Cost–effectiveness of overactive bladder treatments from a US commercial and payer perspective
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The cost–effectiveness of treatment options (anticholinergics, β3-adrenoceptor agonists, onabotulinumtoxinA, sacral nerve stimulation and percutaneous tibial stimulation [the latter two including new rechargeable neurostimulators]) for the management of overactive bladder (OAB) were compared with best supportive care (BSC) using a previously published Markov model. Materials & methods: Cost–effectiveness was evaluated over a 15-year time horizon, and sensitivity analyses were performed using 2- and 5-year horizons. Discontinuation rates, resource utilization, and costs were derived from published sources. Results: Using Medicare and commercial costs over a 15-year time period, onabotulinumtoxinA 100U had incremental cost–effectiveness ratios (ICERs) gained of $39,591/quality-adjusted life-year (QALY) and $42,255/QALY, respectively, versus BSC, which were the lowest ICERs of all assessed treatments. The sensitivity analyses at 2- and 5-year horizons also showed onabotulinumtoxinA to be the most cost-effective of all assessed treatments versus BSC. Conclusion: OnabotulinumtoxinA 100U is currently the most cost-effective treatment for OAB.
Overactive bladder (OAB) is a chronic disorder characterized by urinary urgency, increased urinary frequency and nocturia, which may be accompanied by urgency urinary incontinence [1,2]. The overall prevalence of OAB is similar between men (16.0%) and women (16.9%), and it increases with age [3]. Given the prevalence and chronic nature of OAB, the costs associated with OAB are considerable, with an estimated cost of US $82.6 billion in 2020 [4]. Patients with OAB may receive initial treatment with behavioral therapy including dietary modifications, pelvic floor exercises and supportive care (e.g., incontinence pads); however, treatment often progresses to pharmacotherapy [5–7]. OAB patients treated with oral anticholinergics often cycle through multiple therapies without adequate symptom relief [8], further exacerbating healthcare expenditures and reducing patient health-related quality of life [9]. With only 5–47% of patients with OAB persisting on anticholinergics at 1 year, patients who are inadequately treated with anticholinergics represent a considerable challenge in the management of OAB [10]. Alternative treatment options for these patients include β3-adrenoceptor agonists, intradetrusor onabotulinumtoxinA, implantable sacral nerve stimulation (SNS) and percutaneous tibial nerve stimulation (PTNS) [5,6].
In order to compare the value of OAB treatments within the USA, a Markov model was developed in 2016 to estimate the cost–effectiveness of anticholinergics (solifenacin and tolterodine), mirabegron, onabotulinumtoxinA 100U (BOTOX®, Allergan, an AbbVie company, CA, USA), SNS (InterStim™; Medtronic plc, MN, USA) and PTNS (Urgent® PC; Laborie Medical Technologies, MA, USA), versus best supportive care (BSC) [11]. Treatment with onabotulinumtoxinA produced the largest gain in quality-adjusted life-years (QALYs; 7.179) and the lowest estimated incremental cost–effectiveness ratio (ICER; $32,680/QALY) of all assessed treatments compared with BSC. Thus, onabotulinumtoxinA was found to be the most cost-effective treatment option for patients with OAB. Since the publication of this original cost–effectiveness model, there have been recent additions to the OAB therapeutic landscape. These include a new β3-adrenoceptor agonist, vibegron 75 mg (Gemtesa®; Urovant Sciences, Inc., CA, USA) [12], that received US FDA approval in December 2020. Furthermore, new rechargeable neurostimulators recently emerged, including an SNS device from Axonics (r-SNM®; Axonics Modulation Technologies, CA, USA) [13] and InterStim™ Micro (Medtronic plc, MN, USA). The InterStim Micro neurostimulator is 50% smaller than Axonics r-SNM system, and it shares the same proposed life expectancy of 15 years [14]. InterStim™ II, a nonrechargeable system with a life expectancy of 5–7 years [15], was also introduced since publication of the original model. Finally, Protect PNS™ (Uro Medical Inc, FL, USA) is a new, wireless tibial neuromodulation device currently under investigation.
Given the potential implications of these new treatments in the management of OAB in clinical practice, we conducted an updated assessment of the cost–effectiveness of currently available treatment options (anticholinergics, mirabegron, vibegron, intradetrusor onabotulinumtoxinA, SNS [r-SNM, InterStim II, InterStim Micro] and PTNS [Urgent® PC, Protect PNS]) versus BSC.
Materials & methods
Model structure
The structure of the Markov model used in this cost–effectiveness analysis has been previously published [11] (Figure 1). The model is composed of five health states (i.e., 0 urinary incontinence episodes [UIEs]/day, >0 and ≤2 UIEs/day, >2 and <5 UIEs/day, ≥5 UIEs/day, and dead [acts as an absorbing state that cannot be exited]). The duration of the model cycle was set at 3 months, with the base case employing a 15-year time horizon with an annual discount rate of 3% from a Medicare payer perspective. The base-case analyses were evaluated over a 15-year time horizon to allow a valid comparison with InterStim Micro and Axonics r-SNM, with sensitivity analyses at 2 and 5 years. Cost–effectiveness was assessed from a Medicare perspective (as in the previous model) and a commercial perspective (inflated costs based on the Medicare Payment Advisory Commission report [16]). The primary changes to the original Markov model are summarized in Table 1.

Figure 1. Model diagram and health states.
At baseline and at the end of model cycle 1 (week 12), patients are distributed across health states 1–4 as observed from the pooled onabotulinumtoxinA 100U trial patient level. Patients receive either best supportive care (BSC) or whichever comparator is selected. Patients assigned to BSC remain on this treatment for the duration of the model. Patients assigned to the selected comparator remain on that treatment if they respond; if they do not respond, they revert to BSC for the duration of the model.
Figure is reprinted with permission from Murray et al. (2019) [11].
UIE: Urinary incontinence episode.
| Base-case parameters | Original model | Updated model |
|---|---|---|
| Population | US adults with OAB who were not adequately managed with anticholinergics | US adults with OAB who were not adequately managed with anticholinergics |
| Comparators | Best supportive care | Anticholinergic |
| Anticholinergic | – Solifenacin 5 mg and 10 mg | |
| – Solifenacin 5 mg and 10 mg | – Tolterodine ER 4 mg | |
| – Tolterodine ER 4 mg | – Branded + generic | |
| Mirabegron 25 mg and 50 mg | Generic only | |
| OnabotulinumtoxinA 100U | Best supportive care | |
| SNS InterStim (Medtronic) | Mirabegron: 25 mg and 50 mg | |
| PTNS, urgent PC | Vibegron 75 mg | |
| OnabotulinumtoxinA 100U | ||
| SNS, InterStim II (Medtronic) | ||
| SNS, InterStim Micro (Medtronic) | ||
| SNS (Axonics) | ||
| PTNS, Urgent PC | ||
| PTNS, Protect PNS | ||
| Time horizon | 10-year horizon | 15-year horizon, and sensitivity for 2- and 5-year horizons |
| Perspective | Medicare | Medicare or commercial† |
| Cost inputs | Medical and pharmacy costs (2016) | Medical and pharmacy costs (2020) |
| Outcomes | Total cost | Total cost |
| Quality-adjusted life-years | Quality-adjusted life-years | |
| Cost per urinary incontinence episodes avoided | Cost per urinary incontinence episodes avoided | |
| Incremental cost–effectiveness ratio | Incremental cost–effectiveness ratio |
†
Commercial costs are inflated based on Medicare Payment Advisory Commission report [16].
ER: Extended release; OAB: Overactive bladder; PTNS: Percutaneous tibial nerve stimulation; SNS: Sacral nerve stimulation.
Model comparators & BSC
Based on a 3-month treatment cycle, the model evaluated anticholinergics (solifenacin 5 or 10 mg, tolterodine extended release [ER], generic anticholinergics, generic and branded anticholinergics), mirabegron 25 or 50 mg, vibegron 75 mg, onabotulinumtoxinA 100U, SNS devices (Medtronic InterStim II, InterStim Micro, Axonics r-SNM system), and PTNS (Urgent PC, Protect PNS), compared with a BSC reference therapy that entailed behavioral therapy and urinary incontinence pads. New assumptions to the model included the removal of anticholinergic use from the BSC arm to better reflect clinical practice based on expert opinion. Patients assigned to a treatment option remained on that treatment if they responded (i.e., ≥50% reduction in UIEs), and nonresponders reverted to BSC for the duration of the model. For treatments included in the original model, the proportions of patients in cycle 1 remained the same as previously [11], and assumptions for the newer treatments are in Supplementary Table 1. For vibegron, the proportion of patients was assumed to be the same as for mirabegron across the different health states, and the proportion of patients for oral anticholinergics was assumed to be the same as that for solifenacin 10 mg. Transition probabilities remained the same as in the previous model [11].
Data sources, assumptions & inputs
QALYs were calculated from efficacy, discontinuation rate and utility sources. Efficacy data for the oral pharmacotherapies (anticholinergics and β3-adrenoceptor agonists) were derived from a published network meta-analysis [17]. Efficacy and utilities for generic only and branded and generic anticholinergic medications were assumed to be the same as for solifenacin (highest efficacy) while vibegron was assumed to be similar to mirabegron 50 mg based on current published clinical trial data. Discontinuation rates for oral pharmacotherapies were also derived from the same previously published network meta-analysis [18]. Efficacy and discontinuation data for onabotulinumtoxinA were based on the two pivotal phase III clinical trials [19,20] and a long-term extension study of these trials [21]. Efficacy and safety inputs for SNS devices were based on published clinical trial data [14,22–25]. InterStim II and InterStim Micro were assumed to be identical and based on the latest published InterStim trial data [22,23,26]. Similarly, PTNS efficacy inputs were based on their trial data [27–30]. A 60-month duration for PTNS therapy was based on a National Institute for Health and Clinical Excellence recommendation that PTNS be used for medium-term duration due to lack of longer-term data [31,32]. Utility values were derived by mapping I-QOL scores to the EQ-5D using a pre-existing algorithm [33].
Resource and pharmacy costs were included as previously described [11] but were updated to reflect 2020 costs [16,34]. The updated costs for this model from a Medicare and commercial perspective are summarized in Table 2. Resource utilization and cost data were derived from the same published sources in the original model [27–29,33,35–38] plus recent sources to account for updated medical and pharmacy costs for 2020 [34,39,40], costs and battery life duration for the rechargeable SNS devices [13], and costs for Protect PNS [30]. Costs for the Medtronic InterStim II and InterStim Micro and Axonics r-SNM system were assumed to be the same, using the cost for the implant procedure [41]. In terms of cost assumptions, anticholinergic prices were calculated as the wholesale acquisition price minus 15%, and costs for ‘brand and generic’ and ‘generic only’ arms were based on weighted market share. Finally, in contrast to the original model, which included the cost of battery replacement at the end of the last year of device life expectancy, the new model included the cost of battery replacement at the beginning of the year following the end of device life expectancy.
| Parameter | Original model Medicare | Updated model | |
|---|---|---|---|
| Medicare | Commercial | ||
| Population and devices | |||
| Age at baseline, years | 60.4 | 60.4 | 60.4 |
| Device life expectancy nonrechargeable SNS (Medtronic InterStim I or InterStim II) | 7 [InterStim I] | 4.4 [InterStim II] | 4.4 [InterStim II] |
| Device life expectancy rechargeable SNS (Axonics r-SNM, InterStim Micro) | – | 15 | 15 |
| BSC inputs | |||
|---|---|---|---|
| Cost of incontinence pads | Based on UIE rates | Based on UIE rates | Based on UIE rates |
| Patients on anticholinergics | 23.9% | 0% | 0% |
| Oral drug monthly cost inputs | |||
|---|---|---|---|
| Tolterodine ER 4 mg | $208 | $335.82 | $335.82 |
| Solifenacin 5 and 10 mg | $274 | $262.60 | $262.60 |
| Average, brand and generic anticholinergics | $211 | $188.41 | $188.41 |
| Average, generic anticholinergics only | $211 | $100.05 | $100.05 |
| Mirabegron 25 and 50 mg | $282 | $431.74 | $431.74 |
| Vibegron 75 mg | – | $474.39 | $474.39 |
| OnabotulinumtoxinA inputs | |||
|---|---|---|---|
| Per injection cost | $591 | $643 | $613 |
| Administration, ambulatory clinic or physician office | $311 | $398 | $486 |
| Administration, ambulatory surgery | $1605 | $968 | $1181 |
| SNS inputs | |||
|---|---|---|---|
| Cost of testing prior to SNS (PNE + stage 1)† | $11,080 | $10,398 | $12,686 |
| Cost of testing prior to SNS (PNE)† | $3692 | $4883 | $5957 |
| Cost of testing prior to SNS (stage 1)† | $6980 | $5515 | $6729 |
| Cost of the permanent implant | $16,336 | $18,194 | $22,197 |
| Physician visits for device programming | 2 per year | 2 per year | 2 per year |
| Cost of additional physician visits for reprogramming | $220 | $58 | $70 |
| Cost of battery replacement | $16,336 | $18,194 | $22,197 |
| Cost of revision without replacement | $1091 | $1981 | $2416 |
| Cost of device explantation | $16,336 | $18,194 | $22,197 |
| Patients with success‡ in OAB reduction | 80% [Medtronic] | 80% [Medtronic] 90% [Axonics] | 80% [Medtronic] 90% [Axonics] |
| Patients with device-related adverse events | 25% [Medtronic] | 30% [Medtronic] 16.2% [Axonics] | 30% [Medtronic] 16.2% [Axonics] |
| Patients on SNS receiving revision at 12 months | 7.9% [Medtronic] | 7.9% [Medtronic] 1% [Axonics] | 7.9% [Medtronic] 1% [Axonics] |
| Patients on SNS with device explantation at 12 months | 5% [Medtronic] | 5% [Medtronic] 3.7% [Axonics] | 5% [Medtronic] 3.7% [Axonics] |
| PTNS inputs | |||
|---|---|---|---|
| Time (months) on PTNS procedure - PTNS | 60 | 60 | 60 |
| Probability of success at 3 months - PTNS | 54.5% | 54.5% | 54.5% |
| Weekly cost of treatment (0–3 months) | $1483 | $1566 | $1911 |
| Monthly cost of treatment (3–6 months) | $618 | $653 | $796 |
| Monthly cost of treatment (>6 months) | $371 | $392 | $478 |
| Time (month) on PTNS procedure, Protect PNS | – | 60 | 60 |
| Probability of success at 3 months, Protect PNS | – | 73.3% | 73.3% |
| Cost of Protect PNS implant | – | $3922 | $4785 |
†
There are two different techniques for patient screening prior to SNS, percutaneous nerve evaluation (PNE) test and staged test: PNE testing involves placement of small percutaneous lead followed by test stimulations conducted over several days (PNE only), or alternatively it can involve a surgical procedure in two stages – the placement of a permanent lead for test stimulations followed by SNS device implantation upon success (stage 1); both techniques can be combined, where percutaneous lead and permanent lead are used prior to SNS implantation (PNE + stage 1); patient screening inputs did not change from the original model;
‡
≥50% improvement in urinary incontinence episodes, which was available from published SNS studies.
BSC: Best supportive care; PTNS: Percutaneous tibial nerve stimulation; r-SNM: Rechargeable sacral neuromodulation; SNS: Sacral nerve stimulation; UIE: Urinary incontinence episode.
Model outcomes
Outcomes reported included total and incremental QALYs and costs, and ICERs relative to BSC. The change in utility value induced by a treatment was multiplied by the duration of the treatment effect to provide the number of QALYs gained [42]. An ICER is used to compare the cost–effectiveness of two competing technologies (e.g., A and B), and it is calculated using the formula: (Cost A – Cost B)/(Effectiveness A – Effectiveness B). ICER is a measure of the cost per unit increase in effectiveness (e.g., QALY), and an ICER of $100,000–$150,000/QALY is considered cost-effective in the USA [43]. The base-case analysis used the upper and lower ICER limits as a measure of cost–effectiveness.
Results
Base-case analyses: 15-year time horizon
In the base-case scenario using Medicare costs over a 15-year time horizon, onabotulinumtoxinA 100U was the most cost-effective OAB treatment vs BSC with an ICER of $39,591/QALY (Table 3 and Figure 2). The β3-adrenoceptor agonists were the least cost-effective OAB treatments vs BSC, with ICERs of $1.47 million/QALY (mirabegron 25 mg), $1.29 million/QALY (mirabegron 50 mg) and $1.61 million/QALY (vibegron 75 mg). The ICER for the ‘brand and generic’ anticholinergic arm vs BSC was $324,658/QALY, which was approximately eight-times higher than that for onabotulinumtoxinA. Comparatively, the ICER for the ‘generic only’ anticholinergic arm was $158,866/QALY, which was approximately four times higher than that for onabotulinumtoxinA. Neither of the rechargeable SNS devices were cost-effective vs BSC, with ICERs of $229,891/QALY and $163,783/QALY for the InterStim Micro and r-SNM system, respectively; however, Urgent PC ($98,031/QALY) and Protect PNS ($69,027/QALY) were cost-effective vs BSC.
| Study treatment | Total costs | Total QALYs | Incremental costs vs BSC | Incremental QALYs vs BSC | ICER per QALY gained (15 year) | ICER/QALY (2 year) | ICER/QALY (5 year) |
|---|---|---|---|---|---|---|---|
| BSC | $18,018 | 9.535 | – | – | – | – | – |
| Generic anticholinergics | $18,745 | 9.539 | $728 | 0.005 | $158,866 | $158,889 | $158,867 |
| Brand + generic anticholinergics | $19,505 | 9.539 | $1487 | 0.005 | $324,658 | $324,704 | $324,658 |
| Solifenacin 5 mg | $20,795 | 9.538 | $2778 | 0.004 | $777,759 | $777,900 | $777,760 |
| Solifenacin 10 mg | $20,772 | 9.539 | $2754 | 0.005 | $601,269 | $601,354 | $601,270 |
| Tolterodine ER 4 mg | $20,194 | 9.536 | $2177 | 0.002 | $1,137,428 | $1,137,802 | $1,137,430 |
| Mirabegron 25 mg | $24,082 | 9.539 | $6065 | 0.004 | $1,466,559 | $1,469,053 | $1,466,691 |
| Mirabegron 50 mg | $24,066 | 9.539 | $6049 | 0.005 | $1,287,339 | $1,289,167 | $1,287,436 |
| Vibegron 75 mg | $24,691 | 9.539 | $6674 | 0.004 | $1,613,785 | $1,616,530 | $1,613,932 |
| OnabotulinumtoxinA | $22,810 | 9.656 | $4793 | 0.121 | $39,591 | $84,350 | $50,304 |
| InterStim II | $47,160 | 9.605 | $29,142 | 0.070 | $416,249 | $973,154 | $631,029 |
| InterStim Micro | $34,113 | 9.605 | $16,095 | 0.070 | $229,891 | $973,190 | $450,059 |
| Axonics r-SNM | $31,963 | 9.620 | $13,945 | 0.085 | $163,783 | $829,283 | $362,342 |
| Urgent® PC (PTNS) | $21,661 | 9.572 | $3643 | 0.037 | $98,031 | $123,260 | $98,031 |
| Protect PNS (PTNS) | $21,343 | 9.583 | $3326 | 0.048 | $69,027 | $130,669 | $69,027 |
BSC: Best supportive care; ER: Extended release; ICER: Incremental cost–effectiveness ratio; PTNS: Percutaneous tibial nerve stimulation; QALY: Quality-adjusted life-years; r-SNM: Rechargeable sacral neuromodulation.
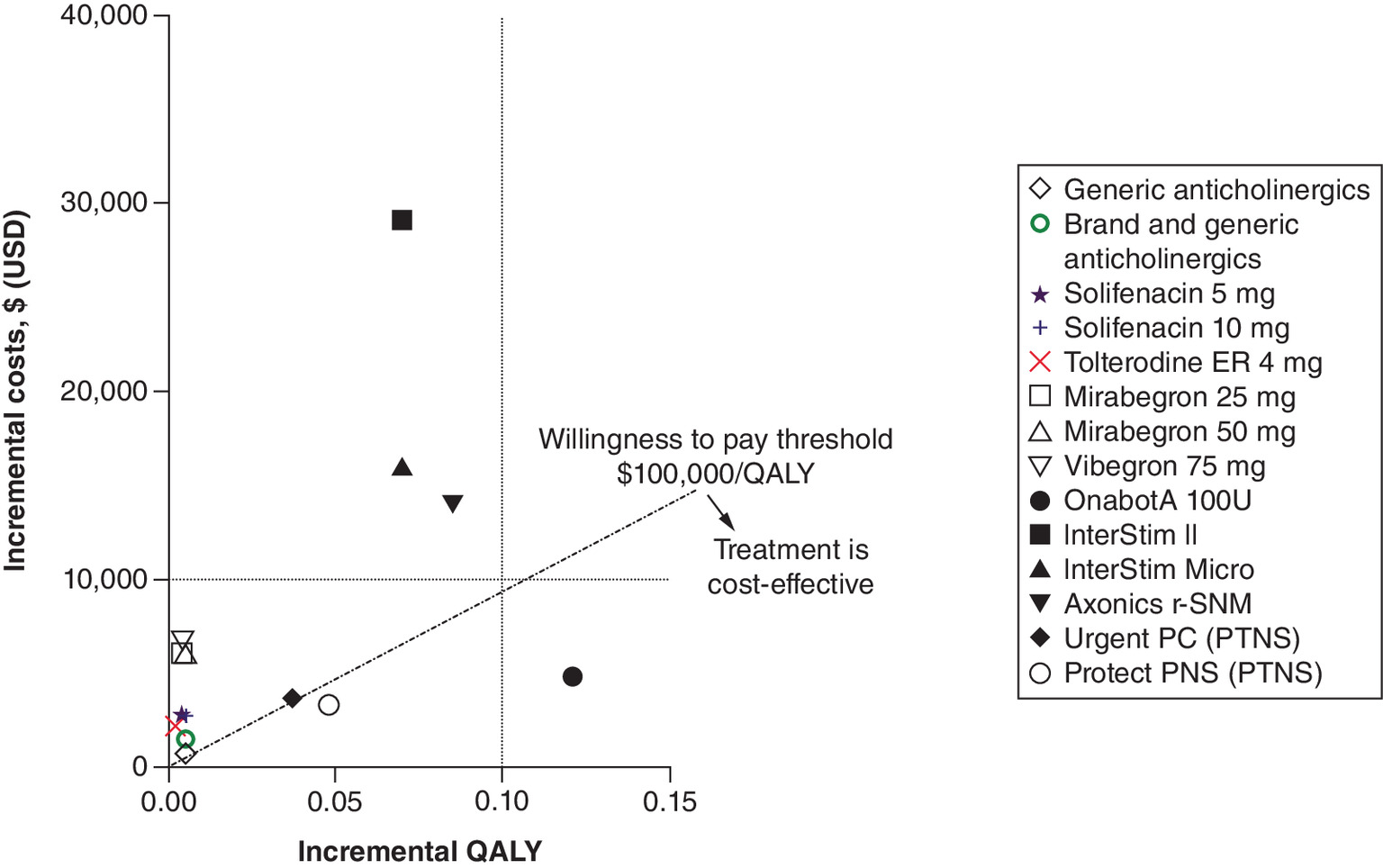
Figure 2. Incremental cost–effectiveness plane using Medicare costs at 15-year time horizon.
OnabotA: OnabotulinumtoxinA; PTNS: Percutaneous tibial nerve stimulation; QALY: Quality-adjusted life-years.
In the base-case scenario using commercial costs at a 15-year time horizon, onabotulinumtoxinA 100U was again the most cost-effective OAB treatment vs BSC, with an ICER of $42,255/QALY (Table 4 and Figure 3). The β3-adrenoceptor agonists were the least cost-effective OAB treatment vs BSC with ICERs >$1,000,000/QALY. The ICER for the ‘brand and generic’ and ‘generic only’ anticholinergic arms were similar to that reported from a Medicare payer perspective ($321,862/QALY and $156,070/QALY), while the ICER for rechargeable SNS devices were approximately $40,000 to $50,000/QALY higher than the Medicare costs. Protect PNS ($69,200/QALY) was cost-effective vs BSC based on the willingness-to-pay threshold of $100,000/QALY, while Urgent PC ($122,446/QALY) was cost-effective when the higher threshold of $150,000/QALY was considered.
| Study treatment | Total costs | Total QALYs | Incremental costs vs BSC | Incremental QALYs vs BSC | ICER per QALY gained (15 year) | ICER/QALY (2 year) | ICER/QALY (5 year) |
|---|---|---|---|---|---|---|---|
| BSC | $20,410 | 9.535 | – | – | – | – | – |
| Generic anticholinergics | $21,125 | 9.539 | $715 | 0.005 | $156,070 | $156,092 | $156,070 |
| Brand + generic anticholinergics | $21,885 | 9.539 | $1474 | 0.005 | $321,862 | $321,907 | $321,862 |
| Solifenacin 5 mg | $23,178 | 9.538 | $2767 | 0.004 | $774,753 | $774,893 | $774,753 |
| Solifenacin 10 mg | $23,152 | 9.539 | $2742 | 0.005 | $598,473 | $598,557 | $598,473 |
| Tolterodine ER 4 mg | $22,580 | 9.536 | $2169 | 0.002 | $1,133,646 | $1,134,019 | $1,133,648 |
| Mirabegron 25 mg | $26,470 | 9.539 | $6059 | 0.004 | $1,465,232 | $1,467,725 | $1,465,365 |
| Mirabegron 50 mg | $26,452 | 9.539 | $6041 | 0.005 | $1,285,791 | $1,287,616 | $1,285,887 |
| Vibegron 75 mg | $27,079 | 9.539 | $6668 | 0.004 | $1,612,459 | $1,615,202 | $1,612,605 |
| OnabotulinumtoxinA | $25,526 | 9.656 | $5115 | 0.121 | $42,255 | $91,019 | $53,924 |
| InterStim II | $56,180 | 9.605 | $35,770 | 0.070 | $510,910 | $1,190,266 | $772,889 |
| InterStim Micro | $40,262 | 9.605 | $19,852 | 0.070 | $283,553 | $1,190,309 | $552,106 |
| Axonics r-SNM | $37,676 | 9.620 | $17,266 | 0.085 | $202,778 | $1,014,643 | $444,986 |
| Urgent® PC (PTNS) | $24,961 | 9.572 | $4551 | 0.037 | $122,446 | $153,229 | $122,446 |
| Protect PNS (PTNS) | $23,744 | 9.583 | $3334 | 0.048 | $69,200 | $130,842 | $69,200 |
BSC: Best supportive care; ER: Extended release; ICER: Incremental cost–effectiveness ratio; PTNS: Percutaneous tibial nerve stimulation; QALY: Quality-adjusted life-years; r-SNM: Rechargeable sacral neuromodulation.
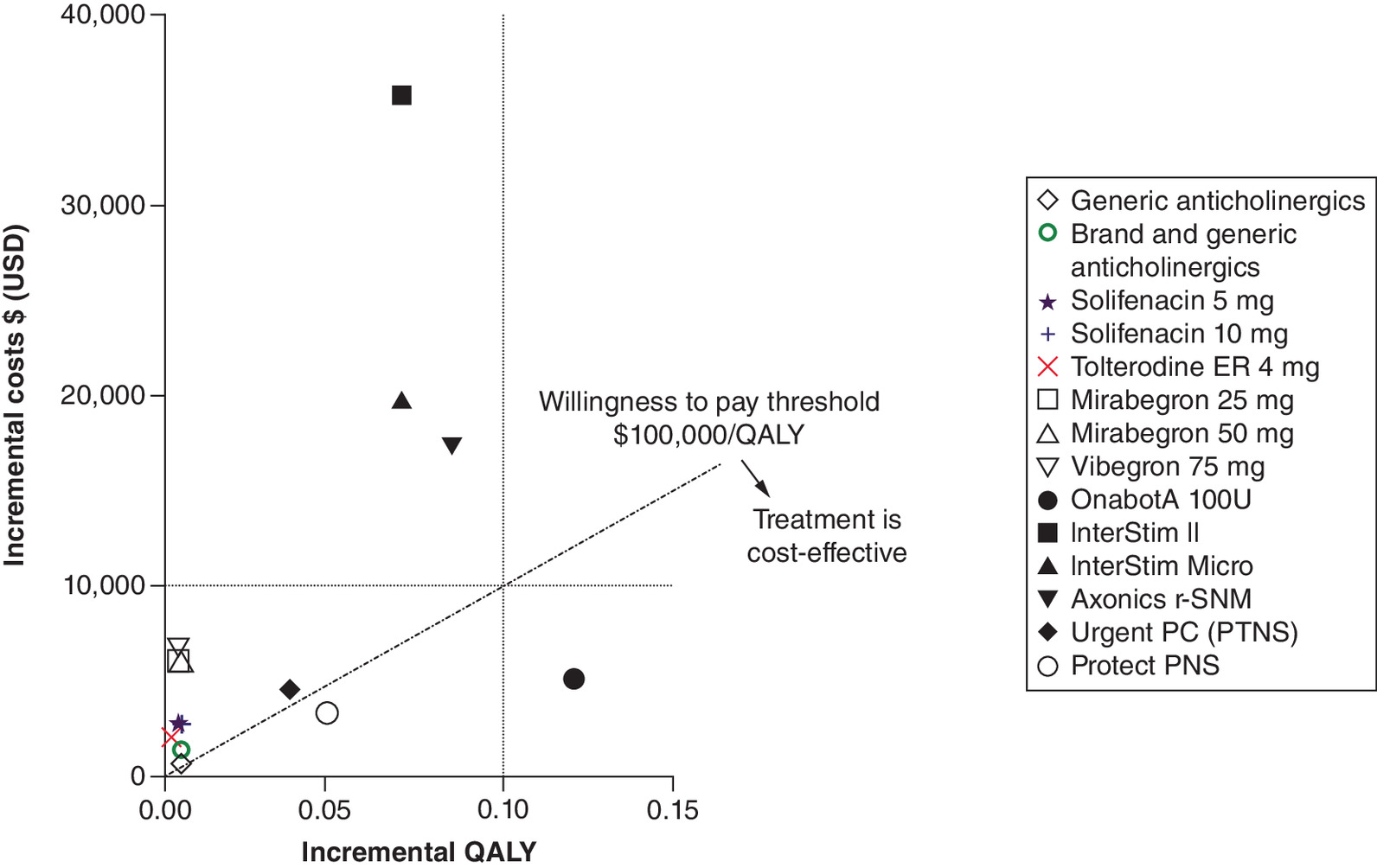
Figure 3. Incremental cost–effectiveness plane using commercial insurance costs at 15-year time horizon.
OnabotA: OnabotulinumtoxinA; PTNS; Percutaneous tibial nerve stimulation; QALY: Quality-adjusted life-years.
Sensitivity analyses: 2- & 5-year time horizons
Based on Medicare costs, onabotulinumtoxinA remained the most cost-effective of all the OAB treatments evaluated vs BSC at a 2- and 5-year time horizon, with ICERs of $84,350/QALY and $50,304/QALY, respectively (Table 3). The β3-adrenoceptor agonists were the least cost-effective OAB treatment vs BSC with ICERs >$1,000,000/QALY at the 2- and 5-year horizons. The ICERs for the ‘brand and generic’ ($324,704/QALY and $324,658/QALY) and ‘generic only’ ($158,889/QALY and $158,867/QALY) anticholinergic arms at the 2- and 5-year time horizons were similar to those reported at the 15-year horizon. Compared with the 15-year horizon, the ICERs for the rechargeable SNS devices were two times greater at 5 years (r-SNM [$362,342/QALY] and InterStim Micro [$450,059/QALY]) and four to five times greater at 2 years (r-SNM [$829,283/QALY] and InterStim Micro [$973,190/QALY]). Urgent PC and Protect PNS were the only other cost-effective interventions at 5 years ($98,031/QALY and $69,027/QALY) and at 2 years ($123,260/QALY and $130,669/QALY), respectively.
OnabotulinumtoxinA was also the most cost-effective of all the evaluated OAB treatments over the 2- and 5-year time horizons when analyzed using commercial insurance costs with ICERs of $91,019/QALY and $53,924/QALY, respectively (Table 4). The β3-adrenoceptor agonists were the least cost-effective OAB treatment vs BSC with ICERs >$1,000,000/QALY at the 2- and 5-year horizons. The ICERs ‘brand and generic’ ($321,907/QALY and $321,862/QALY) and ‘generic only’ ($156,092/QALY and $156,070/QALY) anticholinergics at the 2- and 5-year time horizons were similar to those from a Medicare payer perspective. ICERs for the rechargeable SNS devices at 2 and 5 years were approximately 20% higher than those from a Medicare payer perspective. The only other treatment within the $100,000/QALY cost–effectiveness threshold was Protect PNS ($69,200/QALY) at the 5-year time horizon. Based on the higher threshold ($150,000/QALY), Protect PNS was cost-effective at both 2 and 5 years, and Urgent PC was cost-effective at 5 years.
Discussion
The driving force behind the cost–effectiveness seen with onabotulinumtoxinA was a strong treatment response, as evidenced by the large difference in incremental QALYs vs BSC, while the cost–effectiveness seen with Protect PNS and Urgent PC was driven by low incremental costs. The low cost associated with generic anticholinergics was offset by negligible increases in incremental QALY vs BSC. Given that the QALY is calculated based on efficacy, discontinuation rates, and utility, it is feasible that the large difference in QALY was partly driven by lower discontinuation rates with onabotulinumtoxinA versus oral pharmacotherapies. The continued improvement in cost–effectiveness with onabotulinumtoxinA and SNS devices over time most likely reflects the sustained efficacy with onabotulinumtoxinA and factors in the proposed 15-year longevity of the newer SNS devices, respectively. Studies suggest that the time to request retreatment with onabotulinumtoxinA is approximately 7.5 months [21,44,45], and that efficacy following the first injection persists over multiple treatment cycles [21,46]. For Urgent PC and Protect PNS, treatment is assumed to last for 60 months/5 years, so ICERs were reduced after 5 years but were unchanged at the 15-year horizon despite having a relatively low cost. As such, any incremental improvement in treatment response with these neuromodulation therapies begins to diminish after 5 years. In the case of the oral pharmacotherapies, variations in the time horizon had a lesser impact due to the assumption of a high discontinuation rate at the end of 2 years (only 16% of patients still receiving any oral medication). Therefore, the ICERs vs BSC remain relatively constant over time because there are no additional costs or QALYs gained.
A prospective economic analysis of the Refractory Overactive Bladder: Sacral Neuromodulation vs BoTulinum Toxin Assessment (ROSETTA) randomized trial found higher costs for SNS (Interstim) at 2 years compared with onabotulinumtoxinA but similar QALYs and reductions in urgency UIEs/day [47]. Of note, the ROSETTA trial tested the earlier model of Interstim as well as onabotulinumtoxinA 200U, not the 100U FDA-approved dose evaluated here. Other previous OAB economic models using parameters specific to the Netherlands, UK, Spain, Italy and Canada suggested that SNS devices were more cost-effective than onabotulinumtoxinA [31,48–51]. Yet these models were limited by disparities in assumed treatment costs [48], inconsistencies in QALYs and stated assumptions [48], insufficient description of assumptions [49], conflicting conclusions after applying the stated assumptions [31,50], or failure to report specific cost or utility assumptions [51]. A detailed examination of these prior models was discussed previously [11], and one was retracted [31,52].
As with any cost–effectiveness model, assumptions were required to estimate outcomes, but our model used published literature when possible. Efficacy and discontinuation rates were based on clinical trial data, which may differ from real-world effectiveness and persistence rates. Furthermore, the use of clinical trial data was a limitation, particularly for the newer interventions for which limited short- and long-term data exist. Notably, efficacy data for Protect PNS were sourced from an early clinical trial with a very low sample size (n = 30). Another study limitation was the paucity of head-to-head studies comparing OAB treatments. Additionally, this analysis did not account for newer implantable devices that have recently been introduced, including eCoin® (Valencia Technologies, CA, USA), InterStim™ X (Medtronic plc, MN, USA), and F15™ (Axonics Modulation Technologies, CA, USA), which did not have data available at the time this study was conducted. In addition, non-responders were assumed to revert to BSC. Strengths of this study are that it reflects many of the currently available therapies in OAB and it incorporates the different payer perspectives in the US by analyzing cost–effectiveness from Medicare and commercial contexts.
It is important to recognize that cost and the influence of payers are among many factors that influence the choice of treatment in patients with OAB, and treatment should be individually tailored based on the patient's condition and treatment risks. Patient and disease characteristics that must be considered include age, lifestyle, comorbidities, current medications and willingness to undergo invasive treatment. Furthermore, cost is not always measured in US dollars, and there will be country-specific differences to consider such as the role and influence of payers, the level of healthcare cost reimbursement, and the burden of out-of-pocket costs for the patient.
Conclusion
In this updated cost–effectiveness analysis, onabotulinumtoxinA remains the most cost-effective OAB treatment compared with BSC from a US payer perspective despite the inclusion of the new rechargeable neuromodulation devices for SNS (r-SNM, InterStim Micro) and PTNS (Protect PNS), vibegron, and the stratification of anticholinergics by cheaper generic and costlier brands. None of the oral pharmacotherapies (anticholinergics and β3-adrenoceptor agonists) or rechargeable SNS devices were cost-effective compared to BSC. Protect PNS and Urgent PC were cost-effective although at higher ICERs than onabotulinumtoxinA versus BSC. The model results were unaffected by the varying assumptions assessed in sensitivity (2- and 5-year horizon) and the scenario analyses (Medicare vs commercial costs).
•
Overactive bladder is a prevalent and chronic condition associated with high health care costs and impaired quality of life.
•
Understanding the cost–effectiveness of available treatment options for the management of overactive bladder has important implications to treatment decision-making in clinical practice and access considerations by US payers.
•
The present study reports an updated cost–effectiveness analysis that evaluated current oral pharmacotherapies (anticholinergics [generic and branded], mirabegron, and vibegron), onabotulinumtoxinA, and neuromodulation devices (r-SNM, InterStim II, InterStim Micro, Urgent PC, Protect PNS) compared with best supportive care for the management of OAB from a Medicare and commercial payer perspective.
•
Of the available treatment options examined in this study, onabotulinumtoxinA was the most cost-effective therapy for managing overactive bladder in patients who inadequately respond to or are intolerant of oral anticholinergic therapy. Protect PNS and Urgent PC were also cost-effective. Neither anticholinergics, β3-adrenoceptor agonists, or rechargeable SNS devices were cost-effective compared with BSC.
•
The cost–effectiveness results in the base case (15-year time horizon) were maintained across different time horizons (i.e., 2 and 5 years) and payer type (i.e., Medicare or commercial).
Acknowledgments
All authors met the ICMJE authorship criteria by participating in the study design/conduct, data interpretation, as well as review and final approval of the manuscript for submission. Neither honoraria nor payments were made for authorship.
Financial & competing interests disclosure
The design, study conduct and financial support for the study were provided by Allergan (prior to acquisition by AbbVie). AbbVie participated in the interpretation of data, review and approval of the publication. B Murray has served as a consultant and investigator for Allergan, an AbbVie company, and as a consultant for Astellas, Urovant and Medtronic; J Miles-Thomas has served as a consultant for Allergan, an AbbVie company, and Urovant, and as a speaker for Allergan, an AbbVie company, Astellas and Urovant; AJ Park has served as a speaker for Allergan, an AbbVie company, and received royalties from UptoDate; VW Nitti has served as an investigator for Allergan, an AbbVie company, Astellas and Cook MyoSite; CJ Chermansky has served as an investigator for Allergan, an AbbVie company, and for Cook MyoSite; VB Nguyen is a consultant for Allergan, an AbbVie company; A Tung, P Gillard and A Lalla are employees of Allergan, an AbbVie company. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
S Murray and JL Giel of Evidence Scientific Solutions (PA, USA) provided medical writing and editing services in the development of this manuscript. AbbVie provided funding to Evidence Scientific Solutions for this work.
Ethical conduct of research
Not applicable since the data are based on economic modeling using efficacy and safety inputs from previously published OAB studies.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary table.docx)
- Download
- 38.85 KB
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Abrams P, Cardozo L, Fall M et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol. Urodyn 21(2), 167–178 (2002).
2.
Haylen BT, De Ridder D, Freeman RM et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol. Urodyn. 29(1), 4–20 (2010).
•• Seminal paper defining overactive bladder.
3.
Stewart WF, Van Rooyen JB, Cundiff GW et al. Prevalence and burden of overactive bladder in the United States. World J. Urol. 20(6), 327–336 (2003).
•• Seminal paper on prevalence of overactive bladder.
4.
Coyne KS, Wein A, Nicholson S, Kvasz M, Chen CI, Milsom I. Economic burden of urgency urinary incontinence in the United States: a systematic review. J. Manag. Care Pharm. 20(2), 130–140 (2014).
5.
Gormley EA, Lightner DJ, Burgio KL et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. J. Urol. 188(Suppl. 6), 2455–2463 (2012).
•• Seminal paper describing the most relevant guidelines for overactive bladder (OAB) management in the USA.
6.
Lightner DJ, Gomelsky A, Souter L, Vasavada SP. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline amendment 2019. J. Urol. 202(3), 558–563 (2019).
•• Most recent update of the guidelines for OAB management in the USA.
7.
Chen LC, Kuo HC. Pathophysiology of refractory overactive bladder. Low. Urin. Tract Symptoms 11(4), 177–181 (2019).
8.
Chancellor MB, Yehoshua A, Waweru C et al. Limitations of anticholinergic cycling in patients with overactive bladder (OAB) with urinary incontinence (UI): results from the CONsequences of Treatment Refractory Overactive bLadder (CONTROL) study. Int. Urol. Nephrol. 48(7), 1029–1036 (2016).
9.
Yehoshua A, Chancellor M, Vasavada S et al. Health resource utilization and cost for patients with incontinent overactive bladder treated with anticholinergics. J. Manag. Care Spec. Pharm. 22(4), 406–413 (2016).
10.
Yeowell G, Smith P, Nazir J, Hakimi Z, Siddiqui E, Fatoye F. Real-world persistence and adherence to oral antimuscarinics and mirabegron in patients with overactive bladder (OAB): a systematic literature review. BMJ Open 8(11), e021889 (2018).
11.
Murray B, Hessami SH, Gultyaev D et al. cost–effectiveness of overactive bladder treatments: from the US payer perspective. J. Comp. Eff. Res. 8(1), 61–71 (2019).
12.
Urovant Sciences Inc. Gemtesa (vibegron) prescribing information. (2020).
13.
Axonics. Axonics Sacral Neuromodulation System summary of safety and effectiveness data. (2019).
14.
Mccrery R, Lane F, Benson K et al. Treatment of urinary urgency incontinence using a rechargeable SNM system: 6-month results of the ARTISAN-SNM study. J. Urol. 203(1), 185–192 (2020).
15.
De Wachter S, Knowles CH, Elterman DS et al. New technologies and applications in sacral neuromodulation: an update. Adv. Ther. 37(2), 637–643 (2020).
16.
Medicare Payment Advisory Commission. March 2020 Report to the Congress: Medicare payment policy. (2020). www.medpac.gov/document/http-www-medpac-gov-docs-default-source-reports-mar20_entirereport_sec-pdf/
17.
York Health Economics Consortium. Allergan data on file. Network meta-analysis for BOTOX: mirabegron and anticholinergics. (2016).
18.
Drake MJ, Nitti VW, Ginsberg DA et al. Comparative assessment of the efficacy of onabotulinumtoxinA and oral therapies (anticholinergics and mirabegron) for overactive bladder: a systematic review and network meta-analysis. BJU Int 120(5), 611–622 (2017).
19.
Chapple C, Sievert KD, Macdiarmid S et al. OnabotulinumtoxinA 100 U significantly improves all idiopathic overactive bladder symptoms and quality of life in patients with overactive bladder and urinary incontinence: a randomised, double-blind, placebo-controlled trial. Eur. Urol. 64(2), 249–256 (2013).
20.
Nitti VW, Dmochowski R, Herschorn S et al. OnabotulinumtoxinA for the treatment of patients with overactive bladder and urinary incontinence: results of a phase III, randomized, placebo controlled trial. J. Urol. 189(6), 2186–2193 (2013).
21.
Nitti VW, Ginsberg D, Sievert KD et al. Durable efficacy and safety of long-term onabotulinumtoxinA treatment in patients with overactive bladder syndrome: final results of a 3.5-year study. J. Urol. 196(3), 791–800 (2016).
22.
Noblett K, Siegel S, Mangel J et al. Results of a prospective, multicenter study evaluating quality of life, safety, and efficacy of sacral neuromodulation at twelve months in subjects with symptoms of overactive bladder. Neurourol. Urodyn. 35(2), 246–251 (2016).
23.
Noblett K, Benson K, Kreder K. Detailed analysis of adverse events and surgical interventions in a large prospective trial of sacral neuromodulation therapy for overactive bladder patients. Neurourol. Urodyn. 36(4), 1136–1139 (2017).
24.
Blok B, Van Kerrebroeck P, De Wachter S et al. Three month clinical results with a rechargeable sacral neuromodulation system for the treatment of overactive bladder. Neurourol. Urodyn. 37(S2), S9–S16 (2018).
25.
Blok B, Van Kerrebroeck P, De Wachter S et al. A prospective, multicenter study of a novel, miniaturized rechargeable sacral neuromodulation system: 12-month results from the RELAX-OAB study. Neurourol. Urodyn. 38(2), 689–695 (2019).
26.
Cameron AP, Anger JT, Madison R, Saigal CS, Clemens JQ, Urologic Diseases in America Project. National trends in the usage and success of sacral nerve test stimulation. J. Urol. 185(3), 970–975 (2011).
27.
Peters KM, Carrico DJ, Macdiarmid SA et al. Sustained therapeutic effects of percutaneous tibial nerve stimulation: 24-month results of the STEP study. Neurourol. Urodyn. 32(1), 24–29 (2013).
28.
Peters KM, Carrico DJ, Wooldridge LS, Miller CJ, Macdiarmid SA. Percutaneous tibial nerve stimulation for the long-term treatment of overactive bladder: 3-year results of the STEP study. J. Urol. 189(6), 2194–2201 (2013).
29.
Peters KM, Carrico DJ, Perez-Marrero RA et al. Randomized trial of percutaneous tibial nerve stimulation versus Sham efficacy in the treatment of overactive bladder syndrome: results from the SUmiT trial. J. Urol. 183(4), 1438–1443 (2010).
30.
Micron Medical. Micron Medical Corporate Presentation. (2020).
31.
Autiero SW, Hallas N, Betts CD, Ockrim JL. The cost–effectiveness of sacral nerve stimulation (SNS) for the treatment of idiopathic medically refractory overactive bladder (wet) in the UK [retracted article]. BJU Int. 116(6), 945–954 (2015).
32.
National Institute for Health and Clinical Excellence. Percutaneous posterior tibial nerve stimulation for overactive bladder syndrome: Interventional procedures guidance [IPG362]. (2010). https://www.nice.org.uk/guidance/IPG362 (September 19, 2022).
33.
Kay S, Tolley K, Colayco D, Khalaf K, Anderson P, Globe D. Mapping EQ-5D utility scores from the Incontinence Quality of Life Questionnaire among patients with neurogenic and idiopathic overactive bladder. Value Health 16(2), 394–402 (2013).
•• Primary source for derivation of quality-adjusted life-years in the model.
34.
Ibm Micromedex. RED BOOK Online. A comprehensive, consistent drug pricing resource. www.ibm.com/products/micromedex-red-book
35.
American Medical Association. Code Book. (2016). https://ocm.ama-assn.org/OCM/CPTRelativeValueSearch.do
36.
Allergan Plc. MarketScan. Data on file. (2016).
37.
Noblett KL, Cadish LA. Sacral nerve stimulation for the treatment of refractory voiding and bowel dysfunction. Am. J. Obstet. Gynecol. 210(2), 99–106 (2014).
38.
Noridian Healthcare Solutions Durable Medical Equipment Coding System Fee Schedule Lookup Tool. https://med.noridianmedicare.com/web/jddme/fees-news/fee-schedules/lookup-tool
39.
Centers for Medicare and Medicaid Services. Medicare Physician fee schedule. www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/
40.
Centers for Medicare and Medicaid Services. Ambulatory Surgical Center (ASC) payment rates. www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ASCPayment/archive.html
41.
Blue Cross Blue Shield. Medical coverage policies: sacral nerve stimulation. (2008). www.bcbsri.com/sites/default/files/polices/SacralNerveStimulation.pdf
42.
Prieto L, Sacristán JA. Problems and solutions in calculating quality-adjusted life years (QALYs). Health Qual. Life Outcomes 1, 80 (2003).
43.
Vanness DJ, Lomas J, Ahn H. A health opportunity cost threshold for cost–effectiveness analysis in the United States. Ann. Intern. Med. 174(1), 25–32 (2021).
44.
Hamid R, Lorenzo-Gomez MF, Schulte-Baukloh H, Boroujerdi A, Patel A, Farrelly E. OnabotulinumtoxinA is a well tolerated and effective treatment for refractory overactive bladder in real-world practice. Int. Urogynecol. J. 32(1), 65–74 (2021).
45.
Mccammon K, Gousse A, Kohan A et al. Early and consistent improvements in urinary symptoms and quality of life with onabotulinumtoxinA in patients with overactive bladder and urinary incontinence: results from a randomized, placebo-controlled, phase IV clinical trial. Female Pelvic Med. Reconstr. Surg. 27(7), 450–456 (2021).
46.
Gousse AE, Kanagarajah P, Ayyathurai R, Handa P, Dabas N, Gomez CS. Repeat intradetrusor injections of onabotulinum toxin A for refractory idiopathic overactive bladder patients: a single-center experience. Female Pelvic Med. Reconstr. Surg. 17(5), 253–257 (2011).
47.
Harvie HS, Amundsen CL, Neuwahl SJ et al. Cost–effectiveness of sacral neuromodulation versus onabotulinumtoxinA for refractory urgency urinary incontinence: results of the ROSETTA randomized trial. J. Urol. 203(5), 969–977 (2020).
48.
Leong RK, De Wachter SG, Joore MA, Van Kerrebroeck PEV. Cost–effectiveness analysis of sacral neuromodulation and botulinum toxin A treatment for patients with idiopathic overactive bladder. BJU Int. 108(4), 558–564 (2011).
49.
Arlandis S, Castro D, Errando C et al. Cost–effectiveness of sacral neuromodulation compared to botulinum neurotoxin A or continued medical management in refractory overactive bladder. Value Health 14(2), 219–228 (2011).
50.
Bertapelle MP, Vottero M, Popolo GD et al. Sacral neuromodulation and botulinum toxin A for refractory idiopathic overactive bladder: a cost-utility analysis in the perspective of Italian Healthcare System. World J. Urol. 33(8), 1109–1117 (2015).
51.
Hassouna MM, Sadri H. Economic evaluation of sacral neuromodulation in overactive bladder: a Canadian perspective. Can. Urol. Assoc. J. 9(7–8), 242–247 (2015).
52.
Retraction: The cost–effectiveness of sacral nerve stimulation (SNS) for the treatment of idiopathic medically refractory overactive bladder (wet) in the UK. BJU Int. 122(2), E3 (2018).
Information & Authors
Information
Published In
Copyright
© 2023 AbbVie, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 17 May 2022
Accepted: 10 November 2022
Published online: 19 January 2023
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of overactive bladder treatments from a US commercial and payer perspective. (2023) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0089
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Cindy L. Amundsen, Suzette E. Sutherland, Sara M. Lenherr, Paul J. Niklewski, Peter R. Rodine, Roger R. Dmochowski, Cost-utility of implantable tibial neuromodulation (Revi) versus conservative therapy for urgency urinary incontinence in adults: a US payer perspective, Journal of Medical Economics, 10.1080/13696998.2026.2655592, 29, 1, (1292-1302), (2026).
- Thomas Cyriac, Megha O. Raj, Dhanya Sasidharan Palappallil, Sreedharan Syam, Fredrick Paul, Sabeena Kizhedath, Cost Analysis of Mirabegron Versus Solifenacin in Overactive Bladder Syndrome, Global Journal of Medical, Pharmaceutical, and Biomedical Update, 10.25259/GJMPBU_18_2025, 20, (9), (2025).
- Evelyn Hall, Ayachi Sharma, Thomas F. Goss, Kristin Hung, U.S. payer budget impact of the Leva Pelvic Health System to improve pelvic floor muscle training as first-line treatment of female urinary incontinence compared to real-world clinical practice, Journal of Medical Economics, 10.1080/13696998.2025.2494940, 28, 1, (637-647), (2025).
- Tyler L. Overholt, Davis M. Temple, Adam B. Cohen, Anthony Atala, Marc A. Colaco, Steve J. Hodges, OnabotulinumA toxin injections: A novel option for management of refractory nocturnal enuresis, Journal of Pediatric Urology, 10.1016/j.jpurol.2024.10.010, 21, 1, (47-52), (2025).
- Philippe Onana Ndong, Karine Baumstarck, Véronique Vitton, Urge fecal incontinence: are intramural rectal injections of botulinum toxin a long-term treatment option?, Techniques in Coloproctology, 10.1007/s10151-024-03050-x, 29, 1, (2024).
- Bahman Jabbari, Bahman Jabbari, Cost and Insurance Issues in Botulinum Toxin Therapy, Botulinum Toxin Treatment, 10.1007/978-3-031-54471-2_17, (275-283), (2024).