Design and methods of a tailored approach for diabetes prevention in women with previous gestational diabetes
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To describe the design and methods of an intervention that engaged women with previous gestational diabetes mellitus in a tailored approach for diabetes prevention. Methods: Women participated in biometric tests for BMI and hemoglobin A1c, psychosocial questionnaires and an informed decision-making process to select a lifestyle change program for Type 2 diabetes prevention based on their needs and priorities. Measure time points were at baseline, 6 months and 12 months. Results: The authors recruited 116 women. The outcomes of this study will evaluate the effect of this strategy on participant engagement in lifestyle change programs for Type 2 diabetes prevention. Conclusion: This paper describes a variety of lifestyle change programs and an informed decision-making process for tailoring diabetes prevention programs for a high-risk population.
Gestational diabetes mellitus (GDM), defined as the onset of glucose intolerance during pregnancy [1], is associated with increased risk for Type 2 diabetes (T2D) [2]. Women diagnosed with GDM have a 60% increased lifetime risk for developing T2D [2]. This is concerning, as T2D is a complex, chronic disease, and poor glycemic control predisposes individuals to a host of serious comorbidities, including cardiovascular disease, renal disease, retinopathy and neuropathy. T2D also adversely affects health-related quality of life [3] and decreases life expectancy [4,5].
Fortunately, T2D risk is attenuated by lifestyle modification in women with previous GDM [6]. The seminal Diabetes Prevention Program (DPP) lifestyle intervention decreased T2D risk by 50% in women with a history of GDM [6]. In fact, a variety of lifestyle change programs that focus on weight loss, including WW (formerly Weight Watchers) [7], health coaching [8] and web-based programs [9], are effective at mitigating T2D risk. However, diabetes prevention interventions targeting women of childbearing age often report low levels of engagement [10,11] due to competing responsibilities of home, work and parenthood [12].
Engagement in diabetes prevention programs is also impacted by T2D risk perception. Kim and colleagues reported that while women are often aware of GDM as a risk factor for T2D, many do not perceive themselves to be at higher risk [13]. This is troublesome, as higher risk perception is indicative of intentions to engage in lifestyle changes [13,14]. For these reasons, women with a history of GDM need accurate information about their individual risk for T2D [15] along with tailored options for lifestyle change programs that meet their needs [12,16].
‘Informed decision making’ refers to a patient–clinician partnership where clinicians provide relevant information for decision making and the patients decide on their preferred mode of treatment [17]. Shared decision making, similar to informed decision making, has been shown to increase knowledge of T2D prevention options and engagement in diabetes prevention programs [18]. Facilitating participant decision making by utilizing person-centered communication allows participants to discover their own key reasons for behavior changes based on their vision for their best health according to their values.
This paper describes the methods for a diabetes prevention intervention for women with a history of GDM that informs women of their T2D risk and evidence-based ways to decrease risk, informs women of available programs for T2D risk reduction and facilitates participation in their chosen program via a person-centered communication strategy that outlines their personal needs and values. The authors hypothesize that by using an informed decision-making approach for women at high risk for developing T2D, enrollment and engagement in lifestyle change programs will be increased. The objective of this study is to evaluate the impact of this strategy on engagement and retention in diabetes prevention interventions previously shown to be effective in preventing or delaying T2D.
Methods
Study design
This unrandomized cohort study recruited a total of 116 women with a history of GDM. Women participated in biometric tests for BMI and hemoglobin A1c (HbA1c), psychosocial questionnaires and an informed decision-making process to select a lifestyle change program. Measure time points were at baseline, 6 months and 12 months.
This study was approved by the Indiana University institutional review board. No research activities were conducted prior to informed consent.
COVID-adjusted time line
The study began recruitment in July 2019 and planned to complete recruiting in June 2020. However, the study was suspended in March 2020 due to the COVID-19 pandemic. Therefore, researchers adjusted study activities based on the university's research restart plans. Recruitment of new participants was on hold from March 2020 to October 2020. Research study visits for those already enrolled were stalled for approximately 1 month, and visits were revised to fit a hybrid design of online questionnaire completion and in-person biometric measurements via a drive-thru method at an approved study location site.
Participant eligibility
Eligible participants were 18 years of age or older and had a history of GDM and a BMI of ≥25 kg/m2. Exclusion criteria included pregnancy or a diagnosis of T2D.
Participant recruitment & screening
The researchers used non-probability sampling methods to identify participants in three ways (Figure 1). First, they partnered with the Regenstrief Institute, an Indiana University-affiliated research organization, to obtain contact information for women with a history of GDM. GDM diagnosis was identified through the electronic medical record. Contact information, date of birth, race, ethnicity and date of GDM diagnosis were uploaded into the study's REDCap [19] electronic database. Second, study coordinators from two GDM-related cohort studies, nuMoM2b (NCT01322529) and Hoosier Moms (NCT03696368), provided contact information for women who had completed the studies and indicated interest in participating in future research. Third, women could self-refer to the study. Study information was available on the Indiana Clinical and Translational Sciences Institute iConnect Clinical Trials Finder (https://research.indianactsi.org/).
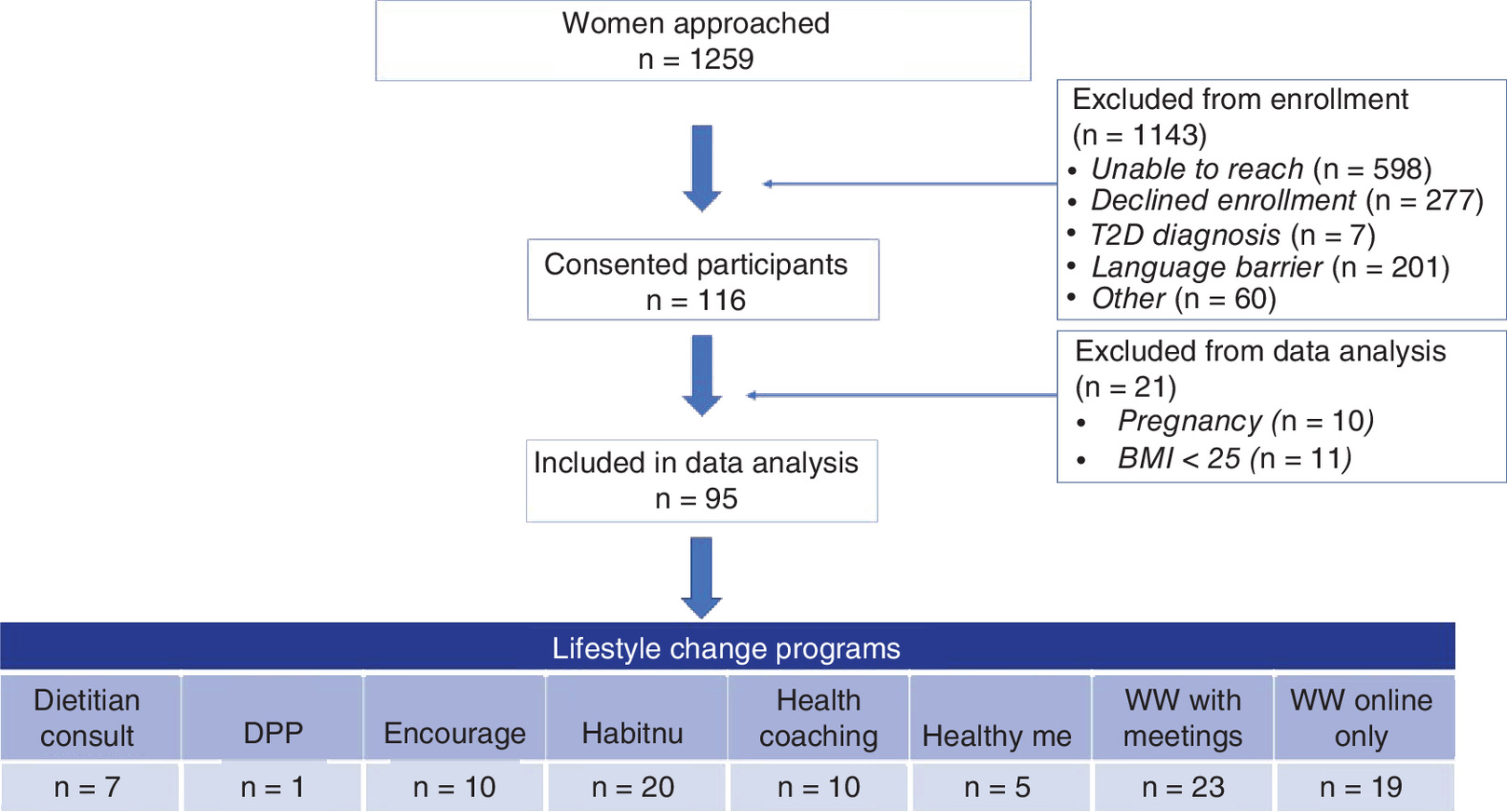
Figure 1. Consort Table: Flow diagram of recruitment and lifestyle change program selection.
DPP: Diabetes Prevention Program; T2D: Type 2 diabetes.
Potential participants were initially contacted with study information letters mailed directly to their home addresses on file. After approximately 3 days, study staff followed up with phone calls to ascertain interest and eligibility. Potential participants were contacted initially by phone when recruitment resumed after the COVID-19 suspension.
Research visit
Interested participants were scheduled for in-person data collection visits. Participants completed the informed consent process, biometric measures, psychosocial surveys and informed decision-making activities. Follow-up data collection visits at 6 and 12 months consisted of biometric measures and surveys. Participants received a US$30, $40 and $50 gift card for their time at baseline, 6-month and 12-month data collection visits, respectively.
COVID-19 modifications
Hybrid data collection model
A hybrid data collection model was implemented from April 2020 until study end as a result of the COVID-19 pandemic.
Online survey data collection
Staff scheduled interested participants for Zoom baseline visits. During the Zoom visit, participants completed the informed consent process and indicated consent, surveys and informed decision-making process. Participants accessed surveys directly online using the REDCap system. Staff scheduled participants for in-person biometric data collection, and participants received partial compensation (US$10) via electronic gift card.
Participants at 6-month or 12-month study time points received emails to complete surveys online and schedule an in-person biometric data collection visit.
In-person biometric data collection
Staff offered drive-thru appointments to collect height, weight and point-of-care HbA1c measurements. Biometric measurements were taken in a private room located off a side entrance door. Participants parked by the side door and texted staff upon arrival. Staff asked COVID screening questions and instructed participants to enter the side door for height, weight and HbA1c measurement. Participants then returned to their car to await HbA1c results, complete any outstanding surveys and receive the remaining compensation via electronic gift card.
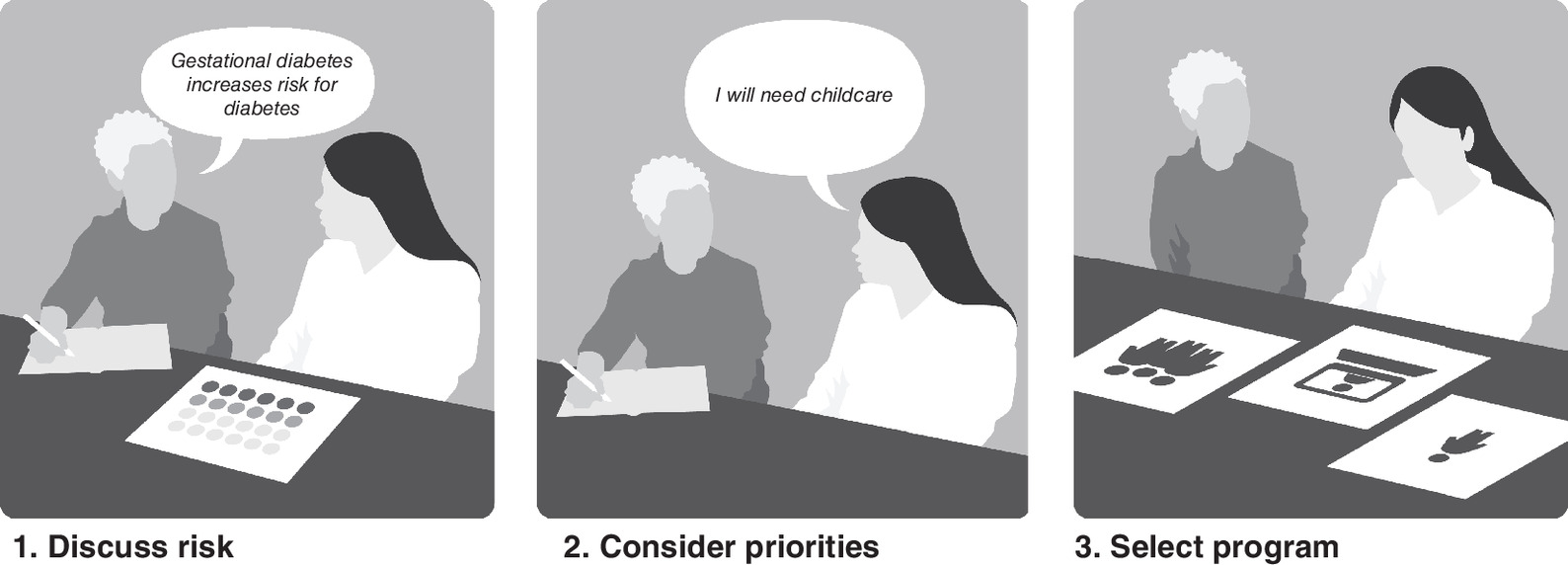
Informed decision-making process
T2D risk, prevention efficacy and lifestyle change program options are central factors in informed decision making for T2D prevention after GDM. Therefore, two activities were used to assist participants in this process. The first was a series of pictures that visually displayed T2D risk after GDM and potential risk reduction through lifestyle change. The second was a decision-making tool to assist in the selection of a lifestyle change program. The informed decision-making process was scripted and facilitated by a Certified Diabetes Care and Education Specialist and Certified Health Education Specialists (Figure 2).
T2D risk & prevention pictures
T2D risk after GDM and potential risk reduction were communicated visually and verbally through a series of three pictures. Participants were asked if they had questions throughout the discussion of T2D risk and prevention efficacy.
1.
The first picture displayed 100 blue dots that were arranged in a grid.
a.
Verbal description:
Each blue dot represents a woman who had GDM during a pregnancy.
2.
The second picture displayed 40 blue dots and 60 red dots.
a.
Verbal description:
Women with a history of gestational diabetes are at high risk of developing diabetes after the pregnancy.
The blue dots represent women with a history of gestational diabetes who do not develop diabetes.
The red dots represent women who develop diabetes after having gestational diabetes (this is without any steps taken to prevent diabetes).
This represents about a 60% risk of developing diabetes.
We don't know if you will be in the blue dots (no diabetes after having GDM) or in the red dots (diabetes after GDM).
3.
The third picture displayed 40 blue dots, 30 red dots and 30 green dots.
a.
Verbal description:
People can take steps to lower their risk of getting diabetes.
For women with a history of gestational diabetes, lifestyle changes lower diabetes risk by about half. If all of the women represented by the red dots engaged in lifestyle changes, about half would prevent diabetes.
The green dots represent women who made lifestyle changes and did not develop diabetes.
The red dots represent women who develop diabetes regardless of lifestyle changes.
We don't know if you will be in the blue dots (no diabetes after GDM) or the green dots (prevented diabetes through lifestyle change) or in the red dots (develop diabetes after GDM regardless of lifestyle change).
Informed decision-making tool
Decision aids are often used in the informed decision-making process to help individuals understand the pros and cons of their options and assess their preferences. The researchers developed an informed decision-making tool based on the Diabetes Medication Choice decision aid [20,21].
The Diabetes Medication Choice decision aid is a validated tool that uses cards to explore the potential effects of different diabetes medications [20,21]. Each card describes a potential medication effect. The patient decides on the first card to discuss, and the provider and patient use the cards to continue to discuss the pros and cons of medication options [20,21].
The researchers developed five cards to describe the different aspects of the lifestyle change programs. For instance, one card was titled ‘group’ or ‘one-on-one’. Underneath the title, each program was listed according to whether it was a group-based program or a one-on-one program. Participants could then see which programs met the criteria of interest. Card titles included childcare or no childcare, day or evening, in-person or virtual, group or one-on-one and program duration (one or two sessions, 3–6 months or 12 months).
Staff displayed the card titles and asked the participant, “Which aspect of a lifestyle change program is most important to you?” The participant selected the corresponding card. The staff member and participant discussed the lifestyle change programs that met the desired criteria. Next, the staff member asked, “What aspect would you like to discuss next?” The staff member and participant continued to discuss lifestyle change program details until the participant selected the program that was the best fit. Staff followed scripts for the informed decision-making process.
The informed decision-making tool is not a validated instrument, as it was developed to frame the discussion around the participants' priorities for a lifestyle change program rather than provide a certain outcome.
Surveys
Participants completed surveys to capture health and psychosocial factors.
Patient activation measure
The Patient Activation Measure (PAM) is a 13-item survey measuring an individual's ‘knowledge, skill, and confidence for managing health conditions’[22]. PAM scores indicate an individual's activation level: disengaged, increasing awareness, action or maintenance.
Adverse childhood experience questionnaire
The Adverse Childhood Experience (ACE) questionnaire is a 10-item tool that assesses 10 types of traumatic childhood experiences, including personal (abuse and neglect) and family-related factors (substance abuse, domestic abuse, mental illness, incarceration and abandonment) [23].
Multidimensional Health Locus of Control Scale
The Multidimensional Health Locus of Control (MHLC) scale, form A, is an 18-item survey that assesses an individual's belief about factors that influence health [24]. This questionnaire has three subscales that assess internal control, powerful others external control and chance.
Perceived Stress Scale Short Form
The Perceived Stress Scale Short Form is a four-item survey that uses a 5-point Likert scale to assess an individual's evaluation of stressful life situations over the previous month [25].
Medical Outcomes Study social support survey
The Medical Outcomes Study social support survey is 20-item tool that measures four domains of social support, including emotional, tangible, affectionate and positive social interaction [26].
International Physical Activity Questionnaire short form
The International Physical Activity Questionnaire (IPAQ) short form is a nine-item tool that uses open-ended questions to assess physical activity over the previous 7 days [27]. It assesses four levels of activity: vigorous-intensity, moderate-intensity, walking and sitting.
Medical Outcomes Study SF-12 health survey
The Medical Outcomes Study SF-12 is a 12-item survey that measures health-related quality of life [28]. The survey includes eight domains that assess limitations in physical, social and usual role activities due to physical or emotional problems and bodily pain. It includes perceptions of general health, mental health and vitality.
CoMac Descriptor tool
The CoMac Communication System is an online tool that provides immediate feedback and guidance to healthcare providers (HCPs) to help them communicate more effectively with patients who have chronic illnesses [29]. In short, the CoMac system provides HCPs with language that reflects patients' own worldviews and health beliefs.
Biometric data
Biometric data were captured to track progress across the 1-year study. Participant height, weight, BMI and HbA1c were measured at baseline, 6 months and 12 months. Height was measured with a stadiometer (SECA Model 213 1821009), weight was measured with a digital scale (Healthometer Professional Model 349KLXN, Dectecto Scale Model 758C), BMI was calculated in the REDCap system and point-of-care HbA1c was measured with an Alere Afinion AS100 machine (Alere, FL, USA).
Lifestyle change programs
The researchers selected seven lifestyle change programs to offer participants variety in regard to the mode of delivery, program duration, time of day, group versus individual format and childcare. Enrollment fees varied among programs and were paid for by the study. The study did not ascertain participants' access to computer or Internet services, nor did it pay for travel-related or computer/Internet expenses, as those considerations were part of the informed decision-making process.
Program selection criteria
In addition to providing a variety of options, lifestyle programs were selected based on the following criteria.
First, lifestyle change programs were required to be evidence-based interventions for reducing T2D risk. Three of the programs (National Diabetes Prevention Program [NDPP], Encourage Healthy Families [Encourage] and HabitNu) use the NDPP curriculum or adaptations of the curriculum. Participation in WW [7] and phone-based health coaching [8] are effective means for achieving lifestyle change for diabetes prevention. The American Diabetes Association recommends dietitian consults as an effective option for diabetes prevention [30,31].
It is notable that program duration varied significantly between some programs. The difference in duration allowed women to select the level of intensity that best suited their needs and preferences. The study outcomes will demonstrate if participants who identify as needing a less intense intervention can benefit from an abbreviated program, given the choice.
Second, in-person programs were required to be available within the geographic area of the research study. Last, program managers agreed to receive study referrals, report program participation to the study and receive payment from the research study.
National Diabetes Prevention Program
The NDPP is a lifestyle change program proven to reduce the risk of T2D [32]. This year-long, group-based program focuses on achieving 5–7% weight loss through healthy food choices and 150 minutes of moderate-intensity physical activity per week. Women were offered participation in the NDPP at one of the YMCA's 12 participating locations in the surrounding metropolitan area.
Encourage Healthy Families
Encourage Healthy Families (Encourage), a modified diabetes prevention program, is designed for women with a history of GDM and their children [10]. The Encourage program has the same program goals and duration as DPP, but the curriculum is modified to relate lifestyle change benefits for both the mom and her children. The session length increased from 60 to 90 min in order to include 30 min of physical activity. In addition, children ages 8–15 are offered youth-oriented sessions while moms attend the adult-focused sessions. Encourage is offered at a local fitness center and includes free childcare for children under the age of 8. Women who select Encourage receive a free membership to the fitness center for the duration of the program.
WW (formerly Weight Watchers)
WW is a point-based weight loss program that focuses on helping individuals create healthy habits through tracking food choices and attending group meetings. Study participants have the option of choosing WW tracking only through the app or WW with meetings for 3–6 months.
Healthy Me
Healthy Me is a local individualized health coaching program that supports clients to improve their overall health and well-being. Coaching is offered in a combination of in-person and phone visits based on individual preferences. Participants work with their health coach weekly for 8 weeks and then bi-weekly for the next 8 weeks. Healthy Me also offers a monthly support group meeting.
Dietitian consult
Patients meet one-on-one with a registered dietitian for guidance in making dietary and physical activity changes to reduce T2D risk. Sessions are personalized to meet individual needs. This program includes an initial consult and the option for a follow-up visit.
HabitNu
HabitNu is a web-based DPP. Participants track food choices and physical activity, learn educational content from videos and receive support from lifestyle coaches through the HabitNu app.
Health coaching
Patients work one-on-one with a health coach to learn about lifestyle changes to reduce T2D risk and set individualized goals. Patients talk with their health coach on the phone weekly for 12 weeks. Health coaches specialize in diabetes prevention.
Statistical analysis
The intention-to-treat principle will be used for all the analyses. Data include the primary outcome of program engagement and demographic, BMI, HbA1c and outcomes variables that are prespecified secondary study outcomes, from baseline through the final 12-month time point. Since the primary purpose is to assess engagement and retention in a variety of intervention programs as well as gather preliminary data on changes in primary outcome and differences between different intervention programs, the study was not designed to detect any group differences with certain power.
To evaluate changes for the group over time, paired t-tests will be used to compare changes in BMI, HbA1c and secondary outcomes from baseline to 12 months. Some participants will have missing data. Unmeasured outcome data after study withdrawal may be imputed using the final measured HbA1c and BMI for unmeasured values. A mixed-model analysis of covariance, including the terms, treatment group, time, race, age and baseline value of BMI, will be used to assess the effects of intervention at 6 and 12 months. An interaction effect between time and treatment group will be assessed first. If there is no interaction effect, the overall treatment difference will be assessed.
Participant descriptive statistics
Baseline characteristics of the participants are shown in Table 1. The researchers recruited 116 women with a mean age of 34.9. The majority of women were White (57.3%), followed by Black (18.2%) and Hispanic/Latino (11.8%). Approximately half had college degrees (47.3%), and the majority were married (69.6%). The mean BMI was 33.8 kg/m2 (standard deviation [SD]: 9.6) and the mean A1c was 5.3% (SD: 0.6).
| Characteristics | Participants (n = 116) |
|---|---|
| Age, years, mean (SD) | 34.9 (5.7) |
| Race/ethnicity, % | |
| – Asian | 3.6 |
| – Black or African American | 18.2 |
| – Hispanic/Latino | 11.8 |
| – Multi-racial | 7.3 |
| – Other | 1.8 |
| – White | 52.3 |
| Education level, % | |
| – Less than a high school degree | 3.5 |
| – High school diploma or GED | 12.1 |
| – Some college but no degree | 21.6 |
| – Associate degree | 15.5 |
| – Bachelor degree | 24.1 |
| – Graduate degree | 23.2 |
| Household income, % | |
| – Less than $25,000 | 15.9 |
| – $25,000–$34,999 | 11.2 |
| – $35,000–$49,999 | 13.1 |
| – $50,000–$74,999 | 16.8 |
| – $75,000–$99,999 | 10.3 |
| – $100,000–$149,999 | 16.8 |
| – $150,000 or more | 15.9 |
| Marital status, % | |
| – Single | 20.9 |
| – Married | 69.6 |
| – Domestic partnership | 2.6 |
| – Divorced | 6.1 |
| – Widowed | 0.9 |
| Clinical variables, mean (SD) | |
| – Height, cm | 161.2 (8.0) |
| – Weight, kg | 87.2 (20.4) |
| – BMI, kg/m2 | 33.8 (9.6) |
| – HbA1c, % | 5.3 (0.6) |
GED: General Educational Development Test; HbA1c: Hemoglobin A1c; SD: Standard deviation.
Discussion
The researchers engaged women with a history of GDM in an informed decision-making process to discuss T2D risk and prevention efficacy, and to offer participation in a variety of lifestyle change programs. This study will evaluate engagement in a tailored approach to lifestyle change programs in the GDM population. The authors hypothesize that the informed decision-making process and increased choice will support greater utilization of lifestyle change programs, thus reducing T2D risk.
The opportunity to delay or prevent T2D in women with previous GDM is significant. Women with a history of GDM are at high risk for developing T2D within 5 to 10 years after delivery [33], which has implications for subsequent pregnancies [34] and long-term health [35]. For instance, T2D during pregnancy increases risk for pre-eclampsia, preterm birth, caesarean delivery, infant congenital anomalies, stillbirth and macrosomia [34,36]. Furthermore, earlier development of T2D in women with previous GDM adversely affects quality of life [3] and increases the risk of comorbidities [35] and early death [5].
This underlines the importance of lifestyle change programs to decrease T2D risk in women with previous GDM. However, program enrollment and participation in real-world settings is challenging, and it is especially difficult for women of childbearing age. In a cohort study of the NDPP, women ages 18–39 were about half as likely to enroll in the program compared with women ages 40 and over [11]. Additionally, younger women had lower session attendance and program completion than older women [11].
A qualitative study of women who declined NDPP participation or did not complete the program revealed that program cost, time commitment and inconvenient locations were barriers to enrollment and participation [37]. Interestingly, some women also felt that the NDPP did not align with their expectations for a lifestyle change program [37]. This is consistent with findings by Palmer and colleagues, who reported that women with previous GDM want lifestyle change programs with more flexible attendance, time of day and location options [16]. Women also expressed a need for childcare, individualized programs and online options [16].
Therefore, this study aimed to maximize programs that offer flexibility, one-on-one counseling and web-based formats. The NDPP is offered at 12 different locations on various days of the week and at different times of day. Encourage meets in the evening and includes childcare. The remaining programs (WW, health coaching, dietitian consult, HabitNu and Healthy Me) offer online and phone availability at flexible times of the day.
The researchers also responded to the desire for programs with a variety of time commitments. The NDPP, Encourage and HabitNu are 12 months in length, while women can select either 3 or 6 months of WW. Coaching programs range in length from 12 to 16 weeks. Women who want less of a time commitment can select one or two dietitian visits. This study recognizes barriers to participation and aims to offer women a variety of modes of lifestyle change programs to promote increased engagement.
Low perceived T2D risk is another barrier to engagement in lifestyle change programs [13]. Therefore, the researchers engaged women in an informed decision-making process to increase education regarding T2D risk and prevention efficacy while facilitating decision making based on each participant's priorities.
Moin and colleagues used shared decision making, similar to informed decision making, to help patients with prediabetes better understand prevention options and select from among the DPP only, metformin only, the DPP and metformin or no intervention [18]. They found that shared decision making increased patient knowledge of T2D prevention options and increased patient engagement in prevention efforts [18].
Both shared decision making and informed decision making involve collaborative information sharing designed to help individuals make decisions that fit their values and preferences, but shared decision making includes more input and guidance from the clinician [17]. Given the nature of the decision making, the informed decision-making model is more appropriate for this intervention. It is reasonable to surmise that informed decision making will lead to outcomes similar to those of shared decision making.
Lifestyle change programs significantly lower the risk of T2D [6], yet the engagement of women with previous GDM in these programs is low [11]. Previous research highlighted a variety of barriers to participation [12,16,37]. This study aims to address these barriers by engaging women in an informed decision-making process and offering lifestyle change programs tailored to meet the needs and priorities of women with previous GDM.
Limitations
This study has limitations. First, the COVID-19 pandemic occurred while the study was enrolling participants and completing follow-up visits. Therefore, the entire study was halted, which prevented the enrollment of the initially targeted number of participants. Additionally, the pandemic postponed baseline and follow-up appointments by a short period of time. Second, the study focused on one geographic area that covered a major metropolitan area and immediate surrounding counties. Therefore, the findings may not be generalizable to the general public. Third, the study did not offer women the option of non-participation in a program, so the study may have attracted participants that were more activated to make lifestyle changes. Fourth, the study was not powered to compare differences in health outcomes between lifestyle change programs. Last, this is a prepost cohort study design, so the findings cannot be compared with a control group.
Conclusion
Women with previous GDM are at high risk for T2D. Lifestyle modification significantly reduces T2D risk, but engagement in lifestyle change programs is low in the GDM population. This study engaged women with a history of GDM in an informed-decision making process and offered a variety of program options. This study will determine if a tailored approach to diabetes prevention improves engagement in lifestyle change programs. The findings of this study may support more flexible prevention programs for high-risk populations.
•
Women with a history of gestational diabetes mellitus (GDM) are at high risk for developing Type 2 diabetes (T2D).
•
Lifestyle change programs decrease the risk for T2D, yet engagement in these programs is low in the GDM population.
•
The researchers engaged women with previous GDM in an informed decision-making process to discuss T2D risk and prevention efficacy, and to offer participation in a variety of lifestyle change programs.
•
Women selected a lifestyle change program based on their needs and preferences.
•
Lifestyle change programs were evidence-based diabetes prevention interventions that varied in regard to the delivery formats (in-person, web-based, phone-based), program duration, time of day, group versus individual format and childcare.
•
Informed decision making is an approach for tailoring diabetes prevention interventions for women with previous GDM.
•
The findings of this study will evaluate the impact of this strategy for lifestyle change program engagement for diabetes prevention in a high-risk population.
Financial & competing interests disclosure
Funding was provided by the Indiana University Grand Challenge Precision Health Initiative grant. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
1.
Metzger BE, Coustan DR. Summary and recommendations of the Fourth International Workshop-Conference on Gestational Diabetes Mellitus. The organizing committee. Diabetes Care 21, B161–B167 (1998).
2.
Li Z, Cheng Y, Wang D et al. Incidence rate of Type 2 diabetes mellitus after gestational diabetes mellitus: a systematic review and meta-analysis of 170,139 women. J. Diabetes Res. 2020, 3076463 (2020).
3.
Glasgow RE, Ruggiero L, Eakin EG, Dryfoos J, Chobanian L. Quality of life and associated characteristics in a large national sample of adults with diabetes. Diabetes Care 20(4), 562–567 (1997).
4.
Alva ML, Hoerger TJ, Zhang P, Cheng YJ. State-level diabetes-attributable mortality and years of life lost in the United States. Ann. Epidemiol. 28(11), 790–795 (2018).
5.
Ang GY. Age of onset of diabetes and all-cause mortality. World J. Diabetes 11(4), 95–99 (2020).
6.
Ratner RE, Christophi CA, Metzger BE et al. Prevention of diabetes in women with a history of gestational diabetes: effects of metformin and lifestyle interventions. J. Clin. Endocrinol. Metab. 93(12), 4774–4779 (2008).
7.
Marrero DG, Palmer KN, Phillips EO, Miller-Kovach K, Foster GD, Saha CK. Comparison of commercial and self-initiated weight loss programs in people with prediabetes: a randomized control trial. Am. J. Public Health 106(5), 949–956 (2016).
8.
Cranney L, O'Hara B, Gale J, Rissel C, Bauman A, Phongsavan P. Telephone based coaching for adults at risk of diabetes: impact of Australia's Get Healthy service. Transl. Behav. Med. 9(6), 1178–1185 (2019).
9.
Joiner KL, Nam S, Whittemore R. Lifestyle interventions based on the diabetes prevention program delivered via eHealth: a systematic review and meta-analysis. Prev. Med. 100, 194–207 (2017).
10.
Hannon TS, Saha CK, Carroll AE, Palmer KN, O'Kelly Phillips E, Marrero DG. The ENCOURAGE healthy families study: a comparative effectiveness trial to reduce risk for type 2 diabetes in mothers and children. Pediatr. Diabetes (2018).
11.
Ritchie ND, Sauder KA, Fabbri S. Reach and effectiveness of the National Diabetes Prevention Program for young women. Am. J. Prev. Med. 53(5), 714–718 (2017).
12.
Dennison RA, Ward RJ, Griffin SJ, Usher-Smith JA. Women's views on lifestyle changes to reduce the risk of developing Type 2 diabetes after gestational diabetes: a systematic review, qualitative synthesis and recommendations for practice. Diabet. Med. 36(6), 702–717 (2019).
13.
Kim C, McEwen LN, Piette JD, Goewey J, Ferrara A, Walker EA. Risk perception for diabetes among women with histories of gestational diabetes mellitus. Diabetes Care 30(9), 2281 (2007).
14.
Jones EJ, Roche CC, Appel SJ. A review of the health beliefs and lifestyle behaviors of women with previous gestational diabetes. J. Obstet. Gynecol. Neonatal Nurs. 38(5), 516–526 (2009).
15.
Parsons J, Ismail K, Amiel S, Forbes A. Perceptions among women with gestational diabetes. Qual. Health Res. 24(4), 575–585 (2014).
16.
Palmer KNB, Garr Barry VE, Marrero DG et al. Intervention delivery matters: what mothers at high risk for Type 2 diabetes want in a diabetes prevention program – results from a comparative effectiveness trial. Diabetes Ther. 11(10), 2411–2418 (2020).
17.
Charles C, Whelan T, Gafni A. What do we mean by partnership in making decisions about treatment? BMJ 319(7212), 780–782 (1999).
18.
Moin T, Duru OK, Turk N et al. Effectiveness of shared decision-making for diabetes prevention: 12-month results from the Prediabetes Informed Decision and Education (PRIDE) trial. J. Gen. Intern. Med. 34(11), 2652–2659 (2019).
19.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 42(2), 377–381 (2009).
20.
Breslin M, Mullan RJ, Montori VM. The design of a decision aid about diabetes medications for use during the consultation with patients with Type 2 diabetes. Patient Educ. Couns. 73(3), 465–472 (2008).
21.
Mullan RJ, Montori VM, Shah ND et al. The diabetes mellitus medication choice decision aid: a randomized trial. Arch. Intern. Med. 169(17), 1560–1568 (2009).
22.
Hibbard JH, Mahoney ER, Stockard J, Tusler M. Development and testing of a short form of the Patient Activation Measure. Health Serv. Res. 40(6p1), 1918–1930 (2005).
23.
Felitti VJ, Anda RF, Nordenberg D et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) study. Am. J. Prev. Med. 14(4), 245–258 (1998).
24.
Wallston KA, Strudler Wallston B, Devellis R. Development of the Multidimensional Health Locus of Control (MHLC) scales. Health Educ. Monogr. 6(1), 160–170 (1978).
25.
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J. Health Soc. Behav. 24(4), 385–396 (1983).
26.
Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 32(6), 705–714 (1991).
27.
Craig CL, Marshall AL, Sjöström M et al. International Physical Activity Questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 35(8), 1381–1395 (2003).
28.
Jenkinson C, Layte R, Jenkinson D et al. A shorter form health survey: can the SF-12 replicate results from the SF-36 in longitudinal studies? J. Public Health 19(2), 179–186 (1997).
29.
Connor U, Kessler L, De Groot M, Mac Neill R, Sandy R. Implementing person-centered communication in diabetes care: a new tool for diabetes care professionals. Patient Prefer. Adherence 13, 1443–1450 (2019).
30.
Committee ADaPP. 3. Prevention or delay of Type 2 diabetes and associated comorbidities: standards of medical care in diabetes – 2022. Diabetes Care 45(Suppl. 1), S39–S45 (2021).
31.
Raynor HA, Davidson PG, Burns H et al. Medical nutrition therapy and weight loss questions for the evidence analysis library prevention of Type 2 diabetes project: systematic reviews. J. Acad. Nutr. Diet 117(10), 1578–1611 (2017).
32.
Knowler WC, Barrett-Connor E, Fowler SE et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. Description of lifestyle intervention 346(6), 393–403 (2002).
33.
Bellamy L, Casas JP, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet 373(9677), 1773–1779 (2009).
34.
Yang J, Cummings EA, O'Connell C, Jangaard K. Fetal and neonatal outcomes of diabetic pregnancies. Obstet. Gynecol. 108(3 Pt 1), 644–650 (2006).
35.
Zoungas S, Woodward M, Li Q et al. Impact of age, age at diagnosis and duration of diabetes on the risk of macrovascular and microvascular complications and death in Type 2 diabetes. Diabetologia 57(12), 2465–2474 (2014).
36.
Temple R, Murphy H. Type 2 diabetes in pregnancy – an increasing problem. Best Pract. Res. Clin. Endocrinol. Metab. 24(4), 591–603 (2010).
37.
Baucom KJW, Pershing ML, Dwenger KM, Karasawa M, Cohan JN, Ozanne EM. Barriers and facilitators to enrollment and retention in the National Diabetes Prevention Program: perspectives of women and clinicians within a health system. Womens Health Rep. (New Rochelle) 2(1), 133–141 (2021).
Information & Authors
Information
Published In
Pages: 477 - 487
PubMed: 35416051
Copyright
© 2022 Future Medicine Ltd.
History
Received: 18 November 2021
Accepted: 25 March 2022
Published online: 13 April 2022
Keywords:
Topics
Authors
Funding Information
Indiana University Bloomington: Indiana University Grand Challenge Precision Health
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Design and methods of a tailored approach for diabetes prevention in women with previous gestational diabetes. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0288
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Julie M. Pike, Noha El Yaman, Kathryn M. Haberlin-Pittz, Luz A. Machuca, Brett M. McKinney, Aric Kotarski, David M. Guise, Tamara S. Hannon, A Tailored Approach to Increase Engagement in Lifestyle Change Programs in Women With Previous Gestational Diabetes Mellitus, Diabetes Obesity and Cardiometabolic CARE, 10.2337/doc25-0019, 1, 1, (87-95), (2026).