Channeling effects in the prescription of new therapies: the case of emicizumab for hemophilia A
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To determine if emicizumab was channeled to clinically complex people with hemophilia A upon approval. Methods: Claims data (16 November 2017, through 31 December 2019) from US-based insurance databases were analyzed to compare the clinical complexity of people with hemophilia A initiating emicizumab with matched individuals receiving factor VIII (FVIII) episodically or prophylactically. People with hemophilia A with evidence of previous bypassing agent use (indicating FVIII inhibitors) were excluded. Outcomes included bleeding events, arthropathy, pain, comorbidities and healthcare costs. Results: A larger proportion of emicizumab users had bleeding events, comorbidities and arthropathy and greater healthcare costs in the year prior to starting emicizumab compared with FVIII users. Conclusion: Claims-based data limitations prevent an absolute conclusion. Nevertheless, emicizumab users appear more clinically complex than FVIII users, suggesting post-approval channeling.
Channeling is an effect seen in the drug market, whereby newly prescribed drugs are channeled to patients who would gain the most [1]. Advantages offered by a new treatment may lead physicians to channel it to patients who could experience additional patient-specific benefits, according to their individual clinical characteristics, compared with the broader population in that therapeutic area [1,2]. In the field of hemophilia A (HA), a bleeding disorder characterized by deficiency of coagulation factor VIII (FVIII) [3], treatments over the last 50 years have mostly been iterative improvements on FVIII replacement therapy [4] or bypassing agents (BPAs) for those with FVIII inhibitors [5]. These well-established, traditional treatments are associated with various limitations and burdens, such as frequent intravenous administration and risk of developing FVIII inhibitors [5].
More recently, a therapy with a novel mechanism of action has been approved for people with HA (PwHA). Emicizumab is a bispecific humanized monoclonal antibody that bridges activated factor IX and factor X to restore the function of deficient activated FVIII [6]. To date, emicizumab is the only non-factor prophylactic treatment in HA. Emicizumab was approved in the USA for PwHA with FVIII inhibitors on 16 November 2017 [7], and for those without FVIII inhibitors on 4 October 2018 [8]. It is subcutaneously administered weekly, every 2 weeks or every 4 weeks [9–12]. During the HAVEN clinical trial program, prophylactic emicizumab demonstrated efficacy and safety in preventing bleeds, which is further supported by real-world evidence [13–15]. Furthermore, when compared with previous FVIII prophylaxis, emicizumab has reduced annualized bleed rates [16]. Therefore, it may be expected that clinically complex PwHA will have been preferentially prescribed emicizumab in the post-approval period.
In this article, channeling effects in the field of novel transformative therapies are explored using emicizumab as a case study. US-based claims data are examined, comparing clinical complexity in PwHA prescribed emicizumab versus PwHA prescribed FVIII in the same time period and PwHA prescribed emicizumab in the post-approval period versus those prescribed emicizumab later. As the population of PwHA with FVIII inhibitors is known to be a distinct and more challenging population than those without FVIII inhibitors, with increased risk of morbidity and mortality [17], they are omitted from this analysis by excluding individuals with evidence of previous BPA use – a proxy measure in claims data for the presence of FVIII inhibitors.
Methods
Data source
Claims data (16 November 2017, through 31 December 2019) were obtained from the US-based IBM MarketScan Commercial Claims and Encounters and PharMetrics Plus databases, which comprise commercial insurance records capturing medical claims and costs related to hospital stays, emergency room visits and prescription treatment usage. National Drug Codes; Healthcare Common Procedure Coding System; International Classification of Diseases, Clinical Modification; Current Procedural Terminology; place of service; provider type and revenue codes were used to identify treatments, comorbidities and healthcare resource utilization (HCRU) (Supplementary Material).
Patient selection
A cohort of PwHA receiving emicizumab or FVIII were identified with ≥1 year of continuous medical and pharmaceutical coverage on or prior to the index date, defined as the date of the first claim for emicizumab or FVIII treatment. When comparing emicizumab use with FVIII treatment, individuals were also required to have ≥2 diagnostic codes for HA during baseline enrollment to ensure a true population, as the first diagnostic code may refer to a suspicion of diagnosis and testing, whereas the second would confirm the diagnosis. The exclusion criteria included individuals receiving BPAs (an imperfect proxy measure for the presence of FVIII inhibitors) and females, as FVIII prophylaxis and emicizumab are typically reserved for males with HA. Because of the nature of this study, ethical approval and informed consent were not required.
Identifying FVIII prophylaxis versus non-prophylactic (on-demand) FVIII treatment
Treatment types were classified using the Shrestha et al. algorithm [18], as claims data do not distinguish between prophylactic and non-prophylactic treatment.
Identifying recorded bleeding events
Here recorded bleeding events refer to bleeding events requiring additional healthcare services outside the individual's home, which would be captured by claims data. Codes relating to hemarthrosis; hematoma; effusions; contusions; and intracranial, neck/throat and gastrointestinal hemorrhages were used to discern typical hemophilia-related bleeds, and the date of treatment and body part affected determined a single bleeding event – a method developed by Shrestha et al. [18].
Outcomes
The primary outcome was the clinical complexity of PwHA during a baseline year prior to starting current treatment. This included recorded bleeding events, comorbidities, central venous access device removal, arthropathy, durable medical equipment use and orthopedic procedures as well as HCRU, including emergency room visits and hospital stays. FVIII treatment costs were excluded. These outcomes were compared between PwHA receiving emicizumab, FVIII prophylaxis and FVIII on demand and PwHA initiating treatment with emicizumab across time, quantified in quarters (Q's) of the year after approval of emicizumab in the USA.
Statistical methods
As the numbers of PwHA for each cohort were too small to allow for inferential analyses, outcomes were assessed by descriptive analysis.
Results
Emicizumab population compared with FVIII prophylaxis & on-demand FVIII populations
In total, 542, 810 and 2517 PwHA receiving emicizumab prophylaxis, FVIII prophylaxis and FVIII on demand, respectively, were identified between 16 November 2017 and 31 December 2019, in the MarketScan and PharMetrics databases. Of these, 172, 79 and 897 met the eligibility criteria, and 144, 79 and 776 PwHA without FVIII inhibitors remained after duplicate removal (n = 10, 0 and 108, respectively) and exclusion of those with evidence of previous BPA use (n = 18, 0 and 13, respectively) (Figure 1A).

Figure 1. Identification of records of PwHA.
(A) Emicizumab prophylaxis, FVIII prophylaxis or on-demand FVIII. (B) Emicizumab prophylaxis across different quarters in MarketScan and PharMetrics databases.
FVIII: Factor VIII; PwHA: People with hemophilia A.
PwHA receiving emicizumab were slightly younger than those receiving FVIII prophylaxis or on-demand FVIII, with a higher proportion (emicizumab: 14.6%; FVIII prophylaxis: 8.9%; on-demand FVIII: 8.6%) being ≤5 years of age (Table 1A). When investigating clinical complexity during the year before starting emicizumab prophylaxis, a greater proportion of PwHA starting emicizumab had recorded bleeding events (27.8%) and arthropathy or a related disorder (22.9%) compared with PwHA receiving FVIII prophylaxis (13.9 and 10.1%, respectively) or on-demand FVIII (21.5 and 13.0%, respectively) (Table 2A). Several relevant comorbidities recorded in the year before emicizumab initiation were investigated, as these are known to affect a significant subset of PwHA. PwHA receiving emicizumab prophylaxis were more likely to have HIV/AIDS (12.5%) compared with PwHA receiving FVIII prophylaxis (3.8%) or on-demand FVIII (7.6%). They were also more likely to have hepatitis C virus (HCV) infection (14.6%) compared with PwHA receiving FVIII prophylaxis (6.3%), although the proportion of those receiving on-demand FVIII with HCV infection was similar (15.2%). PwHA receiving emicizumab were also more likely to have had a central venous access device removed in the year prior compared with those receiving FVIII therapies (Table 2A). Other comorbidities, such as myocardial infarction and cerebrovascular disease, were also analyzed (Table 2A), but events were very few.
| A | ||||||
|---|---|---|---|---|---|---|
| Baseline demographics | Emicizumab prophylaxis‡ | FVIII prophylaxis‡ | FVIII on demand‡ | |||
| Total, n (%) | 144 (100) | 79 (100) | 776 (100) | |||
| Male, n (%) | 144 (100) | 79 (100) | 776 (100) | |||
| Age Mean (SD) Median (IQR) ≤5 years, n (%) | 22.6 (16.2) 18 (9–37) 21 (14.6) | 25.1 (15.1) 25 (15–33) 7 (8.9) | 26.6 (17.4) 23 (13–38) 67 (8.6) | |||
| PPO†, n (%) | 87 (60.4) | 59 (74.7) | 495 (63.8) | |||
| B | ||||||
|---|---|---|---|---|---|---|
| Baseline demographics | Q2/Q3 2018 | Q4 2018 | Q1 2019 | Q2 2019 | Q3 2019 | Q4 2019 |
| Total, n (%) | 6 (100) | 31 (100) | 68 (100) | 30 (100) | 27 (100) | 19 (100) |
| Male, n (%) | 6 (100) | 31 (100) | 68 (100) | 30 (100) | 27 (100) | 19 (100) |
| Age Mean (SD) Median (IQR) ≤5 years, n (%) | 26.3 (21.2) 17.5 (10.5–41) 0 (0) | 21.6 (17.1) 20 (7–32) 7 (22.6) | 22.5 (16.0) 18 (9–37) 9 (13.2) | 25.3 (14.4) 26 (12.8–33.5) 2 (6.7) | 25.6 (14.7) 25 (15–34) 3 (11.1) | 26.1 (15.3) 25 (14.5–39) 1 (5.3) |
| PPO†, n (%) | 5 (83.3) | 22 (71.0) | 41 (60.3) | 15 (50.0) | 17 (63.0) | 12 (63.2) |
†
PPOs are a proxy measure indicating the possession of commercial insurance in the USA.
‡
Data include PwHA identified in Q4 2019 or prior.
FVIII: Factor VIII; IQR: Interquartile range; PPO: Preferred provider organization; PwHA: People with hemophilia A; Q: Quarter; SD: Standard deviation.
| A | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Emicizumab prophylaxis (n = 144)# | FVIII prophylaxis (n = 79)# | FVIII on demand (n = 776)# | |||
| PwHA with recorded bleeding events at baseline, n (%) | 40 (27.8) | 11 (13.9) | 167 (21.5) | |||
| Number of bleeds during baseline period Mean (SD) Median (IQR) | 4.5 (7.5) 2 (1–3.3) | 3.8 (5.0) 2 (1–3.5) | 2.8 (5.8) 1 (1–2) | |||
| CVAD removal, n (%) | 5 (3.5) | 2 (2.5) | 18 (2.3) | |||
| Infusion procedures†, n (%) | 99 (68.8) | 18 (22.8) | 644 (83.0) | |||
| Arthropathy or related disorder, n (%) | 33 (22.9) | 8 (10.1) | 101 (13.0) | |||
| Durable medical equipment use‡, n (%) | 7 (4.9) | 3 (3.8) | 46 (5.9) | |||
| Orthopedic procedures§, n (%) | 1 (0.7) | 0 (0) | 35 (4.5) | |||
| Patient visit procedures¶, n (%) | 1 (0.7) | 0 (0) | 14 (1.8) | |||
| Comorbidities, n (%) HIV/AIDS HCV Myocardial infarction Congestive heart failure Cerebrovascular disease | 18 (12.5) 21 (14.6) 0 (0) 1 (0.7) 2 (1.4) | 3 (3.8) 5 (6.3) 1 (1.3) 0 (0) 0 (0) | 59 (7.6) 118 (15.2) 6 (0.8) 4 (0.5) 12 (1.6) | |||
| Cardiologist visit, n (%) | 6 (4.2) | 7 (8.9) | 50 (6.4) | |||
| Pain diagnosis, n (%) | 46 (31.9) | 23 (29.1) | 276 (35.6) | |||
| Opioid use, n (%) | 32 (22.2) | 17 (21.5) | 210 (27.1) | |||
| B | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Q2/Q3 2018 (n = 6) | Q4 2018 (n = 31) | Q1 2019 (n = 68) | Q2 2019 (n = 30) | Q3 2019 (n = 27) | Q4 2019 (n = 19) |
| PwHA with recorded bleeding events at baseline, n (%) | 2 (33.3) | 8 (25.8) | 17 (25.0) | 7 (23.3) | 5 (18.5) | 3 (15.8) |
| Number of bleeds during baseline period Mean (SD) Median (IQR) | 5 (4.2) 5 (3.5–6.5) | 8 (15.1) 2 (1–5.5) | 3.5 (3.8) 2 (1–3) | 4.0 (5.8) 2 (1.5–2.5) | 3.2 (1.9) 3 (2–4) | 2 (1) 2 (1.5–2.5) |
| CVAD removal, n (%) | 0 (0) | 3 (9.7) | 2 (2.9) | 0 (0) | 1 (3.7) | 0 (0) |
| Infusion procedures†, n (%) | 1 (16.7) | 18 (58.1) | 42 (61.8) | 18 (60.0) | 15 (55.6) | 10 (52.6) |
| Arthropathy or related disorder, n (%) | 0 (0) | 5 (16.1) | 18 (26.5) | 5 (16.7) | 5 (18.5) | 5 (26.3) |
| Durable medical equipment use‡, n (%) | 1 (16.7) | 2 (6.5) | 3 (4.4) | 0 (0) | 1 (3.7) | 2 (10.5) |
| Orthopedic procedures§, n (%) | 0 (0) | 1 (3.2) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Patient visit procedures¶, n (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (3.7) | 0 (0) |
| Comorbidities, n (%) HIV/AIDS HCV Myocardial infarction Congestive heart failure Cerebrovascular disease | 1 (16.7) 0 (0) 0 (0) 0 (0) 1 (16.7) | 5 (16.1) 3 (9.7) 0 (0) 0 (0) 0 (0) | 8 (11.8) 7 (10.3) 0 (0) 1 (1.5) 1 (1.5) | 3 (10.0) 5 (16.7) 0 (0) 0 (0) 0 (0) | 3 (11.1) 4 (14.8) 0 (0) 0 (0) 0 (0) | 2 (10.5) 3 (15.8) 0 (0) 0 (0) 0 (0) |
| Cardiologist visit, n (%) | 2 (33.3) | 3 (9.7) | 2 (2.9) | 0 (0) | 0 (0) | 1 (5.3) |
| Pain diagnosis, n (%) | 3 (50.0) | 10 (32.3) | 21 (30.9) | 8 (26.7) | 6 (22.2) | 5 (26.3) |
| Opioid use, n (%) | 1 (16.7) | 6 (19.4) | 17 (25.0) | 8 (26.7) | 8 (29.6) | 2 (10.5) |
†
Includes injections and other procedures that cannot be self-administered or taken orally.
‡
Includes walking aids and attachments.
§
Includes knee or hip replacements and synovectomies.
¶
Includes office visits and inpatient and outpatient visits.
#
Data include PwHA identified in Q4 2019 or prior.
CVAD: Central venous access device; FVIII: Factor VIII; HCV: Hepatitis C virus; IQR: Interquartile range; PwHA: People with hemophilia A; Q: Quarter; SD: Standard deviation.
HCRU (Table 3A) and average healthcare costs were derived from the year before receiving current treatment. A greater proportion of PwHA receiving emicizumab had visited the emergency room and outpatient hospital (37.5 and 71.5%, respectively) compared with PwHA receiving FVIII prophylaxis (20.3 and 26.6%, respectively) or on-demand FVIII (27.6 and 23.1%, respectively). By contrast, a higher proportion of PwHA receiving FVIII prophylaxis had had an inpatient hospital stay compared with PwHA who went on to receive emicizumab prophylaxis, which is mirrored by higher inpatient costs in this population. Nevertheless, overall reported healthcare costs were highest in PwHA who went on to receive emicizumab prophylaxis, mostly due to much greater outpatient hospital costs (Figure 2A).
| A | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Emicizumab prophylaxis (n = 144)† | FVIII prophylaxis (n = 79)† | FVIII on demand (n = 776)† | |||
| Emergency room visit, n (%) | 54 (37.5) | 16 (20.3) | 214 (27.6) | |||
| ≥1 inpatient hospital stay, n (%) Mean length of stay, days (SD) | 15 (10.4) 4.2 (3.0) | 15 (19.0) 5.3 (5.1) | 75 (9.7) 5.2 (5.4) | |||
| ≥1 outpatient hospital visit, n (%) | 103 (71.5) | 21 (26.6) | 179 (23.1) | |||
| ≥1 office visit, n (%) | 139 (96.5) | 65 (82.3) | 578 (74.5) | |||
| B | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Q2/Q3 2018 (n = 6) | Q4 2018 (n = 31) | Q1 2019 (n = 68) | Q2 2019 (n = 30) | Q3 2019 (n = 27) | Q4 2019 (n = 19) |
| Emergency room visit, n (%) | 2 (33.3) | 10 (32.3) | 20 (29.4) | 9 (30.0) | 9 (33.3) | 10 (52.6) |
| ≥1 inpatient hospital stay, n (%) Mean length of stay, days (SD) | 0 (0) N/A | 6 (19.4) 3.2 (2.6) | 6 (8.8) 6.3 (2.7) | 0 (0) N/A | 3 (11.1) 2 (1) | 0 (0) N/A |
| ≥1 outpatient hospital visit, n (%) | 3 (50.0) | 16 (51.6) | 39 (57.4) | 27 (90.0) | 23 (85.2) | 18 (94.7) |
| ≥1 office visit, n (%) | 5 (83.3) | 27 (87.1) | 66 (97.1) | 29 (96.7) | 25 (92.6) | 17 (89.5) |
†
Data include PwHA identified in Q4 2019 or prior.
FVIII: Factor VIII; N/A: Not applicable; PwHA: People with hemophilia A; Q: Quarter; SD: Standard deviation.
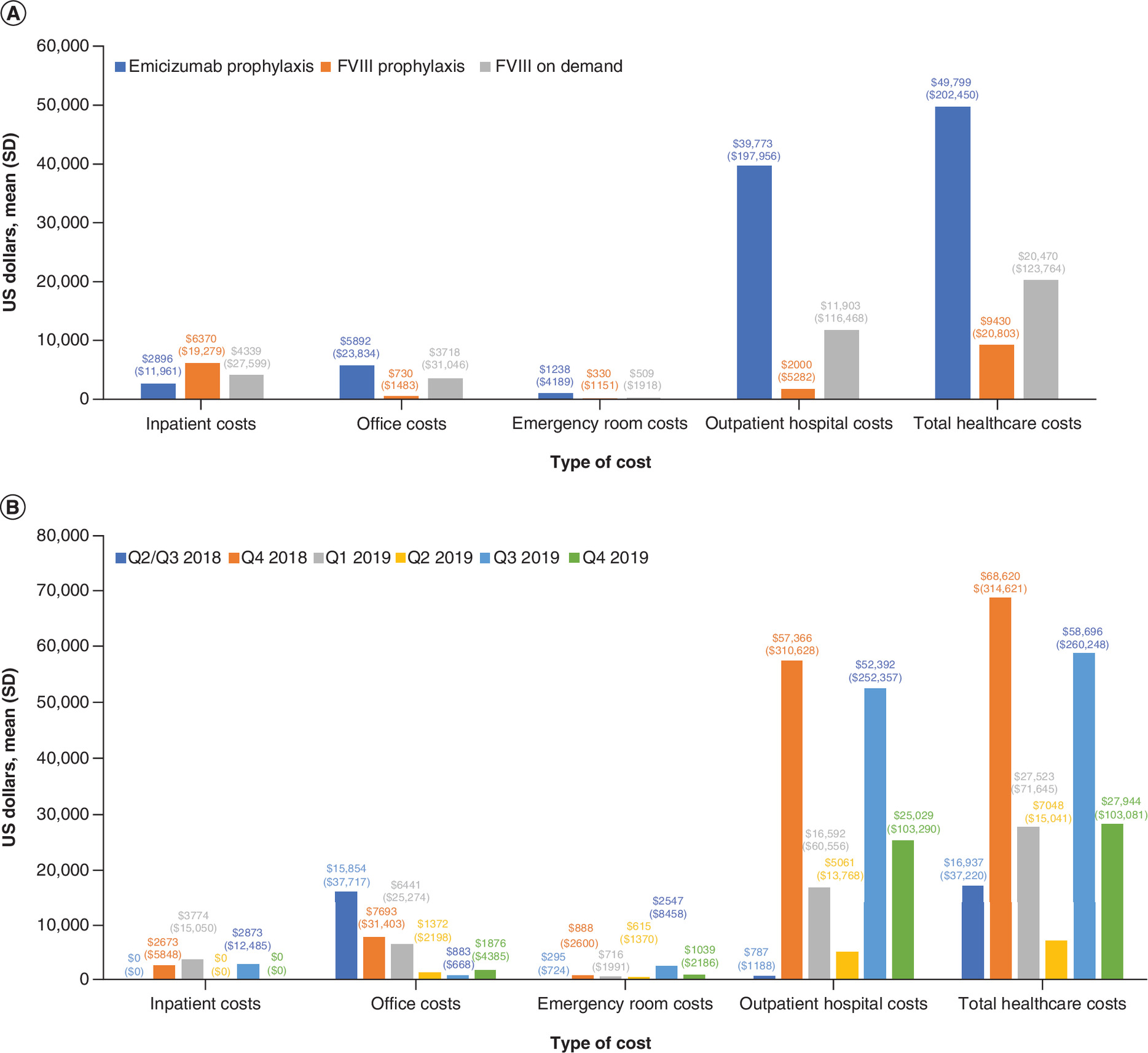
Figure 2. Healthcare costs for the year prior to initiating treatment per individual.
(A) Emicizumab prophylaxis, FVIII prophylaxis or on-demand FVIII. (B) Emicizumab prophylaxis across different quarters, excluding individuals with evidence of previous BPA use.
BPA: Bypassing agent; FVIII: Factor VIII.
Emicizumab across time
A total of 233 and 309 PwHA receiving emicizumab were identified between 16 November 2017 and 31 December 2019, in the MarketScan and PharMetrics databases, respectively. Of these, 212 PwHA met the eligibility criteria. After removal of duplicates (n = 11) and those with evidence of previous BPA use (n = 20), the records of 181 PwHA without FVIII inhibitors were analyzed (Figure 1B). The highest proportion of PwHA excluded because of previous BPA use was from those initiating emicizumab in Q2/Q3 2018, with 11 of 17 individuals excluded compared with none in Q4 2019.
Demographics (Table 1B) and clinical characteristics (Table 2B) were quantified across time after approval of emicizumab in the USA, beginning in Q2/Q3 2018 or before and ending in Q4 2019. The median (interquartile range [IQR]) ages of PwHA initiating emicizumab from Q2/Q3 2018 (median: 17.5; IQR: 10.5–41) to Q1 2019 (median: 18; IQR: 9–37) were generally lower than the ages of PwHA initiating emicizumab from Q2 2019 (median: 26; IQR: 12.8–33.5) to Q4 2019 (median: 25; IQR: 14.5–39). With the exception of the small Q2/Q3 2018 cohort (n = 6), this is aligned with a diminishing proportion of individuals under 5 years of age, from 22.6% in Q4 2018 to 5.3% in Q4 2019. A total of 33.3% of PwHA starting emicizumab in or prior to Q2/Q3 2018 and 25.8% of PwHA starting emicizumab in Q4 2018 had recorded bleeding events during the year prior compared with 15.8% in Q4 2019. PwHA prescribed emicizumab early were more likely to be diagnosed with pain (Q2/Q3 2018 or before: 50.0%; Q4 2018: 32.3%), and this decreased to 26.3% in Q4 2019 (Table 2B). No one who initiated emicizumab in Q2/Q3 2018 had arthropathy or a related disorder. From Q4 2018 to Q4 2019, the proportion of PwHA initiating emicizumab who had arthropathy or a related disorder fluctuated between 16.1 and 26.5%.
Finally, HCRU (Table 3B) and costs (Figure 2B) were extremely variable. The proportion of PwHA with an outpatient hospital visit in the previous year was higher in Q2–Q4 2019 compared with Q2/Q3 2018 to Q1 2019, but this was not reflected by outpatient costs. The highest total healthcare costs were recorded for PwHA who started emicizumab in Q4 2018, the overwhelming majority of which was due to outpatient costs. A similar pattern of high total costs due to high outpatient costs was seen for Q3 2019. Office costs showed a downward trend over time, from a mean (standard deviation) of US$15,854 ($37,717) in Q2/Q3 2018 to US$1876 ($4385) in Q4 2019, despite the mean proportion of PwHA with at least one office visit in the previous year remaining relatively consistent.
Discussion
Channeling may occur when newly approved treatments become available in an existing therapy area [2]. New treatments may be selectively prescribed in accordance with the approved indication but favoring patients who would gain the most – for example, because of poorer prognosis, inadequate control on prior therapy, comorbidities, more severe disease or need for more straightforward administration [1,2]. PwHA with poor health, uncontrolled bleeds, progressive joint damage, comorbidities and/or venous scarring from frequent intravenous FVIII infusions may be more willing to try a new therapy, and physicians treating these PwHA may have prescribed emicizumab anticipating greater clinical improvement relative to existing therapies and a lower treatment burden with subcutaneous administration weekly, every 2 weeks or every 4 weeks [19]. As innovations in HA treatment were gradual for many years [4], this may have created a bottleneck of clinically complex PwHA with progressive concurrent conditions. Hence, a similar channeling effect may occur when other late entry, novel treatments become available. The most advanced of these are concizumab, a monoclonal antibody targeting tissue factor pathway inhibitor [20], and fitusiran, an RNA interference therapeutic targeting antithrombin [21]. The advent of gene therapy for HA is also anticipated in the near future [22]. These treatment options will also be available for hemophilia B, where there may still be a bottleneck of clinically complex patients.
Emicizumab population compared with FVIII prophylaxis & on-demand FVIII populations
As expected, because of the inefficacy of FVIII treatment in PwHA with current FVIII inhibitors, a greater proportion of PwHA starting emicizumab had prior BPA claims compared with PwHA receiving FVIII treatments. Analysis of the US claims-based data suggests that PwHA without FVIII inhibitors receiving emicizumab are a fundamentally different population than those receiving FVIII treatment. In the year prior to receiving their current treatment, PwHA on emicizumab prophylaxis had a higher rate of HIV/AIDS and recorded bleeding events compared with those receiving FVIII treatment. They were also more likely to have arthropathy despite being younger on average and youth generally being associated with less complex disease [23,24]. These factors suggest that physicians may be preferentially prescribing emicizumab to more clinically complex PwHA.
It is worth noting that physician decision may not be the only factor governing the channeling of emicizumab. The effect suggested by these data may also have been biased by insurance company policies, patient or caregiver choice or other causes. It is possible that insurance companies may have reinforced the channeling effect by restricting access to emicizumab to those with more severe disease or confounded it by influencing prescription in another way. PwHA receiving emicizumab were more likely to have had their central venous access device removed in the previous year compared with those on FVIII treatment, which could motivate a switch to subcutaneous emicizumab. Subcutaneous delivery may be a significant factor in the channeling of emicizumab to certain individuals who require more straightforward administration due to difficulties with venous access. Subcutaneous delivery may be suggested through physician recommendation or requested by patient or caregiver choice. This is also reflected in the average younger age of the emicizumab cohort and the larger proportion of individuals under 5 years of age compared with PwHA receiving FVIII treatment, as venous access can be particularly difficult in young children.
In addition to the younger cohort, for whom subcutaneous administration may be of great benefit, those initiating emicizumab early may also include a distinct cohort of older PwHA with other clinical considerations, as a greater proportion of PwHA receiving emicizumab prophylaxis had HIV/HCV infection or AIDS compared with PwHA receiving FVIII prophylaxis. This subgroup of PwHA with HIV/HCV infection is likely to be older, possibly with more advanced hemophilic arthropathy, venous sclerosis and venous access issues, and therefore stands to gain from the channeling of emicizumab. A final important consideration that may contribute to the greater proportion of PwHA receiving emicizumab prophylaxis who have HIV/HCV infection or AIDS, separate from the channeling effect, could be residual fear and anxiety surrounding the use of factor products [25].
A larger proportion of the emicizumab cohort recorded emergency room and outpatient hospital visits in the year before starting their current treatment compared with the FVIII treatment cohorts; this is mirrored by greater healthcare costs, mainly driven by outpatient hospital visits. This may reflect a more clinically complex population with greater healthcare needs, although definitive conclusions are impractical, as the causes for hospitalization are unknown. It may be theorized that they relate to worse outcomes, such as increased time or resources used to treat an acute bleed. However, HCRU did not show a consistent trend of greater need for PwHA who went on to receive emicizumab, as a greater proportion of PwHA receiving FVIII prophylaxis had prior inpatient hospital stays compared with PwHA receiving emicizumab, which was matched by higher inpatient hospital costs.
Emicizumab across time
Corresponding to the approval dates for emicizumab (November 2017 for PwHA with FVIII inhibitors and October 2018 for PwHA without FVIII inhibitors), a decrease in the proportion of PwHA starting emicizumab with prior BPA claims was observed over time. Although it can be presumed that PwHA previously receiving BPAs must be those with FVIII inhibitors, this proxy measure is flawed and is likely to be an underestimate since baseline BPA use should be nearly universal among PwHA starting emicizumab prophylaxis in Q2/Q3 2018, when emicizumab was approved for only PwHA with FVIII inhibitors. By contrast, only 11 of 17 PwHA initiating emicizumab in Q2/Q3 2018 had evidence of previous BPA use. It is possible that some BPA use may not have been captured if administered in only an inpatient setting, where claims may not be individualized (e.g., in the instance of an acute bleed); however, it is expected that over the duration of at least 1 year of coverage most PwHA with FVIII inhibitors would also have received BPAs in an outpatient or pharmacy setting, which would then be captured and the individual excluded.
A greater proportion of PwHA without FVIII inhibitors who started emicizumab when it was first approved had recorded bleeding events, pain and HIV/AIDS during the previous year compared with PwHA who started emicizumab later. However, no trends were seen for the proportion of PwHA with arthropathy or a related disorder or with HCV. Similarly, HCRU and healthcare costs in the year prior to starting treatment with emicizumab were extremely variable, although a greater proportion of later starters on emicizumab had outpatient hospital visits in the previous year, which is contrary to expectations.
Channeling effects in the post-approval period
These data suggest that emicizumab may have been channeled to clinically complex PwHA in the post-approval period. Although the evidence for a time-related component to this channeling (early starters vs later starters) was weaker than hypothesized, perhaps due to the relatively short span of time covered by this analysis, a clear difference can be seen between PwHA initiating emicizumab and PwHA receiving FVIII treatment. This could be an example of channeling bias – ‘a form of allocation bias, where drugs with similar therapeutic indications are prescribed to groups of patients with prognostic differences' [1]. The data are aligned with a Roche Emicizumab Global Safety Database analysis of reported causes of death in PwHA receiving emicizumab, which highlighted the clinical complexity and high prevalence of comorbidities in this population and the prescribing of emicizumab under the compassionate use program, although the bias introduced by assessing only fatalities should be noted [26]. As proposed by the researchers, the impact of being prescribed to a clinically complex subset of PwHA may have skewed emicizumab adverse event reporting post-approval.
The authors believe this theorized effect on safety reporting due to channeling is unlikely to be unique to emicizumab. Therefore, to avoid premature or misleading conclusions about a new treatment's emerging safety profile, perceived or otherwise, the authors suggest that channeling should be considered by clinicians, regulators and patients. This is particularly important in rare diseases or disease subpopulations with a high unmet need, where highly effective novel treatments may be approved with smaller clinical development programs and become rapidly prescribed to patients with poor clinical control. The authors propose that this be known as the Post-Approval Usage Skew Effect (PAUSE). PAUSE refers to the applied effects of channeling bias on pharmacovigilance related to the emerging safety profiles of newly marketed, transformative treatments. These emerging safety profiles may initially appear to vary relative to expectations in the broader patient population based on clinical trial data. However, it is anticipated that once the initial period of channeling has waned, the safety profile will become discernible as treatment utilization becomes more evenly distributed across the labeled population and the epidemiology of the disease itself evolves.
It is unclear when the PAUSE influence may subside; it appears to be present through at least the first year in this study. This is as expected, as many healthcare professionals may wait until their patients' next annual scheduled visit after the approval of emicizumab to discuss a transition. The PAUSE duration is likely to be a function of national prescribing practices, payer reimbursement decisions, the targeted indication, regulatory decision-making and patient acceptance of new therapies based on clinical course. The authors suggest collating data on more established treatments that may have been channeled to specific subgroups upon initial approval to further investigate the PAUSE influence. Moreover, the authors hope that naming the PAUSE phenomenon will draw awareness to it so that it can be given due recognition when considering an innovative new treatment's post-approval benefit–risk assessment, both across the labeled patient population and on an individual basis between patients and their healthcare provider.
Limitations of this analysis
There are some limitations to this analysis. First, although claims data are a valuable method of investigating patient outcomes, they have inherent drawbacks, such as inaccurate or inconsistent professional coding and a lack of individual follow-up [27]. Other disadvantages include not specifying whether PwHA have FVIII inhibitors or the disease severity of PwHA or whether FVIII treatment is prophylactic or episodic. Although a proxy measure for the presence of FVIII inhibitors was used to exclude PwHA with FVIII inhibitors, the authors' data demonstrate that this is an imperfect measure, as discussed earlier. With regard to disease severity, the population of PwHA receiving on-demand FVIII treatment is likely to be biased toward people with nonsevere HA compared with PwHA receiving prophylactic FVIII treatment, which may contribute to differences between these populations. Patient adherence to treatment may also play a role in some people with severe HA appearing to have a nonsevere phenotype or vice versa. Although disease severity is unknown, it may be speculated that emicizumab was channeled to people with severe HA and people with poor adherence, and therefore a severe phenotype, in accordance with the principles of the channeling effect. To remedy the absence of clarification on FVIII treatment, this analysis used the Shrestha et al. algorithm [18], which was developed to distinguish FVIII prophylaxis from on-demand FVIII. However, this is balanced for high specificity and low sensitivity and may underestimate the proportion receiving FVIII prophylaxis [18].
A last limitation is the low numbers of PwHA identified in some cohorts, particularly in the cohorts receiving emicizumab across time, as the data may be unduly influenced by outlying individuals and no inferential analyses were performed. Future studies could provide further insights into the influence of PAUSE on new therapies, and any future longitudinal studies of channeling in emicizumab with larger numbers could attempt further granularity – for example, by distinguishing between life-threatening bleeds such as intracranial hemorrhages and more common bleeds in PwHA such as hematomas, or by in-depth analysis of the populations – to provide more insight into the different cohorts to which emicizumab has been channeled.
Conclusion
Based on data from the year prior to starting their current treatment, PwHA without FVIII inhibitors starting emicizumab appear more clinically complex than those prescribed FVIII prophylaxis or on-demand FVIII, with a higher rate of comorbidities, greater HCRU and higher healthcare costs. Intrinsic limitations of claims-based data and the myriad factors that may influence a change in treatment for PwHA prevent a definitive conclusion. However, these results suggest that emicizumab may have been channeled to a clinically complex patient population upon initial approval and over the following year. The effect of channeling bias on emerging safety profiles of new therapies, here termed ‘PAUSE’, should be considered by regulators, clinicians and patients when objectively evaluating a new therapy's impact. Furthermore, PAUSE may have broader implications and warrants further investigation.
•
Emicizumab, a non-factor therapy for hemophilia A, may have been channeled to clinically complex individuals in the early post-approval period due to perceived benefits such as reduced bleeding and subcutaneous administration.
•
Individuals starting emicizumab had more bleeding and greater healthcare costs in the year prior to initiation compared with individuals receiving traditional factor VIII therapies.
•
Channeling may have impacted the initial safety profile of emicizumab, a consequence here termed the Post-Approval Usage Skew Effect.
•
Intrinsic limitations of claims-based data prevent a definitive conclusion.
Author contributions
F Nissen, P Kuebler, I Faghmous, T Xu, C Flores and T Chang contributed to the initial design and concept of this study. C Flores performed the data analysis. All authors interpreted the data and critically reviewed the manuscript prior to submission. All authors agree to be accountable for all aspects of the work.
Financial & competing interests disclosure
This study was funded by F Hoffmann-La Roche Ltd. None of the authors received honoraria or fees for their contribution to the development of this manuscript or the supplementary material. F Nissen is a current employee of F Hoffmann-La Roche Ltd. I Faghmous is a previous employee of F Hoffmann-La Roche Ltd. and Gilead Sciences, Inc. P Kuebler is a current employee of and holds shares in Genentech, Inc. M Howard is a previous contract employee of Genentech, Inc.; is a current employee of and holds shares in F Hoffmann-La Roche Ltd.; and has received expenses from Genentech, Inc. T Xu is a previous employee of AG Pharma and current employee of F Hoffmann La-Roche Ltd. and has received expenses from AG Pharma and F Hoffmann La-Roche Ltd. C Flores is a current employee of Genesis Research. T Chang is a previous employee of Genentech, Inc., and current employee of Spark Therapeutics. A Mahajerin has been on a speakers’ bureau for Alexion Pharmaceuticals; Spark Therapeutics; and Genentech, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support was provided by P Tate of Ashfield MedComms, an Ashfield Health company, and was funded by F Hoffmann-La Roche Ltd.
Ethical conduct of research
Because of the nature of this study, institutional review board approval and informed consent were not required. The code listings used can be found in the supplementary material.
Data sharing statement
Data are available from the IBM MarketScan Commercial Claims and Encounters and PharMetrics Plus databases.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.xlsx)
- Download
- 485.38 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Petri H, Urquhart J. Channeling bias in the interpretation of drug effects. Stat. Med. 10(4), 577–581 (1991).
•• Introduces the concepts of channeling and channeling bias in drug markets, whereby ‘drugs with similar therapeutic indications are prescribed to groups of patients with prognostic differences’.
2.
Hudson M, Suissa S. Avoiding common pitfalls in the analysis of observational studies of new treatments for rheumatoid arthritis. Arthritis Care Res. 62(6), 805–810 (2010).
3.
Franchini M, Mannucci PM. Past, present and future of hemophilia: a narrative review. Orphanet J. Rare Dis. 7, 24 (2012).
4.
Franchini M. The modern treatment of haemophilia: a narrative review. Blood Transfus. 11(2), 178–182 (2013).
5.
Aledort L, Mannucci PM, Schramm W, Tarantino M. Factor VIII replacement is still the standard of care in haemophilia A. Blood Transfus. 17(6), 479–486 (2019).
6.
Shima M, Hanabusa H, Taki M et al. Factor VIII – mimetic function of humanized bispecific antibody in hemophilia A. N. Engl. J. Med. 374(21), 2044–2053 (2016).
7.
US FDA. FDA approves emicizumab-kxwh for prevention and reduction of bleeding in patients with hemophilia A with factor VIII inhibitors (2017). www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-emicizumab-kxwh-prevention-and-reduction-bleeding-patients-hemophilia-factor-viii
8.
FDA. FDA approves emicizumab-kxwh for hemophilia A with or without factor VIII inhibitors (2018). www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-emicizumab-kxwh-hemophilia-or-without-factor-viii-inhibitors
9.
Oldenburg J, Mahlangu JN, Kim B et al. Emicizumab prophylaxis in hemophilia A with inhibitors. N. Engl. J. Med. 377(9), 809–818 (2017).
• Describes the safety and efficacy outcomes of a pivotal phase III clinical trial for emicizumab prophylaxis in people with severe hemophilia A with factor VIII (FVIII) inhibitors.
10.
Mahlangu J, Oldenburg J, Paz-Priel I et al. Emicizumab prophylaxis in patients who have hemophilia A without inhibitors. N. Engl. J. Med. 379(9), 811–822 (2018).
• Describes the safety and efficacy outcomes of a pivotal phase III clinical trial for emicizumab prophylaxis in people with severe hemophilia A without FVIII inhibitors.
11.
Pipe SW, Shima M, Lehle M et al. Efficacy, safety, and pharmacokinetics of emicizumab prophylaxis given every 4 weeks in people with haemophilia A (HAVEN 4): a multicentre, open-label, non-randomised phase 3 study. Lancet Haematol. 6(6), e295–e305 (2019).
12.
Young G, Liesner R, Chang T et al. A multicenter, open-label, phase 3 study of emicizumab prophylaxis in children with hemophilia A with inhibitors. Blood 134(24), 2127–2138 (2019).
13.
Barg AA, Livnat T, Budnik I et al. Emicizumab treatment and monitoring in a paediatric cohort: real-world data. Br. J. Haematol. 191(2), 282–290 (2020).
14.
Jimenez-Yuste V, Klamroth R, Castaman G et al. Second interim analysis results from the STASEY trial: a single-arm, multicenter, open-label, phase III clinical trial to evaluate the safety and tolerability of emicizumab prophylaxis in people with hemophilia A (PwHA) with FVIII inhibitors. ISTH (2020). (PosterPB0958).
15.
McCary I, Guelcher C, Kuhn J et al. Real-world use of emicizumab in patients with haemophilia A: bleeding outcomes and surgical procedures. Haemophilia 26(4), 631–636 (2020).
16.
Reyes A, Révil C, Niggli M et al. Efficacy of emicizumab prophylaxis versus factor VIII prophylaxis for treatment of hemophilia A without inhibitors: network meta-analysis and sub-group analyses of the intra-patient comparison of the HAVEN 3 trial. Curr. Med. Res. Opin. 35(12), 2079–2087 (2019).
• Compares the efficacy of emicizumab prophylaxis with that of FVIII prophylaxis in people with hemophilia A (PwHA) without FVIII inhibitors.
17.
Witmer C, Young G. Factor VIII inhibitors in hemophilia A: rationale and latest evidence. Ther. Adv. Hematol. 4(1), 59–72 (2013).
18.
Shrestha A, Eldar-Lissai A, Hou N, Lakdawalla DN, Batt K. Real-world resource use and costs of haemophilia A-related bleeding. Haemophilia 23(4), e267–e275 (2017).
•• Reports on an analysis of claims data in hemophilia A and describes the algorithm to differentiate between prophylactic and episodic treatment and the method of identifying recorded bleeding events used in the authors' study.
19.
Parnes A, Mahlangu JN, Pipe SW et al. Patient preference for emicizumab versus prior factor therapy in persons with haemophilia A: results from the HAVEN 3 and HAVEN 4 studies. Haemophilia 27(6), e772–e775 (2021).
•• Describes the results of a preference survey administered to people in the HAVEN 3 and HAVEN 4 trials to investigate whether they preferred emicizumab to their previous therapy and the reason for their preference.
20.
Eichler H, Angchaisuksiri P, Astermark J et al. Efficacy and safety of subcutaneous prophylaxis with concizumab in patients with severe hemophilia A without inhibitors: results from the phase 2 explorer5 trial. Blood 134(Suppl. 1), 2417 (2019).
21.
Pasi KJ, Georgiev P, Mant T et al. Fitusiran, an investigational RNAi therapeutic targeting antithrombin for the treatment of hemophilia: interim results from a phase 2 extension study in patients with hemophilia A or B with and without inhibitors. ISTH. OC 11.13 (2017).
22.
Batty P, Lillicrap D. Advances and challenges for hemophilia gene therapy. Hum. Mol. Genet. 28(R1), R95–R101 (2019).
23.
Angelini D, Sood SL. Managing older patients with hemophilia. Hematology 2015(1), 41–47 (2015).
24.
Siboni SM, Mannucci PM, Gringeri A et al. Health status and quality of life of elderly persons with severe hemophilia born before the advent of modern replacement therapy. J. Thromb. Haemost. 7(5), 780–786 (2009).
25.
Saxena K. Barriers and perceived limitations to early treatment of hemophilia. J. Blood Med. 4, 49–56 (2013).
26.
Peyvandi F, Mahlangu J, Pipe S et al. Application of a hemophilia mortality framework to the Emicizumab Global Safety Database. J. Thromb. Haemost. 19(S1), 32–41 (2020).
•• Discusses an analysis of the fatalities reported to the Roche Emicizumab Global Safety Database and examines the medical complexity of the population.
27.
Tyree PT, Lind BK, Lafferty WE. Challenges of using medical insurance claims data for utilization analysis. Am. J. Med. Qual. 21(4), 269–275 (2006).
• Highlights the challenges and limitations associated with insurance claims data.
Information & Authors
Information
Published In
Pages: 717 - 728
PubMed: 35535702
Copyright
© 2022 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 8 November 2021
Accepted: 13 April 2022
Published online: 10 May 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Channeling effects in the prescription of new therapies: the case of emicizumab for hemophilia A. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0278
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Caitlin Montcrieff, Jorge Caicedo, Alicia Cerretani, Angela (Qi) Fan, Michael Bullano, Ekaterina Ponomareva, Bleeding rates, healthcare utilization, and costs among patients with hemophilia a without inhibitors treated with concomitant octocog alfa or extended half-life factor VIII while on emicizumab prophylaxis, Journal of Medical Economics, 10.1080/13696998.2026.2642552, 29, 1, (835-847), (2026).
- Pratima Chowdary, Letizia Polito, Mark Oellerich, Romain Chafaie, Tom Burke, Tom Blenkiron, Enrico Ferri Grazzi, Mental Health, Work Productivity, and Quality of Life in People with Severe Haemophilia A Receiving Prophylaxis: Findings from the CHESS Data Platform, TH Open, 10.1055/a-2658-6151, 09, CP, (2025).
- Leonie Glasson, Entering a New Era in Protection in Haemophilia A, EMJ Hematology, 10.33590/emjhematol/THKR9677, (25-32), (2025).
- Anouk A.M.T. Donners, Konrad van der Zwet, Carin M.A. Rademaker, Toine C.G. Egberts, Roger E.G. Schutgens, Kathelijn Fischer, The efficacy of the entire-vial dosing of emicizumab: Real-world evidence on plasma concentrations, bleeds, and drug waste, Research and Practice in Thrombosis and Haemostasis, 10.1016/j.rpth.2023.100074, 7, 2, (100074), (2023).
- Víctor Jiménez‐Yuste, Flora Peyvandi, Robert Klamroth, Giancarlo Castaman, Chandrakala Shanmukhaiah, Savita Rangarajan, Jaime García Chavez, Raul Martinez, Gili Kenet, Hazaa Alzahrani, Susan Robson, Christophe Schmitt, Anna Kiialainen, Oliver Meier, Margareth Ozelo, Safety and efficacy of long‐term emicizumab prophylaxis in hemophilia A with factor VIII inhibitors: A phase 3b, multicenter, single‐arm study (STASEY), Research and Practice in Thrombosis and Haemostasis, 10.1002/rth2.12837, 6, 8, (e12837), (2022).