Factors influencing breast cancer awareness: a cross-sectional study in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study aimed to explore the factors that influence breast cancer awareness. Materials & methods: A community-based cross-sectional study was conducted between January and April 2019 in Changchun, Jilin Province, China. Results: A total of 274 women were recruited for this cross-sectional study. Participants had a moderate level of breast cancer awareness (median = 76.50 [68.75, 84.00]). Women in the action/maintenance stages reported higher breast cancer awareness (p = 0.044). Women's breast cancer awareness was positively associated with high health information literacy level, husbands' higher educational degrees, seeing doctors after detecting abnormal breast changes and living within a short distance from the nearest hospital. Conclusion: History of screening and higher health information literacy levels are important positive factors linked to higher breast cancer awareness.
Breast cancer is the most common cancer-related fatal disease among women in both developed and developing countries, including women under 45 years of age [1,2]. The American Cancer Society (ACS) reported that there were approximately 40,610 breast cancer deaths among American women in 2017 [3]. Breast cancer mortality is expected to be 13.4 per 100,000 in European Union countries by 2020 [4]. In addition, the Chinese Cancer Registry reported that there were approximately 71,000 women who died of breast cancer in China in 2015 [5]. The incidence of breast cancer (34.4/105) and mortality (8.5/105) was highest in northeast China [6]. As the most common fatal cancer in women, preventing and reducing breast cancer mortality is a major global health challenge.
A growing body of studies has shown that breast cancer screening (BCS) can significantly improve the prognosis and specific mortality for breast cancer, by detecting breast cancer while it is still curable [7,8]. However, numerous studies have shown that women's BCS rates are generally at low levels [9]. For example, the average BCS participation rate for women in 18 European countries was 53.4% [10]. Notably, the proportion of women in mainland China participating in BCS has been found to be 23.5–40%, or even less than 20% [11,12]. Based on this fact, a better understanding of key influencing factors related to BCS is critical to the development of targeted cancer control interventions and increasing women's screening participation rates.
The WHO states that public awareness related to screening of breast cancer should focus on attention to the signs and symptoms of cancer and participation in screening programs for asymptomatic women [13]. In addition, existing studies have reported that high levels of breast cancer awareness can significantly promote individual screening practices [14–16]. Factors that have been shown to be associated with breast cancer awareness include both individual and systemic factors, such as age, income level and health insurance coverage [17,18], as well as access to medical services, social supports (translation services), health education and national policies [18,19]. In addition, existing studies have found a significant correlation between mammogram awareness and health literacy [20]. However, research is lacking on the association between breast cancer awareness and health information literacy (HIL). Therefore, the aim of this study is to explore the potential factors related to adult women's breast cancer awareness, to comprehensively identify the relevant factors, and to provide evidence for the development of targeted interventions and breast cancer screening programs.
Materials & methods
Participants
A total of 274 women were recruited for this cross-sectional study from January to April 2019. Participants mainly came from Changchun, Jilin Province, China. All participants voluntarily completed the anonymous online survey and paper questionnaires.
Inclusion criteria were as follows: ≥18 years of age [15,21]; ability to communicate normally; undiagnosed with breast cancer; undiagnosed with serious cardiovascular disease or mental disturbance; consent to participate in this study. As the content of the questionnaire is easy to understand, there was no tendentious guidance on the filling process during the survey, so as not to affect the answers of participants. All participants were informed about the aim of this study and had the right to refuse to participate in or withdraw from the study without any consequences.
Measures
Socio-demographics
This part was self-designed and collected, including age, employment and marital status, the education level of the women and their husbands, average income as well as the time required to get to hospital, reproductive history, history of BSE training, family history of breast cancer, abnormal breast symptoms, history of breast disease diagnosis, examination time after detection of breast changes, BCS history and frequency of free screening.
Breast cancer awareness
Women with a good understanding of breast cancer have the ability and confidence to detect breast changes, and report them to healthcare personnel promptly [22]. This includes understanding that breast cancer is the most common cancer in women, knowledge of signs and symptoms of breast cancer, and knowledge of risk factors for breast cancer, primary prevention practices, effective early detection methods and their benefits [23]. The Chinese version of the Breast Cancer Awareness Measure (C-BCAM) was used to assess women's breast cancer awareness, which was based on BCAM [24]. C-BCAM contains three domains with a total of 26 items, including the ‘knowledge of symptoms domain, barriers to seeking medical help domain and knowledge of risk factors‘ domain [25]. C-BCAM has been successfully applied to Chinese women and has shown satisfactory validity and reliability. Results have shown that it has excellent internal consistency (Cronbach's α = 0.90), with alpha coefficients of 0.88, 0.84 and 0.94 in the three domains, respectively. Total scores range from 15 to 108 and a higher score indicates higher breast cancer awareness. In this study, the C-BCAM had good internal consistency (Cronbach's α = 0.91).
Health information literacy
HIL, proposed by the Medical Library Association (MLA), refers to the ability of people in a society to access, understand and evaluate health information and services, and make decisions accordingly [26]. The Health Information Literacy Self-rating Scale (HILSS) developed by Wang [27] was used to evaluate individual HIL. This scale is divided into two parts; the first part includes five domains, including the Health information cognition (HIC) domain; Health information acquisition (HIS) domain; Health information evaluation (HIE) domain; Health information application (HIA) domain; and the Health information morality (HIM) domain; the second part includes a subscale for descriptive comparisons. This subscale contains six items to assess participants' trust in different access to health information. HILSS was demonstrated to be a reliable instrument, with the Cronbach's α higher than 0.75 for all five domains. Total scores range from 22 to 149 and a higher score indicates higher HIL. In this study, the HILSS had satisfactory internal consistency (Cronbach's α = 0.84).
The transtheoretical model
Participants' behavior stages were rated through the transtheoretical model (TTM), which included one item with six options relating to different behavior stages [28]. TTM includes the pre-contemplation stage, relapse stage, contemplation stage, relapse risk stage, action stage and maintenance stage [29,30]. A previous study indicated that women had higher motivation and perceived benefits during the action and maintenance stages of BCS [31]. Therefore, the current study divided the six stages into two phases (pre-contemplation/relapse/contemplation/relapse risk stages versus action/maintenance stages) and analyzed the breast cancer awareness differences between individuals in different phases of behavioral change.
Statistical analysis
Data were analyzed using SPSS, version 25.0. Socio-demographic characteristics were evaluated using a descriptive statistical method. Categorical variables were counted using frequency and percentages; because the continuous variables (the total scores of breast cancer awareness) showed skewed distribution, the median (M) and interquartile range (IQR) were used. In this study, HIL was designed as an independent variable, and breast cancer awareness was the dependent variable. First, the Kruskal–Wallis test and Mann–Whitney test were conducted to examine the relationship between the independent variables and breast cancer awareness, and the Dunn-Bonferroni test for post hoc comparison. The Spearman correlation coefficient method was used to analyze the correlation between breast cancer awareness and associated factors. Multiple regression analysis was used to explore the correlation between socio-demographic characteristics and breast cancer awareness. A p-value of less than 0.05 was considered statistically significant.
Ethics approval
The present study was approved by the Institute Review Board of the University (access number: 2019010701). All participants read and filled out informed consent forms before completing the questionnaires and agreed that their data could be analyzed in this survey.
Results
Characteristics of the participants
Results are presented in Table 1. In this study, a total of 275 women were recruited and 274 valid questionnaires were collected, with a 99.6% response rate. The age of participants varied from 18 to 67 years, with an average age of 32.3 years (SD = 10.5). In general, the majority of women had a spouse (51.1%), had a Specialty/Bachelor degree (55.8%), had no family history of breast cancer (97.4%), had not abnormal breast symptoms (70.1%) or a history of breast disease diagnosis (71.5%) and had not been screened in the past 2 years (52.9%). Only 27.4% of participants were categorized in the action/maintenance stages of TTM.
| Characteristics | N | % | BCAM score Median (P25, P75) | X2/Z | p-value |
|---|---|---|---|---|---|
| Age, years§ | |||||
| – ≤39 years | 195 | 71.2 | 77.00 (68.00, 87.00) | 4.380 | 0.112 |
| – 40–45 years | 42 | 15.3 | 74.50 (69.75, 82.00) | ||
| – ≥46 years | 37 | 13.5 | 72.00 (67.00, 79.00) | ||
| Employment status§ – Employed – Unemployed – Students | 133 59 82 | 48.6 21.5 29.9 | 77.00 (70.00, 84.00) 72.00 (66.00, 80.00) 79.00 (68.00, 89.00) | 10.256 | 0.006 † |
| Marital status¶ | |||||
| – Without spouse | 140 | 51.1 | 78.00 (68.00, 87.00) | -1.961 | 0.050 |
| – With spouse | 134 | 48.9 | 75.00 (69.00, 81.00) | ||
| Education level§ | |||||
| – Junior school or below | 44 | 16.1 | 71.00 (66.00, 76.75) | 24.393 | 0.000† |
| – High school/specialized secondary school | 18 | 6.6 | 72.00 (63.00, 80.00) | ||
| – Specialty/bachelor | 153 | 55.8 | 76.00 (69.00, 83.00) | ||
| – Postgraduate or above | 59 | 21.5 | 80.00 (76.50, 87.00) | ||
| Husband's education level§ | |||||
| – Junior school or below | 38 | 28.4 | 70.00 (66.00, 74.00) | 27.532 | 0.000† |
| – High school/specialized secondary school | 20 | 14.9 | 76.00 (63.50, 79.50) | ||
| – Specialty/bachelor | 60 | 44.8 | 79.00 (71.00, 85.00) | ||
| – Postgraduate or above | 16 | 11.9 | 79.50 (70.25, 83.00) | ||
| Average income (monthly), Yuan§ | |||||
| – <2000 | 60 | 21.9 | 71.00 (63.00, 81.00) | 10.656 | 0.014‡ |
| – 2000–4000 | 102 | 37.2 | 76.00 (67.75, 84.25) | ||
| – 4001–6000 | 51 | 18.6 | 78.00 (69.00, 82.00) | ||
| – >6000 | 61 | 22.3 | 79.00 (73.00, 87.50) | ||
| Time required to get to the hospitals¶ | |||||
| – ≤1 h | 239 | 87.2 | 77.00 (70.00, 84.00) | -2.673 | 0.008† |
| – >1 h | 35 | 12.8 | 70.00 (64.00, 78.00) | ||
| Reproductive history¶ – Yes – No History of BSE training¶ –Yes – No Family breast cancer history¶ – Yes – No Abnormal breast symptoms¶ – Yes – No History of breast disease diagnosis¶ – Yes – No | 129 145 80 194 7 267 82 192 78 196 | 47.1 52.9 29.2 70.8 2.6 97.4 29.9 70.1 28.5 71.5 | 74.00 (68.50, 81.00) 78.00 (68.50, 87.50) 82.50 (76.25, 89.75) 74.00 (67.00, 81.00) 71.00 (50.00, 91.00) 77.00 (69.00, 83.00) 78.00 (70.00, 84.00) 76.00 (68.00, 83.00) 76.00 (70.00, 83.00) 77.00 (68.00, 84.00) | -2.579 -4.981 -0.447 -0.879 -0.374 | 0.010† 0.000† 0.655 0.380 0.708 |
| Examination time after detection of breast changes§ | |||||
| – Immediately | 186 | 67.9 | 77.00 (69.00, 84.00) | 6.127 | 0.047‡ |
| – Check in a few days later | 57 | 20.8 | 77.00 (69.50, 85.00) | ||
| – Do not go to check Breast cancer screening history¶ – Have been screened in the past 2 years – Never had a screening | 31 129 145 | 11.3 47.1 52.9 | 70.00 (62.00, 78.00) 78.00 (71.00, 84.00) 76.00 (67.00, 83.00) | -1.619 | 0.105 |
| Screening frequency (if free)§ | |||||
| – Once a year | 255 | 93.1 | 77.00 (69.00, 84.00) | 13.101 | 0.001† |
| – Every 2 years or more | 13 | 4.7 | 83.00 (67.00, 89.5.00) | ||
| – Do not go to check | 6 | 2.2 | 51.50 (36.75, 63.00) | ||
| TTM¶ – Pre-contemplation/relapse/contemplation/ – Relapse risk stages – Action/maintenance stages C-BCAM total¶ – Screening group – Nonscreening group Domain 1¶ – Screening group – Nonscreening group Domain 2¶ – Screening group – Nonscreening group Domain 3¶ – Screening group – Nonscreening group HILSS total¶ – Screening group – Nonscreening group HIC¶ – Screening group – Nonscreening group HIS¶ – Screening group – Nonscreening group HIE¶ – Screening group – Nonscreening group HIA¶ – Screening group – Nonscreening group HIM¶ – Screening group – Nonscreening group | 199 75 129 145 129 145 129 145 129 145 129 145 129 145 129 145 129 145 129 145 129 145 | 72.6 27.4 47.1 52.9 47.1 52.9 47.1 52.9 47.1 52.9 47.1 52.9 47.1 52.9 47.1 52.9 47.1 52.9 47.1 52.9 47.1 52.9 | 75.00 (67.00, 83.00) 79.00 (73.00, 84.00) 76.5 (68.75, 84.00) 78.00 (71.00, 84.00) 76.00 (67.00, 83.00) 13.00 (10.00, 15.00) 12.00 (10.00, 15.00) 13.00 (10.00, 15.00) 15.00 (13.00, 17.00) 15.00 (13.00, 17.00) 14.00 (12.00, 17.00) 50.00 (45.00, 57.00) 51.00 (46.00, 57.00) 49.00 (45.00, 57.00) 80.00 (73.00, 86.25) 79.00 (73.00, 86.00) 81.00 (73.00, 87.00) 15.00 (14.00, 17.00) 16.00 (14.00, 17.00) 15.00 (14.00, 16.00) 26.00 (21.75, 29.00) 25.00 (21.00, 28.00) 26.00 (22.00, 29.00) 16.00 (14.00, 17.00) 16.00 (14.00, 17.00) 16.00 (14.00, 16.00) 10.00 (9.00, 11.00) 10.00 (10.00, 11.00) 10.00 (9.00, 11.00) 14.00 (12.00, 14.00) 14.00 (12.00, 14.00) 14.00 (12.00, 14.00) | -2.017 -1.619 -0.316 -2.165 -1.314 -0.309 -1.096 -1.359 -0.983 -2.174 -0.396 | 0.044‡ 0.105 0.752 0.030‡ 0.189 0.757 0.273 0.174 0.326 0.030‡ 0.692 |
†
p < 0.01.
‡
p < 0.05.
§
Kruskal–Wallis test.
¶
Mann–Whitney test.
BMI: Body mass index; C-BCAM: Chinese version of Breast Cancer Awareness Measure; Domain 1: Knowledge of symptoms; Domain 2: Barriers to seeking medical helps; Domain 3: Knowledge of risk factors; HIA: Health information application; HIC: Health information cognition; HIE: Health information evaluation; HILSS: Health information literacy self-rating scale; HIM: Health information morality; HIS: Health information acquisition; M: Median; N: Number; SE: Breast self-exam; TTM: Trans-theoretical model.
Participants' level of breast cancer awareness & its comparisons between the screening group & nonscreening group
Results are presented in Table 1. The median breast cancer awareness score was 76.5 (68.75, 84.00). Median scores of the three domains were 13.00 (10.00, 15.00), 15.00 (13.00, 17.00), and 50.00 (45.00, 57.00), respectively. Only in the ‘barriers to seeking medical helps' domain, was there a statistically significant difference in breast cancer awareness scores between the screening group and nonscreening group (p = 0.03).
Differences in participants’ breast cancer awareness by socio-demographic characteristics
Results are shown in Table 1. Employment and marital status, education level of women and their husbands, income levels, the time needed to get to the nearest hospitals, history of reproductive and BSE training, time to get a checkup after detecting abnormal breast changes and frequency of free screening could significantly affect women's breast cancer awareness. Post hoc tests suggested that employed women or students had higher breast cancer awareness scores than unemployed women (p = 0.030; p = 0.006, respectively). Women with Specialty/Bachelor degrees scored higher than women with Junior school or lower degree (p = 0.014). Women with postgraduate or higher degrees scored higher than women with lower degrees (p < 0.05). Compared with women whose husbands had Junior school or lower degrees, women whose husbands had Specialty/Bachelor or Postgraduate or higher degrees scored higher (p = 0.000; p = 0.004, respectively). Women with a monthly income above 6000 Yuan had higher scores than those earning below 2000 Yuan (p = 0.007). If screening was free, women who had an annual screening, or once every 2 years or more, had higher breast cancer awareness than women who did not go to screening (p = 0.001; p = 0.003, respectively). In addition, women in the action/maintenance stages had higher levels of breast cancer awareness (p = 0.044).
Relationship between breast cancer awareness & explanatory factors
Results are presented in Supplementary Table 1. The ‘husband with specialty/bachelor degree and high school/specialized degrees' and 'see doctors when detecting abnormal breast changes (immediately and several days later)' were the predictors for high breast cancer awareness (β = 0.282 ∼ 0.522; p < 0.05); however, 'time required to go to the nearest hospital more than one hour' was a predictor for low breast cancer awareness (β = -0.164; p < 0.05). The results indicate that these four predictors accounted for 31.3% variation in breast cancer awareness.
Participants' level of HIL
Results are shown in Table 1. The median HIL total score was 80.00 (73.00, 86.25). Median scores of the five domains were 15.00 (14.00, 17.00), 26.00 (21.75, 29.00), 16.00 (14.00, 17.00), 10.00 (9.00, 11.00) and 14.00 (12.00, 14.00), respectively. Only in the HIA domain was there a statistically significant difference in the scores reported by the screening group and nonscreening group (p = 0.03).
Correlations between C-BCAM & HILSS
Results are provided in Supplementary Table 2. Spearman's correlation analysis showed that C-BCAM and its domains were positively correlated with HILSS (r = 0.120–0.393; p < 0.01). All three domains of C-BCAM were significantly correlated with HILSS (0.141 < r <0.319; p < 0.05). Except for HIS domain, the other four domains were significant associated with C-BCAM (0.191< r <0.393; p < 0.01).
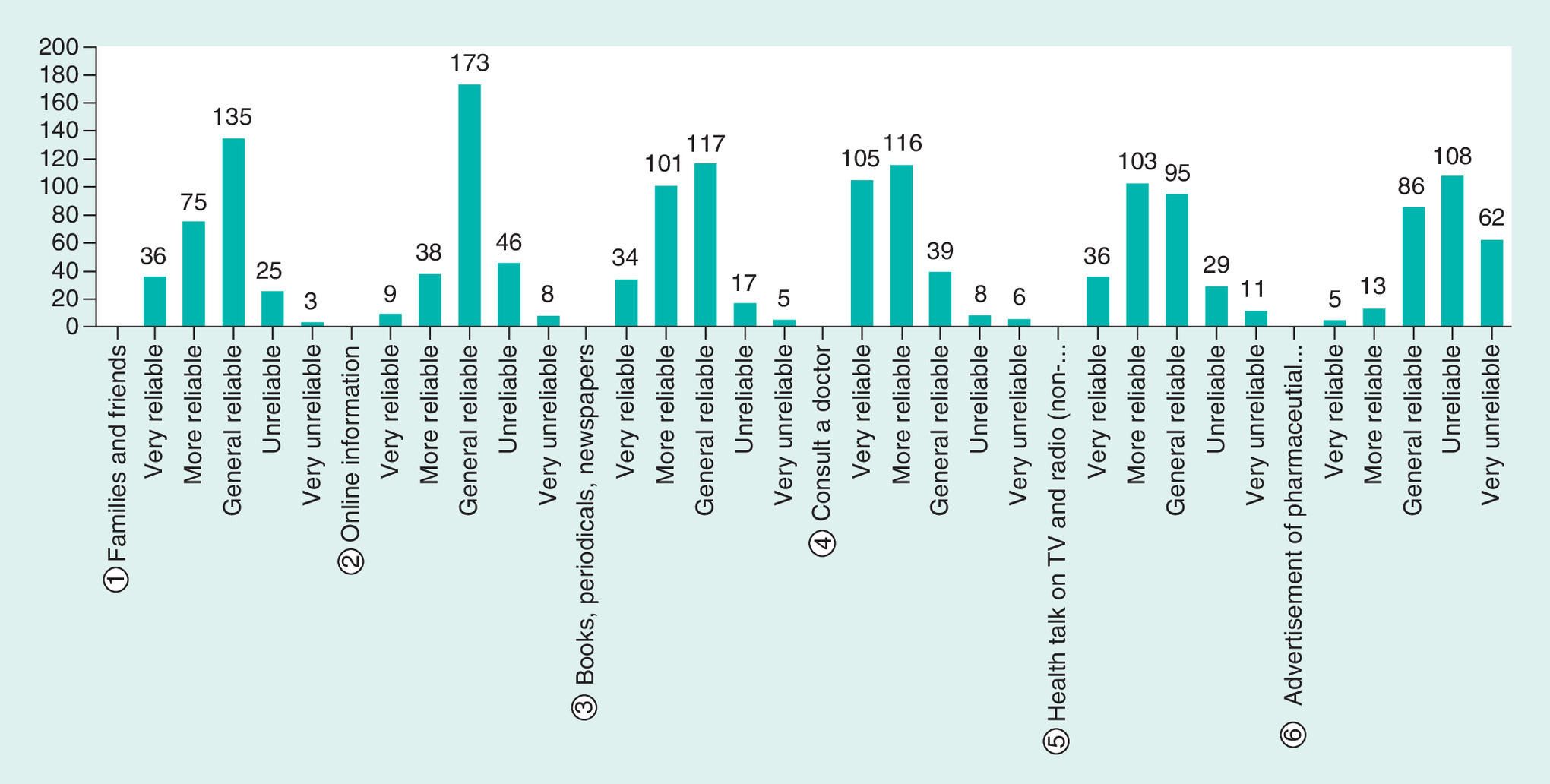
Reliability evaluation of different health information acquisition methods
Results are provided in Figure 1. There are six main methods for individuals to obtain health information, including families and friends, online information, books, periodicals and newspapers, doctors, health talks on TV and radio and advertisements for pharmaceutical promotions. Approximately half of the participants assessed health information from families, friends, and networks as ‘general reliable’ (49.3 and 63.1%, respectively). More than 90% of women trust the health information they learn from books, newspapers and doctors, rating these information sources as reliable to ‘very reliable’. And 85.4% of women believed that health talks on TV and radio were reliable to ‘very reliable’. However, 61.7% of the participants did not believe the information in the advertisements of medical promotion.
Discussion
Breast cancer awareness is a prerequisite for women to make health decisions, as well as a key factor influencing their screening decisions and behaviors. This cross-sectional study revealed that Chinese adult women's breast cancer awareness was at a moderate level (76.5 [68.75, 84.00]), which was consistent with the results of previous studies showing that women in Jilin province had insufficient breast cancer awareness [32]. It also showed that good breast cancer awareness was positively associated with being in the action/maintenance screening stages, having better socio-demographic characteristics and higher HIL levels.
To clarify the influential factors of breast cancer awareness, we explored it in different stages based on TTM. TTM divides the process of health behavior change into five different stages. In the early phase of change, cognition and experience are important, and in the later phase of change, the behavioral process is even more important [33]. Similarly, the current results show that women in the action/maintenance stages receive higher breast cancer awareness scores (p = 0.044), along with women with a history of screening (78.00 vs 76.00; p = 0.105), consistent with previous studies [31,34]. A reasonable reason for the difference may be the interaction between breast cancer awareness and screening. Higher screening awareness is associated with screening practices [16,35], which in turn promote an individual's breast cancer awareness, and the results of this study can also provide evidence for this conclusion. Specifically, women with higher health awareness may pay more attention to preventing disease and maintaining their health, and are more likely to make wise decisions on their health in their daily lives [34,36], and prefer to take active actions to improve health [36], such as BCS. They may be more inclined to ignore some nonobjective factors that prevent them from seeking medical help, such as embarrassment and physician gender preference [37]. As in this study, women in the screening group (that is, women at the action/maintenance stages), had significantly fewer perceived screening barriers than women at other stages (p < 0.05), consistent with previous studies [38,39]. Therefore, history of screening is also a factor that can affect breast cancer awareness; while evaluating women's breast cancer awareness, the stage of their screening behavior should also be measured to identify targeted interventions for them at different behavior stages.
Investigating factors affecting breast cancer awareness and screening behaviors can be a precursor to developing effective national interventions [40]. In addition to screening history, socio-demographic characteristics are also important factors affecting individual screening awareness [41]. Consistent with previous research [42], socioeconomic factors, such as education level, occupation and average income can influence women's awareness of risk factors and early detection (p < 0.05). Of course, there are also a couple of factors, such as their being at high risk for breast cancer and seeking medical help could also have an effect on their awareness. Reproductive history, lifestyle and environmental factors are high risk factors for breast cancer [43,44]. Women with these risk factors, such as no reproductive history, no BSE training and the selection of inappropriate screening intervals, reported lower breast cancer awareness scores (p < 0.05). Therefore, it is reasonable to believe that women who have fewer risk factors for breast cancer, or who know enough about breast cancer, have higher breast cancer awareness. In addition, the availability of the necessary health services is another factor that can affect women's breast cancer awareness. In our study, proximity to health services and timely visits to doctors after finding abnormal breast changes were found to be positive predictors for high breast cancer awareness (p < 0.05). The above results reconfirmed that high action prevention was influential for high breast awareness [45]. Therefore, adjusting the adjustable risk factors and avoiding delay of medical treatment to improve women's awareness of breast cancer, is an important prerequisite for the effective prevention of breast cancer [44].
To further demonstrate the influential factors of breast cancer awareness, we explored HIL. HIL is the ability level and a core element of health literacy, as well as the combination of concepts of health literacy and information literacy, with more emphasis on the utilization ability of health information [46]. High HIL is related to access to and utilization of more health information, which in turn helps to promote and maintain individual health [47]. The more health information women acquire, the better they fully understand disease-related knowledge and conduct healthy behaviors to maintain and promote health, such as BCS [48]. This study suggested that HIL can comprehensively improve women's knowledge of symptoms and risk factors of breast cancer, and reduce the barriers to seeking medical help (p < 0.01). Although the correlation between C-BCAM and the HIS domain was not statistically significant, there was a significant correlation between the domains of ‘knowledge of symptoms’ and 'barriers to seeking medical help’ and HIS domain (r = 0.214–0.279; p < 0.01). This indicates that women's HIL level can affect their understanding of breast cancer symptoms and the perceived barriers to seeking medical help. A possible explanation for the non-statistical correlation between C-BCAM and HIS was that due to the increasing complexity of health service systems, individuals need sufficient ability to search, evaluate and apply medical information in the face of diverse sources of information [47]. Limited HIL can hinder women's cognition, access and utilization of breast health information from multiple information sources. This leads to insufficient understanding of the perceived benefits of screening and disease risk of breast cancer, which is a potential barrier to screening [49]. Meanwhile, women with a screening history in the past 2 years had higher scores in the HIA domain (p = 0.03). In other words, these women are more likely to apply health information to maintaining and promoting their health. It can be seen that the occurrence of health behaviors not only depends on the individuals' access to health information, but also depends on whether they apply the acquired knowledge to the health decision-making process. Therefore, HIL may be a useful focus for developing interventions that raise breast cancer awareness and ultimately reduce the burden of breast cancer.
Given the moderate level of breast cancer awareness, it is critical work to improve this. Healthcare professionals can develop care and improvement measures to reduce negative factors affecting adult women's breast cancer awareness and to raise HIL levels for all women, further raising their awareness level. Through a comprehensive understanding of breast cancer and the necessity of screening, women who have a high level of breast cancer awareness can become more active in BCS. Many guidelines suggest that young women do not need to attend regular screening; however, breast cancer in young women is also a critical leading cause of cancer-related death [2]. The percentage of young women with risk factors for breast cancer was found to be alarmingly high, and tumors in younger women with breast cancer behave more aggressively in most cases than in older women [2,50]. Therefore, awareness of breast cancer in this group is also worthy of attention, especially in high-risk groups. Also, future studies should more specifically assess breast cancer awareness levels, such as setting a reasonable and scientific cut-off value of awareness level to analyze the correlation between different levels of awareness, HIL and different stages of behavior change in more detail to analyze the influencing factors. Healthcare providers can use the results of the study to analyze representative promoters and resolvable screening barriers to provide women with lower screening awareness with more accessible health services and targeted interventions to develop better healthcare policies and systems to enhance women's breast cancer awareness.
The current study has several limitations. First, this study was a cross-sectional study and cannot establish causal relationship inference between breast cancer awareness and the associated factors. Further research should explore the correlation in future prospective studies. Second, the sample population of this study is mainly from an area with the highest incidence and mortality of breast cancer, but due to the limited sample size, the results may not be applicable to the wider population in China. Therefore, caution should be applied when generalizing the results.
Conclusion
This study showed that Chinese women's socio-demographic characteristics and HIL are both related to their breast cancer awareness. Consideration should be given to improve controllable factors that affect women's breast cancer awareness and to strengthen healthcare services for adult women to help them obtain and utilize more health information to achieve the ultimate goal of increasing breast cancer awareness and screening compliance. Greater efforts may be needed to develop targeted interventions to strengthen women's HIL and improve their modifiable risk and protective factors to provide better breast cancer prevention services for Chinese women.
•
Breast cancer is the most common cancer among women worldwide.
•
Diagnosis of advanced breast cancer brings high physical, mental and economic burden to patients, severely affecting their quality of life.
•
Breast cancer screening is an important means to improve prognosis and reduce the specific mortality of breast cancer.
•
Women's breast cancer awareness level is a key factor that influences and predicts the occurrence of women's screening behavior.
•
Breast cancer awareness refers to women's full understanding of breast cancer, the ability to detect abnormalities in time, and explain to medical staff.
•
A community-based cross-sectional study was conducted in China from January to April 2019.
•
Women's breast cancer awareness in Jilin Province of China was found to be at a moderate level.
•
Women who had a history of breast cancer screening and were in the action/maintain behavioral stages of screening had higher levels of breast cancer awareness.
•
Higher health information literacy was significantly associated with women's breast cancer awareness.
•
A highly educated husband, seeing doctors after detecting abnormal breast changes and proximity to the nearest hospitals were positive predictors of high breast cancer awareness.
Author contributions
N Liu, XM Zhang and W Zhang contributed to the conception and design of this study; N Liu and P Li drafted the manuscript; L YU and S Yang were involved in the acquisition and analysis the data; J Wang, PP Guo, and XH Zhang critically reviewed the manuscript and supervised the whole study process. All authors read and approved the final manuscript.
Acknowledgments
Thanks to the students who took time to become involved in the investigation.
Financial & competing interests disclosure
This work was supported by a grant from the China Postdoctoral Science Foundation (2019T120242). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. Individual, de-identified participant data that underlie the results reported in this article (text, tables, figures and appendices) are available from the corresponding author following publication, including the clinical study report and study protocol.
Supplementary Material
File (suppl_file.docx)
- Download
- 19.60 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Ayran G, Firat M, Kucukakca G, Cuneydioglu B, Tahta K, Avci E. The effect of peer education upon breast self-examination behaviors and self-esteem among university students. Eur. J. Breast Health 13(3), 138–144 (2017).
2.
Anastasiadi Z, Lianos GD, Ignatiadou E, Harissis HV, Mitsis M. Breast cancer in young women: an overview. Updates Surg. 69(3), 313–317 (2017).
• Highlights the serious adverse effects of breast cancer in young women.
3.
Desantis CE, Ma J, Goding Sauer A, Newman LA, Jemal A. Breast cancer statistics, 2017, racial disparity in mortality by state. CA Cancer J. Clin. 67(6), 439–448 (2017).
4.
Carioli G, Malvezzi M, Rodriguez T, Bertuccio P, Negri E, La Vecchia C. Trends and predictions to 2020 in breast cancer mortality in Europe. Breast 36, 89–95 (2017).
5.
Sun K, Zheng R, Zhang S et al. Report of cancer incidence and mortality in different areas of China, 2015. China Cancer 28(1), 1–11 (2019).
6.
Chen W, Sun K, Zheng R et al. Cancer incidence and mortality in China, 2014. Chinese J. Cancer Res. 30(1), 1–12 (2018).
• Shows evidence on the incidence and mortality of breast cancer in China.
7.
Niell BL, Freer PE, Weinfurtner RJ, Arleo EK, Drukteinis JS. Screening for breast cancer. Radiol. Clin. North Am. 55(6), 1145–1162 (2017).
8.
Coleman C. Early Detection and screening for breast cancer. Semin. Oncol. Nurs. 33(2), 141–155 (2017).
9.
Uchida K, Ohashi H, Kinoshita S et al. Breast cancer screening and the changing population pyramid of Japan. Breast Cancer 22(2), 172–176 (2015).
10.
Giordano L, Von Karsa L, Tomatis M et al. Mammographic screening programmes in Europe: organization, coverage and participation. J. Med. Screen. 19(Suppl. 1), 72–82 (2012).
11.
Bao Y, Kwok C, Lee CF. Breast cancer screening behaviors among Chinese women in Mainland China. Nurs. Health Sci. 20(4), 445–451 (2018).
12.
Chen Z-C, Zhang Q-J, Wang Q-Y, Feng X-L. Coverage and associated factors of cervical and breast cancer screening among childbearing women in Jilin province. Chinese J. Public Health 33(08), 1170–1173 (2017).
13.
WHO. Guide to Cancer Early Diagnosis (2017). www.who.int/cancer/publications/cancer_early_diagnosis/en/
14.
Gu C, Chan CW, Twinn S, Choi KC. The influence of knowledge and perception of the risk of cervical cancer on screening behavior in mainland Chinese women. Psychooncology 21(12), 1299–1308 (2012).
15.
Roh S, Burnette CE, Lee YS, Jun JS, Lee HY, Lee KH. Breast cancer literacy and health beliefs related to breast cancer screening among American Indian women. Soc. Work Health Care 57(7), 465–482 (2018).
16.
Al-Zalabani AH, Alharbi KD, Fallatah NI, Alqabshawi RI, Al-Zalabani AA, Alghamdi SM. Breast cancer knowledge and screening practice and barriers among women in Madinah, Saudi Arabia. J. Cancer Educ. 33(1), 201–207 (2018).
17.
Islam RM, Bell RJ, Billah B, Hossain MB, Davis SR. Awareness of breast cancer and barriers to breast screening uptake in Bangladesh: a population based survey. Maturitas 84, 68–74 (2016).
18.
Adunlin G, Cyrus JW, Asare M, Sabik LM. Barriers and facilitators to breast and cervical cancer screening among immigrants in the United States. J. Immigr. Minor. Health 21(3), 606–658 (2019).
19.
Sun W, Chen D, Zhang Y, Liu J, Chen D, Zhang W. Research progress on breast cancer screening awareness, behavior status and influencing factors. Maternal Child Health Care China 33(20), 4798–4801 (2018).
20.
Yılmazel G. Health Literacy, Mammogram awareness and screening among tertiary hospital women patients. J. Cancer Educ. 33(1), 89–94 (2018).
21.
Wachira J, Busakhala A, Chite F et al. Refining a questionnaire to assess breast cancer knowledge and barriers to screening in Kenya: psychometric assessment of the BCAM. BMC Health Serv. Res. 17(1), 110 (2017).
22.
O'mahony M, Comber H, Fitzgerald T et al. Interventions for raising breast cancer awareness in women. Cochrane Database Syst Rev 2, Cd011396 (2017).
23.
Yeung MPS, Chan EYY, Wong SYS, Yip BHK, Cheung PS. Hong Kong female's breast cancer awareness measure: cross-sectional survey. World J. Clin. Oncol. 10(2), 98–109 (2019).
24.
Linsell L, Forbes LJ, Burgess C, Kapari M, Thurnham A, Ramirez AJ. Validation of a measurement tool to assess awareness of breast cancer. Eur. J. Cancer 46(8), 1374–1381 (2010).
•• Describes the Breast Cancer Awareness Measure (BCAM), and provides an opportunity to use this assessment instrument and conduct future relevant studies.
25.
Liu N, Li P, Wang J et al. Psychometric properties of the Breast Cancer Awareness Measurement among Chinese women: a cross-sectional study. BMJ Open 10(3), e035911 (2020).
•• Describes the Chinese version of Breast Cancer Awareness Measure (C-BCAM), and provides a reliable assessment tool for Chinese women.
26.
Yuan XL, Fan YY. New research area of information literacy: research and practice of health literacy. J. Med. Informatics (Chinese) 33(6), 2–6 (2012).
27.
Wang F-Z, Luo A-J, Xie W-Z, Hu D-H. Development of health information literacy self-rating scale and its reliability and validity test. China J. Modern Med. 23(30), 89–93 (2013).
•• Describes the health information literacy self-rating scale (HILSS), and provides an opportunity to use this assessment instrument and conduct future relevant studies.
28.
Spencer L, Pagell F, Adams T. Applying the transtheoretical model to cancer screening behavior. Am. J. Health Behav. 29(1), 36–56 (2005).
29.
Rakowski W, Ehrich B, Dubé CE et al. Screening mammography and constructs from the transtheoretical model: associations using two definitions of the stages-of-adoption. Ann. Behav. Med. 18(2), 91–100 (1996).
30.
Rakowski W, Andersen MR, Stoddard AM et al. Confirmatory analysis of opinions regarding the pros and cons of mammography. Health Psychol. 16(5), 433–441 (1997).
31.
Moodi M, Hassanzadeh A, Charkazi A, Shahnazi H, Sharifirad GH. A survey of the psycho-cognitive factors affecting breast cancer screening behaviors at different stages of change among female teachers in Isfahan, Iran. J. Heal. Sys. Res. 7(6), 770–781 (2011).
32.
Miao M. To explore the breast cancer risk factors and its related recognition in Jilin province[D]. Jilin University (2017). https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CMFD&dbname=CMFD201702&filename=1017160724.nh&v=MTQxMjNMdXhZUzdEaDFUM3FUcldNMUZyQ1VSN3FmWXVSdUZ5N2hVTDdBVkYyNkdiSytIdGJPcTVFYlBJUjhlWDE=
33.
Cao H-L. The Chinese Localization of the Readiness for Return to work Scale and the Application in Breast Cancer Patients [D]. Zhengzhou University. 12 (2018). https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CMFD&dbname=CMFD201802&filename=1018109781.nh&v=MzAxNTRxVHJXTTFGckNVUjdxZll1UnVGeTdoVkx6QlZGMjZGcks0RjliRXJwRWJQSVI4ZVgxTHV4WVM3RGgxVDM=
34.
Farajzadegan Z, Fathollahi-Dehkordi F, Hematti S, Sirous R, Tavakoli N, Rouzbahani R. The transtheoretical model, health belief model, and breast cancer screening among Iranian women with a family history of breast cancer. J. Res. Med. Sci. 21, 122 (2016).
35.
Gesink D, Filsinger B, Mihic A et al. Cancer screening barriers and facilitators for under and never screened populations: a mixed methods study. Cancer Epidemiol. 45, 126–134 (2016).
36.
Song W, Tamaki Y, Arakawa Y et al. Correlation of dental health behavior with health awareness and subjective symptoms in a rural population in Japan. Asia Pac. J. Public Health 26(3), 275–284 (2014).
37.
Dodo AM, Sykes P, Powell C. Exploring the barriers to breast and cervical cancer screening in Nigeria: a narrative review. Afr. J. Reprod. Health 20(4), 89–98 (2016).
38.
Abdel-Aziz SB, Amin TT, Al-Gadeeb MB et al. Perceived barriers to breast cancer screening among Saudi women at primary care setting. Asian Pac. J. Cancer Prev. 18(9), 2409–2417 (2017).
39.
Vandyke SD, Shell MD. Health beliefs and breast cancer screening in rural appalachia: an evaluation of the health belief model. J. Rural Health 33(4), 350–360 (2017).
40.
Yilmazel G. Health literacy, mammogram awareness and screening among tertiary hospital women patients. J. Cancer Educ. 33(1), 89–94 (2018).
•• Illustrates the importance of exploring the influencing factors of breast cancer awareness and screening.
41.
Anwar SL, Tampubolon G, Van Hemelrijck M, Hutajulu SH, Watkins J, Wulaningsih W. Determinants of cancer screening awareness and participation among Indonesian women. BMC Cancer 18(1), 208 (2018).
42.
Jeronimo AF, Freitas AG, Weller M. Risk factors of breast cancer and knowledge about the disease: an integrative revision of Latin American studies. Cien Saude Colet 22(1), 135–149 (2017).
43.
Rojas K, Stuckey A. Breast cancer epidemiology and risk factors. Clin. Obstet. Gynecol. 59(4), 651–672 (2016).
44.
Golubnitschaja O, Debald M, Yeghiazaryan K et al. Breast cancer epidemic in the early twenty-first century: evaluation of risk factors, cumulative questionnaires and recommendations for preventive measures. Tumour Biol. 37(10), 12941–12957 (2016).
45.
Liu LY, Wang YJ, Wang F et al. Factors associated with insufficient awareness of breast cancer among women in Northern and Eastern China: a case-control study. BMJ Open 8(2), e018523 (2018).
46.
Zhang S-J, Du J. Health information literacy should become the critical point of health literacy promotion for the Chinese public. J. Med. Intell. 31(2), 45–49 (2010).
47.
Fu S, Deng S, Chen X. Review on the foreign research status and development trend of health information literacy. J. Information Resources Management 6(3), 5–14 (2016).
48.
Abeje S, Seme A, Tibelt A. Factors associated with breast cancer screening awareness and practices of women in Addis Ababa, Ethiopia. BMC Womens Health 19(1), 4 (2019).
49.
Abu-Helalah MA, Alshraideh HA, Al-Serhan AA, Kawaleet M, Nesheiwat AI. Knowledge, barriers and attitudes towards breast cancer mammography screening in Jordan. Asian Pac. J. Cancer Prev. 16(9), 3981–3990 (2015).
50.
Memon ZA, Kanwal N, Sami M, Larik PA, Farooq MZ. Risk of breast cancer among young women and importance of early screening. Asian Pac. J. Cancer Prev. 16(17), 7485–7489 (2015).
Information & Authors
Information
Published In
Pages: 679 - 689
PubMed: 32648473
Copyright
© 2020 Future Medicine Ltd.
History
Received: 1 March 2020
Accepted: 18 May 2020
Published online: 10 July 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Factors influencing breast cancer awareness: a cross-sectional study in China. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0037
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yang Lyu, Wei Guo, Zhen Wang, Catherine Paterson, Frances Lin, Urban residents’ health literacy of four major cancers: a cross-sectional national survey, Frontiers in Public Health, 10.3389/fpubh.2026.1762797, 14, (2026).
- Mengwei Jiang, Bei Wu, Yi Liu, Detian Liu, Xiaoye Chen, Ting Shu, Zijun Yuan, Linxin Xie, Hongzhen Xie, Latent profile analysis of health literacy among breast cancer patients and comparative analysis of quality of life disparities, Frontiers in Oncology, 10.3389/fonc.2026.1769721, 16, (2026).
- Suchan Yao, Weijing Cai, Ling Qin, Coordinated psycho-oncology in young adults with breast cancer: equity gradients, timely access, and out-of-pocket spending in China, Supportive Care in Cancer, 10.1007/s00520-026-10596-z, 34, 4, (2026).
- Andrea Fejer, Mohammad Amin Atbaei, Afshin Zand, Timea Varjas, Zsuzsanna Kiss, Psychometric Properties of the Breast Cancer Awareness Measure (Breast-CAM): A Systematic Review and Meta-Analysis, Cancers, 10.3390/cancers18060956, 18, 6, (956), (2026).
- Rui Li, Sabzali Musa Kahn, Bingyu Duan, Seng Yue Wong, Gamified Versus Nongamified Metaverse Learning for Breast Health Knowledge in Women: Randomized Controlled Trial, JMIR Serious Games, 10.2196/75318, 14, (e75318-e75318), (2026).
- Jiayu Liu, Hao Hu, Carolina Oi Lam Ung, Menghuan Song, Facilitators and barriers to the decision-making of breast cancer screening in female residents in Mainland China: a systematic literature review, BMC Public Health, 10.1186/s12889-026-26233-7, 26, 1, (2026).
- Ecem Çi̇çek Gümüş, Burcu Küçükkaya, The relationship between factors affecting breast cancer knowledge, awareness and prevention behaviors in women aged 20–49 years: the case of Bartın Province, BMC Women's Health, 10.1186/s12905-025-04149-5, 26, 1, (2026).
- Jingru Zhou, Yanjun Liu, Fang Yang, Yanfen Wang, Yan Liu, Wenwen Ming, Sisi Guo, Dan Zhou, Lin He, Xiaoli Zhong, Health-promoting lifestyle among Chinese patients with colorectal polyps: a cross-sectional study, Scientific Reports, 10.1038/s41598-025-90352-1, 15, 1, (2025).
- M. M. Sana, Rahul Radhakrishnan, S Harikrishna, Sulaikha Abdul Kareem, Haritha Mukund, S. J. Sajna, Evaluating Breast Cancer Awareness and Self-Examination Practices Among Women in Low Socio-Economic Areas of South India, Indian Journal of Gynecologic Oncology, 10.1007/s40944-025-00972-8, 23, 1, (2025).
- Ewa Sawicka, Natalia Wiatrowska, The Potential Metalloestrogenic Effect of Aluminum on Breast Cancer Risk for Antiperspirant Users, International Journal of Molecular Sciences, 10.3390/ijms26010099, 26, 1, (99), (2024).
- See more