Clinical and economic impact of oxidized regenerated cellulose for surgeries in a Chinese tertiary care hospital
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the impact of oxidized regenerated cellulose (ORC) on blood transfusion and hospital costs associated with surgeries. Patients & methods: This retrospective cohort study selected ten surgeries to create propensity-score matching groups to compare ORC versus nonORC (conventional hemostatic techniques such as manual pressure, ligature and electrocautery). Results: NonORC was associated with both higher blood transfusion volume and higher hospital costs than ORC in endoscopic transnasal sphenoidal surgery, nonskull base craniotomy, hepatectomy, cholangiotomy, gastrectomy and lumbar surgery. However, nonORC was associated with better outcomes than ORC in open colorectal surgery, mammectomy and hip arthroplasty surgery. Conclusion: When compared with conventional hemostatic technique, using ORC could impact blood transfusion and hospital costs differently by surgical settings.
Bleeding is a common intraoperative complication increasing the risk of infection, postoperative complications and transfusion-related adverse events, which require longer hospital length of stay (LOS) and more health resources utilization [1,2]. Absorbable hemostatic agents (AHA) have been used as adjunctive therapy in surgeries when bleeding is not controlled by conventional methods [3]. Previous clinical evidence has suggested that AHA is effective in controlling capillary bleeding, achieving hemostasis during vascular surgery and controlling bleeding from fistula-puncture sites [4]. For example, oxidized regenerated cellulose (ORC), the most typical AHA, can assist in the control of capillary, venous and small arterial hemorrhage when ligation, electrocoagulation or other conventional methods to control bleeding are impractical or ineffective [5]. ORC facilitates hemostasis likely through the activation of the intrinsic coagulation pathway and also creating a gel-like layer (matrix) that holds clots in place and triggers vasoconstriction by the low pH of the ORC [6].
AHA is essentially needed for bleeding control in neurosurgery [7], hepatectomy [8], spine surgery [9] and vascular surgery [10]. Even though AHA has been used for two decades in China, AHA is rarely assessed for its impact on surgical outcomes and medical costs by surgery settings. Additionally, some Chinese hospitals had restricted the use of AHA irrespective of surgery setting to control budget since June 2016. This practice has raised concerns about the safety and quality of surgeries that are highly correlated with surgery bleeding [11]. With the recognition of the impact of using AHA on the safety and quality of surgery, the Chinese hospitals started to review the AHA restriction policy and seek evidence that could guide the appropriate use of AHA. Thus, this study selected one of the Chinese tertiary hospitals implementing AHA restriction use policy to clarify the impact of no AHA use on blood transfusion and hospital costs in common surgery settings.
Patients & methods
This study selected a Chinese titer III tertiary care hospital, Xiangya Hospital, which did not supply ORC due to budget control in most surgeries since 1 June 2016, as the study setting to retrospectively identify hospital episodes before and after 1 June 2016 to assess the clinical and economic impact associated with ORC use in common surgery settings. Ethical approval was obtained from the Institutional Review Board of Xiangya Hospital.
Patient identification
This study retrospectively identified the patients who underwent ten types of surgeries before and after the stop of supplying ORC in Xiangya Hospital. The rank of the annual surgery volumes in the study hospital was used to guide the selection of surgical settings for the assessment. This study finally included ten surgery settings to identify eligible patients for assessment. These ten surgery settings included three neurosurgeries (endoscopic transnasal sphenoidal surgery [ESTSS], nonskull base craniotomy [NSBC] and cerebrovascular surgery [CVS]), five general surgeries (hepatectomy, open gastrectomy, cholangiotomy, open colorectal surgery and mammectomy) and two orthopedics surgeries (hip arthroplasty surgery and lumbar fusion surgery). The identified patients were further assessed for their eligibility according to the following inclusion and exclusion criteria. The inclusion criteria included the following: patients with age of 18 years or above; patients with using ORC in the above selected ten surgeries from 1 January 2015 to 31 May 2016, and patients without using ORC in the selected ten surgeries from 1 June 2016 to 31 December 2017; patients with general anesthesia for their surgeries; patients were routinely admitted from outpatient settings; and patients were routinely discharged from the study hospital. The patients will be excluded if any of the following criteria were met: patient medical records were missing or incomplete, patients had two or more irrelevant surgeries in the same hospital episode, patients had legal-defined viral diseases (viral hepatitis and human immunodeficiency virus), patients had coagulation disorders (such as hemophilia) and patients with top 2.5% of bleeding volume as the extremely high bleeding volume may due to unexpected circumstances during surgery (such as massive bleeding due to accidentally injuring the artery).
The patients using ORC in the selected ten surgeries from 1 January 2015 to 31 May 2016 were included to create the ‘ORC group’. The patients without using ORC in the selected ten surgeries from 1 June 2016 to 31 December 2017 were included to create the ‘nonORC group’ after stopping the supply of ORC. The hemostasis methods used to control the bleeding in the surgery settings for the ‘nonORC group’ included manual pressure, ligation, electrocoagulation or other conventional hemostasis methods.
Data sources
The data sources in this study were the medical and billing records associated with the hospital episode of the surgeries in the included patients. The medical records included hospital medical summary sheet, surgery anesthesia records, surgical notes, medical notes and laboratory test results. The hospital medical summary sheet was used to extract patient demographics, socio-economic status, admission diagnoses, LOS, surgery methods, and complications. The anesthesia record was used to extract operation time. The surgical notes included information regarding surgery indication, operation site, procedure types, bleeding volume and intraoperative blood transfusion. The laboratory tests before surgery were used to extract the results of blood tests indicating bone marrow function and coagulation function. Additionally, the billing records were used to extract health resources utilization, including the use of blood for transfusion, and medical costs classified by categories.
Outcome measures
The primary outcome measures in this study were the occurrence of intraoperative blood transfusion, blood transfusion volume (based on the used blood units from the billing records, one blood unit was 200 ml), operation time and postsurgery LOS. This study also included hospital costs to clarify the economic impact of restricting ORC use. All costs were adjusted to 2017 Chinese currency according to the Chinese National Consumer Price Index from 2016 to 2017 [12].
Data analysis
This study stratified the patients by ten surgical settings to conduct the following analysis and assessed the impact of not using ORC on the measured outcomes through comparisons with using ORC. The created ‘ORC group’ and ‘nonORC group’ for each surgery setting were included to conduct the following analyses. This study used the propensity-score methods for adjusted comparisons of the measured outcomes associated with the created two groups. The patient baseline characteristics of the two groups were compared with the Student’s t-test or chi-square test to identify the patient characteristics with significant differences between the two groups. These identified patient characteristics were further used to create propensity-score matched groups to compare measured outcomes. The created propensity-score matched groups were compared by using paired Student’s t-test for continuous outcomes, McNemar test for categorical outcomes and Wilcoxon signed-rank test for hospital costs. Statistical software R was used to perform the data analysis described above. The statistical significance in the performed data analyses was defined as a two-sided p-value less than 0.05.
Results
This study initially identified 15,537 patients who underwent the selected ten surgeries from the two defined time windows. After inclusion and exclusion, a total of 5323 patients were included to create propensity score-matched groups for nonORC group versus ORC group for the ten selected surgeries, respectively. The patient identification process from initial screening to creating propensity-score matched groups for the selected ten surgeries is summarized in Table 1.
| Surgery category | Selected neurosurgeries | Selected general surgeries | Selected bone surgeries | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Surgery method | Endoscopic transnasal sphenoidal surgery | Nonskull base craniotomy | Cerebrovascular surgery | Hepatectomy | Open gastrectomy | Cholangiotomy | Open colorectal surgery | Mammectomy | Hip arthroplasty surgery | Lumbar surgery | |
| Initially identified patients | 941 | 2378 | 1768 | 800 | 965 | 737 | 654 | 4134 | 1059 | 2101 | |
| Patent exclusion reasons | Age under 18 years | 29 | 122 | 64 | 0 | 2 | 1 | 3 | 53 | 0 | 22 |
| Admission not from the outpatient setting | 22 | 112 | 846 | 11 | 23 | 55 | 18 | 6 | 45 | 41 | |
| Nonroutine discharge | 6 | 50 | 27 | 3 | 4 | 3 | 4 | 1 | 6 | 49 | |
| Not general anesthesia | 1 | 5 | 1 | 1 | 2 | 2 | 0 | 1463 | 546 | 8 | |
| Missing or incomplete information | 175 | 397 | 113 | 88 | 179 | 140 | 113 | 402 | 47 | 554 | |
| Legally reported viral diseases | 29 | 83 | 25 | 166 | 51 | 33 | 29 | 57 | 20 | 99 | |
| More than one surgery indication | 25 | 60 | 8 | 69 | 8 | 133 | 6 | 1 | 3 | 10 | |
| Patients without using ORC from 1 January 2015 to 31 May 2016, and patients with using ORC from 1 June 2016 to 31 December 2017 | 143 | 436 | 200 | 113 | 193 | 167 | 165 | 643 | 179 | 554 | |
| Platelet infusion in surgery | 10 | 20 | 15 | 7 | 5 | 3 | 1 | 3 | 2 | 11 | |
| Extremely high blood transfusion volume | 102 | 55 | 29 | 52 | 18 | 15 | 12 | 114 | 49 | 118 | |
| Patients used to create propensity-score matched groups | 399 | 1038 | 440 | 290 | 480 | 185 | 303 | 1391 | 162 | 635 | |
| Propensity-score matched pairs | 101 | 270 | 81 | 93 | 111 | 41 | 86 | 261 | 20 | 52 | |
ORC: Oxidized regenerated cellulose.
Comparisons of the outcome measures associated with the nonORC group versus ORC group in neurosurgeries
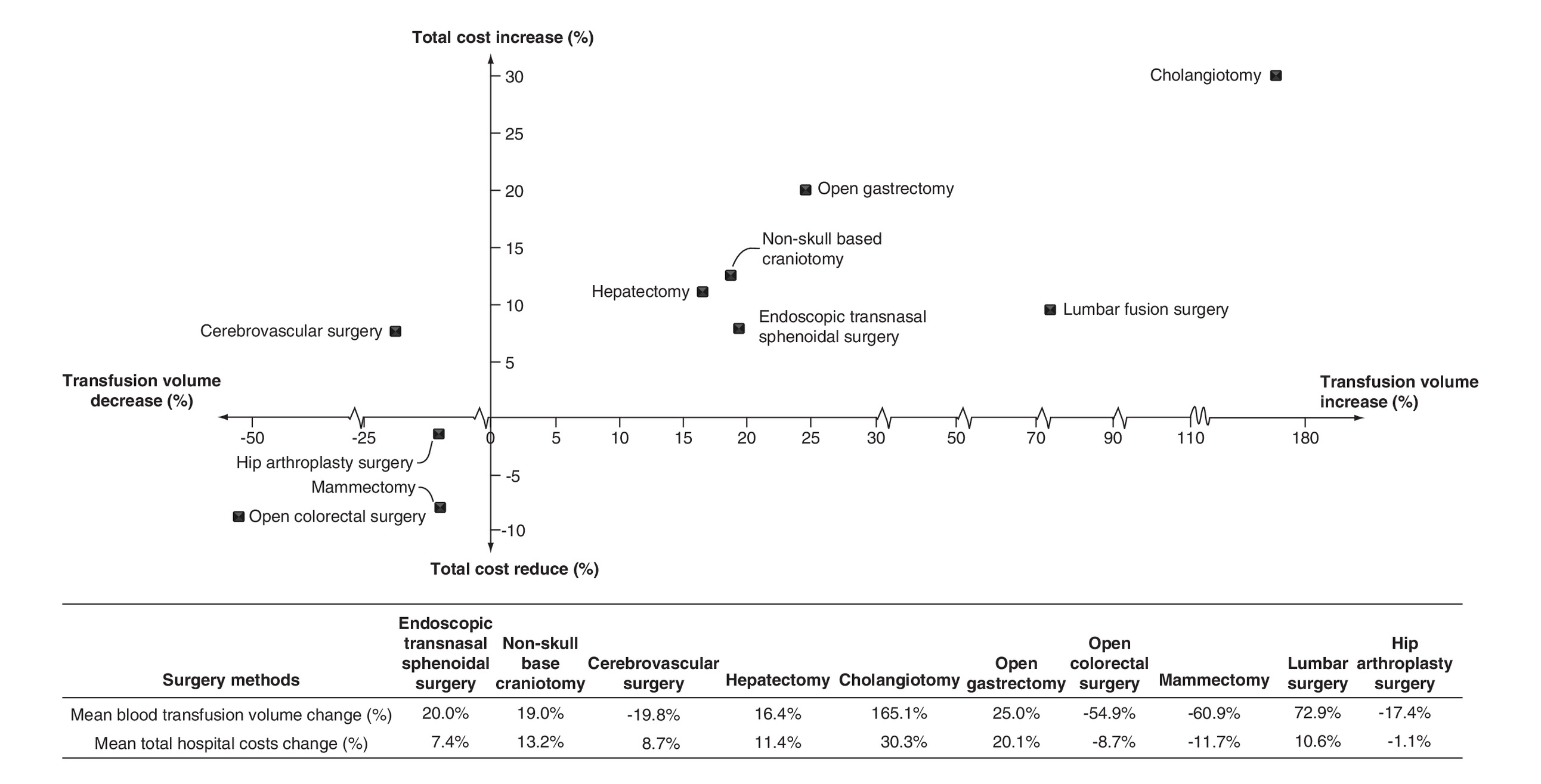
This study created 101 propensity-score matched pairs for ESTSS, 270 propensity-score matched pairs for NSBC and 81 propensity-score matched pairs for CVS. The patient baseline characteristics and measured outcomes of the created propensity-score matched pairs for the three selected neurosurgeries are summarized in Table 2. The matched pairs for the three selected neurosurgeries were well balanced, not demonstrating any significant differences in patient demographics, bone marrow function, primary surgery indications and main comorbidities. Further comparisons for the three selected neurosurgeries identified that the matched nonORC group was associated with both higher blood transfusion volume and hospital costs than the matched ORC group in ESTSS (20.0% higher for blood transfusion volume: 120.2 ± 550.2 ml vs 100.2 ± 552.0 ml, p = 0.799; 7.4% higher for the mean hospital costs: ¥88,101 ± 34,900 vs ¥82,046 ± 29,776, p = 0.101) and NSBC (19.0% higher for blood transfusion volume: 303.6 ± 845.0 ml vs 255.1 ± 539.3 ml, p = 0.427; 13.2% higher for the mean hospital costs: ¥109,774 ± 58,673 vs ¥96,991 ± 48,237, p = 0.002). When compared with the matched ORC group, the matched nonORC group was associated with a lower intraoperative blood transfusion rate (26.4% lower: 30.9 vs 42.0%, p = 0.164) and blood transfusion volume (19.8% lower: 172.9 ± 409.4 ml vs 215.7 ± 405.2 ml, p = 0.509) in CVS. However, the mean hospital costs in the matched nonORC group were 8.7% higher than that for the matched ORC group (¥118,444 ± 51,371 vs ¥108,957 ± 55,829, p = 0.156) in CVS. The other measured outcomes, including operation time and post-surgery hospital length, associated with the created propensity-score matched pairs for the three selected neurosurgeries were comparable.
| Surgery type | Endoscopic transnasal sphenoidal surgery | Nonskull base craniotomy | Cerebrovascular surgery | ||||||
|---|---|---|---|---|---|---|---|---|---|
| nonORC group (n = 101) | ORC group (n = 101) | p-value | nonORC group (n = 270) | ORC group (n = 270) | p-value | nonORC group (n = 81) | ORC group (n = 81) | p-value | |
| Patient baseline characteristics | |||||||||
| Age (years) | 48.5 ± 12.6 | 47.0 ± 11.7 | 0.377 | 49.5 ± 12.3 | 50.8 ± 11.9 | 0.176 | 45.5 ± 12.6 | 49.0 ± 13.7 | 0.099 |
| Male (%) | 42.6% | 42.6% | 41.9% | 41.9% | 40.7% | 53.1% | |||
| Primary surgery indication | |||||||||
| Pituitary tumor (%) | 89.1% | 86.1% | 0.248 | 1.2% | 1.2% | 1.000 | |||
| Meningioma (%) | 43.3% | 43.0% | 1.000 | ||||||
| Glioma (%) | 46.3% | 47.0% | 0.480 | ||||||
| Hemangioblastoma (%) | 40.7% | 40.7% | 1.000 | ||||||
| Aneurysm (%) | 34.6% | 29.6% | 0.556 | ||||||
| Arteriovenous malformation (%) | 16.0% | 17.3% | 1.000 | ||||||
| Bone marrow function | |||||||||
| Normal INR (%) | 97.0% | 99.0% | 0.617 | 99.6% | 98.5% | 0.371 | 96.3% | 96.3% | 1.000 |
| Normal red blood cell counts (%) | 80.2% | 80.2% | 1.000 | 85.2% | 88.5% | 0.313 | 81.5% | 74.1% | 0.377 |
| Normal hemoglobin (%) | 78.2% | 81.2% | 0.248 | 88.1% | 87.8% | 1.000 | 79.0% | 82.7% | 0.710 |
| Normal platelet counts (%) | 92.1% | 95.0% | 0.579 | 94.1% | 93.7% | 1.000 | 93.8% | 92.6% | 1.000 |
| Main comorbidities | |||||||||
| Hypertension (%) | 10.9% | 13.9% | 0.689 | 10.0% | 12.6% | 0.427 | 2.5% | 2.5% | 1.000 |
| Diabetes (%) | 2.0% | 2.0% | 1.000 | 3.3% | 2.6% | 0.803 | 1.2% | 2.5% | 1.000 |
| Cerebrovascular diseases (%) | 3.0% | 3.0% | 1.000 | 1.1% | 3.3% | 0.114 | 27.2% | 14.8% | 0.066 |
| Measured outcomes | |||||||||
| Intraoperative transfusion rate (%) | 9.9% | 6.9% | 0.606 | 30.4% | 33.0% | 0.562 | 30.9% | 42.0% | 0.164 |
| Total transfusion volume (ml) | 120.2 ± 550.2 | 100.2 ± 552.0 | 0.799 | 303.6 ± 845.0 | 255.1 ± 539.3 | 0.427 | 172.9 ± 409.4 | 215.7 ± 405.2 | 0.509 |
| Operation time (h) | 4.3 ± 1.8 | 4.5 ± 1.9 | 0.550 | 6.4 ± 2.2 | 6.4 ± 2.4 | 0.895 | 6.0 ± 1.9 | 6.4 ± 3.0 | 0.269 |
| Postoperative LOS (days) | 9.9 ± 4.4 | 9.4 ± 5.3 | 0.436 | 13.7 ± 7.1 | 13.2 ± 6.8 | 0.313 | 12.5 ± 4.8 | 12.8 ± 6.0 | 0.755 |
| Hospital costs (RMB) | 0.101 | 0.002 | 0.156 | ||||||
| Mean ± SD | 88,101 ± 34,900 | 82,046 ± 29,776 | 109,774 ± 58,673 | 96,991 ± 48,237 | 118,444 ± 51,371 | 108,957 ± 55,829 | |||
| Median | 91,701 | 84,953 | 93,806 | 82,582 | 114,057 | 94,293 | |||
Characteristics and outcomes were described as mean ± standard deviation or percentage as appropriate.
The bold digits signifies the p-value less than 0.05.
LOS: Length of stay; INR: International normalized ratio; ORC: Oxidized regenerated cellulose; SD: Standard deviation.
Comparisons of outcome measures associated with nonORC group versus ORC group in general surgeries
This study created propensity-score matched pairs for five selected general surgeries, which included hepatectomy (93 pairs), biliary resection surgery (41 pairs), gastrectomy (111 pairs), proctocolectomy (86 pairs) and breast surgery (261 pairs). The patient baseline characteristics and measured outcomes of the matched pairs for the five selected general surgeries are summarized in Table 3. The matched pairs were well balanced in their patient baseline characteristics without any significant differences in patient demographics, primary surgery indications, bone marrow function and primary comorbidities. The comparisons observed that the matched nonORC group was associated with higher mean blood transfusion volume in hepatectomy (16.4% higher: 465.3 ± 1238.6 ml vs 399.6 ± 909.8 ml, p = 0.692), cholangiotomy (165.1% higher: 213.4 ± 999.8 ml vs 80.5 ± 292.6 ml, p = 0.329) and gastrectomy (25.0% higher: 325.3 ± 940.1 ml vs 260.2 ± 701.1 ml, p = 0.574) than the matched ORC group. Additionally, the matched nonORC group was associated with higher mean hospital costs in hepatectomy (11.4% higher: ¥128,061 ± 92,950 vs ¥114,959 ± 76,535, p = 0.287), cholangiotomy (30.3% higher: ¥134,996 ± 65,603 vs ¥103,580 ± 48,408, p = 0.031) and open gastrectomy (20.1% higher: ¥91,209 ± 50,353 vs ¥75,971 ± 34,462, p = 0.035). However, the matched nonORC group was associated with an increase in neither blood transfusion volume nor hospital costs in proctocolectomy and breast surgery.
| Patient characteristics | Hepatectomy | Cholangiotomy | Open gastrectomy | ||||||
|---|---|---|---|---|---|---|---|---|---|
| nonORC group (n = 93) | ORC group (n = 93) | p-value | nonORC group (n = 41) | ORC group (n = 41) | p-value | nonORC group (n = 111) | ORC group (n = 111) | p-value | |
| Patient baseline characteristics | |||||||||
| Age (years) | 53.2 ± 10.7 | 52.5 ± 11.5 | 0.665 | 55.1 ± 11.9 | 54.5 ± 11.9 | 0.814 | 56.7 ± 11.5 | 53.9 ± 12.4 | 0.081 |
| Male (%) | 52.70% | 49.50% | 0.749 | 39.00% | 43.90% | 0.823 | 73.00% | 63.10% | 0.170 |
| Primary surgery indication | |||||||||
| Malignant tumors (%) | 62.40% | 54.80% | 0.281 | 7.30% | 19.50% | 0.228 | 89.20% | 91.00% | 0.823 |
| Stone (%) | 14.00% | 14.00% | 1.000 | 68.30% | 58.50% | 0.522 | |||
| Benign tumors (%) | 15.10% | 21.50% | 0.307 | 2.40% | 4.90% | 1.000 | 4.50% | 1.80% | 0.450 |
| Bone marrow function | |||||||||
| Normal INR (%) | 93.50% | 96.80% | 0.505 | 92.70% | 97.60% | 0.617 | 94.60% | 97.30% | 0.450 |
| Normal red blood cell counts (%) | 68.80% | 68.80% | 1.000 | 70.70% | 61.00% | 0.502 | 61.30% | 68.50% | 0.332 |
| Normal hemoglobin (%) | 71.00% | 72.00% | 1.000 | 63.40% | 75.60% | 0.332 | 55.90% | 56.80% | 1.000 |
| Normal platelet counts (%) | 83.90% | 76.30% | 0.265 | 90.20% | 87.80% | 1.000 | 82.90% | 84.70% | 0.855 |
| Primary comorbidities | |||||||||
| Hypertension (%) | 3.20% | 3.20% | 1.000 | 9.90% | 3.60% | 0.121 | |||
| Coronary heart disease (%) | |||||||||
| Diabetes (%) | 2.70% | 4.50% | 0.724 | ||||||
| Cerebrovascular diseases (%) | 0.00% | 1.10% | 1.000 | 2.70% | 0.90% | 0.617 | |||
| Measured outcomes | |||||||||
| Intraoperative transfusion rate (%) | 19.40% | 17.20% | 0.838 | 4.90% | 4.90% | 1.000 | 19.80% | 21.60% | 0.871 |
| Total transfusion volume (ml) | 465.3 ± 1238.6 | 399.6 ± 909.8 | 0.692 | 213.4 ± 999.8 | 80.5 ± 292.6 | 0.329 | 325.3 ± 940.1 | 260.2 ± 701.1 | 0.574 |
| Operation time (h) | 4.6 ± 1.3 | 4.6 ± 1.6 | 0.739 | 3.5 ± 1.4 | 3.8 ± 1.9 | 0.335 | 4.5 ± 1.6 | 4.0 ± 1.4 | 0.033 |
| Postoperative LOS (days) | 13.8 ± 8.9 | 13.7 ± 10.2 | 0.921 | 12.5 ± 6.9 | 12.2 ± 3.8 | 0.834 | 12.4 ± 6.0 | 12.9 ± 5.4 | 0.516 |
| Total hospital costs (RMB) | 0.287 | 0.031 | 0.035 | ||||||
| Mean ± SD | 128,061 ± 92,950 | 114,959 ± 76,535 | 134,996 ± 65,603 | 103,580 ± 48,408 | 91,209 ± 50,353 | 75,971 ± 34,462 | |||
| Median | 99,430 | 98,971 | 117,835 | 101,748 | 68,409 | 65,852 | |||
| Open colorectal surgery | Mammectomy | ||||||||
| nonORC group (n = 86) | ORC group (n = 86) | p-value | nonORC group (n = 261) | ORC group (n = 261) | p-value | ||||
| Patient baseline characteristics | |||||||||
| Age (years) | 55.8 ± 10.2 | 57.9 ± 14.0 | 0.252 | 50.0 ± 10.3 | 49.9 ± 10.0 | 0.788 | |||
| Male (%) | 50.00% | 50.00% | 1.000 | 0.80% | 0.40% | 1.000 | |||
| Primary surgery indication | |||||||||
| Malignant tumors (%) | 86.00% | 89.50% | 0.646 | 95.40% | 94.60% | 0.724 | |||
| Benign tumors (%) | 5.80% | 5.80% | 1.000 | ||||||
| Bone marrow function | |||||||||
| Normal INR (%) | 100.00% | 100.00% | 1.000 | 97.30% | 96.60% | 0.724 | |||
| Normal red blood cell counts (%) | 75.60% | 75.60% | 1.000 | 62.50% | 70.90% | 0.068 | |||
| Normal hemoglobin (%) | 61.60% | 58.10% | 0.700 | 68.20% | 72.00% | 0.411 | |||
| Normal platelet counts (%) | 77.90% | 83.70% | 0.383 | 91.60% | 88.50% | 0.312 | |||
| Primary comorbidities | |||||||||
| Hypertension (%) | 10.50% | 12.80% | 0.814 | 8.00% | 8.00% | 1.000 | |||
| Coronary heart disease (%) | 0.80% | 0.40% | 1.000 | ||||||
| Diabetes (%) | 1.20% | 2.30% | 1.000 | 1.10% | 1.90% | 0.724 | |||
| Cerebrovascular diseases (%) | 1.20% | 2.30% | 1.000 | 0.80% | 0.00% | 0.617 | |||
| Measured outcomes | |||||||||
| Intraoperative transfusion rate (%) | 4.70% | 12.80% | 0.096 | 0.00% | 0.80% | 0.617 | |||
| Total transfusion volume (ml) | 56.6 ± 175.0 | 125.6 ± 438.8 | 0.183 | 0.9 ± 13.9 | 2.3 ± 26.2 | 0.414 | |||
| Operation time (h) | 3.5 ± 1.3 | 3.3 ± 1.0 | 0.183 | 2.9 ± 0.6 | 3.0 ± 0.7 | 0.150 | |||
| Postoperative LOS (days) | 11.0 ± 5.5 | 13.4 ± 10.0 | 0.053 | 11.3 ± 2.9 | 11.3 ± 2.9 | 0.545 | |||
| Total hospital costs (RMB) | 0.005 | 0.000 | |||||||
| Mean ± SD | 60,113 ± 36,126 | 65,806 ± 40,244 | 33,090 ± 12,754 | 37,457 ± 17,071 | |||||
| Median | 51,583 | 58,553 | 30,956 | 33,924 | |||||
Characteristics and outcomes were described as mean ± standard deviation or percentage as appropriate.
INR: International normalized ratio; LOS: Length of stay; ORC: Oxidized regenerated cellulose; SD: Standard deviation.
Comparisons of the outcome measures associated with the nonORC group versus ORC group in orthopedics surgeries
In lumbar surgery (52 pairs) and hip arthroplasty surgery (20 pairs), the matched groups were well balanced in their demographics, primary surgical indicators, bone marrow function and comorbidities (Table 4). The comparisons of the outcomes observed that the matched nonORC was associated with significantly higher intraoperative blood transfusion rate (63.0% higher: 84.6 vs 51.9%, p = 0.001) and significantly higher blood transfusion volume (72.9% higher: 494.7 ± 589.6 ml vs 286.2 ± 388.5 ml, p = 0.028) than the matched ORC group in lumbar surgery. Additionally, the matched nonORC group was associated with slightly higher hospital costs than the matched ORC group in lumbar surgery (10.6% higher: ¥176,191 ± 79,534 vs ¥159,321 ± 80,186, p = 0.253).
| Patient characteristics | Lumbar surgery | Hip arthroplasty surgery | ||||
|---|---|---|---|---|---|---|
| nonORC group (n = 52) | ORC group (n = 52) | p-value | nonORC group (n = 20) | ORC group (n = 20) | p-value | |
| Patient baseline characteristics | ||||||
| Age (years) | 52.8 ± 14.3 | 51.9 ± 12.4 | 0.740 | 56.8 ± 10.5 | 55.8 ± 12.8 | 0.666 |
| Male (%) | 51.90% | 48.10% | 0.850 | 50.00% | 50.00% | 1.000 |
| Primary surgery indication (%) | ||||||
| Fracture (%) | 0.00% | 1.90% | 1.000 | 15.00% | 10.00% | 1.000 |
| Lumbar degeneration (%) | 98.10% | 96.20% | 1.000 | |||
| Osteoarthritis (%) | 15.00% | 15.00% | 1.000 | |||
| Osteonecrosis of the femoral head (%) | 55.00% | 55.00% | 1.000 | |||
| Ankylosing spondylitis (%) | 5.00% | 10.00% | 1.000 | |||
| Bone marrow function | ||||||
| Normal INR (%) | 98.10% | 100.00% | 1.000 | 100.00% | 100.00% | 1.000 |
| Normal red blood cell counts (%) | 82.70% | 86.50% | 0.803 | 85.00% | 75.00% | 0.683 |
| Normal hemoglobin (%) | 75.00% | 84.60% | 0.383 | 85.00% | 70.00% | 0.505 |
| Normal platelet counts (%) | 94.20% | 98.10% | 0.617 | 75.00% | 75.00% | 1.000 |
| Primary comorbidities | ||||||
| Hypertension (%) | 1.90% | 3.80% | 1.000 | 20.00% | 10.00% | 0.683 |
| Diabetes (%) | 3.80% | 3.80% | 1.000 | |||
| Measured outcomes | ||||||
| Intraoperative transfusion rate (%) | 84.60% | 51.90% | 0.001 | 80.00% | 80.00% | 1.000 |
| Total transfusion volume (ml) | 494.7 ± 589.6 | 286.2 ± 388.5 | 0.028 | 511.5 ± 453.1 | 619.0 ± 623.5 | 0.936 |
| Operation time (h) | 4.1 ± 1.2 | 4.5 ± 1.3 | 0.181 | 2.8 ± 0.7 | 3.2 ± 1.1 | 0.231 |
| Postoperative LOS (days) | 12.1 ± 3.2 | 13.2 ± 5.1 | 0.285 | 10.1 ± 4.0 | 9.3 ± 3.2 | 0.409 |
| Hospital costs (RMB) | 0.253 | 0.522 | ||||
| Mean ± SD | 176,191 ± 79,534 | 159,321 ± 80,186 | 112,890 ± 35,641 | 114,196 ± 64,656 | ||
| Median | 169,886 | 160,052 | 99,148 | 98,321 | ||
Characteristics and outcomes were described as mean ± standard deviation or percentage as appropriate.
INR: International normalized ratio; LOS: Length of stay; ORC: Oxidized regenerated cellulose; SD: Standard deviation.
The changes in mean blood transfusion volume and mean hospital costs for the matched two groups in the ten surgery settings were plotted in Figure 1.
Discussion
This study mainly assessed the real-world impact of ORC as an adjunct therapy for bleeding control in ten surgeries that were commonly conducted in Chinese tier III hospitals. This study observed a higher transfusion rate/volume and higher hospital costs in the nonORC group in six of the selected ten surgeries, which included ESTSS, NSBC, hepatectomy, cholangiotomy, open gastrectomy and lumbar surgery. Thus, these six surgeries would gain more clinical benefits if using AHA. As hospital LOS and blood transfusion associated with surgeries usually decrease with improved quality of hospital care over time, the prolonged hospital LOS or increased blood transfusion associated with the ‘nonORC group’, which was identified in the latest time window, might be the indicators of deteriorating quality of hospital care after the restrict use of AHA in Chinese tertiary care hospitals.
Diligent and meticulous bipolar electrocautery is the main method to achieve hemostasis in neurosurgeries [13], while ORC could quickly aid in the hemostasis of slow venous and capillary ooze associated with the excision of intrinsic tumors, lobectomy or the removal of intracerebral hemorrhage [7]. The adjunctive hemostasis effects of ORC could be confounded by the complexity of surgical procedures and were unlikely to be fully demonstrated by the indirect outcome measures [14]. However, this study observed the relatively higher blood transfusion volume and higher hospital costs in the nonORC group in NSBC, which demonstrated the clinical and economic benefits of using ORC as the adjunct hemostasis. Similar findings were also observed in ESTSS, which requires clear visualization under endoscopy. The applications of ORC to control oozing may enhance the visualization in ESTSS [15]. As for CVS, this study observed higher blood transfusion volume, but lower hospital costs in the ORC group. This inconsistency might be caused by unknown confounders, such as the use of other techniques that could decrease blood transfusion but cost more.
Of the selected five general surgeries, hepatectomy could have the highest risk of bleeding due to the hepatic sinusoidal structure of the liver, in which there is no smooth muscle to control bleeding through vasoconstriction [16]. When using conventional hemostasis methods, including suturing and ligation, it is hard to manage multiple bleeding sites on the wide and raw surfaces of the liver after the parenchymal lacerations [17]. Similarly, radical surgery for gastric cancer could leave multiple bleeding sites, while ORC might provide suitable adjunct hemostasis through wrapping [18]. Hence, hepatectomy, open gastrectomy and cholangiotomy could obtain more clinical and economic benefits, indicated by lower blood transfusion and lower hospital costs, through using ORC. The other two general surgeries, proctocolectomy and breast resection surgery, were associated with neither higher blood transfusion volume nor higher total hospitalization cost after the stop of using ORC. The assessment of the clinical and economic impact of restricting the use of ORC in these five selected general surgeries confirmed the need for guidance regarding the appropriate use of ORC by surgery setting.
This study assessed the needs of the appropriate use of ORC in lumbar surgery and hip arthroplasty surgery. This study observed a significantly higher intraoperative blood transfusion rate and also blood transfusion volume in the matched nonORC group in lumbar surgery. Because bipolar cautery can induce thermal injury to adjacent nerve roots in spine surgery, this finding was likely to support the use of ORC, which could better control the epidural oozing during spinal surgery [19]. Though previous research reported that using ORC to fill the bone surface and soft tissue gap before incision closure can effectively reduce hidden blood loss in hip arthroplasty surgery [20], our study did not observe any improved outcomes for blood transfusion or lower hospital costs in the ORC group. Because hip arthroplasty surgery was associated with 80% of the intraoperative blood transfusion rate and the mean total blood transfusion volume above 500 ml, the adjunct hemostasis effects associated with ORC were unlikely to sufficient in hip arthroplasty surgery.
The observed variances of blood transfusion and hospital costs associated with ORC in the selected ten surgeries in this study were well aligned with the hemostasis mechanisms of ORC. For example, (Surgicel, Ethicon, Inc. NJ, USA) the ORC used in our hospital setting, is made of sterile cellulose-based thrombogenic material that can control bleeding originating from delicate and/or friable tissues. Because Surgicel is shaped as a gauze-like material and is easily inserted into the areas that are difficult to reach, Surgicel could be a more practical option to reach the narrow surgical spaces and areas than conventional hemostatic methods for the control of the bleeding. Additionally, Surgicel can form a gelatinous mass upon saturation with blood and create a stable clot, which is highly effective in control massive bleeding associated with the surgical surface. Thus, the better hemostasis effects associated with Surgicel, indicated by the reduced blood transfusion, in ESTSS, NSBC, hepatectomy, cholangiotomy, gastrectomy and lumbar surgery supported the use of ORC to address those hemostasis challenges in surgeries.
Most of our study results are well aligned with the expected correlation between blood transfusion and hospital costs (more blood transfusion drove up hospital costs). However, this study observed the opposite correlation between blood transfusion volume and hospital costs in CVS. We have carefully reviewed the patient characteristics of the created propensity-score matched groups for ORC versus nonORC in this surgery. Even though most patient characteristics were well balanced in the matched group, the matched nonORC group was associated with a doubled rate of cerebrovascular diseases when compared with the matched ORC group (27.2 vs 14.8%, p = 0.066). Because cerebrovascular diseases are well-recognized contributors to medical costs [21], CVS in these patients could consume more hospital resources to stabilize the conditions of cerebrovascular disease before surgery. Additionally, there could be other unknown patient characteristics with strong confounding effects introducing bias in the comparisons. For example, the socio-economic status is always a strong confounder for hospital costs in Chinese real-world hospital settings [22]. However, the socio-economic status information in the hospital records was limited and incomplete. Thus, the impact of clinical benefits associated with ORC on hospital costs could not be fully clarified and demonstrated.
As a retrospective cohort study, the lack of reliable outcome measures to directly assess the adjunct hemostasis effects associated with ORC was the primary limitation in this study. This study selected a proven indirect outcome measure, blood transfusion volume, to measure hemostasis effects. Thus, the actual adjunct hemostasis associated with using ORC in this study could be discounted by the indirect outcome measure. Additionally, the bleeding risk associated with the same surgery could vary substantially by the complexity of surgery procedures. This study did not collect sufficient information for the surgical procedures to adjust their confounding effects in the comparisons of propensity score-matched groups. For example, colorectal resection surgery for colon cancer could experience a much higher risk of bleeding in the advanced cancer stage, which requires expanding the surgical cut area and lymphatic clearance. Moreover, the admission periods of the nonORC group and ORC group were sequential. The confounding effects associated with hospital care quality overtime on the measured outcomes could not be adjusted either in this study. Finally, this study did not adjust the surgeons in the propensity score comparisons due to the small sample size while the surgeon’s skills play crucial roles in surgery bleeding control. Finally, most comparisons between the propensity score-matched groups only observed a nonsignificant trend for the clinical and economic benefits associated with ORC likely due to the small sample size. Given the limitations listed above, future studies are still needed to conduct a randomized clinical trial with sufficient sample size and outcome measures directly assessing hemostasis effects to draw more definitive conclusions for ORC in these surgery settings.
Conclusion
This study observed increased blood transfusion and hospital costs in specific surgery settings in a Chinese tertiary care hospital which used conventional hemostatic techniques without ORC. More specifically, not using ORC would increase the burden of transfusion and total hospital costs in ESTSS, NSBC, hepatectomy, cholangiotomy, gastrectomy and lumbar surgery. Thus, using ORC for adjunct hemostasis in these surgery settings should be encouraged to address their hemostasis needs.
•
Oxidized regenerated cellulose (ORC) could gain more clinical and economic benefits than conventional hemostatic methods in the surgeries with hemostasis challenges due to narrow surgical space and massive bleeding.
•
The varied clinical and economic outcomes associated with ORC across surgery settings indicated the needs of evidence-based clinical decision making regarding the use of ORC in surgeries.
•
Blood transfusion could be a reasonable outcome measure indirectly assessing hemostasis effects in real-world surgery settings.
•
It is challenging to fully control the known and unknown confounding effects in retrospective cohort studies assessing hemostasis effects associated with ORC.
•
Randomized control trial could be a better study design to achieve definitive conclusions on the hemostasis effects of ORC.
Author contributions
Z Qian and W Chen formulated the research idea and developed the study protocol. F Xiong, X Xia, P Gu, Q Wang and A Wu developed data extraction strategies, coordinate the data access and conducted data extraction from the hospital information system. Q Gong, Y Chen and H Zhan followed the study protocol to clean the extracted data and perform the data analysis. Z Qian and W Chen drafted the manuscript. All authors have critically reviewed the manuscript and approved this manuscript submission.
Financial & competing interests disclosure
This study was funded by Ethicon, Inc., Somerville, NJ, USA. Q Gong, Y Chen, H Zhan and W Chen are employed in a consulting firm which receives industry research funds for real-world studies and health economics research. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Murphy GJ, Reeves BC, Rogers CA, Rizvi SI, Culliford L, Angelini GD. Increased mortality, postoperative morbidity, and cost after red blood cell transfusion in patients having cardiac surgery. Circulation 116(22), 2544–2552 (2007).
• Supports the correlation between blood transfusion and hospital costs.
2.
Al-Attar N, Johnston S, Jamous N et al. Impact of bleeding complications on length of stay and critical care utilization in cardiac surgery patients in England. J. Cardiothorac. Surg. 14(1), 64 (2019).
• Supports the explanation of the impact of bleeding on hospital costs.
3.
Samudrala S. Topical hemostatic agents in surgery: a surgeon’s perspective. AORN J. 88(3), S2–S11 (2008).
• Explains the clinical utility of hemostatic agents in surgeries.
4.
Achneck HE, Sileshi B, Jamiolkowski RM, Albala DM, Shapiro ML, Lawson JH. A comprehensive review of topical hemostatic agents: efficacy and recommendations for use. Ann. Surg. 251(2), 217–228 (2010).
• Supports the clinical utility of hemostatic agents in surgeries.
5.
Hutchinson RW, George K, Johns D, Craven L, Zhang G, Shnoda P. Hemostatic efficacy and tissue reaction of oxidized regenerated cellulose hemostats. Cellulose 20(1), 537–545 (2013).
• Explains the hemostasis mechanism of oxidized regenerated cellulose.
6.
Overbey DM, Jones EL, Robinson TN. How hemostatic agents interact with the coagulation cascade. AORN J. 100(2), 148–159 (2014).
7.
Keshavarzi S, MacDougall M, Lulic D, Kasasbeh A, Levy M. Clinical experience with the surgicel family of absorbable hemostats (oxidized regenerated cellulose) in neurosurgical applications: a review. Wounds 25(6), 160–167 (2013).
• This study is the existing evidence to support the use of oxidized regenerated cellulose in neurosurgery setting.
8.
Kakaei F, Sadeghi S, Salim M, Sanei B, Hashemzadeh S, Habibzadeh A. A randomized clinical trial comparing the effect of different haemostatic agents for haemostasis of the liver after hepatic resection. HPB Surg. 2013, 587608 (2013).
9.
Cho SK, Yi JS, Park MS et al. Hemostatic techniques reduce hospital stay following multilevel posterior cervical spine surgery. J. Bone Joint Surg. Am. 94(21), 1952–1958 (2012).
10.
Vyas KS, Saha SP. Comparison of hemostatic agents used in vascular surgery. Expert Opin. Biol. Ther. 13(12), 1663–1672 (2013).
11.
Vera-Llonch M, Hagiwara M, Oster G. Clinical and economic consequences of bleeding following major orthopedic surgery. Thromb. Res. 117(5), 569–577 (2006).
12.
National Bureau of Statistics[Internet]. CPI Query Database. Accessed CPI China, Beijing, China (2020). http://data.stats.gov.cn/easyquery.htm?cn=C01&zb=A0902&sj=2018
13.
Bulsara KR, Sukhla S, Nimjee SM. History of bipolar coagulation. Neurosurg. Rev. 29(2), 93–96 (2006).
14.
Gerlach R, Krause M, Seifert V, Goerlinger K. Hemostatic and hemorrhagic problems in neurosurgical patients. Acta Neurochir. (Wien) 151(8), 873–900 (2009).
15.
Levy ML, Amar AP. The use of oxidized regenerated cellulose in neurosurgical procedures. Surg. Technol. Int. 7, 467–471 (1998).
16.
Clark WR Jr, Leather RP. Haemostasis during liver resection. Surgery 67, 556–557 (1970).
17.
Lochan R, Ansari I, Coates R, Robinson SM, White SA. Methods of haemostasis during liver resection: a UK national survey. Dig. Surg. 30(4–6), 375–382 (2013).
18.
Kasalicky M, Dolezel R, Vernerova E, Haluzik M. Laparoscopic sleeve gastrectomy without over-sewing of the staple line is effective and safe. Videosurg. Other Miniinvasive Tech. 9(1), 46 (2014).
19.
Levy ML, Day JD. Surgicel fibrillar absorbable oxidized regenerated cellulose. Neurosurgery 41(3), 701–702 (1997).
20.
Wang JQ, Chen LY, Jiang BJ, Zhao YM. Oxidized regenerated cellulose can reduce hidden blood loss after total hip arthroplasty: a retrospective study. J. Invest. Surg. 32(8), 716–722 (2019).
21.
Yeh CC, Hsieh CH, Liao CC, Su LT, Wang YC, Li TC. Diabetes mellitus and cerebrovascular disease as independent determinants for increased hospital costs and length of stay in open appendectomy in comparison with laparoscopic appendectomy: a nationwide cohort study. Am. Surg. 78(3), 329–334 (2012).
•• This study helps with the explanation of the confounding effects associated with unbalanced comorbidities in the cost data analysis.
22.
Gong CH, Kendig H, He X. Factors predicting health services use among older people in China: an analysis of the China Health and Retirement Longitudinal Study 2013. BMC Health Serv. Res. 16(1), 63 (2016).
•• This study helps with the explanation of the confounding effects associated with patient socio-economic status in the cost data analysis.
Information & Authors
Information
Published In
Pages: 1079 - 1090
PubMed: 32959666
Copyright
© 2020 Future Medicine Ltd.
History
Received: 7 August 2020
Accepted: 2 September 2020
Published online: 22 September 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Clinical and economic impact of oxidized regenerated cellulose for surgeries in a Chinese tertiary care hospital. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0166
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Chenglong Xiao, Huang Liyin, Chai Sheng, Effectiveness and Safety of Oxidized Regenerated Cellulose for Hemostasis in Joint Arthroplasty: A Systematic Review and Meta-Analysis, Clinical and Applied Thrombosis/Hemostasis, 10.1177/10760296261420230, 32, (2026).
- Kaspars Auslands, Evelina Kocane, Evija Bergfelde, Egils Valeinis, Julija Dolgopolova, Jekabs Aksiks, Igors Aksiks, Evaluation of the Performance of StypCelTM Absorbable Hemostat for Intraoperative Hemorrhage Control in Neurosurgery: A Multicenter, Single-Arm Study in Riga, Latvia, Medicina, 10.3390/medicina61101862, 61, 10, (1862), (2025).
- Bowei Li, Wenjie Pan, Jianbing Ma, Yuanchi Huang, Hemostatic effect of oxidized regenerated cellulose vs. topical tranexamic acid in total knee arthroplasty—a prospective randomized controlled trial, Frontiers in Surgery, 10.3389/fsurg.2024.1515610, 11, (2025).
- Andi Asadul Islam, Juliani Ibrahim, Venansius R. Kurniawan, The Hemostatic Effect of T-Hemocel in Neurosurgery Case, Open Access Macedonian Journal of Medical Sciences, 10.3889/oamjms.2024.11834, 12, (2024).
- Gianluca Franceschini, Letter to the Editor: critical appraisal to optimize clinical and economic impact of oxidized regenerated cellulose in surgical practice, Journal of Comparative Effectiveness Research, 10.2217/cer-2021-0007, 10, 9, (709-710), (2021).