Dacomitinib in first-line treatment of advanced EGFR-mutated non-small-cell lung cancer: a cost–effectiveness analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the cost–effectiveness of first-line treatment with dacomitinib compared with gefitinib in patients newly diagnosed with advanced NSCLC EGFR-positive in the context of Spain. Materials & methods: A partitioned survival model was developed including costs, utilities and disutilities to estimate quality-adjusted life-year (QALY) and incremental cost–effectiveness ratio when treating with dacomitinib versus gefitinib. Results: Dacomitinib presented higher QALYs (0.51) compared with gefitinib (0.45). Dacomitinib costs were €33,061 in comparison with €26,692 for gefitinib arm. An incremental cost–effectiveness ratio of €111,048 was obtained for dacomitinib. Conclusion: Dacomitinib was more effective in terms of QALYs gained than gefitinib. However, to obtain a cost–effectiveness alternative, a discount greater than 25% in dacomitinib acquisition cost is required.
Lay abstract
EGFR tyrosine kinase inhibitors represent the standard of care in patients with EGFR mutation-positive (EGFRm+) non-small-cell lung cancer. The introduction of new oncology therapies can result in financial pressure for healthcare payers. Therefore, the development of a cost–effectiveness study for assessing the gains in health relative to the costs of different health interventions is required. In this study, we compare dacomitinib with gefitinib as first-line treatment from a Spanish National Health System perspective, by estimating how much it costs to gain a unit of a health outcome, like a life year gained or quality-adjusted life-year. Dacomitinib has been proved not to be a cost-effective alternative because despite being more effective in terms of life year gained or quality-adjusted life-year than gefitinib, it was also much more expensive due to the high acquisition cost of dacomitinib.
Lung cancer is the most common cancer and the most frequent cause of cancer death worldwide [1]. In terms of histology, non-small-cell lung cancer (NSCLC), being diagnosed in 80–85% of cases, is the most widespread type of lung cancer [2]. EGFR mutations are reported to be associated in approximately 14–19% of Western patients and 40–48% of Asian patients with NSCLC with adenocarcinoma [3,4]. In Spain, the REASON study revealed that the mutation detection rate in advanced NSCLC patients was found to be 11.6% (17.4% presenting L858R mutation in exon 21 and 82.6% presenting in-frame deletions in exon 19) [5].
EGFR tyrosine kinase inhibitors (TKIs) are the standard treatment for patients with NSCLC harboring an EGFR mutation [6]. To date, three first-line TKIs are normally used in clinical practice: erlotinib, gefitinib and afatinib. These TKIs have demonstrated significantly improved progression-free survival (PFS) as the first-line treatment compared with platinum-based therapy [7–14].
Recently, based on the ARCHER 1050 study [15], the US FDA approved dacomitinib, a second-generation EGFR-TKI, for the first-line treatment of patients with metastatic NSCLC with EGFR mutation-positive [16]. This study showed that dacomitinib was superior to gefitinib in terms of PFS and overall survival (OS). A seven-month improvement in OS was shown in the dacomitinib arm compared with gefitinib [17]. Nonetheless, second-generation EGFR TKIs are frequently associated with EGFR-mediated toxicities due to the relatively potent EGFR inhibition. Therefore, in the ARCHER 1050 study, a dose reduction was performed on the dacomitinib arm. Additionally, in another study, tolerability guided dose modifications enabled patients to continue with dacomitinib and benefit from PFS and OS improvement [18].
Although dacomitinib caused more side effects than gefitinib, these were considered manageable. Therefore, on April 2019, the EMA decided that the benefits of dacomitinib are greater than its risks, and it was authorized for use in the European Union. Consequently, dacomitinib could be considered one of the standard first-line options for patients with advanced EGFR-mutated NSCLC. Additionally, a new network meta-analysis comparing OS have demonstrated that treatment with dacomitinib could be considered a first-line treatment option in comparison with other standard EGFR TKIs as afatinib (hazard ratio [HR] 0.87; 95% CI: 0.61–1.24), erlotinib (HR: 0.79; 95% CI: 0.44–1.42), gefitinib (HR: 0.75; 95% CI: 0.59–0.95) and osimertinib (HR: 0.94; 95% CI: 0.68–1.29) [19].
To our knowledge, no prior incremental cost–effectiveness analysis (ICER) has been performed comparing dacomitinib versus gefitinib in Spain. This study aims to evaluate the cost–effectiveness of first-line treatment with dacomitinib compared with gefitinib in patients newly diagnosed with advanced NSCLC EGFR-positive in the context of Spain. Our study could help clinicians and policymakers in the decision-making process to promote the sustainability of the Spanish National Health System.
Material & methods
Cost–effectiveness analysis: partitioned survival model
Design & perspective analysis
A partitioned survival model model was constructed using clinical data from the ARCHER 1050 randomized study [15]. The quality-adjusted life-years (QALYs), the costs, and ICER of two different treatment strategies (dacomitinib vs gefitinib) were estimated in two hypothetical cohorts of patients with newly diagnosed advanced NSCLC and one EGFR mutation (exon 19 or Leu858Arg). We modeled the health states of patients with similar criteria to those enrolled in the ARCHER 1050 study: patients in IIIB/IV stage, with new or recurrent diagnosis, and histological or cytopathological confirmation. The presence of at least one documented EGFR mutation (exon 19 deletion or the Leu858Arg mutation, with or without the Thr790Met mutation) was required. The model was developed from the perspective of the Spanish National Health System. The threshold for determining the cost–effectiveness of a strategy was €24,000/QALY [20]. All the costs were estimated in euros (€) 2019, and a discount rate of 3% was used for costs and effects throughout the model. The partitioned survival model was developed in Microsoft Excel 2011 (Microsoft Corp., WA, USA) using a 15-year time horizon, which was selected because it was sufficient to collect all the costs and benefits generated in the model. The results were presented in terms of costs (€), QALYs gained and ICER.
Partitioned survival model structure
The model included three mutually exclusive health states: stable disease, progressive disease and death. As shown in Figure 1, all patients were initially on stable disease and received one of the two treatment strategies (dacomitinib or gefitinib). On each 28-day simulation cycle, the model redistributes the hypothetical cohort of patients among the three health states according to the transition probabilities. On progressive disease, the patients received a second-line regimen, and after the occurrence of progressive disease, they could remain in this state or die. Progressive disease was simulated until all the patients died. A half-cycle correction was applied.
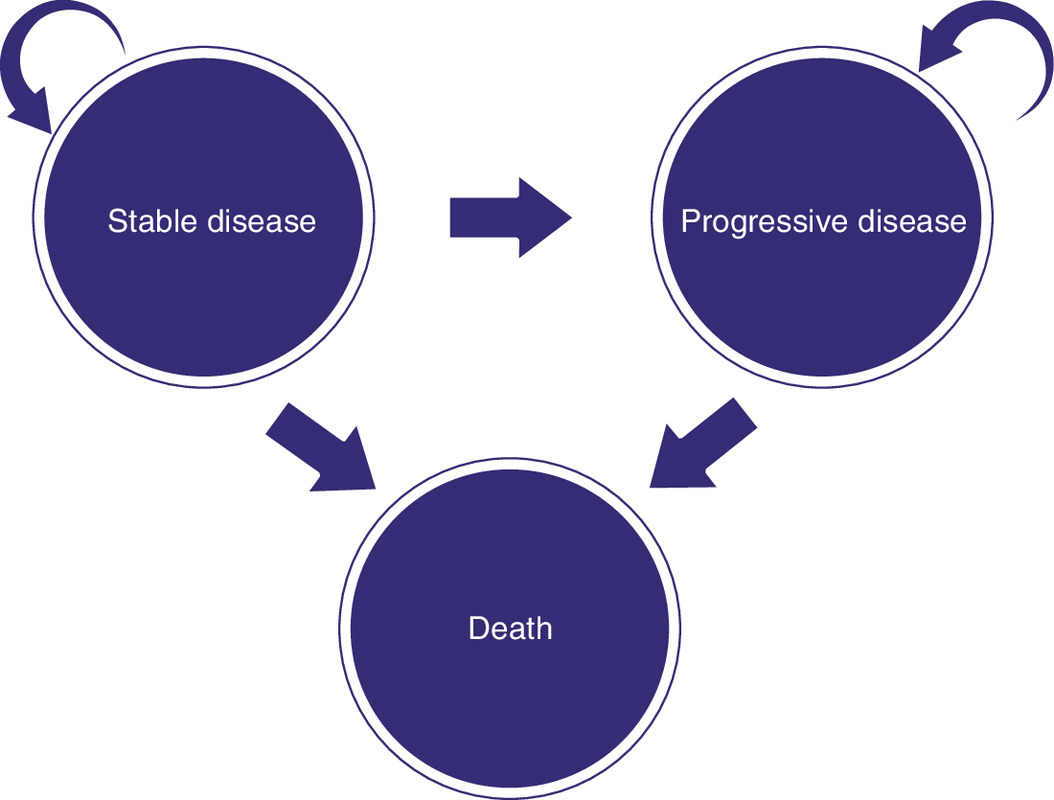
Figure 1. Structure of the partitioned survival model.
Partitioned survival model health states.
Treatment alternatives
The model cycle length was 28 days (4 weeks), consistent with the labeled dose frequency of the two treatments. Patients in the dacomitinib group were treated with oral dacomitinib 45 mg once daily in 28-day cycles. Of the patients in this group, 66% experienced a dose reduction, 38% received the lowest dose of 30 mg/day and 28% received the lowest dose of 15 mg/day, according to the ARCHER 1050 trial [15]. The patients in the gefitinib group received gefitinib 250 mg orally once daily in 28-day cycles.
Transitional probability data
The clinical effectiveness data of PFS and OS were obtained from the ARCHER 1050 trial [15,17], via the techniques outlined in Guyot et al. [21]. WebPlotDigitizer was used to recreate Kaplan–Meier graphs to project outcomes to the end of the 15-year time horizon using Flexurv, an R package for the fully parametric modeling of survival data [22,23] (R version 3.3.3). The following parametric distributions were considered to determine the most appropriate parametric survival curve as recommended by the NICE Decision Support Unit [24]: gamma, log-logistic, Weibull, lognormal, Gompertz, exponential, generalized F and generalized gamma. The distributions were selected based on statistical tests (Akaike Information Criterion [AIC] and Bayesian Information Criterion [BIC]), visual inspection of fit to Kaplan–Meier plots, goodness-of-fit statistics and clinical plausibility. (Figure 2 & Supplementary Table 2).
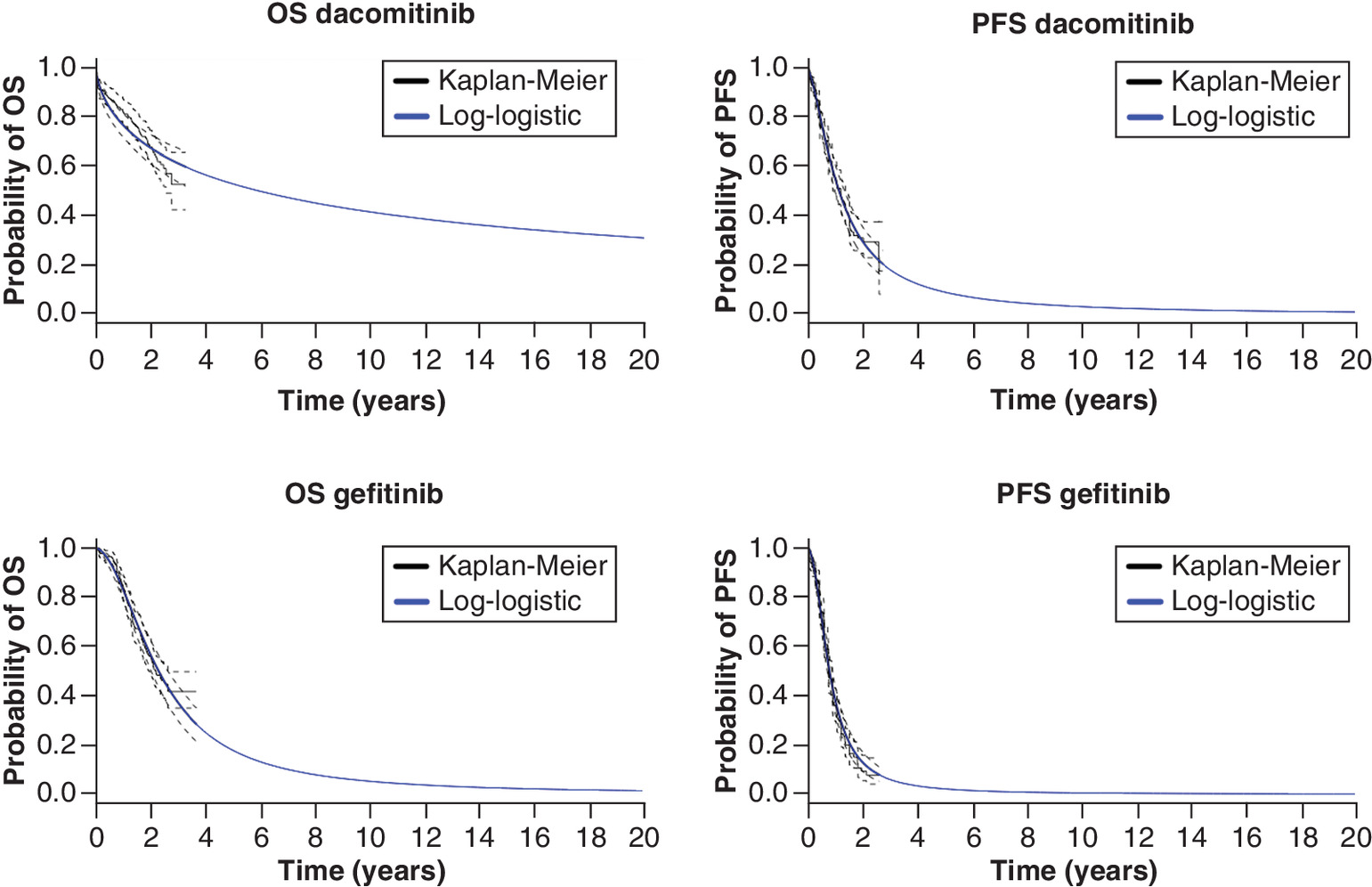
Figure 2. Overall survival and progression-free survival Kaplan–Meier plot and selected fitted curves.
PFS: Progression-free survival; OS: Overall survival.
For PFS and OS, a log-logistic distribution was selected. This distribution has the best visual and statistical fit; the hazards consistent with the observed hazards in the ARCHER 1050 trial [15], do not yield implausible projections with the survival curves for the two arms crossing (Supplementary Material & Figures 1–4). For each TKI, the probability that patients remain in stable disease at each time is determined by the values of the PFS curve at that time. In addition, the probability of patients to achieve the death state is determined as 1 minus the OS curve at that time. From this, the probability of patients in progressive disease follows, as the three states together should always add up to 100%.
Cost estimation
Table 1 outlines the calculated costs. Direct medical costs include treatment costs, disease management costs, end-of-life care costs, adverse events costs and second-line treatment costs. The cost of gefitinib and dacomitinib were calculated according to the officially notified listed prices ([drug price – 7.5% official discount in Spain] x Value added tax [VAT]) [25,26]. The cost of dacomitinib can be considered part of the problem because up to the date of publication of this article, an official Spanish price for this drug has not been published, and it has been obtained from NICE guidance [27].
| Management of NSCLC | Cost per 28-day cycle and patient | Distribution | Ref. |
|---|---|---|---|
| Gefitinib | €2045 | Gamma | [25–27] |
| Dacomitinib | €3023 | Gamma | |
| Second-line cost gefitinib | |||
| – Scheme (43.8% of total patients) | €1233 | Triangular | [15,25,26] |
| – Permetrexed (25.9%) | |||
| – Carboplatin (13.8%) | |||
| – Cisplatin (17.9%) | |||
| – Osimertinib (12.9%) | |||
| – Median number of postprogression systemic treatments per patients in gefitinib arm | 1 (1–6) | [15] | |
| Second-line cost dacomitinib | |||
| – Scheme (59% of total patients) | €1854 | Triangular | [15,25–27] |
| – Permetrexed (23.8%) | |||
| – Carboplatin (13.7%) | |||
| – Cisplatin (13.2%) | |||
| – Osimertinib (7.9%) | |||
| – Median number of postprogression systemic treatments per patients in dacomitinib arm | 2 (1–5) | [15] | |
| End-of-life care cost | €12,909 | Gamma | [28] |
| Grade III–IV adverse events (frequency >3%) | Median cost/cycle | [29,30] | |
| – Diarrhea | €1552 | Gamma | |
| – Dermatitis acneiform | €2.11 | Gamma | |
| – Stomatitis | €1352 | Gamma | |
| – Rash | €2.11 | Gamma | |
| – Maculopapular rash | €2.11 | Gamma | |
| – Postular rash | €2.11 | Gamma | |
| – ALT elevation | €68 | Gamma | |
| – AST elevation | €68 | Gamma | |
| Utilities scenario | Value | [30,31] | |
| – On treatment with no side effects | 0.65 | Beta | |
| – Diarrhea | 0.32 | Beta | |
| – Dermatitis acneiform | 0.15 | Beta | |
| – Stomatitis | 0.25 | Beta | |
| – Rash | 0.15 | Beta | |
| – Maculopapular rash | 0.15 | Beta | |
| – Postular rash | 0.15 | Beta | |
| – ALT elevation | 0 | Beta | |
| – AST elevation | 0 | Beta | |
| – Disease progression | 0.47 | Beta | |
NSCLC: Non-small-cell lung cancer.
Disease management costs were estimated according to an expert panel’s advice. Disease management cost per patient and cycle was calculated by multiplying the cost of healthcare resources employed by the unit cost of each resource consumed over a 15-year time horizon. The unit costs were obtained from an official database published in Spain [32].
End-of-life care costs were applied to each patient entering the death state and were obtained from an article published in Spain [28].
The costs of side effects management from the perspective of the Spanish National Health System (Table 1) were obtained from published articles [29,30]. Adverse effect (grade 3/4 events) frequencies associated with dacomitinib and gefitinib treatments and reported in at least 3% of patients were obtained from the ARCHER 1050 study [15].
The second-line therapy regimens were obtained from Supplementary Table 1 ARCHER 1050 study [15] as is shown in Table 1. In dacomitinib second-line arm, 23.8% of the patients were treated with pemetrexed, 13.7% with carboplatin, 13.2% with cisplatin and 7.9% with osimertinib. In gefitinib second-line arm, 25.9% of the patients were treated with pemetrexed, 13.8% with carboplatin, 17.9% with cisplatin and 12.9% with osimertinib. The patients were assumed to have a body height of 170 cm and a weight of 70 kg, resulting in a body surface area of 1.73 m2.
All cost inputs from prior years were inflated to 2019 Spanish values using the Consumer Price Index. The model costs are presented in Euros (€) 2019 (Table 1).
Utilities estimation
The ARCHER 1050 study has not reported health state utilities. Thus, utility inputs and disutility values for the base case were estimated from the recent data published in the literature [30,31]. In order to estimate QALYs, utility and disutility values were applied considering the different health states (stable disease and progressive disease) and are summarized in Table 1. A health utility of zero was applied to the health state of death.
Disutilities estimation
The disutility values associated with grade 3/4 adverse events while the patients remained in stable disease were adopted from a recently published international study that evaluated the disutilities and complications for advanced NSCLC in different countries like the UK, France, Australia and Republic of China by employing a time trade-off technique [33]. To calculate the disutility values associated with grade 3/4 in stable disease, the disutility parameters of each adverse event extracted from Nafees et al. were multiplied by the relative frequency of the corresponding event obtained from the ARCHER 1050 trial to calculate a weighted average disutility value for each event profile as is shown in Supplementary Table 1. The disutility values calculated for each grade 3/4 adverse event were subtracted from the utility values while the patients remained in stable disease.
Univariate sensitivity analysis
Deterministic sensitivity analysis (DSA) was performed to explore the impact of the essential variables on the ICER estimated value. Thus, a single parameter in the model (drug costs, utilities or discounts) was varied to test the effect on the ICER result. The utilities values were varied in a range of ±20%. The drug acquisition costs were modified in three different ranges (±15, ±20 and ±25%). The end-of-life care costs were varied in two different ranges (±10 and ±20%), and the discounts values in the DSA were modified in a percentage of 0 and 6%. The transition probability values of PFS and OS were varied in a range of ±5. The results of the DSA were presented in a tornado diagram.
Probabilistic sensitivity analysis
A probabilistic sensitivity analysis (PSA) was conducted to assess the influence of parameter uncertainties using 10,000 Monte Carlo simulations. Different parameters (side effects management costs, disease management costs, second-line treatment costs, acquisition costs, end-of-life care costs, utilities and transitions probabilities) of the model were varied to determine the robustness of the model. The results of the PSA was employed to obtain the cost–effectiveness acceptability curves, showing the probability of each alternative being cost-effective across a range of possible values of willingness-to-pay (WTP) for an additional QALY [34].
The different types of probability distributions were applied to variate the model parameters according to the characteristics of each variable [35]. Gamma distributions were employed for costs, beta for utilities and Dirichlet distributions for transitions probabilities. The number of postprogression systemic treatments per patient were assumed to follow a triangular distribution.
Results
The base-case cost–effectiveness results for dacomitinib and gefitinib are reported in Table 2. The total QALYs were 0.51 and 0.45 for dacomitinib and gefitinib, respectively. The incremental number of QALYs gained with dacomitinib compared with gefitinib was 0.06. The number of incremental life-years gained in the base case was 0.06 (0.86 life-years vs 0.80 life-years for dacomitinib and gefitinib, respectively). The mean costs for dacomitinib arm were €33,061 discounted over the 15-years horizon and €26,692 for the gefitinib arm, resulting in an additional cost of €6369. These costs and QALY values yielded an incremental ICER of €111,048 for dacomitinib compared with gefitinib.
| Variable | Strategy | |
|---|---|---|
| Gefitinib | Dacomitinib | |
| Total cost/pt | €26,692 | €33,061 |
| Treatment cost/pt | €11,120 | €22,833 |
| Disease management/pt | €2,219 | €1,869 |
| Adverse events costs/pt | €63 | €87 |
| Ee end-of-life care cost | €12,785 | €7,229 |
| 2L cost/pt | €505 | €1,043 |
| QALY gained/pt | 0.45 | 0.51 |
| ICER (€/QALY) Dacomitinib vs gefitinib | €111,048/QALY | |
pt: Patient; 2L: Second-line; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
The results from the DSA showed significant changes in the ICER after modifying dacomitinib acquisition costs, end-of-life care costs, utilities and discount values as shown in the Tornado diagram (Figure 3) and Supplementary Table 3. The model outcome was sensitive to the drug acquisition cost of dacomitinib, showing that discounts greater than 25% produced an ICER value below the threshold of 24,000€ per QALY gained fixed in Spain.
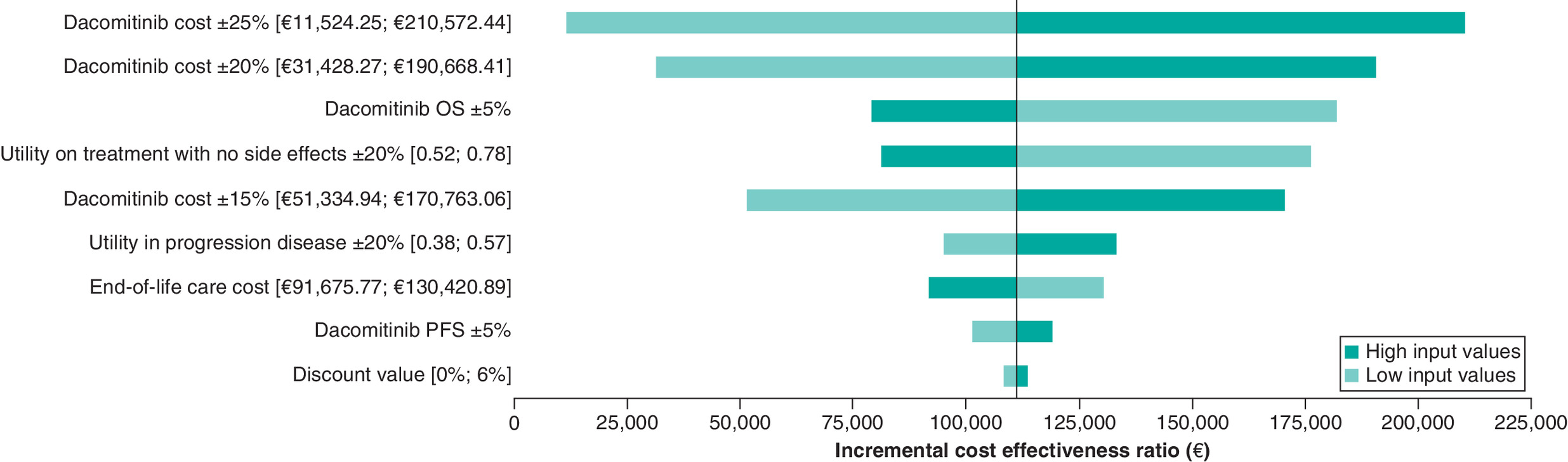
Figure 3. Tornado diagram (deterministic sensitivity analysis).
OS: Overall survival; PFS: Progression-free survival.
As shown in Figure 4, the PSA results were consistent with the base-case analyses. Dacomitinib was non cost-effective in 46.63% of the simulations, dominated in 17.84%, cost-effective in 16.11% and dominant in 19.42%.
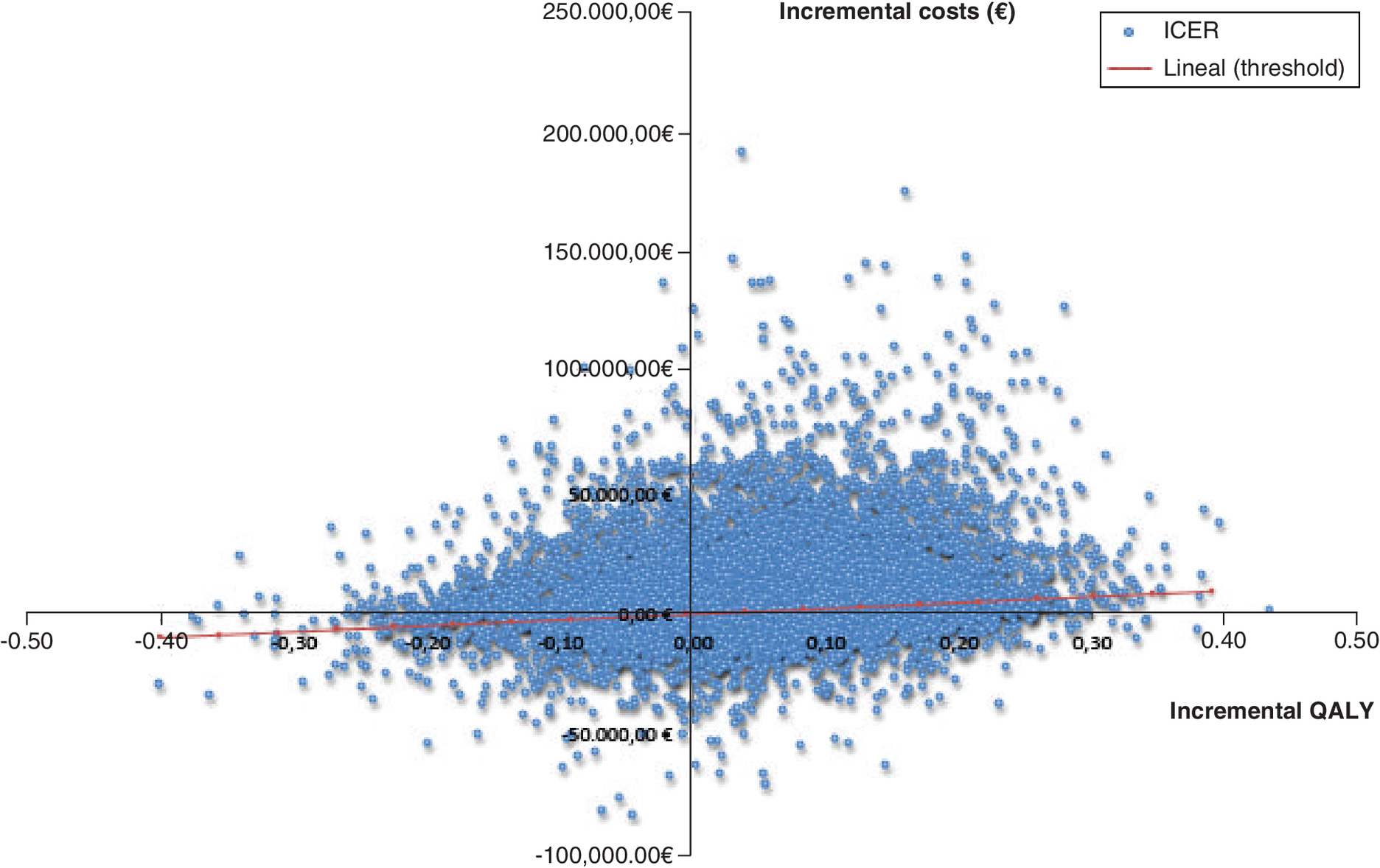
Figure 4. Scatter plot of Monte Carlo probabilistic sensitivity analysis for dacomitinib versus gefitinib.
ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
Finally, the results plotted in a cost–effectiveness plane (Figure 4) were used to construct the cost–effectiveness analysis curve, which shows the probability that dacomitinib becomes cost-effective for different WTP thresholds. Therefore, in the base-case scenario, there is a 35.53% probability of dacomitinib being cost-effective and dominant at a threshold of €24.000/QALY (Figure 5).
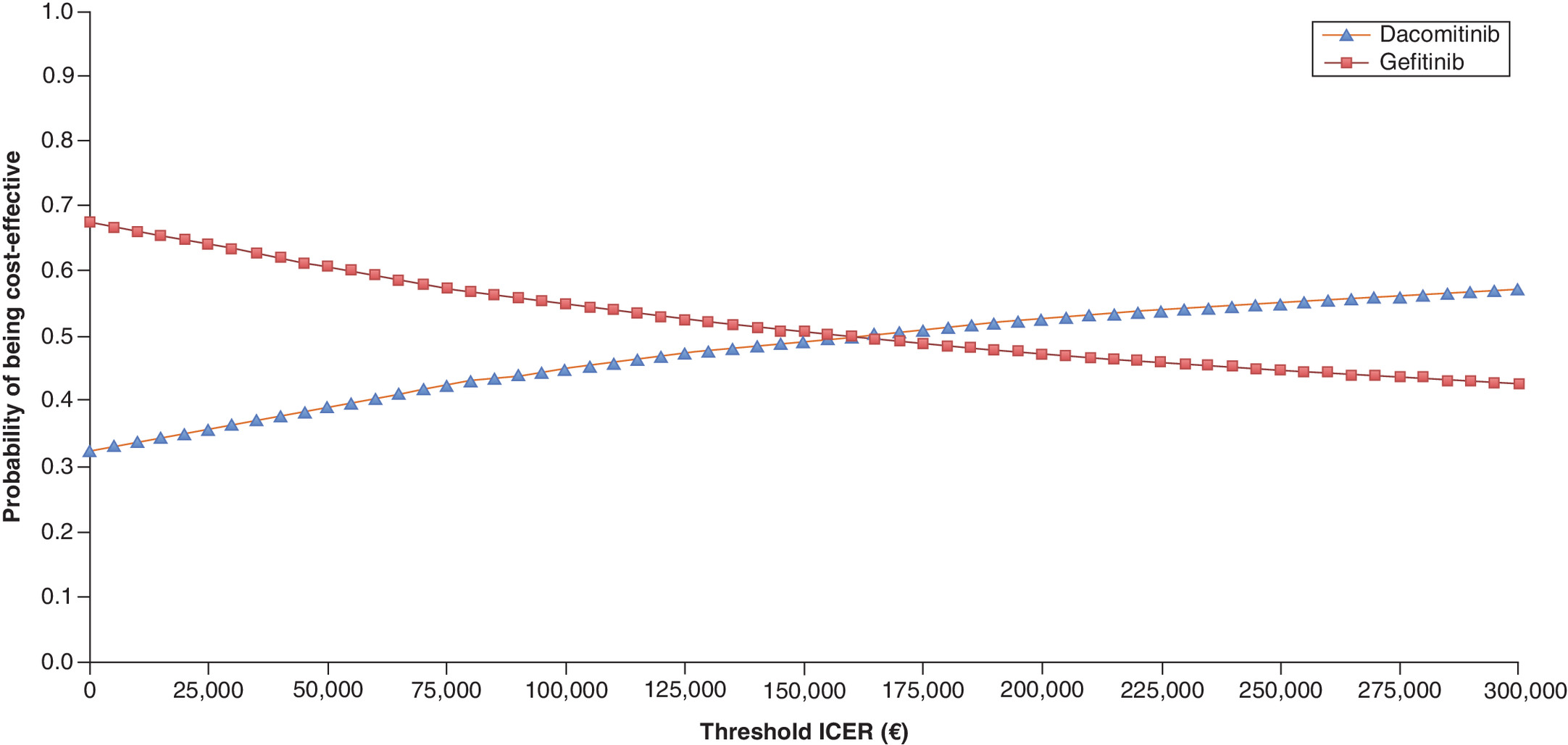
Figure 5. Cost–effectiveness acceptability curve dacomitinib versus gefitinib.
Graph plot WTP scenario (x-axis) versus the likelihood in percentage that the treatment would be considered cost-effective (y-axis).
ICER: Incremental cost–effectiveness ratio; WTP: Willingness-to-pay.
Discussion
Recently, the European Commission has approved dacomitinib for the frontline treatment of adult patients with locally advanced or metastatic NSCLC [36]. Dacomitinib has demonstrated superiority over gefitinib in both PFS and OS in Phase III head-to-head comparison study [15,17]. Additionally, a recent network meta-analysis demonstrated treatment with dacomitinib versus gefitinib (HR: 0.75; 95% CrI: 0.59–0.95), afatinib (HR: 0.87; 95% CrI: 0.61–1.24), erlotinib (HR: 0.79; 95% CrI: 0.44–1.42) and osimertinib (HR: 0.94; 95% CrI: 0.68–1.29) trended directionally toward improved OS, in patients with advanced or metastatic EGFR+ NSCLC [19]. However, the published meta-analysis is not showing a significant difference, CrIs are very wide due to the low number of studies included.
The lack of comparative long-term efficacy data can pose challenges for health technology appraisals. Therefore, we developed a complete cost–effectiveness analysis to compare dacomitinib versus gefitinib in patients with newly diagnosed advanced NSCLC and one EGFR mutation based on the ARCHER 1050 study [15]. Over a 15-year time horizon, we demonstrated that dacomitinib is considered slightly more effective in comparison with gefitinib in terms of QALYs gained (0.06). Nonetheless, our study showed that dacomitinib was not cost-effective compared with EGFR-TKIs because the ICER (€111,048/QALY) was higher than the commonly accepted threshold in Spain of €24,000/QALY [20]. Thus, the base case results indicate that discounts greater than 25% are crucial for the dacomitinib acquisition costs to be considered cost-effective.
At the time of the investigation, this is the first cost–effectiveness analysis to contribute a direct comparison of dacomitinib against the first-generation EGFR-TKI (gefitinib) for patients with newly diagnosed advanced NSCLC EGFR-mutated.
NICE has recommended dacomitinib for locally advanced or metastatic EGFR mutation-positive in adults. The evidence review group of NICE constructed a fixed-effects network meta-analysis using data from the ARCHER 1050 for dacomitinib and from LUX-Lung 7 for afatinib [37,38]. The results of this study showed that PFS and OS might be better for dacomitinib than afatinib, although there was no significant difference between the two treatments (PFS, HR: 0.80; 95% CI: 0.57–1.12; OS, HR: 0.88; 95% CI 0.61–1.29).
In our study, the small difference in the incremental QALY values (0.06) is mainly attributable to the differences in efficacy between the two drugs. The decrease in utility values due to adverse reactions does not have a relevant impact on the model. This fact can be seen in the DSA, where the drug is not able to be cost-effective, despite the decrease of 20% in the utility value of dacomitinib in stable disease.
In our study, dose modifications are needed to reduce the incidence and severity of treatment-related adverse events [18]. However, adjustment to dose reduction is not expected to have a large impact on the cost–effectiveness results since the price of the different doses of dacomitinib are uniformly based on NICE guidance [27].
In addition, a cost–effectiveness acceptability curve was constructed based on the results plotted in a cost–effectiveness plane to obtain the probability that dacomitinib is cost-effective compared with gefitinib for a different WTP threshold. We demonstrated that, with the defined cost–effectiveness threshold in Spain of €24,000/QALY [20], dacomitinib may be considered not cost-effective due to the high price of drug acquisition.
Lung cancer morbidity and mortality have a significant economic impact on the healthcare system and society. The poor long-term prognosis and high healthcare cost highlight the need to balance patient access to best treatment with healthcare sustainability and societal burden, particularly in the advanced NSCLC setting [39]. Economic evaluations, like the present cost–effectiveness analysis, are widely used to inform policymakers and health administrators about which treatment innovations should be reimbursed or promoted and to consider reducing prices in the drug acquisition cost.
Our study has some limitations. First, we employed a partitioned survival model, a theoretical model which, by definition, constitutes a simplified simulation of reality. Second, the utility values in the analysis model were extracted from a verified study published in the population of UK [31] but not from Spain because, to date, these data are not available. Third, until the publication of this article, the acquisition cost of dacomitinib has not yet been approved in Spain. Therefore, the value obtained by NICE was selected [27]. Fourth, patients with brain metastases were excluded from participation in the ARCHER 1050 study because the brain penetration of dacomitinib was not known at the time of the study and this could affect the final QALY values [40].
Conclusion
This study showed that, from Spanish National Health System perspective, treatment with dacomitinib was more effective in terms of QALYs gained than treatment with gefitinib. However, dacomitinib has been proved not to be a cost-effective alternative in first-line therapy for advanced EGFR-mutated NSCLC patients in Spain because the ICER (€111,048/QALY) appears to be too high given the Spanish threshold. The price of dacomitinib should be reduced by 25% to become a cost-effective alternative.
•
In ARCHER 1050 study, the median progression-free survival in patients with newly diagnosed advanced non-small-cell lung cancer (NSCLC) and one EGFR mutation (exon 19 deletion or Leu858Arg) was demonstrated to be significantly longer with dacomitinib than with gefitinib (14.7 vs 9.2 months).
•
Dacomitinib presented higher quality-adjusted life years (QALYs; 0.51) compared with gefitinib (0.45).
•
Dacomitinib total costs of the intervention were €33,061, in comparison with the €26,691.88 for gefitinib arm.
•
An incremental cost–effectiveness analysis of €111,048/QALY was obtained for dacomitinib compared with gefitinib.
•
Dose modifications are needed to reduce the incidence and severity of treatment-related adverse events.
•
From Spanish National Health System perspective, dacomitinib has been proved not to be a cost-effective alternative in first line therapy for advanced EGFR-mutated NSCLC patients, compared with gefitinib due to the high acquisition costs of the drug.
•
A discount greater of 25% in dacomitinib acquisition cost could produce an incremental cost–effectiveness ratio value below the established threshold of €24,000 per QALY gained in Spain to result a cost–effectiveness alternative.
Author contributions
All the authors interpreted data, read and approved the final manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Our study used mathematical modeling and was not an active clinical trial; therefore, no approval was required from the Institutional Research Ethics Board.
Supplementary Material
File (suppl_file.zip)
- Download
- 6.36 MB
File (supplementary figure 1.tif)
- Download
- 10.96 MB
File (supplementary figure 2.tif)
- Download
- 10.94 MB
File (supplementary figure 3.tif)
- Download
- 10.97 MB
File (supplementary figure 4.tif)
- Download
- 10.87 MB
File (supplementary table 1.docx)
- Download
- 13.48 KB
File (supplementary table 2.docx)
- Download
- 23.45 KB
File (supplementary table 3.docx)
- Download
- 23.41 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J. Clin. 69(1), 7–34 (2019).
2.
Sun S, Schiller JH, Spinola M, Minna JD. New molecularly targeted therapies for lung cancer. J. Clin. Invest. 117(10), 2740–2750 (2007).
• Provides background on the epidemiology of non-small-cell lung cancer.
3.
Dearden S, Stevens J, Wu YL, Blowers D. Mutation incidence and coincidence in non small-cell lung cancer: meta-analyses by ethnicity and histology (mutMap). Ann. Oncol. 24(9), 2371–2376 (2013).
4.
Reck M, Hagiwara K, Han B et al. ctDNA determination of EGFR mutation status in European and Japanese patients with advanced NSCLC: the ASSESS study. J. Thorac. Oncol. 11(10), 1682–1689 (2016).
5.
Esteban E, Majem M, Martinez Aguillo M et al. Prevalence of EGFR mutations in newly diagnosed locally advanced or metastatic non-small cell lung cancer Spanish patients and its association with histological subtypes and clinical features: the Spanish REASON study. Cancer Epidemiol. 39(3), 291–297 (2015).
• Provides information on the epidemiology in Spain.
6.
Zhi X, Shi Y, Yu J. Standards for the diagnosis and treatment of primary lung cancer (2015 version) in China. Zhonghua Zhong Liu Za Zhi 37(1), 67–78 (2015).
7.
Mitsudomi T, Morita S, Yatabe Y et al. West Japan Oncology Group. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised Phase III trial. Lancet Oncol. 11(2), 121–128 (2010).
8.
Han JY, Park K, Kim SW et al. First-SIGNAL: first-line single-agent iressa versus gemcitabine and cisplatin trial in never-smokers with adenocarcinoma of the lung. J. Clin. Oncol. 30(10), 1122–1128 (2012).
9.
Zhou C, Wu YL, Chen G et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, Phase III study. Lancet Oncol. 12(8), 735–742 (2011).
10.
Rosell R, Carcereny E, Spanish Lung Cancer Group in collaboration with Groupe Français de Pneumo-Cancérologie and Associazione Italiana Oncologia Toracica et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised Phase III trial. Lancet Oncol. 13(3), 239–246 (2012).
11.
Sequist LV, Yang JC, Yamamoto N et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 31(27), 3327–3334 (2013).
12.
Wu YL, Zhou C, Hu CP et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised Phase III trial. Lancet Oncol. 15(2), 213–222 (2014).
13.
Mok TS, Wu YL, Thongprasert S et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 361(10), 947–957 (2009).
14.
Maemondo M, Inoue A, North-East Japan Study Group et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 362(25), 2380–2388 (2010).
15.
Wu YL, Cheng Y, Zhou X et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, Phase III trial. Lancet Oncol. 18(11), 1454–1466 (2017).
•• Phase III clinical trial from which we have extracted the most important data to elaborate our cost–effectiveness study, such as progression-free survival and overall survival curves and the adverse reaction data, among other data.
16.
Shirley M. Dacomitinib: first global approval. Drugs 78(18), 1947–1953 (2018).
17.
Mok TS, Cheng Y, Zhou X et al. Improvement in overall survival in a randomized study that compared dacomitinib with gefitinib in patients with advanced non-small-cell lung cancer and EGFR-activating mutations. J. Clin. Oncol. 36(22), 2244–2250 (2018).
18.
Corral J, Mok TS, Nakagawa K et al. Effects of dose modifications on the safety and efficacy of dacomitinib for EGFR mutation-positive non-small-cell lung cancer. Future Oncol. 15(24), 2795–2805 (2019).
19.
Farris MS, Larkin-Kaiser KA, Scory T et al. Network meta-analysis of first-line therapy for advanced EGFR mutation positive non-small-cell lung cancer: updated overall survival. Future Oncol. 16(36), 3107–3116 (2020).
• Network meta analysis shows that there is a trend which demonstrates an improvement in overall survival in treatment with dacomitinib versus gefitinib.
20.
Vallejo-Torres L, García-Lorenzo B, Serrano-Aguilar P. Estimating a cost-effectiveness threshold for the Spanish NHS. Health Econ. 27(4), 746–761 (2018).
• Provides the cost–effectiveness threshold for a drug in Spain.
21.
Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 12, 9 (2012).
22.
Rohatgi A. WebPlotDigitizer (2014). https://apps.automeris.io/wpd/
23.
Jackson CH. Flexsurv: a platform for parametric survival modeling in R. J. Stat. Softw. 70, i08 (2016).
24.
Latimer NR. Survival analysis for economic evaluations alongside clinical trials--extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med. Decis. Making 33(6), 743–754 (2013).
25.
Spanish Healthcare Ministry. Drug prices (2019). https://cima.aemps.es/cima/publico/lista.html
26.
Spanish Healthcare Ministry. Official discounts in drug prices (2017). www.msssi.gob.es/profesionales/farmacia/pdf/DeduccionesJunio2017.pdf
27.
National Institute for Health and Care Excellence. Dacomitinib for untreated EGFR mutation-positive non-small-cell lung cancer (NICE technology appraisal guidance No. 595) (2019). www.nice.org.uk/guidance/ta595
28.
Nuño-Solinís R, Herrera Molina E, Librada Flores S, Orueta Mendía JF, Cabrera-León A. Care costs and activity in the last three months of life of cancer patients who died in the Basque Country (Spain). Gac. Sanit. 31(6), 524–530 (2017).
29.
Isla D, De Castro J, Juan O et al. Costs of adverse events associated with erlotinib or afatinib in first-line treatment of advanced EGFR-positive non-small cell lung cancer. Clinicoecon. Outcomes Res. 9, 31–38 (2016).
30.
Villa G, Hernández-Pastor LJ, Guix M, Lavernia J, Cuesta M. Cost-effectiveness analysis of pazopanib in second-line treatment of advanced soft tissue sarcoma in Spain. Clin. Transl. Oncol. 17(1), 24–33 (2015).
31.
Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual. Life Outcomes 6, 84 (2008).
• Provides the useful values needed to calculate the quality-adjusted life-years values.
32.
Osakidetza, The Basque Health Service. Rates for billing health and teaching services of the Basque Health Service for 2019 (2019). www.euskadi.eus/contenidos/informacion/osk_servic_para_empresas/es_def/adjuntos/tarifas_2019.pdf
33.
Nafees B, Lloyd AJ, Dewilde S, Rajan N, Lorenzo M. Health state utilities in non-small cell lung cancer: an international study. Asia Pac. J. Clin. Oncol. 13(5), e195–e203 (2017).
34.
Barton GR, Briggs AH, Fenwick EA. Optimal cost-effectiveness decisions: the role of the cost-effectiveness acceptability curve (CEAC), the cost–effectiveness acceptability frontier (CEAF), and the expected value of perfection information (EVPI). Value Health 11(5), 886–897 (2008).
35.
Aalabaf-Sabaghi M. Decision modelling for health economic evaluation. J. Epidemiol. Community Health 61(9), 839 (2007).
36.
European Agency Medicines. CHMP summary of positive opinion for Vizimpro (2019). www.ema.europa.eu/en/documents/smop-initial/chmp-summary-positive-opinion-vizimpro_en.pdf
37.
Park K, Tan EH, O'Byrne K et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): a Phase IIB, open-label, randomised controlled trial. Lancet Oncol. 17(5), 577–589 (2016).
38.
Paz-Ares L, Tan EH, O'Byrne K et al. Afatinib versus gefitinib in patients with EGFR mutation-positive advanced non-small-cell lung cancer: overall survival data from the Phase IIb LUX-Lung 7 trial. Ann. Oncol. 28(2), 270–277 (2017).
39.
Jakovljevic M, Malmose-Stapelfeldt C, Milovanovic O, Rancic N, Bokonjic D. Disability, European OECD work absenteeism, sickness benefits, and cancer in selected countries-forecasts to 2020. Front. Public Health 5, 23 (2017).
40.
Kudo K, Kawakado K, Kawajiri T et al. Dramatic response of brain metastasis from EGFR-mutation-positive NSCLC to dacomitinib. Intern. Med. 59(14), 1739–1740 (2020).
Information & Authors
Information
Published In
Pages: 325 - 335
PubMed: 33635095
Copyright
© 2021 Future Medicine Ltd.
History
Received: 28 October 2020
Accepted: 16 December 2020
Published online: 26 February 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Dacomitinib in first-line treatment of advanced EGFR-mutated non-small-cell lung cancer: a cost–effectiveness analysis. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0233
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Lili Su, Xiangyu Zhang, Mengrong Li, Ying Li, Dong Wang, Cost-utility analysis of osimertinib and dacomitinib in the first-line treatment of advanced non-small cell lung cancer with EGFR mutation, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2025.2518135, 25, 10, (1437-1444), (2025).
- Angie Raad, Maria Rizzo, Katherine Appiah, Isabella Kearns, Luis Hernandez, Critical Examination of Modeling Approaches Used in Economic Evaluations of First-Line Treatments for Locally Advanced or Metastatic Non-Small Cell Lung Cancer Harboring Epidermal Growth Factor Receptor Mutations: A Systematic Literature Review, PharmacoEconomics, 10.1007/s40273-024-01362-2, 42, 5, (527-568), (2024).
- Xiaojia Yang, Jinfang Li, Taihui Zhang, Qinping Xia, Wei Zhang, Yike Cui, Wen He, Bioequivalence study of dacomitinib and Vizimpro® in healthy Chinese volunteers under fasting and fed conditions: A randomized, open‐label, single‐dose, crossover trial, Clinical and Translational Science, 10.1111/cts.13653, 16, 12, (2591-2603), (2023).
- Joo-Young Byun, Sun-Kyeong Park, Boon Peng Ng, Yi-Shao Liu, Chae-Rin Kim, Chanhyun Park, A systematic review of economic evaluations of tyrosine kinase inhibitors for non-small cell lung cancer (NSCLC), Expert Opinion on Pharmacotherapy, 10.1080/14656566.2022.2095203, 23, 11, (1247-1257), (2022).
- J Aguilar-Serra, V Gimeno-Ballester, a Pastor-Clerigues, J Milara, C Trigo-Vicente, J Cortijo, Cost-effectiveness analysis of the first‐line EGFR‐TKIs in patients with advanced EGFR-mutated non-small-cell lung cancer, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2022.1987220, 22, 4, (637-646), (2021).