Impact analysis of expanding anti-TNF therapy for Crohn’s disease
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To estimate the impact of universal anti-TNF therapy in patients with moderate-to-severe Crohn’s disease. Materials & methods: Developed a population-level Markov model to estimate the impact on health outcomes and medical expenditures of expanding anti-TNF therapy use versus current treatment practices. Results: Reductions in deaths (2600), hip fractures (980), major adverse cardiac events (2700) and patient out-of-pocket medical spending (2%) over 5 years. Total societal costs would be US$22,100 higher per patient per year, primarily due to the high cost of anti-TNF therapy. Conclusion: Expanding anti-TNF therapy use among US adult patients with moderate-to-severe Crohn’s disease would reduce morbidity and mortality, decrease disease-related medical costs and increase treatment costs compared with current practice. Despite the higher costs, this approach could substantially benefit patients.
Crohn’s disease is a type of inflammatory bowel disease (IBD), estimated to affect more than 300,000 adult patients in the USA [1]. Managing Crohn’s disease, which is a chronic condition, may involve ongoing use of an anti-TNF therapy or intermittent use of corticosteroids (CS) to control IBD symptoms [2]. Because symptoms often recur after stopping CS use, IBD patients may experience long periods or repeated use of CS therapy. A recent study by Lewis et al. found that patients who started using anti-TNF therapy after having had at least one prescription for CS therapy in the prior 12 months had lower rates of mortality, hip fracture and major adverse cardiac events (MACE) compared with patients who continued using or repeatedly used CS therapy in the prior 12 months and during the study year [2]. Increasing the use of anti-TNF drugs has the potential to reduce the average disease burden for patients and their families. In light of these benefits, patients could benefit from expanding the use of anti-TNF therapy in patients whose symptoms recur after using CS therapy to treat Crohn’s disease symptoms [2,3].
Lewis et al. conducted a retrospective cohort analysis of Medicaid and Medicare beneficiaries with inflammatory bowel disease (IBD) to analyze differences in mortality and common causes of death for patients who started using anti-TNF after having had at least one CS prescription in the previous year compared with prolonged CS users [2]. Prolonged CS users were identified as patients who had been prescribed at least 3000 mg of prednisone or the equivalent within a 12-month period (i.e., at least two prescriptions). Separate analyses were conducted for Crohn’s disease and ulcerative colitis patients. Lewis et al. found that Crohn’s disease patients with new initiation of anti-TNF therapy had lower odds of death, hip fracture and MACE than patients who were prolonged CS users. Crohn’s disease patients who started anti-TNF therapy had a higher risk of IBD-related hospitalization than patients with prolonged CS use. There were no significant differences in other outcomes between Crohn’s patients using anti-TNF therapy compared with those using CS. The study found no statistically significant differences in outcomes for ulcerative colitis patients by therapy type.
We used the Lewis et al.’s study findings to analyze the impact of expanding anti-TNF treatment for adult Crohn’s disease patients in the USA who have moderate-to-severe disease. Our analysis considered impacts on patients’ health, employment and financial outcomes. We also analyzed the economic impacts for various stakeholder groups, including patients, their families, their employers, healthcare payers and society as a whole. This information can be useful for guiding patient and clinician decisions and policies around using anti-TNF therapy to treat Crohn’s disease.
Methods
We developed an impact analysis spreadsheet model that estimated outcomes under two treatment regimens for Crohn’s disease: current practice, where some patients receive anti-TNF therapy and others have prolonged CS drug therapy and expansion of anti-TNF therapy to all patients with moderate-to-severe disease (Figure 1). We used a Markov model, which simulates disease progression over time through various health states for individuals with Crohn’s disease [4]. In the first year, all prevalent patients enter the model. Incident patients are added in each subsequent year. Patients may stop treatment because of treatment failure, adverse reactions, developing antibodies to the medicine or side effects. Patients who stop treatment do not re-enter the model. Patients who remain on or start using the therapies face risks of death, hip fracture, MACE and IBD-related hospitalization. The base analysis used a 5-year time horizon.
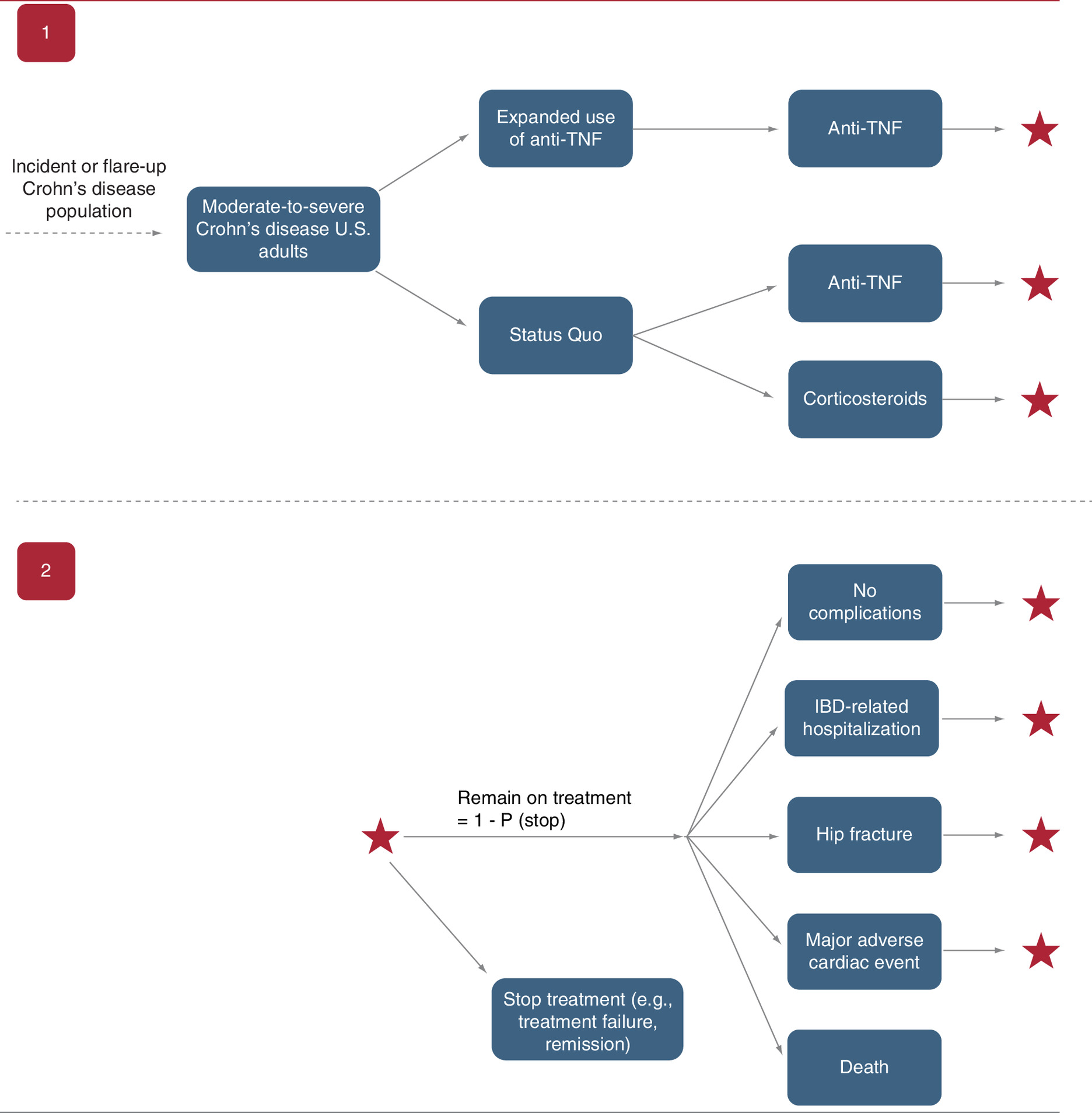
Figure 1. Anti-TNF treatment for Crohn’s impact analysis model.
The figure shows the Markov model used for the impact analysis. In Section 1 of the figure, the ‘Expanded Use of Anti-TNF’ pathway indicates that all patients with moderate-to-severe Crohn’s disease will receive anti-TNF therapy soon after diagnosis and continuing through the end of the modeling analysis, which is 5 years for the primary analysis. The ‘Status Quo’ pathway represents current practice and is the alternative against which expanded anti-TNF use is compared. The two treatment options in the status quo are anti-TNF and corticosteroids therapy. Section 2 of the figure shows the possible outcomes for Crohn’s patients who use anti-TNF or corticosteroids therapy. The stars on the far right of Section 2 indicate that patients who do not stop treatment or die in the current period analyzed will remain on treatment, with the same possible outcomes shown in Section 2 for each annual cycle of the Markov model. The probabilities of transitioning to each of the post-therapy states differ depending on the therapy used.
Model parameters
We obtained model parameters from the literature, publicly available statistics and analysis of national survey data. A clinical expert provided input on the appropriateness of model assumptions. We report all costs in 2018 dollars. Appendix A includes a full list of model parameters, values and sources.
Population & clinical parameters
We estimated the base year population of patients with moderate-to-severe Crohn’s disease by multiplying the estimated number of adults in the United States by disease prevalence [1,5]. We estimated the number of new adult cases of Crohn’s expected in subsequent model years using incidence from Loftus [6]. Sixty percent of Crohn’s disease patients were assumed to have moderate-to-severe disease [7]. In the current practice scenario, we assumed that 15% of eligible Crohn’s patients use anti-TNF therapy. This is similar to the percentage reported in Lewis et al. (18.7%).
We obtained parameter values for the model impacts (e.g., on death, hip fracture, MACE and IBD-related hospitalization) by treatment (e.g., anti-TNF or CS) from the results in Lewis et al. We assumed that 48% of patients stop treatment each year and that death occurs for 8% of patients with hip fractures, 9% with MACE and in 1% of IBD hospitalizations [8–10]. The model assumes patients who stop treatment do not re-enter the model. In clinical practice, however, patients who stop using one treatment often switch to the other therapy or to another type of therapy not captured in the model. The model also assumes a high rate of stopping treatment for anti-TNF therapy, based on clinical expert advice: patients are assumed to remain on anti-TNF therapy for an average of 2 years [7].
Healthcare cost parameters
Crohn’s disease treatment costs
We first estimated average annual costs of anti-TNF treatment for each of two types of anti-TNF therapies most commonly used to treat Crohn’s disease: infliximab and adalimumab. Among Crohn’s disease patients who use anti-TNF therapies, about 68% use infliximab and 32% use adalimumab [11]. Lewis et al. reported a similar distribution among anti-TNF users in the study population. We calculated average annual payer costs for infliximab by multiplying the number of infusions per year, assuming administration every 8 weeks, by average adult dose of 5 mg per kilogram of weight for an average patient weight of 70 kg. We also included administration costs per infusion of approximately US$1500 per year [12]. The average annual cost of infliximab treatment was US$20,700 per patient [13]. Patient out-of-pocket costs for infliximab were assumed to be US$25 per infusion [7]. Adalimumab costs assumed a 40-mg injection every 2 weeks, totaling US$41,100 per patient per year [13], with no facility costs. The weighted average annual cost for anti-TNF treatment was US$27,160 per patient.
For CS costs, we calculated a weighted average of costs for the two most commonly prescribed CS drugs: prednisone and budesonide (Appendix A). The average annual cost of CS therapy used in the model was US$410, with an upper bound of US$760 used in one-way sensitivity analyses [14]. Out-of-pocket costs for CS drugs were assumed to be US$22 per patient per year, based on an analysis of the Medical Expenditure Panel Survey (MEPS) 2010 through 2015 expenditures data [15].
Other healthcare costs
We obtained other healthcare costs to payers from the literature and secondary data analyses [7,15–21]. We used 2010 through 2015 MEPS to estimate the payer costs of an IBD-related visit and out-of-pocket costs for MACE, IBD-related hospitalization and IBD-related office visits. The analysis assumed four visits per year for CS users to monitor their Crohn’s disease and treatment tolerance but only two visits per year for anti-TNF users, because patients who receive intravenous infliximab infusions can often see the clinician and have laboratory tests conducted during their infusion visits [7].
Patient time, travel & productivity cost parameters
Estimates of the number of days of recovery and missed work from serious health events were obtained from the literature [21–23]. We assumed that patients receiving anti-TNF therapy spend an average of 13.2 h per year obtaining treatment and clinical care; patients receiving CS drugs spend 2 h per year for clinical care [11,24,25]. We also included patient travel costs of US$16 per clinician visit and for each infliximab treatment visit [26].
We valued patient time using an hourly wage of US$30, based on median 2018 usual weekly earnings of full-time wage and salary workers and assuming a 30% fringe benefits rate [27,28]. For each day spent in treatment or recovery from hip fracture, MACE and IBD-related hospitalization, we included the value of 16 h of patient time. We also included the value of unpaid caregiving provided by family members for 38% of patients’ time lost to hip fracture, MACE and IBD-related hospitalization [29]. Unpaid caregiving time was valued using an hourly wage of US$17, based on the median 2018 usual weekly full-time earnings of nursing and home health aides [30], including fringe benefits.
To model the impact of worker absenteeism on employers, we assumed that 63% of patients were in the labor force [31]. Absenteeism hours were calculated as 8 h per day times the number of patient or recovery days for hip fracture, MACE and IBD-related hospitalization plus patient time to receive Crohn’s disease treatment [7,11,21–25]. We applied the US$30/h wage rate assumption to value employee absenteeism.
Payer & societal cost estimation
To estimate costs to Medicare, we multiplied total payer costs by the percentage of patients with Medicare as their primary payer, which was reported as 35% in Lewis et al. We applied the percentage of adults aged 18–64 years with Medicaid as their primary payer [32], or 12.5%, to estimate costs to Medicaid. Remaining payer costs were assumed to be incurred by private and other payers.
We estimated total societal costs as the sum of payer spending, patient time cost and out-of-pocket spending for healthcare and healthcare-related travel, and family caregiving costs. Employer costs were not included to avoid double counting of patient time.
Sensitivity analyses
We conducted a series of one-way sensitivity analyses for select model parameters, varying parameter values based on upper and lower bounds in the published literature or from web-based pricing platforms. When reliable data ranges were not available, we allowed parameters to vary by plus or minus 20% from the base value.
We also conducted probabilistic sensitivity analysis to account for the impact of parameter uncertainty on model results, drawing 1000 values from distributions assumed for each input to develop a distribution for each impact analyzed. We identified credible intervals for all model results using the 2.5 and 97.5 percentiles of the distribution of each outcome. Supplementary Table 2 in Appendix A shows the input ranges for the one-way sensitivity analyses and distributions assumed for probabilistic sensitivity analysis.
Results
Our analysis modeled approximately 136,730 patients annually with moderate-to-severe Crohn’s disease in both the current practice and the expanded anti-TNF scenarios. Five-year mortality and health impacts of expanding the use of anti-TNF therapy for Crohn’s disease treatment compared with current treatment practices are shown in the top panel of Table 1. Findings show a 25% reduction in deaths among patients with Crohn’s disease, from 10,170 to 7610; a 46% reduction in hip fractures (from 2120 to 1140); and a 36% reduction in MACEs (from 7470 to 4760). IBD-related hospitalizations are 2% higher than current practice (7570 vs 7440).
| Outcome | A. Current practice | B. Expand anti-TNF therapy | Difference (A - B) | Annual savings per patient |
|---|---|---|---|---|
| Mortality and health impacts (shown as number of patients with each outcome) | ||||
| Deaths | 10,170 | 7610 | 2560 | |
| Hip fractures | 2120 | 1140 | 980 | |
| MACE | 7470 | 4760 | 2700 | |
| IBD-related hospitalizations | 7440 | 7570 | -140 | |
| Patient perspective | ||||
| Patient time, h | 5,803,200 | 11,477,470 | -5,674,270 | -8 |
| Out-of-pocket medical costs | US$146,268,990 | US$143,326,640 | US$2,942,300 | US$4 |
| Time and travel costs | US$220,465,160 | US$413,735,300 | -US$193,270,100 | -US$280 |
| Total costs | US$366,734,140 | US$557,061,940 | -US$190,327,800 | -US$280 |
| Payer perspective | ||||
| Costs for Crohn’s disease treatment | US$4,051,686,860 | US$19,129,764,170 | -US$15,078,077,300 | -US$22,100 |
| Costs for adverse events | US$645,147,870 | US$470,522,630 | US$174,625,200 | US$260 |
| Total payer costs | US$4,696,834,730 | US$19,600,286,800 | -US$14,903,452,100 | -US$21,800 |
| Medicare costs | US$1,643,892,160 | US$6,860,100,380 | -US$5,216,208,200 | |
| Medicaid costs | US$375,746,780 | US$1,568,022,940 | -US$1,192,276,200 | |
| Other payer costs | US$2,677,195,800 | US$11,172,163,480 | -US$8,494,967,700 | |
| Family perspective | ||||
| Hours of unpaid caregiving | 1,239,210 | 922,560 | 316,650 | 0.5 |
| Total unpaid caregiving costs | US$20,942,700 | US$15,591,330 | US$5,351,400 | $8 |
| Employer perspective | ||||
| Hours of absenteeism | 2,614,910 | 6,457,910 | -3,843,010 | -6 |
| Total productivity losses | US$78,404,490 | US$193,414,450 | -US$115,010,000 | -US$170 |
| Societal perspective | ||||
| Total healthcare sector costs | US$4,843,103,720 | US$19,743,613,440 | -US$14,900,509,700 | -US$21,800 |
| Total societal costs† | US$5,084,511,570 | US$20,172,940,070 | -US$15,088,428,500 | -US$22,100 |
†
Total costs from the societal perspective include healthcare sector costs (payer spending, patient spending) and informal healthcare sector costs (travel and time costs plus family costs for unpaid caregiving). Nonhealthcare sector costs of productivity losses are not included to avoid double-counting the same time loss.
Analysis assumes all patients with Crohn’s disease will use anti-TNF therapy, compared with current treatment practice, in which 15% of patients use anti-TNF therapy and the rest are assumed to be prolonged CS users. Negative values reflect larger impacts or costs for the expanded anti-TNF scenario compared with current treatment practice (e.g., more time, higher costs). Estimates have been rounded to the nearest tens place.
CS: Corticosteroids; IBD: Inflammatory bowel disease; MACE: Major adverse cardiac event.
Table 1 also shows economic impacts from the patient, payer, family, employer and societal perspectives. Results for the expanded anti-TNF scenario compared with current practice suggest eight additional hours of patient time per year and 2% lower out-of-pocket medical spending, saving patients US$2.9 million over 5 years. However, total patient cost, which includes travel costs and the value of patient time, increased by 52% or US$280 per patient per year. Payer costs increased by US$21,800 per patient per year, despite annual savings of US$260 per patient for reductions in deaths, hip fractures, MACE and IBD-related hospitalizations.
Expanding anti-TNF therapy compared with current treatment practice resulted in 316,650 h of avoided unpaid caregiving time for families, valued at US$5.4 million. Assuming almost 70% of patients missed work to receive anti-TNF therapy, the net impact of expanding anti-TNF for employers was an increase in absenteeism of about 6 h per patient per year, with associated productivity losses of US$170 per patient.
Widespread adoption of anti-TNF therapy resulted in a fourfold increase in total healthcare costs, from US$4.8 to US$19.7 billion, or by about US$21,800 per patient per year. This was driven by the higher treatment cost for anti-TNF therapy compared with CS. Given the assumed payer mix for adult Crohn’s disease patients, 35% of the additional payer costs were borne by Medicare, 8% by Medicaid and the remaining 57% by other payers. Total societal costs, which include patient time costs, out-of-pocket spending for medical care and travel, payer medical spending and family caregiving costs, were US$22,100 higher per patient per year in the expanded anti-TNF treatment scenario compared with current practice.
Sensitivity analyses
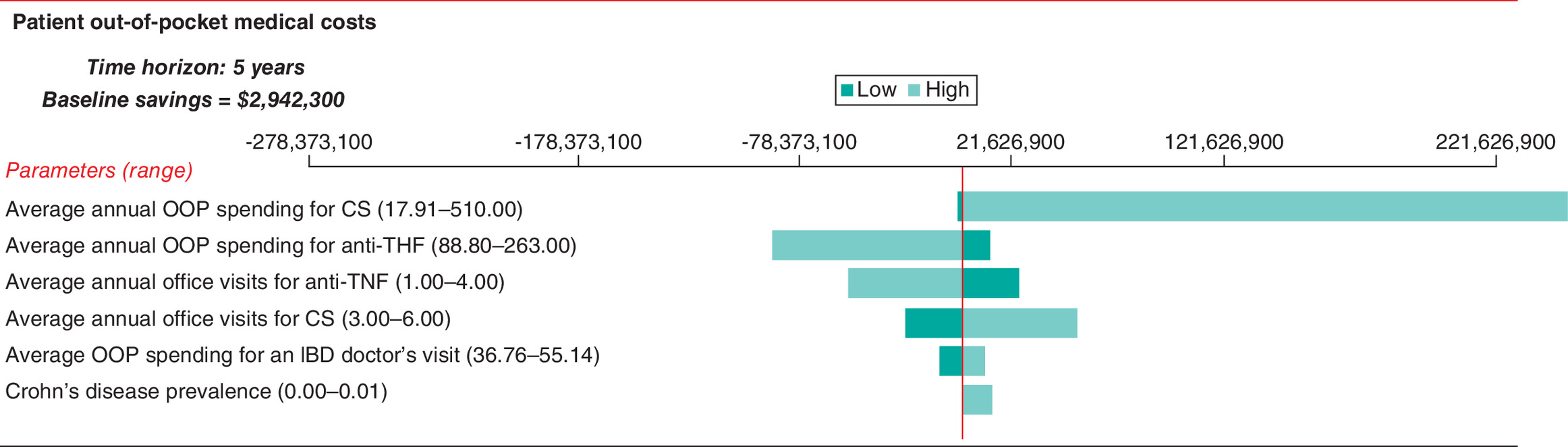
Patient out-of-pocket healthcare costs were most sensitive to the wide range of out-of-pocket spending for CS drugs: higher CS drug spending would raise savings from the expanded anti-TNF scenari (Figure 2). Patient out-of-pocket costs were also sensitive to the relatively wide range of out-of-pocket spending for anti-TNF therapy; higher spending for anti-TNF reduced savings.
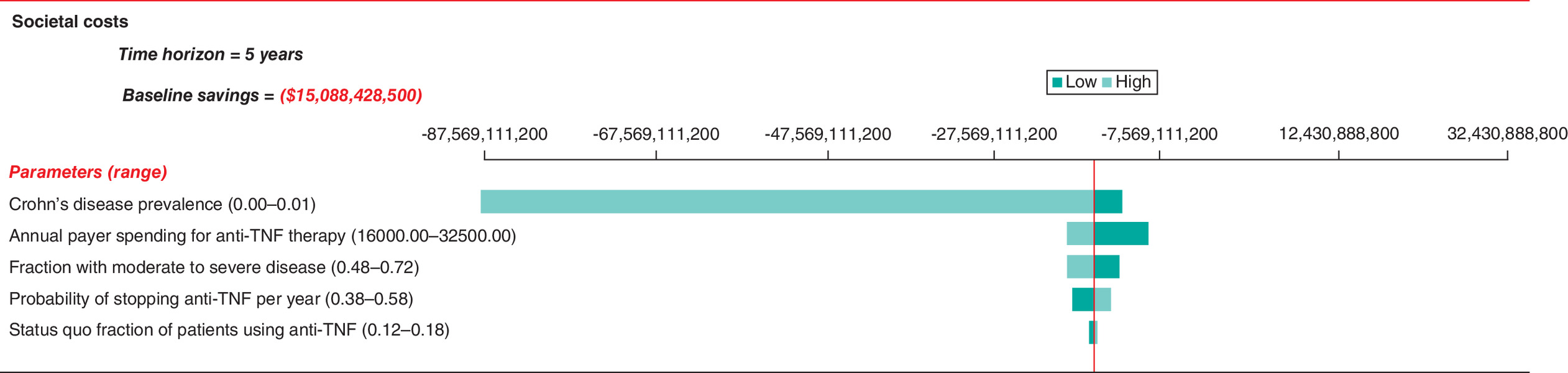
Total societal costs were most sensitive to Crohn’s disease prevalence, with a range of 0.15–1.3%. Societal costs were also sensitive to payer costs for anti-TNF therapy, the fraction of patients with moderate-to-severe disease and the probability of stopping treatment (Figure 3). Higher Crohn’s disease prevalence would result in higher total costs from using anti-TNF therapy for a larger number of patients compared with current practice. Payer costs for anti-TNF therapy also have substantial impact on total societal costs; payer costs of US$16,000 per year (vs the baseline value of US$27,160) imply additional societal costs for the expanded anti-TNF treatment scenario of US$8.6 billion. This number reflects a 43% decrease compared with the baseline estimated societal costs of US$15 billion for expanding anti-TNF treatment.
Finally, results of probabilistic sensitivity show fairly wide credible ranges (Table 2). Ranges that include 0 indicate uncertainty about whether the anti-TNF scenario compared with current practice would result in savings in time and cost or additional costs. For example, results suggest a 56% probability of savings in patient out-of-pocket spending. A credible range for deaths averted is 470 to 5420; a credible range for the increase in total societal costs is US$10.3–21.6 billion.
| Outcome | Impacts avoided or cost savings | Credible range lower bound | Credible range upper bound |
|---|---|---|---|
| Mortality and health impacts | |||
| Deaths | 2560 | 470 | 5420 |
| Hip fractures | 980 | 480 | 1730 |
| MACE | 2700 | 970 | 5030 |
| Patient perspective | |||
| Patient time in hours | -5,674,270 | -8,394,240 | -3,626,430 |
| Patient out-of-pocket medical costs | US$2,942,300 | -US$27,114,630 | US$31,318,420 |
| Total patient costs | -US$190,327,800 | -US$294,451,250 | -US$111,984,200 |
| Payer perspective | |||
| Total medical costs | -US$14,903,452,100 | -US$21,391,465,350 | -US$10,068,284,710 |
| Family perspective | |||
| Unpaid caregiving costs | US$5,351,400 | US$1,885,960 | US$9,859,880 |
| Employer perspective | |||
| Total productivity losses | -US$115,010,000 | -US$193,633,240 | -US$67,274,500 |
| Societal perspective | |||
| Total medical costs (patient and payer) | -US$14,900,509,700 | -US$21,386,685,970 | -US$10,070,588,480 |
| Total societal costs† | -US$15,088,428,500 | -US$21,641,006,880 | -US$10,265,309,760 |
†
Total costs from the societal perspective include healthcare sector costs (payer spending, patient spending) and informal healthcare sector costs (travel and time costs plus family costs for unpaid caregiving). Nonhealthcare sector costs of productivity losses are not included to avoid double-counting the same time loss.
Negative values reflect higher impacts or additional costs for the expanded anti-TNF scenario compared with current treatment practice (e.g., more time, higher costs). Estimates have been rounded to the nearest tens place.
MACE: Major adverse cardiac event.
Discussion
Policy makers, clinicians and Crohn’s disease patients can use the results from Lewis et al. and this impact analysis to inform treatment decisions for Crohn’s disease. Our analysis of the mortality, morbidity and economic impacts of expanding anti-TNF treatment for Crohn’s based on findings from the Lewis et al.’s study supports patients’ ability to engage with clinicians about the risks and benefits of available treatment options. Although anti-TNF therapies for treating Crohn’s disease are currently more expensive than alternatives, they are associated with substantial benefits, including improved survival and lower risks of adverse health events.
Costs to payers increase substantially in the expanded anti-TNF scenario because of the high annual cost of infliximab and adalimumab, the main anti-TNF biologic drugs used to treat Crohn’s disease. On average, these anti-TNF therapies cost approximately US$27,000 per patient per year. However, costs of using anti-TNF therapies to treat Crohn’s disease may decline by 40% or more with the adoption of recently available biosimilars [32,33]. To explore how broader use of biosimilars would affect our results, we analyzed the impact of 30 and 50% lower costs of anti-TNF therapies. We found that a 30% reduction in anti-TNF costs to payers would reduce annual payer costs to US$14,900 per patient versus US$21,800 in the baseline analysis. A 50% reduction in anti-TNF costs would lead to annual payer costs of US$10,400 per patient for anti-TNF treatment compared with current practice. Additionally, because newer and higher priced biologics have recently been approved to treat Crohn’s disease, such as vedolizumab and ustekinumab, future analyses should consider how the health impacts and costs of these medications compare with anti-TNF and CS therapies.
Recent studies have found increases in Crohn’s and IBD incidence and prevalence in the past decade in selected populations or for IBD as a whole [34–36]. If similar increases are occurring for Crohn’s disease in the US adult population, then our impact analysis results will understate the potential benefits of expanding anti-TNF treatment for patients with Crohn’s disease. For example, using the upper bound of prevalence in sensitivity analyses suggests that more than 14,000 deaths could be averted, 5700 hip fracture averted, 2700 MACE averted if anti-TNF therapy was expanded for eligible patients with Crohn’s disease (results not shown). Additionally, costs to expand anti-TNF therapy would increase proportionately to increases in the number of people with Crohn’s disease. The sensitivity analysis shown in Figure 3 shows that the upper bound for prevalence would suggest aggregate increases in societal costs of US$87.5 billion over 5 years for expanding anti-TNF therapy compared with current treatment practices.
Limitations
Potential impacts of Crohn’s disease and any impacts of anti-TNF and CS therapies not examined in Lewis et al. were not modeled. For example, potential side effects and health-related quality of life are important impacts that may differ between the two therapies, but they were not included in the impact analysis model. For example, CS use can cause unpleasant side effects, such as weight gain, which may affect patients’ preference for treatment and their overall quality of life. Treatment decisions about Crohn’s disease may be complex and require frequent communication between patients and their clinicians and adjustments to ensure adequate disease management. The current analysis was focused on the question of how Crohn’s disease patients could benefit from anti-TNF therapy compared with using repeated CS strategies to treat the chronic illness.
The model also assumes patients who stop treatment do not re-enter the model, whereas in clinical practice, patients who stop using one treatment often switch to the other therapy or to another type of therapy not captured in the model. This again suggests that a more complex model may be needed to compare the full range of alternative therapies for Crohn’s disease and to fully capture the impacts of the disease and alternative treatment strategies. The current analysis answers the simple question of the impact of using anti-TNF therapy, one of the most common biologics used for Crohn’s disease treatment, to treat moderate-to-severe Crohn’s disease compared with using CS. To answer questions about long-term treatments for Crohn’s disease and the health and economic impact of various treatment strategies from diagnosis, a more complex model of Crohn’s disease would be required.
The model also assumes a high rate of stopping treatment for anti-TNF therapy, based on clinical expert advice. Patients are assumed to remain on anti-TNF therapy for about 2 years, on average. To maintain balance in the number of patients in both treatment scenarios, the model assumes patients using CS therapy stop treatment at the same rate as those using anti-TNF therapy. Despite this assumption, the lower rate of death among patients using anti-TNF therapies means that, over time, the anti-TNF therapy scenario has more patients than the status quo treatment scenario (0.8% more patients are in the anti-TNF therapy scenario at the end of 10 years). However, the population size difference between the two scenarios is small enough that it has no meaningful effect on the economic impacts estimated in the model.
Another limitation is that our analysis assumes that all patients with Crohn’s disease will benefit equally from using anti-TNF compared with using CS therapies. However, it is possible that the patients who stand to benefit the most are those who are already using anti-TNF in the current practice scenario. If that were the case, our estimates would overstate the potential benefits of expanding anti-TNF therapy. However, because Lewis et al. focused on adverse health effects of using CSs, we expect that the impacts they observed on reducing hip fractures, cardiovascular disease events and deaths, would extend to patients with less severe Crohn’s disease than those already using anti-TNF therapies.
Finally, our model assumes published cost estimates for infliximab and adalimumab that reflect discounts and rebates to all payers. However, some payers may incur lower costs for these drugs because of prices negotiated with the manufacturers. Additionally, costs may fall over time as the use of biosimilars expands, because biosimilars are being introduced at lower prices than comparable biologics.
Conclusion
This impact analysis has highlighted differences across stakeholders in the impact of expanding anti-TNF therapy for Crohn’s disease. Expanding the use of anti-TNF therapy to all patients with moderate-to-severe Crohn’s disease has the potential to avert 2560 deaths, prevents 980 hip fractures and prevents 2700 MACE over 5 years and could save patients a modest amount in out-of-pocket medical spending compared with current practice. However, because of the high current cost of anti-TNF therapies, per patient healthcare costs are likely to be US$21,800 higher per year if anti-TNF therapies are used for all Crohn’s disease patients with moderate-to-severe disease.
•
Crohn’s disease is a type of inflammatory bowel disease, estimated to affect more than 300,000 adult patients in the United States. Management of the chronic disease often involves ongoing use of an antitumor necrosis factor-α (anti-TNF) therapy or episodic use of corticosteroids (CS).
•
Prior research demonstrates mortality and improved health outcomes for patients using anti-TNF compared with CS.
•
This paper presents a population-level Markov model to analyze the potential national impact of expanding anti-TNF therapy to all adults with moderate-to-severe Crohn’s disease.
•
Model parameters were identified from publicly available data sources and the literature.
•
Results indicate reductions in deaths, hip fractures, major adverse cardiac events and modest declines in patient out-of-pocket medical spending over 5 years.
•
Widespread adoption of anti-TNF therapy resulted in a fourfold increase in total healthcare costs, from US$4.8 to US$19.7 billion, or by about US$21,800 per patient per year. This is primarily due to the high cost of anti-TNF therapy.
•
Side effects and health-related quality of life may differ between the two therapies but were not included in the impact analysis model.
Acknowledgments
The authors thank MD Long and TJ Hoerger for valuable feedback.
Disclaimer
The contents of this work are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee.
Financial & competing interests disclosure
Research reported in this manuscript was funded through a contract with the Patient-Centered Outcomes Research Institute (PCORI) (IDIQ-SOW #16-INSIGHT-AOSEPP-ENG). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (appendix.docx)
- Download
- 59.51 KB
References
1.
Kappelman MD, Rifas-Shiman SL, Kleinman K et al. The prevalence and geographic distribution of Crohn’s disease and ulcerative colitis in the United States. Clin. Gastroenterol. Hepatol. 5(12), 1424–1429 (2007).
2.
Lewis JD, Scott FI, Brensinger CM et al. Increased mortality rates with prolonged corticosteroid therapy when compared with antitumor necrosis factor-α-directed therapy for inflammatory bowel disease. Am. J. Gastroenterol. 113(3), 405–417 (2018).
3.
Scott FI, Johnson FR, Bewtra M et al. Improved quality of life with Anti-TNF therapy compared with continued corticosteroid utilization in Crohn’s disease. Inflamm. Bowel Dis. 25(5), 925–936 (2019).
4.
Neumann PJ, Sanders GD, Russell LB et al. Cost-Effectiveness in Health and Medicine (2nd Edition). Oxford University Press, New York, USA (2017).
5.
U.S. Census Bureau. QuickFacts: United States. https://www.census.gov/quickfacts/fact/table/US/IPE120218
6.
Loftus EV. Clinical epidemiology of inflammatory bowel disease: incidence, prevalence, and environmental influences. Gastroenterology 126(6), 1504–1517 (2004).
7.
Long M. Personal communication. (2019).
8.
Alzahrani K, Gandhi R, Davis A, Mahomed N. “In-hospital mortality following hip fracture care in southern Ontario”. Can. J. Surg. 53(5), 294–298 (2010).
9.
Benjamin EJ, Blaha MJ, Chiuve SE et al. Heart disease and stroke statistics – 2017 Update. Circulation 135(10), e146–e603 (2017).
10.
Sewell JL, Yee HF. 13-Year mortality trends among hospitalized patients with inflammatory bowel disease. BMC Gastroenterol. 12, 79 (2012).
11.
Park KT, Sin A, Wu M, Bass D, Bhattacharya J. Utilization trends of anti-TNF agents and health outcomes in adults and children with inflammatory bowel diseases: a single-center experience. Inflamm. Bowel Dis. 20(7), 1242–1249 (2014).
12.
Wong B, Cifaldi MA, Roy S et al. Analysis of drug and administrative costs allowed by U.S. private and public third-party payers for 3 intravenous biologic agents for rheumatoid arthritis. J. Manag. Care Pharm. 17(4), 313–320 (2011).
13.
Institute for Clinical and Economic Review. A look at immune modulators for rheumatoid arthritis. https://icer-review.org/wp-content/uploads/2017/04/rheumatoid_arthritis_042017.pdf
14.
GoodRX. Amoxil. (.2019). https://www.goodrx.com/amoxil
15.
AHRQ (Agency for Healthcare Hesearch and Quality). MEPS: Medical Expenditure Panel Survey 2006-2015 data. (2019). https://meps.ahrq.gov/mepsweb/data_stats/download_data_files.jsp
16.
French EB, McCauley J, Aragon M et al. End-of-life medical spending in last twelve months of life is lower than previously reported. Health Aff. 36(7), 1211–1217 (2017).
17.
Shi N, Foley K, Lenhart G, Badamgarav E. Direct healthcare costs of hip, vertebral, and non-hip, non-vertebral fractures. Bone 45(6), 1084–1090 (2009).
18.
O’Sullivan AK, Rubin J, Nyambose J, Kuznik A, Cohen DJ, Thompson D. Cost estimation of cardiovascular disease events in the US. Pharmacoeconomics 29(8), 693–704 (2011).
19.
Centers for Disease Control and Prevention. Data and statistics: inflammatory bowel disease (IBD) prevalence in the United States. (2019). https://www.cdc.gov/ibd/data-statistics.htm
20.
Song X, Shi N, Badamgarav E et al. Cost burden of second fracture in the US Health System. Bone 48(4), 828–836 (2011).
21.
Bonafede M, Espindle D, Bower AG. The direct and indirect costs of long bone fractures in a working age US population. J. Med. Econ. 16(1), 169–178 (2013).
22.
Sasser AC, Rousculp MD, Birnbaum HG, Oster EF, Lufkin E, Mallet D. Economic burden of osteoporosis, breast cancer, and cardiovascular disease among postmenopausal women in an employed population. Women’s Heal. Issues 15(3), 97–108 (2005).
23.
Cohen RD, Larson LR, Roth JM, Becker RV, Mummert LL. The cost of hospitalization in Crohn’s disease. Am. J. Gastroenterol. 95(2), 524–530 (2000).
24.
Daniel SR, McDermott JD, Le C, Pierce CA, Ziskind MA, Ellis LA. A real-world, multi-site, observational study of infusion time and treatment satisfaction with rheumatoid arthritis patients treated with intravenous golimumab or infliximab. J. Med. Econ. 21(7), 724–731 (2018).
25.
Yokomizo L, Limketkai B, Park KT. Cost-effectiveness of adalimumab, infliximab or vedolizumab as first-line biological therapy in moderate-to-severe ulcerative colitis. BMJ Open Gastroenterol. 3(1), 1–6 (2016).
26.
Schmier J, Ogden K, Nickman N et al. Costs of providing infusion therapy for rheumatoid arthritis in a hospital-based infusion center setting. Clin. Ther. 39(8), 1600–1617 (2017).
27.
BLS DOL (Bureau of Labor Statistics – U.S. Department of Labor). Earnings, median usual weekly earnings, employed full time, 2018, by quarter. Labor Force Stat. from Curr. Popul. Surv. Series ID LEU0252881500 (2018).
28.
U.S. Department of Labor Bureau of Labor Statistics. Employer costs for employee compensation for the regions – September 2019. (2019). https://www.bls.gov/regions/southwest/news-release/employercostsforemployeecompensation_regions.htm
29.
Wolff JL, Roter DL. Family presence in routine medical visits: a meta-analytical review. Soc. Sci. Med. 72(6), 823–831 (2011).
30.
BLS DOL. Earnings, median usual weekly earnings, employed full time, 2018. Labor Force Stat. from Curr. Popul. Surv. Series ID LEU0254543600, LEU0258117500 (2018).
31.
BLS DOL. Civilian labor force participation rate, seasonally adjusted total for all months in 2018 [News release chart]. (2018). https://www.bls.gov/charts/employment-situation/civilian-labor-force-participation-rate.htm
32.
Kay J. The Dawn of the Biosimilars in the Management of IMIDs: understanding and integrating biosimilar data into informed collaborative care. In: Interdisciplinary Autoimmune Summit. MA, USA (2018). https://www.healio.com/news/rheumatology/20180428/biosimilars-drastically-reduced-costs-expanded-availability-in-europe
33.
Rudrapatna VA, Velayos F. Biosimilars for the treatment of inflammatory bowel disease. Pract. Gastroenterol. 43(4), 84–91 (2019).
34.
Dahlhamer JM, Zammitti EP, Ward BW et al. Prevalence of inflammatory bowel disease among adults aged ≥18 years – United States, 2015. MMWR Morb. Mortal. Wkly Rep. 65, 1166–1169 (2016).
35.
Shivashankar R, Tremaine WJ, Harmsen WS et al. Incidence and prevalence of Crohn’s disease and ulcerative colitis in Olmsted County, Minnesota from 1970 through 2010. Clin. Gastroenterol. Hepatol. 15(6), 857–863 (2017).
36.
Freeman K, Ryan R, Parsons N et al. The incidence and prevalence of inflammatory bowel disease in UK primary care: a retrospective cohort study of the IQVIA Medical Research Database. BMC Gastroenterol. 21, 139 (2021).
37.
Medicaid and CHIP Access and Payment Commission. Medicaid and CHIP Access and Payment Commission. Exhibit 40. https://www.macpac.gov/wp-content/uploads/2015/11/EXHIBIT-40.-Use-of-Care-among-Non-Institutionalized-Individuals-Age-0-18-by-Primary-Source-ofHealth-Coverage-2017-NHIS-Data.pdf
Information & Authors
Information
Published In
Copyright
© 2022 Future Medicine Ltd.
History
Received: 14 March 2021
Accepted: 16 November 2021
Published online: 11 January 2022
Keywords:
Topics
Authors
Funding Information
Patient-Centered Outcomes Research Institute,: IDIQ-SOW #16-INSIGHT-AOSEPP-ENG
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact analysis of expanding anti-TNF therapy for Crohn’s disease. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0063
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Thanh Lu, Sophia D'Angelo, Zohra Tayebali, Matthew Dempsey, Kristen Giombi, Olga Khavjou, Impact analysis of expanded access to ketamine for treatment-resistant depression, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0233, 14, 6, (2025).