Real-world economic and clinical outcomes associated with current hemostatic matrix use in spinal surgery
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Bleeding during spine surgery is controlled using topical hemostatic agents. Studies have reported outcomes between Surgiflo® and Floseal, the most widely used flowable hemostatic matrices, but have not included the latest Surgiflo formulation which is more adherent to the bleeding surface than prior formulations. Materials & methods: A propensity score-matched analysis was conducted using the Premier Healthcare Database to compare economic and clinical outcomes of adults undergoing inpatient spinal surgery between 2013 and 2018 receiving current Surgiflo or Floseal. Results: This retrospective study included 28,910 patients in each group and found comparable outcomes for bleeding events, overall transfusion rate, inpatient mortality and readmissions between Surgiflo and Floseal. Surgiflo was associated with $430 (USD) lower hospitalization costs, shorter length of stay and shorter operating room time than Floseal.
Plain language summary
Topical hemostatic agents such as Surgiflo® and Floseal are used during invasive surgery to manage bleeding. We compared outcomes of spine surgeries that used either of two most frequently used topical hemostatic agents, Surgiflo or Floseal. This is the largest retrospective study presenting economic and clinical outcomes of patients receiving Surgiflo versus Floseal during spine surgery using the latest product formulations. The study suggests that clinical outcomes are comparable between Surgiflo and Floseal groups and that Surgiflo is associated with lower hospitalization costs, slightly shorter hospital stay and shorter operating room time among patients undergoing spine surgery.
The USA is seeing an increase in the number and complexity of spinal surgical procedures [1,2]. Although bleeding is anticipated in virtually all types of surgical procedures, spine surgeries are typically longer than other elective surgeries and are frequently associated with major blood loss and transfusions [3]. Due to the intricate nature of spine surgery, excessive bleeding can affect visualization of neural elements [4]. Failure to maintain hemostasis during surgery can result in bleeding and bleeding-related complications and an increase in patient morbidity and mortality, greater healthcare resource utilization and elevated costs [5–7].
Bleeding during spine surgery is often controlled using topical hemostatic agents when bleeding cannot be controlled by conventional methods (such as suturing, cautery or manual compression) [8–13]. In the USA, the most commonly used hemostatic agents are gelatin-thrombin-based flowable topical hemostats; Floseal (Baxter Healthcare Corporation, IL, USA) on the market since 2000 and Surgiflo® (Ethicon Incorporated, NJ, USA) on the market since 2006 [8,14]. Floseal is made of a matrix of bovine gelatin and human thrombin with a preparation time of 168 s, and it is reabsorbed within 6–8 weeks. Surgiflo has a preparation time of 81 s, and reabsorption time of 4–6 weeks [10,11]. Both products have been labeled as hemostatic matrices and have dual mechanisms of action in the blood clotting cascade via contact activation and active biologic agents (e.g., thrombin). Both agents have proven to be advantageous in surgery because of their ability to conform to wound contours and fill deep lesions [15,16]. Previous studies have shown that Surgiflo and Floseal have proven to shorten surgery time, reduce transfusion need, better manage an anticoagulated patient, improve recovery time and reduced wound exposure [17–19].
There is limited economic and clinical evidence comparing Surgiflo and Floseal. Non-observational studies comparing Surgiflo and Floseal have described similar clinical outcomes between the two products. However, conclusions relating to cost, resource use, blood transfusion and complications were mixed [8,19–21]. Further, present day applicability of these studies may be limited due to their focus on a previous formulation of Surgiflo available prior to 2012 and small sample sizes [8,19–22]. A newer, current formulation of Surgiflo possesses a re-engineered gelatin matrix that increased the degree of cross-linking of gelatin particles and increased solid content in the gelatin matrix, leading to increased paste viscosity, less runniness and better adherence to the bleeding surface relative to the prior formulation [23]. Thus, the objective of this study was to assess the comparative economic and clinical outcomes of patients treated with the current formulation of Surgiflo versus Floseal during spinal surgeries.
Materials & methods
Data source
The data for this retrospective study was obtained from the Premier Healthcare Database (PHD) for years 2013–2018. The PHD collects US hospital administrative data for all payers and covers over 700 hospitals representing over 8 million inpatient encounters per year. The PHD is geographically diverse and captures 20% of inpatient hospital discharges in the USA [24].
Cohort selection
All patients included in this study were required to have undergone inpatient spinal surgery (index surgery and admission) between 1 January 2013 and 1 June 2018 and received either the most current Surgiflo formulation or Floseal during the surgery. Spinal surgeries were defined by primary International Classification of Diseases, 9th and 10th Revision (ICD-9-CM/ICD-10-PCS) procedure codes (Appendix A). Patients were required to be ≥18 years at admission date. In patients with multiple eligible surgeries, the first eligible surgery (index surgery and admission) was selected.
Exclusion criteria included: both Surgiflo and Floseal were administered during the index surgery, surgery duration was missing, duration of surgery was less than 1 h or more than 12 h, hospitalization did not have complete information (such as admission and discharge dates missing), patient had secondary procedure codes for other surgeries such as cardiovascular surgery during the same hospitalization, and surgeries used Surgiflo and Floseal with unclear product description (e.g., no description of formulation or dosage).
Clinical information such as diagnoses, procedures, hemostatic matrix use and formulation and comorbidity information were defined using a combination of ICD-9-CM codes, ICD-10-CM codes, procedure codes and text searches in hospital chargemaster data as applicable. Use of Surgiflo and Floseal product and units of product used were verified using product description and quantity of the product reported (Surgiflo 8 ml and Floseal 5 or 10 ml). More information on variable definitions including coding schema is available in Appendix B and C.
Patient & hospital characteristics
Information was collected on patient demographics (age, sex, race and payor), clinical characteristics (admission type, the Charlson Comorbidity Index score [25], a summary measure of overall patient comorbidity that has been widely validated against numerous different patient outcomes, and surgical details) and hospital characteristics (region, type and bed size). Spine surgeries were defined according to the location (cervical, thoracic, lumbar, other and unknown); type (fusion, refusion, fusion or refusion and unknown); approach (anterior, posterior and unknown); and level of fusion (≥2 and others; single-level fusions involve two vertebrae while multilevel fusions involve three or more vertebrae) based on ICD-9-CM/ICD-10-PCS procedure codes.
Outcomes
Clinical outcomes included bleeding diagnoses and transfusions recorded during the index admission. Bleeding diagnoses were documented by ICD-9-CM/ICD-10-CM diagnosis codes designated as not present on admission or any ICD-9-CM/ICD-10-PCS bleeding event procedure codes during the hospitalization (Appendix B). Transfusions were documented by ICD-9-CM/ICD-10-PCS codes and hospital chargemaster records (Appendix C). As topical hemostats are used to control bleeding, the documentation of a bleeding diagnoses despite topical hemostat use was presumed to be a marker of bleeding severity.
Outcome measures such as bleeding and transfusion were assessed during the entire hospitalization and post-operatively. Blood transfusion and units of blood transfused (any blood product) during the hospitalization were defined within day-1 (surgery start to end of the first day post-surgery), and days 2–4 following the surgery. Other outcomes included inpatient mortality assessed using hospital discharge status, healthcare resource utilization and hospital costs.
Hospital costs reported for the index hospitalization were adjusted to 2018 USD using the Medical Care component of the US Bureau of Labor Statistics Consumer Price Index. Resource utilization outcomes included length of stay (LOS) of the index hospitalization; intensive care unit (ICU) admission and days in ICU; duration of surgery; and 30-, 60- and 90-day readmission to the same hospital in which the index spine surgery was performed.
Statistical analysis
A descriptive analysis was conducted to understand the differences between Surgiflo and Floseal groups. Continuous variables (e.g., cost and LOS) were described as means, standard deviation and ranges and compared using student t-tests (normal distribution) or Wilcoxon rank sum tests (skewed distribution, such as costs). Categorical variables were described as frequencies and proportions were compared using Pearson χ2 tests.
Patients in the Surgiflo group were propensity score matched (PSM) to those in the Floseal group using 1:3 variable ratio matching without replacement. The propensity score was derived from a multivariable logistic regression in which the dependent variable was membership in the Surgiflo versus Floseal group and the independent variables were all patient demographics, patient and surgery clinical characteristics and hospital characteristics described above. In addition, patients were exactly matched on index year and type of spinal surgery procedure (by spinal region, type, position and the level of fusion). After PSM, a sampling weight (probability weight for Floseal patients that was inversely proportional to the total number of Floseal patients that were matched to the same Surgiflo patient) was applied to account for the variable-ratio nature of the match, effectively rendering the weighted post matching sample to be 1:1. The standardized differences of the matching covariates were calculated to verify appropriate balance, indicated by an absolute value of 10%.
Outcomes were compared between the matched Surgiflo or Floseal groups using generalized estimating equations with an exchangeable working correlation structure [26]. For binary outcomes (e.g., inpatient mortality), a binomial distribution and logit link was used; for LOS and number of ICU days, a negative binomial distribution and log link was used; for costs, a gamma distribution and log link was used [27]. All post matching multivariable regression models were adjusted for unbalanced characteristics after PSM.
As prolonged surgery time can be reflective of either an outcome of topical hemostat use or instead a potential proxy measure of the inherent complexity of a surgical case, a sensitivity analysis was conducted where multivariable models were repeated adjusting for the duration of the surgery.
All analyses were conducted using SAS version 9.4 (SAS Institute Inc., NC, USA), and a two-sided p-value of <0.05 was considered statistically significant.
Results
Study sample
Prior to matching, 28,913 Surgiflo and 70,271 Floseal patients in the database fulfilled the eligibility criteria. After PSM, there were 28,910 Surgiflo patients matched to 57,820 Floseal patients. After applying the sampling weight, there were 28,910 Surgiflo patients and 28,910 Floseal patients. Figure 1 describes the cohort selection process.
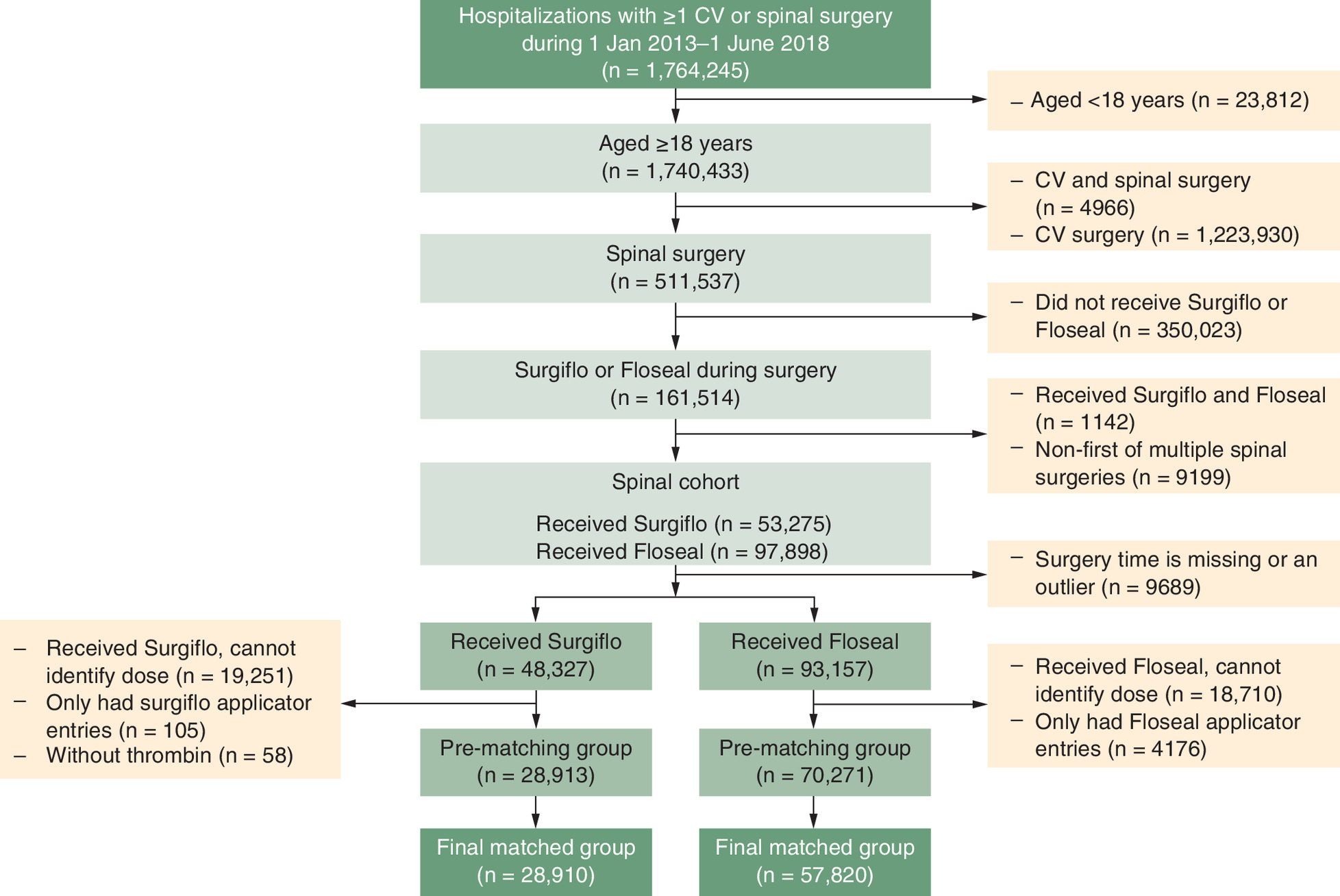
Figure 1. Cohort selection flowchart
CV: Cardiovascular.
Patient & hospital characteristics
Table 1 presents patient demographics, patient and surgery clinical characteristics and hospital characteristics before and after PSM. Prior to matching, average age was 59 years and 47% of the sample were male, slightly higher proportion of patients with Surgiflo were White (81.8 vs 80.4%) and were married (59.9 vs 59.3%) compared with Floseal (p < 0.05). Over 88% spinal surgeries in both groups were elective.
| Prematching | Post matching | |||||
|---|---|---|---|---|---|---|
| Floseal | Surgiflo | p-value | Floseal | Surgiflo | Std diff. (%)† | |
| n = 70,271 | n = 28,913 | n = 28,910 | n = 28,910 | |||
| Patient demographics | ||||||
| Age, mean (SD) | 59.4 (13.2) | 59.2 (13.2) | 0.0307 | 59.2 (13.2) | 59.2 (13.2) | -0.4 |
| Male (vs female) | 33,025 (47.0) | 13,703 (47.4) | 0.2547 | 13,757 (47.6) | 13,701 (47.4) | -0.4 |
| Race, n (%) | ||||||
| White | 56,478 (80.4) | 23,644 (81.8) | <0.0001 | 24,054 (83.2) | 23,642 (81.8) | -3.8 |
| Black | 4801 (6.8) | 3230 (11.2) | <0.0001 | 2898 (10.0) | 3229 (11.2) | 3.7 |
| Other | 8992 (12.8) | 2039 (7.1) | <0.0001 | 1958 (6.8) | 2039 (7.1) | 1.1 |
| Payor, n (%) | ||||||
| Medicare | 31,336 (44.6) | 12,381 (42.8) | <0.0001 | 12,556 (43.4) | 12,380 (42.8) | -1.2 |
| Medicaid | 5173 (7.4) | 1934 (6.7) | 0.0002 | 2018 (7.0) | 1934 (6.7) | -1.2 |
| Commercial | 26,465 (37.7) | 10,934 (37.8) | 0.646 | 10,796 (37.3) | 10,932 (37.8) | 1.0 |
| Other | 7297 (10.4) | 3664 (12.7) | <0.0001 | 3540 (12.2) | 3664 (12.7) | 1.3 |
| Clinical characteristics | ||||||
|---|---|---|---|---|---|---|
| Admission Type, n (%) | ||||||
| Emergency | 4446 (6.3) | 1959 (6.8) | 0.009 | 1982 (6.9) | 1959 (6.8) | -0.3 |
| Urgent | 2592 (3.7) | 974 (3.4) | 0.0139 | 1,078 (3.7) | 974 (3.4) | -1.9 |
| Elective | 62,120 (88.4) | 25,482 (88.1) | 0.2336 | 25,242 (87.3) | 25,479 (88.1) | 2.5 |
| Trauma | 701 (1.0) | 397 (1.4) | <0.0001 | 384 (1.3) | 397 (1.4) | 0.4 |
| Other | 412 (0.6) | 101 (0.4) | <0.0001 | 224 (0.8) | 101 (0.4) | -1.5 |
| CCI, mean (SD) | 0.8 (1.2) | 0.8 (1.2) | 0.437 | 0.8 (1.3) | 0.8 (1.3) | -1.6 |
| Surgery location, n (%) | ||||||
| Cervical | 25,793 (36.7) | 11,436 (39.6) | <0.0001 | 11,433 (39.6) | 11,433 (39.6) | 0.0 |
| Thoracic | 1875 (2.7) | 768 (2.7) | 0.9151 | 768 (2.7) | 768 (2.7) | 0.0 |
| Lumbar | 37,287 (53.1) | 14,703 (50.9) | <0.0001 | 14,703 (50.9) | 14,703 (50.9) | 0.0 |
| Other‡ | 4666 (6.6) | 1825 (6.3) | 0.0577 | 1825 (6.3) | 1825 (6.3) | 0.0 |
| Unknown | 650 (0.9) | 181 (0.6) | <0.0001 | 181 (0.6) | 181 (0.6) | 0.0 |
| Surgery type, n (%) | ||||||
| Fusion | 62,773 (89.3) | 26,100 (90.3) | <0.0001 | 26,097 (90.3) | 26,097 (90.3) | 0.0 |
| Refusion | 1285 (1.8) | 426 (1.5) | <0.0001 | 426 (1.5) | 426 (1.5) | 0.0 |
| Fusion or refusion | 153 (0.2) | 18 (0.1) | <0.0001 | 18 (0.1) | 18 (0.1) | 0.0 |
| Unknown | 6060 (8.6) | 2369 (8.2) | 0.0272 | 2369 (8.2) | 2369 (8.2) | 0.0 |
| Surgery approach, n (%) | ||||||
| Anterior | 36,285 (51.6) | 15,636 (54.1) | <0.0001 | 15,636 (54.1) | 15,636 (54.1) | 0.0 |
| Posterior | 32,629 (46.4) | 12,896 (44.6) | <0.0001 | 12,896 (44.6) | 12,896 (44.6) | 0.0 |
| Unknown | 1357 (1.9) | 381 (1.3) | <0.0001 | 378 (1.3) | 378 (1.3) | 0.0 |
| Surgery fusion level, n (%) | ||||||
| Fusion level <2 | 54,450 (77.5) | 22,357 (77.3) | 0.5822 | 22,357 (77.3) | 22,357 (77.3) | 0.0 |
| Fusion level ≥2 | 15,821 (22.5) | 6556 (22.7) | 0.5822 | 6553 (22.7) | 6553 (22.7) | 0.0 |
| Hospital characteristics | ||||||
|---|---|---|---|---|---|---|
| Region, n (%) | ||||||
| Midwest | 7610 (10.8) | 2946 (10.2) | 0.003 | 2870 (9.9) | 2945 (10.2) | 0.9 |
| Northwest | 18,983 (27.0) | 3314 (11.5) | <0.0001 | 3089 (10.7) | 3314 (11.5) | 2.5 |
| South | 28,920 (41.2) | 15,520 (53.7) | <0.0001 | 15,379 (53.2) | 15,518 (53.7) | 1.0 |
| West | 14,758 (21.0) | 7133 (24.7) | <0.0001 | 7572 (26.2) | 7133 (24.7) | -3.5 |
| Type, n (%) | ||||||
| Urban (vs rural) | 66,016 (93.9) | 26,187 (90.6) | <0.0001 | 26,615 (92.1) | 26,184 (90.6) | -5.3 |
| Teaching (vs non teaching) | 36,613 (52.1) | 10,901 (37.7) | <0.0001 | 10,984 (38.0) | 10,899 (37.7) | -0.6 |
| Bed size, n (%) | ||||||
| 0–100 | 1284 (1.8) | 669 (2.3) | <0.0001 | 801 (2.8) | 669 (2.3) | -2.9 |
| 101–500 | 42,836 (61.0) | 19,764 (68.4) | <0.0001 | 18,322 (63.4) | 19,763 (68.4) | 10.5 |
| >500 | 26,151 (37.2) | 8480 (29.3) | <0.0001 | 9787 (33.9) | 8478 (29.3) | -9.8 |
†
Standardized mean difference (percent): absolute value of <10% is considered as being balanced.
‡
Surgeries including lumbosacral and sacroiliac fusion were categorized as ‘Other’.
CCI: Charlson Comorbid Index; Std diff.: Standardized mean difference.
After PSM, all baseline patient and hospital characteristics were similar between the two groups with the exception of hospital bed size. Therefore, hospital bed size was adjusted for in the post-matching multivariable regression. In the postmatching sample, mean (SD) Charlson Comorbidity Index scores were also similar in Surgiflo versus Floseal groups (Table 1).
Over 90% of surgeries were fusion surgeries and over 50% occurred in the lumbar spine. Approximately half of the patients received surgeries in the South region of the United States (53% in Floseal vs 54% in Surgiflo). Surgical approach was anterior in 54.1% surgeries and posterior in 44.6% surgeries. A majority of the patients had surgeries in urban hospitals (92% in Floseal vs 91% in Surgiflo) and hospitals with 101–500 beds provided care for most of the patients (63% in Floseal vs 68% in Surgiflo).
Comparative outcomes
Table 2 summarizes the results of post-matching multivariable analyses.
| Outcomes | Surgiflo, n (%) n = 28,910 | Floseal, n (%) n = 28,910 | OR‡ | 95% CI | p-value | |
|---|---|---|---|---|---|---|
| Binary outcome† | ||||||
| Any documented bleeding event§ | 460 (1.6%) | 458 (1.6%) | 1.01 | 0.90 | 1.14 | 0.8431 |
| Any postoperative bleeding¶ | 11 (0.0%) | 18 (0.1%) | 0.63 | 0.30 | 1.33 | 0.2247 |
| Any transfusion# | 2776 (9.6%) | 2733 (9.5%) | 1.03 | 0.98 | 1.08 | 0.3056 |
| Any transfusion within 0–1 days of surgery | 2019 (7.0%) | 1991 (6.9%) | 1.02 | 0.96 | 1.08 | 0.4811 |
| Any transfusion within 2–4 days of surgery | 677 (2.3%) | 762 (2.6%) | 0.89 | 0.81 | 0.98 | 0.0159 |
| PRBC transfusion within 0–1 days of surgery | 1001 (3.5%) | 839 (2.9%) | 1.21 | 1.12 | 1.32 | <.0001 |
| PRBC transfusion within 2–4 days of surgery | 507 (1.8%) | 479 (1.7%) | 1.07 | 0.95 | 1.2 | 0.2508 |
| Any ICU admission | 1894 (6.6%) | 3390 (11.7%) | 0.55 | 0.52 | 0.58 | <.0001 |
| Inpatient mortality (reference dead) | 63 (0.2%) | 62 (0.2%) | 1.04 | 0.76 | 1.44 | 0.7928 |
| Any readmission | ||||||
| Within 30 days | 945 (3.3%) | 892 (3.1%) | 1.06 | 0.97 | 1.15 | 0.1960 |
| Within 60 days | 2003 (6.9%) | 1967 (6.8%) | 1.02 | 0.96 | 1.08 | 0.5058 |
| Within 90 days | 2378 (8.2%) | 2313 (8.0%) | 1.03 | 0.98 | 1.09 | 0.2726 |
| Continuous outcome†† | IRR‡‡ | 95% CI | ||||
| LOS (days) | 3.4 (3.2) | 3.5 (2.3) | 0.98 | 0.96 | 0.99 | 0.0016 |
| ICU stay (days)§§ | 3.3 (4.6) | 3.5 (3.1) | 0.95 | 0.88 | 1.03 | 0.2004 |
| Total cost (USD) | 29,949 (20,226.9) | 30,379 (16,280.3) | 0.99 | 0.98 | 1.00 | 0.0193 |
| Duration of surgery (min) | 246.6 (105.0) | 250.8 (76.8) | 0.99 | 0.98 | 0.99 | <.0001 |
†
Based on a GLM with GEE (binomial distribution and logit link), weighted and adjusted for unbalanced characteristics after PSM and marital status.
‡
The OR indicates the probability of having an outcome in Surgiflo as compared with Floseal.
§
Any documented bleeding event was identified using ICD-9-CM/ICD-10-CM bleeding event diagnosis codes (Appendix B) designated as not ‘present on admission’ or any ICD-9-CM/ICD-10-PCS bleeding event procedure codes during the hospitalization.
¶
Any postoperative bleeding event was identified using ICD-9-CM/ICD-10-PCS bleeding event procedure codes (Appendix B) performed after the day of the index surgery.
#
Blood transfusion was identified using ICD-9-CM/ICD-10-PCS procedure codes (Appendix C) and searching for text strings in hospital charge descriptions.
††
Based on a GLM with GEE (negative binomial distribution and log link for LOS, number of ICU days, duration of surgery; gamma distribution and log link for costs) weighted and adjusted for unbalanced characteristics after PSM.
‡‡
IRR indicates the relative risk of an outcome in Surgiflo as compared with Floseal.
§§
ICU admission is defined using chargemaster description.
GEE: Generalized estimating equations; GLM: Generalized linear model; ICU: Intensive care unit; IRR: Incidence risk ratio; LOS: Length of stay; OR: Odds ratio; PRBC: Packed red blood cell; PSM: Propensity score matching.
In all patients, documented bleeding events occurred in less than 2% of patients undergoing spinal surgery (Table 2). Incidence of bleeding was similar between Surgiflo versus Floseal groups (1.6 vs 1.6%; odds ratio [OR]: 1.01; 95% CI: 0.90–1.14; p = 0.843).
Overall rate of blood transfusion was similar in the Surgiflo versus Floseal groups (9.6 vs 9.5%; OR: 1.03; 95% CI: 0.98–1.08; p = 0.306). Within 0–1 days of surgery, 7.0% of Surgiflo and 6.9% of Floseal patients required a blood transfusion and there was no statistical difference between the two groups (OR: 1.02, 95% CI: 0.96–1.08; p = 0.481). Rate of any blood transfusion within 2–4 days of surgery was significantly lower in the Surgiflo versus Floseal group (2.3 vs 2.6%; OR: 0.89; 95% CI: 0.81–0.98; p = 0.016). Rate of PRBC transfusion within 0–1 days was higher in the Surgiflo versus Floseal group (3.5 vs 2.9%; OR: 1.21; 95% CI: 1.12–1.32; p < 0.0001) and comparable within 2–4 days of surgery (1.8 vs 1.7%; OR: 1.07; 95% CI: 0.95–1.12; p = 0.251).
Duration of surgery was shorter in the Surgiflo versus Floseal group (246.6 vs 250.8 min; incidence risk ratio [IRR]: 0.99; 95% CI: 0.98–0.99; p < 0.001). Proportion of patients admitted to the ICU was significantly lower in the Surgiflo versus Floseal group (6.6 vs 11.7%; OR: 0.55; 95% CI: 0.52–0.58; p = 0.2004). Mean length of hospital stay was shorter in the Surgiflo versus Floseal group (3.4 vs 3.5 days; IRR: 0.98; 95% CI: 0.96–0.99; p = 0.0016). Inpatient mortality was similar between the Surgiflo and Floseal groups (0.2 vs 0.2%; OR: 1.04; 95% CI: 0.76–1.44; p = 0.7928). In both Surgiflo and Floseal groups, about 3% patients were readmitted within 30 days, 7% within 60 days and 8% within 90 days (all p < 0.05).
Average adjusted total cost of the index hospitalization was significantly lower in the Surgiflo versus Floseal group ($29,949 vs $30,379 [USD]; IRR: 0.99; 95% CI: 0.98–1.00; p = 0.0193).
Sensitivity & exploratory analyses
A sensitivity analysis adjusting for the duration of the surgery in all the models yielded similar results across the outcomes (p < 0.05; results not presented). As noted above, the proportion of patients admitted to the ICU was substantially lower in the Surgiflo group versus the Floseal group; to investigate whether this could potentially explain the lower costs in the Surgiflo group, we conducted an exploratory descriptive analysis to understand the costs of patients with versus without ICU admission. Indeed, patients admitted to the ICU had substantially higher total cost of the index hospitalization than those who were not admitted: mean (SD) $55,519 ($35,041) for Surgiflo and $53,269 ($27,608) for Floseal when admitted to the ICU versus $28,147 ($17,383) for Surgiflo and $27,389 ($12,605) for Floseal when not admitted to the ICU. Therefore, the higher proportion of patients admitted to the ICU in the Floseal group, combined together with the higher costs of patients with ICU admission, are likely to be a substantial driver of the between group cost differences.
Discussion
Our study provides a real-world economic and clinical comparison of Surgiflo and Floseal in spine surgery during 2013–2018 and the only large retrospective comparison between the two hemostatic matrices using the current Surgiflo formulation. Based on this study, Surgiflo was associated with an average $430 cost saving compared with Floseal. Surgiflo was also associated with a shorter LOS and a shorter surgery duration among patients undergoing spine surgery. Overall transfusion, documented bleeding events, inpatient mortality and readmission up to 90 days post discharge were comparable across the products. The study found that variation in results for blood transfusion may be a function of the data source and coding practices across hospitals when reporting blood transfusions.
Previous studies comparing clinical product performance between Surgiflo and Floseal have found mixed or comparable results indicating that clinical outcomes during spine surgery are not dependent on choice of gelatin hemostatic matrix [19,21]. In a prospective cohort study of 149 thoracic and lumbar spine surgeries, Landi et al. analyzed the time required to stop bleeding completely in the operative field by application of Surgiflo versus Floseal [19]. Landi et al. concluded that Surgiflo and Floseal did not show any relevant differences in terms of their ease of use or efficacy [19]. Similarly, Gazzerri et al. compared bleeding control, efficacy and safety between Surgiflo and Floseal in 318 cranial or spinal surgeries [21]. Gazzeri et al. noted no complications associated with either agent during spine surgery and that hemostasis was achieved in all but eight cases and deemed the two agents ‘equivalent’ [21]. In our study, bleeding outcomes, overall transfusion rates and inpatient mortality was comparable between the Surgiflo and Floseal group. This corroborates the previous findings indicating that clinically, both Surgiflo and Floseal group are efficient and similar in terms of controlling bleeding in spinal surgeries.
A previous study by Price et al. compared clinical outcomes and resource utilization in spinal surgeries between Surgiflo and Floseal during 2006–2012 using the data from PHD. In Price et al., outcomes were reported in surgeries stratified as ‘major’ surgeries (Floseal: n = 12,782; and Surgiflo: n = 1,531) or ‘severe’ surgeries (Floseal: n = 2837; and Surgiflo: n = 174) [8]. Price et al. found that after adjusting for key confounding factors, in ‘major’ spine surgeries, Surgiflo use was associated with higher risk of blood product transfusion in 2–4 days post-surgery (OR: 2.56; p < 0.001), longer surgery time (8.8 min; p < 0.0001) and increased product usage (1.9 ml; p < 0.001) compared with Floseal, but there were no significant differences in complications or resource use [8]. Price et al. reported similar rates of blood transfusions, complications and resource use in ‘severe’ spine surgeries [8]. However, the formulation of Surgiflo was updated in 2012 to increase paste viscosity and thus be more adherent to the bleeding surface, which was after Price et al.’s study was conducted. In our study, compared with Floseal, patients with Surgiflo had a similar risk of any transfusion (OR: 1.03; 95% CI: 0.98–1.08). Surgiflo was associated with a lower average cost of hospitalization, shorter LOS and shorter operating room time compared with Floseal. While Price et al., acknowledges disparity in the sample size (longer duration of Floseal on market compared with Surgiflo), our results are based on a significantly larger sample of patients that were matched on available baseline, hospital and surgery characteristics using propensity score matching. This robust method mitigates confounding due to baseline differences or bias based on the hemostatic matrix used, thus mimicking the properties of randomization to obtain more robust comparisons of the study outcomes between the two groups.
Our study demonstrates a $430 cost difference between Surgiflo and Floseal and reduced healthcare resource use in the Surgiflo group. ICU use has consistently been linked to higher costs during hospitalization. A 2011 survey of US general and surgical hospitals concluded that hospitals with ICU stay typically have 2.5-times higher costs than those without ICU use [28]. In our exploratory analysis, costs of patients admitted to the ICU were approximately two-times higher than those who were not admitted, a likely driver of the between group differences in total costs of the index hospitalization. Our results agree with the limited data available in literature describing cost and healthcare resource use impact of flowable hemostatic agents in spine surgery [20]. A study by David et al. compared cost in patients receiving Surgiflo and Floseal during spinal fusion or refusion surgeries conducted from 2010–2012 using data from PHD [20]. David et al. found that Surgiflo was associated with $65 reduction in cost compared with Floseal in multivariable model and an additional approximately $300 saving when accounting for hospital fixed effects, although no separate information was reported in costs related to ICU use [20].
Capturing blood transfusion reported in PHD is dependent on contributing hospitals and physician preferences. To investigate this, we conducted an exploratory analysis assessing inter-hospital variability in recording transfusion. The exploratory analysis showed that results related to blood transfusions are highly dependent on the way blood transfusions are identified in the PHD. Among 345 hospitals included in the study, 79.1% (n = 273) reported at least one transfusion with a variation in the way the transfusions were recorded in PHD (Transfusion were reported through only ICD procedure codes in 19.4% hospitals while 19.7% of hospitals had only a descriptive mention in hospital chargemaster data). Our sample was matched on hospital characteristics but was not adjusted for these interhospital variations related to capturing transfusions and could be explored in further studies. In addition, the indication for transfusion is not well-reported and could have been surgery related or other conditions such as fatigue. It would be worthwhile to explore if type of surgery would affect the transfusion preference among Surgiflo and Floseal groups.
Limitations
The current study has limitations inherent in retrospective database analyses. The study sample was obtained based on propensity score matching to balance the two comparison groups on confounding factors, but propensity score matching is only able to balance the confounders that are included in the study. Thus, the findings of the current study may still be subject to residual confounding.
The study also has limitations inherent to utilization of data in the PHD. The PHD is a hospital-based database that collects data from hospitals across the US. Coding practices and criteria may not be consistent across different hospitals. However, for variables that were not identifiable by standardized coding, we conducted text searches in hospital chargemaster codes supported by extensive literature search and sensitivity analyses to improve coding accuracy. However, the validity of using text searching in identifying outcomes such as transfusion and other events or procedures is to be verified in future studies using different data sources. Second, the PHD does not allow capturing rehospitalizations across multiple hospitals. Therefore, readmissions rates in the current study may be underestimated. Third, although there is no reason to believe that the type of hemostat received would be subject to channeling bias on the basis of preoperative medication use, the PHD does not contain data on the use of preoperative medications (e.g., anticoagulants or antiplatelets); therefore, we were unable to account for such medications in the propensity score matching. Fourth, there were unmeasured confounders such as surgeon skill, the skill of the supporting surgical team, protocols for blood loss prevention and transfusion, use of tranexamic acid and other factors that we were also unable to account for in the propensity score matching; therefore, as is the case with all nonrandomized, non interventional studies, the results must be interpreted as representing associations rather than causation. At last, PHD data may also be limited to hospitals that have continuously contributed to the database during the time frame assessed. Thus, the findings of the current study may not be generalizable to other hospitals.
Conclusion
In this retrospective study of patients undergoing spine surgery from a large nationwide hospital database, clinical outcomes were comparable between Surgiflo and Floseal and Surgiflo was associated with reduced cost and resource use compared with Floseal.
•
Bleeding during spine surgery is often controlled using topical hemostatic agents such as hemostats Floseal and Surgiflo®.
•
Surgiflo and Floseal both have proven efficacy to shorten surgery time, reduce transfusion need, better manage an anticoagulated patient, improve recovery time and reduced wound exposure.
•
Previous studies comparing Surgiflo and Floseal focused on a prior formulation of Surgiflo and small sample of patients.
•
In our study, the propensity matched study sample included 28,910 patients in each group.
•
In Surgiflo versus Floseal groups, clinical outcomes such as incidence of any documented bleeding event and any transfusion were similar.
•
Compared with patients who received Floseal, patients who received Surgiflo had lower average cost of hospitalization, shorter length of stay and shorter surgery duration.
•
This is the largest retrospective study presenting economic and clinical outcomes of patients receiving Surgiflo versus Floseal during spine surgery using the latest product formulations.
•
The study suggests that clinical outcomes are comparable between Surgiflo and Floseal groups and that Surgiflo is associated with lower hospitalization costs, slightly shorter length of stay and shorter operating room time among patients undergoing spine surgery.
Acknowledgments
A prior peer-reviewed presentation of this work occurred: Real-world economic and clinical outcomes associated with current hemostatic matrix use in spinal surgery. Poster presentation. Virtual ISPOR 2020 Conference, 18–20 May 2020.
Financial & competing interests disclosure
Research funding was provided by Ethicon Inc. W Danker is an employee of Ethicon, Inc., the study sponsor. SS Johnston is an employee of Johnson & Johnson. J Aggarwal, SS Kelkar, X Li Marston and G Poorman are employees of OPEN Health which received consultancy fees from Ethicon. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing/editorial support was provided by G Poorman from OPEN Health, MD, USA.
Ethical conduct of research
Data were deidentified in compliance to the US Health Insurance Portability and Accountability Act (HIPAA) to protect patient confidentiality. As such, there was no requirement for institutional review board approval.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA 303(13), 1259–1265 (2010).
2.
O'Lynnger TM, Zuckerman SL, Morone PJ, Dewan MC, Vasquez-Castellanos RA, Cheng JS. Trends for spine surgery for the elderly: implications for access to healthcare in North America. Neurosurgery 77(Suppl. 4), S136–S141 (2015).
3.
Carabini LM, Zeeni C, Moreland NC et al. Development and validation of a generalizable model for predicting major transfusion during spine fusion surgery. J. Neurosurg. Anesthesiol. 26(3), 205–215 (2014).
4.
Ramirez MG, Deutsch H, Khanna N, Cheatem D, Yang D, Kuntze E. Floseal only versus in combination in spine surgery: a comparative, retrospective hospital database evaluation of clinical and healthcare resource outcomes. Hosp. Pract. (1995) 46(4), 189–196 (2018).
5.
Stokes ME, Ye X, Shah M et al. Impact of bleeding-related complications and/or blood product transfusions on hospital costs in inpatient surgical patients. BMC Health Serv. Res. 11, 135 (2011).
6.
Boucher BA, Traub O. Achieving hemostasis in the surgical field. Pharmacotherapy 29(7 Pt 2), 2S–7S (2009).
7.
Levi M, Cromheecke ME, De Jonge E et al. Pharmacological strategies to decrease excessive blood loss in cardiac surgery: a meta-analysis of clinically relevant endpoints. Lancet (London, England) 354(9194), 1940–1947 (1999).
8.
Price JS, Tackett S, Patel V. Observational evaluation of outcomes and resource utilization from hemostatic matrices in spine surgery. J. Med. Econ. 18(10), 777–786 (2015).
•• Compared clinical outcomes and resource use between Floseal and a previous formulation of Surgiflo.
9.
Spotnitz WD. Active and mechanical hemostatic agents. Surgery 142(Suppl. 4), S34–S38 (2007).
10.
Baxter Healthcare Corporation. FLOSEAL Hemostatic Matrix [package insert]. 2–3 (2014).
11.
Ethicon Incorporated. SURGIFLO® Hemostatic Matrix with EVITHROM® Thrombin, Topical (Human) [package insert]. 2–4 (2018).
12.
Renkens KL Jr, Payner TD, Leipzig TJ et al. A multicenter, prospective, randomized trial evaluating a new hemostatic agent for spinal surgery. Spine 26(15), 1645–1650 (2001).
13.
Oz MC, Rondinone JF, Shargill NS. FloSeal Matrix: new generation topical hemostatic sealant. J. Cardiac. Surg. 18(6), 486–493 (2003).
14.
Lewis KM, Atlee HD, Mannone AJ et al. Comparison of two gelatin and thrombin combination hemostats in a porcine liver abrasion model. J. Invest. Surg. 26(3), 141–148 (2013).
15.
Oz MC, Cosgrove DM, Badduke BR et al. Controlled clinical trial of a novel hemostatic agent in cardiac surgery. Ann. Thoracic Surg. 69(5), 1376–1382 (2000).
16.
Woodworth BA, Chandra RK, Lebenger JD, Ilie B, Schlosser RJ. A gelatin-thrombin matrix for hemostasis after endoscopic sinus surgery. Am. J. Otolaryngol. 30(1), 49–53 (2009).
17.
Vyas KS, Saha SP. Comparison of hemostatic agents used in vascular surgery. Expert Opin. Biol. Ther. 13(12), 1663–1672 (2013).
18.
Ma LDL, Yang Y, Liu H. Comparison the efficacy of hemorrhage control of Surgiflo Haemostatic Matrix and absorbable gelatin sponge in posterior lumbar surgery: a randomized controlled study. Medicine (Baltimore) 97(49), e13511 (2018).
19.
Landi A, Gregori F, Marotta N, Delfini R. Efficacy Security, and manageability of gelified hemostatic matrix in bleeding control during thoracic and lumbar spine surgery: Floseal versus Surgiflo. J. Neurol. Surg. A. Cent. Eur. Neurosurg. 77(2), 139–143 (2016).
•• Compared utility of Surgiflo versus Floseal.
20.
David G, Lim S, Gunnarsson C, Kocharian R, Roy S. Similar patient outcomes yet different hospital costs between flowable hemostatic agents. J. Med. Econ. 18(9), 735–745 (2015).
•• Studied clinical and economic outcomes of Surgiflo versus Floseal.
21.
Gazzeri R, Galarza M, Alfier A. Safety biocompatibility of gelatin hemostatic matrix (Floseal and Surgiflo) in neurosurgical procedures. Surg. Technol. Int. 22, 49–54 (2012).
•• Compared clinical outcomes of Surgiflo versus Floseal.
22.
Chmielewski J. Summary review memo: SURGIFLO hemostatic matrix kit with thrombin. (2011). https://www.accessdata.fda.gov/cdrh_docs/pdf/P990004S019M.pdf
23.
Ethicon Incorporated. SURGIFLO® and Go. 2–4 (2021)
24.
Premier Applied Sciences®. P.I. Premier Healthcare Database White Paper: data that informs and perform. https://learn.premierinc.com/white-papers/premier-healthcaredatabase-whitepaper
25.
Quan H, Li B, Couris CM et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
26.
Ballinger GA. Using generalized estimating equations for longitudinal data analysis. Organizational Res. Meth. 7(2), 127–150 (2004).
27.
Manning WG, Mullahy J. Estimating log models: to transform or not to transform? J. Health Econ. 20(4), 461–494 (2001).
28.
Barrett ML, Smith MW, Elixhauser A, Honigman LS, Pines JM. Utilization of intensive care services, 2011: statistical brief #185. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality, MD, USA (2006).
Information & Authors
Information
Published In
Pages: 1231 - 1240
PubMed: 36306241
Copyright
© 2022 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 13 September 2021
Accepted: 20 September 2022
Published online: 28 October 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world economic and clinical outcomes associated with current hemostatic matrix use in spinal surgery. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0218
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Abdulrahim Saleh Alrasheed, Ameena Manzoor, Abdulaziz S. Almuhaisen, Óscar L. Alves, Saleh S. Baeesa, Safety and Efficacy of Flowable Gelatin Hemostatic Matrix Sealants in Spine Surgery: A Systematic Review and Meta-Analysis, Spine Open, 10.1097/bn9.0000000000000093, 2, 3, (2026).
- Mokshal Porwal, Pishya Muangman, Alexander Yu, Post-market surveillance of gelatin-thrombin hemostats in neurosurgery: a 10-year MAUDE Analysis, Neurological Research, 10.1080/01616412.2026.2686943, (1-11), (2026).
- Sergey V. Kolesov, Aleksandr N. Vasilev, Anton V. Shakhin, Sergei V. Rassovskiy, Arkadiy I. Kazmin, Vladimir V. Shvets, Vladimir S. Pereverzev, Sergei A. Baranov, Tagir V. Abdulin, Samir B. Bagirov, Nataliia S. Morozova, Elizaveta E. Bibikova, The use of topical hemostatic agents in spinal surgery, N.N. Priorov Journal of Traumatology and Orthopedics, 10.17816/vto322763, 32, 1, (293-304), (2025).
- Qianli Gao, Chi Zhang, Rong Xu, Yifeng Shi, Yang Luo, Bin Yu, Dongdong Xia, Opportunities and challenges of adhesive hemostatic hydrogels in spinal surgery, BME Horizon, 10.70401/bmeh.2025.0007, (2025).
- Ashish D. Chakraborty, Yixuan Tong, Charla Fischer, A Comparative Review of Two Major Topical Hemostasis Agents in Spine Surgery, Operative Techniques in Orthopaedics, 10.1016/j.oto.2024.101098, 34, 1, (101098), (2024).
- Ivan B. Ye, Alexandra E. Thomson, Ryan A. Smith, Tyler J. Pease, Navid Chowdhury, Jack Donahue, Vincent Miseo, Julio J. Jauregui, Daniel L. Cavanaugh, Eugene Y. Koh, Steven C. Ludwig, FLOSEAL Versus SURGIFLO in Lumbar Surgery: Similar Outcomes, Different Costs in a Matched Cohort Analysis, World Neurosurgery, 10.1016/j.wneu.2023.06.070, 177, (e425-e432), (2023).