Gender, socioeconomic status and emergency department visits among cancer survivors in the USA: a population-based study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess patterns of emergency department visits and subsequent hospitalization in relation to gender and socioeconomic status among a cohort of cancer survivors in the USA. Materials & methods: National Health Interview Survey datasets (2011–2017) were reviewed and participants with a history of cancer and complete information about emergency department visits in the past 12 months were included. Multivariable logistic regression analyses were used to assess factors associated with emergency department visits and subsequent hospitalization after the most recent emergency department visit. Results: A total of 22,240 cancer survivors were included in the current analysis; of which 16,133 participants (72.5%) who have not visited an emergency department in the past 12 months and 6107 participants (27.5%) who have visited an emergency department in the past 12 months. Multivariable logistic regression analysis suggested the following factors are associated with emergency department visits; younger age (odds ratio [OR] with increasing age: 0.98; 95% CI: 0.98–0.99), female gender (OR: 1.07; 95% CI: 1.00–1.15), African American race (OR: 1.26; 95% CI: 1.13–1.40), unmarried status (OR for married vs unmarried: 0.79; 95% CI: 0.74–0.84), lower yearly earnings (OR: 1.36; 95% CI: 1.20–1.54), poor health status (OR: 7.02; 95% CI: 6.02–8.18) and incomplete health insurance coverage (OR for complete coverage vs incomplete coverage: 0.66; 95% CI: 0.54–0.80). On the other hand, the following factors were associated with subsequent hospitalization: older age (OR: 1.004; 95% CI: 1.000–1.008), male gender (OR for female vs male: 0.86; 95% CI: 0.78–0.94), unmarried status (OR for married vs unmarried status: 0.80; 95% CI: 0.73–0.88), not working (OR: 1.44; 95% CI: 1.23–1.68), lower yearly earnings (OR: 1.31; 95% CI: 1.07–1.60), poor health status (OR: 8.43; 95% CI: 6.76–10.51) and lack of health insurance coverage (OR for complete coverage vs incomplete coverage: 0.71; 95% CI: 0.55–0.93). Conclusion: Female cancer survivors were more likely to visit the emergency department, whereas they were less likely to be subsequently hospitalized. Cancer survivors with lower socioeconomic status were more likely to visit emergency departments and to be subsequently hospitalized.
Many studies have evaluated the association between cancer-related factors (e.g., cancer site, stage or treatment) and emergency department visits [1–3]; however, little is known about the correlation between patient-related factors (e.g., gender, socioeconomic status, insurance coverage or yearly earnings) and emergency department visits among cancer patients. Gender-based differences have been observed within many aspects of cancer presentation, response to treatment and short-term and long-term adverse events of therapy [4–6]. Lower socioeconomic status among cancer survivors has been linked to more advanced disease at presentation, lack of access to effective treatments and worse patient outcomes [7–9]. So, it should be expected that both gender and socioeconomic status would affect the likelihood of emergency presentations and hospitalizations.
Traditional administrative databases used to assess factors associated with emergency presentations and hospitalizations usually provide information about cancer-related variables, but they are notoriously deficient with regards to socioeconomic/insurance variables [10,11]. National Health Interview Survey (NHIS) contains information about cancer diagnosis, emergency department visits, subsequent hospitalizations, gender, insurance status and socioeconomic status. Therefore, it is a suitable dataset to study the above associations [12].
The results of the current study can help better understand how gender and socioeconomic variables (including insurance status) play a role in access to healthcare resources among cancer patients. It can also help policymakers appreciate the potential waste in resources stemming from absent/suboptimal insurance coverage for a portion of the population through assessing its indirect sequelae (including higher use of hospital resources).
Objective
To assess patterns of emergency department visits and subsequent hospitalization in relation to gender and socioeconomic status among a cohort of cancer survivors in the USA.
Materials & methods
Data sources
The current study is based on NHIS datasets (2011–2017). NHIS is the largest community health survey in the USA and it is being collected on an annual basis. It provides comprehensive information about health status, access to health services and interaction with health providers and socioeconomic characteristics of participants. Within this yearly survey, information about the history of cancer diagnosis, type of cancer and visits to the emergency department and subsequent hospitalizations in the past year were included. Sampling of NHIS is based on a complex, multistage probability sample that incorporates stratification and clustering. Comparing the sampling strategy of NHIS datasets (2006–2015) to the sampling strategy of latter datasets, there was an oversampling of racial minorities in the former and no such oversampling (with the exception of participants 65+ years old) in the latter. Details of sampling, data collection processes and quality assurance procedures of the NHIS were provided elsewhere [13]. The inclusion criteria for the current study included: prior cancer diagnosis; and complete information about emergency department visits in the past 12 months. A cancer survivor was identified in the current study as an individual who answers ‘yes’ to the question ‘have you ever been told by a doctor or other health professional that you had cancer or a malignancy of any kind?’.
Data items
The following data were reviewed from the records of each participant (where applicable): age at survey completion, gender, race, marital status, working status, yearly earning, English language proficiency, educational level, self-reported health status, health insurance coverage in the past 12 months, type of insurance (private, Medicaid or Medicare) and primary site of cancer. Emergency department visits in the past 12 months, possible hospitalization after the most recent emergency department visit and patient-reported causes of emergency department visits were also collected. It has to be noted that patient-reported reasons are not mutually exclusive (i.e., some patients can report more than one reason for emergency department visits).
Information about cancer stage or treatment(s) is not provided within the NHIS datasets. Cancer treatment status (ongoing vs finished) is also not provided within the NHIS datasets.
Statistical analysis
Chi-squared testing was initially used to compare the baseline characteristics of participants who have or have not visited the emergency department in the last 12 months. Moreover, differences in socioeconomic variables between men and women were compared through Chi-squared testing. Multivariable logistic regression analysis was used to assess factors associated with emergency department admission and subsequent hospitalizations. Factors included in each model were age at survey completion, race, gender, marital status, working status, yearly earnings, English language proficiency, educational level and self-reported health status and health insurance coverage in the past 12 months. These variables were included because of previous evidence describing the impact of socioeconomic characteristics on emergency department visits and hospitalizations [14]. The primary tumor site was not included in this model because of a small number of individual participants within each tumor site category which would prevent proper statistical assessment of this variable. p < 0.05 represents statistical significance in the current study. Bonferroni adjustments for multiple testing was not used because of concerns about potential increase in type II error with this approach [15]. All statistical analyses were conducted through SPSS statistics (version 26.0; IBM; NY, USA).
Results
Patients’ characteristics
A total of 22,240 cancer survivors were included in the current analysis; of which 16,133 participants (72.5%) who have not visited an emergency department in the past 12 months and 6107 participants (27.5%) who have visited an emergency department in the past 12 months. This latter category included 793 participants (3.6%) have visited an emergency department more than three-times in the past 12 months. Among patients who visited emergency department at least once in the past 12 months, 6096 (27.4%) were subsequently hospitalized. Comparing both groups together, patients who visited an emergency department were more likely to be younger (p < 0.001), females (p < 0.001), unmarried (p < 0.001), unemployed (p < 0.001), have an African American race (p < 0.001), less educated (p < 0.001), have poorer health (p < 0.001) and incomplete health coverage (p < 0.001; Table 1). Emergency department visits were also less likely among individuals with private health insurance (p < 0.001) but more likely among individuals with Medicaid (p < 0.001) or Medicare coverage (p < 0.01). Among the included participants, a total of 2651 participants (11.9%) reported hospitalization after the most recent emergency department visit.
| Variables | No ER visits in the past 12 months (16,133 participants) | ER visits in the past 12 months (6107 participants) | p-value |
|---|---|---|---|
| Age (mean; SD) | 64.89; 13.23 | 63.74; 15.22 | <0.001 |
| Gender – Male – Female | 6746 (41.8%) 9387 (58.2%) | 2384 (39%) 3723 (61%) | <0.001 |
| Race – White – African American – Asian – American Indian – Others | 14332 (88.8%) 1094 (6.8%) 386 (2.4%) 77 (0.5%) 244 (1.5%) | 5139 (84.1%) 677 (11.1%) 99 (1.6%) 51 (0.8%) 141 (2.3%) | <0.001 |
| Marital status – Married – Unmarried – Unknown | 7915 (49.1%) 8193 (50.8%) 25 (0.2%) | 2398 (39.3%) 3703 (60.6%) 6 (0.1%) | <0.001 |
| Working – Yes – No – Unknown | 5717 (35.4%) 10408 (64.5%) 8 (<0.01%) | 1509 (24.7%) 4597 (75.3%) 1 (<0.01%) | <0.001 |
| Yearly earning – ≤$45,000 – >$45,000 – Unknown | 3118 (19.3%) 2457 (15.2%) 10558 (65.4%) | 1114 (18.2%) 495 (8.1%) 4498 (73.7%) | <0.001 |
| English proficiency – Very well – Well – Not well – Not at all – Unknown | 11080 (68.7%) 498 (3.1%) 202 (1.3%) 105 (0.7%) 4248 (26.3%) | 4118 (67.4%) 202 (3.3%) 81 (1.3%) 58 (0.9%) 1648 (27%) | 0.091 |
| Educational level – ≤High school – >High school – Unknown | 6027 (37.4%) 10066 (62.4%) 40 (0.2%) | 2764 (45.3%) 3304 (54.1%) 39 (0.6%) | <0.001 |
| Self-reported health status – Excellent – Very good – Good – Fair – Poor – Unknown | 2674 (16.6%) 5002 (31%) 5253 (32.6%) 2464 (15.3%) 729 (4.5%) 11 (0.1%) | 408 (6.7%) 1142 (18.7%) 1939 (31.8%) 1696 (27.8%) 917 (15%) 5 (0.1%) | <0.001 |
| Any time in the past 12 months without health insurance – Yes – No – Unknown | 277 (1.7%) 15213 (94.3%) 643 (4%) | 200 (3.3%) 5616 (92%) 291 (4.7%) | <0.001 |
| Type of insurance† – Private – Medicaid – Medicare | 10074 (62.4%) 1148 (7.1%) 9745 (60.4%) | 3001 (49.1%) 1104 (18.1%) 3940 (64.5%) | <0.001 <0.001 <0.001 |
†
Some patients have more than one type of insurance.
ER: Emergency room; SD: Standard deviation.
Rates of emergency department visits and subsequent hospitalizations according to the primary tumor site were described in Figure 1. Most common primary tumor with an emergency department visit and subsequent hospitalization was primary liver cancer (55.6 and 32% respectively). Percentages of emergency department visits and subsequent hospitalization across the study years were summarized in Figure 2 (p-value for emergency department visits: 0.286; p-value for subsequent hospitalization: 0.508). Patient-reported reasons for emergency department visits among women versus men were summarized in Figure 3 with the most reported reason for both groups is patients reporting that ‘only hospital could help with their condition’.
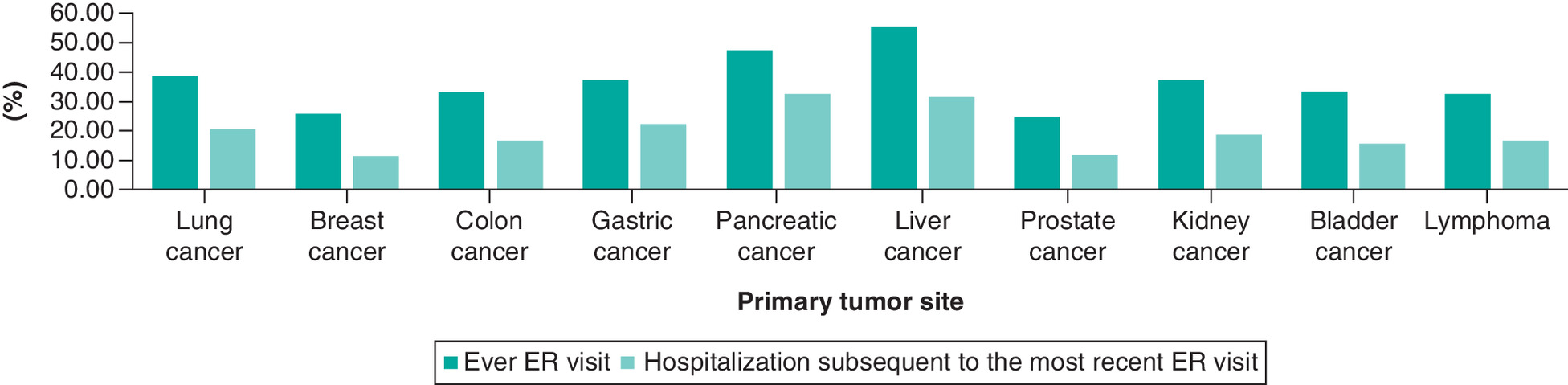
Figure 1. Rates of emergency department visits and hospitalizations according to selected primary tumor sites among cancer survivors in the United States.
ER: Emergency room.
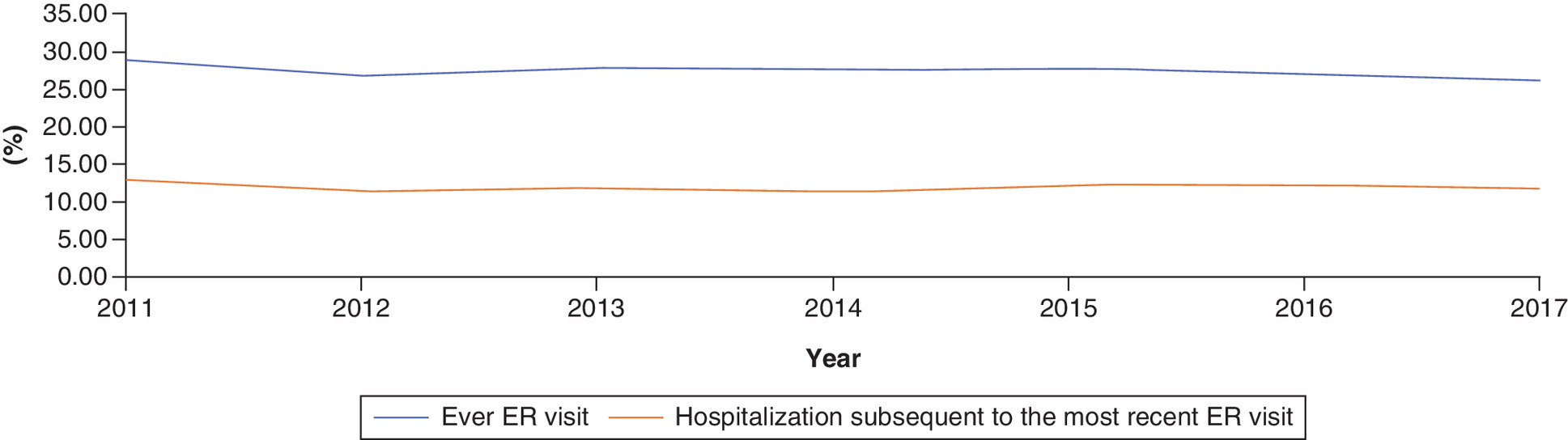
Figure 2. Emergency department visits and hospitalizations in the past 12 months before survey completion throughout the duration of the study.
ER: Emergency room.

Figure 3. Patient-reported reasons for emergency department visits among women versus men.
ER: Emergency room.
Comparing men versus women with regards to three socioeconomic variables (yearly earnings, education and insurance coverage) women were marginally more likely to have incomplete health coverage (2.5 vs 1.6% without insurance coverage in the past 12 months; p < 0.001) and lower income (21.6 vs 15.3% have income ≤$45,000; p < 0.001); but no differences in educational attainment (40.1 vs 38.8% have ≤high school education; p = 0.096).
To further assess the potential impact of affordable care act ‘ACA’ roll out on emergency department visits, rates of emergency visits in the past 12 months among survivors included in the 2011 survey (Pre-ACA) were compared with rates of emergency visits in the past 12 months among survivors included in the 2016 survey (post-ACA) and there was no difference (28.9 for 2011 vs 26.9% for 2016; p = 0.064). Similarly, rates of hospitalizations were not different between both groups of survivors (12.9 vs 12.2%; p = 0.446).
Socioeconomic factors associated with emergency department visits
Multivariable logistic regression analysis suggested the following factors are associated with greater odds of emergency department visit; younger age (OR with increasing age: 0.98; 95% CI: 0.98–0.99), female gender (OR: 1.07; 95% CI: 1.00–1.15), African American race (OR: 1.26; 95% CI: 1.13–1.40), unmarried status (OR for married vs unmarried: 0.79; 95% CI: 0.74–0.84), lower yearly earnings (OR: 1.36; 95% CI: 1.20–1.54), poor health status (OR: 7.02; 95% CI: 6.02–8.18) and incomplete health insurance coverage (OR for complete coverage vs incomplete coverage: 0.66; 95% CI: 0.54–0.80; Table 2).
| Variables | Ever emergency department visits | Hospitalization | ||
|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| Age (mean; SD) | 0.98 (0.98–0.99) | <0.01 | 1.004 (1.000–1.008) | 0.04 |
| Gender – Male – Female | Reference 1.07 (1.00–1.15) | 0.03 | Reference 0.86 (0.78–0.94) | <0.01 |
| Race – White – African American – Asian – American Indian – Others | Reference 1.26 (1.13–1.40) 0.62 (0.49–0.79) 1.21 (0.83–1.77) 1.21 (0.96–1.51) | <0.01 <0.01 0.31 0.09 | Reference 1.15 (1.00–1.32) 0.85 (0.62–1.15) 1.32 (0.82–2.12) 1.17 (0.87–1.56) | 0.05 0.30 0.24 0.27 |
| Marital status – Unmarred – Married | Reference 0.79 (0.74–0.84) | <0.01 | Reference 0.80 (0.73–0.88) | <0.01 |
| Working – Yes – No | Reference 1.35 (1.21–1.50) | <0.01 | Reference 1.44 (1.23–1.68) | <0.01 |
| Yearly earning – >$45,000 – ≤$45,000 | Reference 1.36 (1.20–1.54) | <0.01 | Reference 1.31 (1.07–1.60) | <0.01 |
| English proficiency – Very well – Well – Not well – Not at all | Reference 0.88 (0.73–1.05) 0.79 (0.59–1.04) 0.96 (0.67–1.36) | 0.17 0.09 0.83 | Reference 1.07 (0.85–1.34) 0.88 (0.61–1.27) 1.02 (0.66–1.58) | 0.54 0.50 0.91 |
| Educational level – >High school – ≤High school | Reference 1.03 (0.97–1.11) | 0.27 | Reference 1.03 (0.94–1.13) | 0.50 |
| Self-reported health status – Excellent – Very good – Good – Fair – Poor | Reference 1.48 (1.31–1.69) 2.29 (2.02–2.59) 4.05 (3.56–4.61) 7.02 (6.02–8.18) | <0.01 <0.01 <0.01 <0.01 | Reference 1.52 (1.23–1.88) 2.52 (2.06–3.08) 4.45 (3.63–5.47) 8.43 (6.76–10.51) | <0.01 <0.01 <0.01 <0.01 |
| Any time in the past 12 months without health insurance – Yes – No | Reference 0.66 (0.54–0.80) | <0.01 | Reference 0.71 (0.55–0.93) | 0.01 |
†
Cases with unknown variables were included in the analysis but not reported in this table.
OR: Odds ratio; SD: Standard deviation.
Socioeconomic factors associated with hospitalization after the most recent emergency department visit
Using multivariable logistic regression analysis, the following factors were associated with hospitalization following the most recent emergency department visit: older age (OR: 1.004; 95% CI: 1.000–1.008), male gender (OR for female vs male: 0.86; 95% CI: 0.78–0.94), unmarried status (OR for married vs unmarried status: 0.80; 95% CI: 0.73–0.88), not working (OR: 1.44; 95% CI: 1.23–1.68), lower yearly earnings (OR: 1.31; 95% CI: 1.07–1.60), poor health status (OR: 8.43; 95% CI: 6.76–10.51) and lack of health insurance coverage (OR for complete coverage vs incomplete coverage: 0.71; 95% CI: 0.55–0.93; Table 2).
Discussion
The current study evaluates the impact of gender and socioeconomic status on the rate of emergency department visits and subsequent hospitalization among a cohort of cancer survivors in the USA. It suggested that female cancer survivors were more likely to visit the emergency department; whereas, they were less likely to be subsequently hospitalized. Moreover, cancer survivors with lower socioeconomic status (represented by incomplete insurance coverage, unemployment and lower income) were more likely to visit emergency departments and more likely to be hospitalized because of this. Other factors associated with emergency department visits included poor health status, African American race and unmarried status.
Results from the current analysis add to a growing list of publications highlighting the impact of socioeconomic status on outcomes of cancer survivors. Prior studies suggested that cancer survivors with lower socioeconomic status are more likely to have worse cancer-specific outcomes and a higher risk of suicide [16–18]. The current study highlights the impact of socioeconomic status on health resource utilization including emergency department visits and hospitalizations. The link between socioeconomic status and emergency department visits might lie in gaps in insurance coverage which would limit access to routine care. Higher likelihood of emergency department visits might arise from lack of routine care which would increase the need for emergency services. A prior NHIS-based study evaluated the impact of high-deductible health plans with health savings account and it showed that health savings account was associated with less delayed care among high-deductible health plans cancer survivors (p < 0.05) [19]. Cancer diagnosis and treatment themselves can be explanatory factors for low socioeconomic status and lack of proper insurance coverage (e.g., through inability to return to work post-treatment because of disability) [20].
While there is no clear explanation for the observed gender-based differences, a number of hypotheses can be provided based on previously published data in the general public as well among cancer patients. Previous studies have suggested that women report more frequently physical symptoms potentially related to emotional distress (e.g., headache and back pain) compared with men; and this might have led to more emergency department visits that did not result subsequently in hospitalizations [21]. A prior Swedish unlike-sex twins’ study has also shown that while women had more total health conditions compared with men, there was no excess in life-threatening health conditions among women compared with men [22]. Another study based on 3.8 million patients in the UK, showed higher mean number of visits to the family physician (general practitioner in the UK) in females than males (aged 10–65 years) [23]. A prior qualitative synthesis of studies evaluating delays in cancer presentation suggested a reluctance on the side of men compared with women with regards to seeking help related to cancer symptoms [24]. A previously published study also suggested a higher probability of many nonlife-threatening adverse events among women with metastatic colorectal cancer compared with men without a difference in serious or fatal adverse events [25]. Another possible explanation for this observation is the higher likelihood for atypical presentations of some serious conditions (e.g., stroke or myocardial infarction) among women compared with men [26,27]. This might have (theoretically) led to a higher possibility of missing these diagnoses and; therefore, less hospitalizations. A third possible explanation might be related to the differential rates of different cancers among women versus men. This might have affected the potential short-term and long-term adverse events of cancer treatment that patients have experienced and subsequently their clinical course with regards to the need for emergency department visits and/or hospitalizations. A fourth possible explanation for gender-based differences might be related to differences in socioeconomic status between women and men. As clarified in the current study women were more likely to have lower income and insufficient insurance coverage. Both of these factors might be linked to less access to routine primary care; and subsequently, higher probability of emergency department visits. Consistent with this hypothesis is the reported reasons for emergency department visits among women versus men (Figure 3); 36.6% of women versus 32.8% of men went to the emergency department because ‘they did not have another place to go’. An important caveat for the interpretation of the current study also is the magnitude of reported ORs of gender-based differences (of 0.86 and 1.07). Although these are statistically significant findings, the differences seem to be modest given the large sample size of the study.
The current study is also in line with prior studies conducted in the noncancer population which suggested that incomplete health insurance coverage is associated with a higher probability of emergency department visits/hospitalizations [28,29]. Possible reasons for this observation would include the fact that incomplete health coverage is usually associated with delayed disease presentation, more advanced disease, less access to regular care and hence a higher probability of complications necessitating emergency management [30,31]. Individuals with no or limited coverage are also less likely to have a regular primary care provider. Looking at Figure 3 (which describes patient-attributed reasons for emergency department visits), ‘not having another place to go’ was the reason in a third of participants, this also highlights the potential link between lack of access to a regular care provider and frequent emergency department visits. Another potential reason is the prior observation that poorer Americans are more likely to have poorer health [32]. This means a higher probability for emergency department visits (even for reasons unrelated to cancer).
For uninsured US residents, part of the costs of emergency department visits/hospitalizations is paid as an out-of-pocket expense; but also part of the costs is being absorbed by other entities including some public and private institutions (that serve the uninsured at no/reduced charge); different levels of government (federal and state governments, that support hospitals’ operations); and donations from charities or philanthropic entities [33]. Thus, improving access of cancer survivors to elective insured health services (and possible subsequent decrease in the number of emergency department visits) is likely to be a cost-saving intervention as it will decrease the costs incurred by inpatient hospital care for cancer survivors. Taken together, these findings suggest that inadequate health coverage (and subsequent lack of access to regular providers) would not only worsen health outcomes but also economic outcomes (as hospital/inpatient care is generally more expensive than outpatient care). It is interesting also to note that individuals with private health insurance plans were less likely to visit the emergency department; while individuals with Medicaid coverage plans were more likely to visit the emergency department. This might indicate that not only the mere presence of coverage but also the type/quality of the coverage might be associated with emergency department visits.
It is important here also to highlight the long-term adverse effects, multiple different cancer treatments might have on cancer survivors (e.g., treatment-related cardiotoxicity) [34]. This may have played a role in the increased risk of all-cause hospitalization and/or emergency department visits. There is thus an important role for post-treatment survivorship care and transition back to primary care providers to monitor long-term cancer treatment adverse events and subsequent hospitalizations or emergency department visits.
The current study has several limitations and strengths that need to be recognized. First, information about cancer diagnosis as well as emergency department visits and subsequent hospitalizations was provided through self-reporting of included participants rather than through objective review of administrative records. This is coupled with the fact that NHIS datasets lack information about cancer stage or treatment(s) received. Although this is the nature of population-based surveys like NHIS, this would weaken the veracity of association analyses between socioeconomic status, gender and emergency department visits/hospitalizations. One also is not sure about the sensitivity/ specificity of self-reporting of cancer diagnosis in this setting. Second, NHIS datasets do not provide a distinction between an individual with cancer undergoing active therapy versus a cancer survivor who finished active treatment. This is particularly relevant in the context of assessment of reasons of emergency department visits and subsequent hospitalizations. Third, information about the general condition of the participants is provided through a self-reported health status variable and the medical reasons for emergency department visits/hospitalizations are not mentioned but only patient-reported reasons for emergency department visits were reported. It is possible that background medical conditions other than cancer were the reason for emergency department visits and this was not captured through NHIS datasets. This is compounded by the absence of information about standardized comorbidity indices (e.g., Charlson Comorbidity Index) within NHIS datasets. These limitations highlight the fact that the results of the current analysis indicate association rather than causation. On the other hand, the potential strengths of the current study included the large sample size of the study and the rigorous quality of NHIS datasets. Because of the unique nature of the healthcare system in the US, extrapolation of the results of the current analysis to other healthcare settings (e.g., in Canada or Europe) should be done with caution.
Conclusion
In conclusion and within the study cohort, female cancer survivors were more likely to visit the emergency department, whereas they were less likely to be subsequently hospitalized. Cancer survivors with lower socioeconomic status were more likely to visit emergency departments and more likely to be hospitalized because of this. Further work needs to be done to minimize disparity in access to cancer care services.
•
This study aimed to improve understanding of how gender and socioeconomic variables (including insurance status) can play a role in access to healthcare resources among cancer survivors in the USA.
•
Data from selected participants were reviewed from NHIS datasets (2011–2017), including (where applicable): age at survey completion, gender, race, marital status, working status, yearly earning, English language proficiency, educational level, self-reported health status, health insurance coverage in the past 12 months, type of insurance (private, Medicaid or Medicare) and primary site of cancer. Emergency department visits in the past 12 months, possible hospitalization after the most recent emergency department visit and patient-reported causes of emergency department visits were also collected.
•
The results suggested that female cancer survivors were more likely to visit the emergency department, whereas they were less likely to be subsequently hospitalized.
•
In addition, cancer survivors with lower socioeconomic status (represented by incomplete insurance coverage, unemployment and lower income) were more likely to visit emergency departments and more likely to be hospitalized because of this.
•
Other factors associated with emergency department visits included poor health status, African American race and unmarried status.
•
Results from the current analysis add to a growing list of publications highlighting the impact of socioeconomic status on outcomes of cancer survivors. Further work needs to be done to minimize disparity in access to cancer care services.
Acknowledgments
This work is based on the NHIS annual datasets (2011–2017).
Financial & competing interests disclosure
The author has received advisory board honoraria from Eisai Canada, Roche Canada and Lilly Canada. The author has no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The author state that he has followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
References
1.
Barbera L, Taylor C, Dudgeon D. Why do patients with cancer visit the emergency department near the end of life? CMAJ 182(6), 563–568 (2010).
2.
Alsirafy SA, Raheem AA, Al-Zahrani AS et al. Emergency department visits at the end of life of patients with terminal cancer: pattern, causes, and avoidability. Am. J. Hosp. Palliat. Care 33(7), 658–662 (2016).
3.
Prince RM, Powis M, Zer A, Atenafu EG, Krzyzanowska MK. Hospitalisations and emergency department visits in cancer patients receiving systemic therapy: systematic review and meta-analysis. Eur. J. Cancer Care 28(1), e12909 (2019).
4.
Abdel-Rahman O. Validation of the 8th AJCC prognostic staging system for breast cancer in a population-based setting. Breast Cancer Res. Treat. 168(1), 269–275 (2018).
5.
Zahedi A, Bondaz L, Rajaraman M et al. Risk for thyroid cancer recurrence is higher in men than in women independent of disease stage at presentation. Thyroid 30(6), 871–877 (2019).
6.
Hernando-Cubero J, Grande E, Castellano DE et al. Impact of gender on multikinase inhibitors (MKIs) toxicity in patients (pts) with advanced pancreatic and gastrointestinal neuroendocrine tumors (NETs): a pooled analysis of two Phase II trials with pazopanib and lenvatinib. J. Clin. Oncol. 37(Suppl. 15), 4109–4109 (2019).
7.
Kuhlthau KA, Nipp RD, Shui A et al. Health insurance coverage, care accessibility and affordability for adult survivors of childhood cancer: a cross-sectional study of a nationally representative database. J. Cancer Surviv. 10(6), 964–971 (2016).
8.
Nipp RD, Shui AM, Perez GK et al. Patterns in health care access and affordability among cancer survivors during implementation of the affordable care act. JAMA Oncol. 4(6), 791–797 (2018).
9.
Zheng Z, Han X, Zhao J et al. Financial hardship, healthcare utilization, and health among U.S. cancer survivors. Am. J. Prev. Med. 59(1), 68–78 (2020).
10.
Eskander A, Krzyzanowska MK, Fischer HD et al. Emergency department visits and unplanned hospitalizations in the treatment period for head and neck cancer patients treated with curative intent: a population-based analysis. Oral Oncol. 83, 107–114 (2018).
11.
Tang PL, Chang HT, Cheng CC et al. An analysis of emergency department visits and the survival rate for colorectal cancer patients: a Nationwide Population-Based study. Intern. Med. 56(16), 2125–2132 (2017).
13.
14.
Sloan C, Chandrasekhar R, Mitchel E, Schaffner W, Lindegren ML. Socioeconomic disparities and influenza hospitalizations, Tennessee, USA. Emerg. Infect. Dis. 21(9), 1602–1610 (2015).
15.
Perneger TV. What's wrong with Bonferroni adjustments. BMJ 316(7139), 1236–1238 (1998).
16.
Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population-based study. Cancer Epidemiol. 63, 101601 (2019).
17.
Abdel-Rahman O. Outcomes of nonmetastatic colon cancer patients in relationship to socioeconomic status: an analysis of SEER census tract-level socioeconomic database. Int. J. Clin. Oncol. 24(12), 1582–1587 (2019).
18.
Abdel-Rahman O. Impact of NCI socioeconomic index on the outcomes of nonmetastatic breast cancer patients: analysis of SEER census tract-level socioeconomic database. Clin. Breast Cancer 19(6), e717–e722 (2019).
19.
Zheng Z, Jemal A, Banegas MP, Han X, Yabroff KR. High-deductible health plans and cancer survivorship: what is the association with access to care and hospital emergency department use? J. Oncol. Pract. 15(11), e957–e968 (2019).
20.
De Boer AGEM, Taskila TK, Tamminga SJ, Feuerstein M, Frings-Dresen MHW, Verbeek JH. Interventions to enhance return-to-work for cancer patients. Cochrane Database Syst. Rev. 2015(9), CD007569 (2015).
21.
Piccinelli M, Simon G. Gender and cross-cultural differences in somatic symptoms associated with emotional distress. An international study in primary care. Psychol. Med. 27(2), 433–444 (1997).
22.
Gold CH, Malmberg B, Mcclearn GE, Pedersen NL, Berg S. Gender and health: a study of older unlike-sex twins. J. Gerontol. B Psychol. Sci. Soc. Sci. 57(3), S168–S176 (2002).
23.
Wang Y, Hunt K, Nazareth I, Freemantle N, Petersen I. Do men consult less than women? An analysis of routinely collected UK general practice data. BMJ Open 3(8), e003320 (2013).
24.
Smith LK, Pope C, Botha JL. Patients' help-seeking experiences and delay in cancer presentation: a qualitative synthesis. Lancet 366(9488), 825–831 (2005).
25.
Abdel-Rahman O. Impact of sex on chemotherapy toxicity and efficacy among patients with metastatic colorectal cancer: pooled analysis of 5 randomized trials. Clin. Colorectal Cancer 18(2), 110–115.e112 (2019).
26.
Ferry AV, Anand A, Strachan FE et al. Presenting symptoms in men and women diagnosed with myocardial infarction using sex-specific criteria. J. Am. Heart Assoc. 8(17), e012307 (2019).
27.
Keteepe-Arachi T, Sharma S. Preventing stroke and assessing risk in women. Practitioner 261(1802), 13–17 (2017).
28.
Gushue C, Miller R, Sheikh S et al. Gaps in health insurance coverage and emergency department use among children with asthma. J. Asthma 56(10), 1070–1078 (2019).
29.
Cooper WO, Arbogast PG, Hickson GB, Daugherty JR, Ray WA. Gaps in enrollment from a Medicaid managed care program: effects on emergency department visits and hospitalizations for children with asthma. Med. Care 43(7), 718–725 (2005).
30.
Cooper GS, Kou TD, Dor A, Koroukian SM, Schluchter MD. Cancer preventive services, socioeconomic status, and the affordable care act. Cancer 123(9), 1585–1589 (2017).
31.
Letourneau JM, Smith JF, Ebbel EE et al. Racial, socioeconomic, and demographic disparities in access to fertility preservation in young women diagnosed with cancer. Cancer 118(18), 4579–4588 (2012).
32.
Bor J, Cohen GH, Galea S. Population health in an era of rising income inequality: USA, 1980–2015. Lancet 389(10077), 1475–1490 (2017).
33.
Institute of Medicine (US) Committee on the Consequences of Uninsurance. Hidden costs, values lost: uninsurance in America. In: Spending on Health Care for Uninsured Americans: How Much, and Who Pays? National Academies Press, DC, USA (2003).
34.
Abdel-Rahman O. Risk of cardiac death among cancer survivors in the United States: a SEER database analysis. Expert Rev. Anticancer Ther. 17(9), 873–878 (2017).
Information & Authors
Information
Published In
Pages: 969 - 977
PubMed: 34156279
Copyright
© 2021 Future Medicine Ltd.
History
Received: 10 December 2020
Accepted: 28 May 2021
Published online: 22 June 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Gender, socioeconomic status and emergency department visits among cancer survivors in the USA: a population-based study. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0278
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ramya Walsan, Reema Harrison, Jeffrey Braithwaite, Deepak Bhonagiri, Michelle Moscova, Elizabeth Manias, Ashfaq Chauhan, Anita Vandyke, Natalie Taylor, Virginia Mumford, Prince Peprah, Rebecca Mitchell, Predictors of Unplanned Emergency Department Visits and Hospitalization Among Adults Accessing Virtual Outpatient Oncology Services in Queensland, Australia, Telemedicine and e-Health, 10.1177/15305627261440755, 32, 7, (692-700), (2026).
- Steven Clark Cunningham, Better together: a critical survey of conceptions of religious literacy and analysis of the implications for application to healthcare in the USA, Medical Humanities, 10.1136/medhum-2025-013480, (medhum-2025-013480), (2026).
- Astewle Andargie Baye, Gebre Kassaw Yirga, Yirgalem Abere, Mengistu Ewunetu, Yeshiambaw Eshetie, Birara Ayichew Tilaye, Gebrehiwot Berie Mekonnen, Epidemiology of oncologic emergency in Ethiopia: a systematic review and meta-analysis, BMC Emergency Medicine, 10.1186/s12873-025-01430-6, 26, 1, (2025).
- Ramya Walsan, Reema Harrison, Johanna Westbrook, Ashfaq Chauhan, Michelle Moscova, Anita Vandyke, Elizabeth Manias, Tracey Webster, Natalie Taylor, Prince Peprah, Rebecca Mitchell, Characteristics of Patients Accessing Outpatient Oncology Services Virtually and Predictors of Subsequent Unplanned Emergency Department Presentations: A Retrospective Cohort Study of 78,323 Adults in Australia (Preprint), Journal of Medical Internet Research, 10.2196/87694, (2025).
- Alexis L. Woods, Yueju Li, Theresa H. Keegan, Miriam Nuño, Claire E. Graves, Michael J. Campbell, Hypoparathyroidism After Total Thyroidectomy: A Population-Based Analysis of California Databases, Journal of Surgical Research, 10.1016/j.jss.2025.03.061, 310, (268-274), (2025).
- Justin W. Yan, Kristine Van Aarsen, Joe Thorne, Igor Karp, Tamara Spaic, Selina L. Liu, Nicolas Woods, Ian G. Stiell, A multicenter prospective cohort study evaluating 30-day outcomes after an emergency department visit for hyperglycemia in Canadian adults with type 1 or 2 diabetes, Canadian Journal of Emergency Medicine, 10.1007/s43678-025-00913-6, 27, 7, (551-558), (2025).
- Jeongyoon Moon, Ebram M. Salama, Anna Y. Wang, Mylène Arsenault, Nathalie Leon, Carmen G. Loiselle, Fateme Rajabiyazdi, Marylise Boutros, Lack of Regular Access to Primary Care Physician Associated With Increased Emergency Department Visits Related to Survivorship Needs Among Rectal Cancer Survivors, Diseases of the Colon & Rectum, 10.1097/DCR.0000000000003529, 67, 12, (1536-1543), (2024).
- Karen J. Wernli, Eric C. Haupt, Neetu Chawla, Thearis Osuji, Ernest Shen, Andrew B. Smitherman, Mallory Casperson, Anne C. Kirchhoff, Bradley J. Zebrack, Theresa H.M. Keegan, Lawrence Kushi, Christopher Baggett, Heydon K. Kaddas, Kathryn J. Ruddy, Candice A.M. Sauder, Theodore Wun, Marlaine Figueroa Gray, Jessica Chubak, Hazel Nichols, Erin E. Hahn, Emergency Department Use in Adolescent and Young Adult Cancer Early Survivors from 2006 to 2020, Journal of Adolescent and Young Adult Oncology, 10.1089/jayao.2023.0174, 13, 5, (738-747), (2024).
- Sima Vazquez, Chandler Berke, Victor M. Lu, Eva M. Wu, Michael A. Silva, Ankita Das, Sauson Soldozy, Jose F. Dominguez, Shelly Wang, Pediatric Patients with Intracranial Arteriovenous Malformations: Trends in Emergency Room Presentation, World Neurosurgery, 10.1016/j.wneu.2024.05.099, 188, (e297-e304), (2024).
- Shasank S. Swain, Sanjeeb K. Sahoo, Piperlongumine and its derivatives against cancer: A recent update and future prospective, Archiv der Pharmazie, 10.1002/ardp.202300768, 357, 7, (2024).
- See more