Non-embolic outcomes in patients with cardiovascular disease and atrial fibrillation treated with rivaroxaban
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: It is not well known how comorbidities may change the prognosis of atrial fibrillation (AF) patients. This study was aimed to analyze the impact of cardiovascular disease on this population. Materials & methods: EMIR was a multicenter, prospective study, including 1433 AF patients taking rivaroxaban for ≥6 months. Data were analyzed according to the presence of vascular disease. Results: Coronary artery disease was detected in 16.4%, peripheral artery disease/aortic plaque in 6.7%, vascular disease in 28.3%. Patients with coronary artery disease had higher rates (per 100 patient-years) of major adverse cardiovascular events (2.98 vs 0.71; p < 0.001) and cardiovascular death (1.79 vs 0.41; p = 0.004). Those with vascular disease had higher rates of thromboembolic events (1.47 vs 0.44; p = 0.007), major adverse cardiovascular events (2.03 vs 0.70; p = 0.004), and cardiovascular death (1.24 vs 0.39; p = 0.025). Patients with peripheral artery disease/aortic plaque had similar rates. Conclusion: AF patients with vascular disease have a higher risk of non-embolic outcomes.
Stroke is the most devastating complication associated with atrial fibrillation (AF) [1]. Anticoagulation markedly reduces the risk of thromboembolic outcomes in AF patients [2]; however, relevant residual cardiovascular risk (mainly coronary artery disease [CAD], heart failure and cardiovascular death) persists despite antithrombotic therapy [3,4]. Atherosclerotic cardiovascular disease and AF are common conditions that frequently co-occur. Of note, the presence of one entity may precipitate/exacerbate the development of the other and vice versa. In fact, both conditions share risk factors and comorbidities. In addition, the hypercoagulability, systemic inflammation, oxidative stress, platelet activation and endothelial dysfunction that commonly occur in these patients promote both thromboembolism and atherothrombosis, leading to an increased risk of ischemic stroke and myocardial infarction [3–7]. In this context, the most recent European guidelines recommend a comprehensive approach in the management of patients with AF, with the aim of reducing not only the risk of stroke, but also that of vascular disease [7].
Rivaroxaban is a once-daily direct anticoagulant that safely and effectively reduces the risk of stroke [8,9]. However, it is important to determine whether the results of clinical trials are applicable under real-world conditions [10,11]. The EMIR study (Estudio observacional para la identificación de los factores de riesgo asociados a eventos cardiovasculares mayores en pacientes con fibrilación auricular no valvular tratados con un anticoagulante oral directo [Rivaroxaban] [‘Observational study to identify risk factors associated with major cardiovascular events in patients with nonvalvular atrial fibrillation treated with a direct oral anticoagulant [rivaroxaban]’) evaluated risk 2 major adverse cardiovascular events (MACE) score in AF patients treated with rivaroxaban, showing the frequency of MACE is lower among high-risk patients prescribed with rivaroxaban in clinical practice [12,13].
This study analyzed the impact of atherosclerotic vascular disease, defined as the presence of previous CAD or peripheral artery disease/aortic plaque, on clinical profile and outcomes in AF patients anticoagulated with rivaroxaban in the EMIR population.
Materials & methods
The design and methods of the EMIR study have been described elsewhere [12,13]. Briefly, EMIR was a prospective and observational study that included adult patients with a diagnosis of AF treated with rivaroxaban for at least 6 months before enrollment. All patients had to give their written informed consent before being included in the study and were followed up for 2.5 years according to routine clinical practice. The exclusion criteria were prosthetic heart valves, severe valvopathy, chronic infections, systemic autoimmune diseases, active cancer, severe liver or renal insufficiency and severe cognitive impairment. The study was approved by the local ethics committees. For the purpose of this study, we performed a retrospective analysis of the EMIR database, although all the end points were prospectively collected.
Baseline data, including biodemographic parameters, scales (CHA2DS2-VASc, HAS-BLED, 2MACE), cardiovascular risk factors and history of vascular disease were collected from the patients’ clinical history and via interview and recorded on a specific electronic case report form. Data were analyzed in the overall study population and according to the presence of vascular disease, which was defined as the presence of baseline CAD, cerebrovascular disease or peripheral artery disease. The presence of coronary heart disease, vascular disease and aortic plaque were recorded from the electronic clinical history of patients, according to physicians’ criteria. Chronic kidney disease was defined as an estimated glomerular filtration rate <60 ml/min/1.73 m2 according to the MDRD-4 formula [14].
Outcomes (MACE, thromboembolic events, major bleeding, myocardial infarction, revascularization, cardiovascular death and all-cause mortality) during the study were evaluated by an independent scientific committee. MACE included a combination of non-fatal myocardial infarction, revascularization and cardiovascular death (ischemic heart disease, progressive heart failure and sudden cardiac death). Thromboembolic events included a combination of stroke, systemic embolism and/or transient ischemic attack, together with myocardial infarction. Major bleeding was defined according to definition of the International Society of Thrombosis and Hemostasis [15]. Events were analyzed in the overall study population and according to the presence of previous CAD, peripheral artery disease/aortic plaque and vascular disease. In addition, predictors of MACE, thromboembolic events and major bleeding in patients with previous CAD or vascular disease were determined.
Statistical methods
Qualitative variables were expressed as absolute and relative frequencies. Quantitative variables were reported with measures of central tendency (mean) and dispersion (standard deviation). Qualitative variables were compared using the chi-square test or the Fisher exact test, as required. The t-test was used to compare two means. Incident rates were calculated for each event in the overall study population and according to the presence of previous CAD, peripheral artery disease/aortic plaque and vascular disease. Multivariate logistic regression analyses were performed to assess predictors of MACE, thromboembolic events and major bleeding (dependent variables). The independent variables were age (continuous variable), sex (female vs male), BMI (continuous variable), type of AF (permanent vs paroxysmal), CAD, coronary revascularization, concomitant use of antiplatelet agents, heart failure, previous cerebrovascular disease, peripheral artery disease, dependence level (dependent vs autonomous), diabetes, hypertension, hyperlipidemia, smoking, chronic kidney disease, previous bleeding, liver failure, pulmonary disease, cancer, alcohol use, non-severe dementia, CHA2DS2-VASc (discrete quantitative), HAS-BLED (discrete quantitative) and 2MACE ≥3. The multivariate models were constructed by including those factors with p < 0.150 in the bivariate analysis using automatic forward stepwise selection. Only the significant factors were finally included in the model. Statistical significance was set at <0.05 for all tests. The data were analyzed using the statistical package SPSS (v18.0 or higher).
Results
The initial study population comprised 1503 patients from 83 Spanish centers (hospitals and private clinics). After the exclusion of 70 patients, 1433 (93.7%) patients from 79 Spanish centers, were included in the final analysis. At baseline, 235 (16.4%) had CAD, 96 (6.7%) peripheral artery disease/aortic plaque and 406 (28.3%) vascular disease (Figure 1).
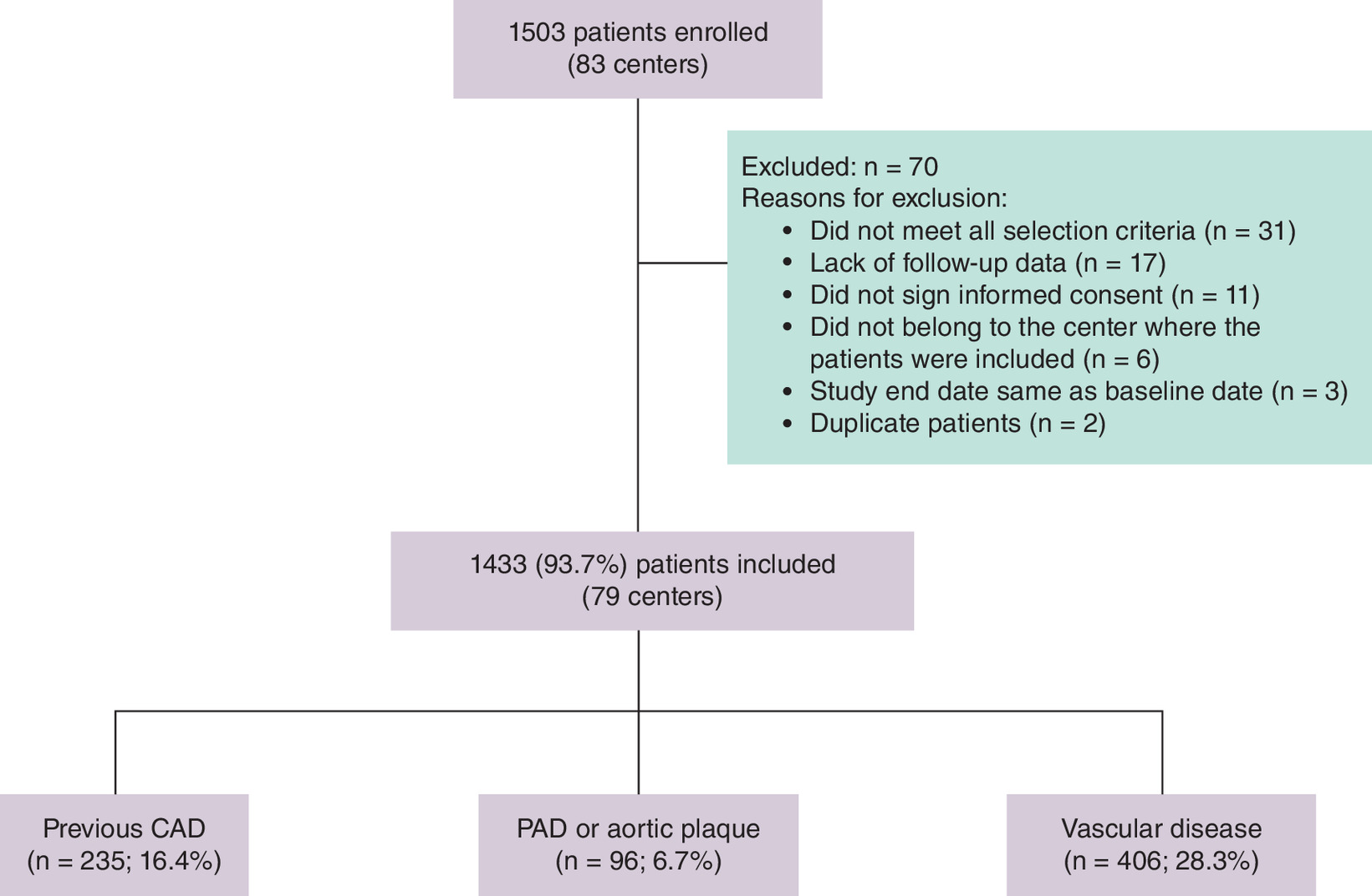
Figure 1. Flow chart of the study population.
Vascular disease: previous CAD and/or previous cerebrovascular disease and/or PAD.
CAD: Coronary artery disease; PAD: Peripheral artery disease.
Table 1 presents the baseline clinical characteristics overall and according to the presence of previous CAD, peripheral artery disease/aortic plaque and vascular disease. Mean age was 74.2 ± 9.7 years, 55.5% of patients were male, 37.5% had permanent AF, mean CHA2DS2-VASc was 3.5 ± 1.5, mean HAS-BLED was 1.6 ± 1.0, and 26.9% had a 2MACE score ≥3. Compared with patients without CAD, those with ischemic heart disease were more commonly men, had higher CHA2DS2-VASc and HAS-BLED scores, and more frequently had diabetes, heart failure and peripheral artery disease. In addition, a greater proportion of patients presented with 2MACE ≥3. Compared with patients without peripheral artery disease/aortic plaque, those with peripheral artery disease/aortic plaque were older, had higher CHA2DS2-VASc and HAS-BLED scores and more frequently had hypertension, diabetes, heart failure and chronic kidney disease. In addition, a greater proportion of patients had 2MACE ≥3. Compared with patients without vascular disease, those with vascular disease were older and more commonly men and had more permanent AF, higher CHA2DS2-VASc and HAS-BLED scores, as well as more frequent diabetes and heart failure. In addition, more patients had 2MACE ≥3.
| Total population (n = 1433; 100%) | No previous CAD (n = 1198; 83.6%) | Previous CAD (n = 235; 16.4%) | p-value | No PAD/aortic plaque (n = 1337; 93.3%) | PAD/aortic plaque (n = 96; 6.7%) | p-value | No vascular disease (n = 1027; 71.7%) | Vascular disease† (n = 406; 28.3%) | p-value | |
|---|---|---|---|---|---|---|---|---|---|---|
| Biodemographic data | ||||||||||
| Age, years | 74.2 ± 9.7 | 74.0 ± 9.7 | 74.8 ± 9.6 | 0.215 | 74.0 ± 9.7 | 77.1 ± 8.3 | 0.002 | 73.6 ± 9.7 | 75.6 ± 9.6 | <0.001 |
| Sex (male), n (%) | 795 (55.5) | 613 (51.2) | 182 (77.4) | <0.001 | 733 (54.8) | 62 (64.6) | 0.063 | 523 (50.9) | 272 (67.0) | <0.001 |
| Permanent AF, n (%) | 535 (37.5) | 437 (36.5) | 98 (41.7) | 0.130 | 492 (36.8) | 43 (44.8) | 0.118 | 367 (35.7) | 168 (41.4) | 0.047 |
| BMI, kg/m2 | 29.1 ± 4.9 | 29.2 ± 4.9 | 28.8 ± 4.8 | 0.214 | 29.1 ± 5.0 | 29.4 ± 4.1 | 0.200 | 29.2 ± 5.0 | 28.8 ± 4.6 | 0.175 |
| Risk stratification | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CHA2DS2-VASc score | 3.5 ± 1.5 | 3.4 ± 1.5 | 4.1 ± 1.6 | <0.001 | 3.4 ± 1.5 | 4.9 ± 1.4 | <0.001 | 3.1 ± 1.3 | 4.6 ± 1.6 | <0.001 |
| 2MACE score ≥3, n (%) | 385 (26.9) | 223 (18.6) | 162 (68.9) | <0.001 | 337 (25.2) | 48 (50.0) | <0.001 | 110 (10.7) | 275 (67.7) | <0.001 |
| HAS-BLED score | 1.6 ± 1.0 | 1.5 ± 1.0 | 1.8 ± 1.0 | <0.001 | 1.5 ± 1.0 | 2.0 ± 1.0 | <0.001 | 1.3 ± 0.9 | 2.1 ± 1.1 | <0.001 |
| Cardiovascular risk factors | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Hypertension, n (%) | 1137 (79.3) | 948 (79.1) | 189 (80.4) | 0.654 | 1,051 (78.6) | 86 (89.6) | 0.010 | 803 (78.2) | 334 (82.3) | 0.086 |
| Diabetes, n (%) | 388 (27.1) | 296 (24.7) | 92 (39.1) | <0.001 | 350 (26.2) | 38 (39.6) | 0.004 | 242 (23.6) | 146 (36.0) | <0.001 |
| Vascular disease | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Previous coronary disease, n (%) | 235 (16.4) | 0 | 235 (100) | <0.001 | 0 | 235 (57.9) | <0.001 | |||
| Heart failure, n (%) | 326 (22.7) | 234 (19.5) | 92 (39.1) | <0.001 | 293 (21.9) | 33 (34.4) | 0.005 | 199 (19.4) | 127 (31.3) | <0.001 |
| Previous cerebrovascular disease, n (%) | 179 (12.5) | 143 (11.9) | 36 (15.3) | 0.152 | 162 (12.1) | 17 (17.7) | 0.109 | 0 | 179 (44.1) | <0.001 |
| Peripheral artery disease, n (%) | 58 (4.0) | 38 (3.2) | 20 (8.5) | <0.001 | 0 | 58 (14.3) | <0.001 | |||
| Chronic kidney disease, n (%) | 350 (24.4) | 286 (23.9) | 64 (27.6) | 0.262 | 313 (23.4) | 37 (38.9) | 0.001 | 242 (23.6) | 108 (26.8) | 0.244 |
†
Vascular disease was defined as the presence of previous CAD and/or previous cerebrovascular disease and/or PAD.
AF: Atrial fibrillation; CAD: Coronary artery disease; MACE: Major cardiovascular event; PAD: Peripheral artery disease.
The mean follow-up was 2.2 ± 0.6 years (median: 2.5 years; interquartile range: 2.2–2.6 years). The incident rates of relevant events were calculated based on 1425 patients (Table 2). Overall, annual percentages of stroke + systemic embolism + transient ischemic attack, MACE, cardiovascular death, death from any cause and major bleeding were 0.72, 1.07, 0.63, 2.73 and 1.04%, respectively. Compared with patients with no previous CAD at baseline, those with ischemic heart disease had a greater annual frequency of MACE, coronary revascularization, cardiovascular death and death from any cause, with a trend toward more thromboembolic outcomes and major bleeding. Compared with patients without previous vascular disease at baseline, those with vascular disease had higher incidence rates of stroke + systemic embolism + transient ischemic attack, MACE, coronary revascularization, cardiovascular death, death from any cause and major bleeding. By contrast, no significant differences were found regarding outcomes according to the presence of peripheral artery disease/aortic plaque.
| Total (n = 1.425) | No previous CAD (n = 1.190) | Previous CAD (n = 235) | p-value | No PAD/aortic plaque (n = 1.329) | PAD/aortic plaque (n = 96) | p-value | No vascular disease (n = 1.019) | Vascular disease† (n = 406) | p-value | |
|---|---|---|---|---|---|---|---|---|---|---|
| Thromboembolic events§ Patients, n (%) Incident rate events (%)‡ | 21 (1.5) 0.66 | 14 (1.2) 0.52 | 7 (3.0) 1.39 | 0.036 0.075 | 20 (1.5) 0.67 | 1 (1.0) 0.47 | 0.716 0.999 | 11 (1.1) 0.48 | 10 (2.5) 1.13 | 0.050 0.085 |
| Stroke + SE + TIA Patients, n (%) Incident rate events (%)‡ | 23 (1.6) 0.72 | 16 (1.3) 0.60 | 7 (3.0) 1.39 | 0.084 0.119 | 22 (1.6) 0.74 | 1 (1.0) 0.47 | 0.999 0.999 | 10 (1.0) 0.44 | 13 (3.2) 1.47 | 0.002 0.007 |
| Major bleeding Patients, n (%) Incident rate events (%)‡ | 29 (2.0) 1.04 | 22 (1.8) 0.86 | 7 (3.0) 1.99 | 0.306 0.055 | 29 (2.2) 1.11 | 0 0 | 0.255 0.204 | 14 (1.4) 0.65 | 15 (3.7) 2.03 | 0.005 0.002 |
| MACE Patients, n (%) Incident rate events (%)‡ | 30 (2.1) 1.07 | 16 (1.3) 0.71 | 14 (6.0) 2.98 | <0.001 <0.001 | 26 (1.9) 0.98 | 4 (4.2) 2.35 | 0.136 0.148 | 14 (1.4) 0.70 | 16 (3.9) 2.03 | 0.002 0.004 |
| Myocardial infarction Patients, n (%) Incident rate events (%)‡ | 5 (0.3) 0.16 | 4 (0.3) 0.15 | 1 (0.4) 0.20 | 0.592 0.999 | 5 (0.4) 0.17 | 0 0 | 0.999 0.999 | 4 (0.4) 0.17 | 1 (0.2) 0.11 | 0.999 0.999 |
| Revascularization Patients, n (%) Incident rate events (%)‡ | 9 (0.6) 0.28 | 4 (0.3) 0.15 | 5 (2.1) 0.99 | 0.008 0.014 | 7 (0.5) 0.24 | 2 (2.1) 0.94 | 0.118 0.235 | 3 (0.3) 0.13 | 6 (1.5) 0.68 | 0.019 0.035 |
| Cardiovascular death Patients, n (%) Incident rate events (%)‡ | 20 (1.4) 0.63 | 11 (0.9) 0.41 | 9 (3.8) 1.79 | 0.002 0.004 | 17 (1.3) 0.57 | 3 (3.1) 1.41 | 0.145 0.292 | 9 (0.9) 0.39 | 11 (2.7) 1.24 | 0.010 0.025 |
| Death from any cause Patients, n (%) Incident rate events (%)‡ | 87 (6.1) 2.73 | 59 (5.0) 2.20 | 28 (11.9) 5.56 | <0.001 <0.001 | 79 (5.9) 2.66 | 8 (8.3) 3.75 | 0.345 0.453 | 42 (4.1) 1.83 | 45 (11.1) 5.08 | <0.001 <0.001 |
†
Vascular disease was defined as the presence of previous CAD and/or previous cerebrovascular disease and/or PAD.
‡
Events/100 patients/year.
§
Ischemic stroke and/or systemic embolism and/or transient ischemic attack and/or myocardial infarction; MACE: Non-fatal myocardial infarction and/or revascularization and/or cardiovascular death.
AF: Atrial fibrillation; CAD: Coronary artery disease; PAD: Peripheral artery disease; SE: Systemic embolism; TIA: Transient ischemic attack.
Multivariate logistic regression analyses were performed to determine the potential predictors of MACE events, thromboembolic events and major bleeding (Table 3). The concomitant use of antiplatelet agents and older age were independent predictive factors associated with MACE in patients with previous CAD, whereas antiplatelet agents and heart failure were independent predictive factors associated with MACE in patients with vascular disease. On the other hand, permanent AF and previous stroke were independently associated with the development of thromboembolic events in patients with previous CAD, and permanent AF was associated with the development of thromboembolic events in patients with vascular disease. Finally, chronic kidney disease was an independent predictor for major bleeding in patients with previous CAD and vascular disease.
| 3.1. Previous coronary artery disease. | ||||||
|---|---|---|---|---|---|---|
| Independent variables | Univariate analysis | Multivariate analysis | ||||
| p-value | OR | 95% CI | p-value | OR | 95% CI | |
| Dependent variable ‘MACE events’ | ||||||
| Antiplatelet agents | 0.003 | 5.71 | 1.83–17.77 | 0.001 | 7.07 | 2.16–23.11 |
| Hyperlipidemia | 0.112 | 5.30 | 0.68–41.36 | |||
| Cancer | 0.130 | 3.52 | 0.69–17.87 | |||
| Chronic kidney disease | 0.045 | 3.11 | 1.02–9.42 | |||
| HAS-BLED (discrete quantitative) | 0.098 | 1.54 | 0.92–2.57 | |||
| Age (continuous variable) | 0.072 | 1.06 | 1.00–1.13 | 0.032 | 1.08 | 1.01–1.17 |
| Dependent variable ‘thromboembolic events’ | ||||||
| Type of AF (permanent vs paroxysmal) | 0.045 | 8.87 | 1.05–74.90 | 0.038 | 9.85 | 1.14–84.95 |
| Previous stroke | 0.047 | 4.77 | 1.02–22.32 | 0.035 | 5.56 | 1.13–27.43 |
| Diabetes | 0.099 | 4.05 | 0.77–21.34 | |||
| HAS-BLED (discrete quantitative) | 0.063 | 1.97 | 0.97–4.02 | |||
| CHA2DS2-VASc (discrete quantitative) | 0.082 | 1.50 | 0.95–2.36 | |||
| BMI (continuous variable) | 0.114 | 0.84 | 0.68–1.04 | |||
| Arterial hypertension | 0.134 | 0.31 | 0.07–1.44 | |||
| Dependent variable ‘Major bleeding’ | ||||||
| Chronic kidney disease | 0.006 | 10.46 | 1.96–55.67 | 0.006 | 10.46 | 1.96–55.67 |
| Cancer | 0.016 | 8.72 | 1.50–50.59 | |||
| Patient autonomy (dependent vs autonomous) | 0.047 | 4.78 | 1.02–22.40 | |||
| HAS-BLED (discrete quantitative) | 0.005 | 3.01 | 1.39–6.52 | |||
| CHA2DS2-VASC (discrete quantitative) | 0.130 | 1.42 | 0.90–2.23 | |||
| Age (continuous variable) | 0.027 | 1.13 | 1.014–1.26 | |||
| 3.2. Vascular disease†. | ||||||
|---|---|---|---|---|---|---|
| Independent variables | Univariate analysis | Multivariate analysis | ||||
| p-value | OR | 95% CI | p-value | OR | 95% CI | |
| Dependent variable ‘MACE events’ | ||||||
| Antiplatelet agents | <0.001 | 8.23 | 2.84–24.10 | <0.001 | 7.98 | 2.71–23.51 |
| Ischemic heart disease | 0.037 | 4.95 | 1.10–22.22 | |||
| Coronary revascularization | 0.025 | 3.77 | 1.18–12.04 | |||
| Heart failure | 0.021 | 3.47 | 1.21–9.97 | 0.032 | 3.28 | 1.11–9.70 |
| Hyperlipidemia | 0.141 | 3.09 | 0.69–13.90 | |||
| Chronic kidney disease | 0.084 | 2.55 | 0.88–7.38 | |||
| Sex (female vs male) | 0.058 | 0.14 | 0.02–1.07 | |||
| Previous stroke | 0.023 | 0.09 | 0.01–0.72 | |||
| Dependent variable ‘thromboembolic events’ | ||||||
| Type of AF (permanent vs paroxysmal) | 0.026 | 5.90 | 1.24–28.15 | 0.026 | 5.90 | 1.24–28.15 |
| Heart failure | 0.061 | 3.41 | 0.95–12.30 | |||
| Diabetes | 0.123 | 2.74 | 0.76–9.88 | |||
| HAS-BLED (discrete quantitative) | 0.145 | 1.52 | 0.87–2.66 | |||
| CHA2DS2-VASc (discrete quantitative) | 0.052 | 1.50 | 0.99–2.25 | |||
| Age (continuous variable) | 0.072 | 1.08 | 0.99–1.17 | |||
| BMI (continuous variable) | 0.095 | 0.87 | 0.73–1.03 | |||
| Dependent variable ‘Major bleeding’ | ||||||
| 2MACE ≥3 | 0.062 | 6.97 | 0.91–53.61 | |||
| Chronic kidney disease | 0.001 | 6.02 | 2.08–17.42 | 0.001 | 6.02 | 2.08–17.42 |
| Previous bleeding | 0.146 | 3.19 | 0.67–15.20 | |||
| Patient autonomy (dependent vs autonomous) | 0.064 | 2.91 | 0.94–8.97 | |||
| CHA2DS2-VASC (discrete quantitative) | 0.108 | 1.31 | 0.94–1.81 | |||
| Age (continuous variable) | 0.016 | 1.09 | 1.02–1.17 | |||
| HAS-BLED (discrete quantitative) | 0.001 | 2.13 | 1.34–3.40 | |||
| Heart failure | 0.146 | 0.33 | 0.07–1.47 | |||
†
Vascular disease was defined as the presence of either previous CAD and/or previous cerebrovascular disease and/or PAD.
Vascular disease: previous coronary artery disease and/or previous cerebrovascular disease and/or peripheral artery disease; MACE: Non-fatal myocardial infarction and/or revascularization and/or cardiovascular death; thromboembolic events: ischemic stroke and/or systemic embolism and/or transient ischemic attack and/or myocardial infarction.
AF: Atrial fibrillation; CAD: Coronary artery disease; OR: Odds ratio; PAD: Peripheral artery disease.
Discussion
Although, it is known that the presence of comorbidities may have a negative impact on the prognosis of AF patients, it has not been well established how cardiovascular disease may impact on AF patients. This is even more relevant among patients taking direct oral anticoagulants. Our study of a wide sample of real-life patients with AF anticoagulated with rivaroxaban showed that patients with atherosclerotic vascular disease have a worse clinical profile and a much higher risk of MACE (cardiac mortality, coronary revascularization, non-fatal myocardial infarction), thromboembolic events and cardiovascular mortality than patients without vascular disease.
In the EMIR study, rivaroxaban was prescribed in high-risk patients, as in the pivotal clinical trial and in other real-life registries [11,16]. In addition, our study showed, in line with the ROCKET-AF substudies [17–19], that patients with CAD, peripheral artery disease/aortic plaque and vascular disease had a worse clinical profile, with more comorbidities and a higher thromboembolic and bleeding risk than patents without these conditions. As a result, our data are representative of this population. Therefore, the management of these patients is more challenging and requires a comprehensive, holistic approach addressing all aspects of prevention of cardiovascular disease [7].
In the EMIR study, patients with ischemic heart disease had greater incidence rates of MACE, coronary revascularization, cardiovascular death and death from any cause. In the ROCKET-AF trial, rates of cardiovascular death and myocardial infarction were higher in patients who had previously had myocardial infarction than in those who had not. Of note, among patients with previous myocardial infarction, the risk of ischemic cardiac events fell by 14% in those treated with rivaroxaban than in those treated with warfarin, although the difference was not significant [17]. A meta-analysis of nine trials from various clinical scenarios (AF, acute coronary syndrome, prophylaxis and treatment of deep venous thrombosis/pulmonary embolism), showed that compared with the control groups, rivaroxaban was associated with an 18% reduction in the risk of myocardial infarction [20]. As a result, although the risk of outcomes is higher in patients with CAD, this risk remains low among real-world AF patients taking rivaroxaban, likely owing to its beneficial effects on these outcomes [21]. A trend toward more major bleeding was observed; however, and is probably associated with the more frequent use of antiplatelet agents in this population [22]. Of note, the AFIRE trial showed that in patients with AF and stable CAD, rivaroxaban in monotherapy had a similar efficacy but better safety profile than the combination of rivaroxaban and a single antiplatelet agent [23].
In our study, similar outcomes were observed regardless of the presence of peripheral artery disease/aortic plaque. Although this could be explained by the low number of patients included in this subgroup, in the pivotal ROCKET AF clinical trial, patients with peripheral artery disease did not have a higher risk of stroke or systemic embolism [18]. However, in the EMIR study, patients with vascular disease had a higher risk of thromboembolic events, MACE and death. Therefore, it is necessary to consider not only the risk of stroke, but also that of other cardiovascular outcomes. In ROCKET AF, compared with warfarin, rivaroxaban exhibited a favorable net clinical benefit in terms of death, stroke, systemic embolism, myocardial infarction and major bleeding [24]. Our data would confirm the effectiveness and safety of rivaroxaban in clinical practice among patients with vascular disease.
Despite bleeding risk or cancer could be associated with more events [25,26], the multivariate analysis showed that concomitant use of antiplatelet agents was associated with a higher risk of MACE, both in patients with previous CAD and in those with vascular disease. This observation was also reported by other authors [27] and could have been associated with the possibility that these patients may have had recent acute coronary syndrome or undergone a myocardial revascularization procedure. It is well known that such patients are at particularly high risk for heart failure, repeated urgent revascularization and cardiovascular death [28]. Another explanation for the adverse outcomes affecting patients taking concomitant antiplatelet and anticoagulation medication is the possible increasing risk of embolic or atherosclerotic complications immediately after bleeding events. Accordingly, patients in the AFIRE trial who experienced major bleeding also had a higher risk of thrombotic complications, especially during the first 30 days after the bleeding event, likely associated with withdrawal of antithrombotic therapy [29]. Remarkably, in real-life patients, the combination of antiplatelet agents and oral anticoagulants among patients with AF does not prevent ischemic events, but rather significantly increases the frequency of major bleeding [30]. As a result, except for the first 12 months after an acute event coronary syndrome or coronary revascularization, antiplatelets agents should be withdrawn and anticoagulation should be considered the only antithrombotic therapy in AF patients with stable CAD (7).
Permanent AF was associated with a higher risk of thromboembolic events in affected patients. Although the type of AF is not included in the CHA2DS2-VASc score, it is important to remember that patients with a higher AF burden may have a higher risk of stroke [31]. Finally, chronic kidney disease was associated with a higher risk of major bleeding. Of note, as chronic kidney disease also markedly increases the risk of stroke, affected patients should be anticoagulated in most cases [32]. In addition, in a previous analysis of the EMIR study, renal function was preserved among patients chronically anticoagulated with rivaroxaban [13]. However, to obtain the maximum benefit, it is important that the dosage of all direct oral anticoagulants be adjusted according to renal function [8].
This study is subject to a series of limitations. Its observational design precluded the inclusion of a control group. Therefore, despite the high number of patients included, the consecutive recruitment, and the high quality of data recorded, confounding factors could be present. In addition, as the presence of coronary heart disease, vascular disease and aortic plaque were recorded from the electronic clinical history of patients, according to physicians’ criteria, some of these conditions could be underdiagnosed. On the other hand, patients with some of these conditions could be included in the other groups, limiting the analysis for each conditions separately. As a result, this was an exploratory analysis and the results should be confirmed in future studies. On the other hand, patients were recruited after at least 6 months of treatment with rivaroxaban in Spain. Consequently, the results of the EMIR study can only be applied to patients with similar clinical characteristics.
Conclusion
Among AF patients anticoagulated with rivaroxaban in clinical practice, approximately 16% have CAD and 28% vascular disease. Overall, rates of thromboembolic events, MACE, cardiovascular death and major bleeding are low. However, patients with atherosclerotic vascular disease exhibit a worse clinical profile and a higher risk of MACE, thromboembolic events and cardiovascular mortality than those without. The management of patients with AF and vascular disease requires a comprehensive approach, with the aim of reducing not only the risk of stroke, but also that of cardiovascular related complications. In this context, rivaroxaban should be considered for the treatment of affected patients in clinical practice.
•
Atherosclerotic cardiovascular disease and atrial fibrillation (AF) are common conditions that frequently co-occur.
•
This study analyzed the impact of the presence of atherosclerotic cardiovascular disease in AF patients anticoagulated with rivaroxaban.
•
This observational, multicenter and prospective study included 1433 AF adults anticoagulated with rivaroxaban ≥6 months.
•
Out of 1433 patients, 235 (16.4%) had coronary artery disease (CAD), 96 (6.7%) peripheral artery disease/aortic plaque and 406 (28.3%) vascular disease. Patients with any of these conditions exhibited a higher-risk clinical profile.
•
Patients with CAD had higher rates of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction or coronary revascularization), coronary revascularization, cardiovascular death and death from any cause.
•
Patients with vascular disease had higher rates of thromboembolic events, major adverse cardiovascular events, coronary revascularization, cardiovascular death, death from any cause and major bleeding.
•
CAD and vascular disease are common in patients with AF. Patients with AF have a worse clinical profile and a higher risk of outcomes.
Financial & competing interests disclosure
F Marín has received consultancy/lecturing fees from Bayer, Boehringer Ingelheim, Pfizer, Bristol Myers Squibb, Daiichi Sankyo and AFNET. M Sanmartín Fernández has received speaker and advisory fees from the following companies in the past 3 years: Bayer, Boehringer Ingelheim, BMS and Pfizer. G Barón-Esquivas has received honoraria as advisor from Bayer, Daiichi-Sankyo, BMS-Pfizer and Rovi; and honoraria as speaker from Boehringer-Ingelheim, Bayer, Daiichi-Sankyo, BMS and Pfizer. V Barrios has received consultancy/lecture fees from Bayer, BMS/Pfizer, Boehringer Ingelheim and Daiichi Sankyo. I Lekuona has received honoraria for presentations from Bayer, Boehringer-Ingelheim, Daiichi Sankyo and Pfizer-BMS. AI Pérez-Cabeza has received personal fees for educational activities or participation in boards from Daiichi Sankyo, Bayer, Boehringer Ingelheim and Bristol Myers Squibb. J Masjuan has received consultancy/lecturing fees from Bayer, Boehringer Ingelheim, Pfizer, Bristol Myers Squibb y Daiichi Sankyo. JM Vázquez Rodríguez has received lecturing fees from Bayer, Pfizer and Daiichi Sankyo. R Freixa-Pamias has received honoraria for presentations from Bayer, Boehringer-Ingelheim, Daiichi Sankyo and Pfizer-BMS. V Roldán Schilling has received honoraria for presentations from Bayer, Boehringer-Ingelheim, Daiichi Sankyo and Pfizer-BMS. F Arribas has received personal fees for educational activities or participation in boards from Daiichi Sankyo, Bayer, Boehringer Ingelheim and Bristol Myers Squibb. C Rafols Priu is an employee Bayer Hispania SL. M Anguita Sánchez has received funding for consulting and conference services from Bayer, Daiichi-Sankyo and Pfizer. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing and editorial assistance was provided by Content Ed Net (Madrid, Spain) with funding from Bayer Hispania.
Ethical conduct of research
The study was approved by each Ethical Committee of the participating centers.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int. J. Stroke 16(2), 217–221 (2021).
2.
Kotalczyk A, Mazurek M, Kalarus Z, Potpara TS, Lip GYH. Stroke prevention strategies in high-risk patients with atrial fibrillation. Nat. Rev. Cardiol. 18(4), 276–290 (2021).
• Shows that atrial fibrillation (AF) was associated with an increased risk of myocardial infarction.
3.
Ziff OJ, Carter PR, McGowan J et al. The interplay between atrial fibrillation and heart failure on long-term mortality and length of stay: insights from the United Kingdom ACALM registry. Int. J. Cardiol. 252, 117–121 (2018).
4.
Belkouche A, Yao H, Putot A et al. The multifaceted interplay between atrial fibrillation and myocardial infarction: a review. J. Clin. Med. 10(2), 198 (2021).
5.
Violi F, Soliman EZ, Pignatelli P, Pastori D. Atrial fibrillation and myocardial infarction: a systematic review and appraisal of pathophysiologic mechanisms. J. Am. Heart Assoc. 5(5), e003347 (2016).
6.
Miao B, Hernandez AV, Roman YM, Alberts MJ, Coleman CI, Baker WL. Four-year incidence of major adverse cardiovascular events in patients with atherosclerosis and atrial fibrillation. Clin. Cardiol. 43(5), 524–531 (2020).
• Shows that the risk of major adverse cardiovascular events increased in non anticoagulated patients with AF.
7.
Hindricks G, Potpara T, Dagres N et al. ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 42(5), 373–498 (2021).
8.
Marín F, Anguita-Sánchez M, Sanmartín M. Direct oral anticoagulants and cardiovascular prevention in patients with nonvalvular atrial fibrillation. Expert Opin. Pharmacother. 18(1), 67–77 (2017).
9.
Barrios V, Escobar C. From clinical trials to clinical practice. Experience with rivaroxaban in the anticoagulant treatment of patients with non-valvular atrial fibrillation. Semergen 43(3), 222–229 (2017).
10.
Pokorney SD, O'Brien EC, Granger CB. Assessing generalizability of trial results in general practice. Eur. Heart J. 37(14), 1154–1157 (2016).
11.
Camm AJ, Amarenco P, Haas S et al. XANTUS: a real-world, prospective, observational study of patients treated with rivaroxaban for stroke prevention in atrial fibrillation. Eur. Heart J. 37(14), 1145–1153 (2016).
•• This real-world study shows that rivaroxaban was effective and safe in clinical practice.
12.
Sanmartin-Fernández M, Marín F, Rafols C et al. the EMIR Study Investigators. Thromboembolic and bleeding events with rivaroxaban in clinical practice in Spain: impact of inappropriate doses (the EMIR study). J. Comp. Eff. Res. 10(7), 583–593 (2021).
• Shows that in clinical practice, rivaroxaban is properly dosed in the majority of patients.
13.
López-Gálvez R, Rivera-Caravaca JM, Anguita Sánchez M et al. Use of rivaroxaban attenuates renal function impairment in patients with atrial fibrillation: insights of the EMIR study. Eur. J. Clin. Invest. 52(9), e13788 (2022).
14.
Kidney Disease, Improving Global Outcomes (KDIGO), CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation, management of chronic kidney disease. Kidney Int. Suppl. 3, 1–150 (2013).
15.
Schulman S, Kearon C. Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of ant hemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 3(4), 692–694 (2005).
16.
Patel MR, Mahaffey KW, Garg J et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 365(10), 883–891 (2011).
17.
Mahaffey KW, Stevens SR, White HD et al. Ischaemic cardiac outcomes in patients with atrial fibrillation treated with vitamin K antagonism or factor Xa inhibition: results from the ROCKET AF trial. Eur. Heart J. 35(4), 233–241 (2014).
• In this substudy of the ROCKET-AF trial, among those patients with prior myocardial infarction, rivaroxaban was associated with a non significant 14% reduction in ischemic cardiac events compared with warfarin.
18.
Jones WS, Hellkamp AS, Halperin J et al. Efficacy and safety of rivaroxaban compared with warfarin in patients with peripheral artery disease and non-valvular atrial fibrillation: insights from ROCKET AF. Eur. Heart J. 35(4), 242–249 (2014).
19.
Hankey GJ, Patel MR, Stevens SR et al. Rivaroxaban compared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a subgroup analysis of ROCKET AF. Lancet Neurol. 11(4), 315–322 (2012).
• The benefits of rivaroxaban (vs warfarin) were independent of the history of previous cerebrovascular disease.
20.
Chatterjee S, Sharma A, Uchino K, Biondi-Zoccai G, Lichstein E, Mukherjee D. Rivaroxaban and risk of myocardial infarction: insights from a meta-analysis and trial sequential analysis of randomized clinical trials. Coron. Artery Dis. 24(8), 628–635 (2013).
21.
Coleman CI, Baker WL, Meinecke AK et al. Effectiveness and safety of rivaroxaban vs. warfarin in patients with non-valvular atrial fibrillation and coronary or peripheral artery disease. Eur. Heart J. Cardiovasc. Pharmacother. 6(3), 159–166 (2020).
• This real-life study shows in AF patients with coronary artery disease and/or peripheral artery disease that rivaroxaban was associated with a lower risk of major thrombotic vascular events than warfarin.
22.
Shah R, Hellkamp A, Lokhnygina Y et al. Use of concomitant aspirin in patients with atrial fibrillation: findings from the ROCKET AF trial. Am. Heart J. 179, 77–86 (2016).
23.
Yasuda S, Kaikita K, Akao M et al. Antithrombotic therapy for atrial fibrillation with stable coronary disease. N. Engl. J. Med. 381(12), 1103–1113 (2019).
24.
Barnett AS, Cyr DD, Goodman SG et al. Net clinical benefit of rivaroxaban compared with warfarin in atrial fibrillation: results from ROCKET AF. Int. J. Cardiol. 257, 78–83 (2018).
25.
Gu HQ. Rivaroxaban vs apixaban and ischemic or hemorrhagic events in patients with atrial fibrillation. JAMA 327(13), 1290 (2022).
26.
Liang B, Liang Y, Zhao LZ, Zhao YX, Gu N. Rivaroxaban for cancer-associated venous thromboembolism. Sci. Prog. 104(2), 368504211012160 (2021).
27.
Akao M, Shimizu W, Atarashi H et al. Oral anticoagulant use in elderly japanese patients with non-valvular atrial fibrillation – subanalysis of the ANAFIE Registry. Circ. Rep. 2(10), 552–559 (2020).
28.
Gibson CM, Mehran R, Bode C et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI. N. Engl. J. Med. 375(25), 2423–2434 (2016).
29.
Kaikita K, Yasuda S, Akao M et al. Bleeding and subsequent cardiovascular events and death in atrial fibrillation with stable coronary artery disease: insights from the AFIRE trial. Circ. Cardiovasc. Interv. 14(11), e010476 (2021).
•• In AF patients with stable coronary artery disease, major bleeding markedly increased the risk of subsequent major adverse cardiac and cerebrovascular events.
30.
Morimoto T, Uchida K, Sakakibara F, Kinjo N, Ueda S. Effect of concomitant antiplatelet therapy on ischemic and hemorrhagic events in patients taking oral anticoagulants for nonvalvular atrial fibrillation in daily clinical practice. Pharmacoepidemiol. Drug Saf. 30(10), 1321–1331 (2021).
31.
Kaplan RM, Koehler J, Ziegler PD, Sarkar S, Zweibel S, Passman RS. Stroke risk as a function of atrial fibrillation duration and CHA2DS2-VASc score. Circulation 140(20), 1639–1646 (2019).
32.
Stefil M, Nabrdalik K, Lip GYH. Renal disease and atrial fibrillation. Card. Electrophysiol. Clin. 13(1), 95–112 (2021).
Information & Authors
Information
Published In
Copyright
© 2023 Becaris Publishing Ltd.
History
Received: 9 March 2022
Accepted: 25 November 2022
Published online: 7 February 2023
Keywords:
Topics
Authors
Funding Information
Bayer Hispania: NA
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Non-embolic outcomes in patients with cardiovascular disease and atrial fibrillation treated with rivaroxaban. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2022-0049
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- J. Polo-García, R.M. Micó-Pérez, E. García-Gabriel, J.C. Romero-Vigara, L. García-Matarín, A. Segura-Fragoso, A. García-Lerín, B. Sánchez-Sánchez, C. Santos-Altozano, Oral anticoagulation in patients with atrial fibrillation in Primary Care in Spain. Rationale, design and baseline data of the RACOVIR study, Medicina de Familia. SEMERGEN, 10.1016/j.semerg.2026.102692, 52, 2, (102692), (2026).
- Carlos Escobar-Cervantes, Pablo Díez-Villanueva, Clara Bonanad Lozano, Antonio Pose Reino, Manuel Almendro-Delia, Lorenzo Facila, Alfonso Valle, Carmen Suárez, Vascular protection with rivaroxaban in the comprehensive management of atrial fibrillation, Expert Review of Cardiovascular Therapy, 10.1080/14779072.2023.2276893, 21, 11, (791-802), (2023).