The cost–effectiveness of oral semaglutide versus empagliflozin in Type 2 diabetes in Denmark
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate the cost–effectiveness of oral semaglutide+metformin versus empagliflozin+metformin in people with Type 2 diabetes uncontrolled on msetformin alone. Materials and methods: The IQVIA Core Diabetes Model was populated with efficacy data from a head-to-head study between oral semaglutide+metformin and empagliflozin+metformin. Danish costs and quality-of-life data were sourced from literature. Price per day was Danish Krone (DKK) 25.53 for oral semaglutide and DKK11.40 for empagliflozin. Discounting was fixed at 4%. Scenario and sensitivity analyses were performed. Results: Over a lifetime, Core Diabetes Model projected 8.78 and 8.75 quality-adjusted life-years and a total cost of DKK 447,633 and DKK 387,786, thereby generating an incremental cost–effectiveness ratio of DKK 1,930,548 for oral semaglutide+metformin versus empagliflozin+metformin. Scenario and sensitivity analyses showed the robustness of the outcomes. Duration of treatment with oral semaglutide is the key driver of the analyses. Conclusion: Oral semaglutide+metformin seems not cost effective versus empagliflozin+metformin in patients uncontrolled on metformin in Denmark.
More than 240,000 Danes live with Type 2 diabetes (T2D) [1], which is expected to increase to 430,000 by 2030 [2]. People with diabetes have a 50–60% excess mortality compared with the background population, primarily because of early cardiovascular disease (CVD) [3]. The cost of management of diabetes is substantial, and the majority of costs are incurred among persons with major complications, illustrating the importance of secondary preventive efforts [4].
The aim of pharmacological treatment for T2D, beyond freedom from symptoms, is to prevent micro- and macrovascular complications, including CVD and heart failure [5]. In line with international guidelines [6,7], Danish clinical guidelines for the treatment of T2D recommend lifestyle changes and, where appropriate, metformin, followed by either oral therapy (DPP-4 inhibitors, SGLT2 inhibitors, SU, pioglitazone) or subcutaneous injectable medications (GLP-1 receptor agonists, insulin) [5].
The clinical guidelines are based on large randomized clinical trials that have been carried out since the US FDA recommended in 2008 that any new T2D treatment must demonstrate that it is not associated with an unacceptable increase in cardiovascular (CV) risk [8]. Beyond demonstration of neutrality with respect to CV risk for a broad range of compounds [9,10], a number of large randomized clinical trials have documented positive benefits on cardiovascular risk for individual SGLT2 inhibitors and injectable GLP-1 receptor agonists. In people with T2D and CVD, there is evidence that treatment with SGLT2 inhibitor and injectable GLP-1 receptor agonist reduce cardiovascular risk and for two of these, GLP-1 receptor agonist liraglutide and SGLT2 inhibitor empagliflozin, also mortality [5].
An oral formulation of GLP-1 receptor agonist (semaglutide) has recently become available in the Danish market. The cardiovascular risk profile of this GLP-1 receptor agonist tablet was investigated in a cardiovascular outcomes trial. In this trial involving patients with T2D and CVD or high cardiovascular risk, the cardiovascular risk profile of oral semaglutide was non inferior to that of placebo [11]. One other cardiovascular outcomes trial for oral semaglutide is ongoing and is expected to conclude in 2024 [12].
This study assessed the long term cost–effectiveness, in a Danish context, of the GLP-1 receptor agonist oral semaglutide tablet added to metformin in comparison to the most used SGLT2 inhibitor empagliflozin added to metformin in people with T2D uncontrolled on metformin alone. The study was based on the available head-to-head Peptide Innovation for Early Diabetes Treatment (PIONEER) 2 study [13].
Materials & methods
Since there is no head-to-head long-term (or short term) clinical trial evaluating hard end points of the two interventions, the IQVIA Core Diabetes Model (CDM) version 9.5 (using the UKPDS 82 cardiovascular risk equations) was used to simulate the clinical and economic results.
The CDM is a non product-specific microsimulation tool that models the effect of glucose monitoring, diabetes therapies and treatment strategies on disease progression and outcomes. Disease progression is based on a series of interdependent Markov submodels that simulate progression of disease-related complications (angina, myocardial infarction, congestive heart failure, stroke, peripheral vascular disease, diabetic retinopathy, macular edema, cataract, hypoglycemia, ketoacidosis, nephropathy and end stage renal disease, neuropathy, foot ulcer, amputation) and non specific mortality. Each submodel uses time-, state- and diabetes type-dependent probabilities derived from published sources. The use of tracker variables bypasses the memoryless properties of standard Markov models. The model facilitates interconnectivity and interaction between the modeled complications, representing the complex and varied sequelae of the disease. The structure of the CDM and the most recent validation are described in detail elsewhere [14,15]. More information on CDM version 9.5 is available online (www.core-diabetes.com/).
The CDM estimated the cost and quality-adjusted life-years (QALYs) with respect to oral semaglutide plus metformin versus empagliflozin plus metformin in persons with T2D uncontrolled on metformin alone. The primary outcome of the model was the incremental cost–effectiveness ratio (ICER). A Danish health sector perspective was used for a long-term (50 years) time horizon for the base case analysis. Future costs, LYs and QALYs were discounted with a rate of 4% as recommended by the Danish guidelines for health economic evaluation of pharmaceuticals [16]. All prices are stated in Danish Krone (DKK) price-level 2020 excluding value-added tax (ex. VAT). Main results are also presented in EUROs (DKK 744 = €100).
Clinical data
This economic evaluation was an adaptation of a UK study on cost–effectiveness of empagliflozin versus oral semaglutide [17], and is based on the results of the 52-week PIONEER 2 trial which enrolled T2D people with glycated hemoglobin (HbA1c) values between 7.0 and 10.5% (53–91 mm/mol) and treated with metformin [13] (Supplementary Table 1). The mean age was 58 years, the mean duration of diabetes was 7.4 years and the mean HbA1c was 8.1%. In this 52-week trial, the GLP-1 receptor agonist oral semaglutide was compared with the SGLT2 inhibitor empagliflozin, in addition to metformin. The primary end point was change in HbA1c at 26 weeks. No CV or renal end points were assessed.
The base case compared the cost–effectiveness of first-line therapy oral semaglutide plus metformin versus empagliflozin plus metformin in people with T2D uncontrolled on metformin alone. After they reach the HbA1c threshold of 7.5%, patients switch to second-line escalation therapy or require treatment intensification which means addition of long-acting insulin on top of oral semaglutide or empagliflozin and metformin in order to regain the glycemic control [17]. This level of HbA1c is in accordance with NICE guidelines [18] and clinical guidelines from the Danish Society of Endocrinology [5].
Treatment effects from the PIONEER 2 trial are shown in Table 1. The treatment policy estimand (intention-to-treat approach) was used for HbA1c and BMI change in the base case analysis, and the trial policy estimand (per protocol approach) was used in a scenario analysis. However, change from baseline in blood pressure and lipid parameters were based on the trial product estimand as these data from the treatment policy estimands were not published [19] (Supplementary Tables 2–4).
| Variable | Empagliflozin | SE | Oral semaglutide | SE | Unit | Ref. |
|---|---|---|---|---|---|---|
| Change in baseline HbA1c | -0.90 | 0.026 | -1.30 | 0.026 | % points | [13] |
| SBP change from baseline | -4.34 | 0.63 | -4.85 | 0.65 | mmHg | [19] |
| DBP change from baseline | -2.67 | 0.44 | -2.27 | 0.45 | mmHg | [19] |
| T Chol change from baseline | 4.74 | 1.57 | -5.08 | 1.62 | mg/dl | [19] |
| HDL Chol change from baseline | 3.11 | 0.34 | 0.73 | 0.35 | mg/dl | [19] |
| BMI Change from baseline | -1.294 | 0.028 | -1.357 | 0.028 | kg/m2 | Recalculated based on [13] |
In Rodbard et al. [13], starting bodyweight, BMI and absolute decrease in bodyweight is reported. Based on this the decrease in BMI per arm was calculated.
DBP: Diastolic blood pressure; HbA1c: Glycated hemoglobin A1c; HDL chol: High-density lipoprotein cholesterol; SBP: Systolic blood pressure; SE: Standard error; T Chol: Total cholesterol.
Evolution of physiological parameters over time was predicted by applying progression equations available in the CDM. For HbA1c this is based on UKPDS 68.
Costs
Unit cost for treatment, including oral semaglutide and empagliflozin were obtained from Medicinpriser.dk (Lægemiddelstyrelsen [Danish medicines agency], Copenhagen, Denmark) in July 2020. For oral semaglutide, it equaled the introduction cost on 27 July 2020 and for empagliflozin, it equaled the average of the lowest unit cost during six tender periods 18 May–27 July 2020 in accordance with guidelines for price comparisons by the Danish Medicines Agency [20]. Pharmacy purchase price excluding VAT and pharmacy fee (In Danish: Apotekets Indkøbspriser) were DKK 25.53 per day and DKK9,326.05 per year for oral semaglutide and DKK 11.40 per day and DKK 4164.70 per year for empagliflozin, respectively.
The costs of treating diabetes-related complications (in the year of the event) and the annual follow-up costs (applied in each year of the simulation subsequent to the first event) were identified through literature reviews and adjusted for inflation using the consumer price index published by Statistics Denmark. The identified costs of CV complications have been obtained from a report prepared by the Danish national institute VIVE [21]. They used the unique Danish registries based on personal identification numbers to identify the average real world cost of patients with a specific CV event compared with a matched control group with no such event.
More information on the applied unit costs for clinical management and complications are available in Supplementary Tables 5–9.
Utilities
To estimate the expected QALY gain of each treatment pathway, the CDM uses a comprehensive set of utility weightings for each model state [22]. Utilities are assessed on a scale from 0 to 1, where 0 represents death (no quality-of-life [QoL]) and 1 indicates a healthy person without complications. Dis utilities due to illness are values in the range -1 to 0, and therefore causes the QoL utility to either decrease or remain constant. Following an event, patients change state and the new state is associated with different state utilities. QoL values are then estimated for every hypothetical patient in each year of the simulation and used to estimate the average quality-adjusted life expectancy. For all simulations, the minimum approach method was applied to calculate the quality-adjusted life utility. In Supplementary Table 10, the values used for this analysis and references are available.
Scenario analyses
A probabilistic sensitivity analysis was conducted with Monte Carlo simulations together with a non parametric bootstrapping approach to capture the impact on the ICER of all parameter uncertainty in the model.
Furthermore, a number of deterministic one-way analyses and scenario-analyses were conducted. This includes evaluating the effects of treatment at a shorter time horizon (i.e., 5 years) and applying treatment intensification at an HbA1c threshold of 8%.
Another scenario analysis with three lines of therapy was made with the hypothetical assumption that after reaching HbA1c level of 7.5% again after second-line escalation therapy (addition of long-acting insulin), as a third-line therapy, patients would discontinue oral semaglutide or empagliflozin and metformin and go to higher doses of long-acting insulin alone.
Finally, a sensitivity analysis assuming an improved effect of oral semaglutide was made. The PIONEER 2 study reported two sets of analyses: the ‘treatment policy estimand’ (intention-to-treat principle) and the ‘trial product estimand’ (a per protocol analyses). We chose the intention-to-treat approach as the base case due to the fact that it is the gold standard study design and represents data closer to real life by not excluding discontinuation of the drug nor rescue mediation, but included the trial product estimand (per protocol) in a sensitivity analysis.
Results
The long-term projection of surrogate end points showed that in the base case analysis over a lifetime horizon (50 years), CDM projected 13.21 and 13.21 life-years, 8.78 and 8.75 QALY and DKK447, 633 and DKK387, 786 total costs, respectively, generating an ICER of DKK 1,930,548 for oral semaglutide plus metformin versus empagliflozin plus metformin (Table 2). Patients switched to next-line therapy after 3 years in the oral semaglutide arm and after 2 years in the empagliflozin arm.
| Lifetime horizon | 5-year horizon | |||
|---|---|---|---|---|
| Oral semaglutide | Empagliflozin | Oral semaglutide | Empagliflozin | |
| LY | 13.21 | 13.21 | 4.31 | 4.31 |
| QALY | 8.78 | 8.75 | 3.00 | 2.98 |
| Total cost | 447,633 | 387,786 | 99,767 | 86,282 |
| ICER (DKK/QALY) | 1,930,548 | 612,931 | ||
DKK: Danish Krone; ICER: Incremental cost–effectiveness ratio; LY: Life-year; QALY: Quality-adjusted life-year.
Assuming a willingness-to-pay threshold (WTP) of DKK 357,100 per QALY gained (one-time Gross Domestic Product per capita, 2020), ICER for oral semaglutide plus metformin was above the WTP threshold.
The results of the probabilistic sensitivity analysis illustrated that in 16% of the simulations, oral semaglutide plus metformin was a cost-effective therapy at this WTP threshold (Figures 1 & 2).

Figure 1. Incremental cost–effectiveness ratio scatter plot for oral semaglutide versus empagliflozin.
DKK: Danish Krone; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life-year; WTP: Willingness-to-pay.

Figure 2. Cost–effectiveness acceptability curve of oral semaglutide versus empagliflozin.
DKK: Danish Krone.
Over a 5-year time horizon an ICER of DKK612,931 per QALY (€82,383 per QALY) was generated, also above the WTP threshold and as such not cost effective (Table 2).
In general, the performed scenario-analyses confirmed that findings were robust (Supplementary Table 11). However, in the hypothetical three-line scenario analysis where oral semaglutide and empagliflozin were discontinued in all patients after they reached an HbA1c level of 7.5% again, oral semaglutide reached cost–effectiveness.
The cost–effectiveness result was driven by a major difference in treatment costs (Supplementary Table 12), reflecting the large unit cost difference of oral semaglutide versus empagliflozin (Figure 3).
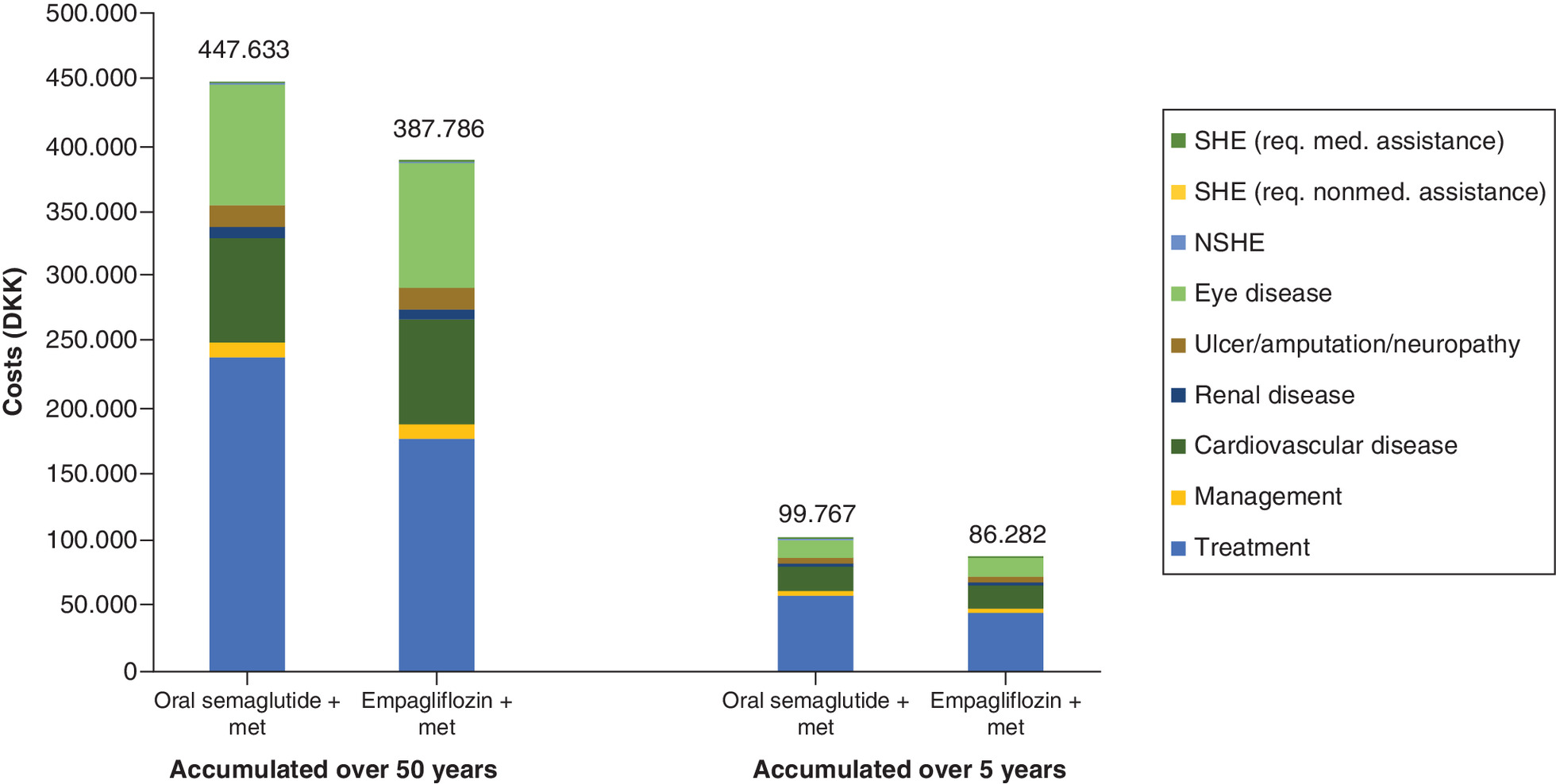
Figure 3. Total costs per individual with Type 2 diabetes uncontrolled on metformin.
DKK: Danish Krone; Met: Metformin; NSHE: No severe hypoglycemic event; SHE: Severe hypoglycemic event; T2D: Type 2 diabetes.
Discussion
Overall, this study finds that oral semaglutide is not a cost-effective treatment option compared with empagliflozin in the management of T2D patients uncontrolled on metformin alone, both in a lifelong (50 years) and 5-year time horizon. Results showed only a marginal QALY gain with oral semaglutide, but considerable cost savings associated with the use of empagliflozin.
Three cost–effectiveness analyses of oral semaglutide versus empagliflozin in patients uncontrolled on metformin have been published recently and with conflicting results.
In an analysis from the independent research done by the Institute for Clinical and Economic Review, cost–effectiveness in the US setting was assessed based on network meta-analysis of available clinical trials including PIONEER 2 and cardiovascular outcomes trials. Institute for Clinical and Economic Review concluded that oral semaglutide was not cost effective versus empagliflozin in the US setting based on estimated net prices [23].
In the UK analysis based on PIONEER 2, it was concluded that oral semaglutide was cost effective versus empagliflozin on top of metformin in a UK setting [19]. This 50-year analysis included the cost of oral semaglutide and empagliflozin for a period of only 3 and 2 years respectively, followed by discontinuation of the two medications under study and initiation of insulin for 47 and 48 years respectively. It also applies the more controversial ‘trial product estimand’ (per protocol) approach rather than the intention-to-treat principle. Under these circumstances the authors conclude that oral semaglutide is cost effective [19].
In the UK analysis (which was adapted to a Danish setting in our study), comparing empagliflozin with oral semaglutide based on intention-to-treat results from PIONEER 2 and keeping the medications under study throughout the 50-year life cycle. Empagliflozin was cost effective versus oral semaglutide, and dominant (better health outcomes with lower costs) when effects on heart failure from a real world study in low-risk patients was taken into account [17]. In a three-line sensitivity analysis, this study also evaluated the effect of discontinuing oral semaglutide or empagliflozin and metformin and going to higher doses of long-acting insulin alone as third-line therapy when patients reached the prespecified HbA1c level of 7.5% again (similar to our three-line sensitivity analysis). This happened after 6 and 5 years respectively and empagliflozin was also cost effective compared with oral semaglutide in this three-line scenario.
It is important to acknowledge that this study has some limitations. First of all, the long-term cost–effectiveness result was based on a 52-week open label head-to-head comparison of surrogate end points for oral semaglutide plus metformin compared with empagliflozin plus metformin. No clinical evidence exists to assess the relative long term benefits of the two interventions, in particular, no evidence exists to compare their relative effects on cardiovascular and renal outcomes. In the PIONEER 2 study, oral semaglutide had a larger glucose reducing effect compared with empagliflozin. The study; however, had weaknesses in terms of a relatively large drop out in the semaglutide arm compared with the empagliflozin arm and the study was unblinded [13]. Since the PIONEER 2 trial is currently the only head-to-head evidence available, it is used as the basis for this cost–effectiveness analysis. Also, in the PIONEER 2 trial two types of analyses were performed. One based on the treatment policy estimand, comparable to intention to treat and as such preferred in health economic analyses, and one called trial product estimand, which is a per protocol analyses. Whereas all the necessary inputs for the trial product estimand were provided in the cost–effectiveness analysis published by Bain et al. [19], unfortunately not all the inputs on the treatment policy estimand were reported in Rodbard et al. [13] what could be considered a limitation of this analyses. Nevertheless, the most important was that HbA1c and BMI change to baseline were reported and as such have been used in the base case analysis. Analyses were run using both estimands anyhow. In our study, the estimated ICER using the trial product estimand (per protocol approach) from the PIONEER 2 study reduced from DKK 1,930,548 to DKK 1,124,537 (Supplementary Table 11). This is still considerably higher than the assumed WTP threshold of DKK357,100; hence, oral semaglutide could not be considered cost effective from a per protocol approach either in our study.
In the model, it was assumed that patients switched treatment when they reached a HbA1c level of 7.5% and as such discontinuation due to for example adverse events is not taken into account. It should be noted that the use of rescue medication and other diabetes medications was not significantly different between the two arms in the PIONEER 2 study. Discontinuation in the oral semaglutide arm was; however, significantly higher than in the empagliflozin arm (10.7 vs 4.4%) [13]; and therefore, adoption of a per protocol analysis (‘trial product estimand’) will run the risk of over-estimating the effects of oral semaglutide. On the other hand, drug cost may be overestimated as not all patients have the full length of therapy in both arms, but more in the oral semaglutide arm and in both estimands analyses. Note, however, that the annual cost of oral semaglutide is more than DKK5,000 higher than the cost of empagliflozin (DKK9,326 vs DKK4,165). Even reducing these costs with 10.7 and 4.4% respectively, it will not be sufficient to bridge the cost difference between the two arms.
The HbA1c progression equation applied was based on the UKPDS study, and as such is not specific for the progression under therapy with oral semaglutide and empagliflozin. Long-term studies that are not allowing rescue therapy options are not available so the real natural progression under those drugs is not known and whether one risk equation is better than the other is also unknown. The UKPDS progression equation is very often used in health economic models in Type 2 diabetes and was also applied by Bain et al. [19] in their analysis. If the progression goes slower, it will take longer to reach the 7.5% and as such switch is made later. This could affect results, mainly in the 3L approach as therapy with oral semaglutide or empagliflozin is stopped in third line but this third line will be reached later, which will result in higher drug costs, and maybe some unknown differences in outcomes. A scenario analysis with a higher switch threshold revealed that patients go to next line 2 years later compared with the base case, with a very similar ICER.
Different from Bain et al. [19] we assumed that after treatment escalation empagliflozin and oral semaglutide were continued, not only on a cost side, but also on effectiveness side. We did this to be in line with the clinical guidelines stating that both drug classes are best continued even if escalation is needed [5–7]. Nevertheless, we also included a 3L scenario where oral semaglutide and empagliflozin were discontinued when again a threshold of 7.5% in HbA1c was reached. This happened after 6 and 5 years, respectively. In this scenario oral semaglutide reached cost–effectiveness (Supplementary Table 11) pointing out that the duration of therapy with oral semaglutide is the key driver of the analyses.
The assumption; however, that patients as third-line therapy would discontinue oral semaglutide or empagliflozin treatment and switch to higher doses of long-acting insulin (instead of adding higher doses of long-acting insulin) would not be in line with current clinical practice in Denmark. Neither would it be in line with recommendations from clinical guidelines which do not recommend discontinuation of previously initiated medications [5–7]. Also, clinical guidelines recommend continuation of treatment with SGLT2 inhibitor or GLP-1 receptor agonist regardless of HbA1c level in persons who have developed CVD, heart failure or renal disease over the cause of this 50-year period [6,7].
Recent guidance from the Danish Health Authorities recommends SGLT2 inhibitors over GLP-1 receptor agonists based on clinical efficacy, safety and price, in patients with T2D in general and in subgroups of patients with either atherosclerotic CVD, heart failure or diabetic nephropathy and/or for whom weight loss is crucial [24]. Effectively, this covers the vast majority of persons with T2D.
In this light, real-life use and costs of the SGLT2 inhibitors and GLP-1 receptor agonists could be an important future research topic.
In Denmark, 75% of 240,000 persons with T2D [1] are estimated to have no CVD [25], equaling 180,000 individuals. Most patients with T2D will progress to second-line treatment. In year 2015, 6343 out of 180,742 persons in Denmark with T2D treated with metformin (3.5%) initiated second-line treatment such as DPP-4 inhibitor, SGLT2 inhibitor, GLP-1 receptor agonist, SU, insulin or other treatment [26]. The potential budget impact of second-line choice among patients with T2D uncontrolled on metformin is; therefore, significant and detailed budget impact analysis incorporating all dynamics of the market is warranted.
Conclusion
This study suggests that oral semaglutide plus metformin is not cost effective in Denmark at current price levels compared with empagliflozin plus metformin in people with T2D uncontrolled on metformin. Key drivers of the results are the drug acquisition cost and the duration of therapy. The better impact of oral semaglutide on HbA1c leads to a modestly increased life expectancy and QALY.
Future perspective
Direct clinical long-term comparisons between SGLT2 inhibitors and GLP-1 receptor agonists could be an important future research topic and real-life data could shed more light on the above predictions.
•
The cost of management of diabetes is significant, and the majority of costs are incurred among persons with major complications.
•
In line with international guidelines, Danish clinical guidelines recommend metformin followed by either oral therapy DPP-4 inhibitors, SGLT2 inhibitors or subcutaneous injectable medications and GLP-1 receptor agonists for the treatment of Type 2 diabetes (T2D).
•
As treatment with GLP-1 or SGLT2 receptor agonists, in addition to metformin, are to be continued long-term, it is important to understand the cost–effectiveness of these therapies for T2D treatment.
•
An analysis of the long-term cost–effectiveness of treatment oral semaglutide added to metformin in comparison to the most used SGLT2 inhibitor empagliflozin added to metformin in people with T2D uncontrolled on metformin alone was conducted in Danish setting.
•
IQVIA Core Diabetes Model version 9.5 was used to simulate the clinical and economic results based on the results of the 52-week PIONEER 2 clinical trial, literature findings, certain assumptions and based on some recalculations.
•
Oral semaglutide plus metformin seems not to be cost effective versus compared with empagliflozin plus metformin for the treatment of patients with T2D not controlled with metformin alone in the Danish setting.
•
Results of the cost–effectiveness analyses were driven mainly by treatment costs, reflecting the cost difference between oral semaglutide and empagliflozin.
Author contributions
LH Ehlers, M Lamotte, MC Ramos, S Sandgaard, P Holmgaard, EC Frary and N Ejskjaer conceptualized the study. LH Ehlers, M Lamotte, MC Ramos, S Sandgaard and P Holmgaard performed calculations. LH Ehlers wrote the first draft. M Lamotte, MC Ramos, S Sandgaard, P Holmgaard, EC Frary and N Ejskjaer provided inputs too and reviewed first draft.
Financial & competing interests disclosure
LH Ehlers is employed by Aalborg University, Aalborg, Denmark. His contributions to the study were supported by an honorarium funded by Boehringer Ingelheim. M Lamotte and MC Ramos are employees of IQVIA, which received consulting fees from Boehringer Ingelheim for adapting the Core Diabetes Model and running the analyses. S Sandgaard, P Holmgaard and EC Frary are employees of Boehringer Ingelheim Denmark A/S. N Ejskjaer received honorarium from Boehringer Ingelheim for his contributions to this study. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors would like to thank C Kumar and A Singhal from IQVIA, Real World Solutions, India for providing writing and editing assistance, funded by Boehringer Ingelheim.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary material.docx)
- Download
- 139.54 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Sundhedsdatastyrelsen. Udvalgte kroniske sygdomme og svære psykiske lidelser (Selected chronic diseases and severe mental disorders (2021). www.esundhed.dk/Registre/Register-for-udvalgte-kroniske-sygdomme
2.
Statens Institut for Folkesundhed. Sygdomsudviklingen i Danmark fremskrevet til 2030 (2017). www.sdu.dk/sif/-/media/images/sif/sidste_chance/sif/udgivelser/2017/sygdomsudviklingen_i_danmark_fremskrevet_til_2030.pdf
3.
Danish Society of Cardiology and Danish Society of Endocrinology. Diabetes and cardiovascular disease (2021). https://nbv.cardio.dk/diabetes
• These guidelines are the basis of the choice of next-line therapies.
4.
Sortsø C, Green A, Jensen PB, Emneus M. Societal costs of diabetes mellitus in Denmark. Diabet. Med. 33(7), 877–885 (2016).
5.
Dansk Endokrinologisk Selskab. NBV: behandling og kontrol af Type 2 Diabetes. www.endocrinology.dk/index.php/nbvhovedmenu/1-diabetes-mellitus/nbv-endokrinologi-behandling-og-kontrol-af-type-2-diabetes-t2d-diabetes-arskontrol-nyopdaget-diabetes-2-peroral-behandling-insulin-behandling-kolesterolbehandling-blodtryksbehandling-glp1-og-dpp4
• These guidelines are the basis of the choice of next-line therapy.
6.
American Diabetes Association. Standards of medical care in diabetes 2018. Diabetes Care 41(Suppl. 1), S1–S159 (2018).
7.
Buse JB, Wexler DJ, Tsapas A et al. 2019 update to: management of hyperglycaemia in Type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 63(2), 221–228 (2020).
• These guidelines are the basis of the choice of next-line therapy.
8.
Food and Drug Administration. Guidance for industry–evaluating cardiovascular risk in new antidiabetic therapies to treat Type 2 diabetes. US Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research, DC, USA (2008). www.fda.gov/media/71297/download
9.
Schnell O, Rydén L, Standl E, Ceriello A. Current perspectives on cardiovascular outcome trials in diabetes. Cardiovasc. Diabetol. 15(1), 139 (2016).
10.
Schnell O, Rydén L, Standl E, Ceriello A. Updates on cardiovascular outcome trials in diabetes. Cardiovasc. Diabetol. 16(1), 128 (2017).
11.
Husain M, Birkenfeld AL, Donsmark M et al. Oral semaglutide and cardiovascular outcomes in patients with Type 2 diabetes. N. Engl. J. Med. 381(9), 841–851 (2019).
12.
Clinicaltrials.Gov. Semaglutide cardiovascular outcomes trial in patients with Type 2 diabetes (2020). https://clinicaltrials.gov/ct2/show/NCT03914326?term=oral+semaglutide&type=Intr&fund=2&draw=5&rank=35
13.
Rodbard HW, Rosenstock J, Canani LH et al. Oral semaglutide versus empagliflozin in patients with Type 2 diabetes uncontrolled on metformin: the PIONEER 2 Trial. Diabetes Care 42(12), 2272–2281 (2019).
•• Basis of efficacy of the drugs under study.
14.
Mcewan P, Foos V, Palmer JL, Lamotte M, Lloyd A, Grant D. Validation of the IMS CORE diabetes model. Value Health 17(6), 714–724 (2014).
15.
Palmer AJ, Roze S, Valentine WJ et al. The CORE Diabetes Model: projecting long-term clinical outcomes, costs and cost-effectiveness of interventions in diabetes mellitus (Types 1 and 2) to support clinical and reimbursement decision-making. Curr. Med. Res. Opin. 20(Suppl. 1), S5–S26 (2004).
16.
Lægemiddelstyrelsen 2018a. Vejledning om udarbejdelse af sundhedsøkonomiske analyser af lægemidler. VEJ nr 9153 af 09/03/2018 (Danish Medicines Agency. Guidelines for the development of health-economic evaluation of medicines) (2018). www.retsinformation.dk/Forms/R0710.aspx?id=199976
17.
Ramos M, Cummings MH, Ustyugova A, Raza SI, De Silva SU, Lamotte M. Long-term cost-effectiveness analyses of empagliflozin versus oral semaglutide, in addition to metformin, for the treatment of Type 2 diabetes in the UK. Diabetes Ther. 11(9), 2041–2055 (2020).
18.
National Institute for Health and Care Excellence (Nice). Type 2 diabetes in adults: management (NICE guideline [NG28]) (2015). www.nice.org.uk/guidance/ng28
19.
Bain SC, Hansen BB, Malkin SJP et al. Oral semaglutide versus empagliflozin, sitagliptin and liraglutide in the UK: long-term cost–effectiveness analyses based on the PIONEER Clinical Trial Programme. Diabetes Ther. 11(1), 259–277 (2020).
•• Provides additional efficacy information.
20.
Lægemiddelstyrelsen 2018b. Vejledning om periodisk revurdering af lægemidlers tilskudsstatus (2018). www.retsinformation.dk/eli/retsinfo/2018/9154
21.
Vive Rapport. En helhjertet indsat - En artikelbaseret klinisk, patientnær og sundhedsøkonomisk kortlægning af hjerte-kar-området, 2018 (VIVE report: a whole-hearted effort – a publication based clinical, patient centric and health economic mapping of the cardiovascular area, 2018) (2018). https://hjerteforeningen.dk/wp-content/uploads/sites/17/2018/02/11162-en-helhjertet-indsats-web.pdf
22.
Beaudet A, Clegg J, Thuresson PO, Lloyd A, Mcewan P. Review of utility values for economic modeling in Type 2 diabetes. Value Health 17(4), 462–470 (2014).
23.
Rind DM, Fazioli K, Borrelli E et al. In: Oral Semaglutide for Type 2 Diabetes: Effectiveness andValue. 4.4 Summary and Comment 7.4 Access and Affordability Alert. Institute for Clinical and Economic Review, MA, USA (2019).
24.
Sundhedsstyrelsen. Farmakologisk glukosesænkende behandling af Type 2-diabetes i almen praksis, Rationel Farmakoterapi nr 10, september 2020 (2020). www.sst.dk/da/Udgivelser/2020/Rationel-Farmakoterapi-10-2020
25.
Rungby J, Schou M, Warrer P, Ytte L, Andersen GS. Prevalence of cardiovascular disease and evaluation of standard of care in Type 2 diabetes: a nationwide study in primary care. Cardiovasc. Endocrinol. 6(4), 145–151 (2017).
26.
Persson F, Bodegard J, Lahtela JT et al. Different patterns of second-line treatment in Type 2 diabetes after metformin monotherapy in Denmark, Finland, Norway and Sweden (D360 Nordic): a multinational observational study. Endocrinol. Diabetes Metab. 1(4), e00036 (2018).
Information & Authors
Information
Published In
Pages: 29 - 37
PubMed: 34841893
Copyright
© 2021 Niels Ejskjaer. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 July 2021
Accepted: 17 September 2021
Published online: 29 November 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The cost–effectiveness of oral semaglutide versus empagliflozin in Type 2 diabetes in Denmark. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0169
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ian W. Campbell, Kerstin M. G. Brand, Ulrike Gottwald-Hostalek, Julian Dettenbach, Evaluating Cost-Effectiveness in Relation to the Supporting Clinical Evidence Across the Type 2 Diabetes Continuum: A Review of Metformin and SGLT2is, Advances in Therapy, 10.1007/s12325-026-03592-6, (2026).
- Lu Wang, Yinglin Wang, Quan Zhao, Economic evaluation of sodium-glucose transporter 2 inhibitors compared with glucagon-like peptide 1 receptor agonist for the treatment of type 2 diabetes: a systematic review, European Journal of Clinical Pharmacology, 10.1007/s00228-026-04015-9, 82, 4, (2026).
- Mari Pesonen, Virpi Jylhä, Eila Kankaanpää, Adverse drug events in cost-effectiveness models of pharmacological interventions for diabetes, diabetic retinopathy, and diabetic macular edema: a scoping review, JBI Evidence Synthesis, 10.11124/JBIES-23-00511, 22, 11, (2194-2266), (2024).
- Milanne Maria Johanna Galekop, Carin Uyl-de Groot, William Ken Redekop, Economic Evaluation of a Personalized Nutrition Plan Based on Omic Sciences Versus a General Nutrition Plan in Adults with Overweight and Obesity: A Modeling Study Based on Trial Data in Denmark, PharmacoEconomics - Open, 10.1007/s41669-023-00461-8, 8, 2, (313-331), (2023).
- Henrik Vitus Bering Laursen, Emmelie Ploug Jørgensen, Peter Vestergaard, Lars Holger Ehlers, A Systematic Review of Cost-Effectiveness Studies of Newer Non-Insulin Antidiabetic Drugs: Trends in Decision-Analytical Models for Modelling of Type 2 Diabetes Mellitus, PharmacoEconomics, 10.1007/s40273-023-01268-5, 41, 11, (1469-1514), (2023).
- Ryan Pulleyblank, Nikolaj Birk Larsen, Cost-Effectiveness of Semaglutide vs. Empagliflozin, Canagliflozin, and Sitagliptin for Treatment of Patients with Type 2 Diabetes in Denmark: A Decision-Analytic Modelling Study, PharmacoEconomics - Open, 10.1007/s41669-023-00416-z, 7, 4, (579-591), (2023).
- E. Biancalana, G. Petralli, F. Raggi, MR. Distaso, G. Piazza, C. Rossi, D. Tricò, A. Solini, Parameters influencing renal response to SGLT2 inhibitors and GLP1 receptor agonists in type 2 diabetes patients with preserved renal function: a comparative, prospective study, Journal of Endocrinological Investigation, 10.1007/s40618-022-01969-2, 46, 5, (991-999), (2022).
- Kristoffer Nilsson, Emelie Andersson, Sofie Persson, Kristina Karlsdotter, Josefin Skogsberg, Staffan Gustavsson, Johan Jendle, Katarina Steen Carlsson, Model‐based predictions on health benefits and budget impact of implementing empagliflozin in people with type 2 diabetes and established cardiovascular disease, Diabetes, Obesity and Metabolism, 10.1111/dom.14921, 25, 3, (748-757), (2022).
- Hiroshi BANDO, Useful Oral Administration of Glucagon-Like Peptide 1 Receptor Agonist (GLP-1RA) as Semaglutide (Rybelsus) for Type 2 Diabetes Mellitus (T2DM), Asploro Journal of Biomedical and Clinical Case Reports, 10.36502/2022/ASJBCCR.6260, 5, 1, (38-41), (2022).
- Samuel J. P. Malkin, Davide Carvalho, Catarina Costa, Vasco Conde, Barnaby Hunt, The long-term cost-effectiveness of oral semaglutide versus empagliflozin and dulaglutide in Portugal, Diabetology & Metabolic Syndrome, 10.1186/s13098-022-00801-4, 14, 1, (2022).