Cost–effectiveness of pembrolizumab for second-line treatment of esophageal squamous cell carcinoma patients with a combined positive score of 10 or more
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study aimed to evaluate the cost-effectiveness of pembrolizumab compared with that of chemotherapy in the second-line treatment of locally advanced or metastatic esophageal squamous cell carcinoma (ESCC) patients with a combined positive score ≥10. Methods: A Markov model was established to compare the lifetime costs and quality-adjusted life years (QALYs) of different treatment options. Sensitivity analysis was performed to test the stability of the model. Results: The increased utility and cost of pembrolizumab were 0.442 QALYs and US$11,826.79 compared with those of chemotherapy. The incremental cost–effectiveness ratio was US$26,757.45/QALY, which was less than the threshold of three-times the GDP per capita. The prices of paclitaxel and pembrolizumab were the most important influencing factors. Conclusion: Pembrolizumab is a cost-effective second-line treatment of ESCC.
Esophageal cancer is one of the most common malignant gastrointestinal tumors. In 2018, esophageal cancer ranked seventh in the incidence of malignant tumors and sixth in deaths in the world [1]. Esophageal squamous cell carcinoma (ESCC) is the main subtype of esophageal cancer in the Asian population. ESCC in China accounts for more than half of the global ESCC [2]. Chemotherapy is a common first-line treatment for patients with advanced or metastatic ESCC. For patients who progress after the first-line treatment, previous single-agent chemotherapy methods, such as docetaxel or paclitaxel, cause various problems, such as low benefit, short survival and poor prognosis [3]. The emergence of immune checkpoint inhibitors has made a new breakthrough in the second-line treatment of patients with advanced esophageal cancer. The guidelines recommends immunotherapy as the standard treatment plan for the second-line treatment of advanced esophageal cancer. The National Medical Products Administration of China and US FDA approved pembrolizumab for patients with recurrent, locally advanced or metastatic ESCC whose tumors express PD-L1 (combined positive score [CPS] ≥10) [4,5]. The KEYNOTE-181 trial (35.4% of patients had PD-L1 CPS ≥10) confirmed that pembrolizumab can significantly improve metastatic ESCC that has received a systemic treatment in the past compared with that of standard chemotherapy [6].
Although pembrolizumab improves survival, studies have yet to clarify whether its relatively high price is economical and whether it brings additional socioeconomic burdens. Therefore, pembrolizumab treatment for patients who are refractory to ESCC or cannot tolerate first-line chemotherapy should be economically evaluated. This study compared the cost–effectiveness of pembrolizumab and chemotherapy for ESCC from the perspective of China’s health service system.
Methods
Model structure
The hypothetical target population of this study included patients who suffered from programmed death receptor-ligand 1 (PD-L1)-positive (CPS ≥10) ESCC and progress after first-line systemic therapy. The Markov model was established on the basis of the disease outcome of ESCC. The model had three health states: progression-free disease (PFD), progressed disease (PD) and death. All the patients initially entered the study with PFD. In each Markov cycle, patients could maintain a certain health state or develop another health state (Figure 1). The model period was set to 21 days, and the time horizon was set to 10 years, which could fully cover the patient’s full life cycle. The main measurement indicators of the study were the total cost and quality-adjusted life years (QALYs), which are discounted at a rate of 5% per year [7]. Incremental cost–effectiveness ratio (ICER) is the increased cost for each additional QALY: ICER = (total cost of the pembrolizumab group – the total cost of chemotherapy group) / (pembrolizumab group QALYs – chemotherapy group QALYs). Considering the chosen threshold is pembrolizumab cost effective, 3 times the national per capita GDP in 2019 (US$10,278.08) was used as the willingness-to-pay (WTP) threshold [7–9]. The model was built and statistical analysis was conducted using the TreeAge Pro 2020 software package.
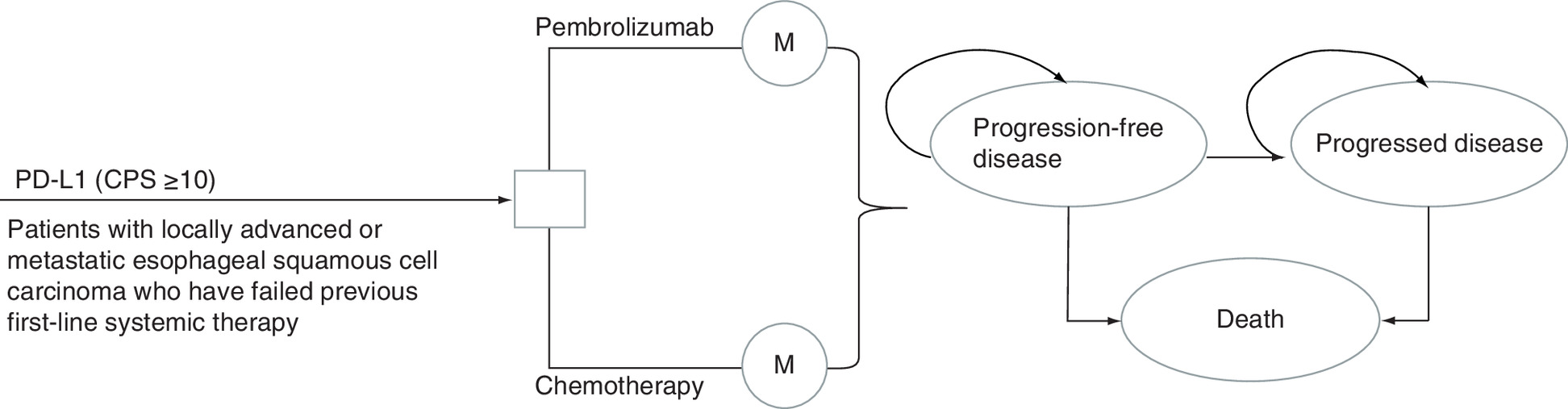
Figure 1. Markov model of esophageal squamous cell carcinoma.
CPS: Combined positive score; M: Markov cycle.
Clinical data
The clinical efficacy and safety data of the second-line treatment for ESCC were mainly from the KEYNOTE-181 clinical trial [6]. The patients received 200 mg of pembrolizumab (once every 3 weeks for no more than 2 years) or any of the following chemotherapy regimens: 90 mg/m2 paclitaxel (80–100 mg/m2, one cycle every 4 weeks on days 1, 8 and 15); 75 mg/m2 docetaxel (once every 3 weeks); or 180 mg/m2 irinotecan (once every 2 weeks) until the disease progressed or tolerable toxicity appeared. Among the Chinese patients with ESCC, the pembrolizumab and chemotherapy groups had median overall survival (OS) of 12 and 5.4 months, respectively [6,10]. The pembrolizumab and chemotherapy groups had median progression-free survival (PFS) of 3.4 and 4.0 months, respectively [6,10]. The transition probability between states was assumed as a fixed value, and the median PFS and median OS of the two treatment groups were extracted and calculated with the following formula: P = 1 - e-rt and r = -ln(1 - P) / t [11–14]. The transition probability was shown in Table 1.
| Value | Lower limit | Upper limit | |
|---|---|---|---|
| Pembrolizumab group | |||
| PPFD-PD | 0.1330 | 0.1064 | 0.1596 |
| PPFD-death | 0.0001 | 0.0001 | 0.0001 |
| PPD-death | 0.0549 | 0.0439 | 0.0659 |
| PPD-PD | 0.9451 | 0.7561 | 1.0000 |
| Chemotherapy group | |||
| PPFD-PD | 0.1142 | 0.0914 | 0.1370 |
| PPFD-death | 0.0002 | 0.0002 | 0.0002 |
| PPD-death | 0.2929 | 0.2343 | 0.3515 |
| PPD-PD | 0.7071 | 0.5657 | 0.8485 |
P: Probability; PD: Progressed disease; PFD: Progression-free disease.
Cost & utility
The cost mainly includes drug cost, follow-up cost, treatment cost for adverse events above grade three and best supportive care cost. To fully reflect the impact of drug prices on results, the drug prices were taken as the median value of the prices in each province, and sensitivity analysis was performed on the lowest and highest values of prices in each province [15]. In the KEYNOTE-181 clinical trial, the proportion of patients receiving specific chemotherapy regimens is unclear. This study assumes that patients have the same opportunity to receive paclitaxel, docetaxel and irinotecan. The average body surface area of patients included in the model was 1.72 m2 (1.5–1.9 m2) [16]. The China Primary Health Care Fund implemented a new assistance program for pembrolizumab on 1 January 2021 – that is, patients could receive two courses of assistance after two courses of treatment, and after another two courses of treatment, patients could continue to receive assistance until the disease progresses, with a cumulative period of no more than 24 months [17]. The cost related to the treatment of adverse events was calculated by multiplying the incidence of adverse events above grade three by the cost of handling each adverse event [18,19]. The incidences of adverse events above grade three in the pembrolizumab and chemotherapy groups were 18.20 and 40.90%, respectively [6]. All cost units were converted to US dollars with an average renminbi (RMB) exchange rate of US$1 to 6.8974 yuan for the full year of 2020.
Utility values for the PFD and PD health states were taken from EQ-5D data from a global, randomized, placebo-controlled, double-blind phase three study, which recruited adults with advanced gastric cancer or gastroesophageal junction adenocarcinoma [20,21]. The study considered the impact of adverse events on the utility value of PFD, including grade three/four adverse events of leukopenia and anemia [22]. The incidences of leukopenia and anemia in the pembrolizumab group were 0 and 1.3%, respectively; in the chemotherapy group, the incidences of leukopenia and anemia were 10.1 and 7.8%, respectively [6]. The utility value and transition probability parameters conform to β distribution, and the cost parameters conform to γ distribution [23]. The cost and utility were shown in Table 2.
Sensitivity analysis
One-way sensitivity analysis was performed to determine the influence of different parameters on ICER when changing within a certain range, and the results were presented in the form of a tornado diagram. The upper and lower limits of the 95% CI of the parameter value were derived from the literature. For some data that could not reach the 95% CI, the value of the parameter was floated by ±25% on the basis value. In the probability sensitivity analysis, the parameters were set as random variables with specific distribution, and 10,000 Monte Carlo simulation was used to run the model to evaluate the overall robustness of the research results. Due to the high cost of pembrolizumab, its price fluctuates 50% downward in the value range.
Results
Basic analysis
In the life cycle set by the model, the pembrolizumab group received 0.861 QALYs, and the medical expenses were US$16,634.76; the chemotherapy group received 0.419 QALYs, and the medical expenses were US$4807.97. The ICER was US$26,757.45/QALY. When the WTP threshold was US$30,834.23/QALY, pembrolizumab was a more cost-effective treatment strategy than chemotherapy.
Sensitivity analysis
One-way sensitivity analysis showed that the prices of paclitaxel and pembrolizumab were the most sensitive model parameters (Figure 2). Other parameters that affected the results of the model included the price of docetaxel, the price of irinotecan, the utility value of PD and the discount rate, but the parameter did not change the results. Under the WTP threshold of US$30,834.23/QALY, the cost-effective probabilities of pembrolizumab and chemotherapy groups were 65.3 and 34.7%, respectively (Figure 3).
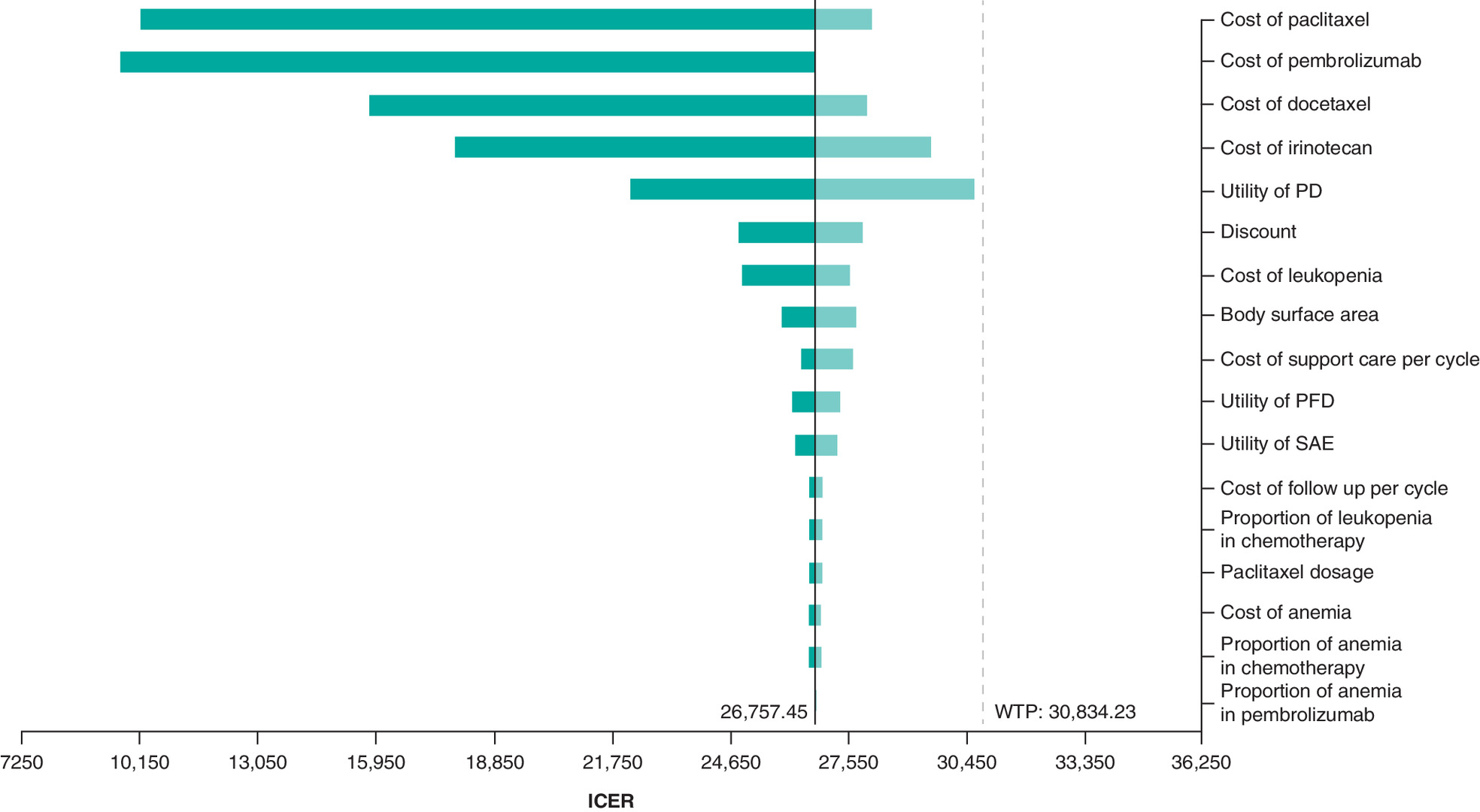
Figure 2. Tornado diagram of one-way sensitivity analyses.
PD: Progressed disease; PFD: Progression-free disease; SAE: Serious adverse event.
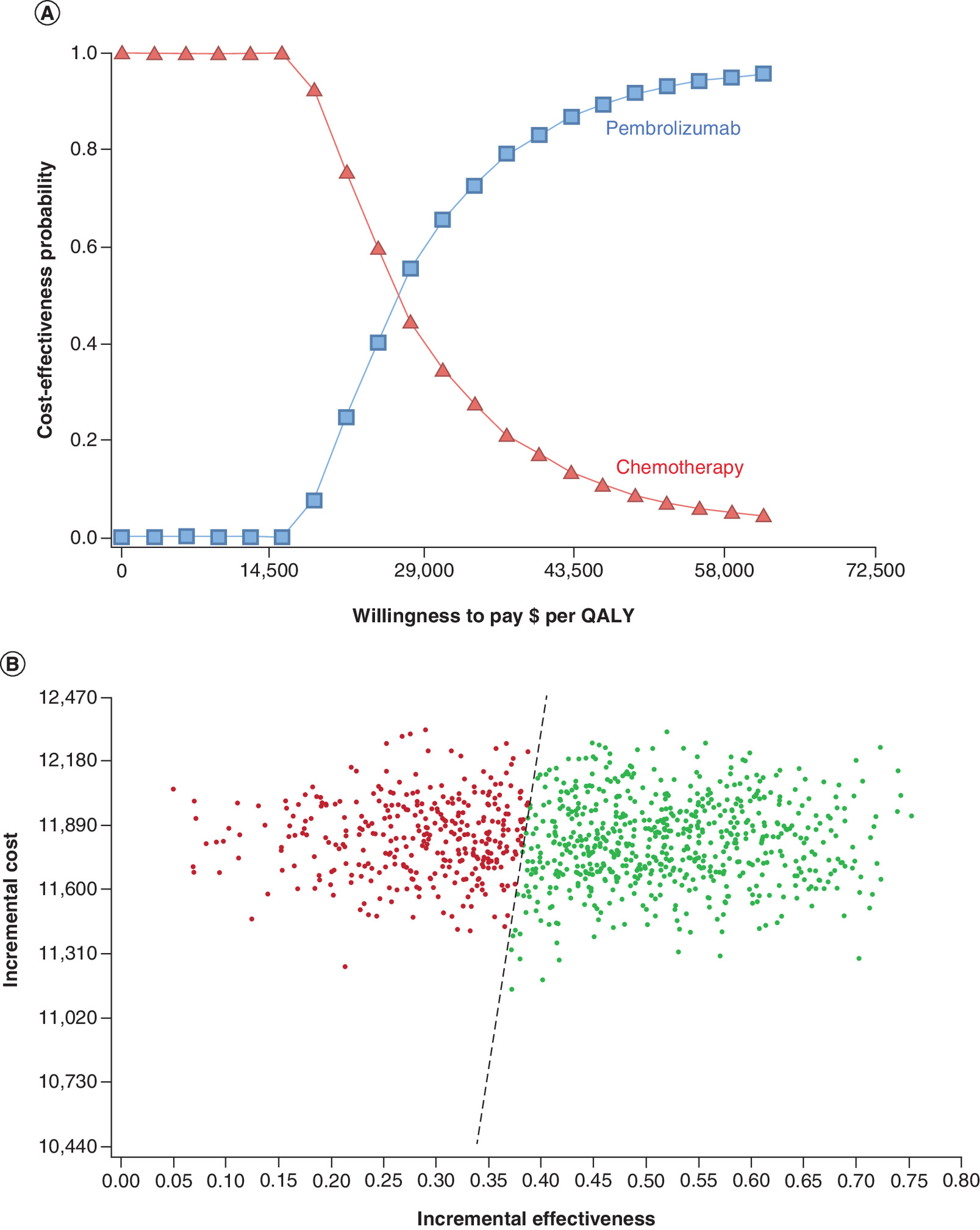
Figure 3. Probabilistic sensitivity analyses.
(A) Cost–effectiveness acceptability curves. (B) Scatter plot.
QALY: Quality-adjusted life year.
| Variable | Baseline value | Range | Ref. | |
|---|---|---|---|---|
| Minimum | Maximum | |||
| Cost (US$) | ||||
| Pembrolizumab per mg | 25.98 | 12.99 | 25.98 | [15] |
| Paclitaxel per mg | 0.72 | 0.04 | 8.48 | [15] |
| Docetaxel per mg | 0.13 | 1.77 | 14.95 | [15] |
| Irinotecan per mg | 0.44 | 1.64 | 4.65 | [15] |
| Follow-up visit per cycle | 49.41 | 43.18 | 56.04 | [21] |
| Best supportive care per cycle | 16.98 | 4.68 | 46.77 | [21] |
| Adverse event for leukopenia per unit | 447.08 | 0.00 | 1371.30 | [21] |
| Adverse event for anemia per cycle | 487.72 | 365.73 | 609.51 | [24] |
| Utility | ||||
| PFD | 0.741 | 0.593 | 0.889 | [20,21] |
| PD | 0.581 | 0.465 | 0.697 | [20,21] |
| Adverse event | 0.280 | 0.210 | 0.350 | [25] |
PD: Progressed disease; PFD: Progression-free disease.
Discussion
ESCC is one of the most common malignant tumors in the world. The prognosis after the first-line treatment is poor, and treatment options are limited. KEYNOTE-181 clinical trials have shown that pembrolizumab can significantly prolong the OS of patients who suffer from ESCC and advanced or metastatic tumors expressing PD-L1 (CPS ≥10) and previously received treatment, thereby providing these patients with a new option for second-line treatment [6]. This study explored the cost–effectiveness of pembrolizumab. The ICER of pembrolizumab is US$26,757.45/QALY compared with that of chemotherapy. The price of the drug is the most important factor. Pembrolizumab is a cost-effective treatment strategy in cities with a GDP per capita of US$8919.01.
The price of immune checkpoint inhibitors is generally high. For some tumors, it can significantly improve the survival rate and quality of life, but long-term use may greatly increase medical expenditures. Therefore, the economics of immune checkpoint inhibitors should be evaluated from the perspective of pharmacoeconomics. However, current economic research on immune checkpoint inhibitors for the treatment of esophageal cancer is limited. In a recent study, a model was established to compare the cost–effectiveness of nivolumab and chemotherapy from the perspective of the Chinese society. Nivolumab increased by 0.107 QALYs and US$14,627.90 compared with that of chemotherapy, and ICER was US$136,709.35/QALY; with a threshold of US$29,306.43/QALY, nivolumab may not have a cost-effective advantage [21]. In contrast to previous studies, our study evaluated the economics of pembrolizumab in the treatment of ESSC through Markov modeling combined with clinical evidence for the first time. The different conclusions of the two studies are mainly due to different efficacy and safety of different immune checkpoint inhibitors, and different research perspectives. These reasons may explain the inconsistencies of the two studies.
One-way sensitivity analysis shows that drug price was the most important parameter that affects the model. The main types of paclitaxel commonly used clinically are injectable, liposomal and albumin-bound paclitaxel, and the price difference is large. The price of the different types of paclitaxel was fully considered in one-way sensitivity analysis to avoid the influence of paclitaxel type selection on the results, so the price of paclitaxel had become the most important parameter in the model. The model was also sensitive to the price of pembrolizumab. On one hand, the price of pembrolizumab was expensive. On the other hand, to avoid the economic result of pembrolizumab’s sharp price reduction in the future, the range of drug price was expanded in sensitivity analysis. All the parameters change within the set range and do not affect the results of the model. Probabilistic sensitivity analysis reveals that the probability of pembrolizumab being economical is 65.3% under the payment threshold of three-times the GDP per capita in China. This probability increases to a greater extent as China’s per capita GDP increases.
This study has some shortcomings. First, the validity of the model is mainly based on the KEYNOTE-181 trial [6], and the bias in the trial affects the results of the model. However, KEYNOTE-181 is the only multicenter phase three clinical trial that explores pembrolizumab in the treatment of ESSC. It is also the best source of clinical data available. Therefore, a model based on the data of the KEYNOTE-181 study can be used to minimize the bias based on the existing evidence. Second, ignoring grade 1-2 adverse reactions in cost and utility may reduce the reliability of the results, but one-way sensitivity analysis shows that results are not sensitive to the relevant parameters of adverse reactions. Third, transition probability changes with time, and the model assumes that the transition probability is fixed. In this study, the transition probability is set to β distribution for probability sensitivity analysis to reduce the influence of the fixed transition probability. Fourth, this study fails to compare the economics of pembrolizumab with other treatment options because of the lack of clinical trials for head-to-head comparisons. Fifth, there are no local data reflecting the proportion of Chinese patients using a different chemo regimen. The model assumes that patients have the same opportunity to receive a different chemo regimen. Despite these limitations, sensitivity analysis showed that the parameters did not affect the economic results. Each parameter in the model did not affect the final result.
Conclusion
In summary, pembrolizumab has more cost advantages than chemotherapy in the second-line treatment strategy for ESCC.
•
This study tested the cost–effectiveness of pembrolizumab for the second-line treatment of locally advanced or metastatic esophageal squamous cell carcinoma in China.
•
The cost–effectiveness analysis suggested that pembrolizumab is a cost-effective second-line treatment of esophageal squamous cell carcinoma.
Author contributions
X Song assisted in conceptualization, methodology, supervision, project administration, formal analysis, writing review and editing. Z Zheng assisted in writing the original draft, writing review and editing. X Li assisted in methodology, software, formal analysis, visualization, writing the original draft. H Cai assisted in formal analysis and visualization of the project. L Zhang assisted in methodology, supervision, project administration and funding.
Financial & competing interests disclosure
This study was supported by Fujian Provincial Health Commission (grant no. 2020QNA014). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Bray F, Ferlay J, Soerjomataram I et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 68(6), 394–424 (2018).
• Provides background on the esophageal cancer.
2.
Zhang HZ, Jin GF, Shen HB. Epidemiologic differences in esophageal cancer between Asian and Western populations. Chin. J. Cancer 31(6), 281–286 (2012).
3.
Zhang L, Li W, Lyu X et al. Adjuvant chemotherapy with paclitaxel and cisplatin in lymph node-positive thoracic esophageal squamous cell carcinoma. Chin. J. Cancer Res. 29(2), 149–155 (2017).
4.
Chinese Society of Clinical Oncology. Guidelines of Chinese Society of Clinical Oncology (CSCO) Esophageal Cancer. People’s Medical Publishing House, Beijing, China (2020).
5.
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: esophageal and esophagogastric junction cancers. Version 1. ESOPH-F4 (2022).
6.
Kojima T, Shah MA, Muro K et al. Randomized Phase III KEYNOTE-181 study of pembrolizumab versus chemotherapy in advanced esophageal cancer. J. Clin. Oncol. 38(35), 4138–4148 (2020).
•• Global phase 3 study of pembrolizumab in advanced esophageal cancer.
7.
Liu G. China Guidelines for Pharmacoeconomic Evaluations Chinese-English version. China Market Press, Beijing, China (2020).
8.
National Bureau of Statistics. Statistical Bulletin of National Economic and Social Development of the People’s Republic of China in 2019. www.stats.gov.cn/tjsj/zxfb/202002/t20200228_1728913.html
9.
World Health Organization. Choosing interventions that are cost effective (WHO-CHOICE). Cost Effectiveness Thresholds. World Health Organization, Switzerland (2011). www.who.int/choice/en/
10.
Drug Instructions for Pembrolizumab Injection (Keytruda®) in China. Date of approval: 17 June 2020.
•• The clinical data of the Chinese subgroup pembrolizumab versus chemotherapy.
11.
Beck JR, Pauker SG. The Markov process in medical prognosis. Med. Decis. Making 3(4), 419–458 (1983).
12.
Zhou K, Zhou J, Huang J et al. Cost–effectiveness analysis of atezolizumab plus chemotherapy in the first-line treatment of extensive-stage small-cell lung cancer. Lung Cancer 130, 1–4 (2019).
13.
Zhan M, Zheng H, Xu T et al. Cost–effectiveness analysis of additional bevacizumab to pemetrexed plus cisplatin for malignant pleural mesothelioma based on the MAPS trial. Lung Cancer 110, 1–6 (2017).
14.
Le QA, Bae YH, Kang JH. Cost–effectiveness analysis of trastuzumab emtansine (T-DM1) in human epidermal growth factor receptor 2 (HER2): positive advanced breast cancer. Breast Cancer Res. Treat. 159(3), 565–573 (2016).
15.
Yaozhi.com. Inquiry about drug bidding information [2020-1-15]. https://db.yaozh.com/yaopinzhongbiao
16.
Zeng X, Peng L, Li J et al. Cost–effectiveness of continuation maintenance pemetrexed after cisplatin and pemetrexed chemotherapy for advanced nonsquamous non-small-cell lung cancer: estimates from the perspective of the Chinese health care system. Clin. Ther. 35(1), 54–65 (2013).
17.
China Primary Health Care Foundation. Key to Life-Tumor Immunotherapy Patient Assistance Project. http://smzy.ilvzhou.com/index.php?m=content&c=index&a=lists&catid=70&article_id=431
18.
Wu B, Ye M, Chen H, Shen JF. Costs of trastuzumab in combination with chemotherapy for HER2-positive advanced gastric or gastroesophageal junction cancer: an economic evaluation in the Chinese context. Clin. Ther. 34(2), 468–479 (2012).
19.
Zhang L, Hang Y, Liu M et al. First-line durvalumab plus platinum-etoposide versus platinum-etoposide for extensive-stage small-cell lung cancer: a cost–effectiveness analysis. Front. Oncol. 10, 602185 (2020).
20.
Büyükkaramikli NC, Blommestein HM, Riemsma R et al. Ramucirumab for treating advanced gastric cancer or gastro-oesophageal junction adenocarcinoma previously treated with chemotherapy: an Evidence Review Group perspective of a NICE Single Technology Appraisal. Pharmacoeconomics 35(12), 1211–1221 (2017).
• This is the primary source for utility.
21.
Zhang PF, Xie D, Li Q. Cost–effectiveness analysis of nivolumab in the second-line treatment for advanced esophageal squamous cell carcinoma. Future Oncol. 16(17), 1189–1198 (2020).
22.
Liu M, Zhang L, Huang Q et al. Cost–effectiveness analysis of ceritinib and alectinib versus crizotinib in the treatment of anaplastic lymphoma kinase-positive advanced non-small cell lung cancer. Cancer Manag. Res. 11, 9195–9202 (2019).
23.
Briggs AH, Weinstein MC, Fenwick EA et al. Model parameter estimation and uncertainty analysis: a report of the ISPOR-SMDM Modeling Good Research Practices Task Force Working Group-6. Med. Decis. Making 32(5), 722–732 (2012).
24.
Liubao P, Xiaomin W, Chongqing T et al. Cost–effectiveness analysis of adjuvant therapy for operable breast cancer from a Chinese perspective: doxorubicin plus cyclophosphamide versus docetaxel plus cyclophosphamide. Pharmacoeconomics 27(10), 873–886 (2009).
25.
Wu B, Ma F. Cost–effectiveness of adding atezolizumab to first-line chemotherapy in patients with advanced triple-negative breast cancer. Ther. Adv. Med. Oncol. 12, 1758835920916000 (2020).
Information & Authors
Information
Published In
Pages: 391 - 397
PubMed: 35179053
Copyright
© 2022 Future Medicine Ltd.
History
Received: 9 May 2021
Accepted: 5 January 2022
Published online: 18 February 2022
Keywords:
Topics
Authors
Funding Information
Fujian Provincial Health Commission: 2020QNA014
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of pembrolizumab for second-line treatment of esophageal squamous cell carcinoma patients with a combined positive score of 10 or more. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0112
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Pingyu Chen, Chang Fu, Lin Shen, Zhengyang Fei, Mengjie Luo, Yanqiu Chen, Hongchao Li, Cost-effectiveness analysis of tislelizumab vs. camrelizumab for the treatment of second-line locally advanced or metastatic esophageal squamous cell carcinoma, BMC Health Services Research, 10.1186/s12913-024-11142-5, 24, 1, (2024).
- Zhiwei Zheng, Jingrong Lin, Huide Zhu, Hongfu Cai, Cost-Effectiveness Analysis of Pembrolizumab Plus Chemotherapy vs. Chemotherapy Alone as First-Line Treatment in Patients With Esophageal Squamous Cell Carcinoma and PD-L1 CPS of 10 or More, Frontiers in Public Health, 10.3389/fpubh.2022.893387, 10, (2022).