Comparative economic outcomes in patients with focal seizures initiating eslicarbazepine acetate versus brivaracetam in the long-term care setting in the USA
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare all-cause and epilepsy-specific pharmacy and total costs associated with initiation of eslicarbazepine acetate (ESL) or brivaracetam (BRV) among patients with focal seizures in long-term care (LTC) in the US. Methods: This retrospective analysis used data from IQVIA's New Data Warehouse. Results: 298 patients initiated ESL and 282 patients initiated BRV. Initiation of ESL versus BRV was associated with 33.3% lower all-cause pharmacy costs, 34.4% lower epilepsy-specific pharmacy costs, 21.3% lower all-cause total costs and 30.9% lower epilepsy-specific total costs (all p < 0.0001). Conclusion: Among patients with focal seizures in LTC in the US, initiation of ESL versus BRV was associated with significant reductions in all-cause and epilepsy-specific pharmacy and total costs compared with initiation of BRV.
Epilepsy is a central nervous system disorder causing recurring, unprovoked seizures and affecting people of all ages, particularly the very young and old [1,2]. In the US the estimated prevalence of epilepsy is 1.2%, including approximately 3.4 million adults aged 18 years or older and 470,000 children [3].
Seizures are characterized by origin as generalized, focal, or unknown onset [4,5]. Focal seizures (FS), previously known by the term partial seizure, are the most common in adults and children [6,7]. The goal of epilepsy treatment is the complete elimination of seizures; however, this is not yet achievable in about one third of patients [8].
Epilepsy in the long-term care (LTC) setting is seven-times more prevalent than in the noninstitutionalized setting [9] and represents a substantial economic burden. In the US, a cross-sectional analysis of an institutionalized (nursing facility) Medicare population with and without epilepsy demonstrated the prevalence of epilepsy was 11.1%, and the risk-adjusted incremental cost of epilepsy was $507.33 per-patient per-month [9]. As the institutionalized population with epilepsy is projected to grow by 1–2% per year [9], there remains an unmet need to identify improvements in epilepsy care that may lower costs.
Antiseizure medications (ASMs) are the centerpiece of epilepsy treatment for most patients [10]. There are three generations of ASMs, including: first-generation (e.g., phenytoin, phenobarbital); second-generation (e.g., clonazepam, valproate, carbamazepine, diazepam, levetiracetam [LEV]); and third-generation (e.g., eslicarbazepine acetate [ESL], brivaracetam [BRV], levetiracetam, lacosamide) ASMs [8]. Third-generation ASMs may demonstrate better tolerability, fewer long-term adverse effects and fewer drug-drug interactions than first- or second-generation ASMs [8,11].
The choice of ASM, or combination of ASMs, should minimize adverse events, reduce the frequency of or eliminate seizures and maintain or improve patient quality of life [10]. ASMs should be selected based on epilepsy and seizure type, and patients' sex, age and comorbidities, including neurologic or psychiatric conditions [10]. Potential drug interactions should be considered [12].
ESL is a third-generation ASM approved by the US FDA in 2013 for the treatment of (partial-onset) FS in patients aged ≥4 years [13]. BRV, a structural analog of LEV, was granted FDA approval in 2016 and is indicated for the treatment of FS in patients aged ≥1 month [14]. ESL is available as an oral formulation; BRV is available both as an oral and intravenous formulation [13,14]. Pivotal clinical trials have demonstrated the safety and efficacy of ESL and BRV in patients with refractory epilepsy [15,16]. In three phase III, multicentre, randomized, double-blind, placebo-controlled clinical trials, ESL significantly reduced seizure frequency compared with placebo as an add-on therapy in patients with FS refractory to one to three concomitant ASMs [17–19]. In three phase III pivotal trials, adjunctive BRV significantly reduced seizure frequency compared with placebo in adults with FS [20–22].
The effectiveness of ESL and BRV has been studied in patients in real-world settings. A 24-week phase IV study conducted in a real-world clinical setting in patients with FS at early or later stages of their treatment history showed ESL to be effective and well tolerated as first or later adjunctive therapy [23]. Median reductions in standardized seizure frequency at 24 weeks were higher in patients initiating ESL as first adjunctive therapy to LEV or lamotrigine (72.8%) compared with in patients initiating ESL as later adjunctive therapy (22.8%). TEAEs were less frequent in the first adjunctive group (73%) than in the later adjunctive group (81%). ESLIBASE, a retrospective multicenter study assessing the efficacy and tolerability of ESL (prescribed according to real-life practice) in patients with FS, showed seizure frequency was reduced by ≥50% from baseline after 12 months in 49.8% of patients who switched to ESL after achieving poor seizure control with carbamazepine or oxcarbazepine [24]. Brivaracetam add-on first Italian network study (BRIVAFIRST), a multicenter study assessing the real-world effectiveness and tolerability of BRV add-on therapy (median daily dose, 100 mg at 3 months, 150 mg at 6 months and 150 mg at 12 months; BRV was added to a median of 2 concomitant ASMs) in patients with FS who were being treated with other ASMs for at least 3 months, showed seizure frequency was reduced by ≥50% from baseline after 12 months in 37.2% of patients, and 16.4% of patients were seizure free [25].
Treatment with third-generation ASMs may help alleviate the economic burden of epilepsy in LTC. ESL initiation in the LTC setting in the US has been associated with significant decreases in healthcare resource utilization, including epilepsy-specific physician office visits, emergency department (ED) visits, hospitalizations and all-cause physician office visits and hospitalizations [26]. In non-LTC setting, initiation of ESL as first adjunctive therapy was associated with significantly larger reductions in medical and non-ASM-related prescriptions charges compared with BRV [27] and ESL as first-line (1 L) monotherapy was associated with significantly greater reductions in any use of all-cause ED and outpatient and FS-related and outpatient services and all-cause medical and outpatient non-FS-related medical and non-ASM-related prescription charges compared with a generic ASM as 1 L monotherapy, in patients with FS [28].
To date, there are no comparative economic outcomes data for ESL and BRV in the LTC setting. The objective of this study was to compare all-cause and epilepsy-specific costs associated with the initiation of ESL or BRV in the LTC setting in the US among patients with FS. LTC settings included the following types of facilities: rehabilitation center, mental health center, LTC non-skilled nursing facility (SNF)/assisted-living facility (ALF), home health, assisted living, nursing home and other/unknown.
A sensitivity analysis examined all-cause and epilepsy-specific costs associated with the initiation of ESL or BRV among patients with any epilepsy or seizure diagnosis, as FS diagnoses are typically under-coded in US LTC settings. Subgroup analyses of patients with any epilepsy or seizure diagnosis stratified by the presence of comorbid intellectual developmental disorders (IDD), age ≥65 years and 0–1 prior ASMs were conducted.
It was hypothesized that initiation of ESL would be associated with lower costs compared with initiation of BRV.
Methods
Data source
The dataset was compiled from IQVIA's New Data Warehouse that includes deterministically linked LTC pharmacy, prescription and professional fee claims data and the IQVIA Hospital Charge Data Master (CDM) database. Linkage to CDM was not mandated [26].
The deidentified dataset is compliant with the Health Insurance Portability and Accountability Act; therefore, it does not constitute Human Subjects Research and approval from an institutional review board was not required [29].
Study design
This retrospective, observational, real-world cohort study included two mutually exclusive cohorts of patients: those who initiated ESL or BRV as monotherapy or as part of an adjunctive regimen in the LTC setting. The study period was from 1 February 2015 to 31 March 2021. The index date was the date of the first prescription of ESL or BRV in the LTC pharmacy data. The study consisted of a baseline period, defined as the 12 months prior to the index date, and a follow-up period, defined as the 12 months following the index date (Figure 1).
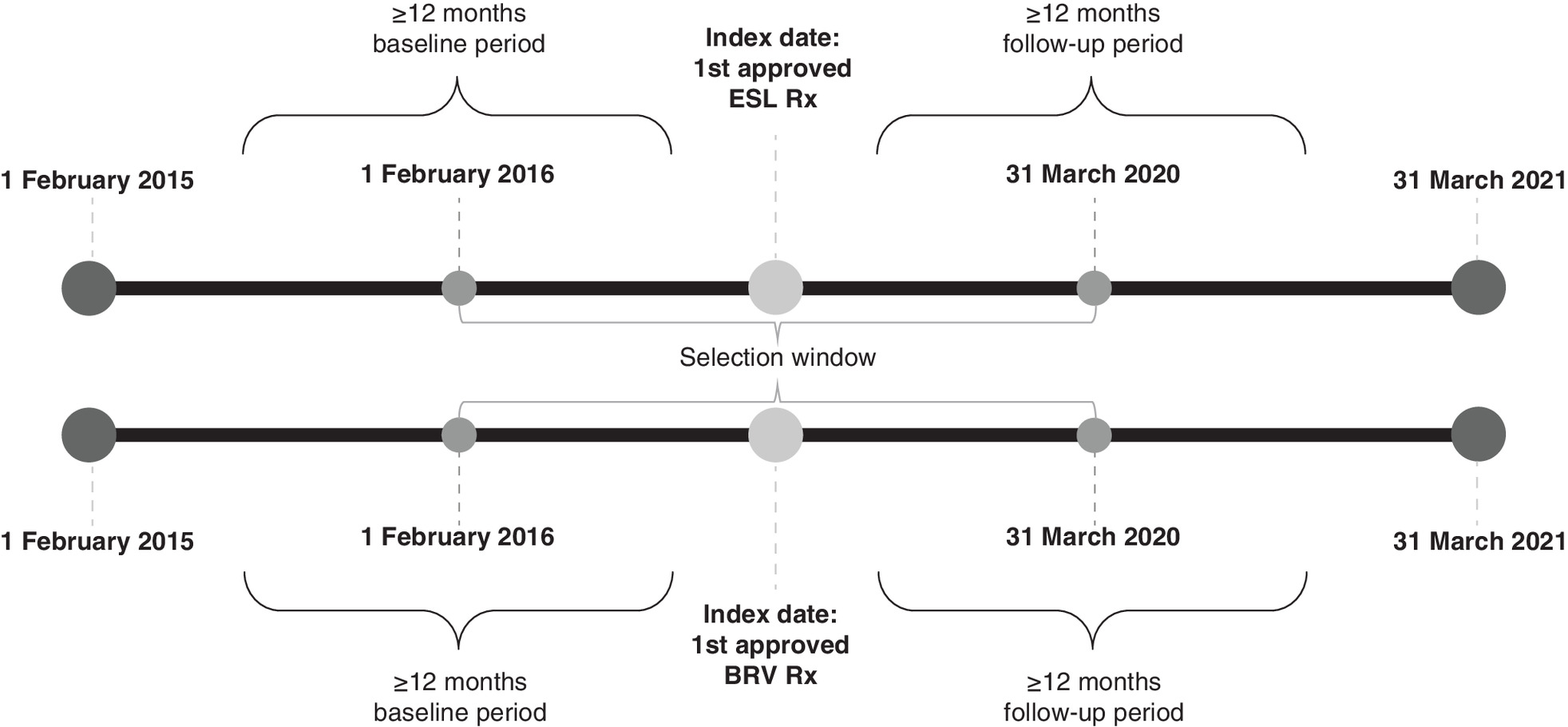
Figure 1. Study design.
BRV: Brivaracetam; ESL: Eslicarbazepine acetate; Rx: Prescription.
Patient population
Patient inclusion and exclusion criteria are described in Figure 2. Key inclusion criteria were: ≥1 prescription of ESL or BRV in the LTC pharmacy data at any time in the selection window between 1 February 2016 and 31 March 2020; deterministic linking of LTC pharmacy database, professional fee claims and prescription claims databases any time between 1 February 2015 and 31 March 2021 (study period); diagnosis code of FS in professional fee claims or CDM during the 12-month pre-index period including index date; activity, defined as ≥1 office visit and ≥1 prescription, in the 12-month baseline and follow-up periods; pharmacy stability in the 12-month baseline and follow-up periods, defined as consistent reporting of data from the pharmacy most frequently visited by the patient in each month during these periods; age ≥4 years at index date; and second prescription of the index medication in the follow-up period.
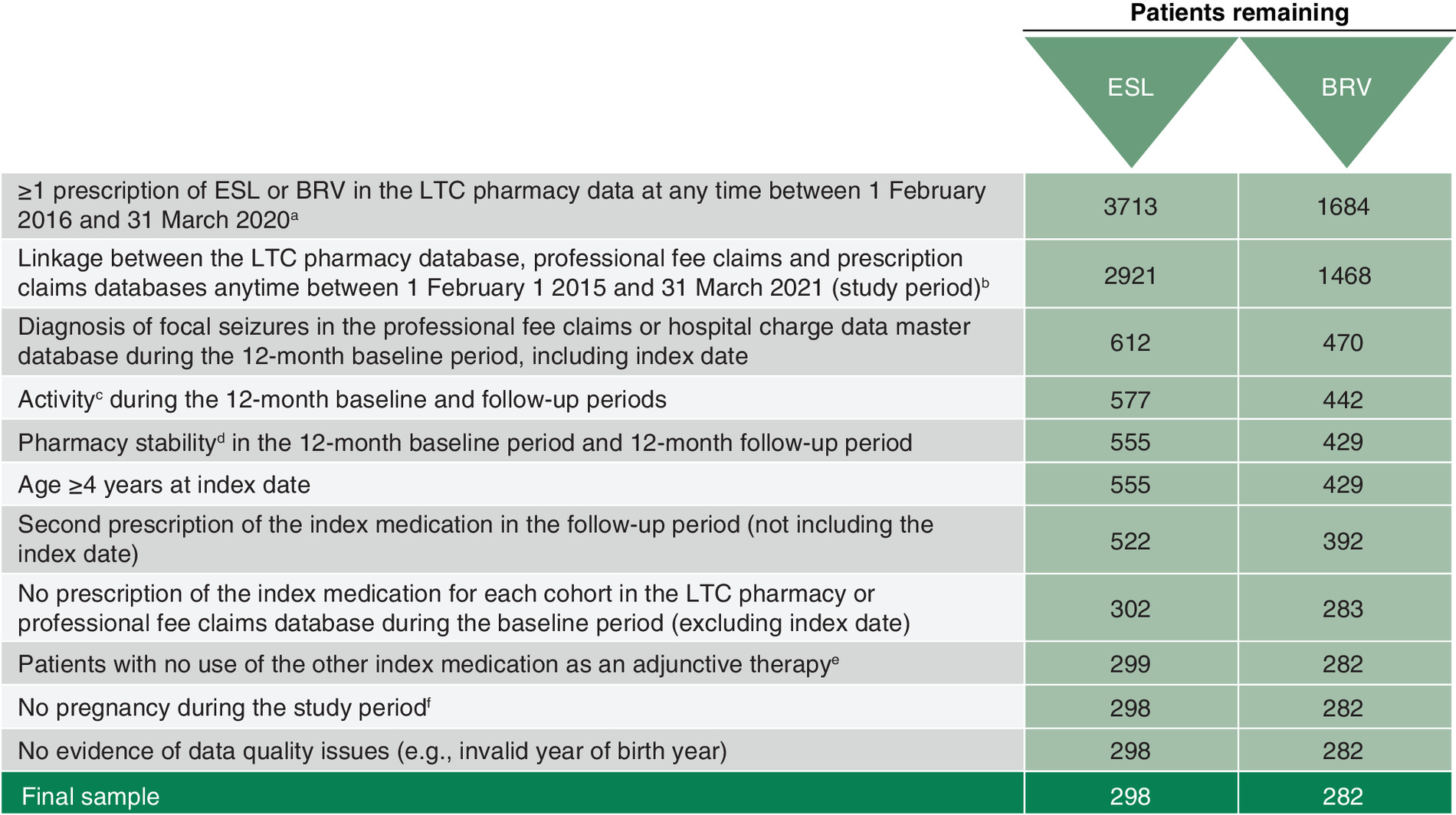
Figure 2. Key inclusion and exclusion criteria.
aThe date of the first prescription of ESL or BRV in the LTC pharmacy data serves as the patient's index date; two mutually exclusive cohorts (ESL users and BRV users) were created based on the index prescription claim. bStudy period is defined as 1 February 2015–31 March 2021. Subjects have a 6- or 12-month baseline and 6- or 12-month follow-up period. cActivity is defined as ≥1 office visit (in Dx) and ≥1 prescription (in Rx or LTC). dDefined as the consistent reporting of data from the most frequently visited pharmacy by the patient and at least 80% coverage rate for each month during the baseline and follow-up periods. eIn the ESL cohort, patients with add-on/adjunctive therapy of BRV were excluded and for the BRV cohort, patients with add-on/adjunctive therapy of ESL were excluded. fCodes indicating pregnancy include ICD-9: 630.xx–679.xx, V22–V24; ICD-10: O00–O9A, Z33, Z34, Z36, Z3A.
BRV: Brivaracetam; Dx: Diagnosis; ESL: Eslicarbazepine acetate; ICD: International Classification of Diseases; LTC: Long-term care; Rx: Prescription.
Patients were excluded from the analysis if they met any of the following criteria: index medication prescription during the baseline period, excluding index date; patients with use of the other index medication as an adjunctive therapy; evidence of pregnancy any time during the study period; or data quality issues (e.g., invalid year of birth, gender, region).
As the FS diagnosis may not be accurately reported in the LTC setting, sensitivity analyses were conducted to examine patients with any epilepsy or seizure diagnosis. Inclusion criteria for the sensitivity analysis were the same as those for the primary analysis except that patients had an epilepsy or seizure diagnosis in professional fee claims or CDM during the 12-month pre-index period, including the index date, instead of FS (Supplementary Figure 1).
Subgroup analyses stratified patients with any epilepsy or seizure diagnosis by the presence of IDD (International Classification of Diseases, 9th and 10th [ICD-9/10] codes: 317, 318, 318.0, 318.1, 318.2, 319, F70, F71, F72, F73, F78, F79), age (≥65 years) and prior ASMs (0–1).
Study measures & statistical analyses
Baseline demographic, clinical, ASM and LTC characteristics were measured during the 12-month pre-index (baseline) period or on the index date.
Baseline demographic characteristics
Baseline demographic characteristics included age, gender, geographic region (Northeast, Midwest, South or West) and payer type (cash, Medicaid, all Medicare, third party or other/unknown).
Baseline clinical characteristics
Baseline clinical characteristics included: Charlson Comorbidity Index (CCI)/Dartmouth-Manitoba adaptation; indicators of frail health status based on ICD-9 and ICD-10 clinical modification diagnosis and procedure codes for home oxygen use, wheelchair use, walker use, dementia, urinary catheter use, falls, fractures and composite of any of the preceding indicators; conditions that often co-occur with epilepsy; mental health disorders of interest; other comorbidities of interest; and medications of interest.
ASM-related characteristics
ASM-related characteristics included number of prior ASMs (0, 1, 2, 3+).
LTC-related characteristics
LTC-related characteristics included days in LTC prior to index; and LTC facility type (rehabilitation center, mental health center, LTC non-SNF/ALF, home health, assisted living, nursing home, other/unknown), which was assessed from LTC data as of the patient's index date if available (first option) or over the 12-month pre-index period.
Index treatment characteristics
Patients receiving ESL or BRV as monotherapy versus adjunctive therapy (combination or add-on therapy) were identified as follows: adjunctive therapy was defined as receipt of ESL or BRV with another ASM on the same day (ESL or BRV index date in LTC pharmacy data), or receipt of ESL or BRV with another ASM (from prescription claims or LTC pharmacy data) as add-on therapy, where the 2 medications were filled on separate days, but had an overlap in days' supply. Adjunctive therapy was confirmed if the same ASM was refilled less than 30 days after its supply had run out. All other patients prescribed ESL or BRV in the LTC setting but not meeting the criteria for adjunctive therapy were classified as receiving monotherapy.
Costs
Mean all-cause and epilepsy-specific costs per patient, including all-cause total and pharmacy costs, epilepsy-specific ASM-related pharmacy costs and total costs with pharmacy were determined over the 12-month follow-up period. A cost to charge ratio was applied for the charges in Professional Fee Claims and CDM to convert charges to cost. Costs were converted to 2021 USD using the medical component of the Consumer Price Index.
Statistical analyses
For baseline characteristics, categorical variables were reported as frequency (n) and percentage and compared using the χ2 test. Continuous variables were reported as mean and SD and compared using the independent sample t-test and Wilcoxon rank-sum test. Adjustments for baseline differences in patients initiating ESL or BRV were accomplished with inverse probability treatment weighting (IPTW). The maximum allowable weight was 5.
Generalized estimating equations (GEE) with gamma distribution and IPTW assessed the relative changes in all-cause and epilepsy-specific pharmacy-related total costs (defined as the sum of pharmacy, outpatient and inpatient costs) during the follow-up period. These models included unbalanced baseline characteristics as additional covariates.
For the subgroup analyses of patients with IDD, ≥65 years and 0–1 prior ASM at baseline, GEE with gamma distribution but without IPTW assessed the relative changes in all-cause and epilepsy-specific pharmacy and total costs during the follow-up period. These models included baseline characteristics that were found to be significantly different at baseline and were associated with the outcome of interest as covariates.
A p value < 0.05 was considered to be statistically significant. Analyses were conducted using SAS® Release 9.4 (SAS Institute Inc., NC, USA).
Results
Primary analysis: patients with FS
Baseline characteristics
A total of 3713 patients with ≥1 prescription of ESL and 1684 patients with ≥1 prescription of BRV during the selection window (1 February 2016 to 31 March 2020) were identified in the LTC pharmacy data. Of these, 612 patients with ≥1 prescription of ESL and 470 patients with ≥1 prescription of BRV had a diagnosis of FS during the baseline period, including the index date, and 298 patients with FS initiating ESL and 282 patients with FS initiating BRV were included in the analyses (Figure 2).
Baseline demographic and clinical characteristics of patients with FS initiating ESL or BRV are summarized in Tables 1 and 2. Prior to IPTW, patients initiating ESL were older (mean [SD] age: 54.2 [17.6] vs 49.2 [17.3] years), had a significantly higher comorbidity burden (mean [SD] CCI: 1.8 [2.2] vs 1.5 [2.1]; p = 0.05), were significantly more likely to have hypertension (115 [38.6%] vs 76 [27.0%]; p = 0.003), were significantly more likely to have statin comedication (101 [33.9%] vs 69 [24.5%]; p = 0.01) and had a significantly lower number of prior ASMs (mean [SD]: 2.7 [1.7] vs 3.1 [1.8]; p = 0.003) compared with patients initiating BRV. There were no significant differences in gender, type of facility, indicators of frail health status, comorbidities that often co-occur with epilepsy, or mental health disorders. After weighting, key differences between ESL and BRV cohorts were balanced.
| Characteristics | Pre-IPTW | Post-IPTW | ||
|---|---|---|---|---|
| ESL (n = 298) | BRV (n = 282) | ESL (n = 301) | BRV (n = 276) | |
| Age (years, mean [SD]) | 54.2 (17.6) | 49.2 (17.3) | 51.7 (17.7) | 51.3 (17.7) |
| Age group (years; n [%]) | ||||
| <65 years | 213 (71.5) | 223 (79.1) | 229 (76.2) | 205 (74.4) |
| ≥65 years | 85 (28.5) | 59 (20.9) | 72 (23.8) | 71 (25.6) |
| Gender (n [%]) | ||||
| Female | 131 (44.0) | 139 (49.3) | 140 (46.6) | 130 (47.0) |
| Male | 167 (56.0) | 143 (50.7) | 161 (53.4) | 146 (53.0) |
| Payer type (in professional claims; n [%]) | ||||
| All Medicare | 158 (53.0) | 160 (56.7) | 160 (53.3) | 149 (53.9) |
| Medicare (i.e., fee-for-service) | 133 (44.6) | 148 (52.5) | 142 (47.1) | 134 (48.5) |
| Medicare part D | 25 (8.4) | 12 (4.3) | 18 (6.1) | 15 (5.4) |
| Third party (i.e., commercial, including Medicare Advantage) | 113 (37.9) | 87 (30.9) | 107 (35.7) | 97 (35.3) |
| Medicaid | 27 (9.1) | 35 (12.4) | 33 (11.1) | 30 (10.8) |
| Facility type‡ (in LTC; n [%]) | ||||
| Other/unknown | 161 (54.0) | 150 (53.2) | 167 (55.4) | 150 (54.3) |
| Nursing home | 70 (23.5) | 66 (23.4) | 62 (20.5) | 68 (24.5) |
| Assisted living | 37 (12.4) | 39 (13.8) | 38 (12.8) | 36 (13.1) |
| Rehabilitation center | 22 (7.4) | 14 (5.0) | 23 (7.8) | 13 (4.8) |
| Mental health center | 7 (2.3) | 11 (3.9) | 9 (2.9) | 8 (2.8) |
| LTC-non SNF/ALF | 1 (0.3) | 2 (0.7) | 2 (0.6) | 2 (0.6) |
†
Assessed as of the patient's index date (if available, as first option) or over the 12-month pre-index period.
‡
Assessed from LTC data as of the patient's index date if available, as first option or over the 6- or 12-month baseline period.
Bolded values indicate p < 0.05.
ALF: Assisted-living facility; ASM: Antiseizure medication; BRV: Brivaracetam; ESL: Eslicarbazepine acetate; IPTW: Inverse probability treatment weighting; LTC: Long-term care; SD: Standard deviation; SNF: Skilled nursing facility.
| Characteristic | Pre-IPTW | Post-IPTW | ||
|---|---|---|---|---|
| ESL (n = 298) | BRV (n = 282) | ESL (n = 301) | BRV (n = 276) | |
| CCI score (in Dx or CDM; continuous) | ||||
| Mean | 1.8 | 1.5 | 1.7 | 1.7 |
| SD | 2.2 | 2.1 | 2.2 | 2.3 |
| Comorbidities that often co-occur with epilepsy (in Dx or CDM; n [%]) | ||||
|---|---|---|---|---|
| Stroke | 76 (25.5) | 61 (21.6) | 70 (23.4) | 64 (23.2) |
| Alzheimer's disease | 66 (22.1) | 52 (18.4) | 61 (20.2) | 63 (22.7) |
| Diabetes | 54 (18.1) | 35 (12.4) | 52 (17.2) | 39 (14.3) |
| Arthritis | 43 (14.4) | 43 (15.2) | 48 (15.8) | 49 (17.7) |
| PVD | 24 (8.1) | 20 (7.1) | 19 (6.4) | 22 (8.1) |
| Mental health disorders of interest (in Dx or CDM; n [%]) | ||||
|---|---|---|---|---|
| IDD | 81 (27.2) | 88 (31.2) | 94 (31.4) | 86 (31.2) |
| Anxiety | 67 (22.5) | 68 (24.1) | 72 (23.9) | 63 (22.7) |
| Depression | 63 (21.1) | 59 (20.9) | 68 (22.6) | 53 (19.3) |
| Schizophrenia | 37 (12.4) | 20 (7.1) | 36 (12.0) | 20 (7.1) |
| Disorders of psychological development (including autism) | 30 (10.1) | 35 (12.4) | 36 (12.1) | 33 (12.0) |
| Bipolar disorder | 22 (7.4) | 22 (7.8) | 24 (7.9) | 21 (7.5) |
| Autism | 16 (5.4) | 26 (9.2) | 20 (6.5) | 25 (9.2) |
| Behavioral/emotional disorders (excluding ADHD) | 16 (5.4) | 16 (5.7) | 18 (6.0) | 17 (6.2) |
| Mood disorders (excluding depression and bipolar disorder) | 16 (5.4) | 17 (6.0) | 22 (7.3) | 18 (6.6) |
| Cognitive impairment | 7 (2.3) | 10 (3.5) | 6 (1.9) | 10 (3.8) |
| ADHD | 6 (2.0) | 5 (1.8) | 7 (2.4) | 4 (1.6) |
| Unspecified developmental delay | 5 (1.7) | 5 (1.8) | 7 (2.2) | 7 (2.4) |
| Other comorbidities of interest (in Dx or CDM; n [%]) | ||||
|---|---|---|---|---|
| Hypertension | 115 (38.6) | 76 (27.0) | 99 (33.0) | 82 (29.7) |
| Atherosclerosis | 35 (11.7) | 32 (11.3) | 29 (9.6) | 39 (14.2) |
| Cancer | 32 (10.7) | 26 (9.2) | 33 (10.8) | 28 (10.3) |
| Hyponatremia | 27 (9.1) | 24 (8.5) | 29 (9.6) | 27 (9.7) |
| Traumatic brain injury | 25 (8.4) | 35 (12.4) | 26 (8.7) | 37 (13.5) |
| Alcohol/drug dependence | 21 (7.0) | 20 (7.1) | 20 (6.7) | 20 (7.4) |
| Sleep apnea | 20 (6.7) | 28 (9.9) | 19 (6.4) | 25 (8.9) |
| Parkinson's disease | 10 (3.4) | 8 (2.8) | 8 (2.7) | 9 (3.4) |
| Nervous system neoplasms | 8 (2.7) | 8 (2.8) | 8 (2.5) | 9 (3.3) |
| Central nervous system infections | 2 (0.7) | 7 (2.5) | 2 (0.6) | 7 (2.5) |
| Indicators of frail health status (in Dx or CDM; n [%]) | ||||
|---|---|---|---|---|
| Dementia | 63 (21.1) | 44 (15.6) | 59 (19.5) | 54 (19.5) |
| Falls | 52 (17.4) | 41 (14.5) | 50 (16.7) | 46 (16.7) |
| Fractures | 47 (15.8) | 46 (16.3) | 48 (16.1) | 47 (17.0) |
| Wheelchair use | 29 (9.7) | 30 (10.6) | 29 (9.7) | 33 (11.8) |
| Urinary catheter use | 13 (4.4) | 14 (5.0) | 11 (3.8) | 13 (4.8) |
| Home oxygen use | 8 (2.7) | 8 (2.8) | 8 (2.8) | 8 (2.9) |
| Walker use | 5 (1.7) | 10 (3.5) | 5 (1.7) | 12 (4.2) |
| Composite of the above (any indicators mentioned above) | 145 (48.7) | 123 (43.6) | 144 (47.9) | 127 (46.1) |
| Medications of interest (in LTC or Rx; n [%]) | ||||
|---|---|---|---|---|
| Antidepressants | 147 (49.3) | 154 (54.6) | 151 (50.3) | 145 (52.4) |
| Antipsychotics | 122 (40.9) | 114 (40.4) | 128 (42.7) | 110 (39.9) |
| Benzodiazepines | 111 (37.2) | 112 (39.7) | 114 (37.8) | 103 (37.4) |
| Statins | 101 (33.9) | 69 (24.5) | 84 (28.1) | 73 (26.4) |
| Thyroid supplements | 59 (19.8) | 67 (23.8) | 61 (20.4) | 70 (25.5) |
| Calcium channel blockers | 52 (17.4) | 45 (16.0) | 43 (14.4) | 51 (18.5) |
| Antacids | 11 (3.7) | 24 (8.5) | 9 (3.1) | 23 (8.3) |
| Prior ASMs (by different brand/generic names) (in LTC or Rx; continuous), n | ||||
|---|---|---|---|---|
| Mean | 2.7 | 3.1 | 2.9 | 3.0 |
| SD | 1.7 | 1.8 | 1.8 | 1.7 |
| Days in LTC prior to index‡ (continuous) | ||||
|---|---|---|---|---|
| Mean | 227.5 | 243.7 | 233.3 | 237.4 |
| SD | 150.5 | 147.7 | 148.4 | 146.8 |
†
All variables are assessed over the pre-index period, not including index date.
‡
Defined as days between first pharmacy LTC claim prior to the index date over the 6- or 12-month pre-index period and index date, inclusive of both boundaries.
Bolded values indicate p < 0.05.
ADHD: Attention-deficit/hyperactivity disorder; ASM: Antiseizure medication; BRV: Brivaracetam; CCI: Charlson Comorbidity Index; CDM: Charge description master; Dx: Diagnosis; ESL: Eslicarbazepine acetate; IDD: Intellectual and developmental disability; IPTW: Inverse probability treatment weighting; LTC: Long-term care; PVD: Peripheral vascular disease; Rx: Prescription; SD: Standard deviation.
Treatment type at index for patients with FS initiating ESL or BRV is summarized in Table 3; 78.9% of patients initiated ESL as adjunctive therapy and 87.2% of patients initiated BRV as adjunctive therapy.
| ESL (n = 298) | |
|---|---|
| Patients with FS receiving ESL as monotherapy, n (%) | 63 (21.1) |
| Patients with FS receiving ESL as adjunctive therapy†, n (%) | 235 (78.9) |
| Top 5 baseline ASMs to which ESL was added, n (%) | |
| Levetiracetam | 42 (14.1) |
| Divalproex sodium DR | 15 (5.0) |
| Lamotrigine | 13 (4.4) |
| Lamotrigine + levetiracetam | 10 (3.4) |
| Gabapentin | 7 (2.3) |
| BRV (n = 282) | |
|---|---|
| Patients with FS receiving BRV as monotherapy, n (%) | 36 (12.8) |
| Patients with FS receiving BRV as adjunctive therapy†, n (%) | 246 (87.2) |
| Top 5 baseline ASMs to which BRV was added, n (%) | |
| Lamotrigine | 19 (6.7) |
| Gabapentin | 9 (3.2) |
| Levetiracetam | 8 (2.8) |
| Oxcarbazepine | 7 (2.5) |
| Clonazepam | 5 (1.8) |
†
Receipt of ESL/BRV with another ASM on the same day (index date in LTC). Receipt of ESL/BRV with another ASM (from Rx or LTC) as add-on therapy, where the 2 medications are filled on separate days but have an overlap in days-supply. Adjunctive therapy was confirmed if the same ASM is refilled less than 30 days after its supply has run out.
ASM: Antiseizure medication; BRV: Brivaracetam; DR: Delayed-release; ESL: Eslicarbazepine acetate; FS: Focal seizure; LTC: Long-term care; Rx: Prescription.
Costs
Post-IPTW differences in economic outcomes during the follow-up period for patients with FS initiating ESL or BRV are summarized in Table 4. Patients initiating ESL had significantly lower all-cause total pharmacy cost (mean [SD]: $15,493.31 [$15,433.35] vs $24,224.61 [$21,854.66]; p < 0.0001), all-cause total cost (mean [SD]: $24,370.27 [28,912.69] vs $31,954.35 [$19,890.01]; p = 0.002), epilepsy-specific total ASM-related pharmacy cost (mean [SD]: $11,825.95 [11,853.22] vs $19,424.39 [$20,009.80]; p < 0.0001) and epilepsy-specific total cost with pharmacy (mean [SD]: $13,366.00 [13,862.72] vs $21,409.59 [22,929.26]; p < 0.0001) compared with patients initiating BRV. Initiation of ESL was associated with 33.3% lower all-cause pharmacy costs (p < 0.0001), 34.4% lower epilepsy-specific pharmacy costs (p < 0.0001) (Figures 3A & B), 21.3% lower all-cause total costs (p < 0.0001) (Figure 3C) and 30.9% lower epilepsy-specific total costs (p < 0.0001) (Figure 3D) compared with initiation of BRV.
| ESL (n = 301) | BRV (n = 276) | p-value independent† | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ESL vs BRV mean | |
| All-cause | |||
| Total pharmacy cost | $15,493 ($15,433) | $24,225 ($21,855) | <0.0001 |
| Total all-cause cost‡ | $24,370 ($28,913) | $31,954 ($29,890) | 0.0021 |
| Epilepsy-specific§ | |||
| Total ASM-related pharmacy cost | $11,826 ($11,853) | $19,424 ($20,010) | <0.0001 |
| Total cost with pharmacy | $13,366 ($13,863) | $21,510 ($22,929) | <0.0001 |
†
Independent comparisons conducted using parametric t-test for continuous variables and χ2 test or Fisher's exact test for categorical variables, as appropriate.
‡
Total all-cause costs with pharmacy: sum of total pharmacy, total outpatient and total inpatient costs among entire cohort.
§
Based on ICD-9/10-CM diagnosis codes for epilepsy or other convulsions in primary position.
Bolded values indicate p < 0.05.
ASM: Antiseizure medication; BRV: Brivaracetam; CM: Clinical modification; ESL: Eslicarbazepine acetate; FS: Focal seizure; ICD: International Classification of Diseases; IPTW: Inverse probability treatment weighting; SD: standard deviation.
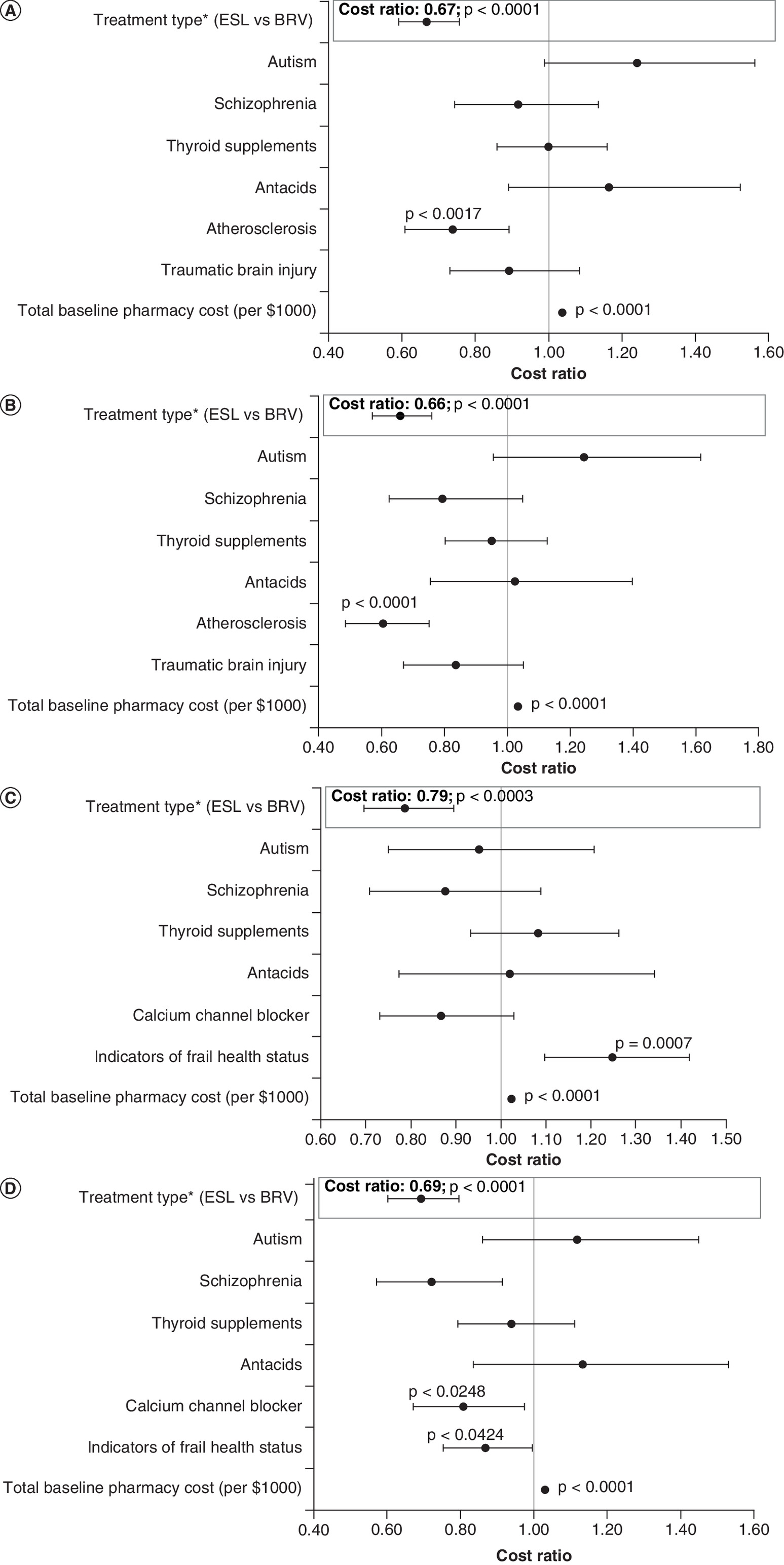
Figure 3. Primary analysis: Relative changes in (A) all-cause and (B) epilepsy-specific pharmacy cost and (C) all-cause and (D) epilepsy-specific total cost during the follow-up period (GLM results post-IPTW) in patients with FS.
*In addition to the treatment type, estimates for covariates unbalanced after IPTW are presented.
BRV: Brivaracetam; ESL: Eslicarbazepine acetate; FS: Focal seizure; GLM: Generalized linear model; IPTW: Inverse probability treatment weighting.
Sensitivity & subgroup analyses: patients with any epilepsy or seizure diagnosis
Sensitivity and subgroup analyses examined a broader definition of epilepsy to include patients with any epilepsy or seizure diagnosis. Of these, 1181 patients initiated ESL and 723 patients initiated BRV (Supplementary Figure 1), including 446 patients with IDD (ESL, n = 230; BRV, n = 216), 587 patients aged ≥65 years (ESL, n = 429; BRV, n = 158) and 492 patients with 0–1 prior ASMs (ESL, n = 351; BRV, n = 141). Adjustments for baseline differences in patients were conducted for the sensitivity analysis but were not conducted for the subgroup analyses.
All patients with any epilepsy or seizure diagnosis
Baseline demographic and clinical characteristics of patients with any epilepsy or seizure diagnosis initiating ESL or BRV are provided in Supplementary Tables 1 & 5. Patients with any epilepsy or seizure diagnosis appeared similar in mean age, comorbidities (mean CCI score), frailty status and number of prior ASMs to patients diagnosed with FS. Patients with any epilepsy or seizure were more likely to be ≥65 years of age or have hypertension. Post-IPTW, differences in economic outcomes during the follow-up period for patients with any epilepsy or seizure diagnosis initiating ESL or BRV are summarized in Supplementary Table 9. Patients initiating ESL had significantly lower all-cause total pharmacy cost (mean [SD] $14,150.85 [$16,095.18] vs $23,102.31 [$19,911.85]; p < 0.0001), all-cause total cost (mean [SD] $24,092.23 [$39,863.64] vs $30,074.79 [$31,788.46]; p = 0.0007), epilepsy-specific total ASM-related pharmacy cost (mean [SD] $9,689.45 [$10,730.83] vs $17,750.17 [$16,970.34]; p < 0.0001) and epilepsy-specific total cost with pharmacy (mean [SD] $11,897.04 [$18,486.45] vs $19,143.96 [$19,612.76]; p < 0.0001) compared with patients initiating BRV. Initiation of ESL was associated with 33.8% lower all-cause pharmacy costs (p < 0.0001) (Supplementary Figure 2A), 38.6% lower epilepsy-specific pharmacy costs (p < 0.0001) (Supplementary Figure 2B), 15.7% lower all-cause total costs (p < 0.0001) (Supplementary Figure 2C) and 31.0% lower epilepsy-specific total costs (p < 0.0001) (Supplementary Figure 2D) compared with initiation of BRV.
Patients with IDD
Baseline demographic and clinical characteristics of patients with any epilepsy or seizure diagnosis with IDD initiating ESL or BRV are provided in Supplementary Tables 2 & 6.
Differences in economic outcomes during the follow-up period for patients with any epilepsy or seizure diagnosis with IDD initiating ESL or BRV are summarized in Supplementary Table 9. Patients initiating ESL had significantly lower all-cause total pharmacy cost (mean [SD]: $16,592.53 [$15,846.02] vs $23,102.31 [$19,911.85]; p < 0.0001), all-cause total cost (mean [SD]: $26,014.61 [$38,026.31 vs $35,525.29 [$34,348.90]; p = 0.006), epilepsy-specific total ASM-related pharmacy cost (mean [SD]: $12,516.63 [$12,205.79] vs $24,372.78 [$26,151.24]; p < 0.0001) and epilepsy-specific total cost with pharmacy (mean [SD]: $15,993.84 [$26,168.25] vs $26,444.67 [$29,824.65]; p < 0.0001) compared with patients initiating BRV. Initiation of ESL was associated with 32.8% lower all-cause pharmacy costs (p < 0.0001) (Supplementary Figure 3A), 37.2% lower epilepsy-specific pharmacy costs (p < 0.001) (Supplementary Figure 3B), 16.5% lower all-cause total costs (p = 0.01) (Supplementary Figure 3C) and 27.3% lower epilepsy-specific total costs (p < 0.0001) (Supplementary Figure 3D) compared with initiation of BRV.
Patients aged ≥65 years
Baseline demographic and clinical characteristics of patients with any epilepsy or seizure diagnosis aged ≥65 years initiating ESL or BRV are provided in Supplementary Tables 3 & 7.
Differences in economic outcomes during the follow-up period for patients with any epilepsy or seizure diagnosis aged ≥65 years initiating ESL or BRV are summarized in Supplementary Table 9. Patients initiating ESL had significantly lower all-cause total pharmacy cost (mean [SD]: $9,303.03 [$9,400.96] vs $19,483.46 [19,149.19]; p < 0.0001), all-cause total cost (mean [SD]: $18,306.27 [$34,970.04] vs $27,173.58 [$35,911.41]; p < 0.0001), epilepsy-specific total ASM-related pharmacy cost (mean [SD]: $5,736.78 [$6,365.43] vs $14,088.87 [$16,637.31]; p < 0.0001) and epilepsy-specific total cost with pharmacy (mean [SD]: $6,612.62 [$8,612.24] vs $15,086.45 [$17,263.80]; p < 0.0001) compared with patients initiating BRV. Initiation of ESL was associated with 37.7% lower all-cause pharmacy costs (p < 0.0001) (Supplementary Figure 4A), 43.5% lower epilepsy-specific pharmacy cost (p < 0.0001) (Supplementary Figure 4A), 22.4% lower all-cause total cost (p = 0.01) (Supplementary Figure 4C) and 41.5% lower epilepsy-specific total cost (p < 0.0001) (Supplementary Figure 4D) compared with initiation of BRV.
Patients with 0–1 prior ASMs
Baseline demographic and clinical characteristics of patients with any epilepsy or seizure diagnosis with 0–1 prior ASMs initiating ESL or BRV are provided in Supplementary Tables 4 & 8.
Differences in economic outcomes during the follow-up period for patients with 0–1 prior ASMs initiating ESL or BRV are summarized in Supplementary Table 9. Patients initiating ESL had significantly lower all-cause total pharmacy cost (mean [SD]: $8,724.28 [$9,011.88] vs $19,092.29 [$18,004.38]; p < 0.0001), all-cause total cost (mean [SD]: $16,802.09 [$38,245.25] vs $30,233.11 [$41,383.91]; p < 0.0001), epilepsy-specific total ASM-related pharmacy cost (mean [SD]: $5,674.35 [$5,467.78] vs $12,965.54 [$10,695.17]; p < 0.0001) and epilepsy-specific total cost with pharmacy (mean [SD]: $6,175.39 [$5,934.72] vs $14,816.32 [$18,718.42]; p < 0.0001) compared with patients initiating BRV. Initiation of ESL was associated with 42.9% lower all-cause pharmacy costs (p < 0.0001) (Supplementary Figure 5A), 49.5% lower epilepsy-specific pharmacy costs (p < 0.0001) (Supplementary Figure 5B), 37.1% lower all-cause total cost (p < 0.001) (Supplementary Figure 5C) and 50.3% lower epilepsy-specific total cost (p < 0.0001) (Supplementary Figure 5D) compared with initiation of BRV.
Discussion
Findings from this retrospective, real-world study show that the initiation of ESL in patients with FS in the LTC setting is associated with a significant reduction in all-cause pharmacy costs, epilepsy-specific pharmacy costs, all-cause total costs and epilepsy-specific total costs compared with the initiation of BRV. The results of the sensitivity analysis in patients with any epilepsy or seizure diagnosis and subgroup analyses in patients with any epilepsy or seizure diagnosis and IDD, age ≥65 years, or 0–1 prior ASM supported the findings of the primary analysis.
LTC facility types that were examined in this study included nursing homes, assisted living, LTC non-SNF/ALF, mental health centers, rehabilitation centers and other or unknown facility types. While most patients were from an unknown facility type, more than one third of patients were in nursing homes or assisted living (ESL vs BRV, 35.9 vs 37.2%). Patients in the ESL and BRV cohorts were frail, as shown by a composite frailty indicator and had high levels of comorbid diseases, including IDD, depression, anxiety and hypertension. Similarly, a previous study of patients ≥65 years in any Medicare/Medicaid-certified nursing home in the US (2003–2007) showed scores for activities of daily living, frailty and cognition were worse in those with an epilepsy or seizure diagnosis compared with those without [30].
The economic benefits associated with initiating ESL versus BRV in patients with FS or any epilepsy or seizure diagnosis in LTC may be driven by the clinical profile of ESL [16,31,32,33]. In the present study, cost reductions associated with initiating ESL compared with BRV were associated with a decrease in pharmacy costs, potentially indicating lower utilization of concomitant medications with ESL compared with BRV. Polypharmacy is an important problem in patients in LTC. Polypharmacy is associated with increases in healthcare costs, adverse drug events, drug interactions and medication non-adherence, decreases in functional status and cognitive impairment and increases in fall rates and urinary incontinence [34].
To date, no study has directly compared the safety and efficacy of ESL versus BRV. In a previous report, initiation of a sodium-channel blocking ASM was associated with better 6-month (61% vs 37%) and terminal seizure freedom (52% vs 30%) versus LEV monotherapy, a structural analogue of BRV, in patients with newly treated focal epilepsy [35]. In a network meta-analysis to assess differences in total psychiatric-emergent adverse event (TEAE) end points between ESL and BRV in patients with FS, the odds of psychiatric TEAEs were lower for ESL compared with BRV (OR: 0.7 95% CrI: 0.5–1.2) and the number needed to harm was greater with ESL compared with BRV (ESL: 172.3, BRV: 32.4) [36]. Another systematic review and network meta-analysis did not find a significant difference in the seizure freedom outcome between BRV and ESL (ESL 800 mg/day vs BRV 50 mg/day OR: 1.2; 95% CI: 0.1–12.4, BRV 100 mg/day OR: 0.4; 95% CI: 0.1–1.9, BRV 200 mg/day OR: 0.5; 95% CI: 0.1–2.7; ESL 1200 mg/day vs BRV 50 mg/day OR: 1.2; 95% CI: 0.1–12.6, BRV 100 mg/day OR: 0.4; 95%: CI 0.1–1.9, BRV 200 mg/day OR: 0.5; 95%: CI 0.1–2.8) in patients with FS and seizures uncontrolled by one or more concomitant ASMs [37]. Further research is needed to better understand the drivers of economic outcomes associated with the initiation of ESL and BRV in patients with FS or any epilepsy or seizure diagnosis in LTC.
Patients with FS or any epilepsy or seizure diagnosis in LTC impose a heavy burden on the healthcare system [9,26], highlighting the need to improve patient care and reduce costs. Factors influencing the costs of epilepsy include the presence of IDD [38] and patient age [39]. IDD is a common comorbidity that accounts for a large proportion of healthcare expenditure for patients with epilepsy. In particular, costs for epilepsy management are higher in patients with IDD than for other patients with epilepsy [38]. In older adults, epilepsy is the third most common neurological disorder after stroke and dementia. Elderly (≥65 years) institutionalized patients with epilepsy have substantially higher healthcare costs than the elderly institutionalized population without epilepsy, mainly driven by inpatient costs [9]. The choice of ASM for patients with epilepsy and IDD is dependent on comorbidities, concurrent medications and general health, social and environmental status [40]. The selection of ASMs for elderly patients with epilepsy should account for potential changes in pharmacokinetic parameters, polypharmacy (including non-AEDs) and susceptibility to adverse drug effects [41]. In the LTC setting, ESL may represent a more favorable treatment for patients with epilepsy and IDD or elderly patients with epilepsy compared with BRV, as ESL may lead to lower all-cause and epilepsy-specific pharmacy and total costs. Monitoring of sodium levels should be considered in elderly patients since all dibenzazepine ASMs, including ESL, are associated with hyponatremia [42–44].
Early initiation of ESL as either first-line therapy or an add-on may reduce the cost of epilepsy care [27,45]. In a retrospective, longitudinal cohort analysis of patients with FS in a non-LTC setting, initiation of first adjunctive therapy with ESL was associated with significantly larger reductions in medical and non-ASM-related prescriptions charges compared with initiation of first adjunctive therapy with BRV [27]. Consistent with this, in the LTC setting, initiation of ESL in patients with any epilepsy or seizure diagnosis and 0–1 prior ASMs was associated with lower all-cause and epilepsy-specific pharmacy and total costs compared with initiation of BRV.
Retention of ASMs may represent an indirect measure of their effectiveness. In a retrospective, multicenter study that assessed the efficacy, tolerability and long-term retention rate of add-on BRV in clinical practice, the probability of remaining on BRV after 12 months was 61.1% (the overall retention rate was 50.8% for the five-year study period). The retention rate did not differ between patients stratified according to prior LEV treatment, although some literature has suggested that prior treatment with LEV may be associated with reduced efficacy of BRV [46]. The efficacy of conversion to BRV monotherapy was examined in an analysis of two phase III historical control studies of adult patients with uncontrolled FS (∼30% converting from LEV). The studies were terminated early because they reached a higher than expected discontinuation rate [47]. The efficacy of gradual conversion to ESL as monotherapy was studied in a phase III historical-control study of adults with FS not well controlled by their current ASMs. The Kaplan–Meier-estimated exit rate (the proportion of patients meeting at least one of the exit criteria, signifying worsening seizure control, during the 16-week study period) was 12.8% (95% CI: 7.5–21.5%) for ESL 1600 mg and 15.6% (95% CI: 8.1–28.7%) for ESL 1200 mg. The upper 95% confidence limits for the Kaplan–Meier-estimated exit rates were below the 65.3% pre-specified threshold for the historical controls [48]. Consistent with this, in a multicenter “withdrawal to monotherapy” historical-control study of patients with FS uncontrolled by current ASMs, the Kaplan–Meier-estimated exit rate for the efficacy population was 28.7% (95%CI 21.1–38.1%) for 1600 mg and 44.4% (32.5–58.3%) for ESL 1200 mg. The upper 95% confidence limits for the Kaplan–Meier-estimated exit rates were lower than the 65.3% pre-specified threshold for the historical controls [49]. A retrospective review in two centers evaluating psychiatric and behavioral side effects (PBSEs; induced psychosis, hypomania, aggressive behavior and other personality changes) in adults with active epilepsy treated with ESL after LEV withdrawal due to PBSEs, or who could tolerate LEV, showed no differences in psychiatric diagnoses or depressive symptoms, implying that ESL may be a treatment option for those who cannot tolerate LEV due to PBSEs [50]. A real world study of patients with FS showed switching to ESL compared with BRV after one generic ASM was associated with larger reductions in all-cause outpatient visits, total charges, all-cause medical, inpatient, emergency department and outpatient charges, FS-related medical, inpatient and emergency department charges and non-FS-related medical charges [51].
This study has several strengths. The use of real-world data to characterize the patient population in the LTC setting may be more representative than patients evaluated in a controlled trial. The sensitivity analyses to include patients using a broader definition of epilepsy may avoid under-coding of FS diagnoses. The LTC data are from large group provider organizations and other multiple independent pharmacies. As such, the data coverage may be representative of the LTC marketplace and thus increase the generalizability of the outcomes.
This study has several limitations. The use of open-source databases did not permit the capture of healthcare activity or consumption at nonparticipating sites. To mitigate this, pharmacy stability and continuous enrollment criteria were applied. Depending on the LTC setting, patients may have accessed healthcare in different ways. For example, a nursing home resident may see a physician at the LTC facility, whereas a resident in an ALF may visit an outpatient clinic to see a physician. ESL and BRV selection and prescribing may have varied as a result of patients' baseline demographic and clinical characteristics. To control for confounding (including due to treatment with prior ASMs), IPTW was implemented. Unobservable characteristics not included in the data may have affected outcomes.
Conclusion
This real-world study of patients in LTC with FS showed initiation of ESL was associated with significant reductions in all-cause and epilepsy-specific pharmacy and total costs compared with initiation of BRV. These results may assist clinicians and payers to make evidence-based therapeutic choices. Further comparative economic investigations with other ASMs in the LTC setting are warranted.
•
The increasing number of patients with epilepsy in long-term care (LTC) drives the need to reduce the cost of epilepsy care.
•
Eslicarbazepine acetate (ESL) and brivaracetam (BRV) are third-generation antiseizure medications (ASMs) approved for the treatment of focal seizures (FS).
•
This retrospective study compared economic outcomes associated with the initiation of ESL versus BRV in patients with FS in the LTC setting.
•
Initiation of ESL was associated with significantly lower all-cause and epilepsy-specific total costs (33.3% and 34.4%) and all-cause and epilepsy-specific pharmacy costs (21.3% and 30.9%) compared with initiation of BRV.
•
Similar findings were observed in a sensitivity analysis of patients with any epilepsy or seizure diagnosis and subgroup analyses of patients with any epilepsy or seizure diagnosis and intellectual developmental disorders, age ≥65 years, or 0–1 prior ASMs.
•
These data imply that initiation of ESL in patients with FS may reduce the costs of epilepsy care in the LTC setting compared with initiation of BRV.
Financial & competing interests disclosure
This study was funded by Sunovion Pharmaceuticals Inc. D Mehta, B Wensel and GR Williams are employees of Sunovion Pharmaceuticals Inc. I Lee and M DeKoven are employees of IQVIA, which received funding from Sunovion Pharmaceuticals Inc. to participate in this research. H Liu was an employee of IQVIA at the time of this study, which received funding from Sunovion Pharmaceuticals Inc. to participate in this research. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support provided by J Kondejewski of SNELL Medical Communication Inc. and funded by Sunovion Pharmaceuticals Inc.
Ethical conduct of research
The deidentified dataset is compliant with the Health Insurance Portability and Accountability Act; therefore, it does not constitute Human Subjects Research and approval from an institutional review board was not required.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 1.48 MB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Beghi E, Giussani G. Aging and the epidemiology of epilepsy. Neuroepidemiology 51, 216–223 (2018).
2.
Sirven JI. Epilepsy: a spectrum disorder. Cold Spring Harb. Perspect. Med. 5, a022848 (2015).
3.
Centers for Disease Control and Prevention. 2019 epilepsy prevalence in the United States. (2022). www.cdc.gov/epilepsy/data/index.html (Accessed 14 July 2022).
4.
Falco-Walter JJ, Scheffer IE, Fisher RS. The new definition and classification of seizures and epilepsy. Epilepsy Res. 139, 73–79 (2018).
5.
Sarmast ST, Abdullahi AM, Jahan N. Current classification of seizures and epilepsies: scope, limitations and recommendations for future action. Cureus 12(9), e10549 (2020).
6.
Hauser WA, Annegers JF, Kurland LT. Incidence of epilepsy and unprovoked seizures in Rochester, Minnesota: 1935–1984. Epilepsia 34(3), 453–458 (1993).
7.
Wirrell EC, Grossardt BR, Wong-Kisiel L. Incidence and classification of new-onset epilepsy and epilepsy syndromes in children in Olmsted County, Minnesota from 1980–2004: a population-based study. Epilepsy Res. 95(1-2), 110–118 (2011).
8.
Löscher W, Klein P. The pharmacology and clinical efficacy of antiseizure medications: from bromide salts to cenobamate and beyond. CNS Drugs 35, 935–963 (2021).
9.
Fitch K, Pan X, Lau J et al. Prevalence and economic burden of epilepsy in the institutionalized medicare fee-for-service population. Am. Health Drug Benefits 12(3), 151–158 (2019).
10.
Kanner AM, Bicchi MM. Antiseizure medications for adults with epilepsy: a review. JAMA 327(13), 1269–1281 (2022).
11.
Hakami T. Efficacy and tolerability of antiseizure drugs. Ther. Adv. Neurol. Disord. 14, 1–21 (2021).
12.
Gidal BE, French JA, Grossman P, Le Teuff G. Assessment of potential drug interactions in patients with epilepsy. Impact of age and sex. Neurology 72(5), 419–425 (2009).
13.
Aptiom. Prescribing information. Sunovion Pharmaceuticals Inc. (2013). www.aptiom.com/Aptiom-Prescribing-Information.pdf?_ga=2.26693117.114043104.1658109087-1842791351.1658109087 (Accessed 17 July 2022).
14.
Briviact. Prescribing information. UCB Inc (2016). www.briviact.com/briviact-PI.pdf (Accessed 17 July 2022).
15.
Feyissa AM. Brivaracetam in the treatment of epilepsy: a review of clinical trial data. Neuropsychiatr. Dis. Treat. 15, 2587–2600 (2019).
16.
Lattanzi S, Brigo F, Cagnetti C et al. Eslicarbazepine acetate in the treatment of adults with partial-onset epilepsy: an evidence-based review of efficacy, safety and place in therapy. Core Evid. 13, 21–31 (2018).
17.
Ben-Menachem E, Gabbai AA, Hufnagel A, Maia J, Almeida L, Soares-da-Silva. Eslicarbazepine acetate as adjunctive therapy in adult patients with partial epilepsy. Epilepsy Res. 89, 278–285 (2010).
18.
Elger C, Halasz P, Maia J, Almeida L, Soares-Da-Silva P. Efficacy and safety of eslicarbazepine acetate as adjunctive treatment in adults with refractory partial-onset seizures: a randomized, double-blind, placebo-controlled, parallel-group phase III study. Epilepsia 50, 454–463 (2009).
19.
Gil-Nagel A, Lopes-Lima J, Almeida L, Maia J, Soares-Da-Silva P. Efficacy and safety of 800 and 1200 mg eslicarbazepine acetate as adjunctive treatment in adults with refractory partial-onset seizures. Acta Neurol. Scand. 120, 281–287 (2009).
20.
Ryvlin P, Werhahn KJ, Blaszczyk B, Johnson ME, Lu S. Adjunctive brivaracetam in adults with uncontrolled focal epilepsy: results from a double-blind, randomized, placebo-controlled trial. Epilepsy. 55(1), 47–56 (2014).
21.
Biton V, Berkovic SF, Abou-Khalil B, Sperling MR, Johnson ME, Lu S. Brivaracetam as adjunctive treatment for uncontrolled partial epilepsy in adults: a phase III randomized, double-blind, placebo-controlled trial. Epilepsia 55(1), 57–66 (2014).
22.
Klein P, Schiemann J, Sperling MR et al. A randomized, double-blind, placebo-controlled, multicenter, parallel-group study to evaluate the efficacy and safety of adjunctive brivaracetam in adult patients with uncontrolled partial-onset seizures. Epilepsia 56(12), 1890–1898 (2015).
23.
Hixson J, Gidal B, Pikalov A et al. Efficacy and safety of eslicarbazepine acetate as a first or later adjunctive therapy in patients with focal seizures. Epilepsy Res. 171, 106561 (2021).
• This phase IV, open-label, non-randomized study showed that among adults with focal seizures in the USA and Canada who were treated with eslicarbazepine acetate (ESL) as first adjunctive therapy to levetiracetam (LEV) or lamotrigine (LTG) monotherapy (n = 36) or ESL as later adjunctive therapy (n = 37), ESL was effective and tolerable both as first adjunctive therapy to LEV or LTG and as a later adjunctive therapy.
24.
Villanueva V, Serratosa JM, Guillamón E et al. Long-term safety and efficacy of eslicarbazepine acetate in patients with focal seizures: results of the 1-year ESLIBASE retrospective study. Epilepsy Res. 108(7), 1243–1252 (2014).
• Among patients with focal seizures (FS) receiving eslicarbazepine acetate (ESL) in 12 hospitals in Spain, seizure frequency (obtained through clinical diaries), adverse events, and changes in concomitant antiseizure medications were retrospectively recorded in the ESLIBASE study, and the 12-month responder rate was 49.8% for those who had poor seizure control at baseline, and 20% of these patients were seizure-free, suggesting that ESL addition to patients already receiving other antiseizure medications could reduce seizure frequency by at least 50% from baseline after 12 months.
25.
Lattanzi S, Canafoglia L, Canevini MP et al. Adjunctive brivaracetam in focal epilepsy: real-world evidence from the brivaracetam add-on first Italian network study (BRIVAFIRST). CNS Drugs. 35(12), 1289–1301 (2021).
• In the BRIVAFIRST retrospective study conducted across 62 Italian centers on patients with focal seizures being treated with one or more antiseizure medications along with adjunctive brivaracetam (BRV) for at least 12 months (median doses of 100, 150 and 150 mg at 3, 6 and 12 months, respectively), 16.4% patients were seizure free and 37.2% patients had their seizure frequency reduced by 50% or more compared to baseline.
26.
Mehta D, Shah D, Desai V et al. Healthcare resource utilization among patients with focal seizures treated with eslicarbazepine acetate in the us long-term care setting: a retrospective claims database analysis. Neurol. Ther. 10(2), 673–691 (2021).
27.
Mehta D, Davis M, Epstein AJ et al. Comparative economic outcomes in patients with focal seizures initiating eslicarbazepine acetate versus brivaracetam as their first adjunctive ASD. J. Med. Econ. 24(1), 939–948 (2021).
•• Retrospective analysis of data from Symphony Health's Integrated Dataverse database (April 2015–June 2018) on patients with focal seizures who initiated eslicarbazepine acetate (ESL) (n = 208) or brivaracetam (BRV) (n = 137) as first adjunctive treatment to a single other baseline antiseizure medication showed that adjunctive ESL use had an economic benefit compared to adjunctive BRV use.
28.
Mehta D, Davis M, Epstein AJ, Wensel B, Grinnell, Williams RG. Comparative economic outcomes in patients with focal seizure initiating first-line eslicarbazepine acetate monotherapy versus generic antiseizure drugs. Clinicoecon. Outcomes Res. 13, 251–261 (2021).
29.
The United States Department of Health and Human Services. Summary of the HIPAA Privacy Rule. (2022). https://www.hhs.gov/sites/default/files/privacysummary.pdf (Accessed 14 July 2022).
30.
Birnbaum AK, Leppik IE, Svensden K, Eberly LE. Prevalence of epilepsy/seizures as a comorbidity of neurologic disorders in nursing homes. Neurology 88(8), 750–757 (2017).
31.
Toledano R, Jovel CE, Jiménez-Huete A et al. Efficacy and safety of eslicarbazepine acetate monotherapy for partial-onset seizures: experience from a multicenter, observational study. Epilepsy Behav. 73, 173–179 (2017).
32.
Trinka E, Ben-Menachem E, Kowacs PA et al. Efficacy and safety of eslicarbazepine acetate versus controlled-release carbamazepine monotherapy in newly diagnosed epilepsy: a phase III double-blind, randomized, parallel-group, multicenter study. Epilepsia 59, 479–491 (2018).
33.
Galiana GL, Gauthier AC, Mattson RH. Eslicarbazepine acetate: a new improvement on a classic drug family for the treatment of partial-onset seizures. Drugs R. D. 17, 329–339 (2017).
34.
Maher RL, Hanlon JT, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin. Drug Saf. 13(1), 57–65 (2014).
35.
Lloyd-Smith A, Hennessy R, Hegde M et al. Comparison of levetiracetam versus sodium channel blockers as first line antiseizure drug in participants with high seizure burden using human epilepsy project data. Am. Epilepsy Soc. Annu. Meeting 2016., Abstract 2.103 (2016).
36.
Mehta D, Azimpour K, Tremblay G et al. Network Meta-analysis comparing the psychiatric -emergent treatment adverse events associated with eslicarbazepine acetate and brivaracetam. Am. Epilepsy Soc. Conf. Proc., Accepted for presentation at AES 2020 (2020).
37.
Lattanzi S, Trinka E, Zaccara G et al. Third-generation antiseizure medications for adjunctive treatment of focal-onset seizures in adults: a systematic review and network meta-analysis. Drugs 82(2), 199–218 (2022).
•• A network meta-analysis of randomized controlled trials comparing oral brivaracetam (BRV), cenobamate (CNB), eslicarbazepine acetate (ESL), lacosamide (LSM) and perampanel (PER) showed that adjunctive CNB had a higher responder rate and the greatest likelihood ranking best for achieving seizure freedom compared to add-on BRV, ESL, LCM and PER.
38.
Pennington M, Prince E, Bateman N et al. Factors influencing the costs of epilepsy in adults with an intellectual disability. Seizure 21, 205–210 (2011).
• Intellectual disability (ID) is a common comorbidity of epilepsy and this prospective study assessing the health and social care costs of managing adults with epilepsy and ID in the community setting in the UK showed that ID increases the costs of epilepsy management, with perception of caregivers of a worse health state being a significant determinant of epilepsy health care utilization.
39.
Leppik IE. Epilepsy in the elderly. Epilepsia 47, 65–70 (2006).
• Polypharmacy is common among elderly patients with epilepsy, making it extremely important to consider age when choosing an antiseizure medication; moreover, lack of drug interactions and better safety profile may offset the additional costs of treatment with newer antiseizure medications compared to older ones.
40.
Watkins L, O'Dwyer M, Kerr M, Scheepers M, Courtenay K, Shankar R. Quality improvement in the management of people with epilepsy and intellectual disability: the development of clinical guidance. Expert Opin. Pharmacother. 21(2), 173–181 (2020).
41.
Lee SK. Epilepsy in the elderly: treatment and consideration of comorbid diseases. J. Epilepsy Res. 9(1), 27–35 (2019).
42.
Gupta DK, Bhoi SK, Kalita J, Misra UK. Hyponatremia following esclicarbazepine therapy. Seizure 29, 11–14 (2015).
43.
Willems LM, Zöllner JP, Paule E, Schubert-Bast S, Rosenow F, Strzelczyk A. Eslicarbazepine acetate in epilepsies with focal and secondary generalised seizures: systematic review of current evidence. Expert Rev. Clin. Pharmacol. 11(3), 309–324 (2018).
44.
Intravooth T, Staack AM, Juerges K, Stockinger J, Steinhoff BJ. Antiepileptic drugs-induced hyponatremia: review and analysis of 560 hospitalized patients. Epilepsy Res. 143, 7–10 (2018).
45.
Mehta D, Davis M, Epstein AJ et al. Impact of early initiation of eslicarbazepine acetate on economic outcomes among patients with focal seizure: results from retrospective database analyses. Neurol. Ther. 9(2), 585–598 (2020).
46.
Strzelczyk A, Zaveta C, von Podewils F et al. Long-term efficacy, tolerability, and retention of brivaracetam in epilepsy treatment: a longitudinal multicenter study with up to 5 years of follow-up. Epilepsia 62(12), 2994–3004 (2021).
47.
Arnold S, Badalamenti V, Diaz A et al. Conversion to brivaracetam monotherapy for the treatment of patients with focal seizures: two double-blind, randomized, multicenter, historical control, phase III studies. Epilepsy Res. 141, 73–82 (2018).
48.
Jacobson MP, Pazdera L, Bhatia P, Grinnell T, Cheng H, Blum D. Efficacy and safety of conversion to monotherapy with eslicarbazepine acetate in adults with uncontrolled partial-onset seizures: a historical-control phase III study. BMC Neurology. 15 46 (2015).
49.
Sperling MR, Harvey J, Grinnell T, Cheng H, Blum D. Efficacy and safety of conversion to monotherapy with eslicarbazepine acetate in adults with uncontrolled partial-onset seizures: a randomized historical-control phase III study based in North America. Epilepsia 56(4), 546–555 (2015).
50.
Jalihal V, Shankar R, Henley W et al. Eslicarbazepine acetate as a replacement for levetiracetam in people with epilepsy developing behavioral adverse events. Epilepsy Behav. 80, 365–369 (2018).
51.
Mehta D, Davis M, Epstein AJ, Wensel B, Thach A, Williams GR. Comparative economic outcomes in patients with focal seizure initiating eslicarbazepine acetate versus brivaracetam after switching from generic antiseizure drug. Presented at ISPOR 2022, May 15–18 (2022).
Information & Authors
Information
Published In
Pages: 1293 - 1308
PubMed: 36331060
Copyright
© 2022 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 23 September 2022
Accepted: 21 October 2022
Published online: 4 November 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative economic outcomes in patients with focal seizures initiating eslicarbazepine acetate versus brivaracetam in the long-term care setting in the USA. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0170
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Wei Jing, Meizhen Sun, Chao Yan, Antiseizure Medications, Pharmacological Treatment of Epileptic Seizures, 10.1007/978-981-96-8520-2_2, (59-327), (2025).
- Walter Garcia-Ubbelohde, Lia Pizzicato, Keith J Boesen, Swapna Munnangi, Liucheng Shi, Nicholas B. Hurst, Mitchell DeKoven, Cost comparison of F(ab’) 2 and Fab antivenoms for pit viper envenomation in the United States: a real-world analysis , Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2025.2462236, 25, 5, (721-728), (2025).