Impact analysis of expanding narrow-spectrum antibiotic use for children with ear, sinus and throat infections
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Estimate the impacts treating acute respiratory tract infections (ARTIs) in children aged 6 months through 12 years with narrow-spectrum antibiotics. Materials & methods: Decision-tree model to estimate children’s health, healthcare utilization and costs, and caregiver’s time and costs for using narrow-spectrum antibiotics in eligible children with an ARTI, compared with current use of narrow- and broad-spectrum antibiotics. Results: Reduced adverse drug reactions by 35,750 (14%) cases) and 4750 (12%) fewer emergency department visits, 300 (12%) fewer hospitalizations, and 50,500 (10%) avoided outpatient visits. Annual healthcare costs fell by US$120 million (22%). Total societal costs declined by US$131 million (20%). Conclusion: National implementation of narrow-spectrum antibiotics to treat ARTIs in children improves patient outcomes and reduces caregiver burden and annual healthcare costs.
The American Academy of Pediatrics and the Infectious Disease Society of America recommend narrow spectrum antibiotics for treating most acute respiratory tract infections (ARTIs) [1,2]. These recommendations follow from evidence that broad-spectrum antibiotics use is associated with higher rates of adverse drug reactions than narrow-spectrum use [3,4] and has led to increased antibiotic resistance, making common infections more difficult to treat [5].
Despite the recommendations of leading professional organizations, children continue to receive high rates of prescriptions for broad spectrum antibiotics. Among children aged 1–17 years prescribed antibiotics between 2004 and 2010, almost half received at least one prescription for broad-spectrum antibiotics [6]. Most of these broad-spectrum antibiotic prescriptions were to treat ARTIs, which include acute otitis media (AOM), acute sinusitis (AS) and group A streptococcal pharyngitis (GAS) [7].
Gerber et al. conducted the first comparative effectiveness study comparing narrow- and broad-spectrum antibiotic therapy for ARTIs in children [8]. They found that for children with ARTIs, broad-spectrum antibiotics were not associated with better patient outcomes compared with narrow-spectrum antibiotics and were associated with a higher incidence of adverse drug reactions [8]. These findings suggest that using narrow-spectrum antibiotics to treat ARTIs in children with no contraindications has the potential to reduce burden on patients and their families, while also introducing healthcare cost savings. Quantifying the potential impacts of expanding the use of narrow-spectrum antibiotics in relation to current practice provides information to clinical decision-makers on the best course of action for treating children with ARTIs.
For this study, we estimated the potential impacts of expanding the use of narrow-spectrum antibiotics for eligible children with ARTIs, following the findings of Gerber et al. (2017). We developed an impact analysis model and estimated potential impacts on patient health, family caregivers’ time and work absenteeism, and healthcare and societal costs over a 1-year time horizon for patients, families, payers and society as a whole.
Overview of Gerber et al.
Gerber et al. compared the effectiveness of broad- and narrow-spectrum antibiotic treatment in children between the ages of 6 months and 12 years diagnosed with an ARTI and prescribed an oral antibiotic [8]. Their study analyzed two clinical outcomes in a retrospective cohort of 30,159 children: treatment failure and adverse drug reactions 14 days after diagnosis. The data included electronic health record data for January 2015 through April 2016 from a network of 31 pediatric primary care practices in Pennsylvania and New Jersey. Although Gerber et al. also analyzed patient-centered outcomes in a prospective cohort, our analysis did not use those findings [8].
Treatment failure was defined as a child having the same ARTI diagnosis and a new antibiotic prescription within 14 days after diagnosis. Adverse reactions included diarrhea, candidiasis, noncandidal rash, vomiting, allergic reaction, and other adverse events experienced between 1 week and 30 days after the start of treatment. Gerber et al. (2017) identified a sample of children prescribed narrow-spectrum antibiotics for ARTIs and used propensity score matching to identify a comparison group of children prescribed broad-spectrum antibiotics for ARTIs. The researchers found that use of broad-spectrum antibiotics was associated with a higher risk of adverse drug reactions than narrow-spectrum (risk difference of 1.1 percentage points [95% CI: 0.4–1.8]). They also found no difference in treatment failure between the children treated with broad-spectrum compared with narrow-spectrum drugs (risk difference of 0.3 percentage points (95% CI: -0.4–0.9). Gerber et al. reported aggregate findings and results stratified by diagnosis [8].
Materials & methods
We developed a decision-tree model to analyze the potential national impact of expanding the use of narrow-spectrum antibiotics to treat all children with AOM, AS and GAS who are not contraindicated for narrow-spectrum drugs. Because of the acute nature of these infections, we used a 1-year time horizon to capture all relevant impacts on outcomes and costs. A decision-tree framework is appropriate for acute conditions and short-term horizon.
The model analyzes the impact of current clinical practice, which involves a mixture of prescribing narrow- and broad-spectrum antibiotics for ARTIs, compared with expanding the use of narrow-spectrum antibiotics for children with ARTIs (Figure 1). The model estimates health outcomes, healthcare utilization, payer and out-of-pocket medical costs, caregiver time and travel costs, and societal costs. Societal costs are the sum of payer and out-of-pocket medical costs and caregivers’ time and travel costs. Each of the three infection types was modeled separately, using site-specific estimates for incidence of infection, current prescribing practices, treatment failure and adverse drug reactions.
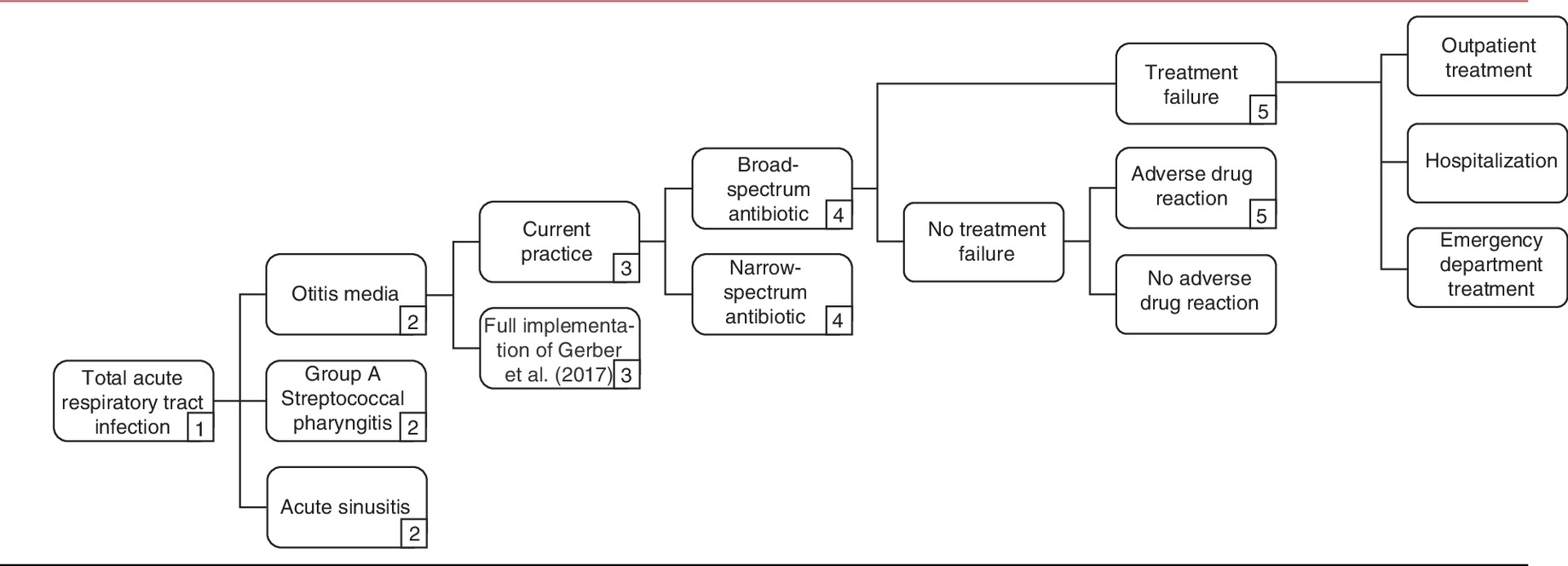
Figure 1. Decision tree model of expanding narrow-spectrum antibiotic use for acute respiratory tract infections in children.
The decision tree shows the pathways of mutually exclusive events. Numbers in squared boxes represent similar branch structure. For example, Strep A follows the same structure as otitis media at node 2; both treatment failure and adverse drug reaction are associated with a probability of outpatient treatment, hospitalization or emergency department treatment.
Model parameters
Parameters used in the model included population, clinical, healthcare costs and productivity measures. Table 1 shows the main input values used in the model and respective sources (details in appendix).
| Parameter description | Value | Source | Ref. |
|---|---|---|---|
| Population parameters | |||
| OM Incidence 6 months–2 years | 50.10 | Kawai et al. (2018) | [9] |
| OM Incidence 2–6 years | 19.20 | Kawai et al. (2018) | [9] |
| OM Incidence 6–12 years | 6.50 | Kawai et al. (2018) | [9] |
| AS incidence | 1.13 | Shapiro et al. (2011) | [10] |
| GAS incidence | 4.95 | Dooling et al. (2014) | [11] |
| Proportion on antibiotics, OM | 0.86 | Suaya et al. (2018) | [12] |
| Proportion on antibiotics, AS | 0.82 | Shapiro et al. (2011) | [10] |
| Proportion on antibiotics, GAS | 1 | Expert opinion | |
| Proportion on narrow spectrum, OM, 6 months–2 years | 0.65 | Suaya et al. (2018) | [12] |
| Proportion on narrow spectrum, OM, 2–6 years | 0.65 | Suaya et al. (2018) | [12] |
| Proportion on narrow spectrum, OM, 6–12 years | 0.65 | Suaya et al. (2018) | [12] |
| Proportion on narrow spectrum, AS | 0.58 | Shapiro et al. (2011) | [10] |
| Proportion on narrow spectrum, GAS | 0.76 | Gidengil et al. (2013) | [13] |
| Exclusion of penicillin-allergic children | 0.88 | Vyles et al. (2017); Nicklas et al. (1999); Kerr (1994); Lee et al. (2000) | [14–17] |
| Gerber et al. (2017) clinical findings | |||
| TF prob, narrow, OM, 6 months–2 years, 2–6 years, 6–12 years | 0.035 | Gerber et al. (2017) and weighted average of age-specific results, personal communication with Gerber | [8] |
| TF prob, narrow, AS | 0.015 | Gerber et al. (2017) | [8] |
| TF prob, narrow, GAS | 0.024 | Gerber et al. (2017) | [8] |
| TF prob, broad, OM, 6 months–2 years, 2–6 years, 6–12 years | 0.046 | Gerber et al. (2017) and weighted average of age-specific results, personal communication with Gerber | [8] |
| TF risk diff, broad, AS | 0.005 | Gerber et al. (2017) | [8] |
| TF risk diff, broad, GAS | -0.013 | Gerber et al. (2017) | [8] |
| ADR prob (retrospective), narrow, OM | 0.031 | Gerber et al. (2017) | [8] |
| ADR prob (retrospective), narrow, AS | 0.018 | Gerber et al. (2017) | [8] |
| ADR prob (retrospective), narrow, GAS | 0.021 | Gerber et al. (2017) | [8] |
| ADR risk diff (retrospective), broad, OM | 0.018 | Gerber et al. (2017) | [8] |
| ADR risk diff (retrospective), broad, AS | -0.004 | Gerber et al. (2017) | [8] |
| ADR risk diff (retrospective), broad, GAS | 0.001 | Gerber et al. (2017) | [8] |
| Unit costs (2017 US$) | |||
| Payer cost, narrow-spectrum antibiotic course, OM | 39.13 | GoodRx (2019); Chahine, Johnson & Costanzo (2014); Wicker & Mohundro (2010); TOP (2008) | [18–21] |
| Payer cost, broad-spectrum antibiotic course, OM | 77.40 | GoodRx (2019); Wicker & Mohundro (2010); Chahine et al. (2014); TOP (2008); Suaya et al. (2018) | [12,18–21] |
| Payer cost, narrow-spectrum antibiotic course, AS | 52.18 | GoodRx (2019); TOP (2008) | [18,21] |
| Payer cost, broad-spectrum antibiotic course, AS | 86.31 | GoodRx (2019); Demuri & Wald (2012); Contopoulous-Ioannidis, Ioannidis & Lau (2003); Leung & Kellner (2004); Suaya et al. (2018) | [12,18,22–24] |
| Payer cost, narrow-spectrum antibiotic course, GAS | 31.61 | GoodRx (2019); Milatovic, Adam, Hamilton & Materman (1993); Syrogiannopoulos et al. (2004); Tack et al. (1997); Chahine, Chamoun & Soucher (2013); Shulman et al. (2014); Choby (2009) | [18,25–30] |
| Payer cost, broad-spectrum antibiotic course, GAS | 71.59 | GoodRx (2019); Syrogiannopoulos et al. (2004); Chahine et al. (2013); Shulman et al. (2014); Tack et al. (1997); Milatovic et al. (1993); Choby (2009); Suaya et al. (2018) | [12,18,25–30] |
| Productivity parameters | |||
| Paid work hours per day per adult with own child | 5.51 | U.S. DOL BLA (2018b) | [31] |
| Average hourly wage ($) | $29.95 | U.S. DOL BLA (2018a) | [32] |
Complete list of parameters is shown in Appendix Table A1. Negative risk difference means broad spectrum is associated with lower risk of ADR or TF.
ADR: Adverse drug reaction; AS: Acute sinusitis; ED: Emergency department; GAS: Group A streptococcal pharyngitis; OM: Otitis media; OOP: Out of pocket; pop: Population; prob: Probability; risk diff: Risk difference; TF: Treatment failure.
Population & clinical parameters
Population size for the targeted age groups was obtained from the US 2017 Census projection for 2019 [33]. The estimated population size for all age groups excluded the 12% of children (range: 5–20%) allergic to penicillin [14–17], because those children are contraindicated for narrow-spectrum antibiotics. Children younger than 3 years diagnosed with GAS were excluded to reflect the American Academy of Pediatrics guidelines that recommend penicillin or amoxicillin treatment [25]. Annual incidence rates of AS, GAS and AOM were applied to the relevant population sizes to estimate the number of infections per year. For AOM, Kawai et al. reported 2012–2014 incidence rates for <2 years, 2–4 years and 5–18 years [9]. We used these Kawai et al. incidence rates for the three AOM age groups modeled [9]. For AS, we weighted the reported incidence rates for ages 0–5 years and 6–11 years in 1998 to 2007 by the proportion of visits in each age group to obtain an overall incidence of AS in ages 6 months to 12 years [10]. To estimate GAS cases, we multiplied the pharyngitis visit rate for ages 3–17 years in 1997–2010 [11] by the reported percentage of pharyngitis visits that were GAS; we applied the resulting GAS rate to the 3- to 12-year population in analyses.
The number of individuals with each type of infection was multiplied by the proportion of children taking antibiotics after diagnosis to identify those treated with an antibiotic for ARTI. The prescription rate for AOM was taken from Suaya et al. (2018), which reported antibiotic prescription rates for ages 0–9 years in 2016 [12]. Shapiro et al. reported prescription rates for AS for ages 0–17 years in 1998–2007 [10]. We assumed 100% antibiotic prescription for GAS because a diagnosis of GAS in children requires antibiotics to reduce rare complications (personal communication with A Hoberman). To model current practices, we assumed that among all ARTIs that resulted in antibiotic prescriptions, narrow-spectrum antibiotics were prescribed for 65% of children with AOM, 58% of children with AS, and 76% of children with GAS [10,12,13]. Based on these assumptions, we calculated that there were 8.3 million incident children aged 6 months to 12 years not contraindicated for narrow spectrum antibiotics. Of these incident children, we estimated 2.7 million cases per year are prescribed broad spectrum antibiotics under current practice and could instead receive narrow spectrum antibiotics under the modeled intervention practice.
We used estimates from Gerber et al. of the probability of treatment failure and adverse drug reactions and the adjusted risk difference between broad- and narrow-spectrum antibiotics for children diagnosed with an ARTI and prescribed an oral antibiotic [8]. To account for higher incidence of AOM among children in younger age groups, AOM was stratified into three age groups: 6 months to <2 years, 2 to <6 years and 6–12 years. For AS, we included children 6 months to 12 years, and for GAS, children 3–12 years.
Healthcare cost parameters
We first estimated the medical costs of ARTI treatment for broad- and narrow-spectrum antibiotics. Average cost of the first treatment course for each type of antibiotic was estimated using the following formula: average weight (kg) × dose (mg/kg/day) × duration of course (days) × average cost per mg ($/mg). The average weight for ages 6 months–12 years was 24.1 kg, which was calculated from the Census population size projection for 2019 and the growth chart published by the CDC in 2001 [33,34]. Recommended doses and durations of treatment course for each infection site and type of antibiotic were obtained from the literature. The average cost per milligram for each type of antibiotic was calculated from GoodRx [18]. Because of the young age of the study population, we assumed all antibiotics would be given in suspension form; we excluded other types of oral medications, such as tablets. We assumed antibiotic costs would be paid by the health insurer.
We next analyzed emergency department, inpatient, and outpatient visits and costs resulting from treatment failure and adverse drug reactions using 2006–2015 expenditure data from the Medical Expenditure Panel Survey [35]. Payer costs for these events were calculated as the sum of all medical costs except out-of-pocket spending. We combined outpatient and office-based events in analyses. All medical costs were estimated using MEPS weights and inflated to 2018 dollars using the Personal Consumption Expenditures: Health index [36].
We used the first three digits of ICD-9 codes to identify conditions associated with treatment failures and adverse reactions (AOM: 381,382 AS: 461, GAS: 034; unspecified adverse event: 995, digestive system events: 787, candidiasis: 112; skin or other integumentary tissue event: 782). Probabilities for emergency department treatment, hospital treatment, and outpatient treatment following a treatment failure or an adverse drug reaction were estimated from MEPS by infection site. Similarly, we obtained site-specific weighted mean payer costs and out-of-pocket costs for hospitalization, emergency department visit, and outpatient visits after treatment failure and adverse drug reaction.
Because of the small sample size for AS treatment failures, we assumed AS had the same treatment failure costs as AOM. The number of observations in MEPS that included a hospitalization for any infection site was very small, and many visits reported zero out-of-pocket costs. This resulted in unrealistically low out-of-pocket hospitalization costs for some events. To address this problem, we pooled the hospitalization sample for all sites of infection and calculated the average ratio between out-of-pocket and payer costs. We applied this ratio to the payer costs for each age group and infection site to calculate out-of-pocket costs for hospitalization by infection site.
Productivity cost parameters
We modeled missed work of family members who provided caregiving for children with an ARTI infection. We calculated forgone caregiver work hours by summing the time to transport and accompany the child to a medical appointment. We assumed a caregiver would lose 1 day of work for outpatient and emergency department visits and 2 days of work for hospitalizations. Average travel time for hospitalization, emergency department visits and outpatient visits was obtained from Ray et al. (2015) [37]. Caregiver costs were valued as a combination of travel cost and forgone wages from work absenteeism. We calculated travel costs as the number of clinician visits for a child’s ARTI multiplied by a travel cost per visit of US$15.70 [38]. Forgone wages were calculated by multiplying work hours missed by the median 2018 usual weekly earnings of full-time wage and salary workers [32] and multiplying by 1.3 to account for fringe benefits [39].
Sensitivity & scenario analyses
We conducted one-way sensitivity analyses to identify parameters to which model outcomes were most sensitive. Parameter values were obtained from the literature, where the 95% CI was assumed to be given by the upper and lower bounds of published parameter values. We varied each parameter individually across the confidence range while holding all other parameters at their base case values. We also conducted several scenario analyses in which we altered model parameter values based on estimates in the published literature. For example, we analyzed a scenario that used adverse drug response rates reported for the prospective cohort rather than the rates for the retrospective cohort in the Gerber et al. (2017) study. A second scenario analysis used an alternate input assumption for narrow-spectrum antibiotic use for GAS at baseline (52% as in Dooling et al., 2014, instead of 76% as in Gidengil et al. 2013) [11,13].
We conducted probabilistic sensitivity analysis to assess the impact of joint parameter uncertainty on model results. We drew 1000 replications from model input distributions to develop a 95% credible range for each model output. Supplementary Table A2 in appendix A shows the ranges and distributions used in sensitivity analysis.
Results
Model analyses indicated that treating children with a diagnosis of ARTI with narrow-spectrum antibiotics, unless contraindicated, reduced adverse drug reactions by approximately 14% (nearly 36,000 adverse events) and resulted in no increase in treatment failure compared with current practice (Table 2). This practice change could result in about a 12% reduction in annual emergency department visits and hospitalizations and about a 10% reduction in annual outpatient visits. Total annual healthcare sector costs, which include payer and out-of-pocket spending, could fall by 22% (US$120 million). Payer costs make up the largest share of this decline, falling by 22% (US$118 million annually) compared with current practice. Further, because 36.5% of US children are covered by Medicaid, estimates suggest US$43 million in cost savings to Medicaid. Annual societal costs, which include total healthcare costs and caregiver travel and time costs, could decrease US$131 million (20%).
| Outcome | Current practice | Expanded use of narrow-spectrum antibiotics | Estimated savings of expanding narrow-spectrum | Credible range of estimated savings | |
|---|---|---|---|---|---|
| Clinical outcomes | |||||
| Treatment failures | 280,400 | 260,560 | 19,830 | (4360) | 49,660 |
| Adverse drug reactions | 262,030 | 226,290 | 35,750 | 6920 | 67,830 |
| Healthcare utilization | |||||
| Emergency department visits | 40,770 | 36,030 | 4750 | 1440 | 8430 |
| Hospitalizations | 2550 | 2260 | 300 | 70 | 580 |
| Outpatient visits | 499,100 | 448,570 | 50,530 | 13,770 | 94,280 |
| Formal healthcare costs | |||||
| Payer costs (US$) | 539,721,890 | 421,737,950 | 117,983,940 | 78,950,720 | 157,226,120 |
| Medicaid costs | 196,998,490 | 153,934,350 | 43,064,140 | 28,817,010 | 57,387,530 |
| Other payer costs | 342,723,400 | 267,803,600 | 74,919,800 | 50,133,710 | 99,838,590 |
| Out-of-pocket costs (US$) | 17,607,920 | 15,717,960 | 1,889,960 | 491,320 | 3,739,560 |
| Total healthcare costs (US$) | 557,329,810 | 437,455,920 | 119,873,890 | 79,615,640 | 159,853,850 |
| Informal costs | |||||
| Total days with child in medical care | 544,980 | 489,110 | 55,880 | 16,250 | 102,820 |
| Total caregiver time | 3,454,870 | 3,100,680 | 354,190 | 101,480 | 652,970 |
| Caregiver lost earnings and travel cost (US$) | 111,973,240 | 100,494,280 | 11,478,970 | 3,320,490 | 21,111,660 |
| Societal perspective | |||||
| Total societal cost (US$) | 669,303,050 | 537,950,190 | 131,352,860 | 84,445,680 | 178,347,950 |
Note: Positive values in column estimated savings correspond to better outcome and negative values to worse outcome. Credible intervals were generated by probabilistic sensitivity analysis. The societal perspective combines costs from the patient and payer perspectives.
Sensitivity analyses
One-way sensitivity analyses for total societal costs and patient out-of-pocket costs showed the impact on base case cost savings of varying the base values of each parameter to lower and higher values. Tornado diagrams present one-way sensitivity analysis results for total societal costs and patient out-of-pocket costs (Figures 2 & 3).

Figure 2. Total annual societal cost savings for expanding narrow-spectrum antibiotic use to treat acute respiratory tract infections in children: shows most impactful inputs in one-way sensitivity analysis.
Sensitivity analysis Shows the range of societal cost saving (horizontal axis; US$) for lower and upper bound input values (vertical axis), when current use of narrow and broad-spectrum antibiotic is compared with using narrow-spectrum only. For example, higher payer cost of broad spectrum antibiotics is associated with larger societal cost savings, and vice versa.

Figure 3. Patient out-of-pocket cost savings for expanding narrow-spectrum antibiotic use to treat acute respiratory tract infections in children: shows most impactful inputs in one-way sensitivity analysis.
Sensitivity analysis Shows the range of patient out of pocket costs (horizontal axis; US$) for lower and upper bound input values (vertical axis), when current use of narrow and broad-spectrum antibiotic is compared with using narrow-spectrum only. For example, a higher adverse events risk difference for acute otitis media is associated with larger patient out of pocket cost savings, and vice versa.
Scenario analysis results show potential annual cost savings based on two alternate input assumptions. When we included adverse drug reaction response rates that Gerber et al. reported for their prospective cohort, estimated total societal cost savings more than doubled to US$318 million [8]. The additional cost savings in this scenario arise because of substantial reductions in adverse drug reactions from narrow- versus broad-spectrum antibiotics found in the prospective Gerber et al. cohort compared with the retrospective cohort analysis findings, especially for AS and GAS [8]. In another scenario analysis, we assumed the Dooling et al. proportion of narrow-spectrum antibiotics use for GAS of 52% rather than the base value of 76% [11,13]. Although GAS treatment failures increased under this scenario, aggregate cost savings increased to US$147 million because cost savings from using lower-cost narrow-spectrum antibiotics offset the increase in costs associated with GAS treatment failure.
Discussion
This is the first study to quantify the health and cost impacts of expanding the use of narrow-spectrum antibiotics for ARTIs in children, in relation to current practice where both narrow- and broad-spectrum antibiotics are used. When the benefits of narrow-spectrum antibiotic use are uncertain or perceived as less than the potential benefits of using broad-spectrum antibiotics, clinicians may be reluctant to prescribe them. Current practice shows that about 40% of ARTIs are treated with broad-spectrum antibiotics, possibly because of uncertainty about an infection’s cause, which might lead to choosing an antibiotic that kills a wider range of bacteria. However, the recommendations are to treat ARTIs with narrow-spectrum antibiotics, and not doing so places patient’s safety and healthcare quality at risk Gerber et al. provide evidence that narrow-spectrum antibiotics are as effective in treating ARTIs, while also leading to fewer adverse reactions, than broad-spectrum antibiotics [8]. Building on the demonstrated clinical benefits, we find substantial financial and time savings for patients, families, and payers of using narrow-spectrum antibiotics to treat most ARTIs in children.
Limitations
Our study used the clinical findings in Gerber et al. to assess the health and cost impacts of national implementation of narrow-spectrum antibiotics to treat ARTIs in young children [8]. However, although conducted in a large and diverse primary care network, the results from Gerber et al. (2017) might not be generalizable outside this setting.
The cost analysis relies on the assumption that the model inputs are a reasonable approximation of costs for treatment failures and adverse drug reactions. As these are relatively rare events, our estimates of costs using MEPS data may be imprecise. Additionally, misdiagnosis of ARTIs may bias estimated treatment failure rates. For example, our model assumes a treatment failure rate of 4.6% for broad-spectrum antibiotics for AOM across all children 6 months to 12 years old. This was based on Gerber et al. findings using claims-based methods to identify treatment of AOM. A prior randomized controlled trial, however, using more conservative methods for diagnosing AOM reported failure rates of 16% for broad-spectrum antibiotics, compared with placebo, for AOM in children younger than 2 years of age [40,41]. However, it should be noted that the findings in Gerber et al. reflect observed clinical practices, where many AOM infections are misdiagnosed, and antibiotics are unnecessarily prescribed to treat what might be an underlying viral infection [8].
Another limitation of our findings is that we did not model the impact of unnecessary use of broad-spectrum antibiotics on increases in antibiotic-resistant strains of common infections [4]. Because greater use of broad-spectrum antibiotics worsens infection resistance, over the long-term, patients, families and payers may incur even greater financial and time costs than our analysis shows. Future research might consider modeling the potential downstream impacts of reducing unnecessary broad-spectrum antibiotic use.
Conclusion
National implementation of narrow-spectrum antibiotics for eligible children aged 6 months to 12 years diagnosed with an ARTI has the potential to prevent nearly 36,000 adverse drug reactions (14% reduction), 4750 emergency department visits (12% reduction), 300 hospitalizations (12% reduction) and 50,530 outpatient visits (10% reduction). Compared with current practices that involve using narrow spectrum antibiotics to treat about 65% of ARTIs in children, expanding the use of narrow spectrum antibiotics could produce considerable healthcare sector and family cost savings. Healthcare sector costs would likely decline by US$120 million annually (22% reduction), consisting of US$118 million in payer costs averted and US$2 million in patient out-of-pocket costs averted. In total, 36% of payer cost savings are for Medicaid (US$43.1 million). Societal cost savings are expected to exceed US$131 million (20% reduction in costs). These savings would add up to US$657 million in societal costs savings over a 5-year period.
•
Narrow spectrum antibiotics are the recommended course of treatment for most acute respiratory tract infections (ARTIs) in children.
•
Despite recommendations, children receive high rates of prescriptions for broad-spectrum antibiotics to treat ARTIs.
•
This paper presents a decision-tree model the impacts of expanded use of narrow-spectrum antibiotics to treat ARTIs in children aged 6 months to 12 years with no contraindications.
•
Model parameters were identified from publicly available data sources and the literature.
•
Estimates indicate treating children with a diagnosis of ARTI with narrow-spectrum antibiotics, unless contraindicated, would meaningfully reduce adverse drug reactions and healthcare utilization.
•
Total annual healthcare sector costs, including payer and patient out of pocket spending, could fall by US$120 million (22%).
•
Annual societal costs, which include total healthcare costs and caregiver travel and time costs, could decrease US$131 million (20%).
•
Model results may underestimate future saving from increased substitution of broad to narrow-spectrum antibiotics since the change in practice will further reduce costs by lowering rates of antibiotic resistance.
Acknowledgments
We thank W Lawrence, A Hoberman, J Siegel, T Hoerger and L Kahwati for clinical guidance and valuable feedback on the study design and analysis approach and Ms Laurel Bates for excellent research assistance.
Disclaimer
The contents of this work are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee.
Financial & competing interests disclosure
Research reported in this manuscript was funded through a contract with the Patient-Centered Outcomes Research Institute (PCORI) (IDIQ-SOW #16-INSIGHT-AOSEPP-ENG). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (cer-2021-0064 supplementary materials.docx)
- Download
- 81.64 KB
References
1.
American Academy of Pediatrics. Pneumococcal infection. In: Report of the Committee on Infectious Diseases. Pickering L, Baker C, Kimberlin D, Long S (Eds). American Academy of Pediatrics, IL, USA, 571–581 (2012).
2.
Chow A, Benninger M, Brook I et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin. Infect. Dis. 54(8), e72–e112 (2012).
3.
Lovegrove MC, Geller AI, Fleming-Dutra KE, Shehab N, Sapiano MRP, Budnitz DS. US Emergency Department visits for adverse drug events from antibiotics in children, 2011–2015. J. Pediatric Infect. Dis. Soc. 8(5), 384–391 (2019).
4.
Shehab N, Lovegrove MC, Geller AI, Rose KO, Weidle NJ, Budnitz DS. US emergency department visits for outpatient adverse drug events, 2013–2014. J. Am. Med. Assoc. 316(20), 2115–2125 (2016).
5.
Bell BG, Schellevis F, Stobberingh E, Goossens H, Pringle M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 14(1), 1–25 (2014).
6.
Sarpong EM, Miller GE. Narrow- and broad-spectrum antibiotic use among U.S. children. Health Serv. Res. 50(3), 830–846 (2015).
7.
Hersh AL, Shapiro DJ, Pavia AT, Shah SS. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics 128(6), 1053–1061 (2011).
8.
Gerber JS, Ross RK, Bryan M et al. Association of broad- vs narrow-spectrum antibiotics with treatment failure, adverse events, and quality of life in children with acute respiratory tract infections. J. Am. Med. Assoc. 318(23), 2325–2336 (2017).
9.
Kawai K, Adil EA, Barrett D, Manganella J, Kenna MA. Ambulatory visits for otitis media before and after the introduction of pneumococcal conjugate vaccination. J. Pediatr. 201, 122–127.e1 (2018).
10.
Shapiro DJ, Gonzales R, Cabana MD, Hersh AL. National trends in visit rates and antibiotic prescribing for children with acute sinusitis. Pediatrics 127(1), 28–34 (2011).
11.
Dooling KL, Shapiro DJ, Van Beneden C, Hersh AL, Hicks LA. Overprescribing and inappropriate antibiotic selection for children with pharyngitis in the United States, 1997–2010. JAMA Pediatr. 168(11), 1073–1074 (2014).
12.
Suaya JA, Gessner BD, Fung S et al. Acute otitis media, antimicrobial prescriptions, and medical expenses among children in the United States during 2011–2016. Vaccine 36(49), 7479–7486 (2018).
13.
Gidengil CA, Kruskal BA, Lee GM. Initial antibiotic choice in the treatment of group A streptococcal pharyngitis and return visit rates. J. Pediatric Infect. Dis. Soc. 2(4), 361–367 (2013).
14.
Vyles D, Chiu A, Simpson P, Nimmer M, Adams J, Brousseau DC. Parent-reported penicillin allergy symptoms in the Pediatric Emergency Department. Acad. Pediatr. 17(3), 251–255 (2017).
15.
Kerr J. Penicillin allergy: a study of incidence as reported by patients. Br. J. Clin. Pract. 48(1), 5–7 (1994).
16.
Lee CE, Zembower TR, Fotis MA et al. The incidence of antimicrobial allergies in hospitalized patients: implications regarding prescribing patterns and emerging bacterial resistance. Arch. Intern. Med. 160(18), 2819–2822 (2000).
17.
Nicklas R, Bernstein I, Li J. β-Lactam antibiotics: the diagnosis and management of anaphylaxis. J. Allergy Clin. Immunol. 101(Suppl.), S498–S501 (1999).
18.
GoodRx. (2019) https://www.goodrx.com
19.
Chahine EB, Johnson AN, Costanzo A. Update on the management of pediatric acute otitis media. US Pharm. 39(7), 27–30 (2014).
20.
McMahon Wicker A, Labruzzo Mohundro B. Management of pediatric otitis media. US Pharm. 35(3), 44–49 (2010).
21.
TOP (Toward Optimized Practice). Diagnosis and treatment of AOM in children: summary of the Alberta clinical practice guideline for acute otitis media (2008 Update).
22.
DeMuri GP, Wald ER. Acute bacterial sinusitis in children. N. Engl. J. Med. 367(12), 1128–1134 (2012).
23.
Contopoulos-Ioannidis DG, Ioannidis JPA, Lau J. Acute sinusitis in children: current treatment strategies. Pediatr. Drugs 5(2), 71–80 (2003).
24.
Leung AKC, Kellner JD. Acute sinusitis in children: diagnosis and management. J. Pediatr. Heal. Care 18(2), 72–76 (2004).
25.
Shulman ST, Bisno AL, Clegg HW et al. Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America [Published correction in Clinical Infectious Diseases (2014), 58(10), 1496]. Clin. Infect. Dis. 58(10), 1496 (2014).
26.
Milatovic D, Adam D, Hamilton H, Materman E. Cefprozil versus penicillin V in treatment of streptococcal tonsillopharyngitis. Antimicrob. Agents Chemother. 37(8), 1620–1623 (1993).
27.
Syrogiannopoulos GA, Bozdogan B, Grivea IN et al. Two dosages of clarithromycin for five days, amoxicillin/clavulanate for five days or penicillin V for ten days in acute group A streptococcal tonsillopharyngitis. Pediatr. Infect. Dis. J. 23(9), 857–865 (2004).
28.
Tack KJ, Henry DC, Manford Gooch W et al. Five-day cefdinir treatment for streptococcal pharyngitis. Antimicrob. Agents Chemother. 42(5), 1073–1075 (1998).
29.
Chahine EB, Chamoun J, Sucher AJ. Management of streptococcal pharyngitis. US Pharm. 38(7), 51–56 (2013).
30.
Choby BA. Diagnosis and treatment of streptococcal pharyngitis. Am. Fam. Physician 79(5), 383–390 (2009).
31.
U.S. Department of Labor Bureau of Labor Statistics. Civilian labor force participation rate, seasonally adjusted total for all months in 2018. News release chart (2018).
32.
US Department of Labor Bureau of Labor Statistics. Current Population Survey: Unadjusted median usual weekly earnings, Employed full time, Wage and salary workers. BLS Data Viewer Series LEU0252881500 (2018).
33.
U.S. Census Bureau. 2017 National Population Projections Datasets: Projections for the United States, 2017 to 2060 (2018) https://www.census.gov/data/datasets/2017/demo/popproj/2017-popproj.html
34.
CDC (Centers for Disease Control and Prevention). Data Table of Infant Weight-for-age Charts. Growth Charts (2001) https://www.cdc.gov/growthcharts/html_charts/wtageinf.htm
35.
AHRQ (Agency for Healthcare Research and Quality). MEPS: Medical Expenditure Panel Survey 2006–2015 data (2019) https://meps.ahrq.gov/data_stats/download_data_files.jsp
36.
U.S. Bureau of Economic Analysis. Personal consumption expenditures: Services: Health care (chain-type price index). FRED. Federal Reserve Bank of St. Louis (2019). https://fred.stlouisfed.org/series/DHLCRG3Q086SBEA
37.
Ray KN, Chari AV, Engberg J, Bertolet M, Mehrotra A. Opportunity costs of ambulatory medical care in the United States. Am. J. Manag. Care 21(8), 567–574 (2015).
38.
Schmier J, Ogden K, Nickman N et al. Costs of providing infusion therapy for rheumatoid arthritis in a hospital-based infusion center setting. Clin. Ther. 39(8), 1600–1617 (2017).
39.
U.S. Department of Labor Bureau of Labor Statistics. Employer costs for employee compensation for the regions – September 2019. News Release #19-19877-DAL (2019).
40.
Hoberman A, Paradise JL, Rockette HE et al. Shortened antimicrobial treatment for acute Otitis media in young children. N. Engl. J. Med. 375(25), 2446–2456 (2016).
41.
Hoberman A, Paradise JL, Rockette HE et al. Treatment of acute otitis media in children under 2 years of age. N. Engl. J. Med. 364(2), 105–115 (2011).
Information & Authors
Information
Published In
Copyright
© 2021 Future Medicine Ltd.
History
Received: 14 March 2021
Accepted: 28 October 2021
Published online: 18 November 2021
Keywords:
Topics
Authors
Funding Information
Patient-Centered Outcomes Research Institute: IDIQ-SOW #16-INSIGHT-AOSEPP-ENG
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact analysis of expanding narrow-spectrum antibiotic use for children with ear, sinus and throat infections. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0064
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Anna Maria Peri, Mark D Chatfield, Weiping Ling, Luis Furuya-Kanamori, Patrick N A Harris, David L Paterson, Rapid Diagnostic Tests and Antimicrobial Stewardship Programs for the Management of Bloodstream Infection: What Is Their Relative Contribution to Improving Clinical Outcomes? A Systematic Review and Network Meta-analysis, Clinical Infectious Diseases, 10.1093/cid/ciae234, 79, 2, (502-515), (2024).
- Diqiong He, Feifeng Li, Jiong Wang, Chao Zhuo, Guanyang Zou, Antibiotic prescription for children with acute respiratory tract infections in rural primary healthcare in Guangdong province, China: a cross-sectional study, BMJ Open, 10.1136/bmjopen-2022-068545, 13, 11, (e068545), (2023).