Indirect treatment comparison of anifrolumab efficacy versus belimumab in adults with systemic lupus erythematosus
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Assess the comparative efficacy of anifrolumab 300 mg versus belimumab 10 mg/kg in adults with moderate-to-severe systemic lupus erythematosus (SLE) receiving standard therapy. Patients and methods: Population-adjusted simulated treatment comparisons (primary analyses) and matching-adjusted indirect comparisons (supporting analyses) were conducted using individual patient data from TULIP-1/TULIP-2 and summary-level data from BLISS-52/BLISS-76. Results: Compared with belimumab-treated patients, anifrolumab-treated patients were more than twice as likely to achieve a reduction of four or more points in SLE Disease Activity Index 2000 score (simulated treatment comparison odds ratio: 2.47; 95% CI: 1.16–5.25) and SLE Responder Index-4 response (odds ratio: 2.61; 95% CI: 1.22–5.58) at 52 weeks. Conclusion: Patients with moderate-to-severe SLE are more likely to achieve an improvement in disease activity with anifrolumab than with belimumab.
Systemic lupus erythematosus (SLE) is a complex autoimmune disorder with varying global prevalence [1]. In SLE, characteristic production of pathogenic autoantibodies and tissue deposition of immune complexes results in inflammation across multiple organ systems [2]. While the specific pathophysiology of SLE is unclear, activation of the type I interferon pathway is known to be a central pathogenic mediator [3–6].
The clinical manifestations of SLE are heterogeneous and may include skin lesions, renal disease, and musculoskeletal, neuropsychiatric, cardiorespiratory and gastrointestinal manifestations, as well as nonspecific symptoms such as fatigue and fever [2]. Treatment of SLE focuses on controlling inflammation, preventing organ damage, improving quality of life and achieving a low disease state or remission to ensure long-term survival [7–9]. Recommended standard-of-care treatments for SLE include antimalarials, oral corticosteroids (OCSs) and adjuvant immunosuppressive/steroid-sparing agents [8]. These treatments are mostly nonspecific and can demonstrate limited efficacy and poor tolerability in some patients [7–9]; for example, long-term OCS therapy is often used to manage SLE despite its contribution to organ damage [10–12]. Thus there is a need for new, alternative treatment options that control disease activity better and allow steroid sparing.
In 2011 the US FDA and the European Medicines Agency (EMA) approved the first biological agent for the treatment of SLE: belimumab (Benlysta®; GlaxoSmithKline), a human IgG1λ monoclonal antibody B-lymphocyte stimulator-specific inhibitor [13–15]. In the USA, belimumab is indicated as add-on therapy for patients aged 5 years or older with active, autoantibody-positive SLE who are receiving standard therapy, and for adult patients with active lupus nephritis who are receiving standard therapy [13,14]. In the European union, belimumab is indicated as an add-on therapy for patients aged 5 years or older with active, autoantibody-positive SLE with a high degree of disease activity (positive anti-dsDNA antibody and low complement) despite standard therapy, and in combination with immunosuppressive therapies for the treatment of adult patients with active lupus nephritis [14]. In patients with treatment-refractory SLE, belimumab can reduce disease activity, including musculoskeletal disease manifestations, OCS dose and flare frequency; recent evidence also suggests a role in slowing organ damage accrual [16–22]. Long-term studies of belimumab have shown a stable safety profile across up to 13 years of exposure [20,23,24]. In 2021 anifrolumab (Saphnelo™; AstraZeneca), an anti-type I interferon receptor humanized IgG1 monoclonal antibody developed to block the type I interferon pathway [25,26], was approved in the USA, Japan and Canada for the treatment of adult patients with moderate-to-severe SLE who are receiving standard therapy [27–29]. Anifrolumab has also recently been approved in the EU as an add-on therapy for the treatment of adult patients with moderate-to-severe, active autoantibody-positive SLE despite standard therapy [30]. The efficacy and safety of anifrolumab in patients with moderate-to-severe active, autoantibody-positive SLE receiving standard therapy were investigated in two phase III, randomized, double-blind, placebo-controlled studies: TULIP-1 [31] and TULIP-2 [32]. Compared with placebo, anifrolumab can reduce disease activity, OCS dose, skin disease severity, swollen and tender joints and flare frequency [26,32–35]. A pooled analysis of phase II and phase III data showed that anifrolumab had an acceptable safety profile across the 52-week study period [36].
No studies have compared the efficacy of anifrolumab and belimumab directly. In the absence of head-to-head trials, indirect treatment comparisons (ITCs) can provide insights into the comparative efficacy of different treatments [37,38]. The objective of this study was to use ITCs – utilizing individual patient data (IPD) from anifrolumab trials – to compare the efficacy of anifrolumab and belimumab for adults with moderate-to-severe SLE receiving standard therapy.
Patients & methods
Scope
Study selection & feasibility assessment
IPD were available from three trials in which patients received intravenous (iv.) anifrolumab 300 mg or placebo: MUSE, TULIP-1 and TULIP-2. The phase II MUSE trial [34] was not included in the primary analyses because of differences in study design and inclusion/exclusion criteria, but was included in sensitivity analyses.
A systematic literature review was conducted to identify randomized controlled trials of belimumab in adults with moderate-to-severe SLE (Supplementary Figure 1 & Supplementary Table 1). A qualitative feasibility assessment was then performed to determine which of these studies could be included in the quantitative analyses for comparison with anifrolumab, and whether the anifrolumab and belimumab studies were similar enough for ITCs to be performed (Supplementary Table 2). Only iv doses approved for use (anifrolumab 300 mg and belimumab 10 mg/kg) were considered [13,27].
Target outcomes of interest were:
•
•
Proportion of patients who achieved an SLE Responder Index-4 (SRI-4) response at week 52 [40];
•
Proportion of patients who achieved a British Isles Lupus Assessment Group (BILAG)-based Composite Lupus Assessment (BICLA) response at week 52 [41];
•
•
Proportion of patients with a reduction in OCS dosage to ≤7.5 mg per day, sustained from week 40 to week 52 among patients with a baseline dosage of ≥10 mg per day;
Indirect treatment comparison
Analyses to determine unadjusted comparative data for anifrolumab versus placebo (pooled TULIP-1 and TULIP-2 data) and belimumab versus placebo (pooled BLISS-52 and BLISS-76 data) were performed. To mitigate the impact of between-trial heterogeneity, two population-adjusted analysis methods were performed: simulated treatment comparison (STC) and matching-adjusted indirect treatment comparison (MAIC). The STC method was selected as the primary analysis because recent research suggests superior performance in eliminating bias when compared with MAICs [38].
All statistical analyses were performed using R version 3.6.1. Statistical significance testing was defined using a two-tailed p-value of <0.05, and all comparisons between groups were reported with point estimates (ie, odds ratios [ORs] and mean differences) and 95% CIs.
Treatment effect modifiers
Treatment effect modifiers (TEMs) are covariates, typically patient characteristics at baseline, that alter the effect of treatment on outcomes. Expert clinicians identified 14 covariates as likely TEMs: sex, race, age, SLEDAI score at baseline, organ domain score of one or more BILAG A items or two or more BILAG B items, antinuclear antibody titer ≥1:80, abnormal low C3, abnormal low C4, anti-dsDNA ≥30 IU/ml, antimalarial use, azathioprine use, methotrexate use, mycophenolate use, and OCS dose ≥7.5 mg at baseline. In the primary STC analysis, all identified TEMs were ranked based on their relative degree of effect modification for each individual outcome and, based on the opinion of the clinician authors and a literature review of the predictors of SLE treatment outcomes written by clinical experts, the two lowest-impact TEMs were removed, with only the 12 highest-impact TEMs included in the regression models if reported by all included studies. For the outcome of OCS reduction, a subgroup analysis of the belimumab BLISS trials was used [21], for which BMI was available and was included as one of eight high-impact TEMs with available baseline data (Supplementary Table 3). As the TULIP and BLISS trials included a placebo comparator arm [16,18,31,32], the STCs and MAICs were ‘anchored’ [43]; adjustments for differences in prognostic variables were therefore not required [43].
Simulated treatment comparisons
Anchored STCs were conducted using the methods outlined in the National Institute for Health and Care Excellence (NICE) Decision Support Unit Technical Support Document 18 [43]. A regression model incorporating TEMs as predictor variables was fitted to the pooled IPD from TULIP-1 and TULIP-2 and then used to predict the effect of anifrolumab in the comparator population for each outcome. Model convergence and fit statistics were used to assess the performance of each regression model.
Matching-adjusted indirect treatment comparisons
MAICs were conducted as validation of the STC results. In brief, this involved the following steps: first, removing patients from the TULIP-1 and TULIP-2 IPD who would not have met the eligibility criteria of the comparator trial; second, reweighting the remaining patients such that the summary statistics of baseline patient characteristics matched those of the comparator trial across the selected characteristics identified as important TEMs; and third, conducting an ITC using this adjusted TULIP population against the aggregate-level data of the included belimumab trials.
Sensitivity analyses
Extensive sensitivity analyses were also conducted for both STCs and MAICs to explore the impact of adjusting for different subsets of TEMs (data not shown). To mitigate against the risk of a potential negative impact on the effective sample size for the MAIC analyses, TEMs were ranked based on their relative degree of effect modification, and the two lowest-impact TEMs were removed from the main MAIC analysis; ie, only the 12 highest-impact TEMs were adjusted. To increase the effective sample size for the OCS reduction outcome, a sensitivity analysis for the MAIC of OCS dose reduction was conducted including fewer TEMs, which were determined to be particularly clinically important: one or more BILAG A or two or more BILAG B items, SLEDAI-2K score and OCS dose at baseline.
Additional sensitivity analyses comprised the studies not included in the primary analyses owing to differences in study design or inclusion/exclusion criteria: the phase II MUSE study (anifrolumab) [34] and the BLISS-SC study (bioequivalent subcutaneous preparation of belimumab 200 mg) [44] (see Supplementary Materials).
Results
Study selection & feasibility assessment
From the systematic literature search, five relevant belimumab publications were retrieved [16,18,23,44,45]. These included primary publications as well as pooled and post hoc analyses of phase III randomized clinical trials. Two placebo-controlled phase III studies, BLISS-52 [18] and BLISS-76 [16], were identified as the most similar to the TULIP trials and therefore the most suitable for conducting ITCs versus anifrolumab (Table 1). Other publications were not included for reasons of insufficient overlap in population characteristics, intervention/comparator, outcome or study design; unsuitable publication type for data analysis (systematic literature review, meta-analysis or network meta-analysis); incomplete or insufficient data; inaccessibility of the full-text article; or publication language other than English (Supplementary Figure 1).
| Study name | Phase | Study duration | Key inclusion criteria | Key exclusion criteria | Ref. | |||
|---|---|---|---|---|---|---|---|---|
| Age criteria | SLEDAI criteria | Current regimen criteria | Other key clinical criteria | |||||
| Anifrolumab | ||||||||
| TULIP-1 (NCT02446912) | III | 52 weeks | 18–70 years | ≥6† | Ongoing stable treatment regimen with at least one of either prednisone or equivalent (monotherapy: 7.5–40 mg/day; combination therapy: ≤40 mg/day), an antimalarial, azathioprine (≤200 mg/day), mizoribine (≤150 mg/day), mycophenolate mofetil (≤2 g/day) or mycophenolic acid (≤1.44 g/day), or MTX (≤25 mg/week) | • Clinical diagnosis according to ACR criteria • BILAG domain score: ≥1 A or ≥2 B • PGA of disease activity score ≥1 • Seropositive for antinuclear antibodies (titer ≥1:80), or anti-dsDNA antibodies, or anti-Smith antibodies | • Active severe SLE-driven renal disease • Active severe or unstable neuropsychiatric SLE • Prior treatment with a small-molecule/biological investigational agent within 4 weeks or five half-lives, whichever was greater | [31] |
| TULIP-2 (NCT02446899) | III | 52 weeks | 18–70 years | ≥6† | Ongoing stable treatment regimen with at least one of either prednisone or equivalent (monotherapy: 7.5–40 mg/day; combination therapy: ≤40 mg/day), an antimalarial, azathioprine (≤200 mg/day), mizoribine (≤150 mg/day), mycophenolate mofetil (≤2 g/day) or mycophenolic acid (≤1.44 g/day), or MTX (≤25 mg/week) | • Clinical diagnosis according to ACR criteria • Organ domain score: ≥1 A or ≥2 B • PGA of disease activity score ≥1 • Seropositive for antinuclear antibodies (titer ≥1:80), or anti-dsDNA antibodies, or anti-Smith antibodies | • Active severe SLE-driven renal disease • Active severe or unstable neuropsychiatric SLE • Prior treatment with a small-molecule/biological investigational agent within 4 weeks or five half-lives, whichever was greater | [32] |
| Belimumab | ||||||||
| BLISS-52 (NCT00424476) | III | 52 weeks | ≥18 years | ≥6‡ | Ongoing stable treatment regimen with at least one of either corticosteroids (prednisone or prednisone equivalent; monotherapy 7.5–40 mg/day; combination therapy 0–40 mg/day) or NSAIDs, antimalarials, or immunosuppressive/ immunomodulatory agents for at least 30 days prior to the first study dose | • Clinical diagnosis according to ACR criteria • Unequivocally positive ANA test results from two independent time points: positive ANA test (titer ≥1:80) and/or positive anti-dsDNA (≥30 IU/ml) serum antibody | • Severe lupus kidney disease • Active CNS lupus • Prior treatment with a biological investigational agent in the past year | [16] |
| BLISS-76 (NCT00410384) | III | 76 weeks§ | ≥18 years | ≥6‡ | Ongoing stable treatment regimen with at least one of either corticosteroids (prednisone or prednisone equivalent; monotherapy 7.5–40 mg/day; combination therapy 0–40 mg/day) or NSAIDs, antimalarials, or immunosuppressive/immunomodulatory agents for at least 30 days prior to the first study dose | • Clinical diagnosis according to ACR criteria • Unequivocally positive ANA test results from two independent time points: positive ANA test (titer ≥1:80) and/or positive anti-dsDNA (≥30 IU/mL) serum antibody | • Severe lupus kidney disease • Active CNS lupus • Prior treatment with a biological investigational agent in the past year | [17] |
†
Scores were calculated using the SLEDAI-2K global score. A score of 6 or higher (excluding points attributable to fever, lupus-related headache or organic brain syndrome) and a score on the clinical SLEDAI-2K (SLEDAI-2K without laboratory results) of 4 or higher were acceptable for study entry.
‡
Scores were calculated using the Safety of Estrogens in Lupus Erythematosus National Assessment (SELENA) version of the SLEDAI score. Scores of ≥6 were acceptable for study entry.
§
Primary efficacy end point reported at 52 weeks.
ACR: American College of Rheumatology; ANA: Antinuclear antibody; BICLA: BILAG-based Composite Lupus Assessment; BILAG: British Isles Lupus Assessment Group; CNS: Central nervous system; ITC: Indirect treatment comparison; MTX: Methotrexate; NSAIDs: Non-steroidal anti-inflammatory drugs; PGA: Physician’s Global Assessment; SLE: Systemic lupus erythematosus; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index.
Outcomes
Four outcomes were reported and feasible to compare between the TULIP and BLISS studies: proportion of patients with ≥4-point reduction in SLEDAI-2K score from baseline to week 52; proportion of patients who achieved an SRI-4 response at week 52; proportion of patients with BILAG flares (one or more new A or two or more new B) from baseline to week 52; and proportion of patients who achieved a reduction in OCS dose to ≤7.5 mg sustained from week 40 to week 52. The BICLA was not developed until after the BLISS trials were under way [46], and the individual BICLA components were not reported in the BLISS publications [16,18]. Similarly, other target outcomes could not be assessed because they were not reported for BLISS-52 and BLISS-76. Overall, outcome definitions were similar between the trials, or the outcome reported in BLISS publications could be replicated from the TULIP IPD.
While the TULIP studies used the SLEDAI-2K global and the BLISS studies used the Safety of Estrogens in Lupus Erythematosus: National Assessment SLEDAI, these measures share many similarities [47,48] and so it was concluded that, for the purposes of this analysis, the potential impact of their differences was not considered to be important.
While the definition of the ‘OCS dose reduction’ end point differed slightly between TULIP and BLISS, the OCS tapering approach differed significantly between trials. TULIP-1 and TULIP-2 mandated a tapering attempt for all patients receiving OCS ≥10 mg/day at baseline to ≤7.5 mg/day between weeks 8 and 40. Patients who achieved a reduction in OCS dose from ≥10 to ≤7.5 mg/day at week 40 through week 52 were defined as ‘OCS dose reduction’ in the TULIP studies [31,32]. In contrast, OCS tapering in BLISS-52 and BLISS-76 was at the investigators’ discretion, with no restrictions on OCS dose during the first 24 weeks (after which the dose needed to return to within 25% or 5 mg of the baseline dose, with no further increases for the remainder of the study) [16,18]. OCS dose reduction in the BLISS studies was defined by patients who reduced their OCS dose by ≥25% from baseline to ≤7.5 mg/day during weeks 40 to 52 [16,18]. To mitigate the impact of these differences, pooled data from patients in BLISS-52 and BLISS-76 who were receiving OCS at baseline (i.e., excluding patients not receiving any OCS) [21] were used for the OCS dose reduction outcome only.
Baseline characteristics
Pooled baseline patient characteristics for the anifrolumab and belimumab studies are shown in Table 2. Several characteristics identified as TEMs were similar between TULIP and BLISS. However, the mean SLEDAI-2K score in the TULIP studies was higher than in the BLISS studies, with a greater proportion of patients with one or more new BILAG A items or two or more new BILAG B items, and lower prevalence of low complement (C3/C4) or elevated anti-dsDNA (Table 2).
| Baseline characteristic | BLISS-52 and BLISS-76 (pooled) | TULIP-1 and TULIP-2 (pooled) |
|---|---|---|
| Female (proportion) | 94.1% | 92.8% |
| White race (proportion) | 47.4% | 66.0% |
| Age (mean [SD]) | 37.8 (11.5) | 41.8 (11.9) |
| Body mass index (kg/m2) (mean [SD]) | 25.1 (5.4)† | 27.6 (6.8) |
| SLEDAI score (mean [SD]) | 9.7 (3.8) | 11.4 (3.8) |
| BILAG ≥1 A or ≥2 B (proportion) | 60.8% | 94.4% |
| ANA titer ≥1:80 (proportion) | 93.0% | 90.0% |
| Abnormal low C3 (proportion) | 45.0% | 36.8% |
| Abnormal low C4 (proportion) | 56.1% | 50.7% |
| Anti-dsDNA ≥30 IU/ml (proportion) | 69.4% | 31.0% |
| Antimalarial use (proportion) | 65.3% | 70.3% |
| Azathioprine use (proportion) | 23.1% | 16.9% |
| Methotrexate use (proportion) | 13.7% | 17.8% |
| Mycophenolate use (proportion) | 11.2% | 13.6% |
| OCS dose >7.5 mg (proportion) | 58.0% | 52.6% |
†
Source: van Vollenhoven [21], which reports a subgroup of the BLISS-52 and BLISS-76 patients.
ANA: Antinuclear antibody; BILAG: British Isles Lupus Assessment Group; OCS: Oral corticosteroid; SD: Standard deviation; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index.
Indirect treatment comparisons
A summary of ITC results is presented in Table 3.
| Outcome | Unadjusted data | Primary ITC: STC results | Sensitivity ITC: MAIC results | |||
|---|---|---|---|---|---|---|
| Anifrolumab vs placebo (pooled TULIP-1 and TULIP-2) | Belimumab vs placebo (pooled BLISS-52 and BLISS-76) | Anifrolumab vs belimumab (ITC results) | n of TULIP patients | Anifrolumab vs belimumab (ITC results) | Neff of TULIP patients | |
| ≥4-point reduction in SLEDAI OR (95% CI) | 1.60 (1.19–2.15) | 1.61 (1.27–2.04) | 2.47 (1.16–5.25) | 709 | 2.74 (1.05–7.16) | 72 |
| SRI-4 response OR (95% CI) | 1.63 (1.21–2.19) | 1.63 (1.29–2.07) | 2.61 (1.22–5.58) | 710 | 2.91 (1.14–7.46) | 71 |
| BILAG flares OR (95% CI) | 0.67 (0.50–0.91) | 0.71 (0.55–0.92) | 0.76 (0.36–1.60) | 710 | 0.96 (0.34–2.67) | 78 |
| OCS reduction OR (95% CI) | 1.87 (1.39–2.51) | 1.59 (1.03–2.47)† | 0.99 (0.45–2.22) | 703 | NA‡ | NA‡ |
Note that the direction of effect differs by outcome depending on whether the outcome is positive or negative. For positive outcomes (ie, SLEDAI response, SRI[4] response, and OCS reduction), an OR of greater than 1 indicates a favorable treatment effect is associated with anifrolumab. For negative outcomes (ie, BILAG flares), an OR of less than 1 indicates a favorable treatment effect is associated with anifrolumab. If the 95% CI does not cross 1, this indicates the result is statistically significant.
†
The source of data for BLISS for the outcome of OCS reduction only was from the pooled publication van Vollenhoven et al., [21].
‡
The indicated analysis could not run.
BILAG: British Isles Lupus Assessment Group; ITC: Indirect treatment comparison; MAIC: Matching-adjusted indirect comparison; NA: Not applicable; n: Sample size; Neff: Effective sample size; OCS: Oral corticosteroid; OR: Odds ratio; SLE: Systemic lupus erythematosus; SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; STC: Simulated treatment comparison; SRI-4: SLE Responder Index-4.
Proportion of patients with reduction of four or more points in SLEDAI score from baseline to week 52
Unadjusted data showed that both anifrolumab and belimumab were associated with a beneficial treatment response versus placebo, as measured by at least a four-point improvement in SLEDAI score at week 52 (Table 3). Both the primary STC analysis and the supporting MAIC analysis showed that anifrolumab-treated patients were significantly more likely than belimumab-treated patients to achieve a SLEDAI response (reduction by at least four points) at week 52 (STC: OR: 2.47; 95% CI: 1.16–5.25; MAIC: OR: 2.74; 95% CI: 1.05–7.16) (Figure 1).

Figure 1. Odds ratios for achieving at least a four-point reduction in Systemic Lupus Erythematosus Disease Activity Index score from baseline to week 52.
Note: the ‘n’ associated with the MAIC result is an effective sample size of TULIP patients after reweighting included patients.
MAIC: Matching-adjusted indirect treatment comparison; n: Sample size; STC: Simulated treatment comparison.
Proportion of patients who achieved an SRI-4 response at week 52
Unadjusted data showed that both anifrolumab and belimumab were associated with a beneficial treatment response versus placebo, as measured by SRI-4 response at week 52 (Table 3). As with the SLEDAI response, anifrolumab-treated patients were significantly more likely than belimumab-treated patients to achieve an SRI-4 response at week 52, in both the primary STC analysis and the supporting MAIC analysis (STC: OR: 2.61; 95% CI: 1.22–5.58; MAIC: OR: 2.91; 95% CI: 1.14–7.46) (Figure 2).

Figure 2. Odds ratios for achieving a SRI-4 response at week 52.
Note: the ‘n’ associated with the MAIC result is an effective sample size of TULIP patients after reweighting included patients.
MAIC: Matching-adjusted indirect treatment comparison; n: Sample size; STC: Simulated treatment comparison.
Proportion of patients with BILAG flares (one or more new A or two or more new B Items) at week 52
Both anifrolumab and belimumab were associated with a significant reduction in the proportion of patients experiencing BILAG flares during the first year of treatment compared with placebo in the unadjusted analysis (Table 3). Comparing anifrolumab with belimumab, the effect estimate was not statistically significant for either the STC or the MAIC (Figure 3).
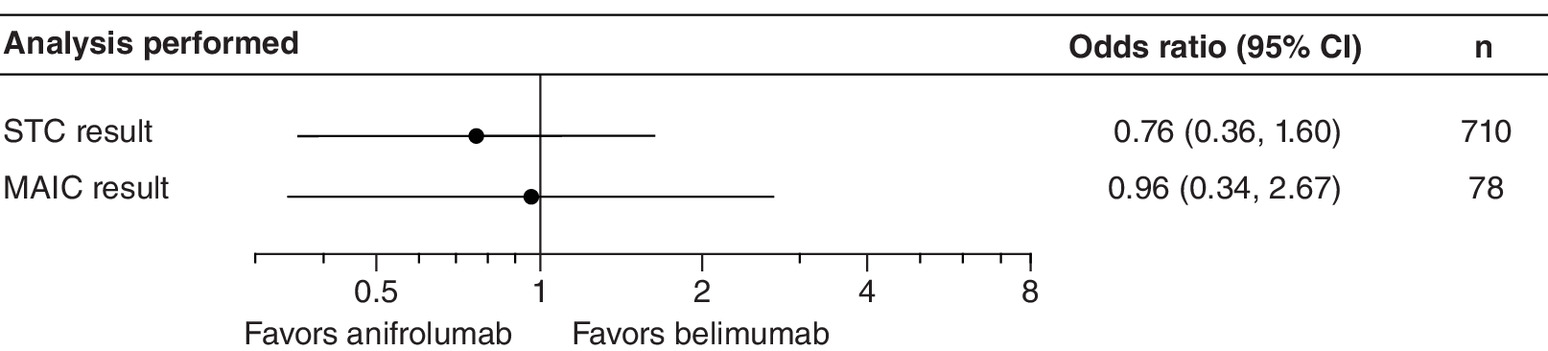
Figure 3. Odds ratios for severe British Isles Lupus Assessment Group flares (one or more new A or two or more new B) from baseline to week 52.
Note: the ‘n’ associated with the MAIC result is an effective sample size of TULIP patients after reweighting included patients.
MAIC: Matching-adjusted indirect treatment comparison; n: Sample size; STC: Simulated treatment comparison.
Proportion of patients who achieved a reduction in OCS dose to ≤7.5 mg sustained from week 40 to week 52
Anifrolumab- and belimumab-treated patients were more likely than placebo-treated patients to achieve a sustained reduction in OCS dose during the first year of therapy in the unadjusted analysis (Table 3). Despite the differences in OCS reduction definition and dose tapering approach between the TULIP and BLISS trials, no difference between anifrolumab and belimumab was detected in the STC analysis (Figure 4). The MAIC analysis could not be performed due to insurmountable differences in patient characteristics.
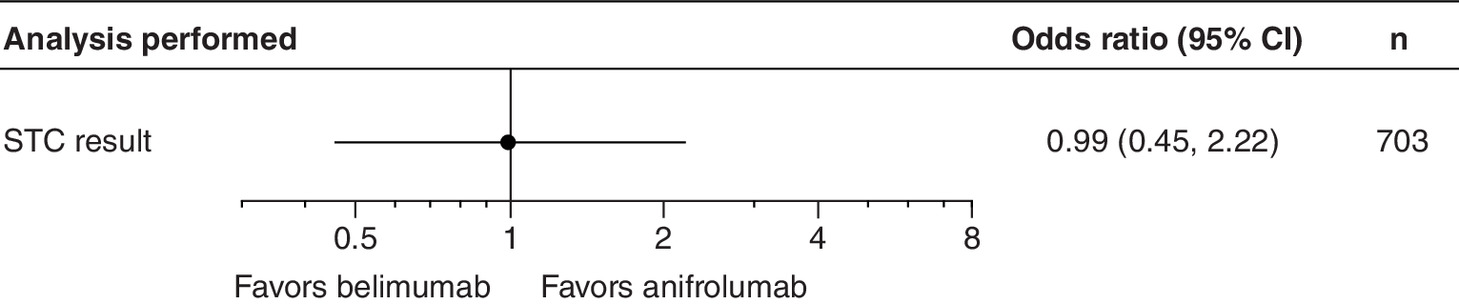
Figure 4. Odds ratio for achieving a reduction in oral corticosteroid dose to 7.5 mg or less, sustained from week 40 to week 52, among patients with a baseline dosage of ≥10 mg per day.
Note: the matching-adjusted indirect treatment comparison analysis could not be undertaken for this outcome so only the STC is presented. The results should be interpreted with caution due to differences in outcome definition between the trials. The source of efficacy data for belimumab for this outcome is van Vollenhoven et al. [21].
n: Sample size; STC: Simulated treatment comparison.
Sensitivity analyses
Results of additional sensitivity analyses can be found in the Supplementary Data. Findings of the sensitivity analyses that included the MUSE study and the BLISS-SC study support the results of the primary STC analyses for SLEDAI and SRI-4 responses.
A MAIC was not feasible for the OCS dose reduction outcome because of the very small effective sample size. In the limited TEMs scenario, the MAIC result was numerically in favor of anifrolumab but the effect estimate was not statistically significant (data not shown).
Discussion
In this study we utilized IPD from the TULIP clinical trials and pooled data from the BLISS clinical trials to compare the efficacy of anifrolumab and belimumab in adults with moderate-to-severe SLE who are receiving standard therapy. Based on population-adjusted ITCs, anifrolumab (300 mg iv.) was associated with significantly greater treatment benefits than belimumab (10 mg/kg iv.) for the outcomes of SLEDAI reduction of at least four points and SRI-4 response at 52 weeks.
Both anifrolumab and belimumab have demonstrated clinically important benefits in markers of disease activity and severity compared with placebo when administered to adults with moderate-to-severe active SLE receiving standard therapy [15,22,26]. In the absence of head-to-head studies, comparative evidence from ITC analyses can provide clinical and healthcare decision-makers with information about the relative efficacy of the available treatments [37,38], making ITC a valuable tool for health technology assessment that is now widely used and endorsed by regulatory bodies and reimbursement agencies [38,43,49–51].
Traditional, unadjusted ITC methods, such as network meta-analysis, rely on an assumption that important patient characteristics are balanced across trials. However, when clinically important covariates differ substantially between trials, this assumption cannot be upheld, and population-adjusted methods are more appropriate [38,51]. Patient characteristics in the TULIP and BLISS studies differed markedly, considering the similar study designs and eligibility criteria. Our feasibility assessment identified substantial differences between trials for patient characteristics that are TEMs, which might potentially bias unadjusted ITC methods. We therefore conducted ITCs while adjusting for potential sources of bias: key differences in baseline characteristics and eligibility criteria between the anifrolumab and belimumab studies were addressed by utilizing IPD for the TULIP-1 and TULIP-2 trials to perform population-adjusted comparisons. This adjustment of the anifrolumab patient population to match more closely the population enrolled in the belimumab trials reduced the risk of bias and improved the credibility of results. STCs and MAICs provided a full, nuanced picture of the relative efficacy of anifrolumab versus belimumab, and sensitivity analyses were conducted to address potential limitations and impacts of assumptions; the results were consistent. To our knowledge, this is the first study to use STC or MAIC methods to compare the efficacy of anifrolumab with belimumab in patients with moderate-to-severe SLE receiving standard therapy.
The STC and MAIC results both demonstrated that anifrolumab was associated with statistically significant improvement compared with belimumab for both SLEDAI response and SRI-4 response. The congruence of these two outcomes is not surprising, because SLEDAI is a driving component of the composite outcome, SRI-4. A four-point, or more, improvement in SLEDAI is a key goal in the management of SLE because it is associated with achievement of a lower disease activity state and improved outcomes [39]. The association between SLEDAI score and organ damage [52,53] also suggests that assessing the relative efficacy of treatments in terms of SLEDAI reduction may represent value for decision-makers to help patients with SLE achieve their treatment goals. The considerable between-trial differences in baseline SLEDAI and BILAG parameters show that, despite similar enrollment criteria, the TULIP population had more active SLE than the BLISS population. The higher SLEDAI scores in the TULIP population were likely driven by more active clinical disease and active organ involvement, as 94% of patients had one or more BILAG A items or two or more B items, compared with 61% of the BLISS population. In contrast, the SLEDAI scores in the BLISS population were more driven by serology, as demonstrated by the higher prevalence of elevated anti-dsDNA and low complement. In this context, the observed differences in treatment effect in favor of anifrolumab have clinical relevance, because clinical disease activity likely drives more of the SLEDAI and SRI-4 outcomes assessed in this comparison. This suggests that anifrolumab may have greater clinical efficacy than belimumab.
The BICLA composite index is used as a measure of improvement in overall disease activity [39]. To be classified as a BICLA responder, a patient must show an improvement in all affected organs [39]. In a post hoc analysis of pooled data from TULIP-1 and TULIP-2, BICLA responders were more likely to show an improvement in flare rate and patient-reported outcomes and a reduction in mean daily OCS dosage than BICLA nonresponders, illustrating that BICLA response aligns with goals in clinical practice [54]. Although BICLA results were available for the TULIP trials, this outcome measure was developed after the BLISS trials were near completion and so these were not available for belimumab [16,18,46]. The BICLA response can be derived from the same components of SRI-4; therefore future analyses of belimumab data may report BICLA as a post hoc outcome, permitting ITC of BICLA response.
In view of the impact of long-term or high-dose OCS treatment on organ damage, OCS dose reduction is an important clinical outcome to evaluate in the treatment of SLE [10–12]. Pivotal anifrolumab and belimumab trials showed that a greater proportion of patients achieved a reduction in OCS dosage with biological treatment than with a placebo [16,18,31,32,34], as reflected in our unadjusted analysis. Between-trial differences in OCS tapering protocols, including direction for mandatory or discretionary tapering, compromised evaluation of this outcome. Using a more comparable BLISS subgroup [21] for the OCS reduction outcome mitigated some, but not all, of the between-trial differences, and the ITCs were ultimately inconclusive. Given these limitations, the STC analysis detected no treatment difference, whereas insufficient overlap in the most impactful TEMs prevented the MAIC analysis. Because the direction and magnitude of potential bias for the OCS reduction outcome is unknown, these results should be interpreted with caution. Development of a standardized procedure for managing and accounting for OCS use in clinical trials would facilitate future comparisons of treatment effects.
Potential limitations of this study include assumptions inherent to all STCs. Measurement of individuals not assigned to the trial is outside the scope of the analysis, so homogeneity of effects (that the outcomes of either treatment or placebo are the same whether or not the patient was included in the trial) [43] is uncertain. Unobserved differences in TEMs may affect the conditional constancy of relative effects assumption (that the relative treatment effects are constant between studies at any specified covariate value) [51]. However, basing our analyses exclusively on well-conducted randomized controlled trials likely meets other STC assumptions, such as stable unit treatment value and ignorable treatment assignment. STCs address major limitations of unadjusted ITCs by accounting for between-trial differences. However, absence of reported patient characteristics in some trials can lead to differences that cannot be adjusted for across outcomes. For example, BMI was reported for a sub-analysis of OCS reduction in the BLISS trials [21] but not in BLISS-52 or BLISS-76. Nevertheless, because all included trials were placebo controlled, the analyses were anchored by way of a placebo arm, which eliminates a potential source of confounding by controlling for known and unknown prognostic factors. Identification and selection of TEMs also present challenges in data interpretation. In STC, all TEMs and prognostic variables are assumed to be balanced between groups, whereas in MAIC, the inclusion of purely prognostic variables in addition to TEMs has the potential to cause over-matching between groups [43]. Because information on TEMs for SLE treatment is not widely reported in the literature, distinguishing between TEMs and prognostic variables is difficult. To supplement the limited evidence available [55], we drew on expert clinical opinion to define TEMs for this study.
Conclusion
In the absence of head-to-head studies, this population-adjusted comparative study provides insights to decision-makers and clinicians about the comparative efficacy of anifrolumab and belimumab in patients with moderate-to-severe SLE who are receiving standard therapy. After adjusting for important cross-trial differences, anifrolumab (300 mg iv.) was associated with significantly greater treatment benefits than belimumab (10 mg/kg iv.) in the outcomes of SLEDAI response (reduction of four or more points) and SRI-4 response at 52 weeks, suggesting that, compared with belimumab, patients with moderate-to-severe SLE may be more likely to show improvement in clinical disease activity when treated with anifrolumab.
•
Two biological therapies are currently approved for the treatment of moderate-to-severe systemic lupus erythematosus (SLE): belimumab (approved in 2011) and anifrolumab (approved in 2021).
•
Both belimumab and anifrolumab have demonstrated efficacy in the treatment of SLE, but no direct head-to-head comparisons have been evaluated.
•
We conducted population-adjusted indirect treatment comparisons, in the form of simulated treatment comparisons and matching-adjusted indirect comparisons, to estimate the relative efficacy of anifrolumab versus belimumab.
•
Individual patient data were available from the anifrolumab TULIP-1 and TULIP-2 trials, and summary-level data were taken from the belimumab BLISS-52 and BLISS-76 trials.
•
Patients in the TULIP trials had higher baseline SLE Disease Activity Index (SLEDAI) (mean: 11.4 [standard deviation: 3.8] vs 9.7 [standard deviation: 3.8]) and British Isles Lupus Assessment Group organ involvement (94 vs 61%) than patients in the BLISS trials, suggesting that the TULIP population had more active SLE than the BLISS population.
•
Compared with belimumab, anifrolumab had greater treatment benefits, as measured by SLEDAI and SLE Responder Index-4 (SRI-4), in patients with moderate-to-severe SLE who were receiving standard therapy.
•
Anifrolumab-treated patients were more likely to achieve a reduction of four or more points on the SLEDAI (odds ratio: 2.47; 95% CI: 1.16–5.25) and achieve an SRI-4 response (odds ratio: 2.61; 95% CI: 1.22–5.58) than belimumab-treated patients.
•
In the absence of head-to-head studies, this population-adjusted comparative study provides insights to decision-makers and clinicians about the comparative efficacy of anifrolumab and belimumab in patients with moderate-to-severe active SLE who are receiving standard therapy.
Author contributions
All authors contributed to the development of the manuscript, including interpretation of results, substantive review of drafts and approval of the final draft for submission. I Bruce and R Tummala were responsible for study conception, design, and critical review and revision of the manuscript; S Golam was responsible for study conception, design and data analysis, developed the first draft of the manuscript, and was responsible for subsequent critical review and revision of the manuscript; J Steenkamp, P Wang and E Worthington were responsible for acquisition of data, data analysis and critical review and revision of the manuscript; B Desta, K Psachoulia and W Erhardt were responsible for data analysis and critical review and revision of the manuscript.
Acknowledgments
I Bruce is a National Institute for Health Research (NIHR) Senior Investigator Emeritus and is funded by the NIHR Manchester Biomedical Research Centre. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Financial & competing interests disclosure
This work was supported by AstraZeneca. I Bruce has received grant support from Genzyme/Sanofi, GSK, Roche and UCB; consulting fees from AstraZeneca, Lilly, GSK, Merck Serono, UCB and ILTOO; and was a speaker for AstraZeneca, GSK and UCB. S Golam, B Desta, K Psachoulia, W Erhardt and R Tummala are employees of AstraZeneca. J Steenkamp, P Wang and E Worthington are employees of EVERSANA™, which was contracted by AstraZeneca to work on this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing and editorial support were provided by R Franklin of JK Associates Inc., part of Fishawack Health, and were funded by AstraZeneca.
Ethical conduct of research
As this study involved deidentified data and data sets that exist in the public domain, it was exempted from the need for institutional or national review committee approval.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of these shared data is in accordance with the terms agreed upon their receipt. Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data sharing policy, described at: https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials (1).docx)
- Download
- 277.04 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Barber MRW, Drenkard C, Falasinnu T et al. Global epidemiology of systemic lupus erythematosus. Nat. Rev. Rheumatol. 17(9), 515–532 (2021).
2.
Justiz Vaillant AA, Goyal A, Bansal P, Varacallo M. Systemic Lupus Erythematosus. StatPearls Publishing, FL, USA (2021).
3.
Crow MK. Type I interferon in the pathogenesis of lupus. J. Immunol. 192(12), 5459–5468 (2014).
4.
Crow MK, Olferiev M, Kirou KA. Type I interferons in autoimmune disease. Annu. Rev. Pathol. 14, 369–393 (2019).
5.
Mai L, Asaduzzaman A, Noamani B et al. The baseline interferon signature predicts disease severity over the subsequent 5 years in systemic lupus erythematosus. Arthritis Res. Ther. 23(1), 29 (2021).
6.
Rönnblom L, Leonard D. Interferon pathway in SLE: one key to unlocking the mystery of the disease. Lupus Sci. Med. 6(1), e000270 (2019).
7.
Fanouriakis A, Bertsias G. Changing paradigms in the treatment of systemic lupus erythematosus. Lupus Sci. Med. 6(1), e000310 (2019).
8.
Fanouriakis A, Kostopoulou M, Alunno A et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 78(6), 736–745 (2019).
9.
van Vollenhoven RF, Mosca M, Bertsias G et al. Treat-to-target in systemic lupus erythematosus: recommendations from an international task force. Ann. Rheum. Dis. 73(6), 958–967 (2014).
10.
Bruce IN, O’Keeffe AG, Farewell V et al. Factors associated with damage accrual in patients with systemic lupus erythematosus: results from the Systemic Lupus International Collaborating Clinics (SLICC) inception cohort. Ann. Rheum. Dis. 74(9), 1706–1713 (2015).
11.
Durcan L, O’Dwyer T, Petri M. Management strategies and future directions for systemic lupus erythematosus in adults. Lancet 393(10188), 2332–2343 (2019).
12.
Segura BT, Bernstein BS, McDonnell T et al. Damage accrual and mortality over long-term follow-up in 300 patients with systemic lupus erythematosus in a multi-ethnic British cohort. Rheumatology (Oxford) 59(3), 524–533 (2020).
13.
Glaxo SmithKline. Benlysta US prescribing information (2021). https://gskpro.com/content/dam/global/hcpportal/en_US/Prescribing_Information/Benlysta/pdf/BENLYSTA-PI-MG-IFU.PDF
14.
European Medicines Agency. Benlysta: summary of product characteristics. www.ema.europa.eu/en/documents/product-information/benlysta-epar-product-information_en.pdf
15.
Levy RA, Gonzalez-Rivera T, Khamashta M et al. 10 Years of belimumab experience: what have we learnt? Lupus 30(11), 1705–1721 (2021).
16.
Furie R, Petri M, Zamani O et al. A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 63(12), 3918–3930 (2011).
•• Pivotal phase III publication of the primary comparator and source of belimumab data for the analyses.
17.
Iaccarino L, Bettio S, Reggia R et al. Effects of belimumab on flare rate and expected damage progression in patients with active systemic lupus erythematosus. Arthritis Care Res. (Hoboken) 69(1), 115–123 (2017).
18.
Navarra SV, Guzmán RM, Gallacher AE et al. Efficacy and safety of belimumab in patients with active systemic lupus erythematosus: a randomised, placebo-controlled, phase 3 trial. Lancet 377(9767), 721–731 (2011).
•• Pivotal phase III publication of the primary comparator and source of belimumab data for the analyses.
19.
Stohl W, Schwarting A, Okada M et al. Efficacy and safety of subcutaneous belimumab in systemic lupus erythematosus: a fifty-two-week randomized, double-blind, placebo-controlled study. Arthritis Rheumatol. 69(5), 1016–1027 (2017).
20.
van Vollenhoven RF, Navarra SV, Levy RA et al. Long-term safety and limited organ damage in patients with systemic lupus erythematosus treated with belimumab: a phase III study extension. Rheumatology (Oxford) 59(2), 281–291 (2020).
21.
van Vollenhoven RF, Petri M, Wallace DJ et al. Cumulative corticosteroid dose over fifty-two weeks in patients with systemic lupus erythematosus: pooled analyses from the phase III belimumab trials. Arthritis Rheumatol. 68(9), 2184–2192 (2016).
•• Pivotal pooled analysis of the primary comparator phase III data and source of belimumab data for the sensitivity analyses.
22.
Von Kempis J, Duetsch S, Reuschling N et al. Clinical outcomes in patients with systemic lupus erythematosus treated with belimumab in clinical practice settings: a retrospective analysis of results from the OBSErve study in Switzerland. Swiss Med. Wkly 149, w20022 (2019).
23.
Tanaka Y, Bae SC, Bass D et al. Long-term open-label continuation study of the safety and efficacy of belimumab for up to 7years in patients with systemic lupus erythematosus from Japan and South Korea. RMD Open 7(2), e001629 (2021).
24.
Wallace DJ, Ginzler EM, Merrill JT et al. Safety and efficacy of belimumab plus standard therapy for up to thirteen years in patients with systemic lupus erythematosus. Arthritis Rheumatol. 71(7), 1125–1134 (2019).
25.
Peng L, Oganesyan V, Wu H, Dall'Acqua WF, Damschroder MM. Molecular basis for antagonistic activity of anifrolumab, an anti-interferon-alpha receptor 1 antibody. MAbs 7(2), 428–439 (2015).
26.
Tanaka Y, Tummala R. Anifrolumab, a monoclonal antibody to the type I interferon receptor subunit 1, for the treatment of systemic lupus erythematosus: an overview from clinical trials. Mod. Rheumatol. 31(1), 1–12 (2021).
27.
US Food and Drug Administration. Saphnelo US prescribing information (2021). www.accessdata.fda.gov/drugsatfda_docs/label/2021/761123s000lbl.pdf
28.
AstraZeneca. Saphnelo approved in Japan for systemic lupus erythematosus (2021). www.astrazeneca.com/media-centre/press-releases/2021/saphnelo-approved-in-japan-for-sle.html
29.
AstraZeneca. Saphnelo recommended for approval in the EU by CHMP for the treatment of patients with systemic lupus erythematosus (2021). www.astrazeneca.com/media-centre/press-releases/2021/saphnelo-recommended-for-eu-approval-for-sle.html
30.
AstraZeneca. Saphnelo approved in the EU for thetreatment of moderate to severe systemic lupus erythematosus (2022). www.astrazeneca.com/media-centre/press-releases/2022/saphnelo-approved-in-eu-for-sle.html
31.
Furie R, Morand E, Bruce IN et al. Type I interferon inhibitor anifrolumab in active systemic lupus erythematosus (TULIP-1): a randomised, controlled, phase 3 trial. Lancet Rheumatol. 1(4), E208–E219 (2019).
•• Pivotal phase III publication of the anifrolumab efficacy data used for the analyses.
32.
Morand EF, Furie R, Tanaka Y et al. Trial of anifrolumab in active systemic lupus erythematosus. N. Engl. J. Med. 382(3), 211–221 (2020).
•• Pivotal phase III publication of the anifrolumab efficacy data used for the analyses.
33.
Chatham WW, Furie R, Saxena A et al. Long-term safety and efficacy of anifrolumab in adults with systemic lupus erythematosus: results of a phase II open-label extension study. Arthritis Rheumatol. 73(5), 816–825 (2021).
34.
Furie R, Khamashta M, Merrill JT et al. Anifrolumab, an anti-interferon-α receptor monoclonal antibody, in moderate-to-severe systemic lupus erythematosus. Arthritis Rheumatol. 69(2), 376–386 (2017).
•• Phase II publication of anifrolumab efficacy data and source of data used for the sensitivity analyses.
35.
Furie R, Morand EF, Askanase AD et al. Anifrolumab reduces flare rates in patients with moderate to severe systemic lupus erythematosus. Lupus 30(8), 1254–1263 (2021).
36.
Tummala R, Abreu G, Pineda L et al. Safety profile of anifrolumab in patients with active SLE: an integrated analysis of phase II and III trials. Lupus Sci. Med. 8(1), e000464 (2021).
37.
Jansen JP, Fleurence R, Devine B et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 1. Value Health 14(4), 417–428 (2011).
38.
Phillippo DM, Dias S, Ades AE, Welton NJ. Assessing the performance of population adjustment methods for anchored indirect comparisons: a simulation study. Stat. Med. 39(30), 4885–4911 (2020).
• Supports the use of simulated treatment comparisons as the base case.
39.
Arora S, Isenberg DA, Castrejon I. Measures of adult systemic lupus erythematosus: disease activity and damage. Arthritis Care Res. (Hoboken) 72(Suppl. 10), 27–46 (2020).
40.
Furie RA, Petri MA, Wallace DJ et al. Novel evidence-based systemic lupus erythematosus responder index. Arthritis Rheum. 61(9), 1143–1151 (2009).
41.
Castrejón I, Tani C, Jolly M, Huang A, Mosca M. Indices to assess patients with systemic lupus erythematosus in clinical trials, long-term observational studies, and clinical care. Clin. Exp. Rheumatol. 32(85 Suppl. 5), S-85-95 (2014).
42.
Isenberg D, Sturgess J, Allen E et al. Study of flare assessment in systemic lupus erythematosus based on paper patients. Arthritis Care Res. (Hoboken) 70(1), 98–103 (2018).
43.
Phillippo DM, Ades T, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU technical support document 18: methods for population-adjusted indirect comparisons in submissions to NICE (2016). https://research-information.bris.ac.uk/en/publications/nice-dsu-technical-support-document-18-methods-for-population-adj
• Provides the methodology for conducting indirect treatment comparisons.
44.
Stohl W, Schwarting A, Okada M et al. Efficacy and safety of subcutaneous belimumab in systemic lupus erythematosus: a fifty-two-week randomized, double-blind, placebo-controlled study. Arthritis Rheumatol. 69(5), 1016–1027 (2017).
45.
Zhang F, Bae SC, Bass D et al. A pivotal phase III, randomised, placebo-controlled study of belimumab in patients with systemic lupus erythematosus located in China, Japan and South Korea. Ann. Rheum. Dis. 77(3), 355–363 (2018).
46.
Wallace DJ, Kalunian KC, Petri MA et al. Epratuzumab demonstrates clinically meaningful improvements in patients with moderate to severe systemic lupus erythematosus (SLE): Results from EMBLEM™, a phase IIb study. Arthritis Rheum. 62(S10), S605 (2010).
47.
Parker B, Bruce IN. Clinical markers, metrics, indices, and clinical trials. In: Dubois’ Lupus Erythematosus and Related Syndromes. Wallace DJ, Hahn B (Eds). Elsevier, Amsterdam, The Netherlands (2019).
48.
Ohmura K. Which is the best SLE activity index for clinical trials? Mod. Rheumatol. 31(1), 20–28 (2021).
49.
National Institute for Heath and Care Excellence Decision Support Unit. Population-adjusted indirect comparisons (MAIC and STC). https://nicedsu.sites.sheffield.ac.uk/tsds/population-adjusted-indirect-comparisons-maic-and-stc
50.
Ivanescu C, Skaltsa K, Kráľ P. Acceptance of population-adjusted indirect treatment comparison methods in NICE assessments. Value Health 20, A399–811 (2017).
51.
Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for population-adjusted indirect comparisons in health technology appraisal. Med. Decis. Making 38(2), 200–211 (2018).
52.
Taraborelli M, Cavazzana I, Martinazzi N et al. Organ damage accrual and distribution in systemic lupus erythematosus patients followed-up for more than 10 years. Lupus 26(11), 1197–1204 (2017).
53.
Urowitz MB, Gladman DD, Ibanez D et al. Effect of disease activity on organ damage progression in systemic lupus erythematosus: University of Toronto lupus clinic cohort. J. Rheumatol. 48(1), 67–73 (2021).
54.
Furie R, Morand EF, Bruce IN et al. What does it mean to be a British Isles Lupus Assessment Group-Based Composite Lupus Assessment responder? Post hoc analysis of two phase III trials. Arthritis Rheumatol. 73(11), 2059–2068 (2021).
55.
van Vollenhoven RF, Petri MA, Cervera R et al. Belimumab in the treatment of systemic lupus erythematosus: high disease activity predictors of response. Ann. Rheum. Dis. 71(8), 1343–1349 (2012).
Information & Authors
Information
Published In
Pages: 765 - 777
PubMed: 35546484
Copyright
© 2022 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 25 February 2022
Accepted: 22 April 2022
Published online: 12 May 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Indirect treatment comparison of anifrolumab efficacy versus belimumab in adults with systemic lupus erythematosus. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0040
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Marco U. Martinez-Martinez, Paul J. Tejada-Llacsa, Larry J Prokop, Cynthia S. Crowson, M. Hassan Murad, Alí Duarte-García, Efficacy and safety of belimumab and anifrolumab in systemic lupus erythematosus: A systematic review and network meta-analysis, Seminars in Arthritis and Rheumatism, 10.1016/j.semarthrit.2026.153022, 79, (153022), (2026).
- Kai Wai Lee, Becky Hooper, Jason Steenkamp, Ian N Bruce, Methodological concerns and data discrepancies in the indirect treatment comparison of belimumab and anifrolumab, Zeitschrift für Rheumatologie, 10.1007/s00393-026-01838-w, (2026).
- Yi Liu, Ling Xiang, Rui-Juan Cheng, Shu-Yue Pan, Advances in understanding the Th17/Treg balance in systemic lupus erythematosus: implications for treatment and management, Frontiers in Immunology, 10.3389/fimmu.2026.1795760, 17, (2026).
- Hesham Almomani, Ahmad Al-Momani, Marya Al-Momani, A Comprehensive Synthesis of Healthcare Leadership and Continuous Improvement, Evaluating Healthcare Leadership (HCL) Effectiveness: A Comprehensive Approach for Organizational Success, 10.4018/979-8-3373-2225-4.ch003, (25-38), (2025).
- Ryota Sato, Masaru Shimizu, Yuya Kondo, Kazushi Maruo, Yuki Kuroda, Hiroshi Ebe, Mizuki Yagishita, Naoto Umeda, Seiji Mogi, Ayako Ohyama, Ayako Kitada, Saori Abe, Hiromitsu Asashima, Haruka Miki, Hiroto Tsuboi, Isao Matsumoto, Real-world effectiveness of belimumab and anifrolumab in systemic lupus erythematosus: comparable trends in disease activity and glucocorticoid reduction, Immunological Medicine, 10.1080/25785826.2025.2528296, 48, 4, (371-380), (2025).
- E. A. Pyadushkina, A. M. Lila, E. E. Yagnenkova, V. I. Ignatyeva, E. V. Derkach, New possibilities for the treatment of systemic lupus erythematosus. How much does the effect cost?, Modern Rheumatology Journal, 10.14412/1996-7012-2025-1-35-43, 19, 1, (35-43), (2025).
- Mochamad Rangga Alif Dharmawan, Maftuchah Rochmanti, undefined Awalia, Citrawati Dyah Kencono Wungu, Systematic Review and Meta-Analysis of the Efficacy and Safety Profile of Belimumab in Combination with Standard Therapy for Adults with Systemic Lupus Erythematosus, Current Internal Medicine Research and Practice Surabaya Journal, 10.20473/cimrj.v6i1.66383, 6, 1, (54-64), (2025).
- Alexander Blagov, Nikolay Orekhov, Alexey Churov, Irina Starodubtseva, Dmitry Beloyartsev, Tatiana Kovyanova, Vasily Sukhorukov, Alexander Orekhov, Current use and development of monoclonal antibodies for the treatment of systemic lupus erythematosus: a review, Antibody Therapeutics, 10.1093/abt/tbae033, 8, 1, (47-55), (2024).
- Alessio Mylonas, Neurological Impact of Type I Interferon Dysregulation, Rare Neurodegenerative Disorders - New Insights [Working Title], 10.5772/intechopen.1006023, (2024).
- Aleksandra Fijałkowska, Joanna Wojtania, Anna Woźniacka, Ewa Robak, Psoriasis and Lupus Erythematosus—Similarities and Differences between Two Autoimmune Diseases, Journal of Clinical Medicine, 10.3390/jcm13154361, 13, 15, (4361), (2024).
- See more