Healthcare utilization in clinically significant tricuspid regurgitation patients with and without heart failure
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study evaluated how the presence of right-sided heart disease (RSHD), other valve disease (OVD) and heart failure (HF) impacts healthcare utilization in patients with tricuspid valve disease (tricuspid regurgitation [TR]). Materials & methods: Of the 33,686 patients with TR: 6618 (19.6%) had TR-only; 8952 (26.6%) had TR with HF; 12,367 (36.7%) had TR with OVD but no HF; and 5749 (17.1%) had TR with RSHD only. Results: The presence of RSHD, OVD or HF in patients with TR was independently associated with increased annualized hospitalizations, hospital days and costs relative to patients with TR alone. Conclusion: All three co-morbidities were associated with increased healthcare utilization, with HF showing the greatest impact across all measures.
Tricuspid regurgitation (TR) is a prevalent valvular disorder in the USA and most frequently occurs when dilation of the right ventricle results in the backward flow of blood through the tricuspid valve into the right atrium [1–4]. Several conditions that cause right-ventricle dilation are associated with TR. These include heart failure (HF) diastolic, systolic, combined or unspecified, right-sided heart disease (RSHD) defined as patients with right ventricular dysfunction (RVD), chronic obstructive pulmonary disease (COPD), idiopathic pulmonary arterial hypertension (IPAH) or atrial fibrillation (AF), patients with other valve disease (aortic or mitral) [4–7].
Severe TR is independently associated with high morbidity and mortality but patients are frequently asymptomatic and therefore the focus of treating this condition is primary based on symptoms [2,3,7–13]. Consequently, TR is often overlooked until it progresses in severity. Current guidelines recommend that surgery to treat severe TR be performed concomitantly with left-sided heart valve surgeries [4,5,7,13–15]. As a result, TR surgery is infrequently performed as a standalone procedure compared with other forms of cardiac surgery [16].
Currently, Topilsky et al. estimate TR prevalence at: approximately 0.55% in the USA, which is adjusted for age and sex [17]. However, the complex pathology of TR and its associated conditions could result in its under-recognition and make it difficult to assess the true prevalence [6,7,9,13,15]. Additionally, confounders likely delay treatment for TR, despite poor prognosis, which increases healthcare utilization [5,18,19].
A recent study by Cork et al. investigated the healthcare burden of TR patients with and without HF, concluding that irrespective of the presence of HF, clinically significant TR is associated with an increase in healthcare utilization and expenditures [6]. An increase in utilization was seen, however, when both diseases (TR and HF) were present.
This study, builds upon Cork by seeking to quantify the incremental economic burden of several different associated conditions in the presence of TR, not just HF. Therefore, the objective of this study was to use real-world data from Optum’s de-identified, all-payer, integrated database of United Healthcare claims and Humedica electronic health records (EHRs) to evaluate how the presence of HF (diastolic, systolic, combined or unspecified) and RSHD without HF (RVD, COPD, IPAH or AF) and OVD without HF or RSHD impact healthcare utilization in patients with TR.
Methods
Data source
This study used data from the Optum® Integrated File, which contains data from both claims and EHRs for patients across the USA [20]. The combination of claims and clinical data offers a more comprehensive view of the patient’s journey and interaction within the healthcare system. Optum’s Integrated Claims – Clinical dataset combines adjudicated claims data with Optum’s EHR data. Optum’s longitudinal clinical and claims repository from Optum Analytics is derived from more than 50 healthcare provider organizations in the USA that include more than 700 hospitals and 7000 clinics, treating more than 103 million patients receiving care in the USA. The Integrated dataset, which leverages a proprietary Optum algorithm that uses both salting and cryptographic hashing, links both claims and clinical data for approximately 24M matched individuals. The Integrated dataset includes historical, linked administrative claim data from pharmacy claims, physician claims and facility claims, with EHR information, inclusive of medications prescribed and administered, lab results, vital signs, body measurements, diagnoses, procedures and information derived from clinical notes using Natural Language Processing [20]. Optum data provide a continuum of treatment and cost including medications by therapeutic area, provider notes with treatment rationale and cost by procedure and condition. All data used to perform this analysis were de-identified and accessed in compliance with the Health Insurance Portability and Accountability Act. As a retrospective analysis of a de-identified database, the research was exempt from Institutional Review Board review under 45 Code of Federal Regulations 46.101(b)(4).
Inclusion/exclusion criteria
Adults 18 years or older in the Optum® Integrated File were included for analysis if they had a minimum of one diagnosis code (ICD10: I36.1 nonrheumatic tricuspid valve insufficiency) for tricuspid insufficiency between October 2015 and June 2019 without a record of end-stage renal disease, valve prolapse or primary organ disease. Patients were also required to have 12 months of continuous health plan enrollment before their first TR diagnosis and 1 month of continuous enrollment post-TR diagnosis. The 1-month post-TR diagnosis was used as a landmark period to capture TR severity. No continuous enrollment was applied to the outcome period and because patients had varying follow-up times, all outcomes were annualized per patient year.
Cohort definitions
The impact of severe TR on mortality among patients with HF is known [21]. However, the impact of TR associated with other conditions (RSHD and OVD) remains unknown. Conventional wisdom assumes that HF should account for the majority of a patient’s clinical burden, so we constructed a hierarchical cohort classification of TR patients as follows: All patients with TR were categorized based on whether or not there was a record of HF (diastolic, systolic, combined or unspecified) before or 1 month (landmark period) following TR diagnosis. For those patients with no record of HF, they were further subdivided first by presence of OVD and next by presence of RSHD at baseline or landmark if OVD was absent.
RSHD was defined as one or more of the following conditions: RVD, COPD, IPAH or AF. Based on this hierarchy four cohorts emerged: TR-only (reference group); TR with HF; TR with OVD (no HF); and TR with RSHD only (no OVD or HF).
Severity
Patients were categorized as having severe TR disease with pulmonary hypertension plus presence of either ascites, edema or hepatic insufficiency before or 1 month following (landmark period) TR diagnosis. Patients were also considered to have severe TR if they had a record of TR surgery during the landmark period, or if TR was quantified as moderate or severe in EHR physician notes of the Humedica database.
Outcomes
Outcomes included all-cause hospitalizations, cardiovascular (CV)-related hospitalizations, total hospital days and the percentage change in total expenditures. All outcomes were annualized to reflect the total outcome in the post period divided by the number of years of follow-up. All count outcomes (hospitalizations and total hospital days) were rounded to the nearest whole number to employ Poisson and negative binomial count-regression methodologies.
Statistical analysis
Zero-inflated methodology was used due to excess number of zeros (>50%) for each count outcome. Both zero-inflated Poisson and negative binomial regression models were created to model all-cause hospitalizations, CV-related hospitalizations and total hospital days. Final models were determined by using diagnostics for overdispersion. Least square means were calculated to show the estimated outcomes given the model results.
Due to the inherent right-skewness of cost data, total expenditures were modeled using gamma log link regression models. For the total expenditure models, relative counts were reported comparing each cohort to the reference group (TR-only) because of restrictions on reporting dollar amounts using Optum data. All models adjusted for the following covariates: age, sex, race, Elixhauser Comorbidity Index (ECI) [22] score and TR severity. Region, payor and income were not included in modeling because each was found to be nonsignificant, or were related to other variables already included (e.g., payor and age). Confidence intervals were reported for each model, with any confidence interval including or crossing one considered statistically not significant. All statistical analyses were performed using SAS software version 9.2-9.4 (SAS Institute, Inc., NC, USA).
Results
Of the 33,686 patients who met all inclusion criteria, 6618 (19.6%) had TR-only; 8952 (26.6%) had TR with HF; 12,367 (36.7%) had TR with OVD but no HF; and 5749 (17.1%) had TR with RSHD only (no HF, no OVD) (Figure 1). The TR with HF cohort had the highest mean (SD) ECI score (11.5 [3.7]) of the four cohorts. Mean standard deviation (SD) ECI scores for the cohorts without HF ranged from 5.7 (3.0) to 8.1 (3.3) (Table 1). The TR with HF cohort was also the oldest and had the highest percentage of patients with severe TR with a mean (SD) age of 73 (11.9) years and 662 (7.4%) patients with severe TR. The TR-only cohort was the youngest and had the fewest number of patients with severe TR, with a mean (SD) age of 61 (17.1) years and 32 (0.5%) patients with severe TR.
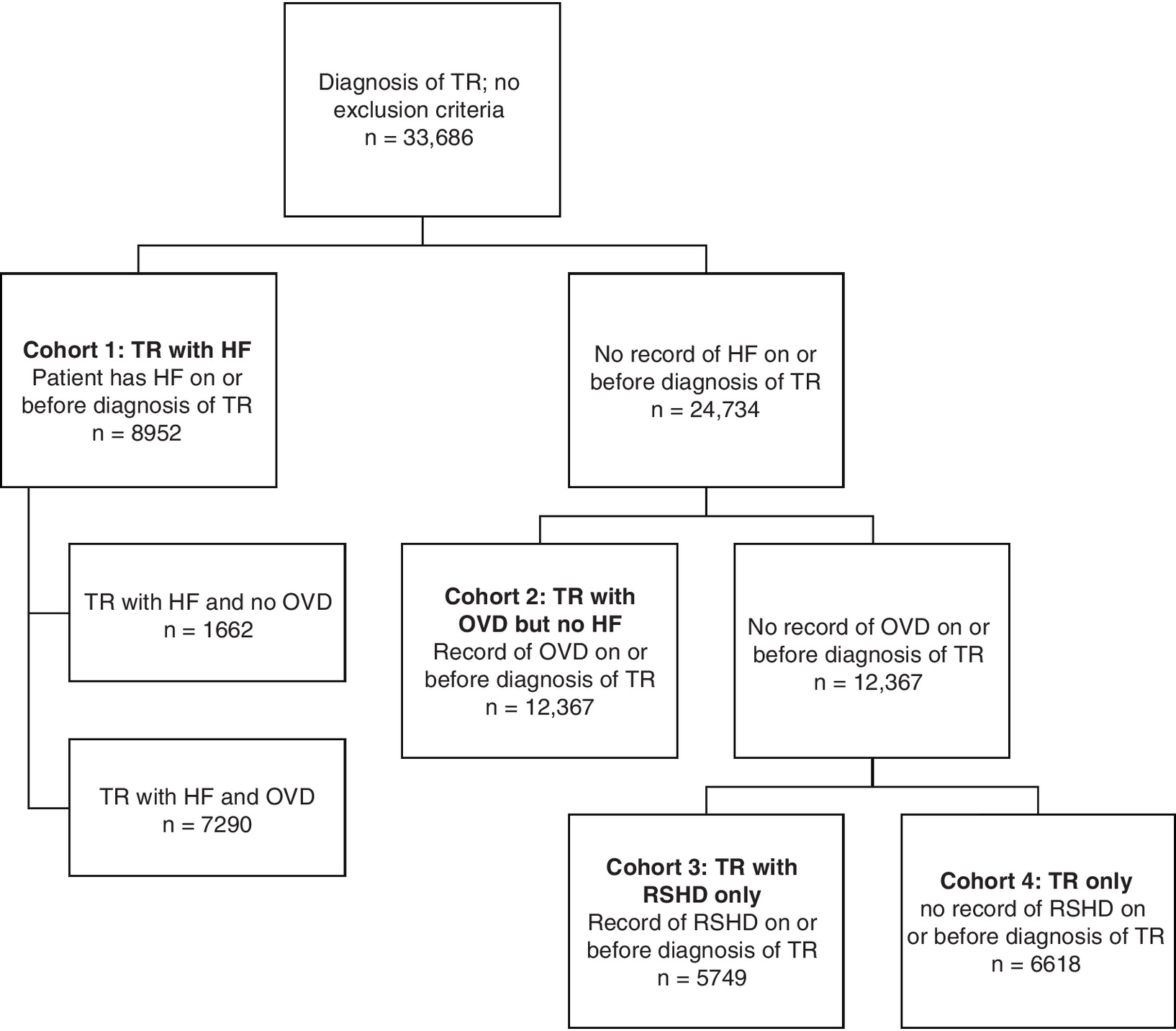
Figure 1. Attrition diagram.
HF: Heart failure; OVD: Other valve disease; RSHD: Right-sided heart disease; TR: Tricuspid regurgitation.
| Characteristics, no. (%)† | TR with HF (n = 8952) | TR with OVD but no HF (n = 12,367) | TR with RSHD only (no HF, no OVD; n = 5749) | TR-only (no HF, no OVD, no RSHD; n = 6618) | ||||
|---|---|---|---|---|---|---|---|---|
| Age (years) | ||||||||
| – Mean (SD) | 73 | (11.9) | 66 | (15.9) | 71 | (12.1) | 61 | (17.1) |
| – Median (IQR) | 76 | (66–83) | 69 | (56–78) | 73 | (64–81) | 62 | (49–74) |
| Sex | ||||||||
| – Male | 4451 | (49.7) | 5388 | (43.6) | 2634 | (45.8) | 2754 | (41.6) |
| – Female | 4489 | (50.1) | 6972 | (56.4) | 3112 | (54.1) | 3860 | (58.3) |
| Unknown | 12 | (0.1) | 7 | (0.1) | 3 | (0.1) | 4 | (0.1) |
| Race | ||||||||
| – Caucasian | 7130 | (79.6) | 10,005 | (80.9) | 4861 | (84.6) | 5144 | (77.7) |
| – Black | 1043 | (11.7) | 1053 | (8.5) | 399 | (6.9) | 654 | (9.9) |
| – Asian | 75 | (0.8) | 281 | (2.3) | 94 | (1.6) | 187 | (2.8) |
| – Other/Unknown | 704 | (7.9) | 1028 | (8.3) | 395 | (6.9) | 633 | (9.6) |
| Region | ||||||||
| – Northeast | 846 | (9.5) | 2702 | (21.8) | 858 | (14.9) | 1844 | (27.9) |
| – Midwest | 4164 | (46.5) | 5003 | (40.5) | 2575 | (44.8) | 2428 | (36.7) |
| – South | 3086 | (34.5) | 3859 | (31.2) | 1912 | (33.3) | 1947 | (29.4) |
| – West | 626 | (7.0) | 531 | (4.3) | 290 | (5.0) | 241 | (3.6) |
| – Unknown | 230 | (2.6) | 272 | (2.2) | 114 | (2.0) | 158 | (2.4) |
| Payor | ||||||||
| – Commercial | 3829 | (42.8) | 7428 | (60.1) | 2839 | (49.4) | 4589 | (69.3) |
| – Medicare | 5121 | (57.2) | 4936 | (39.9) | 2908 | (50.6) | 2028 | (30.6) |
| – Unknown | 2 | (0.0) | 3 | (0.0) | 2 | (0.0) | 1 | (0.0) |
| Income‡,$ | ||||||||
| – Mean (SD) | 42,981 | (10.6K) | 44,468 | (12.3K) | 43,569 | (11,2K) | 45,255 | (13.2K) |
| – Median (IQR) | 40,383 | (36.3–48.6K) | 41,792 | (36.3–49.3K) | 41,676 | (36.3–49.3K) | 42,694 | (36.3–49.3K) |
| Severity | ||||||||
| – Severe TR | 662 | (7.4) | 123 | (1.0) | 91 | (1.6) | 32 | (0.5) |
| ECI score | ||||||||
| – Mean (SD) | 11.5 | (3.7) | 6.8 | (3.4) | 8.1 | (3.3) | 5.7 | (3.0) |
| – Median (IQR) | 11 | (9–14) | 6 | (4–9) | 8 | (6–10) | 5 | (3–8) |
†
All values reported as no. (%) unless otherwise specified.
‡
Sample sizes are reduced, as not everyone reported their income. Values for the four cohorts from left to right are 8666; 11,995; 5602 and 6393.
ECI: Elixhauser Comorbidity Index; HF: Heart failure; IQR: Interquartile range; OVD: Other valve disease; RSHD: Right-sided heart disease; TR: Tricuspid regurgitation; SD: Standard deviation.
Multivariable models estimated that the TR with HF cohort also had the highest rate of annualized all cause ([0.74]; 95% CI: 0.53–1.04) and CV-related ([0.75]; 95% CI: 0.53–1.05) hospitalizations (Figure 2A & B). Patients with TR-only had the lowest annualized hospitalization rates ([0.54]; 95% CI: 0.39–0.77) for all-cause; ([0.50]; 95% CI: 0.35–0.71) for CV-related. Within each cohort, all-cause and CV-related hospitalization rates were similar. In the TR with HF cohort, average annual CV-related hospitalizations were slightly more frequent compared with the cohorts without HF. Annualized hospital days were modeled and results are shown in Figure 3. The TR with HF group had the most days ([7.1]; 95% CI: 6.1–8.3), followed by TR without HF with RSHD ([6.4 days]; 95% CI: 5.4–7.4) and OVD ([6.0 days]; 95% CI: 5.2–7.0), respectively. The TR-only group has the least average annualized days at ([5.5]; 95% CI: 4.7–6.4).
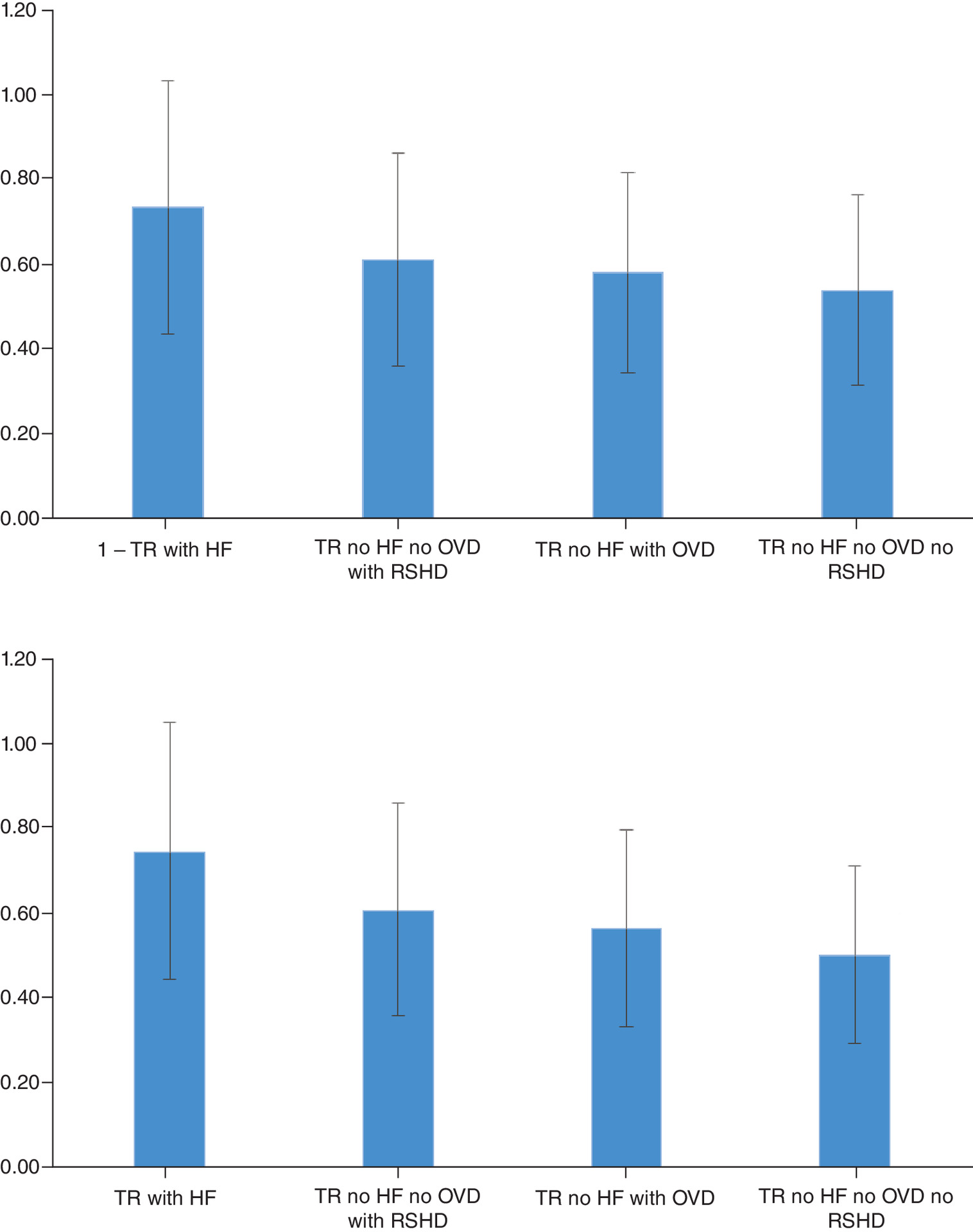
Figure 2. Estimated number of annualized hospitalizations by cohort.
(A) Estimated number of annualized hospitalizations: all-cause. (B) Estimated number of annualized hospitalizations: cardiovascular-related.
Multivariable models adjusted for age, sex, race, Elixhauser Comorbidity Index score and tricuspid regurgitation severity.
CV: Cardiovascular; HF: Heart failure; OVD: Other valve disease; RSHD: Right-sided heart disease; TR: Tricuspid regurgitation.
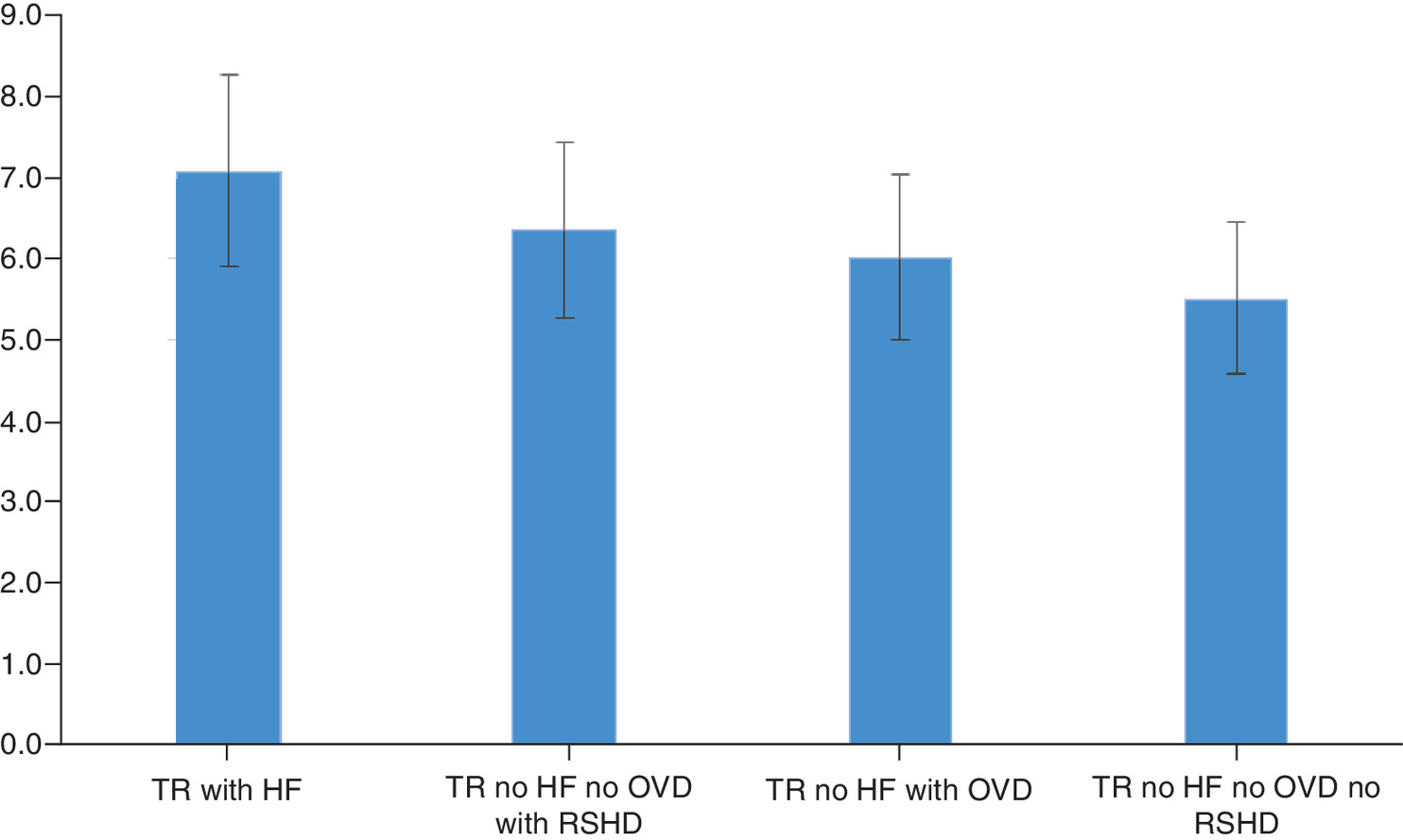
Figure 3. Estimated annualized hospital days by cohort.
Multivariable models adjusted for age, sex, race, Elixhauser Comorbidity Index score and tricuspid regurgitation severity.
HF: Heart failure; OVD: Other valve disease; RSHD: Right-sided heart disease; TR: Tricuspid regurgitation.
Compared with patients with TR-only, annualized all-cause expenditures were significantly higher for all other cohorts with added co-morbidities (Figure 4). Patients with TR and HF had the highest percent difference in annual costs relative to the TR-only group ([15.0%]; 95% CI: 9–21%) higher costs and those without HF. Patients with TR and RSHD but no HF or OVD had ([13.0%]; 95% CI: 7–18%) higher costs than TR-only and those with TR and OVD, but no HF had ([6%]; 95% CI: 2–10%) higher costs versus TR-only.
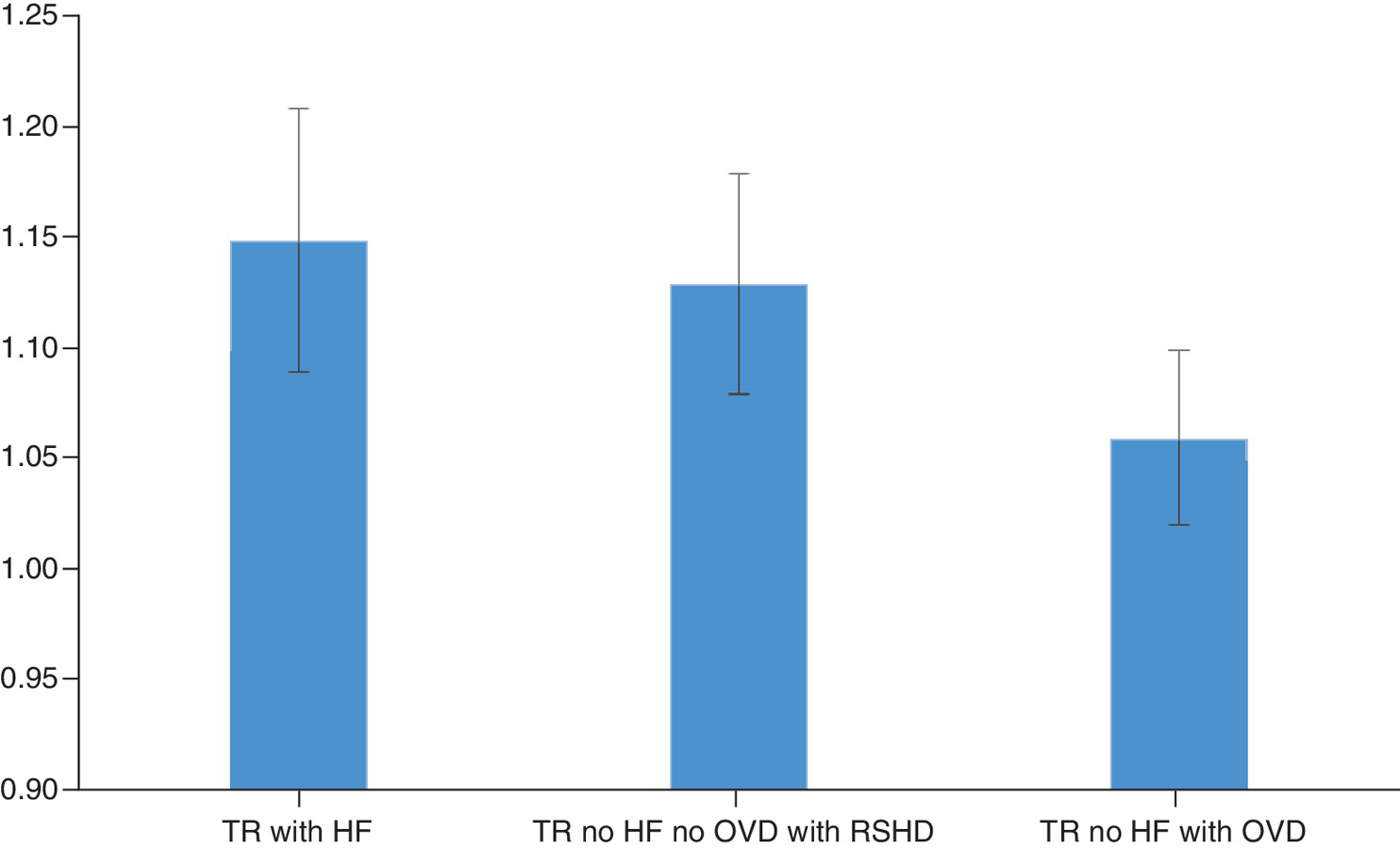
Figure 4. Estimated percent change in annualized all-cause expenditures (reference group: tricuspid regurgitation-only).
Multivariable models adjusted for age, sex, race, Elixhauser Comorbidity Index score, and TR severity.
HF: Heart failure; OVD: Other valve disease; RSHD: Right-sided heart disease; TR: Tricuspid regurgitation.
When TR severity was included as a covariate in the annualized hospital days and the expenditure models, it was found to be statistically significant.
Discussion
This retrospective database analysis of patients with clinically significant TR found that the presence of HF resulted in a larger annualized healthcare burden when compared with patients without HF, regardless of additional co-morbidities or severity. We observed that both all-cause and CV-related hospitalizations were highest for the TR with HF cohort compared with the other three cohorts without HF. Our results are consistent with the recent retrospective analysis by Cork et al., which also found that the annualized healthcare burden of patients with clinically significant TR and HF was greater than those with TR alone [6].
Their study examined data from the IBM® MarketScan® Research Databases over 5 years and found that patients with TR and HF had an annualized healthcare burden of 0.59 for all-cause hospitalizations (about three inpatient hospitalizations every 5 years) compared with 0.41 for patients with TR alone and 0.20 for patients with neither HF nor clinically significant TR. The annualized burden of all-cause hospitalizations in this analysis was slightly higher, but this study used data over 11 years (0.74 annualized all-cause hospitalization burden for the TR and HF cohort [about eight hospitalizations every 11 years] compared with 0.54 for the TR-only cohort). We also observed that RSHD and OVD resulted in a greater annualized burden of all-cause and CV-related hospitalizations, regardless of HF. However, the presence of HF in patients with TR still had the largest influence on the healthcare burden and associated expenditures.
Similarly, the TR plus HF group had the longest annualized hospital days (7.1) compared with the other cohorts, although RSHD and OVD were, again, found to have independent effects on annualized days relative to the TR-only group (6.4 and 6.0 days relative to 5.5 days, respectively). These findings were also consistent with the Cork et al. [6] study, albeit slightly larger (4.31 hospital days for patients with TR and HF vs 3.13 days for patients with TR alone). These findings suggest that whether or not TR was cause or consequence of RSHD, OVD or HF, its presence was clinically important and had financial ramifications.
We also found that the presence of any associated condition – RSHD, OVD or HF – increased annualized all-cause expenditures compared with patients with TR alone. HF had the most significant impact on overall expenditures, with a percent change of 15%. Unfortunately, we could not calculate total dollar amounts because of restrictions using Optum’s data. However, previous studies have shown that annualized expenditures of patients with TR and HF were greater than those with TR alone ($42,255 vs $29,985, respectively) [6].
Limitations
These results should be interpreted with caution for several reasons. We recognize that TR was ascertained through sources of automated data that rely on coding. This could have been biased in terms of over- or undercoding. We could only control for known confounders and lacked the ability to control for unknown confounders, ideally by randomization, stratification and matching. Statistical modeling was used to control for the potential confounding effect of known variables with between-group differences. While statistical models controlled for several factors, models could not control for some variables that are not included in an administrative database, such as echocardiography results. Proxies in automated data were relied upon that suggested significant TR without having the quantitation of TR from imaging data. The use of proxies could have significantly reduced the proportion of patients with severe TR, and our data analysis should not be interpreted as a prevalence study. A strength of the present study, however, is that the data reflect real-world patient characteristics and outcomes across the country from different hospitals and physicians as compared with evidence from controlled clinical trials.
Conclusion
The presence of RSHD, OVD or HF in patients with TR are all independently associated with an increase in annualized hospitalizations (all-cause and CV-related), hospital days and costs relative to patients with TR alone. Regardless of additional conditions, HF has the most significant impact on the annualized healthcare burden of patients with TR.
•
Tricuspid regurgitation (TR) is a prevalent valvular disorder in which blood flows backward through the tricuspid valve into the right atrium because the right ventricle is not closing properly.
•
Severe TR is associated with high morbidity and mortality, but may be overlooked and undertreated as a result of its complex pathology and its associated conditions.
•
The impact of co-morbid heart failure (HF) and severe TR has been established, but the impact of TR in the presence of other commonly associated conditions that cause right-ventricle dilation has not.
•
This analysis quantifies the incremental economic burden of conditions such as HF, right-sided heart disease (RSHD) and other valve disorders (OVD) in the presence of TR.
•
Using real-world data from Optum’s de-identified, all-payer, integrated database of United Healthcare claims and Humedica electronic health records, a hierarchical cohort was constructed consisting of: TR-only (reference group); TR with HF; TR with OVD (no HF); and TR with RSHD only (no OVD or HF).
•
The outcomes used to measure healthcare utilization and expenditures were all-cause hospitalizations, cardiovascular-related hospitalizations and hospital days.
•
All models adjusted for the following covariates: age, sex, race, Elixhauser Comorbidity Index score and TR severity.
•
RSHD and other valve diseases were found to have a higher annualized healthcare burden than the TR-only group, with RSHD having a stronger impact than other valve diseases.
•
Consistent with recent studies, the presence of HF in TR patients had the largest influence on healthcare utilization and expenditures.
•
Taken together, these findings suggest that whether TR is cause or consequence of RSHD, OVD or HF, its presence is clinically important and has financial ramifications.
Financial & competing interests disclosure
This study was sponsored by Edwards Lifesciences. The external authors and study sponsors participated in the study design, data analysis, data interpretation and development of the report, and gave approval to submit for publication. Relevant industry relationships and financial interests are as follows: CM Barker, DP Cork, PA McCullough, HS Mehta and C Gunnarsson have consulting relationships with Edwards Lifesciences. CM Barker is an advisory board member for Medtronic and Boston Scientific. DP Cork has a consulting relationship with Abbott Laboratories and participates in a speaker’s bureau for Boston Scientific. HS Mehta has a consulting relationship with Abbott Laboratories, Boston Scientific and participates in a speaker’s bureau for Actelion Pharmaceuticals, Bayer Healthcare Pharmaceuticals and Bristol-Myers Squibb Company. JV Houten, S Mollenkopf and P Verta are employees of Edwards Lifesciences, the study sponsor. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Stuge B, Holm I, Vollestad N. To treat or not to treat postpartum pelvic girdle pain with stabilizing exercises? Man. Ther. 11(4), 337–343 (2006).
2.
Benfari G, Antoine C, Miller WL et al. Excess mortality associated with functional ricuspid regurgitation complicating heart failure with reduced ejection fraction. Circulation 140(3), 196–206 (2019).
3.
Nath J, Foster E, Heidenreich PA. Impact of tricuspid regurgitation on long-term survival. J. Am. Coll. Cardiol. 43(3), 405–409 (2004).
4.
Harris C, Croce B, Munkholm-Larsen S. Tricuspid valve disease. Ann. Cardiothorac. Surg. 6(3), 294 (2017).
5.
Agarwal S, Tuzcu EM, Rodriguez ER, Tan CD, Rodriguez LL, Kapadia SR. Interventional cardiology perspective of functional tricuspid regurgitation. Circ. Cardiovasc. Interv. 2(6), 565–573 (2009).
6.
Cork DP, McCullough PA, Mehta HS et al. The economic impact of clinically significant tricuspid regurgitation in a large, administrative claims database. J. Med. Econ. 23(5), 521–528 (2020).
•• Investigated the healthcare burden of tricuspid regurgitation (TR) patients with and without heart failure (HF), concluding that irrespective of the presence of HF, clinically significant TR is associated with an increase in healthcare utilization and expenditures our current study bulids upon this article.
7.
Beckhoff F, Alushi B, Jung C et al. Tricuspid regurgitation – medical management and evolving interventional concepts. Front. Cardiovasc. Med. 5, 49 (2018).
8.
Topilsky Y, Nkomo VT, Vatury O et al. Clinical outcome of isolated tricuspid regurgitation. JACC Cardiovasc. Imaging 7(12), 1185–1194 (2014).
9.
Rodes-Cabau J, Hahn RT, Latib A et al. Transcatheter therapies for treating tricuspid regurgitation. J. Am. Coll. Cardiol. 67(15), 1829–1845 (2016).
10.
Antunes MJ, Barlow JB. Management of tricuspid valve regurgitation. Heart 93(2), 271–276 (2007).
11.
Sadeghpour A, Hassanzadeh M, Kyavar M et al. Impact of severe tricuspid regurgitation on long term survival. Res. Cardiovasc. Med. 2(3), 121–126 (2013).
12.
Lee JW, Song JM, Park JP, Lee JW, Kang DH, Song JK. Long-term prognosis of isolated significant tricuspid regurgitation. Circ. J. 74(2), 375–380 (2010).
13.
Bohbot Y, Chadha G, Delabre J, Landemaine T, Beyls C, Tribouilloy C. Characteristics and prognosis of patients with significant tricuspid regurgitation. Arch. Cardiovasc. Dis. 112(10), 604–614 (2019).
14.
Benjamin EJ, Muntner P, Alonso A et al. Heart Disease and Stroke Statistics-2019 Update: a report from the American Heart Association. Circulation 139(10), e56–e528 (2019).
15.
Nishimura RA, Otto CM, Bonow RO et al. 2014 AHA/ACC Guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation 129(23), 2440–2492 (2014).
16.
Zack CJ, Fender EA, Chandrashekar P et al. National trends and outcomes in isolated tricuspid valve surgery. J. Am. Coll. Cardiol. 70(24), 2953–2960 (2017).
17.
Topilsky Y, Maltais S, Medina Inojosa J et al. Burden of tricuspid regurgitation in patients diagnosed in the community setting. JACC Cardiovasc. Imaging 12(3), 433–442 (2019).
•• This is a recent estimate of TR prevalence at: approximately 0.55% in the USA, which is adjusted for age and sex.
18.
Mutlak D, Lessick J, Khalil S, Yalonetsky S, Agmon Y, Aronson D. Tricuspid regurgitation in acute heart failure: is there any incremental risk? Eur. Heart J. Cardiovasc. Imaging 19(9), 993–1001 (2018).
19.
Hahn RT, Waxman AB, Denti P, Delhaas T. Anatomic relationship of the complex rricuspid valve, Right ventricle, and pulmonary vasculature: a review. JAMA Cardiol. 4(5), 478–487 (2019).
20.
Optum. Optum integrated data (2015). https://www.optum.com/content/dam/optum3/optum/en/resources/fact-sheets/Integrated-Data-product-sheet.pdf
21.
Messika-Zeitoun D, Verta P, Gregson J et al. Impact of tricuspid regurgitation on survival in patients with heart failure: a large electronic health record patient-level database analysis. Eur. J. Heart Fail. (2020) (Epub ahead of print).
•• This is the latest publication that estimates the impact of severe TR on mortality among patients with HF and uses Optum’s data.
22.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med. Care 36(1), 8–27 (1998).
Information & Authors
Information
Published In
Pages: 29 - 37
PubMed: 33174767
Copyright
© 2020 Joanna Van Houten et al. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 September 2020
Accepted: 14 October 2020
Published online: 11 November 2020
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Healthcare utilization in clinically significant tricuspid regurgitation patients with and without heart failure. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0198
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Tochukwu R. Nzeako, Chukwuka Elendu, Ali Moradi, Olawale Olanisa, Adekunle Kiladejo, Percutaneous interventions in tricuspid valve disease: a new era in cardiac treatment, Annals of Medicine & Surgery, 10.1097/MS9.0000000000003437, 87, 7, (4262-4280), (2025).
- Mahesh V. Madhavan, Colin M. Barker, Lisa S. Kemp, Sarah Mollenkopf, Michael Ryan, Candace Gunnarsson, David J. Cohen, Real-World Clinical Outcomes and Health Care Utilization in Patients With Severe Tricuspid Regurgitation, Structural Heart, 10.1016/j.shj.2025.100463, 9, 5, (100463), (2025).
- Colin M. Barker, Lisa S. Kemp, Melissa Mancilla, Sarah Mollenkopf, Candace Gunnarsson, Michael Ryan, Guy David, Inequities in Access to Tricuspid Valve Treatments, JACC: Advances, 10.1016/j.jacadv.2024.101342, 3, 11, (101342), (2024).
- Ching-Hu Chung, Healthcare utilization and expenditures in patients with tricuspid regurgitation: A population-based cohort study, IJC Heart & Vasculature, 10.1016/j.ijcha.2024.101495, 54, (101495), (2024).
- Rongyang Xi, Muhammad Ahsan Mumtaz, Dingli Xu, Qingchun Zeng, Tricuspid Regurgitation Complicating Heart Failure: A Novel Clinical Entity, Reviews in Cardiovascular Medicine, 10.31083/j.rcm2509330, 25, 9, (2024).
- Mark A. Lebehn, Rebecca T. Hahn, Valvular Heart Failure due to Tricuspid Regurgitation, Heart Failure Clinics, 10.1016/j.hfc.2023.02.003, 19, 3, (329-343), (2023).
- Colin M. Barker, Kashish Goel, Transcatheter Tricuspid Interventions: Past, Present, and Future, Methodist DeBakey Cardiovascular Journal, 10.14797/mdcvj.1250, 19, 3, (57-66), (2023).