Comparative effectiveness of nivolumab versus standard of care for third-line patients with small-cell lung cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To estimate the comparative effectiveness of nivolumab versus standard of care (SOC) in terms of overall survival (OS) for small-cell lung cancer patients treated with two prior lines of chemotherapy, in other words, third line in the USA. Materials & methods: Data were from CheckMate 032, a single-arm trial of nivolumab, and real-world electronic patient records. Comparisons of OS were conducted using three different methods to adjust for differences (regression, weighting and doubly robust) between the populations. Results: Nivolumab was associated with longer survival compared with SOC (hazard ratio for OS: 0.58–0.70) across all methods for adjustment. Conclusion: Nivolumab was more efficacious in terms of OS as third-line treatment for small-cell lung cancer compared with current SOC in the USA.
Lay abstract
Small-cell lung cancer is an aggressive disease and often patients require multiple treatments to help them live longer. In this study, we looked at how long patients survived when receiving nivolumab compared with other commonly used therapies as their third treatment (known as third line) in the USA. Data came from the CheckMate 032 single-arm clinical trial of nivolumab and real-world electronic patient records from a US database where patients received standard of care treatment. We used several analysis methods and found that patients treated with nivolumab survived for longer than patients treated with standard of care in the USA. There is a high unmet need in the third-line small-cell lung cancer population and results from this study will help inform decision makers of the potential therapeutic option of nivolumab treatment.
Small-cell lung cancer (SCLC) accounts for 10–15% of all lung cancers, and its rapidly progressing nature poses significant challenges for treating clinicians [1–3]. At diagnosis, most patients present with extensive disease (ED), defined as Stage IV (any T, any N and M 1a/b) using American Joint Committee on Cancer TNM classification, and the remainder of patients are classified as having limited disease (LD), defined as stage I–III (any T, any N and M0) [1,4]. For many years, the standard first-line (1L) treatment for ED patients was platinum-based chemotherapy with or without radiotherapy [1,5–7]. The addition of the programmed death-ligand 1 (PD-L1) blocking antibody atezolizumab to carboplatin and etoposide was recently shown to improve overall survival (OS) relative to chemotherapy alone in the IMpower133 trial [8], and this regimen is now the recommended 1L treatment option for ED patients as per National Comprehensive Cancer Network guidelines [7]. Another PD-L1 inhibitor, durvalumab, was also recently shown to improve OS relative to platinum plus etoposide alone [9].
Subsequent systemic therapy options in the USA are currently guided by the time interval from initiation of 1L therapy to relapse. Patients who relapse >6 months after 1L are recommended to be retreated with the original regimen, whereas the preferred options for patients who relapse within 6 months are topotecan therapy or enrollment in a clinical trial [7]. Although treatment in the third-line (3L) setting is rare due to rapid disease progression and poor performance status, approximately 10–20% of patients who receive 1L treatment will subsequently receive 3L therapy [10–12]. These heavily pretreated patients are often symptomatic from disease progression, side effects of prior treatment and comorbidities, which translates into limited treatment options and is associated with a poor prognosis [7,13].
Similar to the observed shift toward immuno-oncology (IO) agents in the 1L setting, programmed death receptor-1 (PD-1) blocking antibodies, such as nivolumab, have been licensed for the 3L treatment of SCLC in checkpoint inhibitor naive patients. In CheckMate 032 (NCT01928394), 3L and beyond (3L+) patients treated with nivolumab (n = 109) had an objective response rate of 11.9% (95% CI: 6.5–19.5) and a median duration of response of 17.9 months (range: 3.0–42.1). The median progression-free survival was 1.4 months (95% CI: 1.3–1.6) and 17.2% of patients were progression free at 6 months. The median OS was 5.6 months (95% CI: 3.1–6.8), and 12- and 18-month OS rates were 28.3 and 20.0%, respectively [13]. These results suggest nivolumab is well tolerated and provides durable responses as a 3L treatment for recurrent SCLC [13]. The US FDA granted accelerated approval of nivolumab monotherapy in August 2018 to treat metastatic SCLC patients whose cancer has progressed after platinum-based chemotherapy and at least one other prior line of therapy, regardless of tumor PD-L1 status [14]. Pembrolizumab has also been granted accelerated approval by the FDA for 3L SCLC based on improved tumor response rate and durability of response from a pooled analysis of SCLC patients enrolled in the KEYNOTE-028 and KEYNOTE-158 trials. At a median follow-up of 7.7 months, the objective response rate was 19.3% (95% CI: 11.4–29.4), median duration of response was not reached (range 4.1–35.8 months), median progression-free survival was 2.0 months (95% CI: 1.9–3.4), and median OS was 7.7 months (95% CI: 5.2–10.1) [15,16].
The availability of PD-1 agents may begin to address some of the unmet need in the 3L SCLC population; however, as neither CheckMate 032 nor the KEYNOTE studies included a chemotherapy control arm, no comparative data exist for PD-1 agents versus regimens that currently comprise standard of care (SOC) for 3L patients with SCLC. The aim of this study was to address this gap by estimating the comparative effectiveness of nivolumab versus SOC in the 3L setting using individual patient data from CheckMate 032 and real-world electronic patient records from a US database.
Materials & methods
Evidence base
Individual patient data (IPD) were provided by Bristol Myers Squibb (NJ, USA) from CheckMate 032 (January 2018 database lock) and the Flatiron Health electronic health record database (Flatiron, USA) from January 2011 to September 2017. A systematic literature review was also conducted to identify any additional studies of chemotherapy that might be suitable for comparison but none were identified (see details in Supplementary Appendix A). Selection criteria applied to both datasets and the resulting attrition of patients can be found in Figure 1. The IPD from CheckMate 032 included patients with one–five prior lines of therapy in the pre-expansion and expansion cohorts (n = 402). This group was restricted to patients with two prior lines of therapy who received 3L nivolumab monotherapy.
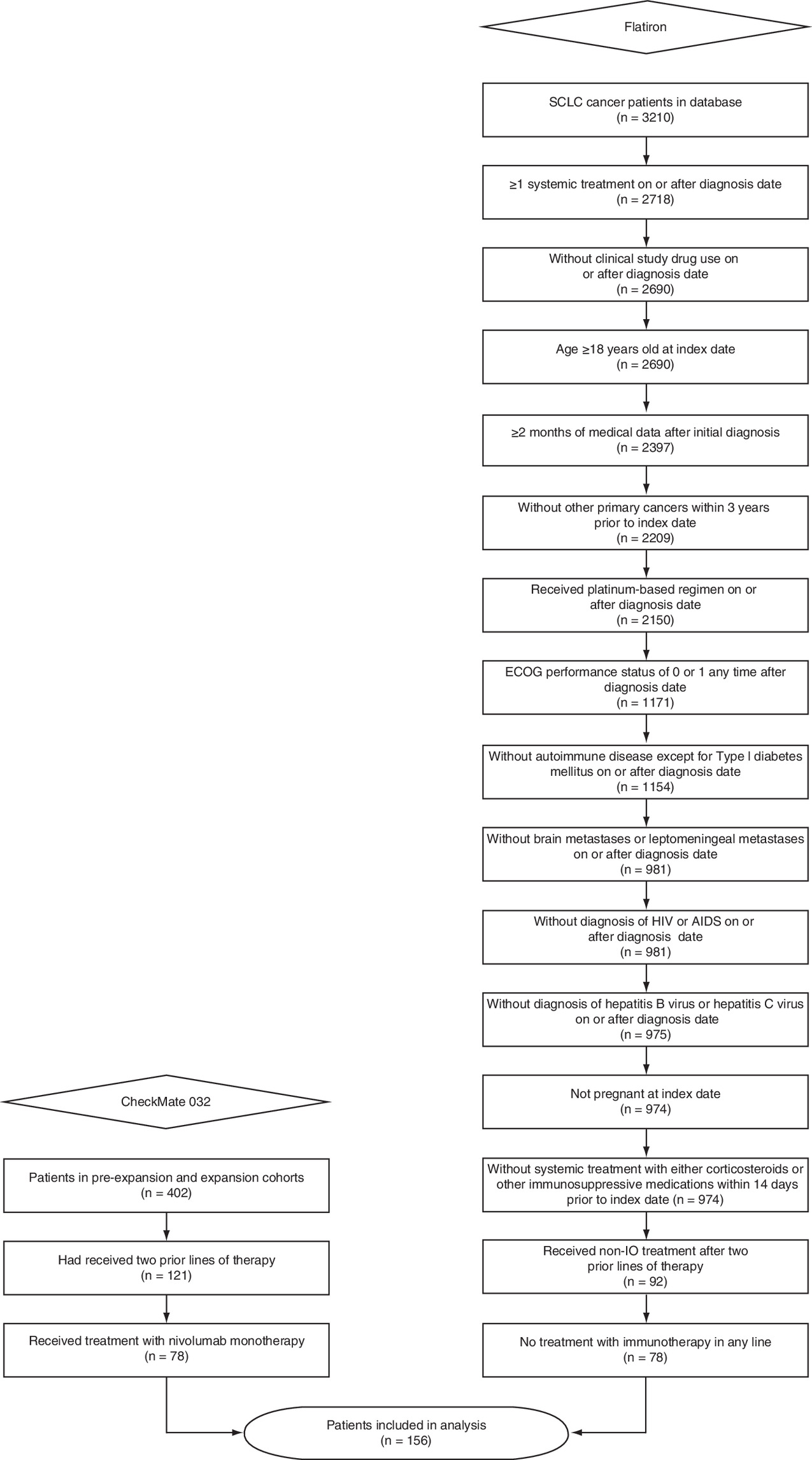
Figure 1. Patient selection criteria applied to CheckMate 032 and the Flatiron database.
ECOG: Eastern Cooperative Oncology Group; IO: Immuno-oncology; SCLC: Small-cell lung cancer.
A subgroup was constructed from the Flatiron SCLC cohort (n = 3210) that matched the eligibility criteria of CheckMate 032. Relevant selection criteria applied on or after SCLC diagnosis date included patients aged ≥18 years who had received at least one systemic treatment, had not received a clinical study drug, had ≥2 months of medical data and had not been diagnosed with other primary cancers within 3 years. This subgroup was further restricted to patients with any platinum-based regimen and Eastern Cooperative Oncology Group performance score (ECOG PS) of 0 or 1 after initial SCLC diagnosis. Patients were excluded if they had autoimmune disease (except for Type 1 diabetes mellitus), brain or leptomeningeal metastases, HIV, AIDS, hepatitis B or C, were pregnant or had received systemic treatment with either corticosteroids (>10 mg/daily prednisone equivalent) or other immunosuppressive medications within 14 days prior to the index date (initiation of 1L therapy for SCLC). Finally, patients who had received treatment with an IO agent in any line were then excluded as patients with prior IO were not permitted in CheckMate 032 and it was not anticipated that such agents would have been available postprogression at the time the study was conducted.
Statistical analysis
The outcome of interest in this analysis was OS. In CheckMate 032, this was measured from the time of treatment initiation to date of death from any cause. Patients who had not died by the specified cut-off date were censored at the last date known alive. For Flatiron, a similar definition was applied; OS was measured from the index date to the date of death from any cause. Patients who were known to be alive at the cut-off date (30 September 2017) or had been lost to follow-up were censored at the last date they were confirmed to be alive (e.g., last office visit). Patients that initiated subsequent lines of therapy continued to be followed, in other words, they were not censored at the initiation of these subsequent lines.
In the absence of a shared control arm to facilitate an anchored indirect comparison between studies, such as a network meta-analysis, the most straightforward approach to estimate relative treatment effect based on noncomparative studies is to simply compare the reported absolute treatment effects from each, assuming that there is no imbalance across the studies in terms of prognostic factors and treatment-effect modifiers. In most cases this assumption is unrealistic, which means that such so-called ‘naive’ comparisons are prone to a significant risk of bias. A more valid approach is to conduct an unanchored population-adjusted indirect comparison, whereby an attempt is made to adjust for between-trial differences in patient characteristics with the goal of reducing bias in the treatment-effect estimates that exist in the naive approach.
The methods for population adjustment employed in this analysis were developed in accordance with the National Institute for Health and Care Excellence (NICE) Decision Support Unit’s recommendations for between-study comparisons to estimate relative treatment effect when dealing with single-arm or observational studies. These methods entail using IPD to adjust for between-study imbalances in baseline characteristics, which allows for the estimation of relative treatment effects [17,18]. The overall methods are similar and include regression models and weighting analyses. When the evidence base consists of IPD from both studies, comparative patient-level analyses are recommended using methods such as multivariable regression (MVR) adjustment, inverse probability weighting (IPW) and a doubly robust method (DRM) [17].
An MVR model was used to account for differences in patient characteristics between the two cohorts and to allow both treatment arms to be analyzed simultaneously within one model. Treatment effects were assumed to be homogeneous, in other words, interactions between treatment and covariates were not included. An IPW approach was also implemented using a propensity score function. The inverse of the propensity scores were used to weight patients in CheckMate 032 and treatment effects were based on the difference in weighted means. Finally, a DRM was employed which combined the use of the MVR and IPW. Note the MVR approach estimates a model for the outcome but does not model treatment selection, while the IPW method estimates a model for the probability of receiving treatment but does not model the outcome. The advantage of the DRM is that only one of the two models needs to be correctly specified to be able to properly identify the treatment effect; if there is misspecification in the MVR, in other words, missing and/or irrelevant covariates, the IPW will help correct for this. Based on this property, the DRM was chosen for the base case, with the MVR and IPW as sensitivity analyses. A naive comparison was also conducted to provide context as to the direction and extent of the population adjustments.
When conducting unanchored comparisons, there will always be uncertainty regarding any unknown or unmeasured prognostic factors that may influence the outcome of interest but are not captured in the statistical models. In order to mitigate this issue as much as possible, we conducted a targeted literature review to identify relevant prognostic factors that could potentially be adjusted for in the comparisons (see details in Supplementary Appendix B). Of the identified prognostic factors, age (<65 or ≥65 years), sex (males or females), race (Caucasian or non-Caucasian), smoking status (never smokers or current/former smokers), disease stage at initial diagnosis (limited or extensive), platinum sensitivity (sensitive or resistant) and ECOG PS (0 or >0) were reported in both CheckMate 032 and Flatiron, and could be considered for inclusion, regardless of the specific approach (MVR, IPW or DRM).
Cox proportional hazards models, with or without weights, were used to estimate naive and population-adjusted hazard ratios (HRs) of nivolumab versus SOC along with 95% CIs. The validity of assuming proportional hazards was assessed visually by inspecting plots of the log cumulative hazards and Schoenfeld residuals. All analyses were performed using R version 3.6.1 (http://www.r-project.org/), and mathematical details for all the models are presented in Supplementary Appendix C.
Results
The characteristics of 3L patients from CheckMate 032 and Flatiron are presented in Table 1. Both cohorts included 78 patients with a median age of 64 years. The proportion of males was slightly higher in CheckMate 032 (52.6%) compared with the Flatiron cohort (48.7%). Most patients were of Caucasian race in both cohorts, although 14.1% of patients from the Flatiron cohort were missing data regarding race. The proportion of current or former smokers was slightly higher in the Flatiron cohort (98.7%) than in CheckMate 032 (93.6%), and the proportion of platinum-sensitive patients was slightly higher in the Flatiron cohort (69.2%) than in CheckMate 032 (66.7%). Both cohorts were similar in terms of disease stage at diagnosis, with 26.9 and 28.2% of patients having LD in CheckMate 032 and Flatiron, respectively.
| Characteristics | CheckMate 032 (nivolumab), n (%) | Flatiron (standard of care), n (%) |
|---|---|---|
| n | 78 | 78 |
| Age (years): | ||
| – Mean (SD) | 63.1 (8.16) | 64 (10) |
| – Median | 64 | 64 |
| – Min, max | 45, 81 | 38, 84 |
| – <65 | 40 (51.3) | 41 (52.6) |
| – ≥65 and <75 | 33 (42.3) | NR |
| – ≥75 | 5 (6.4) | NR |
| – ≥65 | 38 (48.7) | 37 (47.4) |
| Sex: | ||
| – Males | 41 (52.6) | 38 (48.7) |
| – Females | 37 (47.4) | 40 (51.3) |
| Race: | ||
| – Caucasian | 72 (92.3) | 54 (69.2) |
| – Black or African–American | 4 (5.1) | 5 (6.4) |
| – Asian | 1 (1.3) | 2 (2.6) |
| – American–Indian or Alaska Native | 0 (0) | NR |
| – Other | 1 (1.3) | 6 (7.7) |
| – Missing | 0 (0) | 11 (14.1) |
| Smoking status: | ||
| – Current/former | 73 (93.6) | 77 (98.7) |
| – Never smoked | 5 (6.4) | 1 (1.3) |
| – Unknown | 0 (0) | 0 (0) |
| Disease stage at diagnosis: | ||
| – Limited | 21 (26.9) | 22 (28.2) |
| – Extensive | 57 (73.1) | 53 (67.9) |
| – Unknown | 0 (0) | 3 (3.8) |
| 1L platinum-treated subjects: | ||
| – Platinum-resistant | 26 (33.3) | 20 (25.6) |
| – Platinum-sensitive | 52 (66.7) | 54 (69.2) |
| – Unknown | 0 (0) | 4 (5.1) |
| ECOG PS: | ||
| – 0 | 25 (32.1) | 17 (21.8)† |
| – 1 | 52 (66.7) | 28 (35.9)† |
| – ≥2 | 1 (1.3)‡ | 6 (7.7)† |
| – NR | 0 (0) | 27 (34.6)† |
†
Closest score within 15 days prior to index date (start of 1L treatment).
‡
One patient was recorded as having an ECOG PS of 2.
1L: First-line; ECOG PS: Eastern Cooperative Oncology Group performance score; NR: Not reported; SD: Standard deviation.
ECOG PSs were available at the time of initiation of 1L therapy in Flatiron, although approximately one-third of patients had missing data, and showed that the distribution at this point in time was more skewed toward higher scores as compared with CheckMate 032. The lack of data at a comparable time point coupled with the high degree of missing values meant it was not possible to include this variable within the models; however, all of the remaining relevant prognostic factors that were reported in both datasets were included in the MVR, IPW and DRM models.
In the Flatiron cohort, the most commonly used treatments for 3L were paclitaxel and topotecan. Other 3L treatments included single-agent chemotherapy (e.g., gemcitabine, irinotecan or docetaxel), carboplatin-based doublets (e.g., carboplatin + etoposide, carboplatin + paclitaxel and carboplatin + irinotecan), as well as triplet combination chemotherapy regimens (e.g., cyclophosphamide + doxorubicin + vincristine and etoposide + paclitaxel + topotecan).
Figure 2 shows Kaplan–Meier curves for OS from both CheckMate 032 and Flatiron. The median OS estimate for 3L patients receiving nivolumab monotherapy in CheckMate 032 was 5.7 months (95% CI: 3.5–8.0) and the 1-year OS estimate was 28%. In the Flatiron cohort, chemotherapies for the 3L population were associated with a median OS of 3.8 months (95% CI: 2.8–4.9) and a 1-year OS estimate of 4%. Results of the naive, unadjusted comparison showed nivolumab monotherapy to be more efficacious compared with SOC (HR: 0.63; 95% CI: 0.44–0.90). Tests for proportional hazards also suggested this assumption was valid on the basis of the observed data (see details in Supplementary Appendix D).
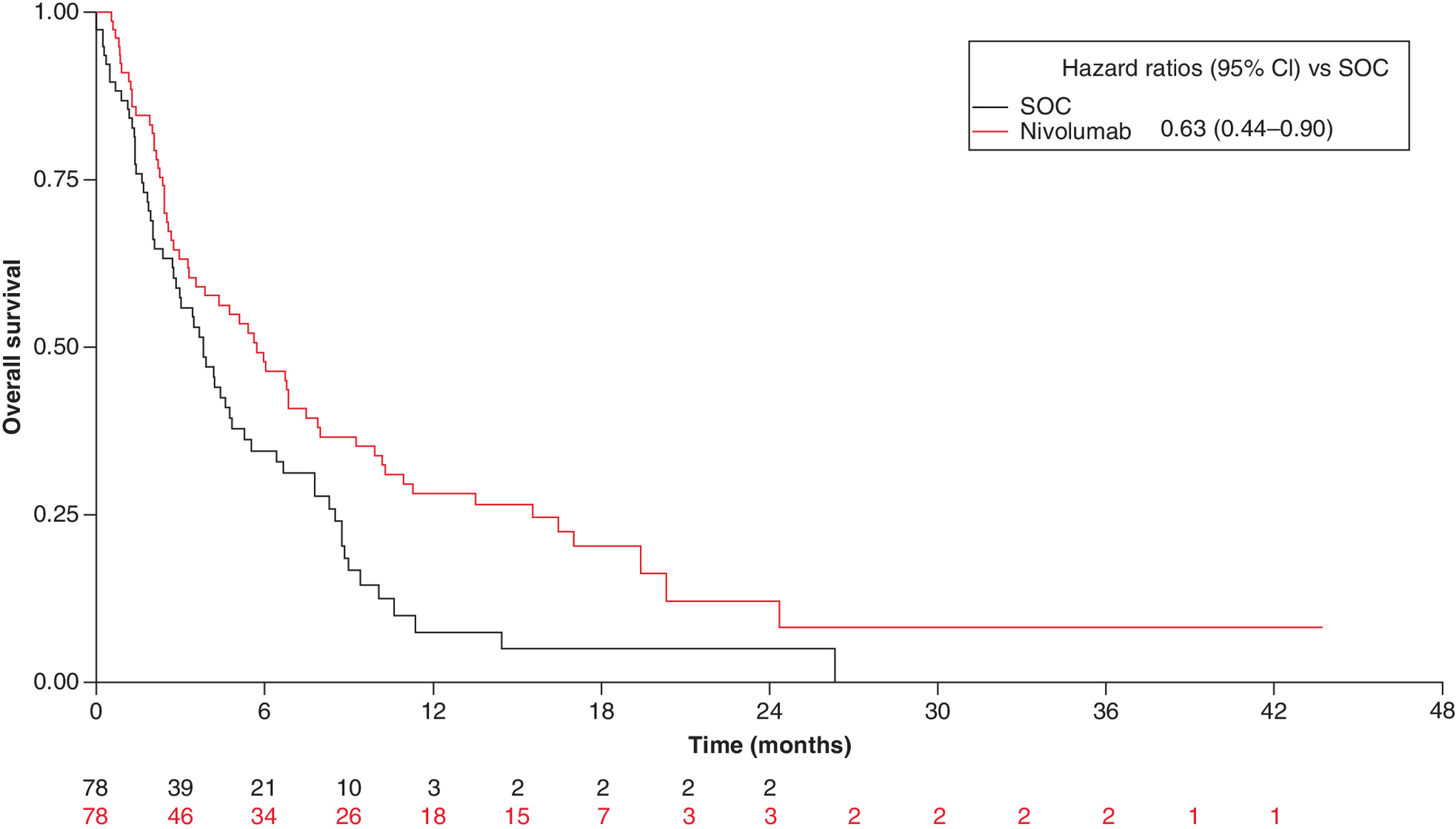
Figure 2. Unadjusted Kaplan–Meier curves for overall survival with nivolumab monotherapy and standard of care for third-line small-cell lung cancer patients.
SOC: Standard of care.
Results from the three different methods used to conduct the population-adjusted comparisons are presented in Table 2. Similar to the naive comparison, all three methods showed nivolumab to be superior to SOC. The base case DRM approach produced a HR of 0.68 (95% CI: 0.52–0.90) for nivolumab, which was closely aligned with the estimate from the IPW approach (HR: 0.70; 95% CI: 0.54–0.89). Conversely, the MVR model improved the HR for nivolumab compared with the naive comparisons, with an HR of 0.59 (95% CI: 0.39–0.88). Parameter estimates from the MVR model and the DRM are provided in Supplementary Appendix E, along with the weighted Kaplan–Meier curves from the IPW analysis.
Discussion
Although SCLC has high initial response rates to 1L therapies, nearly all ED patients experience disease recurrence and go on to develop resistance to subsequent therapies [1–3,19]. Prognosis remains poor for SCLC patients in general; median OS and 5-year survival rates are 8–13 months and 1–2%, respectively, for ED patients, with corresponding numbers for LD patients of 15–20 months and 10–20%, respectively [1,2,19–21]. Prognosis is particularly limited for those who reach 3L, for whom preferred treatment options still include cytotoxic chemotherapy or enrollment in a clinical trial. In the real-world cohort of patients used for this analysis, patients treated with chemotherapy in 3L had a median OS of 3.8 (95% CI: 2.8–4.9 months). The introduction of IO agents to both initial and subsequent lines of treatment for SCLC is intended to address some of the significant unmet need in this population [7].
Unlike the 1L setting where randomized controlled trial (RCT) evidence is available to determine what the extent of benefit with IO might be versus conventional chemotherapy, no RCTs featuring a PD-1 specifically in 3L currently exist (the CheckMate 331 trial compared nivolumab with chemotherapy in a broader population of patients with relapsed SCLC after platinum-based 1L chemotherapy). Furthermore, a systematic literature review that was conducted showed that there are few trials of chemotherapy in this population in general (see Supplementary Appendix A; note observational studies were not included in the review). Only nine potentially relevant studies (one RCT and eight single-arm studies) were identified that included 3L patients, six of which were published over 15 years ago. The three more recently published studies (one RCT [22] and two single-arm studies [23,24]) each included a subgroup of patients who had received two or more prior lines of therapy (16–50% of patients). All three studies demonstrated suboptimal survival outcomes, with median OS ranging from 4.6 to 6.8 months. Despite this weak evidence base, agents included in the single-arm trials (bendamustine [23], temozolomide [24] and irinotecan ± gemcitabine [22]) are recommended alongside nivolumab ± ipilimumab and pembrolizumab by the National Comprehensive Cancer Network for SCLC patients who have failed prior systemic therapy within 6 months in the primary or adjuvant setting, further highlighting the need for new treatment options [7].
Given the lack of published trial data, patient-level analyses were conducted in this study to compare the clinical efficacy in terms of OS for nivolumab monotherapy versus SOC in SCLC patients treated with two prior lines of chemotherapy or chemoradiotherapy, and without exposure to other IO agents. The results of these analyses demonstrate that nivolumab provides an OS advantage in the 3L setting compared with currently available SOC in the USA. All unadjusted and population-adjusted OS comparisons showed nivolumab to be more efficacious than SOC. The methods used for patient-level analyses align with recommendations from the NICE and can be considered as the best attempt to account for between-study differences given the challenge of evaluating comparative efficacy on the basis of observational and single-arm studies [17,18].
Population-adjusted analyses including an outcomes regression-based indirect comparison and matching-adjusted indirect comparison were previously conducted using IPD from CheckMate 032 and aggregate-level data from Flatiron, comparisons based on which are generally more prone to bias than those which utilize patient level data [25]. The results from these analyses were comparable to the current findings and showed improved efficacy in terms of OS in the 3L setting for nivolumab compared with SOC [25]. The similarity of results across these patient-level (i.e., IPD-IPD) and population-level (i.e., aggregate-IPD) methods demonstrates the robustness of the clinical findings and provides further evidence to support the use of nivolumab monotherapy as a 3L treatment option. The findings presented here also align with previous results from an aggregate-level matching analysis of nivolumab ± ipilimumab versus relevant comparators in the 2/3L setting, which showed that nivolumab regimens provided more favorable OS results relative to chemotherapies [26].
The methods used for this analysis were subject to some limitations. Although published information was used to identify prognostic factors and guide model development, there is still uncertainty regarding any unknown or unmeasured prognostic factors that may influence OS but were not captured in the models. The models were also constrained based on the number of covariates reported in CheckMate 032 and Flatiron. Known prognostic factors such as presence of liver metastases, prior surgery and prior radiotherapy were not available in Flatiron, and patients with brain metastases were excluded per eligibility criteria in CheckMate 032. ECOG PS was available at time of 1L treatment, and even at that time was skewed toward higher scores relative to CheckMate 032. In an attempt to control for differences in ECOG as much as possible, patients with a recorded PS of 0 or 1 at any time were included from Flatiron, but there remains a potential for bias as a result of not being able to properly adjust for the functional status of the Flatiron cohort at the time of 3L treatment. In addition, the small sample sizes for each of the treatment groups meant there was substantial uncertainty, particularly in later time periods where numbers at risk were very small. It is also important to highlight that NICE’s recommendations for population adjustment are provisional and that they identified a need for simulation studies to assess how vulnerable these methods are to failures in different assumptions [18]. Finally, no patients had received prior IO, which is now SOC after the positive results from the IMpower133 trial. Given the introduction of IO in earlier lines of therapy will likely have an impact on both the types of patients reaching 3L as well as available treatment options, the generalizability of these results will be limited in the longer term.
Conclusion
For patients with advanced SCLC who have failed two prior lines of chemotherapy, patient-level analyses to compare single-arm trial data with that from a real-world cohort suggest that nivolumab monotherapy improves OS compared with SOC in the USA. Findings from patient-level analyses were not sensitive to alternative regression and weighting methods, lending credibility to the analyses and conclusions. Given the high unmet need in this 3L SCLC population, results from this study will help inform decision makers of the potential therapeutic option of nivolumab monotherapy until results from other studies become available.
Future perspective
Within the next decade, it is anticipated that the role of IO for SCLC patients will be established, based on anticipated results from ongoing trials. It is expected that future clinical research may help to further elucidate the role of biomarkers in SCLC to identify subpopulations that may preferentially benefit from targeted therapies. More studies conducted in the 3L setting will help to provide additional treatment options for heavily pretreated SCLC patients.
•
The majority of patients with small-cell lung cancer (SCLC) are sensitive to first-line chemotherapy, and approximately 10–20% of patients who receive first-line treatment will subsequently receive therapy in the third-line (3L) setting.
•
Nivolumab ± ipilimumab is recommended by the National Comprehensive Cancer Network guidelines for SCLC patients who have failed prior systemic therapy within 6 months in the primary or adjuvant setting; however, the current National Comprehensive Cancer Network guidelines do not provide a specific treatment recommendation for the 3L setting.
•
CheckMate 032 results from the 3L patient population suggest that nivolumab is well tolerated and provides durable responses as a 3L treatment for recurrent SCLC.
•
Since CheckMate 032 does not include a comparator arm of standard chemotherapy, the aim of this study was to address this gap by estimating the comparative effectiveness of nivolumab versus standard of care (SOC) in the 3L setting using individual patient data (IPD) from CheckMate 032 and real-world electronic patient records from a US database.
•
Given that no studies were identified that reported outcomes separately for 3L SCLC patients (other than CheckMate 032), a subgroup of 3L patients that had not received an immuno-oncology agent in any line of therapy was constructed from the Flatiron database (January 2011–September 2017) that matched the eligibility criteria of CheckMate 032.
•
CheckMate 032 IPD from patients with exactly two prior lines of therapy who received 3L nivolumab monotherapy were included in the analysis.
•
Population-adjusted methods including regression models and weighting analyses as recommended by the National Institute for Health and Care Excellence Decision Support Unit were followed to estimate the relative treatment effect in terms of overall survival (OS) for nivolumab versus SOC.
•
Using IPD from both CheckMate 032 and Flatiron, patient-level analyses included a multivariable regression model, inverse probability weighting and a doubly robust method (base case).
•
All unadjusted and adjusted OS comparisons from the patient-level analyses produced statistically significant results in favor of nivolumab compared with SOC.
•
Findings were robust across adjustment methods.
•
For patients with advanced SCLC who have failed two prior lines of chemotherapy, results from patient-level analyses suggest nivolumab improves OS compared with agents that make up the existing SOC in the USA.
•
Given the high unmet need in this population, results from this study may help inform decision makers of the potential therapeutic option of nivolumab until results from other trials become available.
Financial & competing interests disclosure
This study was sponsored by Bristol Myers Squibb. JR Penrod, P Abraham, T Gu, A Juarez Garcia, TK Le, and Y Yuan are employees of Bristol Myers Squibb. B Korytowsky was an employee of Bristol Myers Squibb at the time the study was conducted. DR Camidge received funding from Bristol Myers Squibb. S Keeping, S Cope, K Chan, FR Wilson, and JP Jansen are employees of Precision HEOR. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Precision HEOR, funded by Bristol Myers Squibb, performed all analyses and provided professional editorial assistance.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (appendix.docx)
- Download
- 693.61 KB
References
1.
Byers LA, Rudin CM. Small cell lung cancer: where do we go from here? Cancer 121(5), 664–672 (2015).
2.
Van Meerbeeck JP, Fennell DA, De Ruysscher DK. Small-cell lung cancer. Lancet 378(9804), 1741–1755 (2011).
3.
Alvarado-Luna G, Morales-Espinosa D. Treatment for small cell lung cancer, where are we now?: a review. Transl. Lung Cancer Res. 5(1), 26–38 (2016).
4.
American Joint Committee on Cancer. Lung. In: AJCC Cancer Staging Manual. 8th Edition Springer, NY, USA (2016).
5.
Früh M, De Ruysscher D, Popat S, Crino L, Peters S, Felip E. Small-cell lung cancer (SCLC): ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 24(Suppl. 6), vi99–vi105 (2013).
6.
Rudin CM, Ismaila N, Hann CL et al. Treatment of small-cell lung cancer: American Society of Clinical Oncology Endorsement of the American College of Chest Physicians guideline. J. Clin. Oncol. 33(34), 4106–4111 (2015).
7.
National Comprehensive Cancer Network. Small cell lung cancer (version 1.2020) (2019). https://www.nccn.org/professionals/physician_gls/pdf/sclc.pdf
8.
Horn L, Mansfield AS, Szczesna A et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N. Engl. J. Med. 379(23), 2220–2229 (2018).
9.
Paz-Ares L, Dvorkin M, Chen Y et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomized, controlled, open-label, Phase III trial. Lancet 394(10212), 1929–1939 (2019).
10.
De Jong WK, Ten Hacken NH, Groen HJ. Third-line chemotherapy for small cell lung cancer. Lung Cancer 52(3), 339–342 (2006).
11.
Schwartzberg L, Korytowsky B, Penrod J et al. Developing a real-world 3L comparator to CheckMate 032: overall survival (OS) in patients with small cell lung cancer (SCLC). Presented at: 19th World Conference on Lung Cancer (WCLC 2018) of the International Association for the Study of Lung Cancer (IASLC). Toronto, Ontario, Canada, 23–26 September 2018.
12.
Minami S, Ogata Y, Ihara S, Yamamoto S, Komuta K. Retrospective analysis of outcomes and prognostic factors of chemotherapy for small-cell lung cancer. Lung Cancer (Auckl.) 7, 35–44 (2016).
13.
Ready N, Farago AF, De Braud F et al. Third-line nivolumab monotherapy in recurrent small cell lung cancer: checkMate 032. J. Thorac. Oncol. 14(2), 237–244 (2018).
14.
Antonia SJ, Lopez-Martin JA, Bendell JC et al. Checkmate 032: nivolumab (N) alone or in combination with ipilimumab (I) for the treatment of recurrent small cell lung cancer (SCLC). J. Clin. Oncol. 34(Suppl. 15), 100–100 (2016).
15.
US FDA. FDA approves pembrolizumab for metastatic small cell lung cancer. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pembrolizumab-metastatic-small-cell-lung-cancer
16.
Chung HC, Piha-Paul SA, Lopez-Martin J et al. Pembrolizumab after two or more lines of prior therapy in patients with advanced small-cell lung cancer (SCLC): results from the KEYNOTE-028 and KEYNOTE-158 studies. Presented at: AACR Annual Meeting. Atlanta, GA, USA, (July 2019) (Abstract CT073).
17.
Faria R, Hernandez Alava M, Manca A, Wailoo A. NICE DSU Technical Support Document 17: The Use of Observational Data to Inform Estimates of Treatment Effectiveness in Technology Appraisal: Methods for Comparative Individual Patient Data. NICE, Sheffield, UK (2015).
18.
Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton KJ. NICE DSU Technical Support Document 18: Methods for Population-Adjusted Indirect Comparisons in Submissions to NICE. NICE, Sheffield, UK (2016).
19.
Demedts IK, Vermaelen KY, Van Meerbeeck JP. Treatment of extensive-stage small cell lung carcinoma: current status and future prospects. Eur. Respir. J. 35(1), 202–215 (2010).
20.
Hurwitz JL, Mccoy F, Scullin P, Fennell DA. New advances in the second-line treatment of small cell lung cancer. The Oncologist 14(10), 986–994 (2009).
21.
Chan BA, Coward JI. Chemotherapy advances in small-cell lung cancer. J. Thoracic Dis. 5(Suppl. 5), S565–S578 (2013).
22.
Pallis AG, Agelidou A, Agelaki S et al. A multicenter randomized Phase II study of the irinotecan/gemcitabine doublet versus irinotecan monotherapy in previously treated patients with extensive stage small-cell lung cancer. Lung Cancer 65(2), 187–191 (2009).
23.
Lammers PE, Shyr Y, Li C-I et al. Phase II study of bendamustine in relapsed chemotherapy sensitive or resistant small-cell lung cancer. J. Thoracic Oncol. 9(4), 559–562 (2014).
24.
Pietanza MC, Kadota K, Huberman K et al. Phase II trial of temozolomide in patients with relapsed sensitive or refractory small cell lung cancer, with assessment of methylguanine-DNA methyltransferase as a potential biomarker. Clin. Cancer Res. 18(4), 1138–1145 (2012).
25.
Cope S, Popoff E, Keeping S et al. PCN21 – Comparative efficacy of nivolumab ± ipilimumab versus standard of care (SOC) for third-line (3L) patients with recurrent small cell lung cancer (SCLC) using population-adjusted indirect comparison. Value Health 21(Suppl. 3), S18 (2018).
26.
Cope S, Keeping ST, Goldgrub R et al. Indirect comparison of nivolumab ± ipilimumab (CheckMate 032) versus other treatments for recurrent small-cell lung cancer. J. Comp. Eff. Res. 8(10), 733–751 (2019).
Information & Authors
Information
Published In
Pages: 1275 - 1284
PubMed: 33140652
Copyright
© 2020 Sam Keeping. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 3 July 2020
Accepted: 23 September 2020
Published online: 3 November 2020
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of nivolumab versus standard of care for third-line patients with small-cell lung cancer. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0134
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Franziska Dirnberger, Sachin Patel, Devon J. Boyne, Zhiyi Lan, Jenny Uyei, Jessie Wang, Seoyoon Cho, Lucy DeCosta, Ian M. Bridges, Umit Tapan, Matching-Adjusted Indirect Comparison of Tarlatamab for Patients with Platinum-Refractory or Platinum-Resistant Extensive-Stage Small-Cell Lung Cancer , Advances in Therapy, 10.1007/s12325-026-03659-4, (2026).
- Rumbidzai Takundwa, Gaurav Suri, Franziska Dirnberger, Andre Verhoek, Elizabeth Vinand, Jessie Wang, Stephen Puntis, Xerxes Pundole, Fiona Blackhall, Matching-Adjusted Indirect Treatment Comparison of Tarlatamab Versus Comparator Therapies in England in Patients with Extensive-Stage Small Cell Lung Cancer Who Have Received Two or More Prior Lines of Therapy, Advances in Therapy, 10.1007/s12325-025-03376-4, 42, 12, (6078-6090), (2025).
- Jessie Wang, Gautam Sajeev, Xinglei Chai, Rumbidzai Takundwa, Franziska Dirnberger, Xerxes Pundole, Malaika Pastel, Hongbo Yang, Umit Tapan, Efficacy outcomes between tarlatamab and real-world physicians’ choice of therapies for previously treated extensive stage small cell lung cancer, The Oncologist, 10.1093/oncolo/oyaf256, 30, 9, (2025).
- Jair Bar, Qingqing Xu, Sudeep Karve, Pooja Hingorani, Amin A. Virani, Neal E. Ready, Real‐World Response and Survival Outcomes and Treatment Patterns in Patients With Extensive Stage Small‐Cell Lung Cancer Receiving Third‐Line Treatment, Cancer Reports, 10.1002/cnr2.70289, 8, 8, (2025).
- Eunso Lee, Jeong Yun Jang, Jinho Yang, Uncommon Adverse Events of Immune Checkpoint Inhibitors in Small Cell Lung Cancer: A Systematic Review of Case Reports, Cancers, 10.3390/cancers16101896, 16, 10, (1896), (2024).
- Julie E. Park, Harlan Campbell, Kevin Towle, Yong Yuan, Jeroen P. Jansen, David Phillippo, Shannon Cope, Unanchored Population-Adjusted Indirect Comparison Methods for Time-to-Event Outcomes Using Inverse Odds Weighting, Regression Adjustment, and Doubly Robust Methods With Either Individual Patient or Aggregate Data, Value in Health, 10.1016/j.jval.2023.11.011, 27, 3, (278-286), (2024).
- Jing Zhao, Xiaoli Zhuo, Lei Liu, Zhe Yang, Guobin Fu, Opportunities and challenges of immune checkpoint inhibitors for extensive‐stage small‐cell lung cancer, Cancer Innovation, 10.1002/cai2.23, 1, 2, (183-193), (2022).
- 皓悦 王, Research on Targeting and Immunotherapy of Small Cell Lung Cancer, Advances in Clinical Medicine, 10.12677/ACM.2022.1281009, 12, 08, (7005-7011), (2022).
- Apar Kishor P. Ganti, Billy W. Loo, Michael Bassetti, Collin Blakely, Anne Chiang, Thomas A. D'Amico, Christopher D'Avella, Afshin Dowlati, Robert J. Downey, Martin Edelman, Charles Florsheim, Kathryn A. Gold, Jonathan W. Goldman, John C. Grecula, Christine Hann, Wade Iams, Puneeth Iyengar, Karen Kelly, Maya Khalil, Marianna Koczywas, Robert E. Merritt, Nisha Mohindra, Julian Molina, Cesar Moran, Saraswati Pokharel, Sonam Puri, Angel Qin, Chad Rusthoven, Jacob Sands, Rafael Santana-Davila, Michael Shafique, Saiama N. Waqar, Kristina M. Gregory, Miranda Hughes, Small Cell Lung Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology, Journal of the National Comprehensive Cancer Network, 10.6004/jnccn.2021.0058, 19, 12, (1441-1464), (2021).
- Caitlin Smare, Kiran Dave, Ariadna Juarez-Garcia, Pranav Abraham, John R. Penrod, D. Ross Camidge, Yong Yuan, Cost-effectiveness of nivolumab monotherapy in the third-line treatment of small cell lung cancer, Journal of Medical Economics, 10.1080/13696998.2021.1974763, 24, 1, (1124-1133), (2021).