Golimumab improves patient-reported outcomes in daily practice of inflammatory rheumatic diseases in Germany
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To analyze the quality of life (QoL), work productivity and activity impairment (WPAI) and healthcare resource utilization (HCRU) in rheumatoid arthritis (RA), psoriatic arthritis (PsA) and ankylosing spondylitis (AS) patients receiving golimumab under routine clinical settings in Germany. Materials & methods: Prospective observational study, GO-ART, analyzed changes in WPAI, QoL and HCRU during 24 months of golimumab therapy. Results: Seven hundred and forty-eight patients (RA = 250, PsA = 249 and AS = 249) were enrolled. Substantial improvements in WPAI scores presenteeism, activity impairment and total work productivity impairment and QoL were observed at month three and were maintained through month 24. Fewer patients had disease-related hospitalizations and consulted physician at month 24 than at the baseline. Conclusion: Golimumab induces sustained improvements in WPAI and QoL and reduces healthcare resource utilization in RA, PsA and AS.
Rheumatoid arthritis (RA), psoriatic arthritis (PsA) and ankylosing spondylitis (AS) are inflammatory diseases affecting joints and are associated with pain, joint damage and reduced mobility [1]. In consequence, these rheumatic diseases lead to impaired work and daily activities and decreased quality of life (QoL). RA, PsA and AS are furthermore associated with significant healthcare resource utilization (HCRU) due to a high number of hospitalizations and intensive out-patient care [2].
Several therapeutic approaches, including steroids, nonsteroidal anti-inflammatory drugs and biologics, were shown to improve the clinical outcomes of RA, PsA and AS. In addition, there is an increased interest in evaluating the patients’ perspective on their health condition under the therapy. Several disease-tailored tools were developed and validated to measure patient-reported outcomes (PRO), including QoL, in rheumatic diseases. Additionally, the introduction of Work Productivity and Activity impairment (WPAI) questionnaire allowed an insight into how disease and therapy influence work productivity. For instance, the impact of biologic therapies on work attendance, at-work productivity and QoL was assessed in a number of clinical trials and observational studies [3–7].
Golimumab is a human TNF-α-targeting antibody approved in the USA and Europe for treatment of RA, PsA and AS. Several large scale randomized controlled clinical trials [8–10] and noninterventional studies [3,11,12] have demonstrated clinical efficacy and safety of golimumab therapy in these diseases. However, the data on the impact of golimumab on PRO and HCRU in daily clinical practice are scarce. Currently available real-world evidence (RWE) showed that golimumab improves the WPAI scores in RA, PsA and AS patients [7] and decreases HCRU in AS patients [3].
Here, we present the RWE data from the GO-ART study aiming to investigate the impact of golimumab therapy on WPAI, QoL and HCRU among the German patients suffering from RA, PsA and AS.
Materials & methods
Study design & participants
This was a prospective noninterventional, open-label study conducted from March 2014 (first patient, first visit) to May 2018 (last patient, last visit) at 63 study sites in Germany. Adult patients with RA, AS or PsA, who were not previously treated with golimumab, were enrolled into the study. Patients, who switched to golimumab from prior biologic treatment due to a serious adverse event, opportunistic infection or hypersensitivity were excluded from enrollment. Patients with active tuberculosis or other severe infections (such as sepsis, abscesses and opportunistic infections) as well as moderate-to-severe heart failure (New York Heart Association class III/IV) were also excluded.
Golimumab was prescribed as part of routine clinical practice in accordance with the terms of the marketing authorization in Germany, the treatment decision was independent of participation in the study. All subjects were initially followed for 1 year (also if golimumab treatment was stopped or interrupted). Patients, who were still on golimumab treatment at month 12, were eligible for the observation period extension and were followed for one additional year; in other words, a total period of 2 years. Each patient gave written informed consent prior to inclusion (a separate informed consent was obtained for the second year extension). The study was conducted in compliance with the Declaration of Helsinki, national regulatory recommendations for noninterventional studies, and all applicable laws and regulations. The study was approved on 9 December 2013 by the competent independent ethics committee of the Bavarian State Medical Association, Munich, Germany (approval number 13113). Data management, statistical analysis and preparation of the study report were performed by MedPharmTec GmbH, Munich, Germany, and sponsored by MSD Sharp & Dohme GmbH.
Assessments
The results of tuberculosis screening, and medical and medication history (including disease-related hospitalizations from the physician's own record), were collected at the baseline visit. Patient demographic data, information on concomitant disease and medications and vital signs as well as physical exam including skin examination were documented by physicians at the baseline and on each subsequent study visit. Any hospitalization and HCRU, doses and dates of golimumab administration as well as reasons for treatment discontinuation and the date of the last dose of golimumab, if applicable, were recorded by the patient in a paper diary and verified by the physician at each post-baseline visit.
PRO related to loss of work productivity and impairment of nonwork activity were measured with WPAI questionnaire. WPAI is a 1D questionnaire consisting of six questions addressing four domains: presenteeism (reduced on-the-job effectiveness), absenteeism (work time missed), total work productivity impairment (TWPI, absenteeism and presenteeism combined) and activity impairment. Scores for each domain range from 0 to 100% with higher values indicating greater impairment. Disease-specific QoL questionnaires included rheumatoid arthritis quality of life (RAQoL), ankylosing spondylitis quality of life (ASQoL) and nail assessment in psoriasis and psoriatic arthritis quality of life (NAPPA-QoL) questionnaires. NAPPA-QoL is a 20-item nail-specific QoL questionnaire (scored from 0 to 4) assessing nail status, stigma and emotional status and everyday life. The RAQoL questionnaire consists of 30 dichotomous questions (answered ‘yes’ and ‘no’) that assess moods and emotions, social life, hobbies, everyday tasks, personal and social relationships and physical contact. Eighteen questions of ASQoL questionnaire (scored 1 and 0) address the influence of the disease on daily activities, fatigue, pain, sleep, independence, relationships and mood. For each questionnaire, individual item scores are summed to give a total score or index, with a high score indicating a worse QoL. All PROs (WPAI and disease-specific QoL) were captured on hardcopy questionnaires and assessed at the baseline and after 3, 6, 12 and 24 months. The minimal clinically important difference (MCID) was set to two score points for change in RAQoL and 1.8 score points for change in ASQoL, according to previous literature [13,14].
For the HCRU analysis, the number of disease-related hospitalizations during 1 year period before baseline was compared with number of number of disease-related hospitalizations within the 2 years after the baseline. The investigator determined whether hospitalization was disease-related based on the following criteria: any medical intervention with a direct, causal relation to RA, AS or PsA which aimed at the prevention of disease progression or prevention, reduction, or cure of symptoms/damage induced by RA or secondary diseases due to the underlying rheumatic disease. Hospitalizations due to intolerance of therapy, drug interactions, pregnancy or treatment of adverse events related to prescribed drug, for example, opportunistic infection, allergic reaction, injection site reaction were not considered as disease-related. Additionally, a number and type of medical specialty consultations (general practitioner, gastroenterologist, ophthalmologist, rheumatologist, dermatologist, radiologist, cardiologist, neurologist, psychiatrist, orthopedist and other) was compared between the periods covering 3 months before baseline and month 21–24 after baseline.
Statistical analysis
The primary end point of the study was the change from baseline in WPAI scores after 3, 6, 12 and 24 months of treatment. Secondary end points included the change from baseline in disease-specific QoL after 3, 6, 12 and 24 months, and the evaluation of the administration frequency and dosage of golimumab. For the longitudinal analysis of the changes in the primary and secondary end points from the baseline, a repeated measurement model was applied where patient and time point were considered as random factors and error term and additional covariates (including age, gender and prior biologic therapy) were considered as fixed factors. Changes from baseline were analyzed by means of t-test or, if normality assumptions did not apply for the end point under consideration (i.e., if p for Shapiro-Wilk test was less than 0.05), by Wilcoxon signed-rank test. Pearson’s correlation coefficients (r) were used to assess the correlations between the WPAI and QoL scores at each study visit.
Results for primary end point analysis are shown for the modified intention-to-treat population (mITT), which included all patients who received at least one dose of golimumab, had a baseline assessment and at least one additional visit, and for the mITT subset with full-time or part-time employed patients at the baseline (mITTe). Secondary end point analysis was performed on mITT population. Additionally, the primary and secondary end points were analyzed according to treatment continuation (patients with ongoing golimumab treatment vs patients who permanently discontinued therapy).
Results
Patient disposition & baseline characteristics
Out of 749 patients enrolled into the study, 748 started golimumab therapy (safety population [SAF], Figure 1): 250 patients with RA, 249 with PsA and 249 with AS. Table 1 shows the baseline characteristic of the SAF population. Median age at registration was 50 years, 57% of patients were female. Two hundred and nineteen patients (29.3%) were smokers. Four hundred and sixty patients (61.5%) had concomitant diseases, most often hypertension (n = 192, 25.7%), followed by osteoarthritis (n = 61, 8.2%), diabetes mellitus (n = 60, 8.0%), osteoporosis (n = 43, 5.7%), depression (n = 41, 5.5%), psoriasis (n = 40, 5.3%) and latent tuberculosis (n = 26, 3.5%). Concomitant medication was documented for 637 patients (85.2% of SAF population, Supplementary Table 1), most frequently methotrexate (n = 297, 39.7%, particularly in RA and PsA patients), nonsteroidal anti-inflammatory drugs (n = 280, 37.4%, most often in AS patients) and systemic glucocorticoids (n = 244, 32.6%, most frequently in RA patients). Overall, 243 patients (32.5%) received prior biologic treatment, mainly anti-TNF therapies (Supplementary Table 1).

| n | Median (range), % | |
|---|---|---|
| Age at registration (years) | 748 | 50 (18–82) |
| BMI (kg/m2) | 748 | 26.5 (16.5–58.9) |
| Sex | ||
| Female | 426 | 57.0 |
| Male | 322 | 43.0 |
| Employment status | ||
| Full-time employment | 404 | 54.0 |
| Part-time employment | 121 | 16.2 |
| Retired | 51 | 6.8 |
| Incapable of working | 45 | 6.0 |
| Complete reduction in earning capacity | 44 | 5.9 |
| Other | 83 | 11.1 |
| Marital status | ||
| Married/living together | 507 | 67.8 |
| Single | 162 | 21.7 |
| Divorced | 49 | 6.6 |
| Widowed | 30 | 4.0 |
| Concomitant diseases | 460 | 61.5 |
| Concomitant medications | 637 | 85.2 |
| Prior biologic therapies | 243 | 32.5 |
BMI: Body mass index.
In total, 700 patients had at least one additional visit after the baseline (mITT population, 237 patients with RA, 235 with PsA and 228 with AS, Figure 1). Among this number, there were 493 patients full-time or part-time employed at the baseline (mITTe population, 158 patients with RA, 157 with PsA and 178 with AS). Six hundred and sixty-six patients in mITT population had documented visit at month 3 (95.1%), 634 had visit at month 6 (90.6%) and 552 had visit at month 12 (78.9%). Patients who remained on golimumab therapy (n = 348) were enrolled into the 1-year extension of the observational period, of which 303 patients had a visit at month 24 and 260 completed the study on treatment (37.1% of mITT, 91 patients with RA, 81 with PsA and 88 with AS). One hundred and eleven patients discontinued the study (15.9% of mITT), with the reason for discontinuation documented for 60 (withdrawal of consent, n = 45; relocation, n = 11; holiday, n = 3; and death n = 1). Golimumab treatment was prematurely terminated in 233 patients (33.3% of mITT). The main reasons for premature termination were lack of efficacy (n = 113), adverse drug reaction (n = 58) and switch to other therapy (n = 40).
Golimumab therapy
Most patients were initiated with the recommended induction dose of 50 mg (n = 737/748 patients, 98.5%). The remaining 11 patients were initiated with 100 mg dose (four patients had a body weight >100 kg). The vast majority of patients received 50 mg maintenance dose during the observational period (month 3: n = 649/660 patients, 98.3%; month 6: n = 587/598, 98.1%; month 12: n = 477/491, 97.1%; month 24: n = 286/301, 95.0%).
WPAI
WPAI was analyzed for patients with RA, PsA and AS employed at the baseline (mITTe set). Most pronounced improvements in scores for TWPI, absenteeism, presenteeism and activity impairment were observed during the first 3 months of golimumab treatment (Supplementary Figure 1; Table 2). Similar improvements in activity impairment were seen in the mITT population (Table 2). Scores for presenteeism, TWPI and activity impairment in all indications continued to improve until the end of the observation period (24 months). Regarding the absenteeism, improvements until month 24 were more pronounced in AS patients than in RA and PsA patients. Overall, improvements in all WPAI domain scores over the 24-month therapy period were most pronounced in AS patients (Supplementary Figure 1; Table 2).
| RA | PsA | AS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean (SD) | p-value | n | Mean (SD) | p-value | n | Mean (SD) | p-value | |
| TWPI (mITTe) | |||||||||
| Month 3 | 78 | -11.3 (23.77) | <0.0001† | 81 | -13.8 (25.02) | <0.0001† | 104 | -16.9 (26.62) | <0.0001‡ |
| Month 6 | 76 | -8.7 (30.74) | 0.0058‡ | 80 | -16.8 (28.26) | <0.0001‡ | 101 | -14.3 (32.82) | <0.0001† |
| Month 12 | 67 | -13.2 (23.40) | <0.0001† | 77 | -10.6 (30.40) | 0.0046‡ | 93 | -16.8 (31.92) | <0.0001† |
| Month 24 | 43 | -13.7 (25.84) | 0.0012† | 39 | -9.5 (28.99) | 0.0472† | 46 | -24.7 (32.71) | <0.0001† |
| Absenteeism (mITTe) | |||||||||
| Month 3 | 110 | -5.8 (29.37) | 0.0429‡ | 109 | -4.9 (28.33) | 0.0449‡ | 135 | -8.9 (30.73) | 0.0001‡ |
| Month 6 | 106 | -2.1 (36.42) | 0.5649‡ | 103 | -6.7 (29.48) | 0.0202‡ | 127 | -9.0 (32.43) | 0.0007‡ |
| Month 12 | 89 | -8.8 (35.51) | 0.0128‡ | 99 | -4.6 (30.62) | 0.2028‡ | 120 | -6.1 (31.46) | 0.0141‡ |
| Month 24 | 55 | -7.8 (30.73) | 0.0647‡ | 48 | -1.9 (31.56) | 0.6084‡ | 64 | -14.1 (33.29) | 0.0002‡ |
| Presenteeism (mITTe) | |||||||||
| Month 3 | 83 | -12.5 (23.00) | <0.0001‡ | 85 | -15.4 (25.98) | <0.0001‡ | 111 | -15.8 (24.66) | <0.0001‡ |
| Month 6 | 87 | -10.2 (27.58) | 0.0012‡ | 88 | -16.8 (28.20) | <0.0001‡ | 113 | -12.5 (29.38) | <0.0001‡ |
| Month 12 | 75 | -12.7 (22.08) | <0.0001‡ | 80 | -12.7 (27.82) | 0.0001‡ | 100 | -16.1 (30.45) | <0.0001† |
| Month 24 | 45 | -12.2 (26.10) | 0.0030† | 41 | -16.5 (26.84) | 0.0003† | 50 | -22.0 (28.64) | <0.0001† |
| Activity impairment (mITTe) | |||||||||
| Month 3 | 133 | -13.9 (26.77) | <0.0001‡ | 128 | -17.4 (30.44) | <0.0001‡ | 162 | -18.3 (26.43) | <0.0001‡ |
| Month 6 | 127 | -12.3 (28.73) | <0.0001‡ | 128 | -18.5 (30.65) | <0.0001‡ | 144 | -19.7 (29.85) | <0.0001† |
| Month 12 | 114 | -15.2 (24.23) | <0.0001‡ | 118 | -18.3 (30.28) | <0.0001† | 130 | -22.8 (28.77) | <0.0001† |
| Month 24 | 67 | -18.4 (26.32) | <0.0001† | 63 | -23.4 (31.36) | <0.0001† | 72 | -28.3 (29.79) | <0.0001‡ |
| Activity impairment (mITT) | |||||||||
| Month 3 | 192 | -12.4 (25.33) | <0.0001‡ | 188 | -18.1 (29.61) | <0.0001‡ | 203 | -17.9 (26.56) | <0.0001‡ |
| Month 6 | 173 | -12.1 (27.59) | <0.0001‡ | 189 | -17.7 (30.21) | <0.0001‡ | 187 | -19.7 (28.72) | <0.0001‡ |
| Month 12 | 158 | -14.6 (23.38) | <0.0001‡ | 166 | -18.4 (30.87) | <0.0001† | 160 | -22.7 (27.60) | <0.0001‡ |
| Month 24 | 91 | -19.8 (25.90) | <0.0001† | 84 | -25.4 (30.60) | <0.0001‡ | 95 | -26.8 (28.74) | <0.0001‡ |
†
t-test.
‡
Wilcoxon signed-rank test.
AS: Ankylosing spondylitis; mITT: Modified intention-to-treat population; mITTe: Modified intention-to-treat population employed at the baseline; PsA: Psoriatic arthritis; RA: Rheumatoid arthritis; SD: Standard deviation; TWPI: Total work productivity impairment.
We also compared WPAI scores between the patients within the mITTe population (irrespectively of indication) who continued and patients who discontinued golimumab during the 24-month observational period (n = 343 and n = 149, respectively; information on continuation or discontinuation of golimumab was missing for one patient). Patients who continued golimumab treatment had significant improvements in each WPAI domain at all time points up to the 24-month visit (Figure 2; Supplementary Table 2). In patients who discontinued the treatment, significant improvements were mainly restricted to the 3-months visit (TWPI, presenteeism and activity impairment) or were completely lacking (absenteeism).
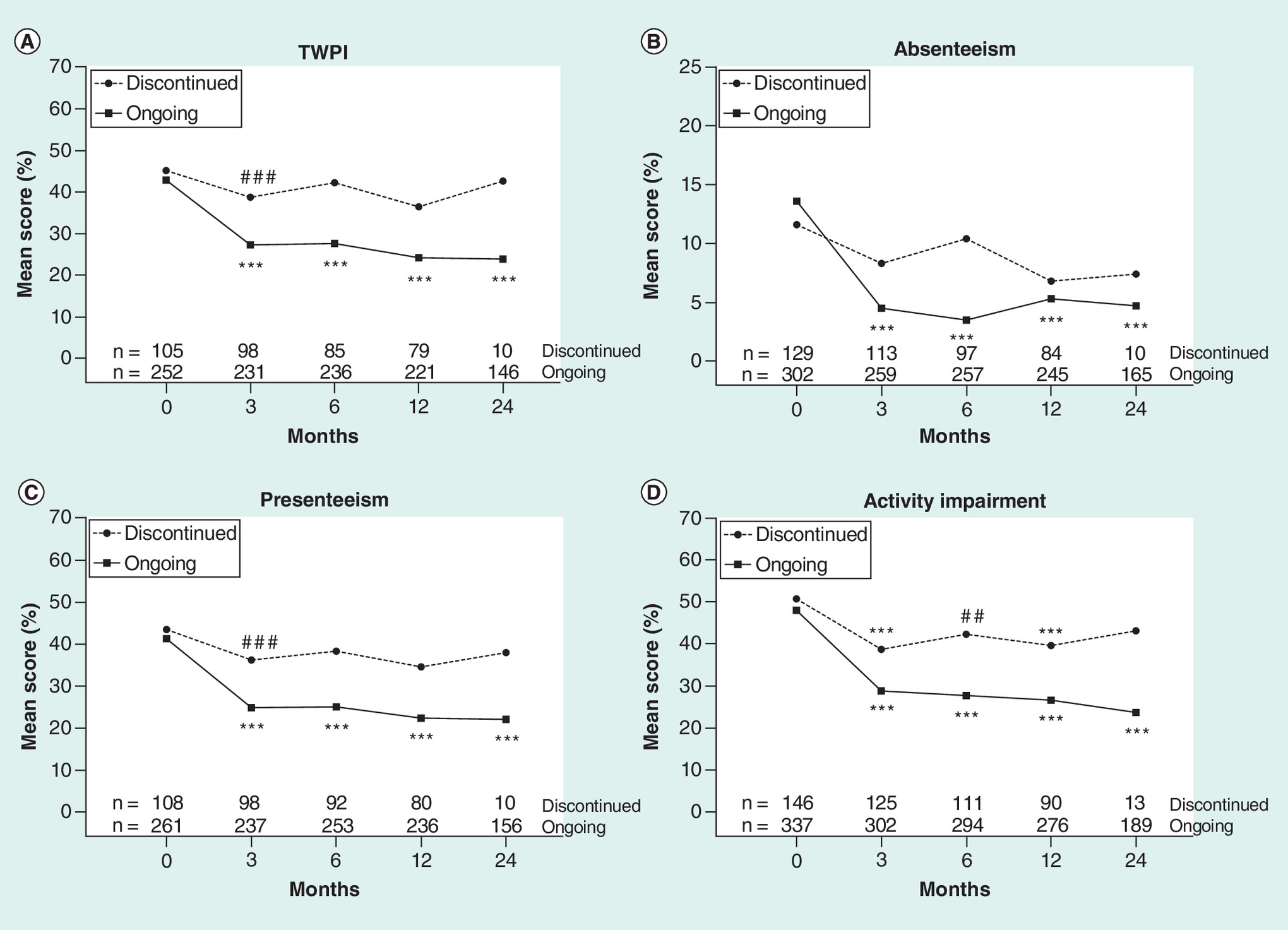
Figure 2. Mean Work Productivity and Activity Impairment scores according to golimumab continuation.
Scores are expressed as percentages (from 0 to 100%), with higher values indicating greater impairment. Allocation to ‘discontinued’ or ‘ongoing’ golimumab treatment category was based on overall treatment status (from the baseline to month 24).
***p < 0.001 (using Wilcoxon signed-rank test), ##p < 0.01, ###p < 0.001 (using t-test).
mITTe: Modified intention-to-treat population employed at the baseline; TWPI: Total work productivity impairment.
Quality of life
QoL was analyzed based on questionnaire data from 237 RA patients, 235 PsA patients and 228 AS patients from mITT set. Disease-specific QoL gradually improved over the entire observational period. Improvements were significant at each study visit and were most pronounced during the first 3 months of treatment (Supplementary Figure 2; Table 3).
| RAQoL | NAPPA-QoL | ASQoL | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean (SD) | p-value | n | Mean (SD) | p-value | n | Mean (SD) | p-value | |
| Month 3 | 203 | -1.7 (6.25) | <0.0001 | 196 | -4.8 (12.89) | <0.0001 | 203 | -3.0 (4.45) | <0.0001 |
| Month 6 | 190 | -2.3 (7.07) | <0.0001 | 195 | -5.9 (13.61) | <0.0001 | 185 | -3.4 (4.79) | <0.0001 |
| Month 12 | 166 | -2.7 (6.46) | <0.0001 | 169 | -6.7 (14.79) | <0.0001 | 162 | -4.1 (5.11) | <0.0001 |
| Month 24 | 95 | -3.2 (7.14) | <0.0001 | 83 | -10.3 (15.17) | <0.0001 | 95 | -4.4 (5.22) | <0.0001 |
All p-values are based on Wilcoxon signed-rank test.
ASQoL: Ankylosing Spondylitis Quality of Life; mITT: Modified intention-to-treat population; NAPPA-QoL: Nail Assessment in Psoriasis and Psoriatic Arthritis Quality of Life; RAQoL: Rheumatoid Arthritis Quality of Life; SD: Standard deviation.
QoL was also compared between the patients from mITT set who continued (RA, n = 152; PsA, n = 152; AS, n = 164) and who discontinued the therapy during the 24-month period (RA, n = 84, treatment status was missing for one patient; PsA, n = 83; AS, n = 64). Overall, the benefit in disease-specific QoL was greater in patients who continued treatment with statistically significant changes at each study visit (Figure 3; Supplementary Table 3). In patients who discontinued treatment, gains in QoL were less pronounced (as in RA and AS patients) or not observed (in PsA patients).
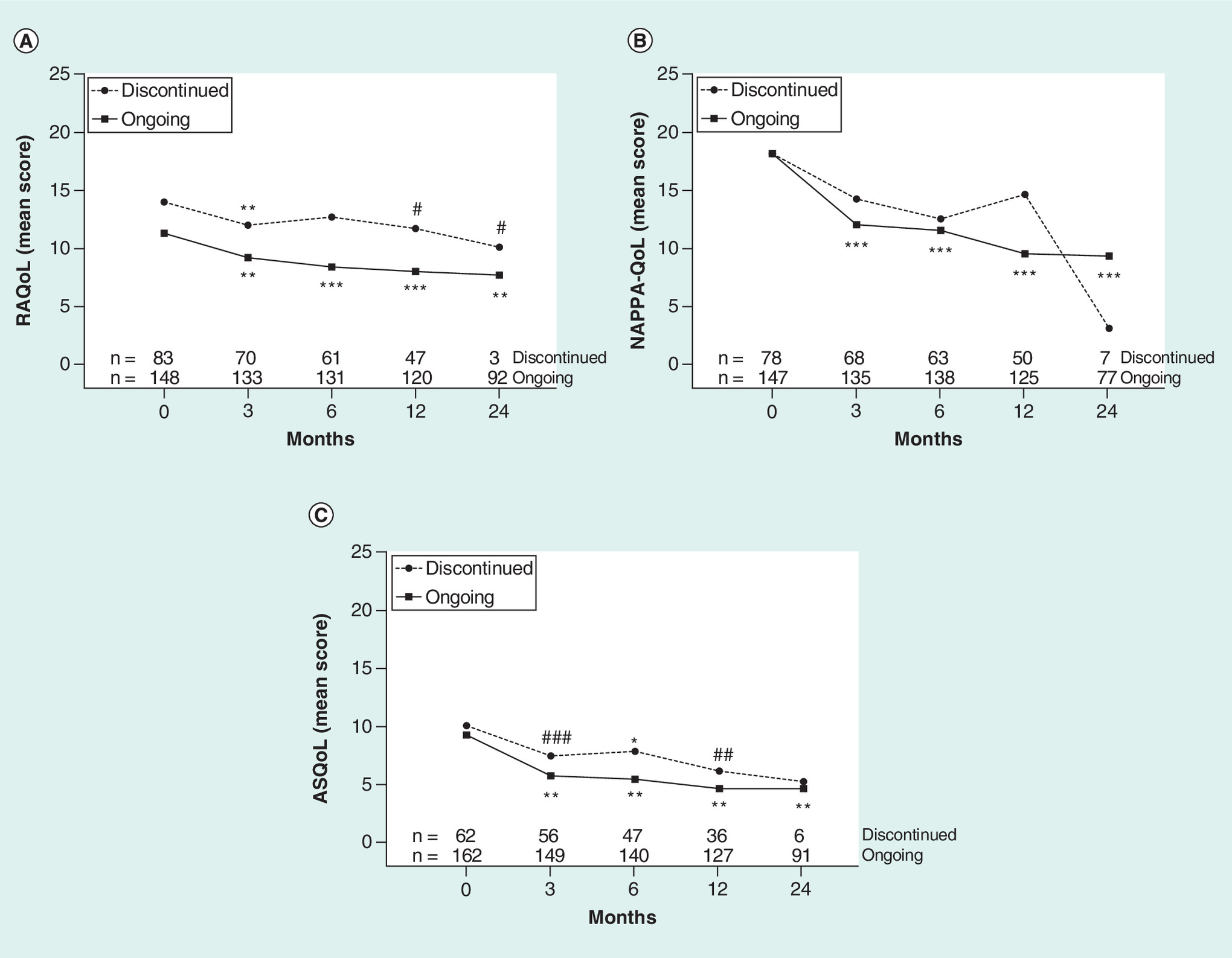
Figure 3. Mean health-related quality of life scores according to golimumab continuation (modified intention-to-treat).
Rheumatoid Arthritis Quality of Life, Nail Assessment in Psoriasis and Psoriatic Arthritis Quality of Life and Ankylosing Spondylitis Quality of Life questionnaire scores are expressed on range from 0 to 30, 80 and 18, respectively, with higher scores indicating poorer quality of life. Allocation to ‘discontinued’ or ‘ongoing’ golimumab treatment category was based on overall treatment status (from the baseline to month 24).
*p < 0.05; **p < 0.01; ***p < 0.001 (using Wilcoxon signed-rank test), #p < 0.05; ##p < 0.01; ###p < 0.001 (using t-test).
ASQoL: Ankylosing spondylitis quality of life; mITT: Modified intention-to-treat population; NAPPA-QoL: Nail assessment in psoriasis and psoriatic arthritis quality of life; RAQoL: Rheumatoid Arthritis Quality of Life.
A share of RA patients with MCID in RAQoL (≥2 points improvement) increased over time from 44.8% at month 3 to 65.3% at month 24 (Supplementary Table 4). Proportion of AS patients with MCID in ASQoL (≥1.8 points improvement) increased from 51.2% at month 3 to 59.9% and 57.9% at month 12 and 24, respectively. Therapy continuation did not affect the MCID rates in RA patients, with the exception of month 6 when a numerically larger proportion of patients who remained on golimumab therapy had a higher MCID than those who discontinued the study drug (50.4 vs 41.7%). Regarding the AS patients, improvements were greater in patients with ongoing golimumab treatment than in patients who discontinued (53.4 vs 45.5%, 55.4 vs 39.1% and 61.9 vs 52.8% after 3, 6 and 12 months, respectively). MCID was evaluable for only a few patients with treatment discontinuation at month 24 (three RA patients and six AS patients). Therefore, no comparative statements were drawn for this time point (Supplementary Table 4).
Relationship between WPAI & QoL
Additionally, we investigated the relationship between WPAI and disease-specific QoL during the 24 months of therapy in the mITTe set (Table 4). We observed a statistically significant positive linear correlation (Pearson’s correlation coefficient >0) between the scores for WPAI presenteeism and activity impairment and scores for RAQoL, NAPPA-QoL and ASQoL at each study visit. TWPI scores correlated with RAQoL and ASQoL scores over the entire observation period and with NAPPA-QoL scores up until month 12. In general, the association of absenteeism and QoL was weaker with a statistically significant correlation observed at the baseline and at month 3, 6 and 24 for RAQoL and up until month 12 for ASQoL. Statistically significant correlation between the scores for the absenteeism and NAPPA-QoL was observed only at month 6 (Table 4).
| Study visit | RAQoL | NAPPA-QoL | ASQoL | ||||
|---|---|---|---|---|---|---|---|
| Pearson’s r | p-value | Pearson’s r | p-value | Pearson’s r | p-value | ||
| TWPI | Baseline | 0.653 | <0.0001 | 0.36 | 0.0001 | 0.646 | <0.0001 |
| Month 3 | 0.556 | <0.0001 | 0.269 | 0.0068 | 0.737 | <0.0001 | |
| Month 6 | 0.688 | <0.0001 | 0.407 | <0.0001 | 0.696 | <0.0001 | |
| Month 12 | 0.614 | <0.0001 | 0.518 | <0.0001 | 0.71 | <0.0001 | |
| Month 24 | 0.687 | <0.0001 | 0.268 | 0.0684 | 0.554 | <0.0001 | |
| Absenteeism | Baseline | 0.351 | <0.0001 | 0.16 | 0.0624 | 0.314 | <0.0001 |
| Month 3 | 0.26 | 0.004 | 0.056 | 0.5448 | 0.345 | <0.0001 | |
| Month 6 | 0.218 | 0.0171 | 0.213 | 0.0221 | 0.277 | 0.0013 | |
| Month 12 | 0.165 | 0.0985 | 0.154 | 0.1024 | 0.304 | 0.0005 | |
| Month 24 | 0.4 | 0.0014 | -0.107 | 0.4349 | 0.104 | 0.397 | |
| Presenteeism | Baseline | 0.617 | <0.0001 | 0.358 | <0.0001 | 0.646 | <0.0001 |
| Month 3 | 0.606 | <0.0001 | 0.272 | 0.0044 | 0.723 | <0.0001 | |
| Month 6 | 0.703 | <0.0001 | 0.358 | <0.0001 | 0.673 | <0.0001 | |
| Month 12 | 0.588 | <0.0001 | 0.511 | <0.0001 | 0.744 | <0.0001 | |
| Month 24 | 0.636 | <0.0001 | 0.561 | <0.0001 | 0.509 | <0.0001 | |
| Activity impairment | Baseline | 0.646 | <0.0001 | 0.311 | <0.0001 | 0.702 | <0.0001 |
| Month 3 | 0.707 | <0.0001 | 0.439 | <0.0001 | 0.747 | <0.0001 | |
| Month 6 | 0.713 | <0.0001 | 0.479 | <0.0001 | 0.732 | <0.0001 | |
| Month 12 | 0.668 | <0.0001 | 0.452 | <0.0001 | 0.798 | <0.0001 | |
| Month 24 | 0.672 | <0.0001 | 0.408 | 0.0001 | 0.751 | <0.0001 | |
ASQoL: Ankylosing Spondylitis Quality of Life; mITTe: Modified intention-to-treat population employed at the baseline; NAPPA-QoL: Nail Assessment in Psoriasis and Psoriatic Arthritis Quality of Life; RAQoL: Rheumatoid Arthritis Quality of Life; TWPI: Total work productivity impairment.
Healthcare resource utilization
In patients who remained on golimumab therapy, the rate of disease-related hospitalizations decreased during the 2 years of the study compared with the year prior to baseline by 5.3% in RA, 4% in PsA and 6.6% in AS patients.
Moreover, number of medical specialty consultations per patient was lower at month 24 than at the baseline (retrospective evaluation for the past 3 months, mITT, Supplementary Table 5). The number of rheumatologist consultations decreased from the baseline to month 24 among the patients with RA (2.4 vs 2 visits), PsA (2.1 vs 1.5 visits) and AS (3.3 vs 1.6 visits). Similarly, there was a reduction in the mean number of general practitioner consultations from the baseline to month 24 in RA patients (2 vs 1.6 visits), PsA patients (2.4 vs 2.2 visits) and in AS patients (2.4 vs 1.8 visits). However, the mean number of radiologist consultations slightly increased from the baseline to month 24 among the RA (1.1 vs 1.5 visits) and PsA patients (1.2 vs 2 visits) but not in AS patients (1.6 vs 1 visits). The mean number of dermatologist consultations among the PsA patients remained unchanged (1.3 visits at the baseline and 1.4 visits at month 24). Finally, share of patients that consulted the physicians was lower at month 24 compared with the baseline (Supplementary Table 5). Changes in other medical specialty consultations were not observed (data not shown).
Discussion
Our study demonstrated that golimumab therapy improves PRO under real-world conditions and reduces HCRU in patients suffering from RA, PsA and AS.
Golimumab improved scores in all WPAI domains and QoL in patients suffering from RA, PsA and AS within 3 months of therapy and this effect was preserved over the 24-month observation period. Our results suggest that therapy continuation through 24 months maintained these improvements, whereas the discontinuation of golimumab appeared to reduce the magnitude and duration of therapy benefit.
Compared with previous RWE on golimumab from the noninterventional GO ACTIVE study, improvements in TWPI after 3 months of therapy reported here were lower in patients with RA (19.7 vs 40%, relative to the baseline = 100%), similar in patients with PsA (29.6 vs 31%) and higher in patients with AS (37.8 vs 31% [7]). The GO ACTIVE study also demonstrated similar improvements in QoL among PsA patients (4.8 vs -5) and better gains in QoL in RA (-1.7 vs -7) and AS patients (3 vs -5 [7]) than shown in the present study. These differences could be attributed to the facts that in the GO ACTIVE study, mean disease duration was shorter and more patients were biologics-naive than in the present analysis (77 vs 67.5%) which could improve the PRO in some groups of patients. The observational QUO-VADIS study demonstrated that after 6 months of golimumab or infliximab therapy, AS patients had larger reduction in all WPAI domain scores than reported here [3]. However, all patients included into the QUO-VADIS study were biologic-naive which again could result in a higher magnitude of benefit from TNF-α inhibition. In Phase III ATLAS study, adalimumab improved ASQoL scores by 3.2 at month 3 and 3.6 at month 6 [14], which was comparable to gains in QoL observed here (3.0 and 3.4, respectively).
We showed that improvement in TWPI, presenteeism and activity impairment scores during golimumab therapy in RA, PsA and AS patients was greater than in absenteeism. Studies investigating other TNF-α inhibitors also demonstrated lower improvements in absenteeism than in other WPAI domains. For instance, in the ATLAS study, mean improvements from baseline to month 6 induced by adalimumab in AS patients was only 2.7% for absenteeism while it was 17.2% for presenteeism, 16.2% for TWPI and 19.3% for activity impairment [4]. Compared with these results, changes at month 6 in AS patients receiving golimumab in our study were higher for absenteeism (9.0%), lower for presenteeism (12.5%) and similar for TWPI and activity impairment. In RA, an observational study investigating etanercept, a 6 month therapy induced similar improvements as reported here in scores for presenteeism and absenteeism whereas gains in TWPI (15.2%) and activity impairment (21.4%) were higher than in our study (8.7 and 12.3%, respectively [15]). In PsA, 6 months adalimumab therapy investigated in another observational study [16] resulted in a comparable improvements in absenteeism as in our patients, however, gains in TWPI (25.2%), presenteeism (24.3%) and activity impairment (27.1%) were higher than in the present study (16.8, 16.8 and 18.5%, respectively). Conversely, smaller improvements were reported for a 4-month adalimumab therapy in Phase III REVEAL study for TWPI (13.4%), presenteeism (12.9%) and absenteeism (1.9%), but not for activity impairment (18.8% [16]). However, considering the different study designs and the fact that most of the above mentioned studies enrolled patients that were not previously treated with biologics and had diverse baseline WPAI scores, a definitive conclusion on the relative impact of different TNF-α inhibitors on work productivity and activity cannot be drawn as of now.
To our knowledge, this study is the first to analyze the relationship between changes in WPAI and QoL in RA, PsA and AS patients receiving golimumab. Scores for TWPI, presenteeism and activity impairment showed a very strong positive correlation with QoL in patients with RA, PsA and AS. However, the correlation between scores for absenteeism and QoL was weak in patients with RA and AS while no correlation was observed in PsA patients. Similarly, studies investigating other TNF-α antagonists demonstrated a weak correlation between scores for absenteeism, in contrast to other WPAI domains, and different QoL instruments. For instance, in the ATLAS study in AS patients treated with adalimumab for 3 years, the correlation between ASQoL and absenteeism was weak (Pearson’s r = 0.44) while ASQoL moderately correlated with presenteeism (0.60), activity impairment (0.61) and TWPI (0.57) [4]. Compared with these results, our data from a 2 year treatment with golimumab revealed slightly higher correlation with ASQoL for activity impairment (0.75), comparable for TWPI (0.55) and weaker for presenteeism (0.51) and absenteeism (0.10). However, it should be noted that patients included into our study received golimumab for shorter period of time, and approximately a third of them received prior biologic therapy which could account for the differences in correlation levels. Also in adalimumab-treated RA patients, correlation between QoL (Health Assessment Questionnaire-Disability Index and EQ-5D-3L) and absenteeism was weaker than in case of other WPAI domains [6]. Our data indicate that the weak association of QoL with scores for absenteeism could be attributed to the fact that this WPAI domain demonstrated smaller improvements over the course of golimumab therapy, especially in RA and PsA patients. Alternatively, QoL questionnaires may not fully capture the patient’s perspective on the absence from work due to the disease. Unfortunately, head-to-head studies directly comparing several TNF-α inhibitors in regard to correlation between WPAI and QoL are lacking.
In addition to PROs improvement, golimumab therapy reduced the rates of disease-related hospitalizations and rheumatologist and GP consultations in all three groups of patients. Previously [3], 6 months therapy with golimumab was shown to reduce the percentage of biologic-naive AS patients with disease-related hospitalizations to a similar extent as shown here. Furthermore, 1 year therapy with TNF-α antagonists reduced both the number of emergency room visits and days of hospitalization in Taiwanese patients with RA, however, the number of outpatients visits was higher [17]. Overall, our data demonstrated that therapy with golimumab leads to reduction of HCRU, suggesting that golimumab may improve health economics in RA, PsA and AS patients. This notion is supported by the analyses demonstrating a cost–effectiveness of golimumab therapy among patients with PsA and AS [18,19]. Furthermore, a recent systematic review of 12 studies showed that patients treated with golimumab had higher persistence when compared with other anti-TNF treatments, especially in RA and PsA setting [20]. Therefore, use of golimumab might reduce HCRU also due to a high long-term persistence among the patients with rheumatic diseases using this medication.
Our study has several limitations. For instance, single-arm study design precluded the comparison of PROs and HCRU between patients treated and never treated with golimumab. Furthermore, 2-year follow-up may not be sufficiently long to capture long-term therapy outcomes in the chronic diseases investigated. Since the study was based in Germany, the results may not be generalizable to other national healthcare systems. Furthermore, given that primary and secondary objectives of the study focused on the analysis of QoL and HCRU, we did not report here data on efficacy and safety of golimumab which however has been done in numerous other studies on golimumab. Finally, analysis of HCRU was performed on 303 patients in mITT population who completed the entire 24-month follow-up period (with 260 remaining on golimumab therapy). It is thus reasonable to expect a higher HCRU particularly in patients with more severe disease and in those who did not respond to golimumab. Therefore, our results may not accurately reflect the rates of disease-related hospitalizations and physician consultations in all patients who received a golimumab at any point of therapy.
Conclusion
This prospective noninterventional, open-label study in Germany supported a beneficial effect of golimumab therapy in terms of improving PROs and reducing HCRU in patients with RA, PsA and AS in a routine clinical setting. Observed improvements in work productivity, daily activities and QoL were induced early during the therapy and maintained over the 24 months observation period. Furthermore, gains in presenteeism, TWPI and activity impairment correlated with improvements in QoL in all three indications. Given that fewer patients were hospitalized due to the disease and attended physicians during the second year of study, our results suggest that golimumab therapy may be cost-effective in RA, PsA and AS patients in the long-term.
•
Rheumatoid arthritis (RA), psoriatic arthritis (PsA) and ankylosing spondylitis (AS) are associated with work productivity and activity impairment (WPAI), decreased quality of life (QoL) and significant healthcare resource utilization (HCRU).
•
Golimumab, a human TNF-α-targeting antibody approved in the USA and Europe for treatment of RA, PsA and AS, demonstrated a clinical efficacy and manageable safety profile in several clinical trials and noninterventional studies. However, real-world evidence on WPAI, QoL and HCRU is scarce.
•
This prospective noninterventional study in Germany analyzed WPAI, QoL and HCRU among 748 patients with RA, PsA and AS that newly received golimumab for up to 24 months.
•
Golimumab improved WPAI domains absenteeism, presenteeism, activity impairment and total work productivity impairment (TWPI) during the first 3 months of therapy; benefits in presenteeism, activity impairment and TWPI were maintained through 24 months of therapy.
•
QoL improved over the entire golimumab therapy period in RA, PsA and AS patients as assessed by Rheumatoid Arthritis Quality of Life, Nail Assessment in Psoriasis and Psoriatic Arthritis Quality of Life and Ankylosing Spondylitis Quality of Life questionnaires, respectively.
•
QoL scores correlated with scores for WPAI domains presenteeism, activity impairment and TWPI in each indication.
•
Fewer patients had disease-related hospitalizations and consulted physician at month 24 than at the baseline.
•
In RA, PsA and AS patients, golimumab induces sustained improvements in the work productivity and QoL and reduces healthcare resource utilization in a routine clinical setting.
Author contributions
K Kruger contributed to the study design and was responsible for data acquisition and analysis, interpretation of results, and manuscript writing and editing. S Remstedt and A Thiele were responsible for data acquisition and analysis, and interpretation of results. S Hohenberger was responsible for interpretation of results, and manuscript writing and editing.
Acknowledgments
The authors thank the participating investigators and their staff for their commitment. We thank I Klaudius, MSD Sharp & Dohme GmbH, for support of the GO-ART study and insightful discussions relating to this work.
Financial & competing interests disclosure
This study was funded by MSD Sharp & Dohme GmbH, Haar, Germany. K Krueger received grants/research support from AbbVie, BMS, Celgene, Gilead, Hexal, Janssen Biologics, Lilly, MSD Sharp & Dohme GmbH, Pfizer, Roche, Sanofi-Aventis, UCB. S Remstedt received grants/research support from AbbVie, BMS, Celgene, Chugai, Hexal, Janssen Biologics, MSD Sharp & Dohme GmbH, Novartis, Pfizer, Roche, Sanofi-Aventis, UCB. A Thiele received grants/research support from Biogen, Celgene, Chugai, Hexal, Janssen-Cilag, Lilly, MSD Sharp & Dohme GmbH, Novartis, Pfizer, UCB. S Hohenberger is an employee of MSD Sharp & Dohme GmbH. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing and editorial support were provided by Y Holighaus and L Wujak, Alcedis GmbH, Giessen, Germany, and were funded by MSD Sharp & Dohme GmbH.
Ethical conduct of research
The authors state that they have obtained institutional review board approval from the competent independent ethics committee of the Bavarian State Medical Association, Munich, Germany, for the research described. The authors obtained written informed consent from the patients for the inclusion of their medical and treatment history and employment and marital status within this work.
Data sharing statement
The authors certify that this manuscript reports original non-interventional study data. The study protocol and synopsis of the study report are posted publicly at https://www.pei.de/SharedDocs/Downloads/DE/awb/nis-0201-0300/0256-beoplan.pdf?__blob=publicationFile&v=3 and at https://www.pei.de/SharedDocs/Downloads/DE/awb/nis-0201-0300/0256-abschlussb.pdf?__blob=publicationFile&v=4, according to the required timelines. Additional data will not be made publicly available.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_data.zip)
- Download
- 376.94 KB
References
1.
Schett G, Coates LC, Ash ZR, Finzel S, Conaghan PG. Structural damage in rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis: traditional views, novel insights gained from TNF blockade, and concepts for the future. Arthritis Res. Ther. 13(Suppl. 1), S4 (2011).
2.
Greenberg JD, Palmer JB, Li Y, Herrera V, Tsang Y, Liao M. Healthcare resource use and direct costs in patients with ankylosing spondylitis and psoriatic arthritis in a large US cohort. J. Rheumatol. 43(1), 88–96 (2016).
3.
Claudepierre P, van den Bosch F, Sarzi-Puttini P, Vastesaeger N, Govoni M, Kachroo S. Treatment with golimumab or infliximab reduces health resource utilization and increases work productivity in patients with ankylosing spondylitis in the QUO-VADIS study, a large, prospective real-life cohort. Int. J. Rheum. Dis. 22(6), 995–1001 (2019).
4.
Maksymowych WP, Gooch KL, Wong RL, Kupper H, van der Heijde D. Impact of age, sex, physical function, health-related quality of life, and treatment with adalimumab on work status and work productivity of patients with ankylosing spondylitis. J. Rheumatol. 37(2), 385–392 (2010).
5.
Nakagawa H, Tanaka Y, Sano S et al. Real-world postmarketing study of the impact of adalimumab treatment on work productivity and activity impairment in patients with psoriatic arthritis. Adv. Ther. 36(3), 691–707 (2019).
6.
Takeuchi T, Nakajima R, Komatsu S et al. Impact of adalimumab on work productivity and activity impairment in japanese patients with rheumatoid arthritis: large-scale, prospective, single-cohort ANOUVEAU study. Adv. Ther. 34(3), 686–702 (2017).
7.
Dejaco C, Mueller T, Zamani O et al. FRI0108 Golimumab improves work productivity and activity and quality of life in patients with rheumatoid arthritis (RA), psoriasis arthritis (PSA) and axial spondyloarthritis (AXSPA): interim results from a non-interventional study in austria (go active). Ann. Rheumatic Dis. 77(Suppl. 2), 598–599 (2018).
8.
Keystone EC, Genovese MC, Klareskog L et al. Golimumab, a human antibody to tumour necrosis factor (alpha) given by monthly subcutaneous injections, in active rheumatoid arthritis despite methotrexate therapy: the GO-FORWARD study. Ann. Rheum. Dis. 68(6), 789–796 (2009).
9.
Kavanaugh A, Mcinnes I, Mease P et al. Golimumab, a new human tumor necrosis factor alpha antibody, administered every four weeks as a subcutaneous injection in psoriatic arthritis: twenty-four-week efficacy and safety results of a randomized, placebo-controlled study. Arthritis Rheum. 60(4), 976–986 (2009).
10.
Inman RD, Davis JC Jr, Heijde D et al. Efficacy and safety of golimumab in patients with ankylosing spondylitis: results of a randomized, double-blind, placebo-controlled, Phase III trial. Arthritis Rheum. 58(11), 3402–3412 (2008).
11.
Scrivo R, Giardino AM, Salvarani C et al. An observational prospective study on predictors of clinical response at six months in patients with active psoriatic arthritis treated with golimumab. Clin. Exp. Rheumatol. 38(1), 107–114 (2020).
12.
Kruger K, Burmester GR, Wassenberg S, Bohl-Buhler M, Thomas MH. Effectiveness and safety of golimumab in patients with rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis under real-life clinical conditions: non-interventional GO-NICE study in Germany. BMJ Open 8(6), e021082 (2018).
13.
Marra CA, Woolcott JC, Kopec JA et al. A comparison of generic, indirect utility measures (the HUI2, HUI3, SF-6D, and the EQ-5D) and disease-specific instruments (the RAQoL and the HAQ) in rheumatoid arthritis. Soc. Sci. Med. 60(7), 1571–1582 (2005).
14.
Davis JC Jr, Revicki D, van der Heijde DM et al. Health-related quality of life outcomes in patients with active ankylosing spondylitis treated with adalimumab: results from a randomized controlled study. Arthritis Rheum. 57(6), 1050–1057 (2007).
15.
Hone D, Cheng A, Watson C et al. Impact of etanercept on work and activity impairment in employed moderate to severe rheumatoid arthritis patients in the United States. Arthritis Care Res. (Hoboken) 65(10), 1564–1572 (2013).
16.
Kimball AB, Yu AP, Signorovitch J et al. The effects of adalimumab treatment and psoriasis severity on self-reported work productivity and activity impairment for patients with moderate to severe psoriasis. J. Am. Acad. Dermatol. 66(2), e67–e76 (2012).
17.
Chen KC, Wu CH, Tang CH, Huang KC. Healthcare resource utilization and costs among patients with rheumatoid arthritis on biologic therapies in Taiwan: a 1-year mirror-image study using a national claims database. PLoS ONE 13(7), e0200758 (2018).
18.
Cummins E, Asseburg C, Prasad M, Buchanan J, Punekar YS. Cost–effectiveness of golimumab for the treatment of active psoriatic arthritis. Eur. J. Health Econ. 13(6), 801–809 (2012).
19.
Borse RH, Brown C, Muszbek N, Chaudhary MA, Kachroo S. Cost–effectiveness of golimumab in ankylosing spondylitis from the UK payer perspective. Rheumatol. Ther. 4(2), 427–443 (2017).
20.
Luttropp K, Dozier M, Justo N et al. Real-world treatment persistence of golimumab in the management of immune-mediated rheumatic diseases in Europe: a systematic literature review. BMJ Open 9(5), e027456 (2019).
Information & Authors
Information
Published In
Pages: 891 - 902
PubMed: 32722921
Copyright
© 2020 Merck Sharp & Dahme Corp., a subsidiary of Merck & Co., lnc.,. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 26 May 2020
Accepted: 6 July 2020
Published online: 29 July 2020
Keywords:
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Golimumab improves patient-reported outcomes in daily practice of inflammatory rheumatic diseases in Germany. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0092
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Juan Luis Sánchez Sevila, José Rosas, José María Ramada Rodilla, Mar Seguí-Crespo, Self-Perceived Difficulty in Job Performance by Working Patients with Uveitis: Global Assessment and by Subscales of Work Demands, Ocular Immunology and Inflammation, 10.1080/09273948.2024.2415539, 33, 3, (423-431), (2024).
- Murray W. Enns, Charles N. Bernstein, Lesley Graff, Lisa M. Lix, Carol A. Hitchon, John D. Fisk, Brenden Dufault, Ruth Ann Marrie, A longitudinal study of distress symptoms and work impairment in immune-mediated inflammatory diseases, Journal of Psychosomatic Research, 10.1016/j.jpsychores.2023.111473, 174, (111473), (2023).
- Panagiotis Athanassiou, Dimitrios Psaltis, Athanasios Georgiadis, Gkikas Katsifis, Athina Theodoridou, Souzana Gazi, Prodromos Sidiropoulos, Maria G. Tektonidou, Andreas Bounas, Anna Kandyli, Periklis Vounotrypidis, Grigorios T. Sakellariou, Dimitrios Vassilopoulos, Zhiping Huang, Evangelia Petrikkou, Dimitrios Boumpas, Real-world effectiveness of golimumab in adult patients with rheumatoid arthritis, psoriatic arthritis, and axial spondyloarthritis and an inadequate response to initial TNFi therapy in Greece: the GO-BEYOND prospective, observational study, Rheumatology International, 10.1007/s00296-023-05376-5, 43, 10, (1871-1883), (2023).
- Christian Dejaco, Thomas Mueller, Omid Zamani, Ulrike Kurtz, Stefan Egger, Johannes Resch-Passini, Anna Totzauer, Babak Yazdani-Biuki, Thomas Schwingenschloegl, Peter Peichl, Angelika Kraus, Gerhard W. Naerr, A Prospective Study to Evaluate the Impact of Golimumab Therapy on Work Productivity and Activity, and Quality of Life in Patients With Rheumatoid Arthritis, Psoriasis Arthritis and Axial Spondyloarthritis in a Real Life Setting in AUSTRIA. The GO-ACTIVE Study, Frontiers in Medicine, 10.3389/fmed.2022.881943, 9, (2022).
- Philipp Sewerin, Kathrin Borchert, Dominic Meise, Matthias Schneider, Jörg Mahlich, Health Resource Utilization and Associated Health Care Costs of Biologic Disease‐Modifying Antirheumatic Drugs in German Patients With Psoriatic Arthritis , Arthritis Care & Research, 10.1002/acr.24598, 74, 9, (1435-1443), (2022).
- Dimitrios Psaltis, Loukas Settas, Athanasios Georgiadis, Eftichia Koukli, Andreas Bounas, Achilleas Livieratos, Evangelia Petrikkou, Heleni Kalogiannaki, Argyro Repa, Dimitrios Vassilopoulos, Prodromos Sidiropoulos, The effects of golimumab on patient centric outcomes amongst rheumatoid arthritis patients in Greece. The GO-Q study, Rheumatology International, 10.1007/s00296-021-05073-1, 42, 4, (639-650), (2022).
- Panagiotis Athanassiou, Anastasios Kotrotsios, Ioannis Kallitsakis, Andreas Bounas, Theodoros Dimitroulas, Alexandros Garyfallos, Maria G. Tektonidou, Giorgos Vosvotekas, Achilleas Livieratos, Evangelia Petrikkou, Gkikas Katsifis, The effects of golimumab on work productivity and quality of life among work-active axial spondyloarthritis and psoriatic arthritis patients treated in the routine care in Greece: the ‘GO-UP’ study, Quality of Life Research, 10.1007/s11136-021-03044-4, 31, 5, (1385-1399), (2021).