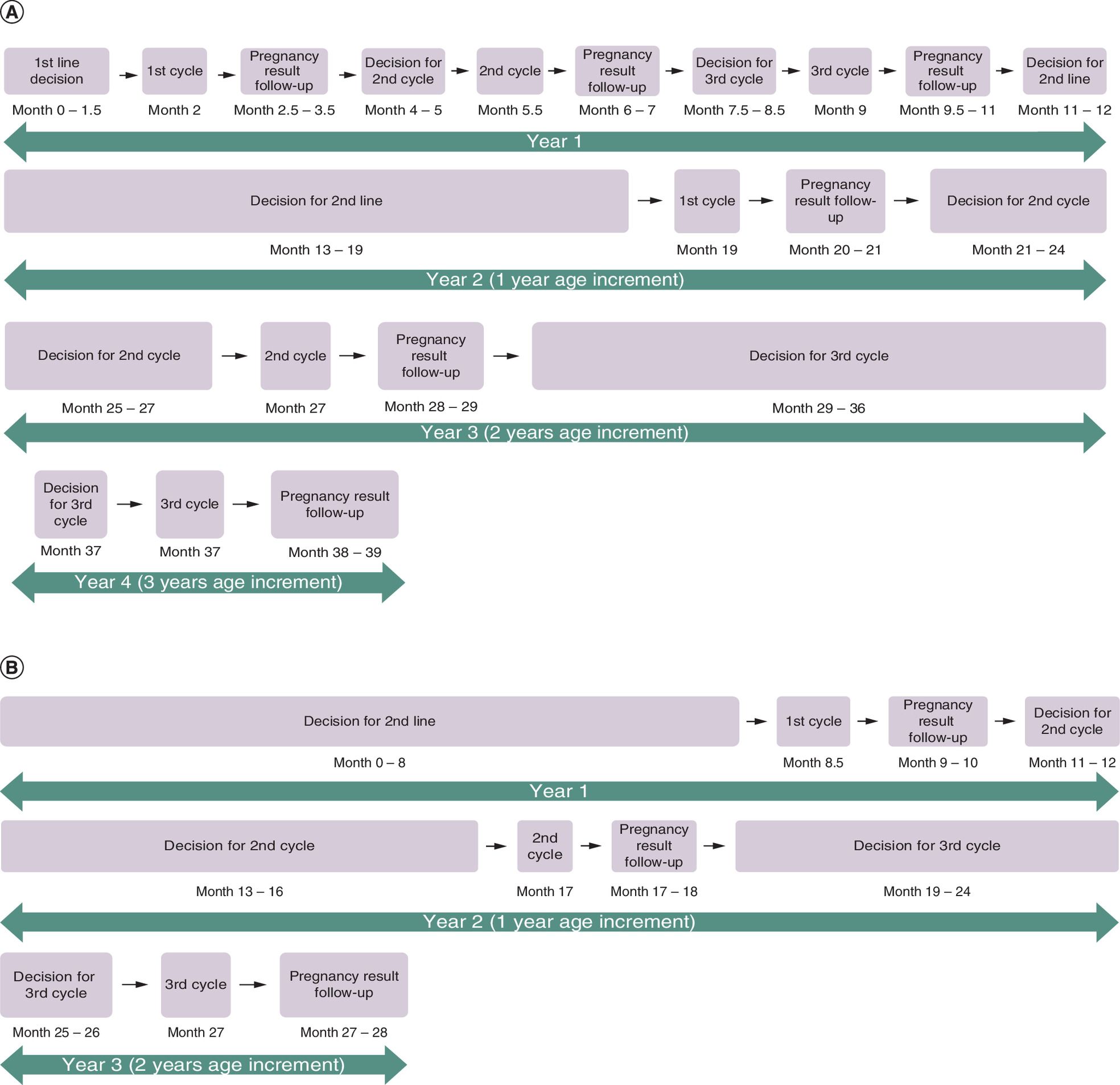
Figure 1. Elapsed time, steps and patient's age once referred to medically assisted reproduction.
(A) First-line medically assisted reproduction as first choice. (B) Second-line medically assisted reproduction as first choice.
In accordance with the recommendations of the experts, it was assumed that patients who first attempted a second-line treatment and failed all three cycles would not go through first-line treatments. Therefore, if pregnancy was not achieved after the conclusion of these cycles, the case is classified as a failure.
Proposed practice (with AMH screening)
The proposed practice begins with the first family planning appointment. In this study arm, it was assumed that women had not yet started their reproductive project. To evaluate the maximum potential impact of implementing a nationwide screening for diminished OR, the analysis assumed that 100% of the target population would be eligible for AMH testing. However, in the base-case analysis, the target population was adjusted by the percentage of women that would be interested in (80%) and would definitely (88.3%) perform the AMH test, according to the survey results [22], with the remaining women following the current practice.
From literature review, and further validation with the expert panel [28], it was assumed that 10% of women among the general population would have low AMH (>0.4 ng/ml; <1.09 ng/ml) [29], with 2% of these being extremely low levels (<0.4 ng/ml) [30–35]. It was assumed that women with normal AMH would follow the current practice, as their reproductive plan would not be affected.
As already discussed above, if a low AMH was revealed, it was assumed that 35.9% of women would accelerate their first pregnancy to the upcoming 2 years [22]. Considering the NHS perspective, cryopreservation and alternative methods are not covered in this analysis.
The ‘starting’ age was estimated in the same way as the current practice (Supplementary Materials & Supplementary Table 1). The model assumed that if a women received a low AMH result, that: 1) the 35.9% of women originally planning a later pregnancy (≥2 years from present) would instead begin attempts within the next 2 years [split equally between one and two years]; and 2) the decisions of those already planning to get pregnant within the next two years were not affected by receiving a low AMH result. In a conservative approach, the probabilities of a successful natural pregnancy, search for medical assistance (50%) and proceeding to MAR (44%) were assumed to be the same as for the current practice and, thus, low AMH results were not assumed to have a direct impact on the success rates (Supplementary Materials & Supplementary Table 2). Patient flow and elapsed time while performing MAR cycles were also assumed not to be influenced by AMH levels, unless extremely low (Supplementary Materials & Supplementary Table 2). However, low/extremely low AMH have an impact in the choice of MAR technique (Supplementary Materials & Supplementary Table 3), as reported by the expert panel.
The model flow diagram is presented in Figure 2.
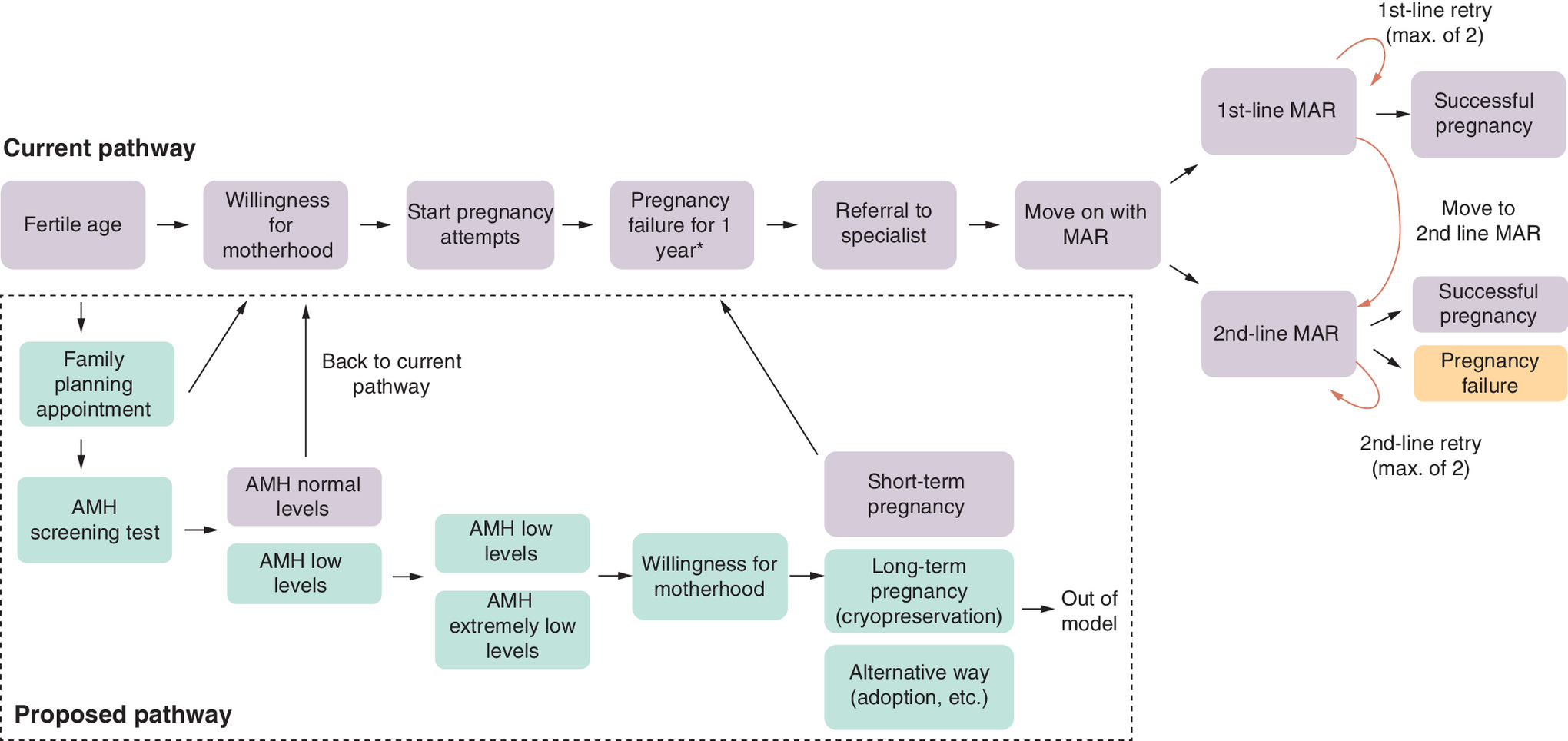
Figure 2. Model structure diagram.
*Infertility diagnosis is assumed, per definition
AMH: Anti-Müllerian hormone; MAR: Medically assisted reproduction.
Sensitivity analysis
One way sensitivity analysis
A one-way deterministic sensitivity analysis (DSA) was conducted to test the impact of some variables uncertainty and assess the robustness of the findings. Despite the eligible population, all sensitivity analysis followed an exploratory range of variation (+/-15%). Per definition, any nationwide screening program should consider the entire target age group as eligible population [36], therefore it was assumed as 100% in the base case. The DSA assumed two arbitrary degrees of coverage reduction (60% and 80%), to exclude women with clinical reproductive disorders, women that have already been or tried to get pregnant, or women not enrolled in family planning appointments. Additionally, a range of +/-15% was applied to the percentage of women performing the test, similarly to the adherence reported for breast and cervical cancer screening programs in Portugal (65–88%) [37]. The selected parameters and variations applied are presented in the Supplementary Materials (Supplementary Table 4).
Impact of reduced AMH on Women's family planning
An important piece of information in this model is how women react and potentially change their family planning efforts in response to obtaining a reduced AMH level. The model presents three options in response to this result – (1) attempt to have children within the next two years, (2) pursue a long-term strategy for having children (cryopreservation), or (3) pursue alternative methods of having a child, such as adoption. The distribution among these three options is dependent on age (different probabilities based on the women's age). These probabilities were estimated using the results of a survey; however, as this component potentially has a high degree of variability, to better assess the uncertainty around the estimated distribution among these three options, a separate deterministic sensitivity analysis was performed.
Among women that received an abnormal AMH result, one at a time the base case value for the probability of choosing to do each of the respective options was changed by ± 25%. As these three options must always equal 100%, the net change in each option was split among the other two (for example, if the proportion attempting in the next two years increased by 10%, then both the other options decreased by 5% each). The incremental budget impact was then observed and compared with the baseline result.
Discount rate
As a portion of the simulated costs happen years in the future, a sensitivity analysis was performed to determine the impact of the discount rate. Annual discount rates of 3.5% and 5% were tested and compared with the base case model. No additional assumptions were changed, and all other model parameters were held constant.
Results
By introducing the AMH test in the context of a nationwide screening for diminished OR, in a population of 330,181 women aged 25–30 years [21], it is expected a nine month reduction in the time until a successful pregnancy, and a 9.3 Million € reduction to the NHS budget (Table 2). These cost-savings are driven by the decision of 35.9% of women to accelerate their reproductive plans to the upcoming 2 years, after receiving a low AMH result, which avoids the need to undergo MAR in 23.7% of the cases, comparing to the current practice.
| Current practice | Proposed | Incremental | |
|---|---|---|---|
| Budget Impact (€) | 76,587,534 € | 67,211,674 € | -9,375,860 € |
| Cost per case (€) | 228 € | 200 € | -28 € |
| Aging (years) | 3.52 | 2.79 | -0.7 |
| MAR (%) | 4.32 | 3.30 | -23.7 |
| First line (%) | 2.22 | 2.16 | 28.0§ |
| No retries (%) | 13.3‡ | 14.3‡ | 7.84 |
| 1 retry (%) | 11.6‡ | 12.1‡ | 3.69 |
| 2 retries (%) | 10.4‡ | 11.5‡ | 10.6 |
| Moved to 2nd line (%) | 64.7‡ | 62.1‡ | -3.98 |
| Second line (%)† | 3.54 | 2.48 | -8.25§ |
| No retries (%) | 25.8‡ | 26.4‡ | 2.48 |
| 1 retry (%) | 18.7‡ | 20.0‡ | 6.83 |
| 2 retries (%) | 14.1‡ | 13.8‡ | -2.25 |
| Failure after 2nd line (%) | 41.4‡ | 39.8‡ | -3.87 |
| Total Failure (%) | 1.47 | 0.99 | -11.79 |
| Only 2nd line (%) | 2.11 | 1.14 | -29.41 |
†
The percentage of second-line performance includes the ones that have performed second line as first option of treatment and those who failed the first line and moved to second line afterward.
‡
Values adjusted to 100% of patients within each group undergoing first or second line. MAR: Medically assisted reproduction.
§
Change vs those that performed ART.
Among women that went through fertility treatments, the model estimated improved success rates for first-line treatments (4% reduction in pregnancy failures) and a substantial decrease in referrals for second-line treatments (∼30% reduction when indicated as first option and 8% after first-line failure). Overall, using AMH test in the proposed practice is expected to result in a 12% reduction in post-treatment pregnancy failures, therefore optimizing treatment efficacy.
Sensitivity analysis
One way sensitivity analysis
The results of the model were found to be robust (Figure 3) to expected changes in the input values, as only the eligible population size had an impact of more than 4% on the base case result. The impact of population size on the results was expected, as it represents the population covered and therefore, more patients tested and/ or treated. The proposed OR screening implementation retained a cost savings for the NHS in all simulated scenarios–ranging from 5.6 to 9.7 million €.
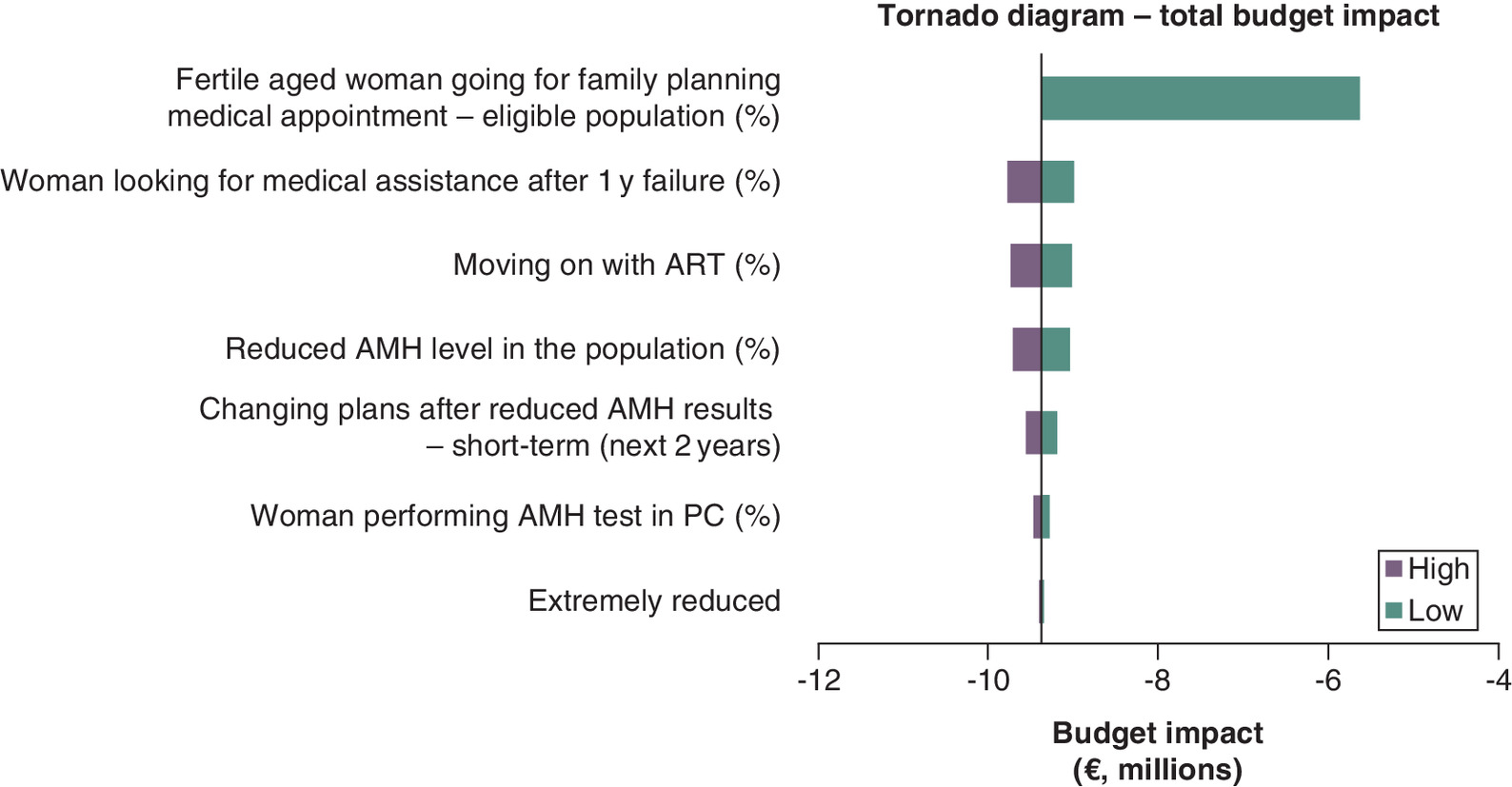
Figure 3. One-way sensitivity analysis results.
AMH: Anti-Müllerian hormone; MAR: Medically assisted reproduction; PC: Primary care.
Impact of reduced AMH on Women's family planning
The probability for each of the three options included in the model for changes to family planning after receiving a reduced AMH result was varied in a deterministic sensitivity analysis. The full results of this analysis are shown in the Supplementary Materials (Supplementary Table 5). The analysis showed relatively modest changes to the overall budget impact results when the probabilities of a women choosing each of the options was varied, ranging from a decrease of 6.85% to an increase of 6.42%. Changing the proportion that would attempt to have children in the next two years had a much larger impact that changes in the other two options – with an increase in the incremental budget impact of 6.85% when the base value was decreased 25% (Supplementary Materials & Supplementary Table 5).
Discount rate
As the base case did not include cost discounting, a separate DSA was conducted to assess the impact of discounting on the findings (Supplementary Materials & Supplementary Table 6). As expected, when a discount rate was applied, decreasing the impact of future costs avoided, the total cost-savings were reduced by approximately 8% and 12% when discount rates of 3.5% and 5% were applied, respectively.
Discussion
An economic model was developed to estimate the economic impact of implementing a nationwide OR screening with the AMH test, for women 25–30 years old. This model intends to simulate the reproductive/fertility journey of Portuguese women in the public sector, from the first medical appointment with their GP/Ob-Gyn for family planning purposes, through the conclusion of their reproductive effort (first pregnancy only). To ensure representativeness of the local clinical practice, an expert panel validated the entire model structure, patient flow, assumptions, input data and interpretations and, when needed, assumptions were adjusted and revalidated. Furthermore, the model proved to be congruent in the correlation of the predicted and observed results, considering the input data.
The simulation model estimated that the introduction of AMH testing early in the reproductive journey is expected to lead to 9.3 million € savings for the NHS. Applying the AMH test in young women starting their reproductive plans is expected to ultimately lead to a 12% reduction in post-treatment pregnancy failures, which suggests that knowing the OR status in advance is not only expected to be cost-saving, but it may also promote a better use of fertility treatments and, in-turn, leading to a potential increase in the probability of live-birth per treatment. All sensitivity analysis scenarios demonstrated cost-savings for the NHS and nearly all resulted in a variation of less than 5% in the budget impact, which corroborates the robustness of the model and parameters. Moreover, applying annual discount rates of 3.5% and 5% to costs within the model still resulted in substantial savings.
Due to the limitations of the model and available data, an extremely conservative approach was taken. First, it does not consider second or third pregnancies, as the decision for a second child may change after having a first, and it also would likely depend on the women's age at the first child and time-interval until the second. Moreover, success rates for both natural and MAR second pregnancies are uncertain, and AMH result's impact on women's decision to attempt a subsequent pregnancy would likely differ after achieving the first one, as well as the MAR of choice.
Secondly, although national estimates suggest that 48.2% of women had their first child within the ages of 30–39 years [1], there is no data confirming when they started trying and number of previous attempts before achieving a successful pregnancy. Ideally, the target population of an OR screening are those women that have never tried before, as this represents the greatest potential impact. The observed improvement could also be explored in a broader population, for women aged 31–35 years, but due to the lack of specific data for this age group and the countless uncertainties related to women's preferences and medical history, a conservative approach was taken not to further extrapolate this analysis.
Alternative options such as oocyte cryopreservation were not covered in this analysis either, since the NHS, except for special situations (e.g., cancer patients; women with endometriosis; others), does not cover the costs. Additionally, there would be a great deal of uncertainty in trying to estimate the number of births resulting from this procedure, due to some particularities related to the practice, as well as the costs, destination, and timing for using the frozen oocytes.
The results were tested in terms of statistical significance, and the only non-significant difference was the success rates for second-line MAR. This was expected since it was assumed that low AMH doesn't have any effect on the success rates of MAR treatments, and because the success rate in second-line treatments doesn't vary greatly between 25–35 years (25.8%–26.8%, respectively). Furthermore, there is a delay of 1.5 years between the first cycle and third cycle, meaning that time-gains with second-line techniques would not be as significant for this age group.
Finally, we recognize that the proposed practice would affect the reproductive process for individual women. Infertility by itself has a strong Impact on patients, sometimes leading to distress and depression, as well as discrimination and ostracism [38], which could significantly impact women's decisions over time.
Conclusion
This economic analysis supports the hypothesis that the implementation of a nationwide screening program in Portugal for diminished ovarian reserve in young women, through an AMH test, not only could provide women with valuable information needed to make more informed decisions about their reproductive plans, but also help shorten the extensive journey that is the infertility process. While doing so, it can also lead to more efficient use of fertility treatments and an increase in live births per treatment, substantially reducing costs to the NHS.
•
By testing the levels of a biomarker known as anti-Müllerian hormone (AMH) in women, physicians can provide vital information regarding potential fertility issues, namely a diminished ovarian reserve (OR), which allows women to make more informed family planning decisions.
•
A budget impact model was developed to estimate the potential cost savings of implementing a nationwide screening for diminished ovarian reserve (OR), using the AMH test, for women ages 25–30 years old in Portugal.
•
Two scenarios were compared using a patient-level Markov microsimulation model – (1) the current practice, where no screening is performed, and (2) a proposed scenario, where AMH test is offered at a family planning appointment with a GP or an Ob-Gyn.
•
The model simulated the reproductive/fertility journey of Portuguese women in the public sector, from the first medical appointment with their GP/Ob-Gyn for family planning purposes, through the conclusion of their reproductive effort (first pregnancy only), capturing the affect that reduced or severely reduced AMH levels would have on the timeline and medically assisted reproduction (MAR) treatment selection.
•
Two primary data sources used in this analysis: (1) a nationwide survey of Portuguese women to assess their willingness to perform an AMH test and the impact an abnormal result would have on their family planning, and (2) an expert panel of local clinicians that validated the entire model structure, patient flow, assumptions, input data and interpretations to ensure they reflect local practice.
•
The simulation model estimated that the introduction of AMH testing early in the reproductive journey is expected to lead to 9.3 million € savings for the National Health System in Portugal, driven by a 24% reduction in MAR use, while also leading to a shift toward more first-line versus second-line MAR treatments, when they were needed.
•
Applying the AMH test in young women starting their reproductive plans is expected to ultimately lead to a 12% reduction in post-treatment pregnancy failures, which suggests that implementing screening for diminished OR promote more efficient use of MAR treatments, indirectly leading to a potential increase in the live-births per treatment used.
•
In conclusion, AMH screening can potentially allow women to make more informed decisions in their family planning and could lead to a shorter overall fertility journey, more efficient use of MAR treatments, and, ultimately, provide a substantial cost-savings for the National Health System in Portugal.
Author contributions
P Xavier, S Dantas, T Almeida-Santos, SR Soares and H Gens provided insights, data validation, and manuscript revision and approval; V Genovez, RJ Imhoff and C Modesto performed data collection, analysis and interpretation, and manuscript writing; I Correia performed data collection, analysis and interpretation, manuscript revision and approval; and CS manuscript revision and approval.
Financial & competing interests disclosure
H Gens, C Catalão and I Correia are employees of Roche Sistemas de Diagnósticos Portugal, sponsor of the study. RJ Imhoff is, and V Genovez and C Modesto previously were, employees of CTI Clinical Trial and Consulting, a consultant to Roche Sistemas de Diagnósticos Portugal, the sponsor of the study. P Xavier, S Dantas, T Almeida-Santos and SR Soares were consultants to Roche Sistemas de Diagnósticos Portugal, the sponsor of the study. This work was supported by Roche Sistemas de Diagnósticos Lda. (Portugal), who participated in the collection, analysis and interpretation of data, revision and approval of the manuscript. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The study was conducted in accordance with applicable regulations, including relevant European Union directives and regulations, and the principles of the Declaration of Helsinki. The model did not use any patient data from any institution and was based only on published data, expert's opinion, and (anonymous) aggregate summary results of a previously conducted, voluntary electronic survey performed for marketing purposes. According to local Portuguese Law No. 21/2014 of 16 April, the survey, whose results were used in this analysis, did not meet the criteria for a clinical study, and thus, no ethics committee vote was required.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Pordata. Idade média da mãe ao nascimento do primeiro filho. INE - Indicadores Demográficos, Fontes de Dados. www.pordata.pt/portugal/idade+media+da+mae+ao+nascimento+do+primeiro+filho-805 (2020).
2.
Birth rate by country - Thematic Map - Europe. https://www.indexmundi.com/map/?v=25&r=eu&l=en (2020).
3.
Pordata. Saldos populacionais anuais: total, natural e migratório. INE - Estatísticas de Nados-Vivos; INE - Estimativas Anuais da População Residente; INE - Estatísticas de Óbitos, Fontes de Dados. www.pordata.pt/portugal/saldos+populacionais+anuais+saldo+total++saldo+natural+e+saldo+migratorio-657 (2020).
4.
Conselho Nacional De Procriação Medicamente Assistida (CNPMA). Relatório - Atividade Desenvolvida pelos Centros de PMA em 2017. www.cnpma.org.pt/cnpma/Paginas/Relatorios-da-Atividade-em-pma.aspx (2021).
• Report developed from The National Council for Medically Assisted Procreation (CNPMA) detailing various trends and practice results in Portugal. This was used to both develop the model structure and clinical care pathway, as well as populate data elements.
5.
ESHRE. Factsheet on ART. www.eshre.eu/Europe/Factsheets-and-infographics (2020).
6.
ASRM. Quick Facts About Infertility. www.reproductivefacts.org/faqs/quick-facts-about-infertility/ (2020).
7.
Direção-Geral da Saúde (DGS) Norma nº 003/2011 de 19/01/2011 - Conduta em Infertilidade. www.dgs.pt/directrizes-da-dgs/normas-e-circulares-normativas/norma-n-0032011-de-19012011.aspx (2020).
8.
NICE - National Institute for Health and Care Excellence. Guidance - Fertility problems: assessment and treatment. www.nice.org.uk/guidance/cg156 (2020).
9.
Associação Portuguesa de Fertilidade (APF). Conceber: guia para profissionais e pessoas com problemas de fertilidade. www.apf.pt/sites/default/files/media/2015/conceber_guia_infertilidade.pdf (2020).
10.
World Health Organization (WHO) - IRIS. Family planning: a global handbook for providers. update: evidence-based guidance developed through worldwide collaboration. https://apps.who.int/iris/handle/10665/44028 (2011).
11.
Associação Portuguesa de Fertilidade (APF). Infertilidade. https://apfertilidade.org/infertilidade/ (2020).
12.
Carlsson IB, Scott JE, Visser JA, Ritvos O, Themmen APN, Hovatta O. Anti-Müllerian hormone inhibits initiation of growth of human primordial ovarian follicles in vitro. Hum. Reprod. 21(9), 2223–2227 (2006).
13.
Dewailly D, Andersen CY, Balen A et al. The physiology and clinical utility of anti-Mullerian hormone in women. Hum. Reprod. Update 20(3), 370–385 (2014).
14.
La Marca A, Broekmans FJ, Volpe A, Fauser BC, Macklon NS, Reprodu ESIG. Anti-Mullerian hormone (AMH): what do we still need to know? Hum. Reprod. 24(9), 2264–2275 (2009).
15.
Committee ACOOaGCOGPaP. Female age-related fertility decline. Committee Opinion No. 589. Fertil. Steril. 101(3), 633–634 (2014).
16.
Hansen KR, Knowlton NS, Thyer AC, Charleston JS, Soules MR, Klein NA. A new model of reproductive aging: the decline in ovarian non-growing follicle number from birth to menopause. Hum. Reprod. 23(3), 699–708 (2008).
17.
Heffner LJ. Advanced maternal age–how old is too old? N. Engl. J. Med. 351(19), 1927–1929 (2004).
18.
Mills M, Rindfuss RR, Mcdonald P, Te Velde E. Force ERaST. Why do people postpone parenthood? Reasons and social policy incentives. Hum. Reprod. Update 17(6), 848–860 (2011).
19.
Modi D, Bhartiya D, Puri C. Developmental expression and cellular distribution of Mullerian inhibiting substance in the primate ovary. Reproduction 132(3), 443–453 (2006).
20.
Igarashi H, Takahashi T, Nagase S. Oocyte aging underlies female reproductive aging: biological mechanisms and therapeutic strategies. Reprod. Med. Biol. 14(4), 159–169 (2015).
21.
Instituto Nacional de Estatística (INE). Estimativas anuais da população residente. https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&indOcorrCod=0008273&xlang=pt (2019).
22.
Roche Diagnostics Portugal. Internal data, unpublished results. (2020).
• The unpublished results, housed internally at Roche Diagnostics Portugal, of a survey that had been previously conducted on 300 women, aged 25–30 years, randomly selected from an online access panel. This data was used to model the decision-making process of a woman's willingness to undergo the AMH test, along with the potential impact that the results could have on fertility choices and family planning.
23.
Administração Central Do Sistema De Saúde (ACSS). Circular Normativa nº15/2019. www.acss.min-saude.pt/2016/11/24/circulares-normativas/ (2020).
24.
Diário Da República Eletrónico (DRE). Lei n.º 17/2016, de 20 de Junho - Procriação medicamente assistida. https://dre.pt/dre/analise-juridica/lei/17-2016-74738646 (2020).
• National Portuguese legislation/fee schedule used to estimate the line item costs for the various healthcare resources used in the model.
25.
Healthnews. Portugal sem resposta eficaz para casos de infertilidade. https://healthnews.pt/2020/05/19/portugal-sem-resposta-eficaz-para-casos-de-infertilidade/ (2021).
26.
HealthNews. Associação Portuguesa de Fertilidade quer 45 anos como limite para fertilização in vitro. https://healthnews.pt/2020/07/23/associacao-quer-45-anos-como-limite-para-fertilizacao-in-vitro/ (2021).
27.
Diário de Notícias. Centros públicos com dois anos de atraso nos tratamentos de fertilidade. www.dn.pt/sociedade/centros-publicos-com-dois-anos-de-atraso-nos-tratamentos-de-fertilidade-13333723.html (2021).
28.
Rasool S, Shah D. Fertility with early reduction of ovarian reserve: the last straw that breaks the Camel's back. Fertil. Res. Pract. 3(1), 15 (2017).
29.
Reichman DE, Goldschlag D, Rosenwaks Z. Value of antimüllerian hormone as a prognostic indicator of in vitro fertilization outcome. Fertil. Steril. 101(4), 1012–1018.e1011 (2014).
30.
Kedem A, Haas J, Geva LL et al. Ongoing pregnancy rates in women with low and extremely low AMH levels. A multivariate analysis of 769 cycles. PloS One 8(12), e81629 (2013).
31.
La Marca A, Sighinolfi G, Radi D et al. Anti-Mullerian hormone (AMH) as a predictive marker in assisted reproductive technology (ART). Hum. Reprod. Update 16(2), 113–130 (2010).
32.
Lin P-Y, Huang F-J, Kung F-T et al. Evaluation of serum anti-mullerian hormone as a biomarker of early ovarian aging in young women undergoing IVF/ICSI cycle. Int. J. Clin. Exp. Pathol. 7(9), 6245–6253 (2014).
33.
Lukaszuk K, Kunicki M, Liss J, Bednarowska A, Jakiel G. Probability of live birth in women with extremely low anti-Müllerian hormone concentrations. Reprod. Biomed. Online 28(1), 64–69 (2014).
34.
Sefrioui O, Madkour A, Aboulmaouahib S, Kaarouch I, Louanjli N. Women with extreme low AMH values could have in vitro fertilization success. Gynecol. Endocrinol. 35(2), 170–173 (2019).
35.
Weghofer A, Dietrich W, Barad DH, Gleicher N. Live birth chances in women with extremely low-serum anti-Mullerian hormone levels. Hum. Reprod. 26(7), 1905–1909 (2011).
36.
Direção-Geral da Saúde(DGS). Programa Nacional para as Doenças Oncológicas - Relatório. https://comum.rcaap.pt/bitstream/10400.26/15554/1/d190354.pdf (2015).
37.
Serviço Nacional de Saúde (SNS). Relatório Anual - Acesso a Cuidados de Saúde nos Estabelecimentos do SNS e Entidades Convencionadas. www.sns.gov.pt/wp-content/uploads/2020/09/Relatorio_Anual_Acesso_2019.pdf ( 2021).
38.
Mascarenhas MN, Flaxman SR, Boerma T, Vanderpoel S, Stevens GA. National, regional, and global trends in infertility prevalence since 1990: a systematic analysis of 277 health surveys. PLOS Med. 9(12), e1001356 (2012).
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 January 2023
Accepted: 29 May 2023
Published online: 22 June 2023
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Screening for diminished ovarian reserve in Portugal: a cost-saving answer to shorten the fertility journey. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0003
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Artur Bjelica, Jelena Curcic, Dragan Stajic, Marko Ilincic, Reproductive health screening for endometriosis, reduced ovarian reserve, polycystic ovary syndrome and the most common sexually transmitted diseases, Medicinski pregledMedical review, 10.2298/MPNS2406171B, 77, 5-6, (171-176), (2024).