Cost–effectiveness of ensartinib for patients with anaplastic lymphoma kinase-positive non-small-cell lung cancer in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: Crizotinib and ensartinib improved survival in patients with ALK arrangement non-small-cell lung cancer (NSCLC); however, the economic outcomes of using ensartinib versus crizotinib are still unclear. Aim: The objective of this study was to assess the cost–effectiveness of ensartinib versus crizotinib for ALK-positive NSCLC patients from the perspective of China's healthcare system. Methods: A partitioned survival model with three health states (stable, progressive and death) was developed. Survival data were obtained from published eXalt3 clinical trials of ensartinib verses crizotinib for patients with anaplastic lymphoma kinase-positive non-small-cell lung cancer. Parametric models were used to extrapolate outcomes beyond the trial period. The drug cost comes from the local drug procurement platform. Other costs and utility values were obtained from published literature, and one-way and probabilistic sensitivity analyses were carried out to determine the robustness of the model outcomes. Results: In the whole life cycle, the average annual cost of ensatinib was US$77,636.63, and utility value was 5.5 quality adjusted life years (QALYs). Patients receiving crizotinib had 3.315QALYs and US$32,935.88 costs over the same time horizon. The incremental cost utility ratio is US$19,810.55/QALYs. In 2021, the per capita GDP of China is US$12,721.33, and the incremental cost utility is lower than the threshold of willingness to pay US$38,163.99. Conclusion: Compared with crizotinib, ensatinib is economical in the treatment of ALK-positive NSCLC and should be promoted.
Lung cancer is one of the diseases with the highest incidence and mortality worldwide. According to the latest global cancer burden data in 2020 released by the International Agency for Research on Cancer (IARC) of the World Health Organization, the number of new cases of lung cancer in China in 2020 was 820,000 and the number of deaths was 710,000, ranking first in incidence and mortality [1,2]. Lung cancer can be divided into small-cell-lung cancer and non-small-cell lung cancer (NSCLC) according to different pathological types, of which NSCLC accounts for 80%–85% [3,4]. ALK gene mutations occur in 3%–7% of NSCLC patients [5], mostly in younger women and never or light smokers. With the advent of molecular targeted drugs, cancer patients' survival time was significantly prolonged, and the patient's health status has improved too.
Crizotinib is the first molecular-targeted drug used in the treatment of ALK-positive NSCLC, which has a significant effect compared to traditional chemotherapy drugs, prolonging the progression-free survival (PFS) and overall survival (OS) of patients. However, with the promotion of clinical use, the tolerance of crizotinib and adverse reactions hinder the further promotion of clinical treatment [6,7]. To overcome the tolerability and adverse reactions, crizotinib, ceritinib, alectinib, brigatinib and lorlatinib have been used successively. Although these drugs have made some progress in tolerability and adverse reactions, they still produce certain tolerability because they cannot cover all known mutation targets [8].
Ensartinib is a new oral second-generation potent and highly selective ALK-TKI. It showed significant inhibitory effect on all evaluated ALK mutants and showed strong inhibitory effect on wild-type ALK fusion and secondary mutation sites such as F1174, C1156Y, L1196M, S1206R and T1151 [8]. At present, there is no relevant study on pharmacoeconomic of ensartinib in China. The purpose of this study is to conduct the cost–effectiveness analysis of ensartinib and crizotinib in the treatment of ALK-positive NSCLC and provide reference for clinical decision making and adjustment of national medical insurance catalog.
Data & methods
Clinical inputs
Clinical data was obtained from eXalt3 tests [9]. Inclusion criteria were as follows: ALK-positive patients with advanced or recurrent or metastatic NSCLC confirmed by histology or cytology; patients with 0–2 physical activity scores were assessed by the Eastern Oncology Collaboration; ALK inhibitors were newly treated or had received most of the previous chemotherapy regiments for one type of metastatic disease; patients who had not previously received one ALK-TKI or PD-1/PD-L1 treatment. Exclusion criteria are the following: Patients who have received ALK-TKI or PD-1/PD-L1 therapy, and patients who are currently receiving cancer treatment (other targeted therapies, chemotherapy, radiation, immunotherapy, biotherapy, hormone therapy, surgery, or tumor embolization); patients with primary central nervous system tumors and pia meningeal diseases; patients with a history of malignant tumor in the past 3 years; patients with active gastrointestinal disease or other conditions that seriously interfere with drug absorption, distribution, metabolism, or excretion.
Model structure
From the perspective of medical insurance, this study constructed a partitioned survival model of PFS, disease progression (PD) and death (Figure 1). The model cycle is consistent with the follow-up period of the clinical trial, which is set as one month. The simulation time is the whole life cycle of the patients, and the patients in the advanced stage and the death state cannot be returned to the previous state. Assuming 1000 patients were in PFS at the start of the trial, the model was terminated when 99% of the patients died. In the partitioned survival model, when the model cycle is in the follow-up period, the required data are directly obtained from the survival curve; when the model cycle exceeds the follow-up period, the parameter method is used to extrapolate the survival data [10].
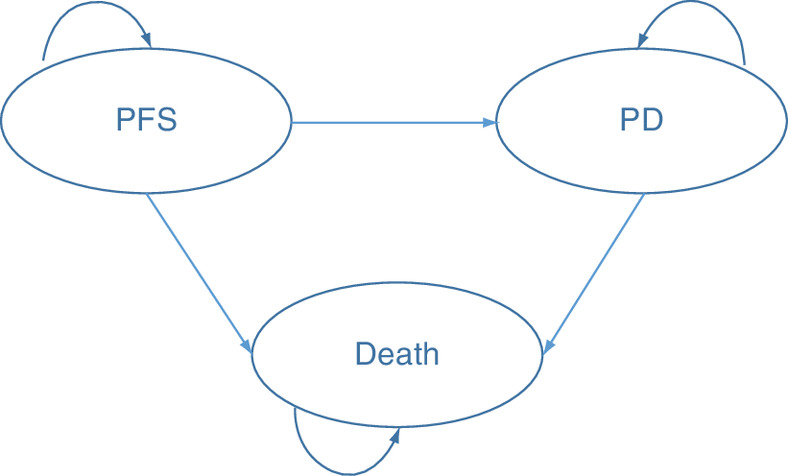
Figure 1. Three-state partition survival model.
PD: Disease progression; PFS: Progression-free survival.
Model parameters
Efficacy information
The clinical efficacy of ensartinib and crizotinib is derived from the fitting and extrapolation of the survival curves of eXalt3. GetData Graph Digitizer was used to read the PFS and (OS) curves of the two groups, and Stata software was used to convert the survival data into survival data for survival analysis [11]. According to Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC), the distribution function with the highest goodness of fit was selected. According to the survival function formula corresponding to the distribution with the highest fitting degree, the number of people in each state in each cycle was calculated.
Cost
The costs in this study include drug costs, follow-up costs, nursing costs, treatment costs after disease progression, hospice care and treatment costs for adverse reactions [12–15]. Owing to the long operation cycle of the model, all costs are discounted at a discount rate of 5%, and only grade 3 or above of adverse reactions caused using drugs are considered.
Effectiveness
Due to the lack of utility data studies on NSCLC in China, the utility value is based on published literature [16], and the utility value is also discounted by 5% discount rate. See Table 1 for all parameter descriptions.
| Parameter | Parameter value (range) | Distribution | Source | Ref. |
|---|---|---|---|---|
| Cost (US$) | ||||
| Crizotinib, per month | 2156.67 (1725.34–2588) | Gamma | Provincial procurement platform | |
| Ensartinib, per month | 6363.96 (5091.17–7636.76) | Gamma | Provincial procurement platform | |
| PFS follow-up costs, per month | 73.84 (59.07–88.6) | Gamma | [12] | |
| PD follow-up costs, per month | 105.23 (84.2–126.31) | Gamma | [12] | |
| Supportive care costs, per month | 373.11 (175.64–878.5) | Gamma | [14] | |
| Cost of chemotherapy treatment after disease progression, per month | 2445.89 (1997.21–4556.84) | Gamma | [14] | |
| Hospice costs | 2262.08 (878.5–6042.07) | Gamma | [13] | |
| Adverse reaction treatment costs | ||||
| Rash | 3.16 (2.53–3.797) | Gamma | [14] | |
| ALT/AST increased | 91.9 (73.52–110.28) | Gamma | [14] | |
| Other adverse reactions | 376.25 (301–451.51) | Gamma | [14] | |
| Utility value (QALYs) | ||||
| PFS | 0.804 (0.644–0.966) | Beta | [16] | |
| PD | 0.321 (0.257–0.385) | Beta | [16] | |
| Incidence of adverse reactions to ensatinib | ||||
| Rash | 11.2% (8.96%–13.44%) | Beta | [15] | |
| ALT/AST increased | 4.9% (3.92%–5.88%) | Beta | [15] | |
| Other adverse reactions | 13.3% (10.64%–15.96%) | Beta | [15] | |
| Incidence of adverse reactions to crizotinib | ||||
| Rash | / | |||
| ALT/AST increased | 10.2% (8.16%–12.24%) | Beta | [15] | |
| Other adverse reactions | 11.9% (9.52%–14.28%) | Beta | [15] | |
| Discount rate | 5% (0–8%) | Beta | ||
ALT: Glutamic pyruvic transaminase (GPT); AST: Glutamic oxaloacetic transaminase; PD: Disease progression; PFS: Progression-free survival; QALYs: Quality-adjusted life years.
Analysis method
Excel was used to build a partitioned survival model to calculate the average annual personal cost and the average annual personal utility of the two treatment plans, and then the cost-utility ratio and incremental cost-utility ratio were obtained. One-way sensitivity analysis and probability sensitivity analysis were used to analyze the uncertainty of parameters in the model to verify the reliability of the results. In one-way sensitivity analysis, using parameter values to fluctuate 20% or according to the published literature and expert opinion approach to evaluate the maximum and minimum values of a single variable changes affect the results of the analysis, according to the China pharmacoeconomic evaluation guidelines, set the scope of the discount rate is 0–8%, used in one-way sensitivity analysis. In probabilistic sensitivity analysis, it is assumed that all parameters obey a certain probability distribution, such as the Gamma distribution for cost data greater than 0, the Beta distribution for utility value less than 0 and the incidence of adverse reactions. A Monte Carlo simulation was used to perform 1000 result calculations and evaluate the probability distribution of different amplitude changes of various uncertain factors and its influence on the economic effect of the program.
Cost–utility threshold
At present, there is no clear definition of the threshold of cost utility in China. For the threshold of cost utility, this study adopts the recommendation of the World Health Organization and takes GDP per capita as the reference standard. When incremental cost effective ratio (ICER) is less than GDP per capita, it is considered that the increased cost is completely worthwhile. When ICER is between GDP per capita and three times GDP per capita, the increased cost is considered acceptable; when ICER is more than three times GDP per capita, the increased cost is considered unworthy. The GDP data comes from the journal article of Economic Daily that the GDP per capita in 2021 is US$12,721.33 [17]. In this study, the willingness to pay (WTP) is determined to be three times the GDP per capita, namely US$38,163.99.
Results
Analysis results
According to the survival curve of eXalt3 test, curve fitting and extrapolation were carried out using parameter method, and the optimal fitting of PFS data was determined as Lognormal distribution, and the optimal fitting of OS data was determined as exponential distribution. Then, by substituting Lognormal survival formula S(t) = 1-ø{(log(t)-μ)/σ and exponential distribution survival function S(t) = e-λt [18], the personnel distribution in each state of each cycle can be calculated. Cost–utility ratio and incremental cost–utility ratio can be calculated by substituting cost and utility data.
Cost–utility analysis
The cost–effectiveness analysis is shown in Table 2. The average annual cost of ensartinib is US$77,209.32, and the average annual utility of ensartinib is 5.55QALYs. Compared with crizotinib, although the cost has increased, better therapeutic effect has been achieved. The incremental utility ratio is US$19,810.55/QALYs, less than three times of GDP per capita (US$38,163.99). According to the reference threshold range of cost utility, the increased cost of ensartinib is acceptable, and ensartinib has a cost utility advantage.
| Treatment options | Cost (US$) | Utility value (QALYs) | Incremental cost | Incremental utility | ICER |
|---|---|---|---|---|---|
| Crizotinib | 32,935.89 | 3.315 | / | / | / |
| Ensartinib | 77,212.46 | 5.55 | 44,276.58 | 2.235 | 19,810.55 |
ICER: Incremental cost effective ratio; QALYs: Quality-adjusted life years.
Sensitivity analysis
One-way sensitivity analysis
One-way sensitivity analysis changes the value of a parameter for a single time, observe the change of research results, and intuitively express them through graphics (Figure 2). One-way sensitivity analysis of this study showed that the drug cost and PFS utility value had the greatest impact on the results, the main reason was that ensartinib prolonged the PFS of patients, resulting in increased drug cost and more utility in the PFS period of patients. One-way sensitivity analysis results were consistent with the actual situation of the study.
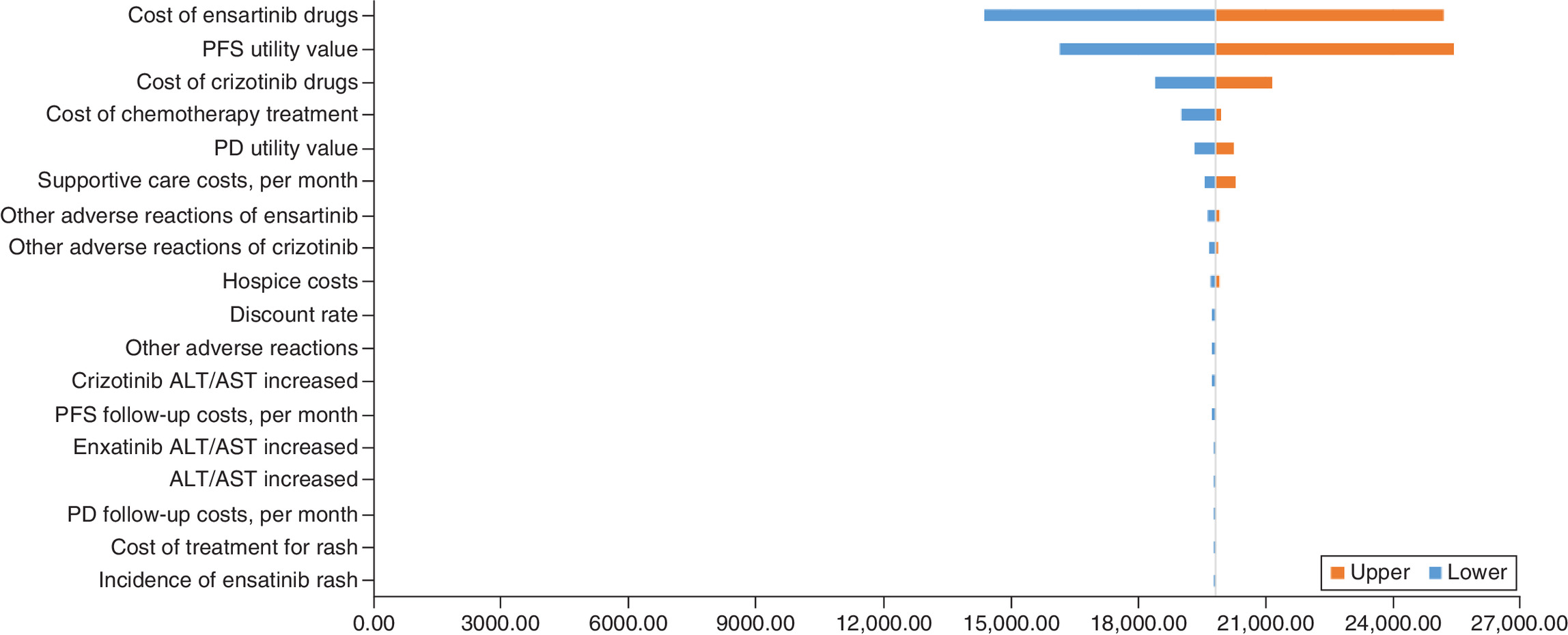
Figure 2. One-way sensitivity analysis.
ALT: Glutamic pyruvic transaminase (GPT); AST: Glutamic oxaloacetic transaminase; PD: Disease progression; PFS: Progression-free survival.
Probabilistic sensitivity analysis
Probabilistic sensitivity analysis is to make a probability description of the economic effect index of the scheme by studying the probability distribution of different amplitude changes of various uncertain factors and its influence on the economic effect of the scheme, to make a more accurate judgment on the risk of the scheme. In this research, Excel was used to construct a Monte Carlo simulation and 1000 times of repetition sampling were simulated to obtain the results of probability sensitivity analysis (Figure 3). The results show that all scatter points are 100% distributed below the payment threshold, indicating that ICER value is lower than the payment threshold.
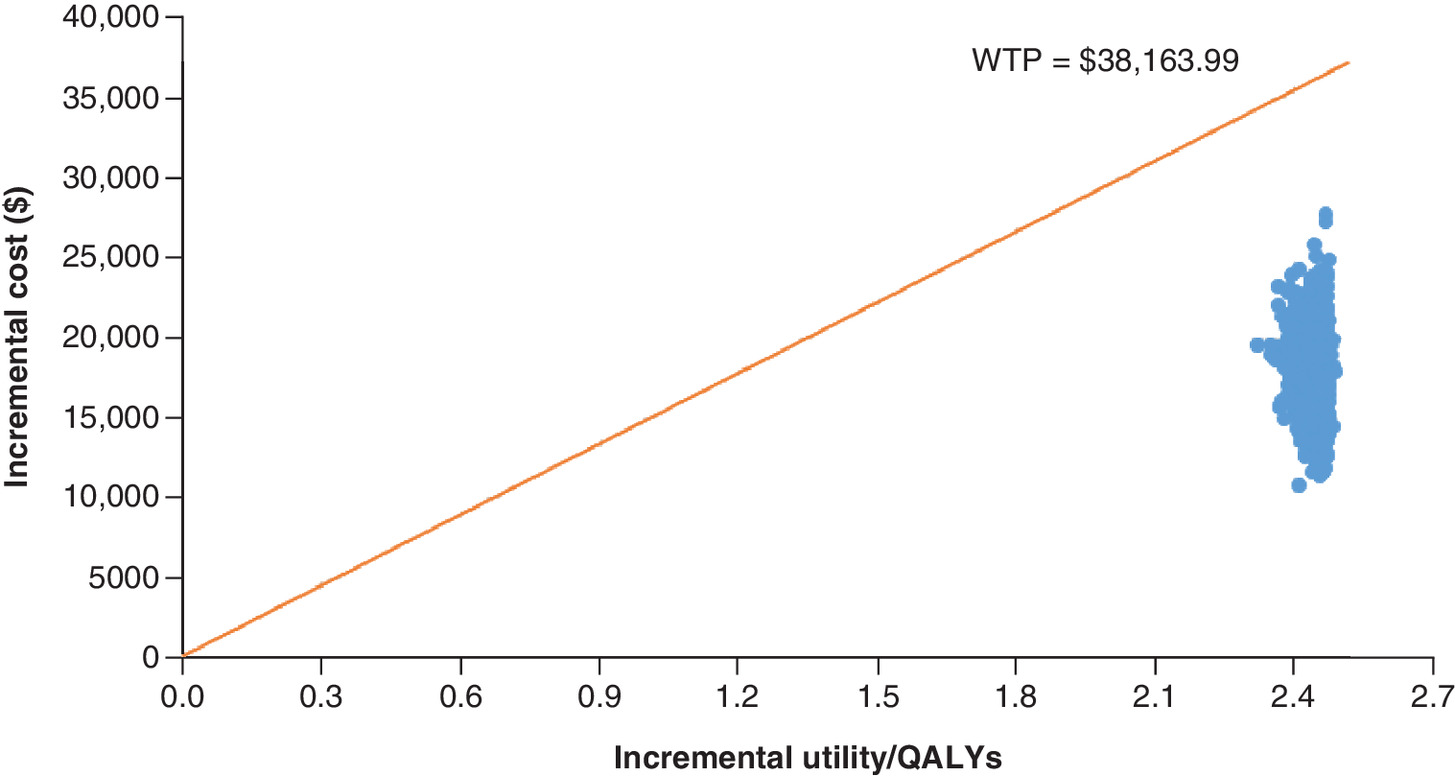
Figure 3. Probabilistic sensitivity analysis.
QALYs: Quality-adjusted life years; WTP: Willingness to pay.
Discussion
In recent years, cancer has been on the rise in our country. With the development of science and technology, a variety of new drugs are constantly coming out, and the medical insurance department is actively including various cancer drugs into the medical insurance list, but the high cost of drug research and development still leads to the high price of cancer drugs. In the context of uneven distribution of domestic medical data and huge pressure of medical insurance funds, it is necessary to choose a treatment plan with better effectiveness and lower cost.
In recent years, economic studies on ALK-TKI have also been carried out both domestic and abroad. In China, Zhang et al. [19] evaluated the long-term cost–effectiveness of alectinib compared with crizotinib in first-line treatment of Chinese ALK-positive advanced or metastatic NSCLC from the perspective of the whole society. Compared with crizotinib, alectinib can significantly prolong life years and bring significant QALYs benefits, effectively save costs related to brain metastases and progressive states, and can be considered to have a cost–effectiveness advantage. Lei Weicheng et al. [20] conducted cost–effectiveness analysis on second-line crizotinib for advanced ALK-positive NSCLC, suggesting that second-line crizotinib has economic advantages compared with chemotherapy group. Li H C et al. [21] studied the cost–effectiveness of ceritinib, alectinib and crizotinib in the treatment of first-line ALK-positive advanced NSCLC, and the results showed that, compared with crizotinib and alectinib, ceritinib is a cost–effective option for the treatment of ALK-positive advanced NSCLC. Herbert H.Loong et al. [22] studied the cost–effectiveness analysis of ceritinib versus crizotinib in the treatment of untreated ALK-positive NSCLC in Hong Kong, and the results showed that ceritinib provided a more cost–effective option compared with crizotinib for ALK-positive advanced NCSLC in Hong Kong. Meijuan Huang et al. [23] studied cost–effectiveness of crizotinib and platinum-based combined chemotherapy as first-line treatment for ALK-positive NSCLC based on real-world data, and the results showed that crizotinib improved PFS in ALK-positive patients compared with chemotherapy. Crizotinib can be an effective and economical first-line treatment for ALK-positive advanced non-small-cell lung cancer.
Marine Sivignon et al. [24] evaluated the cost–effectiveness comparison of alectinib against crizotinib in first-line treatment of ALK-positive advanced NSCLC in the French environment. The results obtained a better clinical outcome with crizotinib for first-line treatment of ALK-positive NSCLC with alectinib and were cost–effective for the French healthcare system. Josh J. Carlson et al. [25] studied the cost–effectiveness of alectinib and crizotinib in the treatment of first-line ALK-positive advanced NSCLC, and the analysis showed that compared with crizotinib, alectinib extended the time of progressive-free state and quality-adjusted life. Alectinib may be a cost–effective treatment for ALK-positive NSCLC. Manjusha Hurry et al. [26] studied the cost–effectiveness analysis of ceritinib in ALK-positive NSCLC patients in Canada. Based on the WTP threshold of end-of-life cancer drugs, ceritinib may be considered as a more cost–effective option compared to other alternative drugs with crizotinib progression or intolerance in Canada.
Domestic and abroad about the ALK-positive NSCLC pharmacogenomics studies have shown that for most new developed drugs, the prices are higher, but the treatment effect is much better than traditional drugs. And there would be a greater cost–effectiveness advantage if these drugs were covered by medical insurance.
The launch of ensartinib in November 2020 offers a new option for patients with ALK-positive NSCLC eXalt3 test and other studies [8,9] have shown that ensartinib has significantly improved the survival time and quality of life of patients, but the economic evaluation of ensartinib treatment has not been studied domestically or abroad.
In this study, the ensartinib remedy was more effective than crizotinib. In the patient life cycle study, ensartinib obtained more PFS. Although the extension of PFS resulted in an increase in cost, the increased cost was acceptable to patients. The dosage of crizotinib was 250 mg twice a day. The daily dosage of ensartinib was 225 mg once a day [27], and ensartinib had better compliance than crizotinib.
In this study, the economics of ensartinib was analyzed by using the partitioned survival model and parametric extrapolation to simulate the whole life cycle of patients. Limitations: (1) Survival data from eXalt3 test, the test from the global 290 cases randomly into the ALK gene mutation of NSCLC patients, 140 cases patients in China, while Chinese patients accounted for nearly 50%, but still can produce certain effect on the result. (2) In the partitioned survival model, it is assumed that the initial number of patients is 1000, which expands the patient base of clinical trials and may affect the uncertainty of research results. (3) The PFS and OS survival curves in the eXalt3 trial are incomplete and the clinical trial is still ongoing, with only 36 months of follow-up as of press time, and OS data of ensartinib and crizotinib are greater than 60%. The subsequent survival information is extrapolated according to the existing survival curve using the parameter method. Long-term extrapolation will lead to the decrease of the reliability of the results. (4) Currently, there is a lack of health utility values based on the Chinese population. Most domestic studies on utility values refer to or cite foreign research data. It is expected that more scholars will conduct research and summary on health utility values of the Chinese population.
In the new round of national medical insurance negotiations, ensartinib has successfully entered the medical insurance list. With continuous clinical use, the economics of ensartinib can be further studied and discussed through real world data in the later stage.
Conclusion
From the perspective of medical insurance payment, according to the three times GDP per capita WTP standard recommended by the World Health Organization, ensartinib is more economical than crizotinib for patients with ALK-positive NSCLC, which can provide a reference for clinical decision-making and adjustment of national medical insurance catalog.
•
A series of studies of ensatinib have shown better efficacy and less adverse reactions than other ALK inhibitors.
•
Currently, there is a lack of studies on the pharmacoeconomics of ensatinib.
•
A three-state partitioned survival model was constructed to simulate disease progression.
•
Clinical data were extracted from the eXalt3 trial.
•
Cost and utility values are mainly obtained from the literature.
•
The incremental cost–effectiveness ratio of ensatinib was US$1,9810.55/quality-adjusted life years, less than three times GDP per capita.
•
Ensatinib was cost effective compared with crizotinib for non-small-cell lung cancer in China.
•
The overall survival time of ensatinib had the substantial impact on the economic outcomes.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Our study used mathematical modeling and was not an active clinical trial; therefore, no approval was required from the Institutional Research Ethics Board.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Oncology Forum. The latest global cancer data for 2020. Chin.J.Clin.Oncol.Rehab. 28(03), 301 (2021).
2.
Li M, Hou X, Zhou C et al. Prevalence and clinical impact of concomitant mutations in anaplastic lymphoma kinase rearrangement advanced non-small-cell lung cancer (Guangdong Association of Thoracic Oncology Study 1055). Front Oncol. 10, 1216 (2020).
3.
Herbst RS, Redman MW, Kim ES et al. Cetuximab plus carboplatin and paclitaxel with or without bevacizumab versus carboplatin and paclitaxel with or without bevacizumab in advanced NSCLC (SWOG S0819): a randomised, phase 3 study. Lancet Oncol. 19(1), 101–114 (2018).
4.
Salem A, Mistry H, Hatton M et al. Association of chemoradiotherapy with outcomes among patients with stage I to II vs stage III small cell lung cancer: secondary analysis of a randomized clinical trial. JAMA Oncol. 5(3), e185335 (2019).
• Provides background on the epidemiology of non-small-cell lung cancer.
5.
Hida T, Nakagawa K, Seto T et al. Pharmacologic study (JP28927) of alectinib in Japanese patients with ALK+ non-small-cell lung cancer with or without prior crizotinib therapy. Cancer Sci. 107(11), 1642–1646 (2016).
6.
Cui S, Zhao Y, Dong L et al. Is there a progression-free survival benefit of first-line crizotinib versus standard chemotherapy and second-line crizotinib in ALK-positive advanced lung adenocarcinoma? A retrospective study of Chinese patients. Cancer Med. 5(6), 1013–1021 (2016).
7.
Radaram B, Pisaneschi F, Rao Y, Yang P, Piwnica-Worms D, Alauddin MM. Novel derivatives of anaplastic lymphoma kinase inhibitors: synthesis, radiolabeling, and preliminary biological studies of fluoroethyl analogues of crizotinib, alectinib, and ceritinib. Eur. J. Med. Chem. 182, 111571 (2019).
8.
Wang Y, Yuan X, Xiong J et al. Pharmacology and clinical evaluation of ensartinib hydrochloride capsule. Zhongguo Fei Ai Za Zhi 23(8), 719–729 (2020).
• Shows that ensartinib significantly improves survival benefit and reduces the risk of mortality.
9.
Horn L, Wang Z, Wu G et al. Ensartinib vs crizotinib for patients with anaplastic lymphoma kinase-positive non-small-cell lung cancer: a randomized clinical trial. JAMA Oncol. 7(11), 1617–1625 (2021).
•• EXalt3 trial from which we have extracted the most important data to elaborate our cost–effectiveness study, such as progression-free survival and overall survival curves and the adverse reaction data, among other data.
10.
Shao R, Tang W, Ma A. Application of partitioned survival model in pharmacoeconomic evaluation. Chin. Health Econ. 38(09), 60–63 (2019).
11.
Wei Y, Royston P. Reconstructing time-to-event data from published Kaplan-Meier curves. Stata. J. 17(4), 786–802 (2017).
12.
Wang Y, Wu J, Wu D. Pharmacoeconomic evaluation of sunitinib in the treatment of advanced gastrointestinal stromal tumor resistant to imatinib. Chin. J. Pharmacoepidemol. 30(01), 33–38 (2021).
•• Provides information on the cost of follow-up costs.
13.
Wu B, Gu X, Zhang Q, Xie F. Cost-effectiveness of osimertinib in treating newly diagnosed, advanced EGFR-mutation-positive non-small-cell lung cancer. Oncologist 24(3), 349–357 (2019).
•• Provides information on the cost of Hospice costs.
14.
Cai H, Zhang L, Li N et al. Cost-effectiveness of osimertinib as first-line treatment and sequential therapy for EGFR mutation-positive non-small-cell lung cancer in China. Clin. Ther. 41(2), 280–290 (2019).
•• Provides information on the cost of adverse events.
15.
Bertranou E, Bodnar C, Dansk V, Greystoke A, Large S, Dyer M. Cost-effectiveness of osimertinib in the UK for advanced EGFR-T790M non-small-cell lung cancer. J Med. Econ. 21(2), 113–121 (2018).
•• Provides information on the cost of incidence of adverse reactions rash.
16.
Nafees B, Lloyd AJ, Dewilde S, Rajan N, Lorenzo M. Health state utilities in non-small-cell lung cancer: an international study. Asia Pac. J. Clin. Oncol. 13(5), e195–e203 (2017).
•• Utility values are from the report of Nafees et al.
17.
Xiong L. With a year-on-year growth of 8.1 percent and an average growth of 5.1 percent over the past two years, China's GDP has jumped to 110 trillion yuan. Economy. 2(02), 69–71 (2022).
18.
Diaby V, Adunlin G, Montero AJ. Survival modeling for the estimation of transition probabilities in model-based economic evaluations in the absence of individual patient data: a tutorial. Pharmacoeconomics 32(2), 101–108 (2014).
19.
Zhang L, Zhou C, Zhao J et al. Cost-effectiveness of alectinib in first-line treatment of AlK-positive advanced or metastatic non-small-cell lung cancer in China. China Health Insurance, 56–62 (2019).
20.
Lei W, Du B, Lin X et al. Cost-effectiveness analysis of crizotinib in second-line treatment of advanced non-small-cell lung cancer. Pharmacy Today 29(04), 234–236 (2019).
21.
Li H, Lai L, Wu B. Cost effectiveness of ceritinib and alectinib versus crizotinib in first-line anaplastic lymphoma kinase-positive advanced non-small-cell lung cancer. Clin. Drug Investig. 40(2), 183–189 (2020).
22.
Loong HH, Wong CKH, Leung LKS et al. Cost-effectiveness analysis of ceritinib vs. crizotinib in previously untreated anaplastic lymphoma kinase (ALK)-positive non-small-cell lung cancer (NSCLC) in Hong Kong. Cost Eff. Resour. Alloc. 18(1), 50 (2020).
23.
Huang M, Tian Y, He M et al. Crizotinib versus chemotherapy: a real-world cost-effectiveness study in China. J. Comp. Eff. Res. 9(2), 93–102 (2020).
24.
Sivignon M, Monnier R, Tehard B, Roze S. Cost-effectiveness of alectinib compared to crizotinib for the treatment of first-line ALK+ advanced non-small-cell lung cancer in France. PLoS One 15(1), e0226196 (2020).
25.
Carlson JJ, Suh K, Orfanos P, Wong W. Cost effectiveness of alectinib vs. crizotinib in first-line anaplastic lymphoma kinase-positive advanced non-small-cell lung cancer. Pharmacoeconomics 36(4), 495–504 (2018).
26.
Hurry M, Zhou ZY, Zhang J et al. Cost-effectiveness of ceritinib in patients previously treated with crizotinib in anaplastic lymphoma kinase positive (ALK+) non-small-cell lung cancer in Canada. J. Med. Econ. 19(10), 936–944 (2016).
27.
Yang Y, Zhou J, Zhou J et al. Efficacy, safety, and biomarker analysis of ensartinib in crizotinib-resistant, ALK-positive non-small-cell lung cancer: a multicentre, phase 2 trial. Lancet Respir. Med. 8(1), 45–53 (2020).
Information & Authors
Information
Published In
Pages: 871 - 878
PubMed: 35748298
Copyright
© 2022 Future Medicine Ltd.
History
Received: 13 April 2022
Accepted: 9 June 2022
Published online: 24 June 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of ensartinib for patients with anaplastic lymphoma kinase-positive non-small-cell lung cancer in China. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0066
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Qiang Guo, Xiang-Yu Luo, Hua Liu, Min Zeng, Jun Zhou, Jun Zhang, Jia-Long Guo, Cheng-Yi Lin, Treatment with ensartinib improves postoperative survival in a patient with stage IIB LUAD carrying a rare ALK mutation: case report, Open Life Sciences, 10.1515/biol-2025-1266, 21, 1, (2026).
- Gang Fang, Zhipeng Pi, Yiping An, Xinxin Cao, Wei Li, Xiangjun Zhu, Jinxi Ding, Cost-effectiveness analysis of gumarontinib versus savolitinib for the treatment of advanced or metastatic NSCLC with MET exon 14 skipping mutations in China using partitioned survival model, Frontiers in Pharmacology, 10.3389/fphar.2025.1400422, 16, (2025).
- Ya-Ning Zhu, Meng Tang, Ke-Xin Sun, Bei Gao, Xian-Peng Shi, Peng Zhang, Cost-effectiveness of sotorasib as a second-line treatment for non-small cell lung cancer with KRASG12C mutation in China and the United States, Frontiers in Pharmacology, 10.3389/fphar.2024.1348688, 15, (2024).
- Xiaowen Wang, Yiqun Yu, Hongrui Liu, Fengjiao Bu, Chunying Shen, Qingfeng He, Xiao Zhu, Pin Jiang, Bing Han, Xiaoqiang Xiang, Prediction of Drug–Drug Interactions with Ensartinib as a Time-Dependent CYP3A Inhibitor Using Physiologically Based Pharmacokinetic Model, Drug Metabolism and Disposition, 10.1124/dmd.123.001373, 51, 11, (1515-1526), (2023).
- Lara Chayab, Natalia Konstantelos, Natasha B. Leighl, Mina Tadrous, William W. L. Wong, A Systematic Review of the Cost-Effectiveness Analyses of Anaplastic Lymphoma Kinase (ALK) Inhibitors in Patients with Locally Advanced or Metastatic Non-small Cell Lung Cancer (NSCLC), PharmacoEconomics, 10.1007/s40273-023-01279-2, 41, 8, (945-980), (2023).