Impact of pain and nonpain co-morbidities on opioid use in women with endometriosis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate impact of co-morbidities on opioid use in endometriosis. Patients & m ethods: This was a retrospective analysis of data obtained from the Symphony Health database (July 2015–June 2018), which contains medical and pharmacy claims information on 79,947 women with endometriosis. Relative risk (RR) of postdiagnosis opioid use and supply duration associated with baseline co-morbidities were determined. Results: Women with endometriosis using opioids at baseline were 61% more likely to receive opioids postdiagnosis (RR: 1.61; 95% CI: 1.59–1.63). Risk of prolonged opioid supply postdiagnosis was highest for those with prolonged supply at baseline (RR: 21.14; 20.14–22.19), and was 1.32 (1.26–1.38) for patients with ≥1 co-morbidity, 1.37 (1.31–1.43) for pain co-morbidities and 1.07 (1.04–1.11) for psychiatric co-morbidities. Conclusion: Risk of opioid use after endometriosis diagnosis was greater in patients who used opioids before diagnosis. Risk of prolonged opioid use was greater if co-morbidities existed before diagnosis.
Lay abstract
In this study, researchers looked at patients with endometriosis and their use of certain types of pain relief, known as opioids. In particular, the study looked at whether having other conditions as well as endometriosis (‘co-morbidities’) affected the use of opioids, by looking at information found in an insurance claims database. The researchers found that women who were treated with opioids before they were diagnosed with endometriosis were 61% more likely to be treated with opioids after diagnosis. Risk of opioid use over a long period of time was greater in women who had more than one co-morbidity and in those who had various pain or psychiatric co-morbidities. These findings suggest that it is important to carefully screen patients with endometriosis for co-morbidities, to make sure pain is managed properly, to reduce the use of opioids where they are not needed and to lower the risk of opioid abuse.
Endometriosis, a chronic inflammatory disease, can present with a variety of symptoms, including chronic pelvic pain, dysmenorrhea, painful ovulation, dyspareunia, dysuria and dyschezia [1,2]. Women with endometriosis also experience menorrhagia, fatigue and infertility [2]. Moreover, endometriosis is associated with other co-morbid pain and psychiatric conditions such as irritable bowel syndrome, interstitial cystitis, fibromyalgia, anxiety and depression [3–5]. Consequently, the burden of endometriosis extends beyond symptoms, with negative impacts on mental health and women’s social and professional lives [6].
Current treatment guidelines for endometriosis emphasize the management of pain and infertility [1,2,7,8]. Most treatment guidelines recommend the use of nonsteroidal anti-inflammatory drugs, combined hormonal contraceptives, progestogens (or antiprogestogens), gonadotropin-releasing hormone agonists and antagonists, surgical fulguration or excision of endometrial lesions, or hysterectomy with and without bilateral salpingo-oophorectomy [1,2,7,8]. The majority of guidelines do not include recommendations to use opioid analgesics for pain management [1,8,9]. The Journal of Obstetrics and Gynaecology Canada endometriosis guideline is one of the few to suggest that physicians may use clinical judgment in prescribing analgesics, ranging from nonsteroidal anti-inflammatory drugs to opioids, while waiting for resolution of symptoms from directed medical or surgical treatments [7].
Despite the minimal role of opioids in endometriosis practice guidelines, a survey of American College of Obstetricians and Gynecologists (ACOG) members found that 24% of obstetricians/gynecologists prescribed opioids for endometriosis [10] and 89% prescribed opioids after laparoscopic hysterectomy [10]. Opioid-prescribing practices varied widely among obstetricians/gynecologists with a lack of adherence to published recommendations on opioid use from the Centers for Disease Control and Prevention and ACOG [7,11]. Consistent with the ACOG survey [10], a retrospective claims analysis found that 79% of women with endometriosis received ≥1 day’s supply of opioids after their diagnosis, most commonly after surgical procedures [12]. Notably, women with endometriosis were at greater risk of filling a longer-term opioid prescription and a prescription for a higher dose than women without endometriosis [12]. Lack of evidence-based guidelines for postoperative opioid prescribing among patients with gynecological conditions may contribute to excessive postsurgical opioid supply reported in several studies [12–14]. The prevalence of opioid prescriptions and the increased likelihood of prolonged opioid use among women with endometriosis is concerning in light of increasing rates of opioid abuse/overdose and limited evidence of efficacy in managing chronic pain [11]. Therefore, we sought to identify potential risk factors for opioid use and prolonged opioid use in women with endometriosis, which, although established in other patient populations, remain largely undefined in endometriosis.
Methods
Study design & data source
A retrospective analysis of United States administrative claims data was performed using data from the Symphony Health (previously Source Healthcare Analytics) claims database. Women with an International Classification of Diseases, Ninth Revision (ICD-9) code 617.x or Tenth Revision (ICD-10) code N80.x for endometriosis diagnosis on one inpatient or two outpatient claims (on two separate days) from January 2006 to November 2019 were identified. The date of the first endometriosis diagnosis was considered the index date, and the 1-year period preceding the index date was considered the baseline period. Women included in the analysis were aged 18–49 years at the index date and had continuous pharmacy and medical enrollment for ≥1 year before and after endometriosis diagnosis (i.e., at least one pharmacy claim every 3 months during the study period). Patients with a diagnosis of cancer or who underwent a radical hysterectomy at any time were excluded. The final sample included women with the first endometriosis diagnosis from 1 July 2015 to 30 June 2018.
Data analysis
The following three opioid use outcomes were assessed for the 1-year postdiagnosis period: whether opioids were dispensed (yes/no), duration of opioid supply (days) and receipt of prolonged (≥90 days’) opioid supply (yes/no). Opioid prescriptions included buprenorphine, butorphanol, codeine, dihydrocodeine, fentanyl, hydrocodone, hydromorphone, levorphanol, meperidine, methadone, morphine sulfate, oxycodone, oxymorphone, pentazocine, tapentadol and tramadol. The frequency of baseline opioid use (patients who had an opioid prescription) and duration of baseline opioid supply were assessed. The days’ supply of opioids during the baseline period and after diagnosis were also assessed. Receipt of ≥90-days' opioid supply means the total number of days opioids were prescribed to a patient was 90 days or greater over a 1-year period. Patients could have received one of several permutations (e.g., 3 × 30 days, 10 × 9 days or 7 × 12 days + 6 days). Regression modeling was used to describe associations between the postdiagnosis opioid-use outcomes and covariates during the baseline period. Covariates included demographic variables; opioid use (yes/no, prolonged supply); and the presence, number and type of co-morbidities. A total of 14 co-morbidities reported to occur with higher prevalence in women with endometriosis than in women without endometriosis [5,15] were included in this analysis (pain, psychiatric, nonpain gynecological conditions and other; ICD-9/-10 codes provided in Supplementary Table 1).
Categorical variables were analyzed descriptively using frequencies and continuous variables were analyzed using means, medians and standard deviation (SD). Linear regression models were used to determine the association between baseline covariates and postdiagnosis duration of opioid supply. Poisson regression models with robust standard errors (SE) were used to determine relative risk (RR) estimates of postindex opioid use and receipt of prolonged opioid supply associated with baseline covariates. All regression models adjusted for age, geographic region (regions based on the diagnosing physician’s location in the four United States Census Bureau geographic regions) and household income as independent variables. Statistical significance of differences between cohorts (defined based on covariates described above) and between prediagnosis and postdiagnosis variables were assessed using χ2 tests for categorical variables and analysis of variance and t-tests for continuous variables. p < 0.05 was considered statistically significant. All data analyses were performed using SAS version 9.4 (SAS Institute, NC, USA).
Results
Study population characteristics
Analysis of United States claims data from January 2006 to November 2019 in the Symphony Health claims database identified 2,580,645 patients diagnosed with endometriosis. Among female patients with endometriosis, 303,054 were aged 18–49 years at the time of the first endometriosis diagnosis; had received one inpatient or two outpatient endometriosis diagnoses; and received the first endometriosis diagnosis from 1 July 2015 to 30 June 2018 (Figure 1). After applying inclusion and exclusion criteria, data from 79,947 women with endometriosis were included in this analysis.
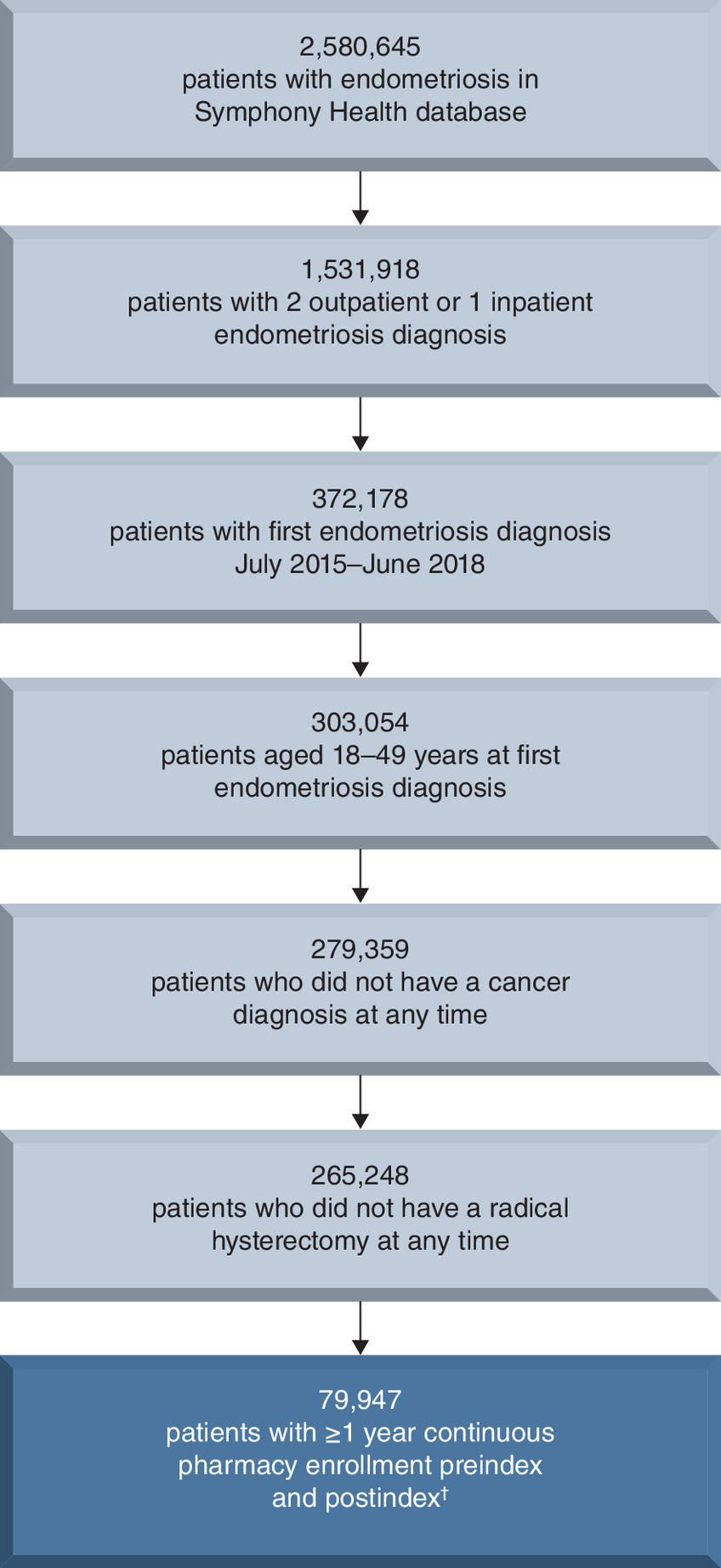
Figure 1. Study population attrition.
Stepwise selection criteria for patients whose claims data were included in the analysis. Bolded box indicates final sample.
†Continuous pharmacy eligibility with at least one pharmacy claim each quarter during study period.
Demographics of the study population are shown in Table 1. The mean (SD) age of women included in the analysis was 36.6 (8.0) years. The four United States geographic regions were relatively evenly represented by the study population, with a slightly higher representation of women from the Northeast (31.6%). Household income data were available for approximately 55% of women in this analysis.
| Parameter | n = 79,947 |
|---|---|
| Age at first endometriosis diagnosis, years: | |
| – Mean ± SD | 36.6 ± 8.0 |
| – Median (range) | 37 (18–49) |
| Age group at first endometriosis diagnosis (years), n (%): | |
| – 18–24 | 7406 (9.3) |
| – 25–29 | 9591 (12.0) |
| – 30–34 | 13,595 (17.0) |
| – 35–39 | 16,547 (20.7) |
| – 40–44 | 17,037 (21.3) |
| – 45–49 | 15,771 (19.7) |
| Race, n (%): | |
| – Caucasian | 32,372 (40.5) |
| – African American | 6846 (8.6) |
| – Hispanic | 4385 (5.5) |
| – Other | 1046 (1.3) |
| – Unknown | 35,298 (44.2) |
| Geographic location, n (%) | |
| – Northeast | 25,292 (31.6) |
| – Southeast | 19,434 (24.3) |
| – Central | 18,149 (22.7) |
| – West | 11,801 (14.8) |
| – Unknown | 5271 (6.6) |
| Household income, n (%): | |
| – $0–29,999 | 13,289 (16.6) |
| – $30,000–49,999 | 7306 (9.1) |
| – $50,000–74,999 | 6760 (8.5) |
| – $75,000–99,999 | 6010 (7.5) |
| – ≥$100,000 | 10,481 (13.1) |
| – Unknown | 36,101 (45.2) |
SD: Standard deviation.
During the baseline period, 63.9% of the study population had at least one co-morbidity (Table 2). Among the study population, 25.1% of women had one baseline co-morbidity, 17.6% had two and 21.2% had three or more co-morbidities. Approximately half of the study population had any of the seven specified pain co-morbidities and 29.5% had any of the three specified psychiatric co-morbidities. The most common pain co-morbidities were arthritis/joint pain (34.2%), back/neck pain (24.2%) and migraine/headache (12.0%) (Figure 2). Anxiety and episodic mood disorder/depression were present with comparable frequencies (21.8 and 18.6%, respectively).
| Parameter, n (%) | n = 79,947 |
|---|---|
| Patients with co-morbidities† | 51,068 (63.9) |
| Number of co-morbidities: | |
| – 0 | 28,879 (36.1) |
| – 1 | 20,042 (25.1) |
| – 2 | 14,063 (17.6) |
| – ≥3 | 16,963 (21.2) |
| Type of co-morbidity:‡,§ | |
| – Pain | 39,061 (48.9) |
| – Psychiatric | 23,612 (29.5) |
†
Women could have more than one co-morbidity.
‡
Women with more than one pain co-morbidity were counted only once within the number of patients with pain co-morbidities, and women with more than one psychiatric co-morbidity were counted only once within the number of patients with psychiatric co-morbidities.
§
Frequencies of specific co-morbidities (pain, psychiatric, nonpain gynecological and other) are shown in Figure 2.
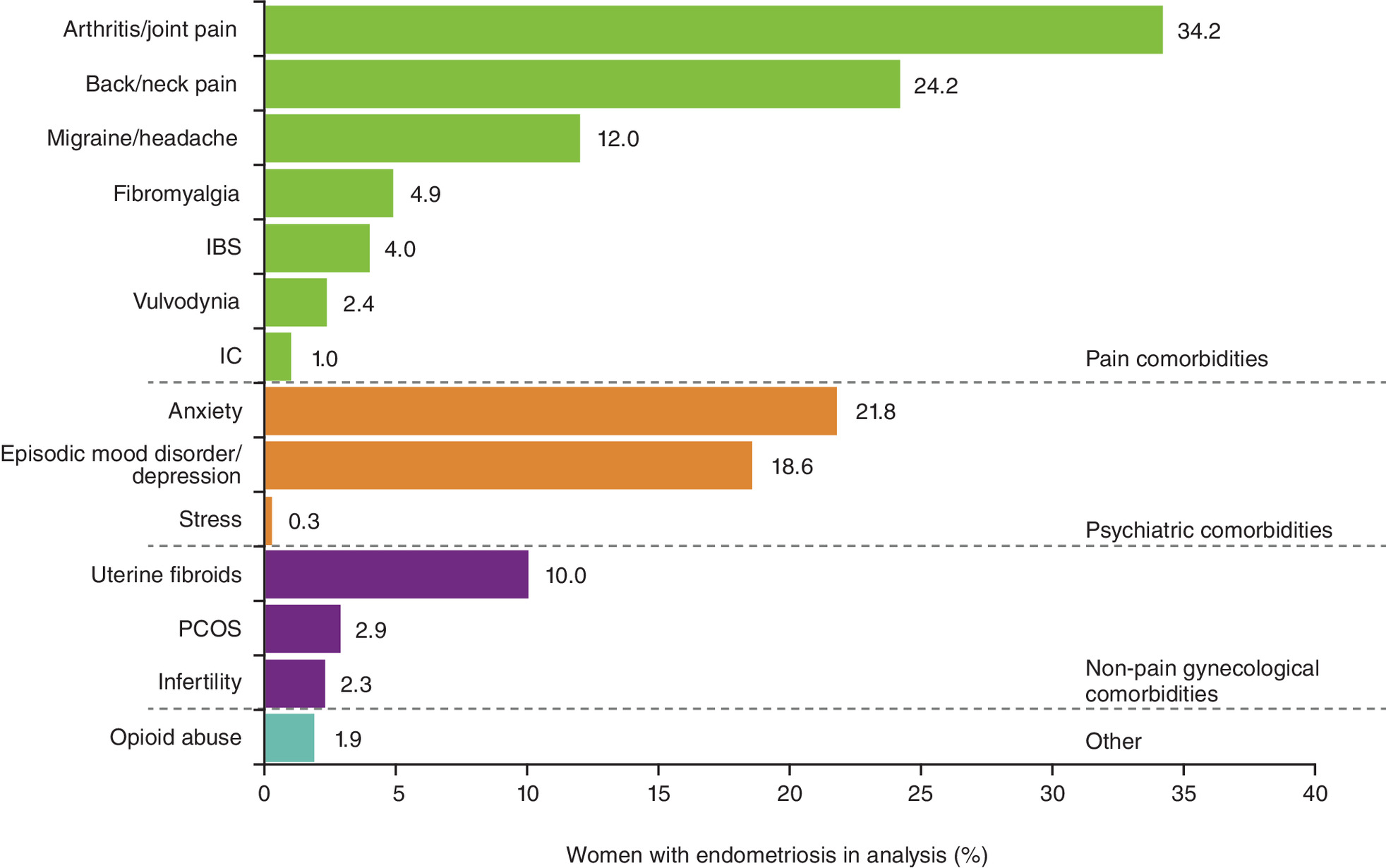
Figure 2. Frequency of co-morbidities during the baseline period.
Percentage of women with endometriosis in the study population (n = 79,947) with indicated co-morbidities, grouped into four overall categories (pain, psychiatric, nonpain gynecological and other co-morbidities). Women in the analysis could have more than one co-morbidity.
IBS: Irritable bowel syndrome; IC: Interstitial cystitis; PCOS: Polycystic ovary syndrome.
At baseline, 39.5% of patients had received an opioid prescription. Of all patients in this analysis, 27.3% had a baseline opioid supply of 1–30 days, 2.9% had a supply of 31–59 days, 1.6% had a supply of 60–89 days and 7.7% had a prolonged supply of ≥90 days. The mean (SD) days’ opioid supply for all patients during baseline was 26.4 (85.8) days. After diagnosis, 57% of all patients had received an opioid prescription. Among all patients after diagnosis, 8.7% had an opioid supply of ≥90 days; and the mean (SD) days’ opioid supply for all patients was 31.0 (91.9) days.
Opioid use risk factors
The greatest risk factor for opioid use after endometriosis diagnosis was opioid use before diagnosis. Women were 61% more likely to be prescribed opioids after endometriosis diagnosis if they had used opioids during the baseline period (adjusted RR ratio: 1.61; 95% CI: 1.59–1.63). The type of co-morbidity present during baseline (pain or psychiatric) had a minimal influence on the risk of being prescribed opioids after endometriosis diagnosis (pain co-morbidity adjusted RR ratio: 1.08; 95% CI: 1.07–1.10; psychiatric co-morbidity adjusted RR ratio: 1.05; 95% CI: 1.04–1.07). The number of co-morbidities present during baseline somewhat affected the risk of being prescribed opioids after endometriosis diagnosis. The presence of one co-morbidity during baseline had an adjusted RR ratio of 1.17 (95% CI: 1.16–1.19), two co-morbidities had an adjusted RR ratio of 0.94 (95% CI: 0.92–0.97) and three or more co-morbidities had an adjusted RR ratio of 1.08 (95% CI: 1.06–1.10) when compared with no baseline co-morbidities.
Factors associated with the duration of opioid supply
Linear regression models were run to evaluate the association of baseline factors with increased duration of opioid supply after endometriosis diagnosis. The duration of opioid supply in women with endometriosis was significantly greater (all p < 0.05) in those with at least one baseline co-morbidity compared with those without co-morbidities (Figure 3A). Women with one co-morbidity during baseline had a mean (SE) of 1.01 (0.49) additional days of opioid supply compared with women with no co-morbidities. Women with two and three or more co-morbidities had a mean (SE) of 3.16 (0.55) and 5.91 (0.53) additional days of opioid supply compared with women with no co-morbidities, respectively. Women with at least one of the specified pain co-morbidities during baseline had a mean (SE) of 3.89 (0.40) additional days of opioid use compared with women with none of the specified pain co-morbidities. Women with at least one of the three psychiatric co-morbidities evaluated had a mean (SE) of 1.32 (0.43) additional days of opioid use compared with women with none of the three psychiatric co-morbidities. Women with opioid abuse during the baseline period had a mean (SE) of 7.32 (1.43) additional days of opioid use postdiagnosis compared with women with no baseline opioid abuse. The following baseline co-morbid pain conditions were associated with the most added days of opioid supply compared with those in women without said co-morbidity: interstitial cystitis (mean [SE]: 8.32 [1.90]); back/neck pain (4.64 [0.49]) and fibromyalgia (3.55 [0.94]) (Figure 3B).
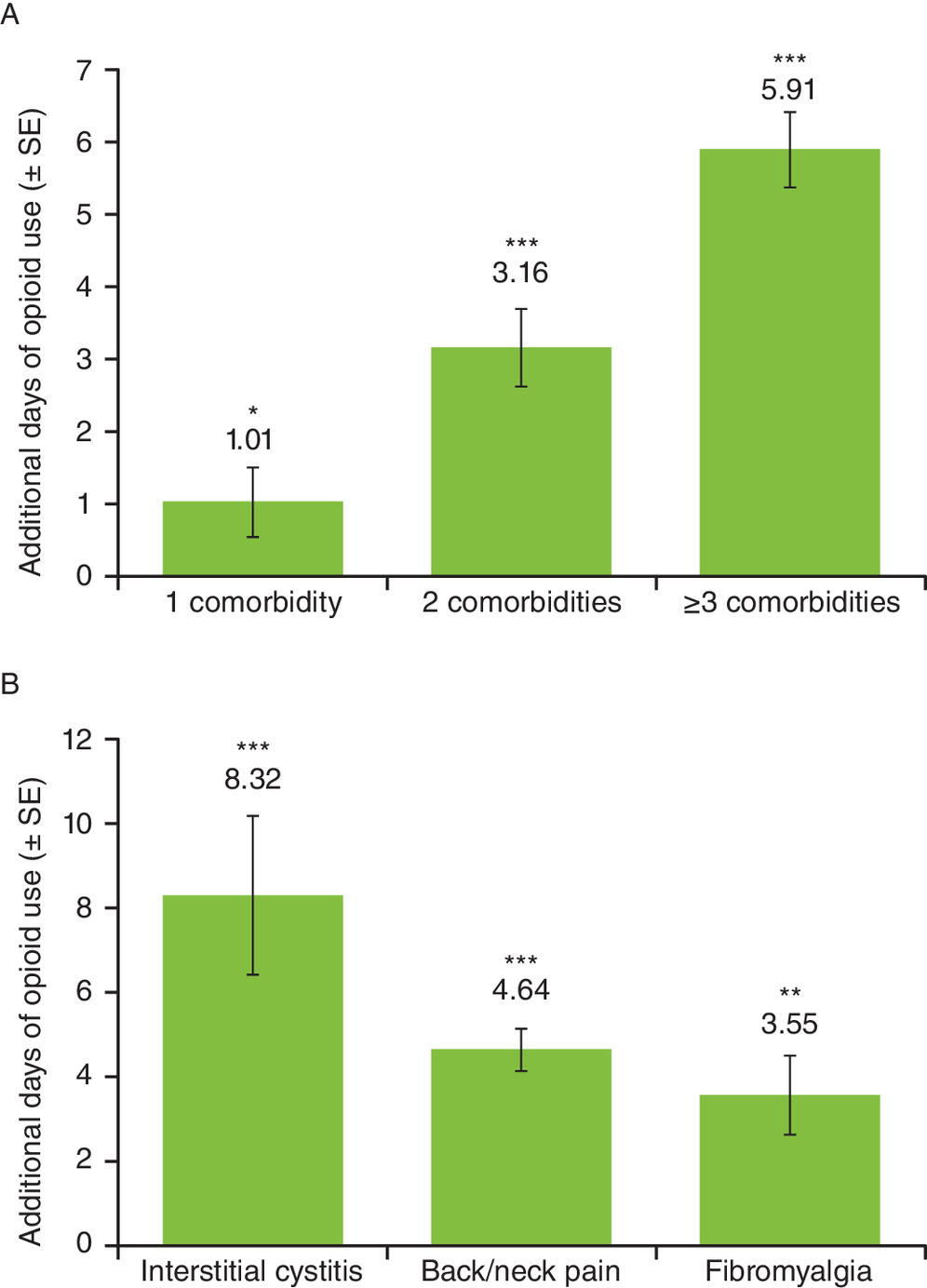
Figure 3. Association between co-morbidities and added days of opioid use.
Regression analysis estimates of days of added opioid use (A) in women with indicated number of co-morbidities versus women with no co-morbidities and (B) in women with indicated pain co-morbidity versus women without indicated pain co-morbidity. Error bars indicate ± SE; *p < 0.05; **p < 0.01; ***p < 0.001.
SE: Standard error.
Risk factors for prolonged (≥90 days') opioid supply
Poisson regression analyses were performed to assess baseline risk factors for prolonged (≥90 days') opioid supply after endometriosis diagnosis. The greatest risk factor was receipt of ≥90 days’ opioid supply during the baseline period (adjusted RR ratio: 21.14; 95% CI: 20.14–22.19) (Table 3). Additional risk factors included the presence of at least one co-morbidity during baseline, which was associated with a 32% greater risk of receiving a prolonged opioid supply postdiagnosis than that observed for women with no baseline co-morbidities. The presence of one or more of the specified pain co-morbidities during baseline was associated with a 37% greater risk of prolonged opioid supply postdiagnosis than that observed for women with none of these pain co-morbidities. Psychiatric co-morbidities (anxiety, episodic mood disorder and/or stress) during the baseline period were associated with a 7% greater risk of prolonged opioid supply than that observed for women with none of these psychiatric co-morbidities.
| Risk factors present during the baseline period† | Adjusted RR ratio (95% CI) | p-value |
|---|---|---|
| ≥90 days’ opioid supply | 21.14 (20.14–22.19) | <0.001 |
| ≥1 co-morbidity | 1.32 (1.26–1.38) | <0.001 |
| Pain co-morbidity | 1.37 (1.31–1.43) | <0.001 |
| Psychiatric co-morbidity | 1.07 (1.04–1.11) | 0.001 |
†
Additional covariates assessed in this regression model included age, geographic region, household income and the four nonpain, nonpsychiatric co-morbidities (opioid abuse, infertility, polycystic ovary syndrome and uterine fibroids).
RR: relative risk.
Discussion
Recent research shows that opioids are used in a significant number of women with endometriosis for acute pain management in postsurgical settings and for management of chronic pain [10,12–14]. Despite wide use, few guidelines are available on when or how to use opioids for the treatment of endometriosis-associated pain [1,8,9,16], while data continue to emerge on the potential negative consequences of opioid use in the general population [11,17–19]. In the current analysis, we found that before endometriosis diagnosis, 39.5% of women with endometriosis had received an opioid prescription and almost 8% received a prolonged (≥90 days’) opioid supply. Opioid use prior to diagnosis was the greatest risk factor for opioid use after diagnosis. Likewise, the greatest risk factor for receiving a prolonged (≥90 days’) opioid supply after diagnosis was having received a prolonged opioid supply before diagnosis.
Many studies have reported a high co-morbidity burden among patients with endometriosis [4,5,20,21]. One study found that 65% of women with endometriosis had three or more co-morbidities at the time of diagnosis, which increased to 85% by 2 years postdiagnosis [5]. Among endometriosis-associated co-morbidities, pain and psychiatric conditions are highly prevalent [3–5,12,22,23]. Research has revealed a complex association between pain and psychiatric disorders; chronic pain negatively affects mental health, but psychological disorders such as depression may also amplify pain conditions [3,21,24]. Indeed, patients with severe endometriosis-associated pain are more likely to have multiple psychiatric disorders [21]. Given the significant co-morbidity burden in patients with endometriosis and the inter-relatedness of pain and psychiatric co-morbidities, we reasoned that these co-morbidities may influence opioid use for endometriosis-associated pain management.
In this retrospective claims analysis, both the type and number of baseline co-morbidities influenced the duration of opioid supply after diagnosis. The presence of one of the specified pain or psychiatric co-morbidities significantly increased the number of days of prescribed opioid supply when compared with the number of days of prescribed opioid supply in patients without that specific baseline pain or psychiatric co-morbidity. In particular, baseline interstitial cystitis, back/neck pain and fibromyalgia were associated with significantly increased added days of opioid supply. Having two or more baseline co-morbidities was also associated with added days of opioid supply, which increased with each additional co-morbidity. Furthermore, women with more than one co-morbidity before diagnosis were at an increased risk of receiving an opioid supply of ≥90 days, particularly if a pain co-morbidity was present.
Opioid use trends in the treatment of endometriosis are concerning for multiple reasons. First, there is limited evidence to suggest that long-term opioid therapy is effective in treating other chronic (>3 months) pain conditions; clinical trials have only demonstrated efficacious analgesia lasting 12 weeks or less [11]. Second, the risk of opioid-related adverse events is correlated with the dose and duration of opioid use [16,17,19] and can include the development of opioid-induced hyperalgesia, which counterproductively amplifies pain [25]. Third, some evidence indicates that high daily doses and prolonged use of opioids for chronic noncancer pain increase the risk of opioid abuse [11,18]. This remains contentious, as other studies have found that only a small percentage of patients with chronic pain receiving long-term opioid therapy develop opioid abuse disorders [26,27]. Finally, co-morbid psychiatric disorders in patients with chronic pain conditions (e.g., low back pain) are associated with opioid misuse [28,29]. The high prevalence of psychiatric co-morbidities in patients with endometriosis [3,5,12,21,22] suggests that this population may be vulnerable to opioid misuse. Optimal endometriosis treatment should take a patient-centric approach, integrating pharmacological and surgical options to manage symptoms in conjunction with therapies to improve health-related quality of life (e.g., physiotherapy, acupuncture, mental health counseling) [8,30]. Opioids may effectively manage pain for some patients with endometriosis, but their use should be carefully considered and weighed against potential harms [11,16].
The results of our analysis reinforce the need for comprehensive co-morbidity screening in patients with endometriosis to guide treatment decisions (i.e., whether to initiate opioid therapy) and identify patients at increased risk of prolonged opioid use. There are several risk assessment tools that can be implemented in clinical practice to facilitate weighing the risks and benefits of opioid therapy for individual patients [16]. If patients and healthcare providers agree to initiate opioid therapy, appropriate patient counseling is recommended, including setting realistic pain management and evaluation goals and informing the patient of the risks associated with opioid use [11,16]. Increased awareness and recognition of aberrant drug-related behaviors is needed among healthcare providers to mitigate opioid abuse [10,11,16]. Overall, multidisciplinary care with adequate management of co-morbidities may optimize endometriosis management and reduce inappropriate or excessive treatment with opioids.
To our knowledge, this is the first study to investigate potential prediagnosis risk factors for opioid use and receipt of prolonged opioid supply in women after endometriosis diagnosis. The results of our study must be viewed within the context of the following limitations. Women with endometriosis who were included in this analysis were identified based on diagnostic codes, which do not provide information on the method of diagnosis or whether diagnosis was surgically confirmed. Our analysis captured the first occurrence of endometriosis diagnosis in the database, which may not necessarily reflect the first-ever diagnosis of endometriosis. We tried to account for this possibility by requiring patients to have no sign of endometriosis in the 12 months prior to the first occurrence of an endometriosis diagnostic code. This analysis relied on the completeness of administrative claims to fully capture endometriosis-related treatments and symptoms. As pharmacy claims are not associated with a diagnosis code, opioid use could not be fully attributed to endometriosis pain. Moreover, claims for opioid prescriptions merely indicated that a prescription was filled but could not confirm whether prescribed opioids were used compliantly.
While the regression analyses herein controlled for demographic variables, other unobservable factors could have affected the assessed outcomes. The severity of endometriosis pain and of co-morbidities was not controlled for, both of which may have influenced opioid use. In general, the prevalence rates of co-morbid conditions in our analysis were lower than rates reported in the literature [4,21–23]. However, the frequencies of co-morbidities in this analysis were based on claims with co-morbidity diagnostic codes incurred before endometriosis diagnosis. Thus, our analysis does not reflect the true prevalence of co-morbidities among women diagnosed with endometriosis, as patients may receive a diagnosis of a co-morbidity after endometriosis diagnosis or develop further co-morbidities over time. Finally, results of this analysis may not be generalizable to the overall population of women with endometriosis, but rather only to commercially insured, reproductive-aged patients. Despite these limitations, particular strengths of the analysis included assessment of many covariates and circumventing reporting bias by using claims data. Another strength was the large study sample, with data from a geographically and socioeconomically diverse United States commercial insurance database.
Conclusion
Analysis of United States claims data from 79,947 women with endometriosis indicates that opioid use before endometriosis diagnosis significantly increases the risk of opioid use after diagnosis. Prolonged (≥90 days') opioid supply before endometriosis diagnosis greatly increases the risk of prolonged opioid supply after diagnosis, as does the presence of at least one co-morbidity, particularly pain conditions. Although further research is needed to evaluate the effects of both short- and long-term opioid use among women with endometriosis, the insights gained from this retrospective claims analysis may contribute to improved management strategies for endometriosis-related pain and associated co-morbidities and optimization of opioid prescribing practices.
•
Risk factors for opioid use and prolonged opioid use in women with endometriosis are largely unknown but are important to understand given limited evidence for long-term efficacy of opioids and increasing rates of opioid abuse.
•
At baseline, 63.9% of women in this analysis had a co-morbidity, 48.9% had a co-morbid pain condition and 29.5% had a co-morbid psychiatric condition.
•
Women were 61% more likely to be prescribed opioids after the diagnosis of endometriosis if they used opioids during the baseline period (relative risk [RR] ratio = 1.61; 95% CI: 1.59–1.63).
•
The type of co-morbidity present during baseline (pain or psychiatric) had a minimal influence on the risk of being prescribed opioids after endometriosis diagnosis (pain co-morbidity-adjusted RR ratio = 1.08; 95% CI: 1.07–1.10; psychiatric co-morbidity-adjusted RR ratio = 1.05; 95% CI: 1.04–1.07).
•
The number of co-morbidities present during the baseline period somewhat affected the risk of being prescribed opioids after endometriosis diagnosis. The presence of one co-morbidity had an adjusted RR ratio of 1.17 (95% CI: 1.16–1.19), two co-morbidities had an adjusted RR ratio of 0.94 (95% CI: 0.92–0.97) and three or more co-morbidities had an adjusted RR ratio of 1.08 (95% CI: 1.06–1.10) when compared with no baseline co-morbidities.
•
Women with at least one of the specified pain co-morbidities during the baseline period had a mean (standard error [SE]) of 3.89 (0.40) additional days of opioid use compared with women with none of the specified pain co-morbidities.
•
The greatest risk factor for prolonged opioid supply (≥90 days) after diagnosis of endometriosis was prolonged opioid supply (≥90 days) during the baseline period (adjusted RR ratio = 21.14; 95% CI: 20.14–22.19; p < 0.001).
•
Women were at a 32% higher risk of receiving a prolonged supply of opioids (≥90 days) if they had ≥1 co-morbidity versus no co-morbidities during the baseline period (adjusted RR ratio = 1.32; 95% CI: 1.26–1.38; p < 0.001).
•
The risk of prolonged opioid supply increased by 37% in women with a pain co-morbidity versus those without a pain co-morbidity (adjusted RR ratio = 1.37; 95% CI: 1.31–1.43; p < 0.001) and by 7% in those with a psychiatric co-morbidity versus those without a psychiatric co-morbidity (adjusted RR ratio = 1.07; 95% CI: 1.04–1.11; p < 0.001).
•
Risk of opioid use after endometriosis diagnosis was greater in patients who used opioids before diagnosis, and risk of prolonged opioid use was greater if co-morbidities existed before diagnosis.
Author contributions
All authors substantially contributed to the development and critical revision of the intellectual content and approved the final version.
Acknowledgments
Data were presented at the International Pelvic Pain Society (IPPS) 2019 Annual Scientific Meeting on Pelvic Pain, 17–20 October 2019, Toronto, Ontario, Canada.
Financial & competing interests disclosure
This study was funded by AbbVie Inc. AbbVie sponsored the study; contributed to the design; participated in collection, analysis and interpretation of data; and in writing, reviewing and approval of the final version. G Lamvu has received research support from Pfizer and is a research consultant for AbbVie and Uroshape LLC. AM Soliman, B Johns and JB Vora are AbbVie employees and own stock/stock options. SJ Estes is a faculty member at Penn State Hershey Medical Center and has served in a consulting role for and has received research support from AbbVie. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by Emily Mercadante, PhD, of JK Associates, Inc., a member of the Fishawack Group of Companies, Conshohocken, PA, USA, and was funded by AbbVie Inc., North Chicago, IL, USA.
Ethical conduct of research
Ethical approval was not required as this is a retrospective analysis of administrative claims data.
Data sharing statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_data.docx)
- Download
- 68.91 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
The American College of Obstetricians and Gynecologists. Practice bulletin no. 114: management of endometriosis. Obstet. Gynecol. 116(1), 223–236 (2010).
2.
Kennedy S, Bergqvist A, Chapron C et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum. Reprod. 20(10), 2698–2704 (2005).
3.
Laganà AS, La Rosa VL, Rapisarda AMC et al. Anxiety and depression in patients with endometriosis: impact and management challenges. Int. J. Womens Health 9, 323–330 (2017).
4.
Sinaii N, Cleary SD, Ballweg ML, Nieman LK, Stratton P. High rates of autoimmune and endocrine disorders, fibromyalgia, chronic fatigue syndrome and atopic diseases among women with endometriosis: a survey analysis. Hum. Reprod. 17(10), 2715–2724 (2002).
5.
Surrey ES, Soliman AM, Johnson SJ, Davis M, Castelli-Haley J, Snabes MC. Risk of developing comorbidities among women with endometriosis: a retrospective matched cohort study. J. Womens Health (Larchmt) 27(9), 1114–1123 (2018).
6.
Culley L, Law C, Hudson N et al. The social and psychological impact of endometriosis on women’s lives: a critical narrative review. Hum. Reprod. Update 19(6), 625–639 (2013).
7.
Leyland N, Casper R, Laberge P, Singh SS. Endometriosis: diagnosis and management. J. Obstet. Gynaecol. Can. 32(7 Suppl. 2), S1–S3 (2010).
8.
Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis: a committee opinion. Fertil. Steril. 101(4), 927–935 (2014).
9.
Dunselman GA, Vermeulen N, Becker C et al. ESHRE guideline: management of women with endometriosis. Hum. Reprod. 29(3), 400–412 (2014).
10.
Madsen AM, Stark LM, Has P, Emerson JB, Schulkin J, Matteson KA. Opioid knowledge and prescribing practices among obstetrician-gynecologists. Obstet. Gynecol. 131(1), 150–157 (2018).
• Survey showing that current opioid prescribing practices vary widely among obstetricians and gynecologists.
11.
Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain–United States, 2016. JAMA 315(15), 1624–1645 (2016).
•• CDC guideline developed to improve communication between clinicians and patients about the benefits and risks of long-term opioid therapy for chronic pain, including misuse, overdose and death.
12.
Lamvu G, Soliman AM, Manthena SR, Gordon K, Knight J, Taylor HS. Patterns of prescription opioid use in women with endometriosis: evaluating prolonged use, daily dose, and concomitant use with benzodiazepines. Obstet. Gynecol. 133(6), 1120–1130 (2019).
•• Retrospective cohort study showing that opioid use is prevalent among women with endometriosis compared with those without endometriosis. The findings of this study emphasize the need for better healthcare provider education and appropriate patient selection and counseling before selecting opioids for pain management.
13.
As-Sanie S, Till SR, Mowers EL et al. Opioid prescribing patterns, patient use, and postoperative pain after hysterectomy for benign indications. Obstet. Gynecol. 130(6), 1261–1268 (2017).
•• Results of a prospective quality initiative study showed that gynecologists prescribe twice the amount of opioids as the average person uses after hysterectomy and suggest that a personalized approach to prescribing opioids for postoperative pain be implemented that utilizes opioid and nonopioid strategies.
14.
Surrey ES, Soliman AM, Yang H, Du EX, Su B. Treatment patterns, complications, and health care utilization among endometriosis patients undergoing a laparoscopy or a hysterectomy: a retrospective claims analysis. Adv. Ther. 34(11), 2436–2451 (2017).
15.
Soliman AM, Yang H, Du EX, Wu EQ, Castelli-Haley J, Winkel C. Comorbidities and symptoms among endometriosis patients: a systematic literature review. Value Health 19(3), A172 (2016).
16.
Findley AD, Kemner E. Selecting the appropriate patient for opioid therapy: risk assessment and treatment strategies for gynecologic pain. Clin. Obstet. Gynecol. 62(1), 48–58 (2019).
• The goal of this article is to help physicians identify patients who may benefit from opioid therapy for gynecologic pain and aid in establishing treatment goals, selecting appropriate medications, monitoring efficacy of treatment and developing a plan for periodic reassessment to determine when discontinuation of opioid therapy is appropriate.
17.
Chou R, Turner JA, Devine EB et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann. Intern. Med. 162(4), 276–286 (2015).
18.
Edlund MJ, Martin BC, Russo JE, Devries A, Braden JB, Sullivan MD. The role of opioid prescription in incident opioid abuse and dependence among individuals with chronic noncancer pain: the role of opioid prescription. Clin. J. Pain 30(7), 557–564 (2014).
• The study provides data on how exposure to different levels of prescribed opioids affects the likelihood of an opioid use disorder in patients experiencing a new episode of chronic pain who were not previously prescribed opioids.
19.
Els C, Jackson TD, Kunyk D et al. Adverse events associated with medium- and long-term use of opioids for chronic non-cancer pain: an overview of Cochrane reviews. Cochrane Database Syst. Rev. 10, CD012509 (2017).
20.
Mirkin D, Murphy-Barron C, Iwasaki K. Actuarial analysis of private payer administrative claims data for women with endometriosis. J. Manag. Care Pharm. 13(3), 262–272 (2007).
21.
Vannuccini S, Lazzeri L, Orlandini C et al. Mental health, pain symptoms and systemic comorbidities in women with endometriosis: a cross-sectional study. J. Psychosom. Obstet. Gynaecol. 39(4), 315–320 (2018).
• This cross-sectional study provides evidence that severe endometriosis-related pain is associated with psychiatric symptoms indicative of the presence of somatic symptom disorder.
22.
Soliman AM, Coyne KS, Gries KS, Castelli-Haley J, Snabes MC, Surrey ES. The effect of endometriosis symptoms on absenteeism and presenteeism in the workplace and at home. J. Manag. Care Spec. Pharm. 23(7), 745–754 (2017).
23.
Ferrero S, Pretta S, Bertoldi S et al. Increased frequency of migraine among women with endometriosis. Hum. Reprod. 19(12), 2927–2932 (2004).
24.
Steele A. Opioid use and depression in chronic pelvic pain. Obstet. Gynecol. Clin. North Am. 41(3), 491–501 (2014).
25.
Lee M, Silverman SM, Hansen H, Patel VB, Manchikanti L. A comprehensive review of opioid-induced hyperalgesia. Pain Physician 14(2), 145–161 (2011).
26.
Fields HL. The doctor’s dilemma: opiate analgesics and chronic pain. Neuron 69(4), 591–594 (2011).
27.
Fishbain DA, Cole B, Lewis J, Rosomoff HL, Rosomoff RS. What percentage of chronic nonmalignant pain patients exposed to chronic opioid analgesic therapy develop abuse/addiction and/or aberrant drug-related behaviors? A structured evidence-based review. Pain Med. 9(4), 444–459 (2008).
28.
Barry DT, Cutter CJ, Beitel M, Kerns RD, Liong C, Schottenfeld RS. Psychiatric disorders among patients seeking treatment for co-occurring chronic pain and opioid use disorder. J. Clin. Psychiatry 77(10), 1413–1419 (2016).
• This study found a high prevalence of anxiety disorder, mood disorder, nonopioid substance abuse disorder or personality disorder among patients seeking treatment for co-occurring opioid use disorder and chronic pain. These findings suggest that effective treatments for co-occurring chronic pain and opioid dependence may need to include treatment for co-occurring psychiatric disorders.
29.
Haller DL, Acosta MC. Characteristics of pain patients with opioid-use disorder. Psychosomatics 51(3), 257–266 (2010).
30.
As-Sanie S, Black R, Giudice LC et al. Assessing research gaps and unmet needs in endometriosis. Am. J. Obstet. Gynecol. 221(2), 86–94 (2019).
Information & Authors
Information
Published In
Pages: 17 - 27
PubMed: 33140993
Copyright
© 2020 Abbvie Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 18 August 2020
Accepted: 12 October 2020
Published online: 3 November 2020
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact of pain and nonpain co-morbidities on opioid use in women with endometriosis. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0181
Export citation
Select the citation format you wish to export for this article or chapter.