Cost–effectiveness of second-line nivolumab for platinum-treated advanced non-small-cell lung cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To analyze the economic impact of nivolumab and chemotherapy in patients with non-small-cell lung cancer (NSCLC) who developed disease progression after platinum-containing dual-drug chemotherapy. Materials & methods: The partitioned survival model was used to analyze the cost-utility of two NSCLC treatments by nivolumab and docetaxel. The clinical data resulted from the Phase III clinical trial. The cost parameters were derived from our previous studies, and the utility parameters were derived from the literature. Results: The quality-adjusted life-years of nivolumab and docetaxel were 0.778 and 0.336. The lifetime direct medical expenses of nivolumab and docetaxel were US$44,707.17 and US$12,826.72. The incremental cost–effectiveness ratio was $72,127.71/quality-adjusted life-year. Conclusion: The combination of chemotherapy, nivolumab is not a cost-effective choice in the second-line treatment of NSCLC.
Lung cancer is the malignant tumor with the highest morbidity and mortality in the world. GLOBOCAN data [1] revealed about 2 million new cases of lung cancer worldwide in 2018, accounting for 11.6% of all new cancer cases. About 1.8 million deaths occurred in 2018, accounting for 18.4% of all tumor deaths. Given the large population base in China, the number of new cases and deaths due to lung cancer far exceeds that of other countries. According to the China National Cancer Center, the incidence and mortality rate of lung cancer in China increased from 57.26/100,000 in 2015 and 45.87/100,000 in 2011, respectively [2,3]. Most primary lung cancer is non-small cell lung cancer (NSCLC), accounting for about 80% [4]. Most patients with NSCLC are advanced at the time of diagnosis, eliminating the opportunity for surgery [5,6]. Chemotherapy and radiotherapy have become their main treatment options.
Following the targeted therapy of tumors, immunotherapy drugs have provided new treatment options for NSCLC in recent years [7]. To date, the US FDA has approved four immunosuppressive agents for NSCLC: nivolumab and pembrolizumab, which target PD-1, and atezolizumab and durvalumab, which target PD-L1. In China, only nivolumab was approved in 2018 for the treatment of EGFR gene mutation-negative and ALK-negative patients with intolerable previously advanced or metastatic NSCLC who have undergone disease progression after platinum-containing chemotherapy. Nivolumab is a fully humanized IgG4 PD-1 inhibitor antibody. Its main function is to block the interaction with PD-L1 and PD-L2, as well as the immunosuppressive response mediated by PD-1 pathway, including antitumor immune response, so as to induce antitumor effect [8]. The recommended level of nivolumab monotherapy as a second-line treatment for NSCLC is in Category 1 in NCCN guidelines [9]. CheckMate017 [10,11] and CheckMate057 [11,12] demonstrated that nivolumab significantly prolongs the overall survival (OS) of patients with advanced nonsquamous and squamous NSCLC relative to chemotherapy. CheckMate078 [13] showed that nivolumab significantly prolongs survival compared with docetaxel in previously treated Chinese patients with advanced NSCLC, and their median survival is 12 (10.4–14) and 9.6 (7.6–11.2) months, respectively. The incidence of grade 3 or grade 4 adverse events is significantly lower than that of the control group (10 vs 48%).
Although nivolumab is a new treatment that can significantly improve the survival rate of patients with advanced NSCLC, the economic burden of treatment is also an important concern of the public. At present, there is no pharmacoeconomic study on nivolumab in the treatment of Chinese patients with NSCLC. A model was built based on the recommendations of the latest clinical guidelines, and recent clinical efficacy data were used to provide strong support for clinical decision-making through cost-benefit analysis to determine the economic impact of nivolumab as second-line treatment for advanced patients with NSCLC.
Materials & methods
Research object & intervention measures
Subjects were patients with advanced or metastatic squamous and nonsquamous NSCLC, excluding EGFR mutations in nonsquamous NSCLC or known ALK translocations. Patients (18 years or older) showed disease progression during or after treatment with a platinum-containing two-drug regimen and had an Eastern Cooperative Oncology Group (ECOG) performance status score of 0 or 1. Patients were selected regardless of the tumor’s PD-L1 expression status. Baseline characteristics of patients were consistent with those in the clinical trial CheckMate078. Nivolumab (3 mg/kg) was administered once every 2 weeks, whereas docetaxel (75 mg/m2) was administered every 3 weeks. Drug administration was continued until progression or intolerable toxicity.
Model structure
A model was developed based on a ‘partitioned survival analysis’ analytical framework to compare nivolumab and docetaxel on the basis of China’s health service system. According to the current existing lung cancer-related pharmacoeconomic studies [14,15] and real-world situations, the structure of the model was divided into three different mutually exclusive health states. The model structure and transition between states are shown in Figure 1. All patients are in the initial state of progression-free survival (PFS) and their health status cannot be reversed. In the next cycle, some people will still be in PFS, and the rest will be in progressed survival (PS) depending on the transfer probability. Entering PS can only be in PS or into a state of death. Patients receive treatment until the disease progresses, and the patients enter the best support treatment after progression. The cycle time in the model was set to 21 days based on clinical research and treatment options. After 10 years of model operation, all patients were in a state of death. To fully present the lifelong benefits of the two treatment options, the study duration was set to 10 years.

Figure 1. Markov model for non-small-cell lung cancer.
A Markov model comprising three health states (progression-free survival, progressed survival and death) was built.
Clinical data
Clinical efficacy data were derived from a Phase III randomized, open-label study (CheckMate-078) [13]. The efficacy and safety of nivolumab and docetaxel in patients with stage IIIb/IV NSCLC who developed disease after platinum-based dual-agent chemotherapy were compared through a Phase III clinical study of the first PD-1 inhibitor in the field of lung cancer in China. The research was mainly conducted in China, with research centers in Hong Kong, Singapore and Russia. The study population was mainly Chinese patients (n = 451) and a small number of Russian (n = 45) and Singapore (n = 8) patients. The trial enrolled 504 patients with squamous and nonsquamous NSCLC, including patients with PD-L1 expression levels <1 and ≥1%. The graphic digitization software GetData Graph Digitizer (version 2.25) was used to read the PFS and OS curve data of the CheckMate-078 trial nivolumab group and docetaxel group, respectively, to obtain the cumulative survival probability at each time point. The survival proportions in CheckMate 078 at the end of the study are close to zero, only one person and zero people survived at 24 months in the two groups. The long-term clinical outcome survival function came from the fitting and extrapolation of the K-M curve. The goodness-of-fit was based on a visual inspection, Akaike information criterion and Bayesian information criterion [16–18]. A Weibull distribution was fitted to the pseudo-individual patient data as it provided the best fit among the gompertz, exponential, log-logistic and log-normal distribution.
Cost & utility
As this study was based on the perspective of health service system, only direct medical cost was considered. The direct medical costs in the model included drug costs, follow-up costs, costs for the treatment of severe adverse events, and costs for post-progression of the disease. The cost of disease progression was from our previously published literature [19] and the drug price was adjusted based on the price in China’s latest National Food Protection Bureau’s 4 + 7 City Drug Centralized Procurement Document [20]. This policy was a bargaining price under the group purchase model of public hospitals, and the price of medicines has dropped significantly. Other cost data were derived from published relevant literature [21].
According to the Nivolumab drug package insert and guidelines in China, the recommended dose for treating NSCLC is 3 mg/kg, delivered intravenously every 2 weeks. Although the FDA has approved a dosing regimen every 4 weeks, China has not yet approved this usage. Nivolumab (3 mg/kg) was intravenously injected every 2 weeks, and docetaxel (75 mg/m2) was given intravenously every 3 weeks. We assumed that the patient entered the model with a body surface area of 1.6 m2 and an average body weight of 60 kg. To avoid the impact of this hypothesis on the results, sensitivity analysis of body surface area and bodyweight was performed. The average exchange rate in 2018 was 6.6174 yuan to 1 dollar, and all costs were converted from RMB to USD [22].
The utility values for each state in this study were obtained from studies by Klazien [23], and the effect of two major adverse events above the third grade on utility values was considered [24]. The incidence rates of docetaxel-related neutropenia, rash, anemia were 19, 0 and 2%, respectively, and the incidence of nivolumab-related neutropenia, rash, anemia were 0.3, 1 and 0.3% [13]. Both cost and utility were discounted at a rate of 3%. The cost and utility values used in the model are shown in Table 1.
| Parameter | Value | PSA distribution | Ref. | |
|---|---|---|---|---|
| Nivolumab | Docetaxel | |||
| Log-logistic survival model | ||||
| PFS | Scale = 0.222264; shape = 1.311032; r2 = 0.9657941 | Scale = 0.184894; Shape = 1.742256; r2 = 0.9802700 | Fixed | [13] |
| OS | Scale = 0.054293; shape = 0.836117; r2 = 0.9896381 | Scale = 0.067665; shape = 0.839898; r2 = 0.9891647 | Fixed | [13] |
| Quality of life | ||||
| Utility of PFS | 0.784 (0.431–0.974) | 0.784 (0.431–0.974) | Beta | [23,24] |
| Utility of PS | 0.470 (0.184–0.773) | 0.470 (0.184–0.773) | Beta | [23] |
| Disutility of toxicities | ||||
| Diarrhea | 0.047 (0.016–0.077) | 0.047 (0.016–0.077) | Beta | [24] |
| Neutropenia | 0.09 (0.058–0.122) | 0.09 (0.058–0.122) | Beta | [24] |
| Rash | 0.032 (0.01–0.055) | 0.032 (0.01–0.055) | Beta | [24] |
| Anemia | 0.073 (0.037–0.11) | 0.073 (0.037–0.11) | Beta | [24] |
| Cost data (US$) | ||||
| Cost of drug | 2786.88 (2229.50–2786.88) per cycle | 216.25 (173.00–216.25) per 20 mg | Fixed | Local charge |
| Cost of SAEs per unit | 362 (272–453) | 362 (272–453) | Gamma | [21] |
| Cost of follow-up per cycle | 59.2 (44.4–74) | 59.2 (44.4–74) | Gamma | [21] |
| Cost of supportive care per cycle | 359 (169–845) | 359 (169–845) | Gamma | [21] |
| Cost after disease progression cycle | 866.45 (693.16–1,039.74) | 866.45 (693.16–1039.74) | Gamma | [19,20] |
OS: Overall survival; PFS: Progression-free survival; PS: Progressed survival; PSA: Probability sensitivity analysis; SAE: Serious adverse event (≥grade 3).
Basic analysis & sensitivity analysis
Basic analysis and sensitivity analysis were conducted through a model constructed by Treeage Pro 2015 software. A queue model was established to evaluate the quality-adjusted life-years (QALYs) and lifetime costs of patients with NSCLC. By calculating the incremental cost–effectiveness ratio (ICER), cost-utility analysis was carried out by comparing it with the threshold value. The threshold for patients with NSCLC in China remains undefined. According to Chinese pharmacoeconomics guidelines and WHO recommendations: ICER >three-times per capita GDP, the increased cost is not acceptable. In this study, the threshold is determined to be three-times of the national per capita GDP in 2018 [25,26]. Therefore, this study adopted the China’s 2018 triple GDP per capita of US$29,306.37 as the threshold value.
In order to test the influence of the variables on the results of cost–effectiveness analysis, one-way sensitivity analysis was carried out for all the parameters of input model. The variation range of the parameters mainly came from the relevant research results, with 95% CIs or ± 20% changes. The discount rate was between 0 and 8%. Considering that the Chinese government is pushing forward the reform in the field of drugs and promoting the reduction of drug prices, it is unlikely that drug prices will increase in the short term. Therefore, the drug prices were only set to decline by 20%.
Probability sensitivity analysis (PSA) was repeated 1000 second-order Monte Carlo simulations to calculate the ICER based on each sampling of two different treatment schemes. The utility value was set to beta distribution and the cost was set to gamma distribution. This was mainly based on the suggestions from the the ISPOR-SMDM Modeling Good Research Practices Task Force [24,27]. The prices of nivolumab and docetaxel were fixed in PSA because they are branded drugs. The two treatment schemes were calculated based on the ICER value of each sample and presented in the form of a scatter plot.
Results
Basic analysis
Table 2 shows that the lifetime cumulative cost of nivolumab was US$44,707.17 (CNY 295,845), the cumulative utility was 0.778 QALYs, and the life year was 1.417 years. The lifetime cumulative cost of docetaxel was US$12,826.72 (CNY 84,879), the cumulative utility was 0.336 QALYs, and the life year was 0.561 years. Nivolumab had an ICER of US$72,127.71/QALY (CNY 477,297/QALY) compared with docetaxel. The ICER was much larger than the threshold set in this study (US$29,306.37).
| Strategy | Costs (US$) | QALY | LY | Medican PFS months | Median OS months | ΔCosts (US$) | ΔQALY | ΔLY | ICER (US$/QALY) |
|---|---|---|---|---|---|---|---|---|---|
| Nivolumab | 44,707.17 | 0.778 | 1.417 | 3.3 | 12.0 | 31,880.45 | 0.442 | 0.856 | 72,127.71 |
| Docetaxel | 12,826.72 | 0.336 | 0.561 | 2.8 | 9.0 | NA | NA | NA | NA |
ICER: Incremental cost–effectiveness ratio; LY: Life year; OS: Overall survival; PFS: Progression-free survival; QALY: Quality adjusted life year.
Sensitivity analysis
One-way sensitivity analyses revealed that progressive quality of life, progression-free state quality of life, body weight and nivolumab’s drug cost were the main influencing factors. These parameters may cause large changes in the ICER by adjusting their values. The cost of follow-up only slightly influenced the outcome. The results are presented in a tornado diagram in Figure 2. When these parameters fluctuated within their range, nivolumab still had a cost advantage over docetaxel. Therefore, the change in parameters did not affect the conclusion of the study, that is, docetaxel was economical. The results of the scatter plot are shown in Figure 3. All scatter points of nivolumab, compared with those of docetaxel, were above the willingness-to-pay (WTP) threshold line. Thus, under the threshold, the probability of docetaxel having a cost effect was 100%. The cost–effectiveness curve of PSA is shown in Figure 4. The cost-effective acceptable curve showed that the probability that nivolumab had a cost effect increased as the social average WTP increased. When WTP was US$80,000 (CNY 52,939), the acceptable probability of nivolumab was greater than that of docetaxel, that is, the probability of nivolumab exerting a cost effect was 59.9%. As the value of WTP increased, the probability that nivolumab was economical also increased. With a WTP was US$100,000 (CNY 66,174), the probability of nivolumab being most cost-effective was 78.9%.
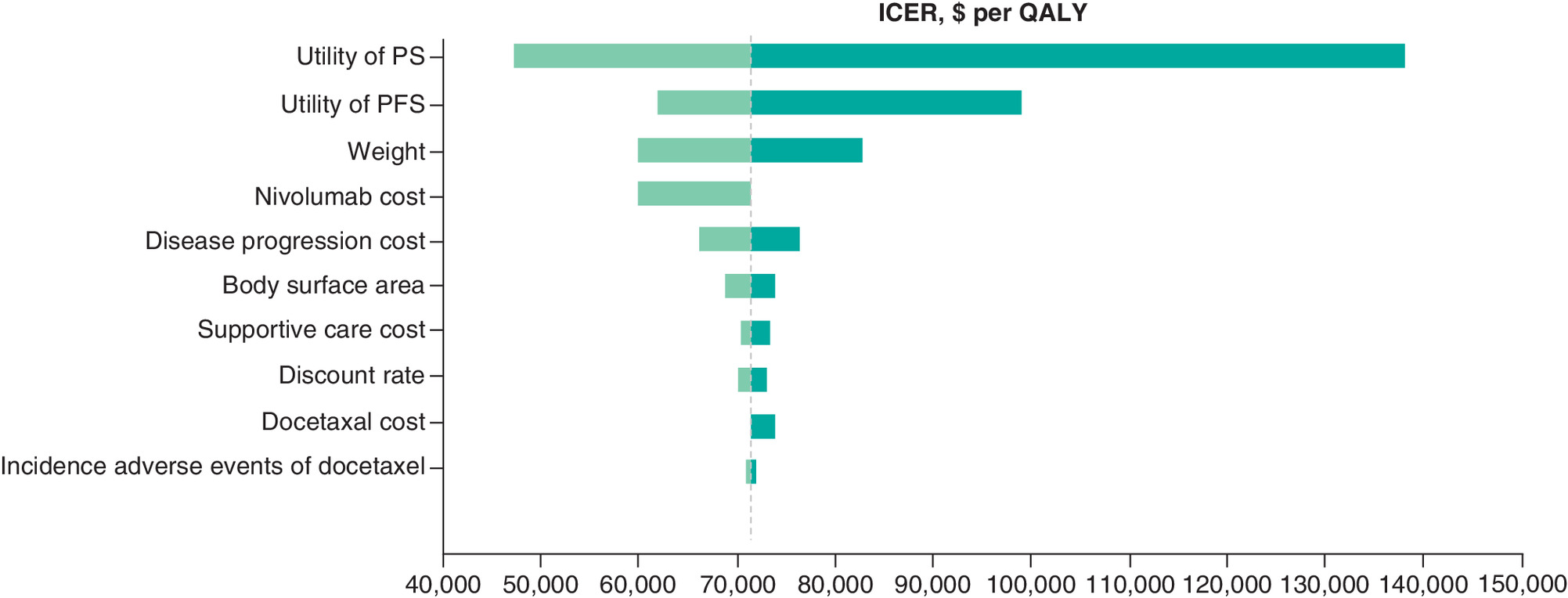
Figure 2. One-way sensitivity analysis.
Tornado diagrams show the influence of factors on the Markov model. The factors are listed in descending order of the influence on ICER with variation of factor values.
ICER: Incremental cost–effectiveness ratio; PFS: Progression-free survival; PS: Progressed survival; QALY: Quality-adjusted life years.
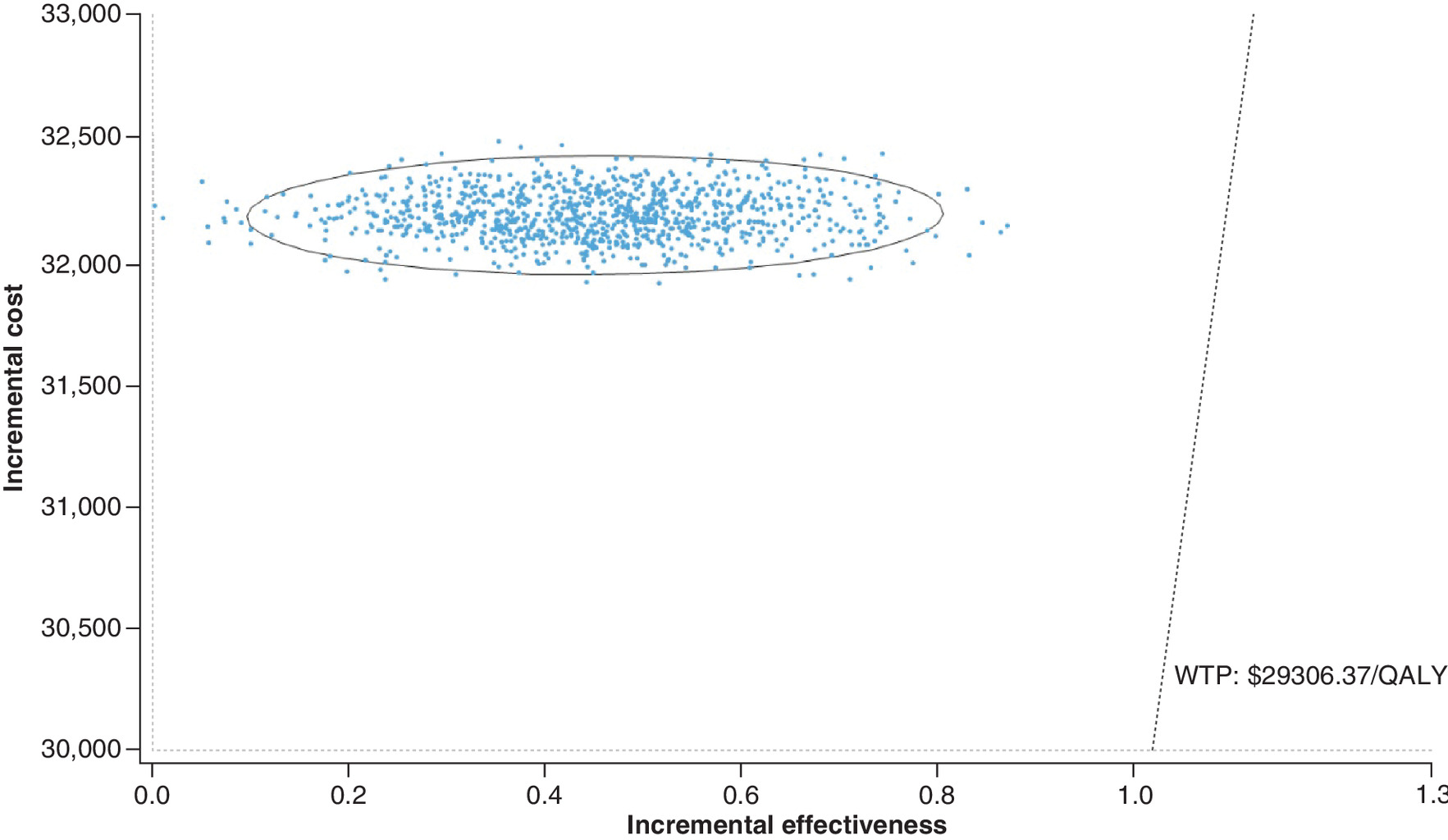
Figure 3. Probabilistic sensitivity analyses.
The dot represents the result of the Monte Carlo simulation, and the ellipse represents the 95% CI. The diagonal line represents the WTP value, and the dot falls below the diagonal line to indicate that the test group has a cost effect compared with the corresponding control group.
QALY: Quality-adjusted life years; WTP: Willingness-to-pay.
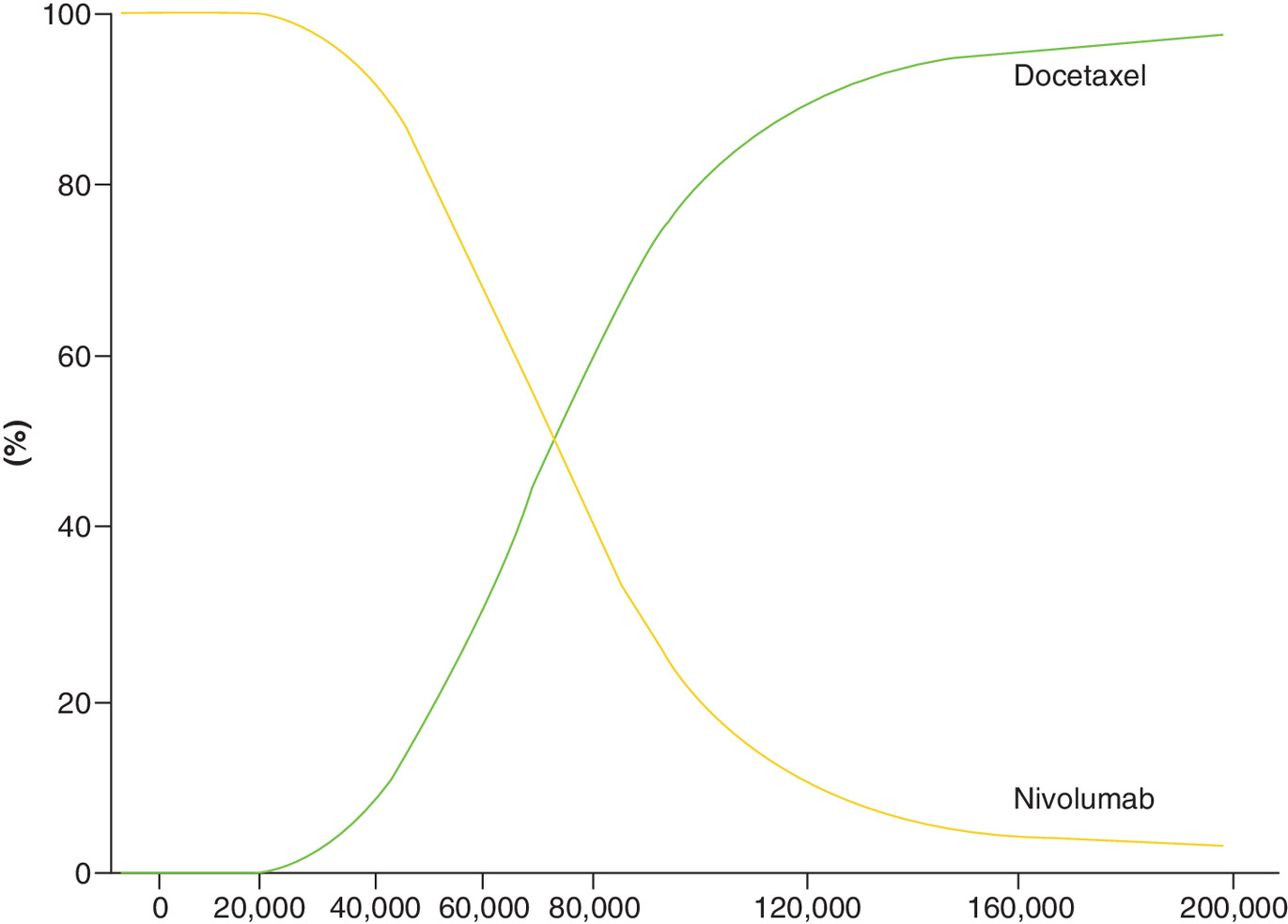
Figure 4. Cost–effectiveness acceptability curves.
The cost–effectiveness acceptability curves reflected the results of probabilistic sensitivity analysis by estimating probabilities of different treatments being considered as optimal strategies at different WTP thresholds.
WTP: Willingness-to-pay.
Discussion
The pharmacoeconomic evaluation of nivolumab in the treatment of NSCLC in China is crucial. Nivolumab was just launched in China in mid-2018. China has a large population base and a large absolute number of patients with lung cancer. After the listing of nivolumab, it will impose a heavy economic burden on patients and the medical insurance fund. Clinicians, healthcare and patients are extremely interested in the long-term economics of NSCLC. At present, there have been two economic studies on nivolumab compared with docetaxel, which are evaluated in the Switzerland and China. But these studies differ in perspective, model and data source. Matter-Walstra et al. studied the treatment of nonsquamous NSCLC in Switzerland [23]. When nivolumab has an ICER value of CHF124,891/QALY compared with docetaxel and exceeds the threshold of CHF100,000/QALY, no cost effect is observed. Although the results are consistent with our study, the medical costs and thresholds values of Switzerland and China are considerably different, which can not directly reflect the economic evaluation in China. Liu et al. established Markov model to evaluate the economics of nivolumab and docetaxel second-line treatment of NSCLC [28]. They found that nivolumab is unlikely to be cost-effective. Liu et al. and our study are both researched in China’s geo-environment, but there are differences in the research perspective, model structure and PFS curve extrapolation methods. Therefore, there are some differences in cost-utility analysis results. For the nivolumab arm, Liu et al. used hazard ratio (HR) to adjust the Weibull parameters, but we fitted and extrapolated the K-M curves of PFS and OS were based on the CheckMate 078 trial. In addition, their model assumed that the patient's starting age was 60 years old, this is inconsistent with clinical trials. Participants in the CheckMate 078 trial and our model were 18 years of age and older. Their assumption would reduce the credibility of the results. The above study assessed the cost–effectiveness of nivolumab from different aspects and provided more comprehensive evidence for decision makers.
This study found that nivolumab works better and costs more than docetaxel, and ICER was significantly above the threshold. One-way sensitivity analysis showed that the quality of life and the cost of nivolumab were the most important sensitive parameters. In order to reduce the burden of patients’ medical treatment, the Chinese medical insurance department will make dynamic adjustments to the medical insurance catalogue. Innovative targeted drugs will be negotiated nationally to determine whether they are reimbursed, and to determine payment criteria. Through equal negotiation and consultation between medical insurance and pharmaceutical enterprises, a relatively reasonable payment standard will be formulated [29]. The average decrease rate of drugs for cancer and diabetes is about 65% in 2019 Medical Insurance Catalogue [30]. In order to improve the economics of nivolumab, the national medical insurance department could reduce the price through medical insurance negotiations. Our research would improve the scientificity, standardization and effectiveness of nivolumab negotiations. Combining the level of China’s per capita gross national income, exploring the reasonable medical payment standard of nivolumab will help further improve the utilization rate and accessibility of targeted drugs, enhance the quality of life, and decrease the patients’ burden.
This study had some limitations. First, the CheckMate 078 trial was the only large-scale randomized controlled clinical trial that compared nivolumab with docetaxel in Chinese patients with NSCLC. However, our model depended on the validity and universality of the trial, and any deviations in the trial were reflected in our research. Second, the study hypothesized that patients enrolled did not require PD-L1 testing. This consideration was mainly because the PFS and OS curves reported by the CheckMate 078 study included PD-L1 negative (<1%) and PD-L1 positive (≥1%) populations. In the CheckMate 078 study, a subgroup analysis of the effects of PD-L1 expression on OS was performed (pre-set subgroup). In patients with PD-L1 expression levels <1 and ≥1%, OS HR was 0.75 (95% CI: 0.52–1.09) and 0.62 (95% CI: 0.45–0.87). The PD-L1 negative (<1%) subgroup’s OS benefit was slightly lower than that of the PD-L1 positive (≥1%) subgroup (effect value HR: 0.75 vs 0.62). Although the 95% CI upper limit of the PD-L1 negative subgroup exceeded 1, the benefit of the effector HR was significant. Compared with the control group of docetaxel monotherapy, nivolumab still improved the OS of patients with negative PD-L1 expression. Therefore, nivolumab poses varying degrees of survival benefit to patients with positive or negative PD-L1 expression, and patients with negative PD-L1 were not excluded in our model. Third, the CheckMate-078 study included some Russian and Singaporean populations, but nearly 90% of the population was Chinese. This clinical trial is believed to be a good representation of the Chinese population. Fourth, the utility values of PFS and PS status were not derived from Chinese NSCLC patients. One-way sensitivity analysis showed that the utility values of PFS and PS in both groups were the main influencing factors. The utility values of specific treatment schemes for Chinese lung cancer patients have not been retrieved from published literature, and the only measurement of the utility value of lung cancer patients in China is the patients with first-line treatment. Fifth, the use of nivolumab may change the clinical path of third-line drug treatment in patients with NSCLC, but we did not consider other individualized treatment decisions. Despite some limitations, the variables in the model did not affect the final result. Sensitivity analysis showed that probability, utility and cost data were unlikely to affect the final result.
Conclusion
Under the threshold of three-times GDP per capita in China, docetaxel is more economical than the nivolumab in the treatment regimen for patients with NSCLC and disease progression after platinum-based dual-agent chemotherapy. The Chinese government could try to reduce the price of nivolumab through medical insurance negotiations.
•
Nivolumab is not likely to be more cost-effective than chemotherapy in the second-line treatment of non-small-cell lung cancer in China.
•
The Chinese government could try to reduce the price of nivolumab through medical insurance negotiations.
Author contributions
L Zhang contributed toward methodology, software, writing-original draft preparation and writing-review and editing. X Zeng contributed toward formal analysis, visualization, project administration and formal analysis. H Cai contributed toward conceptualization, methodology and supervision. N Li contributed toward writing-original draft preparation, and writing-review and editing. M Liu contributed toward methodology, supervision, project administration, resources. L Qiu contributed toward investigation, data curation, conceptualization. B Zheng contributed toward formal analysis and visualization.
Financial & competing interests disclosure
This study was supported by Fujian Provincial Department of Science & Technology (grant no. 2017Y0035) of the People’s Republic of China and National Natural Science Foundation of China (grant no. 71804025). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 68(6), 394–424 (2018).
2.
Chen W, Zheng R, Baade PD et al. Cancer statistics in China, 2015. CA Cancer J. Clin. 66(2), 115–132 (2016).
• Provides background on the epidemiology of non-small-cell lung cancer.
3.
Zheng RS, Sun KX, Zhang SW et al. Report of cancer epidemiology in China, 2015. Zhonghua Zhong Liu Za Zhi 41(1), 19–28 (2019).
4.
Miller KD, Siegel RL, Lin CC et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 66(4), 271–289 (2016).
5.
National Cancer Institute. Cancer stat facts: lung and bronchus cancer (2020). https://seer.cancer.gov/statfacts/html/lungb.html
6.
Ting J, Tien HP, Xiang P, Sugay A, Abdel-Sattar M, Wilson L. Cost–effectiveness and value of information of erlotinib, afatinib, and cisplatin-pemetrexed for first-line treatment of advanced EGFR mutation-positive non-small-cell lung cancer in the United States. Value Health 18(6), 774–782 (2015).
7.
Xia L, Liu Y, Wang Y. PD-1/PD-L1 blockade therapy in advanced non-small-cell lung cancer: current status and future directions. Oncologist 24(Suppl. 1), S31–S41 (2019).
8.
Fessas P, Lee H, Ikemizu S, Janowitz T. A molecular and preclinical comparison of the PD-1-targeted T-cell checkpoint inhibitors nivolumab and pembrolizumab. Semin. Oncol. 44(2), 136–140 (2017).
9.
NCCN Clinical Practice Guidelines in Oncology: non-small cell lung cancer (Version 2.2019) (2019). www.nccn.org/professionals/physician_gls/ default.aspx
10.
Brahmer J, Reckamp KL, Baas P et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 373(2), 123–135 (2015).
11.
Vokes EE, Ready N, Felip E et al. Nivolumab versus docetaxel in previously treated advanced non-small-cell lung cancer (CheckMate 017 and CheckMate 057): 3-year update and outcomes in patients with liver metastases. Ann. Oncol. 29(4), 959–965 (2018).
12.
Borghaei H, Paz-Ares L, Horn L et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 373(17), 1627–1639 (2015).
13.
Wu YL, Lu S, Cheng Y et al. Nivolumab versus docetaxel in a predominantly Chinese patient population with previously treated advanced NSCLC: CheckMate 078 Randomized Phase III Clinical Trial. J. Thorac. Oncol. (2019).
•• Nivolumab versus docetaxel in a predominantly chinese patient population with previously treated advanced non-small-cell lung cancer.
14.
Aguiar PN Jr, Haaland B, Park W, San TP, Del GA, de Lima Lopes G Jr. Cost–effectiveness of osimertinib in the first-line treatment of patients with EGFR-mutated advanced non-small cell lung cancer. JAMA Oncol. 4(8), 1080–1084 (2018).
15.
Wu B, Gu X, Zhang Q, Xie F. Cost–effectiveness of osimertinib in treating newly diagnosed, advanced EGFR-mutation-positive non-small cell lung cancer. Oncologist 24(3), 349–357 (2019).
16.
Wu B, Zhang Q, Sun J. Cost–effectiveness of nivolumab plus ipilimumab as first-line therapy in advanced renal-cell carcinoma. J. Immunother. Cancer 6(1), 124 (2018).
17.
Wan X, Zhang Y, Tan C, Zeng X, Peng L. First-line nivolumab plus ipilimumab vs sunitinib for metastatic renal cell carcinoma: a cost-effectiveness analysis. JAMA Oncol. 5(4), 491–496 (2019).
18.
Chouaid C, Luciani L, LeLay K et al. Cost–effectiveness analysis of afatinib versus gefitinib for first-line treatment of advanced EGFR-mutated advanced non-small cell lung cancers. J. Thorac. Oncol. 12(10), 1496–1502 (2017).
19.
Cai HF, Wen WT, Chen S, Zheng B, Li N, Liu MB. Economic evaluation of pemetrexed versus docetaxel as second-line therapy of patients with advanced non-small cell lung cancer. Chin. J. Mod. Appl. Pharm. 34(8), 1175–1179 (2017).
20.
General Office of the State Council of the People's Republic of China. Notice on the issuance of a pilot program for the centralized procurement and use of drugs by national organizations (2019). www.gov.cn/zhengce/content/2019-01/17/content_5358604.htm
21.
Cai H, Zhang L, Li N et al. Cost–effectiveness of osimertinib as first-line treatment and sequential therapy for EGFR mutation-positive non-small cell lung cancer in China. Clin. Ther. 41(2), 280–290 (2019).
22.
National Bureau of Statistics. Statistical Bulletin of National Economic and Social Development in 2018 (2018). www.stats.gov.cn/tjsj/zxfb/201902/t20190228_1651265.html
23.
Matter-Walstra K, Schwenkglenks M, Aebi S et al. A cost–effectiveness analysis of nivolumab versus docetaxel for advanced nonsquamous NSCLC including PD-L1 testing. J. Thorac. Oncol. 11(11), 1846–1855 (2016).
•• This is the primary source for derivation of quality-adjusted life-years (QALYs) in the model.
24.
Gu X, Zhang Q, Chu YB et al. Cost–effectiveness of afatinib, gefitinib, erlotinib and pemetrexed-based chemotherapy as first-line treatments for advanced non-small cell lung cancer in China. Lung Cancer 127, 84–89 (2019).
•• This is the primary source for derivation of QALYs in the model.
25.
World Health Organization. Choosing Interventions that are Cost Effective (WHO-CHOICE), Threshold values for intervention cost–effectiveness by Region (2011). www.who.int/entity/choice/costs/CER_thresholds_regions.xls
26.
Liu G. 2015 China Guidelines for Pharmacoeconomic Evaluations and Manual. Science Press, Beijing, China, 33 p (2015).
27.
Briggs AH, Weinstein MC, Fenwick EA et al. Model parameter estimation and uncertainty analysis: a report of the ISPOR-SMDM Modeling Good Research Practices Task Force Working Group-6. Med. Decis. Making 32(5), 722–732 (2012).
28.
Liu Q, Luo X, Peng L et al. Nivolumab Versus docetaxel for previously treated advanced non-small cell lung cancer in China: a cost–effectiveness analysis. Clin. Drug Investig. 40(2), 129–137 (2020).
29.
Cai H, Zhang L, Li N, Zheng B, Liu M. Cost–effectiveness analysis on binary/triple therapy on the basis of ixazomib or bortezomib for refractory or relapsed multiple myeloma. Leuk. Lymphoma 60(12), 2951–2959 (2019).
Information & Authors
Information
Published In
Pages: 1301 - 1309
PubMed: 33325265
Copyright
© 2020 Future Medicine Ltd.
History
Received: 2 April 2020
Accepted: 22 September 2020
Published online: 16 December 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of second-line nivolumab for platinum-treated advanced non-small-cell lung cancer. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0053
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Kai Xu, Yuting Yan, Zhaoliu Cao, Jinchun Liu, Hongting Yao, Yuyang Sun, Jingyu Zhang, Hong Wu, Cost-effectiveness analysis of sacituzumab tirumotecan vs. chemotherapy for patients with EGFR-TKI–resistant, EGFR-mutated advanced non-small cell lung cancer in China, Frontiers in Public Health, 10.3389/fpubh.2026.1843636, 14, (2026).
- Shanlian Hu, Zhiliu Tang, James P. Harrison, Nadine Hertel, John R. Penrod, Jessica R. May, Ariadna Juarez-Garcia, Orban Holdgate, Economic Evaluation of Nivolumab Versus Docetaxel for the Treatment of Advanced Squamous and Non-squamous Non-small Cell Lung Cancer After Prior Chemotherapy in China, PharmacoEconomics - Open, 10.1007/s41669-022-00383-x, 7, 2, (273-284), (2023).
- Zhuo-miao Ye, Zi-Qing Tang, Zhe Xu, Qin Zhou, Huan Li, Cost-effectiveness of nivolumab plus ipilimumab as first-line treatment for American patients with unresectable malignant pleural mesothelioma, Frontiers in Public Health, 10.3389/fpubh.2022.947375, 10, (2022).