Effectiveness and safety of anti-TNF therapy for ankylosing spondylitis: a real-world study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate the effectiveness and safety of anti-TNF drugs for ankylosing spondylitis. Materials & methods: A prospective cohort study was performed at a pharmacy in the Brazilian Public Health System. Effectiveness by Bath Ankylosing Spondylitis Disease Activity Index, functionality by Health Assessment Questionnaire Disability Index, quality of life by European Quality of Life Five-Dimensions and safety was assessed at 6 and 12 months of follow-up. Results: About 160 patients started the treatment with adalimumab, etanercept or infliximab. There was a statistically significant improvement in disease activity, functionality and quality of life at 6 and 12 months (p < 0.05). Conclusion: This real-world study has shown that anti-TNF drugs are effective and well tolerated for ankylosing spondylitis patients.
Ankylosing Spondylitis (AS) is a chronic and immune-mediated inflammatory disease mainly featured by axial manifestations [1–4]. It presents higher prevalence in men and often starts between their second and third decades of life. AS incidence can range from 0.5 to 14 individuals per 100,000 inhabitants per year in different countries [1–3,5].
The Brazilian Public Health System (BPHS) provides treatment to AS patients based on a Clinical Protocol and Therapeutic Guideline [6,7]. Drug treatment comprises nonsteroidal anti-inflammatory drug (NSAIDs), glucocorticoids, conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), biological disease-modifying antirheumatic drugs (bDMARDs) and target-specific synthetic disease-modifying antirheumatic drugs. The bDMARDs avaliable by BPHS are the TNF inhibitors (anti-TNF) such as, adalimumab, etanercept, infliximab, golimumab and certolizumab, as well as the IL-17 inhibitor (anti-IL-17) known as secuquinumab [2,3,5,8–10].
The aims of the AS treatment are to reduce pain and inflammation, as well as to maintain spinal flexibility and normal posture in order to reduce functional limitations and complications, in addition to preserve patients’ work capacity and quality of life (QoL) [1,3,6]. Treatment effectiveness can be evaluated based on instruments capable of measuring disease activity, patients’ functionality level and QoL [3,6].
BPHS faces challenges due to increased costs with the incorporation of new health technologies, population aging and judicialization in health [11,12]. Thus, it is important for assessing the performance of different technologies (benefits, risks and costs) to enable better resource allocation, since budgets are finite and demands keep on increasing [11,12]. Therefore, information about the performance of this drugs in a real-world scenario can subsidize decision makers with focus in expand benefits for health, access and equity [11,12]. The objective of this study is to evaluate the disease activity, functionality, QoL and safety of patients treated with adalimumab, etanercept and infliximab for the treatment of AS in Brazil.
Materials & methods
Type of study
Open prospective cohort study was conducted at BPHS pharmacy in Minas Gerais State, Brazil. The cohort period was between August 2011 and June 2018.
Inclusion criteria
The study population consisted of patients aged 18 years or older, diagnosed with AS by the Assessment of Spondyloarthritis International Society (ASAS) classification criteria or the modified New York criteria [10,13] and treated with adalimumab, etanercept and infliximab in the recommended doses by the AS Clinical Protocol and Therapeutic Guideline.
Exclusion criteria
Patients treated with certolizumab and golimumab were not included because these drugs were incorporated into BPHS after the study started. Also, patients who refused to participate or were unable to attend the service were excluded.
Data collection & outcomes
Patients who had their treatment approved by BPHS were invited to participate. All those who agreed to participate signed a free and informed consent form. The date of the first bDMARD dispensation was defined as the first day of inclusion in the cohort.
Questionnaire for data collection was developed by the research group. The first interview focused on sociodemographic (age, sex, race, education, marital status) and clinical features (duration of disease, previous and current drugs). In addition, the following parameters were also measured in the beginning, 6 and 12 months: disease activity by Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), functionality by Health Assessment Questionnaire (HAQ), and QoL by European Quality of Life Five-dimension Questionnaire (EQ-5D). The safety was evaluated at 6 and 12 months.
BASDAI is a clinical disease activity index used to assess domains associated with fatigue, back pain, joint pain/swelling, enthesitic points, intensity and duration of morning stiffness. BASDAI score higher than or equal to, four means active disease. Response to treatment (clinical effectiveness) was observed when the patient reaches an improvement of BASDASI of ≥50% and/or absolute improvement of two units [3,10,14]. The factors associated with the best response by BASDAI was also investigated.
In addition, HAQ was used to assess patients’ functionality based on a self-administered questionnaire comprising 20 questions about the difficulty in performing daily activities [15], whereas EQ-5D was applied to investigate patients’ QoL based on a generic instrument used to analyze five dimensions, namely: mobility, personal care, usual activities, pain/discomfort and anxiety/depression. Visual analog scale was used to assess patients’ health condition [16].
Safety of anti-TNF drugs was measured through patients’ self-reports asking if there were any adverse drug reactions (ADR) with these drugs.
Statistical analyses
Frequency distributions were applied to categorical variables, whereas measures of central tendency and dispersion were applied to continuous variables.
Continuous variables were compared with each other through Student’s t-test, whereas categorical variables were assessed through Pearson’s Chi-square test (X2). Paired Student’s t-test was used to assess continuous variables (BASDAI, HAQ and EQ-5D) at 6 and 12 months, in comparison to the baseline.
Linear regression was performed to investigate factors associated with the best response to treatment by BASDAI [17]. BASDAI at 12 months was the dependent variable. Independent variables were sex, disease duration in years, race, education, marital status, use of NSAIDs, corticosteroids and csDMARDs, HAQ, EQ-5D and comorbidities at the beginning of follow-up. Variables presenting p < 0.20 in the simple analysis were included in the multiple analysis. Variables presenting p-value < 0.05 remained in the final model.
The R® software 3.6.1 (2019) (Vienna, Austria) was used for statistical analysis. The study was approved by the Research Ethics Committee of Federal University of Minas Gerais (COEP-UFMG) under n. 0069.0.203.000-11.
Results
One hundred and sixty patients started the treatment with some anti-TNF drug; of whom 127 (79,38%) and 113 (70,63%) completed 6 and 12 months of follow-up, respectively. The reasons to withdraw treatment in the first 6 months were described as follows: six patients presented therapeutic failure, five were not able to attend the pharmacy service, ten could not be contacted for interview scheduling, six presented ADR, two had their drug suspended by the doctor due to disease remission, two withdrew consent and one did not start the treatment. The reasons to withdraw treatment between 6 and 12 months were described as follows: five patients presented therapeutic failure, three were not able to attend the pharmacy service, two could not be contacted for interview scheduling, one ran out of drug, three withdrew consent and one presented ADR.
Patients’ mean age was 41.5 years (standard deviation [SD]: 11.9 years) and mean disease duration was 7.6 years (SD: 9.4 years). In addition, 59.4% of patients were male, 43.8% were white, 55.6% were married, 87.5% had 8 or more, years of education, 87.5% were bDMARD naive and 61.3% previously used csDMARDs. At the beginning of follow-up 57.5, 33.8, 31.3% were in use of NSAID, glucocorticoids and csDMARD, respectively.
Male had a longer period of disease duration and had a higher proportion of married patients. Female had worse BASDAI (including all domains), HAQ and EQ-5D, in addition to a higher proportion of them with some comorbidity when compared with male (p < 0.05). The other variables did not show statistically significant differences between groups (Table 1).
| Characteristics | Anti-TNF (n = 160) | Female (n = 65) | Male (n = 95) | p-value |
|---|---|---|---|---|
| Age in years – mean (SD) | 41.00 (11.91) | 40.4 (11.70) | 42.30 (12.10) | 0.061‡ |
| Education – n (%) | 0.081§ | |||
| – ≤8 years | 20 (12.5) | 11 (16.9) | 9 (9.5) | |
| – 9–11 years | 65 (40.6) | 20 (30.8) | 45 (47.4) | |
| – ≥12 years | 75 (46.9) | 34 (52.3) | 41 (43.1) | |
| Race n (%) | 1.000§ | |||
| – White | 70 (43.8) | 28 (43.1) | 42 (44.2) | |
| – No white | 90 (56.2) | 35 (53.8) | 53 (55.8) | |
| Marital status – n (%) | 0.014†,§ | |||
| – Not married | 54 (33.8) | 29 (44.6) | 25 (26.3) | |
| – Married | 89 (55.6) | 28 (43.1) | 61 (55.6) | |
| Disease duration in years – mean (SD) | 8 (9.4) | 6.35 (7.64) | 8.48 (10.3) | 0.011†,‡ |
| Previous drugs – n (%) | ||||
| – csDMARDs | 98 (61.3) | 41 (63.1) | 57 (60.0) | 0.543§ |
| – bDMARDs | 20 (12.5) | 10 (15.4) | 10 (10.5) | 0.503§ |
| Current drugs – n (%) | ||||
| – NSAID | 92 (57.5) | 40 (61.5) | 52 (54.7) | 0.489§ |
| – Corticosteroids | 54 (33.8) | 25 (38.5) | 29 (30.5) | 0.383§ |
| – csDMARDs | 50 (31.3) | 22 (33.9) | 28 (29.5) | 0.680§ |
| Clinical Measures – mean (SD) | ||||
| – HAQ | 1.15 (0.66) | 1.29 (0.68) | 1.06 (0.63) | 0.003†,‡ |
| – EQ-5D | 0.60 (2.38) | 0.57 (0.20) | 0.63 (0.18) | 0.040†,‡ |
| – VAS | 60.73 (20.39) | 59.40 (20.70) | 61.60 (20.30) | 0.055‡ |
| – BASDAI | 5.44 (2.38) | 5.97 (2.54) | 5.07 (2.21) | 0.011†,‡ |
| – Fatigue | 5.23 (2.90) | 6.03 (2.74) | 4.70 (2.90) | 0.008†,‡ |
| – Axial pain | 6.54 (2.89) | 7.06 (2.82) | 6.19 (2.90) | 0.014†,‡ |
| – Peripheral pain | 4.27 (3.20) | 4.29 (3.62) | 4.25 (2.91) | 0.003†,‡ |
| – Entesite | 5.81 (3.21) | 6.56 (3.23) | 5.31 (3.10) | 0.009†,‡ |
| – Morning stiffness¶ | 5.37 (2.92) | 5.68 (3.09) | 5.16 (2.80) | 0.007†,‡ |
| Comorbidity – n (%) | 30 (18.8) | 43 (66.2) | 40 (40.8) | 0.005†,§ |
†
p-value < 0.05.
‡
Independent Student t-test;
§
Chi-square test;
¶
Morning stiffness: Arithmetic average morning stiffness and duration of morning stiffness.
BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; bDMARD: biologic disease-modifying antirheumatic; csDMARD: Conventional synthetic disease-modifying antirheumatic drugs; EQ-5D: European Quality of Life five dimensions; HAQ: Health Assessment Questionnaire; n: sample size; SD: Standard deviation; VAS: Visual analog scale.
Follow-up at 6 & 12 months
There was statistically significant improvement in disease activity, with a reduction in mean BASDAI at 6 and 12 months (p < 0.05; Table 2). All BASDAI domains have shown statistically significant differences at 6 and 12 months, in comparison with the beginning of follow-up (p < 0.05). Morning stiffness, enthesitis and axial pain were the domains showing the greatest reduction in mean values due to anti-TNF using (Figure 1). In addition, 74 (57.8%) and 63 (55.8%) patients achieved the clinical effectiveness by BASDAI at 6 and 12 months, respectively.
| Clinical features | Baseline | 6 months (n = 127) | p-value‡ | 12 months (n = 113) | p-value§ |
|---|---|---|---|---|---|
| Mean (SD) | |||||
| BASDAI | 5.43 (2.38) | 3.18 (2.48) | <0.0001† | 3.20 (2.55) | <0.0001† |
| HAQ | 1.15 (0.66) | 0.69 (0.61) | <0.0001† | 0.68 (0.60) | <0.0001† |
| EQ-5D | 0.60 (0.19) | 0.73 (0.21) | <0.0001† | 0.74 (0.19) | <0.0001† |
| VAS | 60.73 (20.40) | 73.87 (18.87) | <0.0001† | 75.52 (18.28) | <0.0001† |
†
p-value < 0.05.
‡
Comparison between baseline and 6 months by paired Student t-test.
§
Comparison between baseline and 12 months by paired Student t-test.
BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; EQ-5D: European Quality of Life five dimensions; HAQ: Health Assessment Questionnaire; SD: Standard deviation; VAS: Visual analog scale.
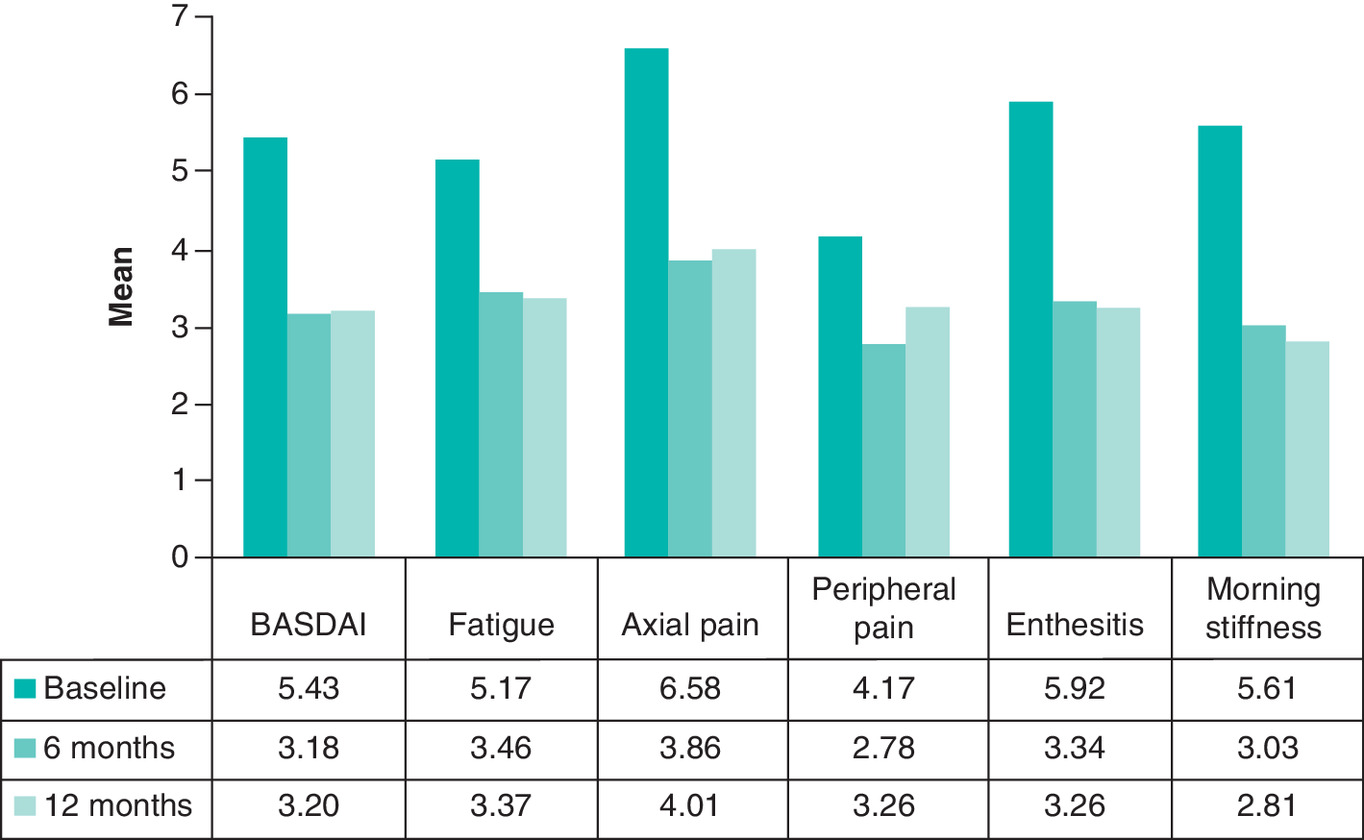
Figure 1. Mean Bath Ankylosing Spondylitis Disease Activity Index domains – baseline, 6 and 12 months.
BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; Morning stiffness: Arithmetic average of morning stiffness and morning stiffness duration.
Also, there was statistically significant improvement in functionality and QoL, with a reduction in mean HAQ values and an increase in mean EQ-5D values at 6 and 12 months (p < 0.05; Table 2).
Moreover, 154 and 156 ADR were reported by 83 (65.4%) and 68 (60.2%) patients at 6 and 12 months of follow-up, respectively. The most common ones comprised headaches, reactions at the application site, flu-like symptoms, asthenia, alopecia and upper respiratory infection. (Table 3).
| Adverse drug event, n (%) | 6 months (n = 128) | 12 months (n = 113) | ||||||
|---|---|---|---|---|---|---|---|---|
| All (128) | Adalimumab (97) | Etanercept (23) | Infliximab (8) | All (113) | Adalimumab (85) | Etanercept (21) | Infliximab (7) | |
| Headaches | 25 (19.5) | 19 (19.6) | 5 (21.7) | 1 (12.5) | 19 (16.8) | 17 (20.0) | 2 (6.5) | 0 |
| Application site reactions | 19 (15.1) | 14 (14.6) | 5 (21.7) | 0 | 13 (11.5) | 11 (12.9) | 2 (9.5) | 0 |
| Alopecia | 15 (11.7) | 13 (13.4) | 2 (8.7) | 0 | 12 (0.1) | 10 (0.1) | 1 (0.05) | 1 (14.3) |
| Flu symptoms | 15 (11.7) | 14 (14.4) | 1 (4.4) | 0 | 25 (22.1) | 19 (22,5) | 5 (23.8) | 1 (14.3) |
| Asthenia | 15 (11.7) | 15 (15.5) | 0 | 0 | 9 (8.0) | 9 (10.6) | 0 | 0 |
| Upper respiratory infection | 11 (8.7) | 10 (10.4) | 1 (4.4) | 0 | 12 (0.1) | 12 (0.1) | 0 | 0 |
n: Sample size.
Predictors of effectiveness measured by BASDAI
Factors associated with the best response to treatment based on BASDAI at 12 months comprised not using concomitant corticosteroids, not having comorbidities and better QoL at the beginning of follow-up (Table 4).
| Baseline characteristics | SIMPLE | MULTIPLE† | ||||
|---|---|---|---|---|---|---|
| β co-efficient | CI 95% | p-value | β co-efficient | CI 95% | p-value | |
| Female sex | 1.02 | (0.062; 1.971) | 0.037 | |||
| Corticosteroid use | 1.22 | (0.238; 2.202) | 0.015 | 1.012 | (0.16; 1.87) | 0.021 |
| NSAID use | 0.96 | (0.016; 1.910) | 0.046 | |||
| Comorbidity | 1.83 | (0.935; 2.714) | <0.0001 | 1.242 | (0.40; 2.09) | 0.004 |
| Disease duration in years | -0.043 | (-0.092; 0.006) | 0.085 | |||
| HAQ | 1.69 | (1.006; 2.372) | <0.0001 | |||
| EQ | -6.71 | (-9.066; -4.345) | <0.0001 | -5.279 | (-7.67; -2.89) | <0.001 |
†
Multiple R2 adjusted = 0.2869.
EQ-5D: European Quality of Life five dimensions; HAQ: Health Assessment Questionnaire; NSAID: Nonsteroidal anti-inflammatory drug.
Discussion
The current study has outlined the profile of patients with AS and evaluated disease activity, functionality, QoL and safety in anti-TNF drug using at 6 and 12 months of follow-up.
The profile of AS patients was similar to the studies available in the literature [17–22]. However, the proportion of male patients in the present study was lower than that of other studies [1–3,17–22]. This finding can be hypothetically explained by the type of patient selection (convenience sampling) adopted in the present study. Therefore, patients should agree to participate in the research and attend the health service to be included in the study. According to the National Household Sampling Survey [23,24], most ‘economically active’ and ‘employed’ groups living in the Brazilian Southeastern region comprised male individuals [23,24].
Women presented shorter disease duration and worse clinical results for HAQ, EQ-5D, BASDAI. In addition, they presented larger number of comorbidities at the beginning of follow-up. This result was also observed in the literature [25,26], except for disease duration, which was longer in women [26]. A possible hypothesis for these findings found by other authors is associated with a later diagnosis, due to less radiological progression that can lead to greater disease activity and less efficacy/treatment effectiveness [15,25].
Observational studies have also found significant improvement in AS patients treated with anti-TNF drugs, who presented a statistically significant reduction in disease activity by BASDAI [3,4,6,17,25], as well as a statistically significant improvement in functionality by HAQ [3,4,6,26] and QoL by EQ-5D [3,4,6,27]. Therefore, anti-TNF drugs play an important role in AS treatment.
Approximately 60% of patients reached the response to treatment by BASDAI (2 points or 50% improvement). This result was similar to a British study that evaluated AS patients through a Rheumatology Biologics Register that found 52% of treatment response [17]. However, another study reported that 31.2% of patients achieved the treatment response [22]. These differences can be explained by the characteristics of the patients among the studies such articular manifestations and previous use of biological drugs.
Given the high cost of bDMARD for BPHS (in comparison with csDMARD) and, consequently, for society, multidisciplinary teams can perform continuous pharmacotherapeutic monitoring of patients who did not achieve the expected response to treatment. According to LIANG and collaborators (2019), multidisciplinary team performance helps improving clinical results of AS patients [28].
Factors associated with the best response to treatment by BASDAI comprised not using corticosteroids, not having comorbidities and better QoL by EQ-5D at the beginning of follow-up. Patients using corticosteroids at the beginning of follow-up had worse prognosis and greater difficulty in controlling the disease activity [26], a fact that may explain the worst response to treatment. Wailoo and collaborators (2015) have found linear correlation between EQ-5D and BASDAI, which means that as BASDAI decreases, the likelihood of better QoL increases [26,29] – this outcome corroborates findings in the current study. Some authors have found a greater loss of productivity and greater disease activity in patients with comorbidities, especially psychopathological conditions, uveitis and intestinal diseases. Further studies would be needed to prove this relationship, but this increased activity may be an explanation for worse effectiveness [26,29].
The main adverse drug events were headache, flu-like symptoms, upper respiratory tract infection and reaction at the application site, similar to the findings of studies available in the literature [8,9,30,31]. Another study demonstrated that there was no statistically significant difference between treatment with or without anti-TNF and the main reactions were upper respiratory tract infection and opportunistic herpes simplex infection [8]. A systematic review evaluated the risk of infections in patients treated with anti-TNF and observed a statistically significant increase in the occurrence of any infections (20%), serious infections (40%) and tuberculosis (250%) [31]. However, in this study, no cases of tuberculosis and herpes were reported.
Study limitations
The current study was carried out during daily drug dispensing at BPHS and it did not enable controlling some biases. It was a nonrandomized study without control group and the anti-TNF drugs were administered according to rheumatologists’ prescriptions. However, it reflects the reality of real-world studies conducted with BPHS patients. Patients with a poor prognosis may not have been followed due to the difficulty to attend the service. The authors are also aware of the relatively small number of patients participating in this real-world study. BASDAI is a measure that evaluates the patients’ disease activity in important aspects of the AS disease that affects the functionality and QoL. So HAQ and EQ-5d complements the results of BASDAI because they are multidimensional measures reported by patients, being especially important to assess the patient globally. In addition, this study brings the need for further studies and especially reflections on policies aimed at women and access to these drugs.
Conclusion
Anti-TNF drugs were effective in AS patients, since it reduced disease activity, as well as improved patients’ functionality and QoL. In addition, they were well tolerated by the investigated patients. Therefore, it is possible saying that these drugs play an important role in AS treatment.
About 40% of patients did not show the response to treatment based on BASDAI (2 points or 50% improvement). In these cases, a multidisciplinary team could work together with rheumatologists to identify the main reasons for treatment failure and, consequently, to help improve patients’ clinical outcomes.
Not using corticosteroids, not having comorbidities and presenting better QoL at the beginning of follow-up were factors associated with the best response to treatment by BASDAI.
Future perspective
In the era of biosimilars, further studies will be carried out to compare the effectiveness and safety of these drugs with the current biological drugs supplied by BPHS.
•
One hundred and sixty patients started the treatment with some anti-TNF drug.
•
Male had a longer period of disease duration and had a higher proportion of married patients than female.
•
Female had worse Bath Ankylosing Spondylitis Disease Activity Index, Health Assessment Questionnaire and European Quality of Life Five-dimension Questionnaire, in addition to a higher proportion of them with some comorbidity when compared with male (p < 0.05).
•
There was a statistically significant improvement in disease activity, functionality and quality of life at 6 and 12 months (p < 0.05).
•
The most common adverse drug reactions were headaches, application site reactions, flu-like symptoms, asthenia, alopecia and upper respiratory infection.
•
Anti-TNF were well tolerated.
•
Better response by BASDAI was associated with the absence of comorbidities, absence of treatment with corticosteroids and better quality of life at the beginning of treatment.
•
A multidisciplinary team could work together with rheumatologists to identify the main reasons for treatment discontinuation and, consequently, to help improving patients’ clinical outcomes.
Author contributions
PRK Pimenta and JBR dos Santos were involved in the drafting of the paper. AM Kakehasi, FA Acurcio and J Alvares-Teodoro were involved in the conception and design of the study. PRK Pimenta, MRR da Silva and JBR dos Santos were involved in the collection and interpretation of the data. PRK Pimenta and MRR da Silva were involved in the analyses of the data. All authors revising the paper critically for intellectual content and agreed to be accountable for all aspects of the work.
Acknowledgments
PRK Pimenta, MRR da Silva and JBR dos Santos thank the Coordination of Improvement of Higher Education Personnel for granting post-doctorate scholarships.
Financial & competing interests disclosure
This work was supported by the National Council for Scientific and Technological Development – CNPq (grant number: 471819/2013-1) and the Minas Gerais Research Support Foundation – FAPEMIG (grant numbers: PPM-0015-15 and 03799-16). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors have obtained appropriate institutional review board approval and an informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Braun J, Sieper J. Ankylosing spondylitis. Lancet 369(9570), 1379–1390 (2007).
• Explains about clinical manifestations, epidemiology and treatment of ankylosing spondylitis (AS).
2.
Duba AS, Mathew SD. The seronegative spondyloarthropathies. Prim. Care 45(2), 271–287 (2018).
3.
Ward MM, Deodhar A, Akl EA et al. American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network 2015 recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Rheumatol. 68(2), 282–298 (2016).
• An international guideline for the treatment of AS.
4.
Ajmani S, Keshri A, Srivastava R, Aggarwal A, Lawrence A. Hearing loss in ankylosing spondylitis. Int. J. Rheum. Dis. 22(7), 1202–1208 (2019).
5.
Machado NP, Nogueira E, Oseki K et al. Clinical characteristics and frequency of TLR4 polymorphisms in Brazilian patients with ankylosing spondylitis. Rev. Bras. Reumatol. Engl. Ed. 56(5), 432–440 (2016).
6.
Sampaio-Barros PD, Valderílio FA, Bonfiglioli R et al. First update on the Brazilian consensus for the diagnosis and treatment of spondyloarthropathies: ankylosing spondylitis and psoriatic arthritis. Rev. Bras. Reumatol. 47(4), 233–242 (2007).
7.
BRAZIL. Specialized component of pharmaceutical assistance (CEAF). Pharmaceutical Assistance Ministry of Health, Brasília, Brazil (2019). www.saude.gov.br/assistencia-farmaceutica/medicamentos-rename/componente-especializado-da-assistencia-farmaceutica-ceaf
•• Brazilian law that regulates the dispensing and monitoring of high-cost drugs. Brazilian guideline for AS (inclusion criteria, diagnosis criteria and treatment).
8.
Wroński J, Fiedor P, Głuszko P. Adverse events in patients with ankylosing spondylitis treated with TNF inhibitors: a cross-sectional study. Int. J. Clin. Pharm. 41(4), 864–871 (2019).
9.
Ma Z, Liu X, Xu Xe et al. Safety of tumor necrosis factor-alpha inhibitors for treatment of ankylosing spondylitis: ameta-analysis. Medicine (Baltimore) 96(25), e7145 (2017).
•• Meta-analysis about safety of anti-TNF therapy for AS.
10.
BRAZIL. Joint ordinance n°25 / 2018. Approves the clinical protocol and therapeutic guidelines for ankylosing spondylitis. In: Secretariat of Science, Technology and Strategic Inputs and Secretariat of Health Care, [2018]. DF: Ministry of Health, Brasília, Brazik (2018). http://portalarquivos2.saude.gov.br/images/pdf/2019/abril/29/Portaria-Conjunta-n--25---PCDT-espondilite-ancilosante.29.04.2019.pdf
11.
Elias FTS. A Importância da Avaliação de Tecnologias para o Sistema Único de Saúde. BIS 14(2), 143–150 (2013).
12.
Elias FTS. A importância da avaliação de tecnologias para o sistema único de saúde. BIS 14(2), 143–150 (2013).
13.
Rudwaleit M, van der Heijde D, Landewé R et al. The development of Assessment of Spondyloarthritis International Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann. Rheum. Dis. 68(6), 777–783 (2009).
14.
Shinjo SK, Gonçalves R, Kowalski S, Gonçalves CR. Brazilian-Portuguese version of the Health Assessment Questionnaire for Spondyloarthropathies (HAQ-S) in patients with ankylosing spondylitis: a translation, cross-cultural adaptation, and validation. Clin. Rheumatol. 26(8), 1254–1258 (2007).
15.
Fitzgerald G, Gallagher P, O'SHEA F. Multimorbidity is common in axial spondyloarthropathy and is associated with worse disease outcomes: results from the ASRI cohort. J. Rheum. 47(2), 218–226 (2019).
16.
Nucleus of evaluation and technology in health-nats inc. Qaly Brazil. National Institute of Cardiology (2019). http://natsinc.org/wpress/euroqol/?page_id=767
17.
Lord PA, Farragher TM, Lunt M et al. BSR Biologics register. Predictors of response to anti-TNF therapy in ankylosing spondylitis: results from the British Society for Rheumatology Biologics Register. Rheumatology (Oxford) 49(3), 563–570 (2010).
18.
Machado MA, Moura CS, Ferré F, Bernatsky S, Rahme E, Acurcio Fde A. Treatment persistence in patients with rheumatoid arthritis and ankylosing spondylitis. Rev. Saude Publica 22, 50 (2016).
19.
Machado NP, Nogueira E, Oseki K et al. Clinical characteristics and frequency of TLR4 polymorphisms in Brazilian patients with ankylosing spondylitis. Rev. Bras. Reumatol. Engl. Ed. 56(5), 432–440 (2016).
20.
Acurcio FA, Guerra Junior AA, da Silva MRR et al. Comparative persistence of anti-tumor necrosis factor therapy in ankylosing spondylitis patients: a multicenter international study. Curr. Med. Res. Opin. 36(4), 677–686 (2020).
21.
Callhoff J, Sieper J, Weiß A, Zink A, Listing J. Efficacy of TNFα blockers in patients with ankylosing spondylitis and non-radiographic axial spondyloarthritis: a meta-analysis. Ann. Rheum. Dis. 74(6), 1241–1248 (2015).
22.
Lubrano E, Parsons WJ, Perrotta FM. Assessment of response to treatment, remission, and minimal disease activity in axial psoriatic arthritis treated with tumor necrosis factor inhibitors. J. Rheumatol. 43(5), 918–923 (2016).
23.
BRAZIL. National Household Sample Survey-PNAD. IBGE Brazilian Institute of Geography and Statistics, Brasília, Brazil (2020). www.ibge.gov.br/estatisticas/sociais/educacao/9127-pesquisa-nacional-por-amostra-de-domicilios.html?=&t=o-que-e
24.
BRAZIL. National Household Sample Survey-PNAD. IBGE Brazilian Institute of Geography and Statistics, Brasília, Brazil (2020). https://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia-de-noticias/releases/18992-pnad-continua-2016-51-da-populacao-com-25-anos-ou-mais-do-brasil-possessed-at-maximum-the-complete-elementary-education-access
25.
Rusman T, van Vollenhoven RF, van der Horst-Bruinsma IE. Gender differences in axial spondyloarthritis: women are not so lucky. Curr. Rheumatol. Rep. 20(6), 35 (2018).
26.
Stolwijk C, Boonen A, van Tubergen A, Reveille JD. Epidemiology of spondyloarthritis. Rheum. Dis. Clin. North Am. 38(3), 441–476 (2012).
27.
Escudero-Vilaplana V, Ramírez-Herráiz E, Alañón-Plaza E et al. Efficiency of adalimumab, etanercept and infliximab in ankylosing spondylitis in clinical practice. Int. J. Clin. Pharm. 37(5), 808–814 (2015).
• Verifies worse results for women than men in axial spondyloarthritis.
28.
Liang L, Pan Y, Wu D, Pang Y, Xie Y, Fang H. Effects of multidisciplinary team-based nurse-led transitional care on clinical outcomes and quality of life in patients with ankylosing spondylitis. Asian Nursing Research 13(2), 107–114 (2019).
29.
Wailoo A, Hernández M, Philips C, Brophy S, Siebert S. Modeling health state utility values in ankylosing spondylitis: comparisons of direct and indirect methods. Value Health 18(4), 425–431 (2015).
30.
Zeren M, Xiaoping L, Xiaosheng X et al. Safety of tumor necrosis factor-alpha inhibitors for treatment of ankylosing spondylitis: a meta-analysis. Medicine (Baltimore) 96, 25 (2017).
31.
Minozzi S, Bonovas S, Lytras T et al. Risk of infections using anti-TNF agents in rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis: a systematic review and meta-analysis. Expert Opin. Drug Saf. 15(Suppl. 1), 11–34 (2016).
Information & Authors
Information
Published In
Pages: 509 - 517
PubMed: 33728937
Copyright
© 2021 Future Medicine Ltd.
History
Received: 9 December 2020
Accepted: 5 February 2021
Published online: 17 March 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Effectiveness and safety of anti-TNF therapy for ankylosing spondylitis: a real-world study. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0275
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Y. A. Levashova, A. M. Aibatirov, G. A. Makarov, M. A. Beradze, D. D. Khamdamov, EFFECTIVENESS OF ANTI-CYTOKINE THERAPY IN AUTOIMMUNE DISEASES, Bulletin of Pirogov National Medical & Surgical Center, 10.25881/20728255_2026_21_1_139, 21, 1, (139-145), (2026).
- Bárbara Rodrigues Alvernaz dos Santos, Gerusa Araújo de Oliveira, Jessica Barreto Ribeiro dos Santos, Augusto Afonso Guerra Junior, Francisco de Assis Acurcio, Juliana Alvares-Teodoro, Avaliação do desempenho de medicamentos biológicos no tratamento da espondilite anquilosante: estudo de coorte, Minas Gerais, 2018-2023, Epidemiologia e Serviços de Saúde, 10.1590/s2237-96222025v34e20240116.pt, 34, (2025).
- Bárbara Rodrigues Alvernaz dos Santos, Gerusa Araújo de Oliveira, Jessica Barreto Ribeiro dos Santos, Augusto Afonso Guerra Junior, Francisco de Assis Acurcio, Juliana Alvares-Teodoro, Evaluation of the performance of biological drugs in the treatment of ankylosing spondylitis: cohort study, Minas Gerais, 2018-2023, Epidemiologia e Serviços de Saúde, 10.1590/s2237-96222025v34e20240116.en, 34, (2025).
- Zhumin Sun, Yang Zhang, Haiyan Zhou, Jingyun Li, Yue Zhou, Liyun Wang, Serum interα-trypsin inhibitor heavy chain H4 may be an anti-inflammatory marker reflecting disease risk, activity and treatment outcome of ankylosing spondylitis, Scandinavian Journal of Clinical and Laboratory Investigation, 10.1080/00365513.2023.2250986, 83, 8, (540-547), (2023).
- Jie Yuan, Lei Xiang, Feng Wang, Lin Zhang, Gaozhan Liu, Xiuli Chang, Anbing Zhang, Ying Tao, MALT1 positively relates to Th17 cells, inflammation/activity degree, and its decrement along with treatment reflects TNF inhibitor response in ankylosing spondylitis patients, Journal of Clinical Laboratory Analysis, 10.1002/jcla.24472, 36, 7, (2022).
- Felipe A. Moraes, Michael R.R. da Silva, Jéssica B.R. dos Santos, Francisco A. Acurcio, Alessandra M. Almeida, Adriana M. Kakehasi, Juliana Alvares-Teodoro, Health-Related Quality of Life in Psoriatic Arthritis: Findings and Implications, Value in Health Regional Issues, 10.1016/j.vhri.2021.06.003, 26, (135-141), (2021).