Healthcare and economic burden of anticholinergic use in adults with overactive bladder: a systematic literature review
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To determine the economic burden associated with anticholinergic medication use in adults with overactive bladder (OAB) in the USA. Methods: A systematic literature review was conducted to identify articles assessing healthcare resource utilization (HCRU) and costs associated with anticholinergic use in adults with OAB. Results: From the 34 articles identified, increased anticholinergic burden, switching anticholinergic treatments and potentially inappropriate anticholinergic use were associated with increased HCRU and/or costs. However, studies comparing patients with OAB receiving anticholinergics to individuals with untreated OAB or without OAB reported a mix of increases and decreases in HCRU and costs. Conclusion: Additional controlled studies assessing the economic impact of anticholinergics in OAB are needed and may enable optimization of economic and potentially patient outcomes.
Graphical abstract

Overactive bladder (OAB) is a urologic condition with symptoms including urinary urgency, with or without urge urinary incontinence (UUI); increased daytime urinary frequency; and nocturia [1]. It is estimated that at least 30 million individuals ≥40 years of age in the USA experience bothersome OAB symptoms [2]. OAB is associated with increased incidence of comorbidities, including depression, anxiety and falls, as well as reduced health-related quality of life [3–5]. OAB is also associated with a high economic burden, including medical costs, lost productivity and healthcare resource utilization (HCRU); average healthcare costs (including inpatient, emergency room, outpatient, pharmacy and other costs) for patients with OAB have been estimated at $3003 per patient per month versus $1123 per patient per month for a matched control group without OAB [6,7].
Current American Urological Association/Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction (AUA/SUFU) guidelines recommend behavioral therapy as first-line treatment and pharmacologic interventions with β3-adrenergic receptor agonists or anticholinergic medications as second-line treatment for patients with OAB [1]. Anticholinergic medications are the most prescribed OAB treatments in the USA [8–10].
Long-term use of anticholinergic medications is associated with side effects including dry mouth, constipation and potential for cognitive impairment [1,11–17]. Increasing anticholinergic burden is associated with increased risk of falls/fractures, all-cause mortality and major adverse cardiovascular events, as well as clinically relevant drug–drug interactions [1,18]. Furthermore, the use of anticholinergic medications is associated with an estimated 46% increase in the risk of developing dementia compared with nonuse [19]. Both using a single anticholinergic medication and switching anticholinergic medications have been reported to cumulatively increase the risk of incident dementia [17]. Furthermore, use of urologic anticholinergic medications has been associated with increased risk of dementia even when the drug exposure occurs 15–20 years before a dementia diagnosis [15]. Anticholinergic medication use has also been associated with increased brain atrophy, cognitive dysfunction and clinical decline [16]. Because of the increased risk of cognitive decline, the current American Geriatrics Society (AGS) Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults recommend minimizing anticholinergic medication burden, and AUA/SUFU guidelines recommend that clinicians should exercise caution before recommending anticholinergic medications for patients with OAB who are frail or using other anticholinergic medications [1,20].
A retrospective claims analysis showed that 88% of patients taking an anticholinergic medication to treat OAB discontinued or switched medications within 12 months and only 31% of patients who had ≥2 prescription claims for an anticholinergic medication remained adherent (defined as >80% of days covered by index medication) after 12 months [21]. Common patient-reported reasons for discontinuing an OAB medication include lack of efficacy, adverse effects and learning to manage their symptoms without medication [22,23].
The available evidence on the impact of anticholinergic medications on HCRU and associated healthcare costs has not been comprehensively reviewed among patients with OAB. Therefore, a systematic literature review was conducted to identify and summarize the burden associated with anticholinergic medication use in adult patients with OAB in the USA in terms of HCRU and costs to the payor.
Methods
Protocol & registration
The systematic literature review was conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions [24] and reported in alignment with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [25]. The protocol was registered in the PROSPERO database (registration no.: CRD42021258363) [26].
Search strategy
The search strategy was developed by an experienced information specialist and was peer reviewed by a second information specialist. Two reviewers (Corinne Duperrouzel [CD] and Coby Martin [CM]) independently reviewed studies for inclusion; data extraction and quality assessments were performed by a single reviewer and validated by a second. Any disagreements that could not be resolved by consensus were resolved by a third reviewer (Ari Mendell [AM] or Megan Bourque [MB]).
Studies published before 28 May 2021 were identified from MEDLINE, Embase and the Cochrane Database of Systematic Reviews using a combination of controlled vocabulary and keywords relating to OAB, anticholinergic medications, HCRU and costs. Published and validated economics and cost filters were applied, including both balanced and sensitive filters (see Supplementary Table 1 for full search strategy). Opinion and animal studies were excluded in the search and no gray literature searches were conducted because it was assumed that clinical trial registries and health technology assessment bodies would be unlikely to report on the outcomes of interest. Conference abstracts older than 2 years before the date of the search were excluded, as it was expected that full-text publications of relevant studies would be available by the time the search was conducted.
Eligibility criteria
The review focused on observational studies, randomized controlled trials and economic evaluations of healthcare use and costs to payors for adult patients (≥18 years) with OAB treated with anticholinergic medications. Eligibility criteria were established using the population, intervention, comparator, outcomes and study design (PICOS) framework (Table 1). Abstracts published >2 years before the date of the search were excluded, along with opinion articles, case studies, reviews and meta-analyses. However, the bibliographies of relevant meta-analyses and systematic literature reviews identified during the screening process were reviewed to identify any additional relevant references. Articles were also excluded if they were not in English or focused on populations exclusively outside the USA. Articles assessing OAB caused by neurogenic detrusor overactivity were included; this prevented the exclusion of articles that did not distinguish between patients with neurogenic and non-neurogenic OAB. No time horizon was specified in the database searches and manuscripts were not omitted based on publication date alone.
| Criteria | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Primary considerations | ||
| Population | • Adults (≥18 years) with a diagnosis of OAB • Adults without OAB were included as a control arm | • Patients <18 years • Patients without OAB, unless included as a control arm • Animals |
| Intervention | • Anticholinergic medications approved for the treatment of OAB in the USA (darifenacin, fesoterodine, oxybutynin, solifenacin, tolterodine, trospium) | • Other pharmacologic medications, including anticholinergics not approved for the treatment of OAB in the USA • Medical devices • Surgery • Nerve stimulation |
| Comparator | • A different anticholinergic medication approved for the treatment of OAB in the USA (see Intervention) • Placebo • No treatment | • See Intervention |
| Outcomes | • HCRU (hospitalizations, inpatient stays, outpatient visits, emergency room/department visits, length of hospital and/or ICU stay) • Costs associated with HCRU outcomes from the payor perspective | • Studies that do not report ≥1 of the outcomes of interest |
| Study design | • Prospective or retrospective (including database studies and chart reviews) single-arm or comparative observational studies • Economic analyses • RCTs • Conference abstracts published in 2019 or later | • Narrative reviews • Editorials • Letters • Case studies • Opinion pieces • Conference abstracts published before 2019 • Systematic reviews and meta-analyses† |
| Additional considerations | ||
|---|---|---|
| Language | • English | • Non-English |
| Location | • USA | • Outside the USA |
| Date limit | • Conference abstracts and posters published in 2019 or later • No date restrictions were placed on full-text articles | • Conference abstracts and posters published before 2019 |
†
Systematic reviews and meta-analyses were not eligible for inclusion but were captured and used to identify additional studies meeting the eligibility criteria.
HCRU: Healthcare resource use; ICU: Intensive care unit; OAB: Overactive bladder; RCT: Randomized controlled trial.
Study selection
The study records and corresponding full-text articles were reviewed for inclusion using DistillerSR software.
Data extraction
Studies meeting the inclusion criteria were extracted into a standardized form; the extraction data included publication characteristics, study design characteristics, study participant and baseline characteristics, model methods, HCRU outcomes, cost outcomes and study conclusions. All HCRU and cost outcomes related to the population and comparators of interest were extracted. For HCRU outcomes, mean values were prioritized and median values were extracted if means were not reported.
Risk of bias assessment
Results
Overview of search results
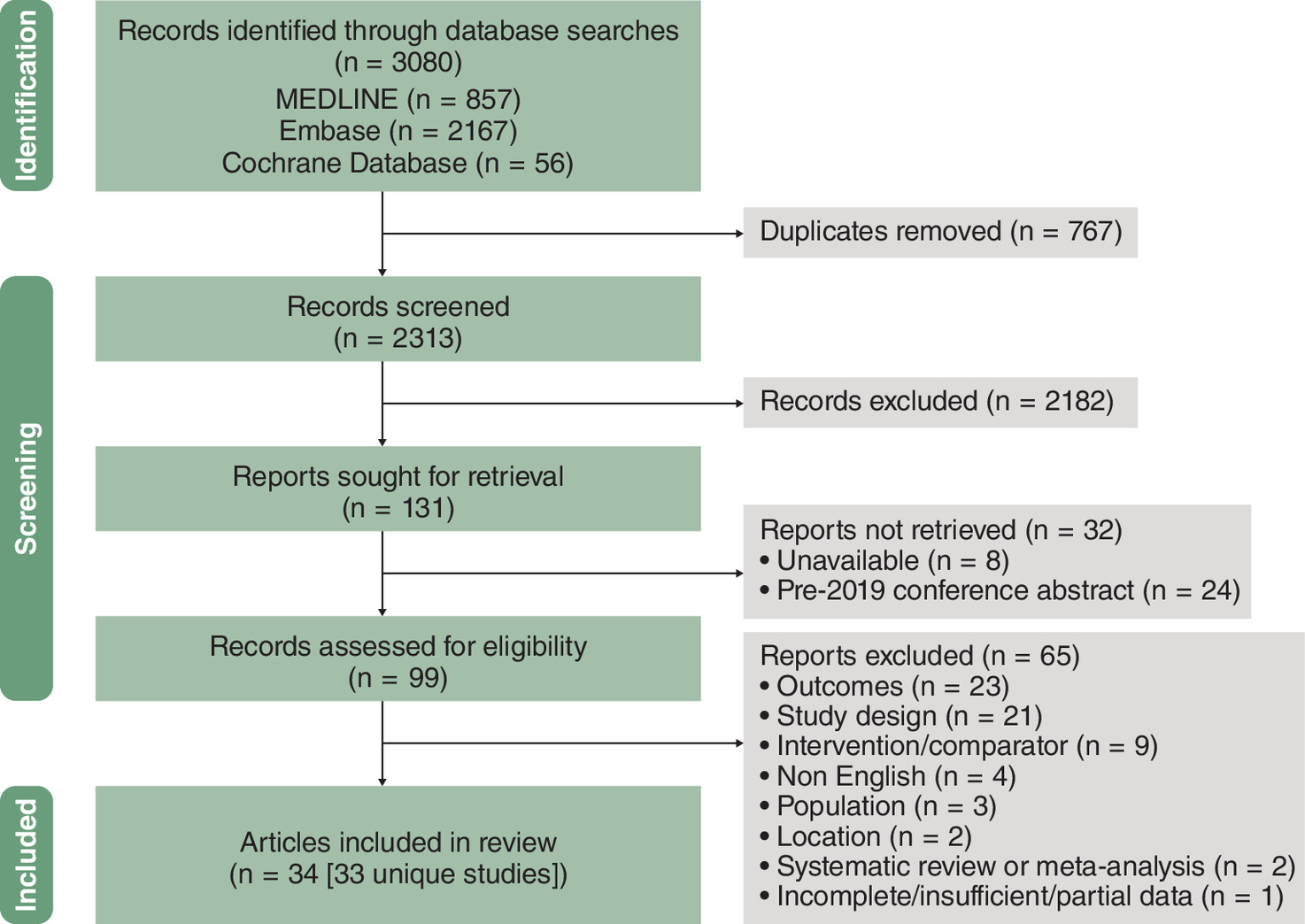
The electronic search returned 3080 citations. A total of 2313 records were screened after removing duplicates and 2182 were excluded because they did not meet the prespecified inclusion criteria. Of the remaining 131 records, 24 were conference citations published before 2019, 8 did not have available full-text articles and 99 were retrieved for full-text review. After assessing full-text articles, 65 were excluded and 34 were included in the review (Figure 1, Table 2).
| Study (year) | Study design | Cost year | n | Treatments† | Patients | Ref. |
|---|---|---|---|---|---|---|
| Economic evaluations | ||||||
| Arikian et al. (2000) | Cost–effectiveness analysis | NR | 1363 | Oxybutynin ER, oxybutynin IR, tolterodine | Patients with OAB | [29] |
| Armstrong et al. (2012) | Cost–effectiveness analysis | 2011 | NA | Solifenacin, trospium IR, trospium ER, darifenacin, fesoterodine, oxybutynin IR, oxybutynin ER, oxybutynin TD, oxybutynin gel, tolterodine IR, tolterodine ER | Patients with OAB | [30] |
| Chen et al. (2012) | Cost–effectiveness analysis | 2010 | 100 | Tolterodine ER, PTNS | Female patients with OAB | [31]‡ |
| Ko et al. (2006) | Cost–effectiveness analysis | 2005 | NA | Oxybutynin IR, oxybutynin ER, oxybutynin TD, tolterodine IR, tolterodine ER, trospium, solifenacin, darifenacin | Patients with OAB | [32] |
| Murray et al. (2019) | Cost–effectiveness analysis | 2014 | NA | Tolterodine ER, solifenacin, BSC | Patients with refractory OAB | [33] |
| Murray et al. (2021) | Cost–effectiveness analysis | NR | NR | BSC, solifenacin, tolterodine ER | Patients with OAB | [34] |
| Noe et al. (2002) | Cost–minimization analysis | 2000 | NA | Tolterodine ER, oxybutynin CR | Patients aged 20–89 years with OAB, currently using behavioral therapy and drug treatment | [35] |
| Perfetto et al. (2005) | Cost–minimization analysis | NR | 59,984 | Tolterodine ER, oxybutynin ER | Patients with new diagnosis of OAB or new use of a treatment of interest | [36] |
| Perk et al. (2016) | Budget impact model | 2015 | 1-M-member plan | Fesoterodine, darifenacin, solifenacin, tolterodine IR, tolterodine ER, oxybutynin, trospium | Hypothetical patients in a commercial plan or Medicare Advantage plan; patients aged 24–64 years with OAB | [37] |
| Qin et al. (2016) | Decision analytic cost model | 2013 | 7096 | Fesoterodine, no OAB treatment | Patients aged ≥65 years with OAB wet; 2–15 UUI episodes per day, at risk of deteriorating health (score of ≥3 on Vulnerable Elders Survey) | [38] |
| Shepherd et al. (2018) | Cost–effectiveness analysis | 2016 | NA | Tolterodine, solifenacin | Patients with OAB | [39] |
| St Martin et al. (2020) | Cost–effectiveness analysis | NR | NA | Oxybutynin | Medicare-eligible women with OAB refractory to conservative management | [40] |
| Wielage et al. (2016) | Cost–effectiveness analysis | 2015 | NR | Solifenacin, tolterodine ER, fesoterodine, trospium, tolterodine IR, oxybutynin | Commercial plan: 2% of patients aged ≥65 years; Medicare plan: ≥83.2% of patients aged ≥65 years | [41] |
| Yehoshua et al. (2018) | Cost analysis | NR | NA | Darifenacin, fesoterodine, oxybutynin IR, oxybutynin ER, oxybutynin gel, solifenacin, tolterodine IR, tolterodine LA, trospium IR, trospium ER, SNS, PTNS | Patients with OAB | [42] |
| Observational studies | ||||||
|---|---|---|---|---|---|---|
| Balkrishnan et al. (2006) | Longitudinal cohort | NR | 275 | ACHs | Patients with OAB aged ≥65 years; enrolled in an HMO; treated with ACHs | [43] |
| Campbell et al. (2021) | Retrospective cohort | 2017 | 226,712 | Concurrent use of ≥2 unique ACHs for ≥30 days | Older adults with OAB with Medicare coverage from 2006–2017 | [44] |
| Hall et al. (2001) | Retrospective database analysis | NR | 8661 | Oxybutynin, flavoxate, tolterodine IR, hyoscyamine sulfate, propantheline | Patients aged 18–64 years with OAB diagnosis or ACH claim | [45] |
| Ivanova et al. (2014) | Database analysis | 2012 | 10,318 | ACHs | Patients aged 18–64 years with OAB and ACH claim; enrolled in non-HMO plan | [46] |
| Ju et al. (2014) | Cross-sectional | NA | 516.8 M§ visits; 8.1 M ACH visits | ACHs | Women aged ≥18 years who had an ambulatory visit in 2009 | [47] |
| Jumadilova et al. (2006) | Retrospective cohort | 2003 | 26,386 | Tolterodine ER, oxybutynin ER, oxybutynin IR | Patients with OAB and ACH claim | [48] |
| Kachru et al. (2021) | Retrospective cohort | NA | 18,075 | Nonselective or selective ACHs | Older Medicare patients with OAB and dementia; treated with ACHs after dementia diagnosis | [49] |
| Lozano-Ortega et al. (2021) | Retrospective cohort | 2019 | 154,432 with OAB; 9939 with falls/fractures | ACHs | Patients aged ≥18 years with OAB-related claim | [50] |
| Nitz et al. (2005) | Retrospective database analysis | NR | 14,582 | Oxybutynin IR, oxybutynin ER, tolterodine ER | Patients aged ≥18 years with OAB with OAB-related claim; commercial or Medicare insurance with prescription drug benefit | [51] |
| Pelletier et al. (2009) | Retrospective cohort | 2007 | 86,734 | ACHs, nonpharmacologic management | Patients aged ≥18 years with OAB diagnosis or ACH claim; enrolled in a health plan | [52] |
| Rogula et al. (2019) | Retrospective cohort | 2017 | 154,432 | ACHs | Patients with OAB | [53] |
| Suehs et al. (2016) | Retrospective cohort | 2013 | 46,140 | ACHs | Patients aged 65–89 years with ACH prescription; enrolled in Medicare Advantage prescription drug plan | [54] |
| Suehs et al. (2017) | Retrospective database analysis | NR | 10,220 | ACHs | Patients aged 65–89 years with OAB taking ACHs; Medicare Advantage prescription drug plan | [55] |
| Tang et al. (2014a) | Retrospective cross-sectional | NA | 1730 overall; 411 from the USA | ACHs | Outpatients aged >18 years with OAB treated with ACHs | [56] |
| Tang et al. (2014b) | Retrospective database analysis | NA | 313 overall; 89 from the USA | ACHs | Outpatients aged >18 years with OAB and underlying neurologic conditions treated with ACHs | [57] |
| Varadharajan et al. (2005) | Retrospective cohort | 2004 | 26,386 | Tolterodine ER, oxybutynin ER, oxybutynin IR | Patients with OAB and ACH claim | [58] |
| Walker et al. (2021) | Database analysis | NR | 1548 | ACHs | Patients aged ≥65 years with ACH dispensation | [59] |
| Yehoshua et al. (2016) | Retrospective claims analysis, real-world observational | 2013 | 2480 | ACHs | Patients covered by HealthCare Partners; patients with OAB and UI and ACH claim; patients without OAB or an ACH claim | [60] |
| Zinner et al. (2008) | Prospective open-label trial | NA | 440 | Solifenacin 5 or 10 mg | Ambulatory patients aged ≥18 years with OAB; treated with tolterodine 4 mg/d for ≥4 weeks immediately preceding study entry without sufficient improvement in urgency episodes | [61] |
| Zinner et al. (2009) | Prospective open-label trial | NA | 440 | Tolterodine ER 4 mg/d followed by solifenacin 5/10 mg/d | Patients with OAB aged ≥18 years; treated with tolterodine 4 mg/d for ≥4 weeks immediately preceding study entry without sufficient improvement in urgency episodes | [62] |
†
All treatments analyzed in the study are listed in the table; however, only outcomes relating to anticholinergic medications were extracted. Individual anticholinergic medications are listed for studies that provided this information. In studies that assessed anticholinergic medications collectively, the treatment is described as “ACHs”.
‡
Chen et al. reported a model input based on a personal communication for number of physician visits and reported total cost from a societal perspective, which did not meet the PICOS criteria. Because the study did not meet PICOS criteria and only included model inputs, Chen et al. is included with identified studies, but results are not cited nor discussed in the main text.
§
Ju et al. report conflicting numbers for the total number of outpatient office visits made by women in 2009 between the abstract and full text. The abstract indicates that 516.8 million adult women made outpatient office visits, whereas the full text notes that this is the number of women who had a visit not associated with active use of an anticholinergic medication for OAB. The number from the abstract is provided herein as this value was used for the calculation of the proportion of total outpatients visits where a patient reported active use of an anticholinergic medication.
ACH: Anticholinergic medication; BSC: Best supportive care; CR: Controlled release; ER: Extended release; HMO: Health Maintenance Organization; IR: Immediate release; LA: Long acting; M: Million; NA: Not applicable; NR: Not reported; OAB: Overactive bladder; PICOS: Population, Intervention, Comparator, Outcomes and Study design; PTNS: Percutaneous tibial nerve stimulation; SNS: Sacral nerve stimulation; TD: Transdermal; UI: Urinary incontinence; UUI: Urge urinary incontinence.
Characteristics & quality of included studies
The 34 publications included 33 unique studies; 18 were observational studies, 2 reported results from a single prospective trial and 14 were economic evaluations or economic models. The observational studies were of overall fair to poor quality (scoring ≤19 on the Downs and Black checklist; Supplementary Table 2) and were predominantly retrospective cohort/database analyses assessing HCRU and collective costs of anticholinergic medications, often focusing on comorbidities including dementia and falls/fractures. Eleven studies did not clearly define the interventions of interest; in general, these studies stated that patients had a prescription for an anticholinergic medication without listing the medications included. Most articles did not describe the characteristics of patients lost to follow-up. Studies generally recruited patients from a single population (i.e., from the same database) over the same period of time and adjusted for confounders; common sources of bias included not accounting for compliance or different lengths of follow-up between comparator arms.
The economic studies included cost–effectiveness analyses, cost–minimization analyses, a budget impact model, a decision analytic model and a cost analysis. The studies generally reported on most applicable items on the Drummond and Jefferson checklist (Supplementary Table 3). All studies answered their posed research question and all but 2 articles provided limitations for their conclusions. Articles varied in whether they justified the variables and ranges in sensitivity analyses; some studies did not clearly define the source of model inputs, currency, price date or inflation adjustments. Many of the economic evaluations compared the costs of anticholinergic medications over a period of 3 months to 10 years.
Baseline patient characteristics
Patients were predominantly white (range: 52.4–88.9%) and female (range: 17.8–100%) with differing mean ages (range: 44–74.2 years). Reported geographic locations were predominantly in the midwestern and southern USA. Most studies did not report baseline comorbidities; among the studies that did, the most frequently reported baseline comorbidities were falls/fractures and urinary tract infections (UTIs).
Overview of findings
The included studies primarily reported on HCRU and cost outcomes associated with the use of anticholinergic medications in patients with OAB. HCRU outcomes generally fell into 4 groups: inpatient hospitalizations, outpatient visits, physician visits and emergency department visits. Cost outcomes generally fell into 6 groups: total healthcare costs, inpatient hospitalization costs, outpatient visit costs, physician visit costs, emergency department costs and cost of individual OAB-related conditions (UTI, depression, falls/fractures and skin irritation/infection). The remainder of the review is structured according to these categories.
HCRU
Inpatient hospitalizations
Overall, 11 of the 34 articles reported data on inpatient hospitalizations (Table 3 & Supplementary Table 4). Across all studies, the proportion of patients requiring hospitalization ranged from 0 to 5% for OAB-related hospitalizations [46,56,57] and 9.9 to 49.0% for all-cause hospitalizations [43,46,49,60].
| Study (year) | Outcome† | Ref. | |||
|---|---|---|---|---|---|
| Inpatient hospitalization | Outpatient visits | Physician visits | ED or ICU visits | ||
| Balkrishnan et al. (2006) | Patients with hospitalization (%): ≥1, 23%; ≥2, 24%; ≥3: 28% | ≥1, 1.48; ≥2, 1.25; ≥3, 1.12 | NR | Mean ED visits (n): ≥1, 1.61; ≥2, 1.26; ≥3, 1.61 | [43] |
| Chen et al. (2012) | NR | NR | Model input: mean 5 visits per 3 months | NR | [31] |
| Hall et al. (2001) | 0.2 hospitalizations per patient per month | Tolterodine/oxybutynin/no OAB drug: 0.23/0.21/0.18 visits per patient per month | Tolterodine/oxybutynin/no OAB drug: 1.51/1.26/1.17 visits per patient per month | 0.03 visits per patient per month | [45] |
| Ivanova et al. (2014) | Persisters/switchers/discontinuers with hospitalization (%): All cause, 9.9%/14.9%/14.9%; OAB related, 0.4%/1.0%/0.5% | Persisters/switchers/discontinuers with visit (%): All cause, 95.1%/96.6%/93.4%; OAB related, 29.4%/43.0%/22.2% | NR | Persisters/switchers/discontinuers with ED visit (%): All cause, 15.9%/16.4%/17.6%; OAB related, 0.2%/0.4%/0.3% | [46] |
| Ju et al. (2014) | NR | 1.6% of all patients had an outpatient visit; annual rate of outpatient visits, 6.8% | NR | NR | [47] |
| Jumadilova et al. (2006) | Hospitalizations, n (range): UTI related, 0.01–0.03; depression related, 0.01–0.02; OAB unrelated, 0.19–0.25 | Management visits, n (range): UTI related, 0.16–0.26; depression related, 0.55–0.68; OAB unrelated, 12.25–12.86 | NR | ED visits, n (range): UTI related, 0.04–0.09; depression related, 0.01–0.03; OAB unrelated, 0.91–1.36 | [48] |
| Kachru et al. (2021) | Hospitalization within 6 months of ACH medication use (%): Nonselective, 24.1%; selective, 21.6% | NR | NR | NR | [49] |
| Lozano-Ortega et al. (2021) | Hospitalizations per 100 person-year, n (no-low/medium-high ACB‡; %): Pre-fall/fracture, 17.1%/31.6%; post-fall/fracture, 22.5%/39.8% | Visits, n (no-low/medium-high ACB‡) Total outpatient: Pre-fall/fracture, 22.6/28.5; post-fall/fracture, 27.6/33.6 Other outpatient service: Pre-fall/fracture, 8.1/10; post-fall/fracture, 10.6/12.8 | Visits, n (no-low/medium-high ACB‡) General practitioner: Pre-fall/fracture, 3.6/5; post-fall/fracture, 4.2/5.7 Specialist: Pre-fall/fracture, 11/13.5; post-fall/fracture, 12.7/15.2 | Visits, n (no-low/medium-high ACB‡) ED visits: Pre-fall/fracture, 7.9/15.4; post-fall/fracture, 12.6/22 ICU visits: Pre-fall/fracture, 2.6/5.2; post-fall/fracture, 3.8/7.1 | [50] |
| Perk et al. (2016) | NR | Mean 1.135 outpatient visits per increase in ACB score | NR | 0.114 additional visits/year per increase in ACB score | [37] |
| Tang et al. (2014a) | Patients with OAB-related hospitalizations (%): Continent, 0%; incontinent, 1.4% | NR | OAB-related visits in past 3 months (n): Continent, 1.3; incontinent, 1.2 | NR | [56] |
| Tang et al. (2014b) | Patients with OAB-related hospitalizations (%): Continent, 5%; incontinent, 4.6% | NR | OAB-related visits in past 3 months (n): Continent, 1.3; incontinent, 1.5 | NR | [57] |
| Varadharajan et al. (2005) | Hospitalizations (n): OAB related, 0.01; all other, 0.21–0.29 | Management visits (n): OAB related, 0.46–0.53; all other, 12.99–13.8 | NR | ED visits (n): OAB related, 0.01–0.02; all other, 0.96–1.47 | [58] |
| Walker et al. (2021) | Median 0 hospitalizations/month in each treatment group | NR | NR | NR | [59] |
| Yehoshua et al. (2016) | Patients with hospitalization (%): OAB, 49.0%; no OAB, 37.6% | Patients with visit (%): OAB, 100%; no OAB, 98.7% | NR | ED visits (n): OAB, 1.92; no OAB: 1.41 | [60] |
| Zinner et al. (2008) | NR | NR | Nonprotocol-related visits/12 weeks (n): Prewashout, 1.24; end of study, 0.24 | NR | [61] |
| Zinner et al. (2009) | NR | NR | Nonprotocol-related visits/12 weeks (n): Prewashout/end of study, for aged <65 years, 1.32/0.20; for aged 65–74 years, 1.20/0.25; for aged ≥75 years, 1.07/0.34 | NR | [62] |
†
Reported as per patient per year unless otherwise noted.
‡
ACB is a unitless, cumulative score that considers daily dose of anticholinergic medications, the Anticholinergic Burden Scale and the duration of anticholinergic exposure. No ACB is defined as 0, low is 0–89, medium is 90–499 and high is ≥500 [63].
ACB: Anticholinergic burden; ACH: Anticholinergic medication; ED: Emergency department; ICU: Intensive care unit; NR: Not reported; OAB: Overactive bladder; UTI: Urinary tract infection.
Three studies included a comparator arm with patients who were not treated with anticholinergic medications; however, comparators differed between studies [45,59,60]. A claims analysis by Yehoshua et al. reported that patients who experienced OAB with incontinence (i.e., OAB wet) and received anticholinergic medications experienced significantly more yearly all-cause hospitalizations (0.301) compared with patients without OAB (0.235; p = 0.001) [60]. A claims analysis by Hall et al. reported no differences in monthly hospitalizations in patients receiving tolterodine or oxybutynin versus patients with OAB who did not receive pharmacotherapy [45]. In a 2021 claims analysis by Walker et al., no significant difference in inpatient visits was shown among frail patients with OAB receiving anticholinergic medications or a β3-receptor agonist (both groups had a median of 0 monthly inpatient visits) [59].
The remaining 8 studies did not include nonanticholinergic comparators but instead assessed anticholinergic medication burden [50], medication persistence [46] and anticholinergic medication [48,49,58] or patient [43,56,57] characteristics. Anticholinergic burden was assessed by one study, a claims analysis by Lozano-Ortega et al. [50], which estimated the impact of falls/fractures on HCRU and costs according to levels of anticholinergic burden among individuals with OAB. HCRU and costs were compared before and after a fracture and the anticholinergic burden measure [64] was used to calculate anticholinergic burden as a unitless score, accounting for dose and potency. It showed that medium to high anticholinergic burden (score ≥90 on the cumulative anticholinergic burden measure) was associated with a greater mean number of hospitalizations per 100 person-years than no to low anticholinergic burden (score <90) [50]. Persistence with anticholinergic medications was also assessed by one study, a claims analysis by Ivanova et al., which found that patients with OAB who switched from one anticholinergic medication to another had significantly higher rates of hospitalization in the following 6 months than those who persisted with or discontinued an anticholinergic medication [46].
Three studies assessed hospitalizations according to anticholinergic medication characteristics. A claims analysis by Kachru et al. found that patients using nonselective anticholinergic medications, which have an affinity for muscarinic receptors M1–M5 (oxybutynin, fesoterodine, tolterodine, trospium), experienced a higher all-cause hospitalization rate over the 6 months after initiation than patients using selective anticholinergic medications, which have a high affinity for the M3 muscarinic receptors that are responsible for bladder contraction (solifenacin, darifenacin; 24.14 vs 21.58%, respectively; p = 0.0007) [49]. Jumadilova et al. assessed inpatient hospitalizations, categorized as those related to UTI or depression or unrelated to OAB, among patients with OAB taking tolterodine extended release (ER), oxybutynin ER or oxybutynin immediate release (IR) [48]. It was found that patients taking tolterodine ER experienced fewer yearly UTI-related hospitalizations than patients taking oxybutynin ER or IR, fewer yearly depression-related hospitalizations versus oxybutynin ER but not versus oxybutynin IR and fewer yearly OAB-unrelated hospitalizations versus oxybutynin IR but not versus oxybutynin ER [48]. In contrast, a 2005 claims analysis by Varadharajan et al. found no significant differences in total OAB-related inpatient hospitalizations among patients taking tolterodine ER versus oxybutynin ER or IR [58].
Three studies assessed hospitalizations in patients with OAB taking anticholinergic medications according to patient characteristics. A claims analysis by Balkrishnan et al. found that patients who were enrolled in a Health Maintenance Organization (HMO) health plan for 1 to 3 years and continuously on anticholinergic medications experienced a numeric increase in the rate of hospitalizations over time, with 23, 24 and 28% of patients in years 1, 2 and 3, respectively, having experienced a hospitalization in the previous year [43]. Two analyses by Tang et al. compared hospitalizations between patients with OAB [56] or neurogenic detrusor overactivity [57] with or without incontinence; no significant difference was found in the 12-month rate of OAB-related hospitalizations between patients in the USA with OAB or neurogenic detrusor overactivity, with or without urinary incontinence.
Outpatient visits
Nine studies reported data on outpatient visits, with variation between studies on the type of outpatient visits (i.e., physician visits and emergency department visits). Across all studies, the percentage of patients with ≥1 OAB-related outpatient visit ranged from 20.3 to 100%; however, observation periods varied from 1 month to 1 year. An analysis by Ju et al. used the National Ambulatory Medical Care Survey database to estimate the prevalence of outpatient visits associated with an anticholinergic medication to treat OAB among adult female patients in the USA and found that women actively taking anticholinergic medications for OAB had 8.1 million outpatient visits in 2009, accounting for 1.6% of all outpatient visits in the USA [47].
Two studies included a comparator arm with patients who were not treated with anticholinergic medications; however, comparators differed between studies. Yehoshua et al. reported that patients with OAB wet and receiving an anticholinergic medication had more yearly outpatient visits per patient than those without OAB (16.96 vs 11.25, respectively) [60]. Similarly, Hall et al. reported 0.21 to 0.23 monthly outpatient hospitalizations in patients with OAB taking an anticholinergic medication compared with 0.18 monthly outpatient hospitalizations in patients not receiving any drug treatment for OAB; however, no statistical comparisons were made [45].
The remaining studies did not include nonanticholinergic comparators. They instead stratified by medication persistence [46], anticholinergic medication burden [37,50] and reason for outpatient visit [48,58].
Ivanova et al. was the only study to assess the effect of anticholinergic medication persistence on outpatient visits. Patients with OAB who switched from 1 anticholinergic medication to another had a greater mean number of all-cause and OAB-related outpatient visits in the 6 months following switching than patients who persisted with an anticholinergic medication and had more outpatient visits than patients who discontinued an anticholinergic medication [46].
Two studies assessed the effect of anticholinergic burden on outpatient visits. Lozano-Ortega et al. found that medium to high anticholinergic burden was associated with a greater mean number of outpatient visits per 100 person-years than no to low anticholinergic burden [50]. In the course of developing a budget impact model, Perk et al. [37] performed a retrospective medical record analysis to assess the relationship between the 6-point anticholinergic cognitive burden (ACB) scale score [65] and outpatient visits in adults ≥65 years. Consistent with results from Lozano-Ortega et al., Perk et al. estimated a mean increase of 1.14 annual outpatient visits per unit increase in ACB score.
Two studies reported annual outpatient visits by reason for visit among patients with OAB and an anticholinergic medication claim. Jumadilova et al. found that, depending on the specific anticholinergic agent used, patients had 0.16 to 0.26 outpatient management visits related to UTIs, 0.55 to 0.59 outpatient management visits related to depression and 12.25 to 12.86 outpatient management visits related to non-OAB causes per year [48]. Varadharajan et al. found that patients with OAB and an anticholinergic medication claim had 0.46 to 0.53 outpatient management visits related to OAB and 12.99 to 13.8 outpatient management visits related to other causes per year [58].
Physician visits
Six studies reported data on physician visits; however, only 1 study included a comparator arm with patients who were not treated with an anticholinergic medication. Hall et al. found that patients with OAB and taking anticholinergic medications experienced a numerically greater mean number of physician visits per month than patients with OAB who were not receiving pharmacologic treatment (1.26–1.51 with treatment vs 1.17 without treatment) [45]. A single study assessed the relationship between physician visits and anticholinergic burden; Lozano-Ortega et al. found that patients with OAB with medium to high anticholinergic burden had a greater mean number of general practitioner visits than patients with no to low anticholinergic burden [50]. Two studies by Tang et al. assessed the relationship between continence and physician visits, finding similar numbers of physician visits related to OAB or neurogenic detrusor overactivity in patients with versus without urinary incontinence taking anticholinergic medications [56,57]. Two studies by Zinner et al. assessed the relationship between anticholinergic medication and physician visits, finding that patients in the VESIcare Efficacy and Research Study US (VERSUS) trial had fewer nonprotocol-related office visits after switching from tolterodine to solifenacin [61,62].
Emergency department visits
Eight studies reported data on emergency department visits. Across all studies reporting emergency department visits, 15.9 to 46.9% of anticholinergic-treated patients with OAB required ≥1 emergency department visit per year, with a yearly average of 0.96 to 1.92 emergency department visits per patient. Two studies included a comparator arm with patients with OAB not treated with anticholinergic medications [45,60]; the remainder stratified by anticholinergic burden [37,50], medication persistence [46] and medication [48,58] or patient characteristics [43].
Two studies included a comparator arm of patients not treated with anticholinergic medications, but comparators differed between studies. Yehoshua et al. found that patients with OAB wet taking anticholinergic medications had more annual emergency department visits than those without OAB (1.92 vs 1.41, respectively) [60]. In contrast, Hall et al. found no difference in annual emergency department visits among patients taking tolterodine IR, taking oxybutynin or receiving no pharmacologic treatment (0.03 unadjusted emergency department encounters per patient per month in all groups) [45].
Ivanova et al. was the only study to assess the effect of anticholinergic medication persistence on emergency department visits and reported no differences in OAB-related emergency department visits in the 6 months after switching anticholinergic medications [46].
Two studies assessed the relationship between anticholinergic burden and emergency department visits. Lozano-Ortega et al. reported that patients with OAB and medium to high anticholinergic burden had increased mean emergency department visits compared with those with no to low anticholinergic burden [50]. Similarly, the previously described analysis reported by Perk et al. found that the number of annual emergency department visits increased by 0.114 per unit increase in anticholinergic burden score [37].
The relationship between specific anticholinergic medications and emergency department visits was evaluated in two studies. Jumadilova et al. found that patients receiving tolterodine ER experienced a decrease in frequency of UTI-related emergency department visits and no changes in frequency of depression-related or other OAB-unrelated emergency department visits versus oxybutynin ER or IR [48]. However, Varadharajan et al. found no significant differences between anticholinergic types in OAB-related and non–OAB-related emergency department visits [58].
Balkrishnan et al. assessed the relationship between emergency department visits and patient characteristics. Patients who were enrolled in an HMO health plan for 1 to 3 years and continuously on anticholinergic medications experienced a numeric increase in the rate of emergency department visits over time, with 26, 29 and 30% of patients in years 1, 2 and 3, respectively, having experienced an emergency department visit in the previous year [43].
Healthcare costs
Total healthcare costs
Total cost estimates were reported in 26 of the 34 studies; metrics included total healthcare (23 studies), total medical (10 studies), total pharmacy (13 studies) and OAB-related condition (2 studies) costs (Table 4 & Supplementary Table 5). Some articles compared patients with and without pharmacologically managed OAB [37,45,52,60], whereas others stratified by adherence [35,36,46], anticholinergic burden or potentially inappropriate anticholinergic prescribing [44,50,53,54,64] or type of OAB medication [29,33,34,37,39–42,51,59].
| Study (year) | Outcome† | Ref. | ||||
|---|---|---|---|---|---|---|
| Total healthcare costs | Hospitalization costs | Outpatient visit costs | Physician visit costs | ED and ICU costs | ||
| Arikian et al. (2000) | 6-month per patient total healthcare costs, $1,530; net cost to HMO per patient per month, $0.29–$0.32 | NR | NR | NR | NR | [29] |
| Armstrong et al. (2012) | Mean healthcare cost lowest for oxybutynin IR, $754; range: $952–$1243 for other medications | NR | NR | NR | NR | [30] |
| Balkrishnan et al. (2006) | Total: ≥1, $5692; ≥2, $6099; ≥3, $5447; Lower during year 1 and 3 among patients with high vs low adherence | NR | NR | NR | NR | [43] |
| Campbell et al. (2021) | Total medical: 0 years, $8645; ≥1 year, $9762 | NR | NR | NR | NR | [44] |
| Hall et al. (2001) | Increased medical/pharmacy costs per patient per month for all patients and those receiving OAB drugs vs untreated; at follow-up: medical, $361–$430; pharmacy, $60–$155 | NR | NR | NR | NR | [45] |
| Ivanova et al. (2014) | Increased all-cause and OAB-related medical and pharmacy for all treatment groups; lowest OAB-related medical for persisters and highest for switchers | Higher for switchers (all-cause, $2505; OAB related, $68) vs persisters ($1462; $22) or discontinuers ($1744; $22) | Higher for switchers (all cause: $4063; OAB related: $394) vs persisters ($2972; $116) or discontinuers ($2977; $139) | NR | OAB related, $1–$5; lower all-cause for persisters ($185) and highest for switchers ($229) vs discontinuers ($231) | [46] |
| Ko et al. (2006) | Range per patient per 3 months: $3373–$3769 | NR | NR | NR | NR | [32] |
| Lozano-Ortega et al. (2021) | Higher mean all-cause in patients with higher vs lower ACB‡ ($24,428–$18,930 vs $15,439–$19,463) | Higher in patients with higher vs lower ACB‡ ($6684–$7943 vs $3931–$5343) | Higher in patients with higher vs lower ACB‡ ($11,526–$14,758 vs $8638–$11,079) | NR | NR | [50] |
| Murray et al. (2019) | Lower per 10 years for tolterodine ER ($12,776) vs solifenacin 5 and 10 mg ($13,342 and $13,335) | NR | NR | NR | NR | [33] |
| Murray et al. (2021) | Lower per 10 years for tolterodine ($13,193) vs solifenacin 5 and 10 mg ($14,822 and $14,830) | NR | NR | NR | NR | [34] |
| Nitz et al. (2005) | Increased total medical for all patients; lower for tolterodine ER ($5074); highest for oxybutynin ER ($14,766) | NR | NR | NR | NR | [51] |
| Noe et al. (2002) | Mean total 3-month treatment cost per patient (tolterodine/oxybutynin): $1207/$1283 | NR | NR | No difference in cost per visit ($40 PCP follow-up; $144 specialist follow-up) | NR | [35] |
| Pelletier et al. (2009) | Total: $9917 (healthcare), $2796 (pharmacy) for ACH medications; $9657 (healthcare), $2150 (pharmacy) for no pharmacotherapy | Lower for ACH medications (all cause: $2164; OAB related, $47) vs no pharmacotherapy ($2325; $93) | Lower total ACH medications (OAB unrelated, $4734; OAB related, $176) vs no pharmacotherapy ($4812; $277) | Lower for ACH medications (all cause: $803; OAB related, $42) vs no pharmacotherapy ($892; $70) | OAB related: $1 for ACH medications vs $9 for no pharmacotherapy; all cause: $240 vs $235 | [52] |
| Perfetto et al. (2005) | Similar medical costs regardless of time on therapy, increased pharmacy costs with length of therapy | NR | NR | NR | NR | [36] |
| Perk et al. (2016) | Lowest total pharmacy for oxybutynin ($638), highest for darifenacin ($3405) | NR | $551 (commercial); $595 (Medicare Advantage) | $354–$536 (commercial); $232–$350 (Medicare Advantage) | $166 (commercial); $217 (Medicare Advantage) | [37] |
| Qin et al. (2016) | Costs per cohort for fesoterodine vs no treatment: $92,889,606 vs $100,162,050 (total medical); $7,832,919 vs $0 (total pharmacy) | Lower for fesoterodine ($41,407,439 per cohort/year) vs no treatment ($44,111,891) | Lower for fesoterodine ($15,242,498 per cohort/year) vs no treatment ($17,019,337) | Lower for fesoterodine ($36,239,668 per cohort/year) vs no treatment ($39,030,822) | NR | [38] |
| Rogula et al. (2019) | Lowest for patients with no ACB or fall/fracture, highest with ACB and fall/fracture | NR | NR | NR | NR | [53] |
| Shepherd et al. (2018) | Lower cost per 2 years including/excluding refractory untreated OAB for tolterodine ($6122/$1457) vs solifenacin ($9166/$5108) | NR | NR | NR | NR | [39] |
| St Martin et al. (2020) | Total 10-year healthcare cost per patient: $28,497 | NR | NR | Input cost per appointment: $112 | NR | [40] |
| Suehs et al. (2016) | OAB related (no PIM vs PIM): $83 vs $104 (medical), $478 vs $560 (pharmacy); all-cause: $6515 vs $13,380 (medical), $2415 vs $3888 (pharmacy) | NR | NR | NR | NR | [54] |
| Suehs et al. (2017) | Total medical (2015 vs 2012 Beers Criteria®): $13,555 vs $11,484; pharmacy: $3142 vs $3532 | NR | NR | NR | NR | [55] |
| Varadharajan et al. (2005) | Total: $188–$279 for OAB-related medical, $5575–$8045 for all other medical, $2204–$2791 for total pharmacy | $78–$160 for OAB related, $2328–$3720 for all other | Total outpatient management: $32–$40 for OAB related, $782–$923 for all other; total outpatient/ancillary: $72–$109 for OAB related, $2197–$3076 for all other | NR | OAB related, $1; all other, $98–$137 | [58] |
| Walker et al. (2021) | Median total cost per patient per month: $1197 (healthcare), $255 (pharmacy) | Median cost per patient per month: $0 | Median cost per patient per month: $498 | NR | NR | [59] |
| Wielage et al. (2016) | Similar total 3-year medical costs across treatment groups (commercial, $2416–$2431; Medicare: $2573–$2612); varied pharmacy costs (commercial: $1392–$4077; Medicare: $1239–$3847) | NR | Input cost per patient per 3 years: $214.83 | Input cost per patient per 3 years: $112.38 | Input cost per patient per 3 years: $800.05 | [41] |
| Yehoshua et al. (2016) | Higher for patients with OAB wet receiving ACH medications (healthcare, $7562; pharmacy, $1697) vs without OAB (healthcare, $5293; pharmacy, $1046) | Higher for patients with OAB wet receiving ACH medications ($2239) vs without OAB ($1719) | Higher for patients with OAB wet receiving ACH medications ($2326) vs those without OAB receiving no treatment ($1609) | NR | Higher for patients with OAB wet receiving ACH medications ($330) vs without OAB ($193) | [60] |
| Yehoshua et al. (2018) | Increased total healthcare cost with duration of therapy; higher with tolterodine ($3472) vs oxybutynin ($500) | NR | NR | NR | NR | [42] |
†
Reported as per patient per year unless otherwise noted.
‡
ACB is a unitless, cumulative score that considers daily dose of anticholinergic medications, the Anticholinergic Burden Scale and the duration of anticholinergic exposure. No ACB is defined as 0, low is 0–89, medium is 90–499 and high is ≥500 [63].
ACB: Anticholinergic burden; ACH: Anticholinergic medication; ED: Emergency department; ER: Extended release; HMO: Health Maintenance Organization; ICU: Intensive care unit; IR: Immediate release; NR: Not reported; OAB: Overactive bladder; PCP: Primary care physician; PIM: Potentially inappropriate medication.
An analysis conducted by Yehoshua et al. found that patients with OAB wet treated with anticholinergic medications had higher annual healthcare costs ($7562) than those without OAB ($5293) [60]. In a study by Hall et al., patients with OAB who were treated with tolterodine IR or oxybutynin had higher monthly total healthcare costs ($585–$593) than patients with OAB who received no OAB drug treatment ($420) [45]. A study by Pelletier et al. also compared total healthcare costs between patients with OAB receiving anticholinergic medications and patients who received no OAB drug treatment, reporting costs of $9917 and $9657, respectively [52].
Several studies showed that low adherence or persistence led to higher costs among patients taking anticholinergic medications. Ivanova et al. found that patients who switched anticholinergic medications had higher total adjusted all-cause and OAB-related healthcare costs 6 months after index (all cause: $8806; OAB related: $797) than patients who persisted with the original anticholinergic medication (all cause: $7017; OAB related: $642) [46]. A pharmacoeconomic model by Noe et al. also predicted that patients who continued with either tolterodine ER or oxybutynin ER monotherapy would have lower total healthcare costs ($963 and $1040, respectively) than those who discontinued ($1545 and $1539), switched ($1482 or $1491) or added a new anticholinergic medication ($1668 or $1649) [35].
A cost-minimization analysis by Perfetto et al. showed that annual costs for patients taking tolterodine ER or oxybutynin ER increased with greater persistence ($8714–$8766 for patients who discontinued in the first month vs $9136–$9761 for patients who remained on therapy for a year) [36]. The increase in costs was driven by higher pharmacy costs among patients who persisted versus those who discontinued therapy in the first month ($1192–$1217 vs $99–$101, respectively). However, medical costs were lower over time among patients who persisted than among those who discontinued ($7944–$8544 vs $8615–$8665, respectively) [36].
Potentially inappropriate medication (PIM) use of anticholinergics (according to AGS Beers Criteria) and increased anticholinergic medication burden were associated with increased costs. A study by Lozano-Ortega et al. examined the impact of falls/fractures on HCRU and costs according to the level of cumulative anticholinergic burden. Compared with patients who had medium to high anticholinergic burden, patients with no to low anticholinergic medication burden had lower total annual healthcare costs (before fall/fracture, $15,439 vs $24,428; after fall/fracture, $19,463 vs $28,930) and pharmacy costs (before fall/fracture, $2870 vs $6217; after fall/fracture, $3041 vs $6229) [50]. Two studies by Suehs et al. showed that PIM use of anticholinergic medications increased costs among patients with OAB [54,55]. Patients with PIM use of anticholinergic medications according to the 2012 Beers Criteria had total adjusted all-cause healthcare costs of $12,001 per patient per year compared with $9373 for those with non-PIM use [54]. In a follow-up study comparing the 2012 and 2015 Beers Criteria, the 2015 Criteria identified increased PIM use of anticholinergic medications; however, this was found in a younger population with a lower comorbidity burden, resulting in lower total healthcare costs versus the 2012 Criteria (all-cause total healthcare costs: $16,698 based on 2012 Beers Criteria vs $15,016 based on 2015 Beers Criteria; prevalence of PIM use: 20.6 vs 25.0%, respectively) [55].
Pharmacy costs accounted for most OAB-related costs, whereas medical costs – including outpatient and physician visits, hospitalizations and emergency department or intensive care visits – usually accounted for most total healthcare costs [36,38,54,58]. One exception was from a cost–effectiveness model of mirabegron by Wielage et al., which reported that costs were differentially driven by pharmacy costs or medical costs depending on the type of anticholinergic medication and/or the health plan (commercial or Medicare Advantage) [41].
A budget impact model by Perk et al. reported comorbidity costs for patients receiving anticholinergic medications [37]. The model predicted that comorbidity costs (per patient per year) would be higher for patients who did not receive treatment (commercial: $229.78 for prescriptions, $172.95 for medical fees; Medicare Advantage: $150.19 and $113.04, respectively) than for patients receiving anticholinergic medications (commercial: $69.13 for prescriptions, $60.01 for medical fees; Medicare Advantage, $45.18 and $39.22, respectively) [37].
Several studies assessed the costs of anticholinergic medications relative to other approved treatments for OAB, including botulinumtoxin derivatives [33,34,39,42] and a β3-adrenergic receptor agonist [40,59]. These analyses generally found that anticholinergic medications were not cost-effective compared with other treatments for OAB. One study, a claims analysis by Walker et al., found that frail older adults taking a β3-adrenergic receptor agonist (mirabegron) had higher total costs than patients taking anticholinergic medications, potentially driven by improved adherence [59].
Hospitalization costs
Seven studies reported on the hospitalization costs of patients taking anticholinergic medications for OAB. However, this included 1 abstract, a claims analysis by Walker et al. that did not identify any inpatient visits in their cohort and thus reported median hospitalization costs of $0 [59]. Of the remaining 6 studies, 3 included a comparator arm comprising patients without pharmacologically managed OAB [38,52,60] and 3 stratified by anticholinergic burden [63], medication adherence [46] or medication type [58].
A claims analysis by Yehoshua et al. reported hospitalization costs of patients with OAB wet relative to a matched cohort of patients without OAB, finding that patients with OAB wet who were treated with anticholinergic medications had significantly higher annual hospitalization costs ($2239) than those without OAB ($1719) [60]. A claims analysis by Pelletier et al. found significantly lower hospitalization costs among patients with OAB who received an anticholinergic medication versus those who were not pharmacologically managed [52]. Similarly, an economic impact model by Qin et al. predicted that patients with OAB treated with fesoterodine would have lower 1-year hospitalization costs than untreated patients [38].
Ivanova et al. was the only study to assess the relationship between adherence to anticholinergic medications and hospitalization costs in patients with OAB, reporting that patients who switched anticholinergic medications had higher all-cause ($2505) and OAB-related ($68) hospitalization costs in the 6 months after switching than patients who persisted with an anticholinergic medication (all cause: $1462; OAB related: $22) or discontinued (all cause: $1744; OAB related: $22) [46].
Lozano-Ortega et al. was the only study to assess the relationship between anticholinergic burden and hospitalization costs in patients with OAB. It showed that patients who experienced falls/fractures and had medium to high anticholinergic burden had higher mean hospitalization costs (prefalls/fractures, $6684; post-falls/fractures, $7943) than patients who experienced falls/fractures and had no to low anticholinergic burden (prefalls/fractures, $3931; post-falls/fractures, $5343) [50].
A claims analysis by Varadharajan et al. assessed hospitalization costs in 2 cohorts of patients with OAB receiving tolterodine ER to matched cohorts receiving either oxybutynin ER or oxybutynin IR; OAB-related hospitalization costs ranged from $78 to $160 per patient per year, whereas non–OAB-related hospitalizations ranged from $2328 to $3720 per patient per year [58]. It found no significant differences in OAB-related hospitalization costs when patients received tolterodine ER versus oxybutynin ER or IR; non–OAB-related related hospitalization costs were significantly lower with tolterodine ER versus oxybutynin IR (p = 0.0148) but not versus oxybutynin ER [58].
Outpatient visit costs
Eight studies reported on outpatient visit costs of patients taking anticholinergic medications for OAB. Four studies compared patients with OAB taking anticholinergic medications to patients without pharmacologically managed OAB [37,38,52,60]. The remaining studies focused on anticholinergic burden [50], medication adherence [46] or comparing patients taking different OAB medications [58,59].
A claims analysis by Yehoshua et al. reported outpatient visit costs of patients with OAB wet relative to a matched cohort of patients without OAB, finding that patients with OAB wet who were treated with anticholinergic medications had significantly higher average annual outpatient visit costs ($2326) than those without OAB ($1609) [60]. Pelletier et al. found significantly lower outpatient costs among patients with OAB who were on an anticholinergic medication versus those who were not pharmacologically managed [52]. Similarly, an economic impact model by Qin et al. predicted that patients treated with fesoterodine would have lower 1-year outpatient costs than those with no pharmacologic management [38]. However, a budget impact model by Perk et al. predicted that patients taking anticholinergic medications would have higher anticholinergic medication–related outpatient costs than patients not receiving pharmacologic treatment from both the Medicare Advantage and commercial perspectives, with higher costs for patients on Medicare Advantage versus commercial plans [37].
The claims analysis by Ivanova et al. was the only study to assess the relationship between adherence to anticholinergic medications and hospitalization costs in patients with OAB, reporting that patients who switched anticholinergic medications had higher all-cause and OAB-related outpatient visit costs in the 6 months after switching than patients who persisted with or discontinued an anticholinergic medication [46].
The claims analysis by Lozano-Ortega et al. was the only study to assess the relationship between anticholinergic burden and outpatient visit costs in patients with OAB. It reported that patients with medium to high anticholinergic medication burden who had experienced falls/fractures had higher outpatient visit costs (mean all-cause cost per patient: pre-fall/fracture, $11,526; post-fall/fracture, $14,758) than those with no to low anticholinergic burden (pre-fall/fracture, $8638; post-fall/fracture, $11,079) [50].
The claims analysis by Varadharajan et al. compared mean annual per patient outpatient costs of 2 cohorts of patients receiving tolterodine ER with matched cohorts of patients receiving oxybutynin ER or oxybutynin IR [58]. It reported that patients on tolterodine ER had significantly lower outpatient management costs (OAB related, $33; all other, $782) than patients on oxybutynin ER (OAB related, $40; all other, $829) [58]. There was no significant difference in OAB-related outpatient management costs between patients treated with tolterodine ER ($34) and oxybutynin IR ($32); however, all other outpatient management costs were lower in the tolterodine ER–treated group ($816) than the oxybutynin-treated group ($923) [58]. OAB-related and all other outpatient ancillary costs were lower for tolterodine ER (OAB related, $72; all other, $2197) than oxybutynin ER (OAB related, $109; all other, $2372) and lower in a second tolterodine ER cohort (OAB related, $82; all other, $2558) than for oxybutynin IR (OAB related, $74; all other, $3076) [58].
Two articles compared outpatient visit costs between patients with OAB receiving anticholinergic medications and a β3-adrenergic receptor agonist (mirabegron). A 2021 claims analyses by Walker et al. included patients with OAB who were aged ≥65 years, frail (claims-based frailty index [66] score ≥0.25) and taking either anticholinergic medications or mirabegron [59]. It found that patients taking anticholinergic medications had slightly lower monthly outpatient visit costs than patients taking the β3-adrenergic receptor agonist ($498 vs $549, respectively) [59]. In contrast, the 2016 budget impact model by Perk et al. compared patients with OAB taking anticholinergic medications to patients taking mirabegron and predicted that patients taking anticholinergics would have higher outpatient costs than patients taking mirabegron owing to increased anticholinergic burden–related outpatient visits; the cost of anticholinergic burden related to outpatient visits was estimated at $594.50 (vs $138.90 for mirabegron) for Medicare Advantage and $551.40 (vs $5.58 for mirabegron) for a commercial insurance plan [37].
Physician visit costs
Three articles reported data or model results on physician visit costs of patients taking anticholinergic medications for OAB. The 2009 claims analysis by Pelletier et al. found that annual physician visit costs were lower among patients with OAB who received an anticholinergic medication (OAB related, $42; all other, $803) than among those who were not pharmacologically managed (OAB related, $70; all other, $892) [52]. Similarly, the 2016 economic impact model by Qin et al. predicted that older adult patients with OAB treated with fesoterodine would have lower annual physician visit costs ($36,239,668 for a cohort of 7096 patients) than those with no pharmacologic management ($39,030,822) [38]. The 2016 budget impact model by Perk et al. assumed that differences in physician visit costs between OAB medications would be most influenced by persistence, with lower persistence (and therefore increased medication switching) driving increased physician visits [37]. The lowest annual physician visit costs per patient were predicted in patients treated with mirabegron (commercial, $248.59; Medicare Advantage, $162.48). Among anticholinergic medications fesoterodine had the lowest physician visit costs (commercial, $456.77; Medicare Advantage, $298.54) and trospium had the highest (commercial, $536.10; Medicare Advantage, $350.39) [37].
Emergency department costs
Five articles reported data or model results on the emergency department costs of patients taking anticholinergic medications for OAB. Three articles compared patients with OAB taking anticholinergic medications to patients without pharmacologically managed OAB [37,52,60], whereas other articles assessed medication adherence [46] or compared anticholinergic medications [58].
The 2016 claims analysis by Yehoshua et al. reported that patients with OAB wet who were treated with anticholinergic medications had higher average annual emergency department visit costs ($330) than those without OAB ($193) [60]. Similarly, Pelletier et al. found slightly lower OAB-related emergency department costs among patients with OAB who were on an anticholinergic medication ($1) versus those who were not pharmacologically managed ($9; p < 0.001) [52]. A 2016 budget impact model by Perk et al. predicted that patients with OAB taking anticholinergic medications would have higher anticholinergic medication–related emergency department costs than patients not receiving pharmacologic treatment from both the commercial and Medicare Advantage perspectives (commercial, $166.42 vs $1.17, respectively; Medicare Advantage, $216.77 vs $48.98) [37].
The 2014 claims analysis by Ivanova et al. examined the relationship between persistence with OAB medication and emergency department costs in patients with OAB. All-cause emergency department costs were highest among patients who discontinued an anticholinergic medication ($231), followed by those who switched anticholinergic medications ($229) or who persisted with the original anticholinergic medication ($185) [46].
The 2005 claims analysis by Varadharajan et al. compared mean annual per-patient emergency department costs of 2 cohorts of patients receiving tolterodine ER with matched cohorts of patients receiving oxybutynin ER or oxybutynin IR [58]. In each group, the average cost of emergency department visits was $1 for OAB-related visits; average cost of emergency department visits related to other causes ranged from $98–$137 [58].
Cost of individual OAB-related conditions
Two articles reported data or model results on the costs of OAB-related conditions in patients taking anticholinergic medications. A 2016 economic analysis by Qin et al. predicted that a cohort of 7096 patients who were treated with fesoterodine would have lower 1-year costs than nonpharmacologically managed patients for falls/fractures (fesoterodine, $62,308,176 vs no treatment, $66,983,236), UTIs ($8,759,786 vs $10,763,598) and depression ($31,982,765 vs $36,551,387) [38]. A 2006 model by Ko et al. calculated the average cost of falls/fractures over 3 months for patients taking an anticholinergic medication and found that costs ranged from $3373 with solifenacin to $3769 with oxybutynin IR [32].
Discussion
The objective of this analysis was to determine the healthcare and economic burden associated with use of anticholinergic medications in adults with OAB in the USA. Among the 34 captured articles, relatively few studies included a comparator group of patients with OAB who were not receiving anticholinergic medications. Many articles compared patients with OAB who were managed by different anticholinergic medications or assessed the effects of medication adherence/persistence or anticholinergic medication burden on HCRU and costs.
The observational studies that did include control groups of patients without pharmacologically managed OAB reported mixed results. Findings from retrospective claims analyses showed that anticholinergic use was associated with increases in hospitalizations, emergency department visits, outpatient visits and their associated costs, as well as total healthcare costs, relative to individuals without OAB [60] or with OAB who did not receive pharmacologic therapy [45]. However, one retrospective analysis showed that treatment of OAB with anticholinergic medications was associated with reduced total costs, OAB-related outpatient and inpatient costs and non–OAB-related total outpatient and inpatient costs relative to patients with nonpharmacologically managed OAB [52].
Economic modeling studies that included patients without pharmacologically managed OAB also reported mixed results. A model by Qin et al. predicted that patients with OAB treated with fesoterodine would have lower yearly hospitalization, outpatient visit and physician visit costs, as well as fewer comorbidity-related costs, than patients receiving no pharmacologic management [38]. However, a budget impact model by Perk et al. predicted that anticholinergic burden would drive increased physician, outpatient and emergency visit costs in anticholinergic-treated patients relative to untreated controls [37].
A few studies examined the effects of increasing anticholinergic medication burden on HCRU and costs; these generally found that increased exposure to anticholinergic medications was associated with increased HCRU and costs [50,53]. Similarly, concurrent use of ≥2 anticholinergic medications for ≥1 year was associated with greater rates of falls, fractures, altered mental states and increased annual medical care spending [44]. Furthermore, patients with OAB and potentially inappropriate anticholinergic use (according to 2012 or 2015 Beers Criteria) had increased healthcare, medical and pharmacy costs relative to patients without potentially inappropriate anticholinergic use [54].
A claims analysis found that 88% of patients taking anticholinergic medications discontinue or switch therapies within 12 months [21]. Switching anticholinergic medications [46] and lower adherence to anticholinergic medications [43] were associated with increased HCRU and healthcare costs in patients with OAB, suggesting that low adherence to anticholinergic medications may contribute to healthcare costs in this population. OAB treatments with reduced side effects and improved efficacy may result in improved medication adherence and persistence, leading to reduced HCRU and costs. For example, a systematic literature review has reported that a greater proportion of patients persist with mirabegron for 1 year (range: 32–38%) compared with anticholinergic medications (range: 8–25%) [67].
Anticholinergic medications are the most commonly prescribed OAB treatments in the USA [8–10], despite associations with debilitating and costly adverse outcomes including cognitive impairment and dementia [1,19,68]. Surprisingly, this analysis identified multiple key data gaps in the literature reporting the HCRU and economic burden of anticholinergic medication use in patients with OAB. There are relatively few reports comparing HCRU and healthcare costs between patients with OAB taking anticholinergic medications and those taking other pharmacotherapy (i.e., β3-adrenergic receptor agonists) or untreated controls; in the studies that were available, heterogenous methodologies may have contributed to variable conclusions. No studies specifically compared HCRU or costs associated with OAB-related comorbidities between patients with OAB taking anticholinergic medications and untreated controls; thus, the economic impact of anticholinergic-related comorbidities, particularly cognitive impairment and dementia, remains incompletely understood. Further, well-controlled studies are needed to assess the impact of anticholinergic medications on HCRU and costs associated with OAB, relative to other treatment alternatives.
The observational studies were of poor to fair quality and heterogeneity in study design and outcome definitions made it difficult to directly compare results between studies. Furthermore, comparisons between studies must be made with caution because costs were analyzed over different time periods and reported in various cost years from the perspective of different payors. Only studies in English were included; however, because this analysis focused on burden in the USA, this filter is unlikely to bias results.
Conclusion
Among the articles included in this systematic literature review of the burden of anticholinergic medications for treatment of OAB in the USA, there was high variability in study design, outcome reporting and findings across available studies. Higher anticholinergic medication use or burden, potentially inappropriate anticholinergic use (as defined by Beers Criteria) and low adherence and persistence with anticholinergic medications were associated with increased HCRU and costs. Additional studies assessing the impact of anticholinergic medications on HCRU and costs among patients with OAB in comparison with appropriate control groups are needed and may enable optimization of economic and potentially patient outcomes.
•
Overactive bladder (OAB) is associated with a high healthcare and economic burden.
•
Anticholinergic medications are the most frequently prescribed OAB treatments in the USA; long-term use is associated with dry mouth, constipation, potential for cognitive impairment and increased risk of dementia, and increasing anticholinergic burden is associated with increased risk of falls/fractures, all-cause mortality, major adverse cardiovascular events and clinically relevant drug–drug interactions.
•
A systematic literature review was conducted to identify and summarize the burden associated with anticholinergic medication use in adult patients with OAB in terms of healthcare resource utilization (HCRU) and costs to the payor.
•
MEDLINE, Embase and the Cochrane Database were searched on 28 May 2021 for articles (observational studies, randomized controlled trials and economic evaluations) assessing HCRU and costs associated with use of anticholinergic medications in adult patients with OAB in the USA.
•
3080 articles were identified and 34 met the inclusion criteria including 18 articles reporting observational studies, 2 articles reporting results from a single clinical trial and 14 articles reporting economic evaluations or economic models.
•
The observational studies were of overall fair to poor quality, scoring ≤19 on the Downs and Black checklist; the economic studies generally reported on most applicable items on the Drummond and Jefferson checklist.
•
In general, greater anticholinergic medication use or burden, potentially inappropriate anticholinergic medication use (according to American Geriatrics Society Beers Criteria®) and poor persistence with anticholinergic medications were associated with greater HCRU and costs.
•
Among the 34 captured articles, relatively few included a comparator group of patients with OAB who were not receiving anticholinergic medications, limiting assessment of anticholinergic impact on HCRU and costs.
•
The observational studies that did include control groups of patients without pharmacologically managed OAB reported mixed results.
•
Real-world studies assessing the impact of oral pharmacologic therapy on HCRU and costs among patients with OAB using proper control groups, along with practical provider and patient experience, are needed and may enable optimization of economic and potentially patient outcomes and health equity.
Author contributions
C Duperrouzel, C Martin, A Mendell, M Bourque, A Carrera, A Mack and J Nesheim were involved in the study design. C Duperrouzel, C Martin, A Mendell and M Bourque were responsible for executing the systematic searches and data extraction. All authors were involved in data analysis, contributed to the development and critical revision of the manuscript for intellectual content and approved the final version for submission.
Acknowledgments
The authors thank Joanna Bielecki and Becky Skidmore for their assistance with search strategy development.
Financial & competing interests disclosure
This study was funded by Urovant Sciences (CA, USA). C Duperrouzel, C Martin and A Mendell were employees of EVERSANA™, a paid consultant of Urovant Sciences, at the time the analysis was conducted. M Bourque is an employee of EVERSANA™, a paid consultant of Urovant Sciences. A Carrera is an employee of Urovant Sciences and Duke Health. A Mack was an employee of Urovant Sciences at the time the work was conducted. J Nesheim is an employee of Urovant Sciences. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing and editorial support were provided by Joseph Kruempel, PhD, and Krystina Neuman, PhD, CMPP, of The Curry Rockefeller Group, LLC (NY, USA), and were funded by Urovant Sciences (CA, USA).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary tables.pdf)
- Download
- 367.26 KB
References
1.
Gormley EA, Lightner DJ, Burgio KL et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. American Urological Association, MD, USA (2019).
2.
Coyne KS, Sexton CC, Vats V, Thompson C, Kopp ZS, Milsom I. National community prevalence of overactive bladder in the United States stratified by sex and age. Urology 77(5), 1081–1087 (2011).
3.
Kinsey D, Pretorius S, Glover L, Alexander T. The psychological impact of overactive bladder: a systematic review. J. Health Psychol. 21(1), 69–81 (2016).
4.
Milsom I, Kaplan SA, Coyne KS, Sexton CC, Kopp ZS. Effect of bothersome overactive bladder symptoms on health-related quality of life, anxiety, depression, and treatment seeking in the United States: results from EpiLUTS. Urology 80(1), 90–96 (2012).
5.
Szabo SM, Gooch KL, Walker DR, Johnston KM, Wagg AS. The association between overactive bladder and falls and fractures: a systematic review. Adv. Ther. 35(11), 1831–1841 (2018).
6.
Powell LC, Szabo SM, Walker D, Gooch K. The economic burden of overactive bladder in the United States: a systematic literature review. Neurourol. Urodyn. 37(4), 1241–1249 (2018).
7.
Durden E, Walker D, Gray S, Fowler R, Juneau P, Gooch K. The economic burden of overactive bladder (OAB) and its effects on the costs associated with other chronic, age-related comorbidities in the United States. Neurourol. Urodyn. 37(5), 1641–1649 (2018).
8.
Goldman HB, Anger JT, Esinduy CB et al. Real-world patterns of care for the overactive bladder syndrome in the United States. Urology 87, 64–69 (2016).
9.
Kinlaw AC, Jonsson Funk M, Conover MM, Pate V, Markland AD, Wu JM. Impact of new medications and $4 generic programs on overactive bladder treatment among older adults in the United States, 2000–2015. Med. Care 56(2), 162–170 (2018).
10.
Linder BJ, Gebhart JB, Elliott DS, Van Houten HK, Sangaralingham LR, Habermann EB. National patterns of filled prescriptions and third-line treatment utilization for privately insured women with overactive bladder. Female Pelvic Med. Reconstr. Surg. 27(2), e261–e266 (2021).
11.
Maman K, Aballea S, Nazir J et al. Comparative efficacy and safety of medical treatments for the management of overactive bladder: a systematic literature review and mixed treatment comparison. Eur. Urol. 65(4), 755–765 (2014).
12.
Rai BP, Cody JD, Alhasso A, Stewart L. Anticholinergic drugs versus non-drug active therapies for non-neurogenic overactive bladder syndrome in adults. Cochrane Database Syst. Rev. 12(12), CD003193 (2012).
13.
Coupland CAC, Hill T, Dening T, Morriss R, Moore M, Hippisley-Cox J. Anticholinergic drug exposure and the risk of dementia: a nested case-control study. JAMA Int. Med. 179(8), 1084–1093 (2019).
14.
Gray SL, Anderson ML, Dublin S et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Int. Med. 175(3), 401–407 (2015).
15.
Richardson K, Fox C, Maidment I et al. Anticholinergic drugs and risk of dementia: case-control study. BMJ 361, k1315 (2018).
16.
Risacher SL, McDonald BC, Tallman EF et al. Association between anticholinergic medication use and cognition, brain metabolism, and brain atrophy in cognitively normal older adults. JAMA Neurol. 73(6), 721–732 (2016).
17.
Wang YC, Chen YL, Huang CC et al. Cumulative use of therapeutic bladder anticholinergics and the risk of dementia in patients with lower urinary tract symptoms: a nationwide 12-year cohort study. BMC Geriatr. 19(1), 380 (2019).
18.
Hanlon P, Quinn TJ, Gallacher KI et al. Assessing risks of polypharmacy involving medications with anticholinergic properties. Ann. Fam. Med. 18(2), 148–155 (2020).
19.
Dmochowski RR, Thai S, Iglay K et al. Increased risk of incident dementia following use of anticholinergic agents: a systematic literature review and meta-analysis. Neurourol. Urodyn. 40(1), 28–37 (2021).
20.
American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 67(4), 674–694 (2019).
21.
Sussman D, Yehoshua A, Kowalski J et al. Adherence and persistence of mirabegron and anticholinergic therapies in patients with overactive bladder: a real-world claims data analysis. Int. J. Clin. Pract. 71(3–4), (2017).
22.
Benner JS, Nichol MB, Rovner ES et al. Patient-reported reasons for discontinuing overactive bladder medication. BJU Int. 105(9), 1276–1282 (2010).
23.
Pindoria N, Malde S, Nowers J, Taylor C, Kelleher C, Sahai A. Persistence with mirabegron therapy for overactive bladder: a real life experience. Neurourol. Urodyn. 36(2), 404–408 (2017).
24.
Higgins JPT, Thomas J, Chandler Jet al. et al. (Eds). Cochrane handbook for systematic reviews of interventions version 5.1.0. John Wiley & Sons, Chichester, UK (2011).
25.
Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
26.
Booth A, Clarke M, Ghersi D, Moher D, Petticrew M, Stewart L. An international registry of systematic-review protocols. Lancet 377(9760), 108–109 (2011).
27.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 52(6), 377–384 (1998).
28.
Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ Economic Evaluation Working Party. BMJ 313(7052), 275–283 (1996).
29.
Arikian SR, Casciano J, Doyle JJ, Tarride JE, Casciano RN. A pharmacoeconomic evaluation of two new products for the treatment of overactive bladder. Manag. Care Interface 13(2), 88–94 (2000).
30.
Armstrong EP, Malone DC, Bui CN. Cost-effectiveness analysis of anti-muscarinic agents for the treatment of overactive bladder. J. Med. Econ. 15(Suppl. 1), 35–44 (2012).
31.
Chen HW, Bercik RS, Werner EF, Thung SF. Cost-effectiveness of percutaneous tibial nerve stimulation versus extended release tolterodine for overactive bladder. Int. Urogynecol. J. 187(1), 178–184 (2012).
32.
Ko Y, Malone DC, Armstrong EP. Pharmacoeconomic evaluation of antimuscarinic agents for the treatment of overactive bladder. Pharmacotherapy 26(12), 1694–1702 (2006).
33.
Murray B, Hessami SH, Gultyaev D et al. Cost-effectiveness of overactive bladder treatments: from the US payer perspective. J. Comp. Eff. Res. 8(1), 61–71 (2019).
34.
Murray B, Miles-Thomas J, Sussman D et al. Botox, nerve stimulation devices, mirabegron, and anticholinergics versus best supportive care for overactive bladder: an updated US cost-effectiveness analysis. Neurourol. Urodyn. 40, S157–S157 (2021).
35.
Noe L, Becker R, Williamson T, Chen D. A pharmacoeconomic model comparing two long-acting treatments for overactive bladder. J. Manag. Care Pharm. 8(5), 343–352 (2002).
36.
Perfetto EM, Subedi P, Jumadilova Z. Treatment of overactive bladder: a model comparing extended-release formulations of tolterodine and oxybutynin. Am. J. Manag. Care 11(Suppl. 4), S150–S157 (2005).
37.
Perk S, Wielage RC, Campbell NL et al. Estimated budget impact of increased use of mirabegron, a novel treatment for overactive bladder. J. Manag. Care Spec. Pharm. 22(9), 1072–1084 (2016).
38.
Qin L, Luo X, Zou KH, Snedecor SJ. Economic impact of using fesoterodine for the treatment of overactive bladder with urge urinary incontinence in a vulnerable elderly population in the United States. J. Med. Econ. 19(3), 229–235 (2016).
39.
Shepherd JP, Carter-Brooks CM, Chermanksy C. A cost-effectiveness analysis of onabotulinumtoxin A as first-line treatment for overactive bladder. Int. Urogynecol. J. 29(8), 1213–1219 (2018).
40.
St Martin BS, Wallace SL, Lee K, Park A, Sokol ER. Cost-effectiveness analysis of mirabegron vs. anticholinergic for initial medical therapy of overactive bladder accounting for risk of dementia. Female Pelvic Med. Reconstr. Surg. 26(10 Suppl. 1), S22–S23 (2020).
41.
Wielage RC, Perk S, Campbell NL et al. Mirabegron for the treatment of overactive bladder: Cost-effectiveness from US commercial health-plan and Medicare Advantage perspectives. J. Med. Econ. 19(12), 1135–1143 (2016).
42.
Yehoshua A, Murray BP, Vasavada SP, Sand PK. Comparing direct medical costs of onabotulinumtoxinA with other common overactive bladder interventions. Am. J. Pharm. Benefits. 10(1), 11–17 (2018).
43.
Balkrishnan R, Bhosle MJ, Camacho FT, Anderson RT. Predictors of medication adherence and associated health care costs in an older population with overactive bladder syndrome: a longitudinal cohort study. J. Urol. 175(3 Pt 1), 1067–1071; discussion 1071–1072 (2006).
44.
Campbell N, Shiozawa A, Epstein A, Walker D, Lockefeer A, Hines L. A retrospective study of the prevalence of anticholinergic poly-pharmacy use and its associated outcomes among Medicare patients with overactive bladder. J. Am. Geriatr. Soc. 69, S139–S139 (2021).
45.
Hall JA, Nelson MA, Meyer JW, Williamson T, Wagner S. Costs and resources associated with the treatment of overactive bladder using retrospective medical care claims data. Manag. Care Interface 14(8), 69–75 (2001).
46.
Ivanova JI, Hayes-Larson E, Sorg RA, Birnbaum HG, Berner T. Healthcare resource use and costs of privately insured patients who switch, discontinue, or persist on anti-muscarinic therapy for overactive bladder. J. Med. Econ. 17(10), 741–750 (2014).
47.
Ju R, Garrett J, Wu JM. Anticholinergic medication use for female overactive bladder in the ambulatory setting in the United States. Int. Urogynecol. J. 25(4), 479–484 (2014).
48.
Jumadilova Z, Varadharajan S, Girase P, Ollendorf DA. Retrospective evaluation of outcomes in patients with overactive bladder receiving tolterodine versus oxybutynin. Am. J. Health Syst. Pharm. 63(23), 2357–2364 (2006).
49.
Kachru N, Holmes HM, Johnson ML, Chen H, Aparasu RR. Comparative risk of adverse outcomes associated with nonselective and selective antimuscarinic medications in older adults with dementia and overactive bladder. Int. J. Geriatr. Psychiatry 36(5), 684–696 (2021).
50.
Lozano-Ortega G, Schermer CR, Walker DR et al. Fall/fracture-related healthcare costs and their association with cumulative anticholinergic burden in people with overactive bladder. Pharmacoecon. Open 5(1), 45–55 (2021).
51.
Nitz NM, Jumadilova Z, Darkow T, Frytak JR, Bavendam T. Medical costs after initiation of drug treatment for overactive bladder: effects of selection bias on cost estimates. Am. J. Manag. Care. 11(Suppl. 4), S130–S139 (2005).
52.
Pelletier EM, Vats V, Clemens JQ. Pharmacotherapy adherence and costs versus nonpharmacologic management in overactive bladder. Am. J. Manag. Care. 15(Suppl. 4), S108–S114 (2009).
53.
Rogula B, Lozano-Ortega G, Gooch K et al. Falls or fractures and anticholinergic burden are associated with higher annual all-cause healthcare costs among those with overactive bladder. Neurourol. Urodyn. 38, S110–S110 (2019).
54.
Suehs BT, Davis C, Franks B et al. Effect of potentially inappropriate use of antimuscarinic medications on healthcare use and cost in individuals with overactive bladder. J. Am. Geriatr. Soc. 64(4), 779–787 (2016).
55.
Suehs BT, Davis C, Ng DB, Gooch K. Impact of 2015 update to the Beers Criteria on estimates of prevalence and costs associated with potentially inappropriate use of antimuscarinics for overactive bladder. Drugs Aging 34(7), 535–543 (2017).
56.
Tang DH, Colayco DC, Khalaf KM et al. Impact of urinary incontinence on healthcare resource utilization, health-related quality of life and productivity in patients with overactive bladder. BJU Int. 113(3), 484–491 (2014a).
57.
Tang DH, Colayco D, Piercy J, Patel V, Globe D, Chancellor MB. Impact of urinary incontinence on health-related quality of life, daily activities, and healthcare resource utilization in patients with neurogenic detrusor overactivity. BMC Neurol. 14, 74 (2014b).
58.
Varadharajan S, Jumadilova Z, Girase P, Ollendorf DA. Economic impact of extended-release tolterodine versus immediate- and extended-release oxybutynin among commercially insured persons with overactive bladder. Am. J. Manag. Care. 11(Suppl. 4), S140–S149 (2005).
59.
Walker D, Johnson T, Kimura T et al. Cost and resource utilization in frail patients with overactive bladder treated with mirabegron or an antimuscarinic. J. Am. Geriatr. Soc. 69, S140–S140 (2021).
60.
Yehoshua A, Chancellor M, Vasavada S et al. Health resource utilization and cost for patients with incontinent overactive bladder treated with anticholinergics. J. Manag. Care Spec. Pharm. 22(4), 406–413 (2016).
61.
Zinner N, Noe L, Rasouliyan L, Marshall T, Seifeldin R. Impact of solifenacin on resource utilization, work productivity and health utility in overactive bladder patients switching from tolterodine ER. Curr. Med. Res. Opin. 24(6), 1583–1591 (2008).
62.
Zinner N, Noe L, Rasouliyan L, Marshall T, Runken MC, Seifeldin R. Impact of solifenacin on quality of life, medical care use, work productivity, and health utility in the elderly: an exploratory subgroup analysis. Am. J. Geriatr. Pharmacother. 7(6), 373–382 (2009).
63.
Lozano-Ortega G, Walker DR, Johnston K et al. Comparative safety and efficacy of treatments for overactive bladder among older adults: a network meta-analysis. Drugs Aging 37(11), 801–816 (2020).
64.
Szabo SM, Gooch K, Schermer C et al. Association between cumulative anticholinergic burden and falls and fractures in patients with overactive bladder: US-based retrospective cohort study. BMJ Open 9(5), e026391 (2019).
65.
Campbell N, Maidment I, Fox C, Khan B, Boustani M. The 2012 update to the anticholinergic cognitive burden scale. J. Am. Geriatr. Soc. 61(S1), S142–S143 (2013).
66.
Kim DH, Schneeweiss S, Glynn RJ, Lipsitz LA, Rockwood K, Avorn J. Measuring frailty in Medicare data: development and validation of a claims-based frailty index. J. Gerontol. A Biol. Sci. Med. Sci. 73(7), 980–987 (2018).
67.
Yeowell G, Smith P, Nazir J, Hakimi Z, Siddiqui E, Fatoye F. Real-world persistence and adherence to oral antimuscarinics and mirabegron in patients with overactive bladder (OAB): a systematic literature review. BMJ Open 8(11), e021889 (2018).
68.
Alzheimer's Association. 2019 Alzheimer's disease facts and figures. Alzheimers Dement. 15(3), 321–387 (2019).
Information & Authors
Information
Published In
Pages: 1375 - 1394
PubMed: 36354285
Copyright
© 2022 Urovant Sciences. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 September 2022
Accepted: 12 September 2022
Published online: 10 November 2022
Keywords:
Authors
Funding Information
Urovant Sciences
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Healthcare and economic burden of anticholinergic use in adults with overactive bladder: a systematic literature review. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0160
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Kwanghee Jun, Hee-Jae Lee, Young-Mi Ah, Anticholinergic Burden in Aging Populations: Measurement Tools, Clinical Impact, and Implications for Practice, Drug Targets and Therapeutics, 10.58502/DTT.26.0004, 5, 1, (89-98), (2026).
- Jennifer M. Wu, Nazema Y. Siddiqui, Tim Wiltshire, Deepak Voora, Kenneth Schmader, Can Pharmacogenetics Be Used to Predict the Response to Fesoterodine Fumarate?, Urogynecology, 10.1097/SPV.0000000000001668, 32, 1, (27-33), (2026).
- Holly E Richter, Benjamin Chastek, Adam Carrera, Christina Steiger, Daniel Snyder, Laleh Abedinzadeh, Tim Bancroft, Jeffrey Nesheim, Roger R Dmochowski, Adonis K Hijaz, Jeffrey Frankel, Health outcomes and costs in patients prescribed anticholinergic medications for overactive bladder, Journal of Comparative Effectiveness Research, 10.57264/cer-2025-0054, 15, 1, (2025).
- Pornkamol Tiranaprakij, Sahaphume Srisuma, Krongtong Putthipokin, Sirasa Ruangritchankul, Anticholinergic burden and clinical outcomes among older adults admitted in a tertiary hospital: a prospective cohort study, PLOS One, 10.1371/journal.pone.0332946, 20, 9, (e0332946), (2025).
- Mohamed Abdel-Fattah, Christopher Chapple, Suzanne Breeman, David Cooper, Helen Bell-Gorrod, Preksha Kuppanda, Karen Guerrero, Simon Dixon, Nikki Cotterill, Karen Ward, Hashim Hashim, Ash Monga, Karen Brown, Marcus Drake, Andrew Gammie, Alyaa Mostafa, Rebecca Bruce, Victoria Bell, Christine Kennedy, Suzanne Evans, Graeme MacLennan, John Norrie, Invasive urodynamic investigations in the management of women with refractory overactive bladder symptoms: FUTURE, a superiority RCT and economic evaluation, Health Technology Assessment, 10.3310/UKYW4923, (1-139), (2025).
- Baitong Chen, Jiongming Wang, Yueting Huang, Nanhui Chen, Triglyceride-glucose index and overactive bladder syndrome: evidence from the NHANES 2005-2018, Frontiers in Endocrinology, 10.3389/fendo.2025.1610140, 16, (2025).
- Zhipeng Zhang, Deyi Luo, Zhong Chen, Peng Zhang, Ganping Zhong, Keji Xie, Zhuoqun Xu, Xudong Li, Jianye Wang, Yingfan Yang, Farid Abdul Hadi, Arianne Schild, An open-label, randomized, post-authorization study of mirabegron in Chinese participants with overactive bladder, Asian Journal of Urology, 10.1016/j.ajur.2024.04.007, 12, 1, (79-86), (2025).
- Musab M. Alghamdi, Kwang Jin Ko, Kyu-Sung Lee, An update on the cognitive safety of antimuscarinics in the treatment of overactive bladder, Expert Opinion on Drug Safety, 10.1080/14740338.2024.2392000, 23, 10, (1227-1236), (2024).
- Shaoming Huang, Chuan Guo, Shengcheng Tai, Hongxiang Ding, Dikai Mao, Jiaguo Huang, Biao Qian, Prevalence of overactive bladder in Chinese women: A systematic review and meta-analysis, PLOS ONE, 10.1371/journal.pone.0290396, 18, 12, (e0290396), (2023).
- A. Lenore Ackerman, Penny-wise but Pound-foolish: The Hidden Costs of Step Therapy for Overactive Bladder, Journal of Urology, 10.1097/JU.0000000000003430, 209, 6, (1045-1047), (2023).