Venous stenting for patients with outflow obstruction and leg ulcers: cost–effectiveness and budget impact analyses
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To perform cost–effectiveness analysis (CEA) and budget impact analysis (BIA) comparing stenting to standard medical treatment (SMT) for the management of deep venous outflow obstruction and leg ulcers from the Italian Healthcare Service perspective. Materials & methods: A Markov model was developed to project costs and quality-adjusted life-years (QALYs) over 3 years, based on data from literature combined with real-world data. Moreover, a BIA was performed comparing the current scenario (100% SMT) with increasing utilization rates of stenting over SMT from 0.5 to 5%, in the next 5 years. Results: Stenting is a cost-effective (incremental cost-utility ratio €12,388/QALY) or dominant option versus SMT, according to in-patient or day-hospital settings, respectively. Increasing use of stenting over SMT, in the next 5 years, is expected to yield additional costs of 39.5 million Euros (in-patient) or savings of 5.1 million Euros (day-hospital). Conclusion: Stenting is a cost-effective option compared with SMT for patients with deep vein occlusion and ulceration in Italy.
Deep vein outflow obstruction is a hemodynamic condition due to stenosis and/or occlusion of the cava and/or iliofemoral veins. It is mainly secondary, caused by post-thrombotic deep veins fibrosis and scarring, but it can be also primary, due to iliac vein nonthrombotic lesions such as compression.
Post-thrombotic syndrome (PTS) is a common long-term complication of deep vein thrombosis (DVT), which consists in chronic venous symptoms and/or signs. Among these, ulcer occurrence is the ultimate and most severe presentation of PTS. Peak prevalence of leg ulceration occurs in the age group 60–80 years and the prevalence rate is expected to increase as the population ages [1]. The disease severity is usually assessed using the Villalta score [2]. Post-thrombotic syndrome occurs in about 20–50% of patients with DVT. The variety of diagnostic scoring systems may be a cause of lack of precision in the reported epidemiological data related to this condition [3].
The mainstay of treatment for the prevention of PTS is elastic compression therapy. So far, few studies have assessed the value of this treatment starting in the acute or subacute phase after DVT, reporting divergent results [4–7]. Moreover, the best onset of compression therapy for the prevention of PTS is unwell defined and narrowly explored.
Compression therapy, with or without anticoagulants, is considered the standard conservative treatment modality [8] for patients with deep venous obstruction and venous ulceration.
In the last years, the endovascular approach to outflow obstruction treatment opened the way to minimally invasive recanalization of the obstructed vein through stent placement, thus drawing the attention on these therapeutic opportunities [9]. These procedures are safe and effective leading to alleviation of the symptoms in the lower extremities [10]. On the other hand, the evidences are derived mainly from retrospective studies conducted in single centers and with limited sample sizes.
The aim of the present study was to develop knowledge on the clinical and economic implications of both treatment strategies in order to support the stakeholders at national level in the management of patients with deep venous obstruction and leg ulcers. In particular, the main aim of the study was to perform a cost–effectiveness analysis comparing endovascular venous stenting procedure to standard medical treatment (SMT, compression therapy ± anticoagulation), from the Italian Healthcare System perspective. The second aim of the study was to assess the budget impact on the public healthcare expenditure of an increased diffusion of the endovascular treatment over SMT for patients with deep venous obstruction and leg ulcers.
In the preliminary phase of the study, a systematic literature review has been performed to derive the clinical evidences for the two options in order to populate the cost–effectiveness model, as better specified in the Methods section.
Methods
Literature review
A literature review has been conducted in order to retrieve clinical evidences on deep vein obstruction and presence of ulcers, and in particular rates of ulcers healing and recurrence for both stenting procedure and SMT. The search focused on studies published in the last ten years. A systematic literature search has been performed through Pubmed and Web of Science databases in July 2019. The search strategy and PRISMA diagrams are presented in Supplementary Material 1.
Studies were considered if published in English and if they referred to an adult population. Studies were included in case they provided data on clinical evidence for the use of the two treatment options. Both comparative and single-arm studies were considered. Editorials, case reports, letters and reviews were not considered.
The selection of abstracts and full-texts was conducted independently by two expert reviewers (CR, RT). In case of debate on eligibility, studies were verified in a collaborative way until a consensus was obtained. Through a customized template developed in Microsoft Excel, the following data were extracted from the retrieved studies: study features, participants’ characteristics and clinical outcomes.
As much importance is given to the collection and analysis of real-world data for the evaluation of outcomes and costs of health technologies [11,12], clinical data on endovascular stenting, collected at Hesperia Hospital, which is the hospital in Italy presenting the largest case-series, have been retrieved in order to estimate rates of ulcers healing and recurrence in the clinical practice, to integrate the literature search.
Clinical data synthesis
Twenty-nine studies have been retrieved reporting data for stenting procedure, of which 19 reported data on ulcer healing rates and recurrence rates. Concerning standard medical therapy, eight studies with available data were extracted. Those studies considered different types of compression therapy, in particular stockings, bandages (with different number of layers: two, four, multi-layer) and Unna's boot.
Tables 1 & 2 show the study characteristics and retrieved data. Table 2 includes also the real-world data on stenting regarding 64 patients affected by primary obstruction, collected at Hesperia Hospital in Modena, Italy (study Lugli-Longhi-Maleti). These real-world data reported 11 active ulcers with 91% healing rate (mean healing time 3 months) and 0% of recurrences considering a follow-up of 24 months.
| Study (year) | Study type | Country | Type of therapy | FUP (months) | N pts | N ulcers | % healed | Healing time (days) | % recurrences† | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| Adderley et al. (2014) | Multicenter randomized controlled trial | England and Northern Ireland | Bandages | 12 | 224 | 224 | 70% | 98 | 23% | [13] |
| Stockings | 12 | 230 | 230 | 71% | 99 | 14% | ||||
| Alden et al. (2013) | Retrospective study | USA | Compression | 12 | 47 | 47 | 85% | 154 | 49% | [14] |
| Dolibog et al. (2013) | Prospective, randomized, comparative study | Poland | Stockings | 2 | 30 | 30 | 57% | NA | NA | [15] |
| Multi-layer short-stretch bandaging | 2 | 29 | 29 | 59% | NA | NA | ||||
| Two-layer short-stretch bandaging | 2 | 30 | 30 | 17% | NA | NA | ||||
| Unna's boot | 2 | 30 | 30 | 20% | NA | NA | ||||
| O'Hare et al. (2010) | Randomized controlled trial | UK | Four-layer compression bandages | 6 | 20 | 20 | 85% | NA | 6% | [16] |
| Four-layer compression bandages with additional foam sclerotherapy | 6 | 13 | 13 | 92% | NA | 0% | ||||
| Pham et al. (2012) | Randomized trial | Canada | Four-layer bandage | 12 | 215 | 215 | 83% | 62 | 10% | [17] |
| Short-stretch bandage | 12 | 209 | 209 | 92% | 77 | 13% | ||||
| Szewczyk et al. (2010) | Randomized trial | Poland | Stockings | 3 | 15 | 15 | 53% | NA | NA | [18] |
| Taradaj et al. (2009) | Prospective randomized clinical trial | Poland | Compression stockings and drug therapy | 2 | 40 | 40 | 38% | NA | NA | [19] |
| Short-stretch bandages and drug therapy | 2 | 40 | 40 | 13% | NA | NA | ||||
| Yin et al. (2015) | Retrospective review | China | Stockings | 24 | 94 | 41 | 71% | NA | NA | [20] |
†
Percentages are calculated on the number of healed ulcers.
FUP: Follow-up; NA: Not available; pts: Patients.
| Study (year) | Study type | Country | FUP (months) | N pts | N stents | Procedural success | N ulcers | % ulcers healed | Mean healing time (months) | % recurrences† | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Black et al. (2018) | Retrospective single-center study | UK | 12 | 88 | 101 | NA | 9 | 71% | NA | NA | [21] |
| Blanch Alerany et al. (2014) | Prospective study | Spain | 21 | 36 | 41 | 95% | 5 | 100% | NA | 0% | [22] |
| de Wolf et al. (2015) | Prospective study | NA | 5.4 | 40 | 40 | 100% | 4 | 50% | NA | 100% | [23] |
| George et al. (2014) | Retrospective review of a case series | India | 15 | 38 | 44 | NA | 44 | 60% | 1.5 | 14% | [24] |
| Hartung et al. (2009) | Prospective study | France | 38 | 89 | 89 | 98% | 6 | 100% | NA | 17% | [25] |
| Khafagy et al. (2016) | Prospective study | Egypt | 12 | 12 | 12 | 67% | 1 | 100% | NA | NA | [26] |
| Kurklinsky et al. (2012) | Retrospective study | USA | 11.3 | 89 | 91 | 100% | 17 | 53% | NA | NA | [27] |
| Lichtenberg et al. (2019) | Prospective study | Germany | 6 | 80 | 116 | NA | 10 | 80% | NA | NA | [28] |
| Liu et al. (2014) | Prospective cohort study | China | 12 | 48 | 48 | 96% | 7 | 71% | NA | 29% | [29] |
| Lugli-Longhi-Maleti et al. (2019)‡ | Real-world data | Italy | 24 | 64 | 64 | 100% | 11 | 91% | 3 | 0% | |
| Nayak et al. (2012) | Retrospective study | USA | 11.7 | 44 | 50 | 96% | 7 | 71% | NA | NA | [30] |
| Raju et al. (2009) | Prospective study | USA | 33 | 159 | 167 | 83% | 32 | 56% | NA | 0% | [31] |
| Rollo et al. (2017) | Retrospective study | USA | 3 | 31 | 42 | 100% | 3 | 67% | 3 | NA | [32] |
| Rosales et al. (2010) | Prospective study | Norway | 33 | 34 | 34 | 94% | 7 | 57% | 3 | NA | [33] |
| Sang et al. (2014) | Retrospective study | China | 36.2 | 67 | 67 | 94% | 3 | 100% | NA | 0% | [10] |
| Sarici et al. (2014) | Prospective study | Turkey | 6 | 52 | 59 | 100% | 8 | 75% | NA | NA | [34] |
| Stuck et al. (2018) | Prospective study | Switzerland | 21 | 64 | 64 | 98% | 4 | 75% | NA | NA | [35] |
| Tosenovsky et al. (2019) | Prospective study | Australia | 12 | 109 | 118 | 100% | 32 | 53% | 3 | 18% | [36] |
| Ye et al. (2014) | Retrospective study | China | 25 | 110 | 118 | 95% | 46 | 78% | NA | 0% | [37] |
| Yin et al. (2015) | Retrospective study | China | 24 | 122 | 122 | 95% | 49 | 87% | NA | 0% | [20] |
†
Percentages are calculated on the number of healed ulcers.
‡
Real-world data from Hesperia Hospital, Modena, Italy.
FUP: Follow-up; NA: Not available; pts: Patients.
The evidences retrieved from the literature were retrospective or prospective studies presenting data on healing and recurrence rates. Evidence was neither available from head-to-head trials comparing the two options, nor from trials comparing each of the interventions of interest with the same comparator (e.g. placebo), so the method of indirect comparisons [38] was not applicable and, therefore, separate meta-analyses have been performed for stenting and SMT considering single arm data on percentage of ulcer healing and recurrence. In order to facilitate comparisons, for meta-analyses and CEA modeling, ulcers recurred have been reported as a percentage of the number of active ulcers.
The analyses have been performed using Stata software (metaprop command). A random-effect model was applied assuming that the true effect size varies among the studies [39]. A test on the summary effect measure has been reported, as well as a test for heterogeneity quantified by I2 (range 0%–100%, higher values representing higher heterogeneity among the studies) [40]. Figures 1 & 2 report the forest plots obtained. Studies concerning SMT and stenting considered a maximum follow-up of 24 and 36.2 months, respectively.
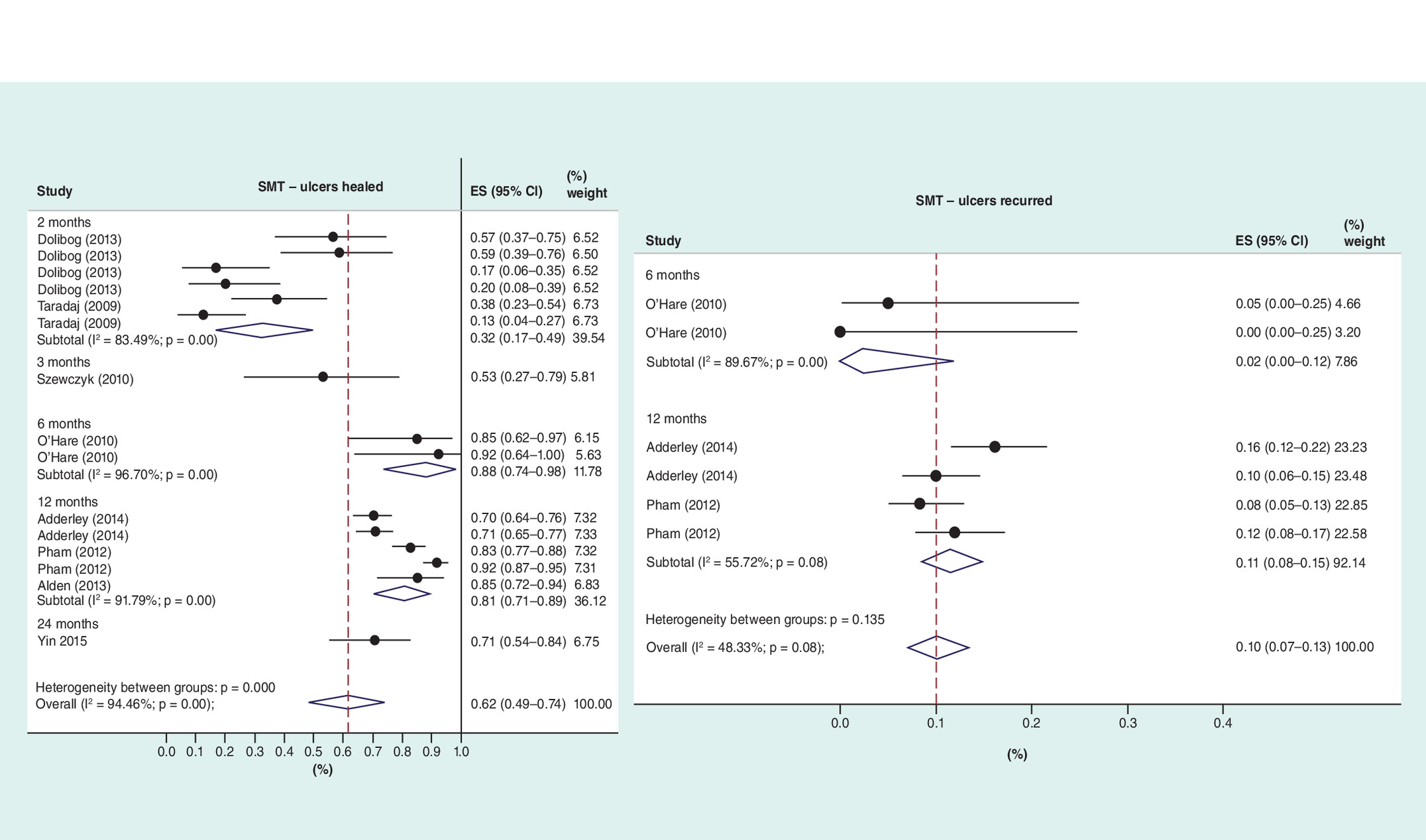
Figure 1. Forest plots for % of ulcers healed and % of ulcers recurred for SMT.
ES: Effect size; SMT: Standard medical treatment.
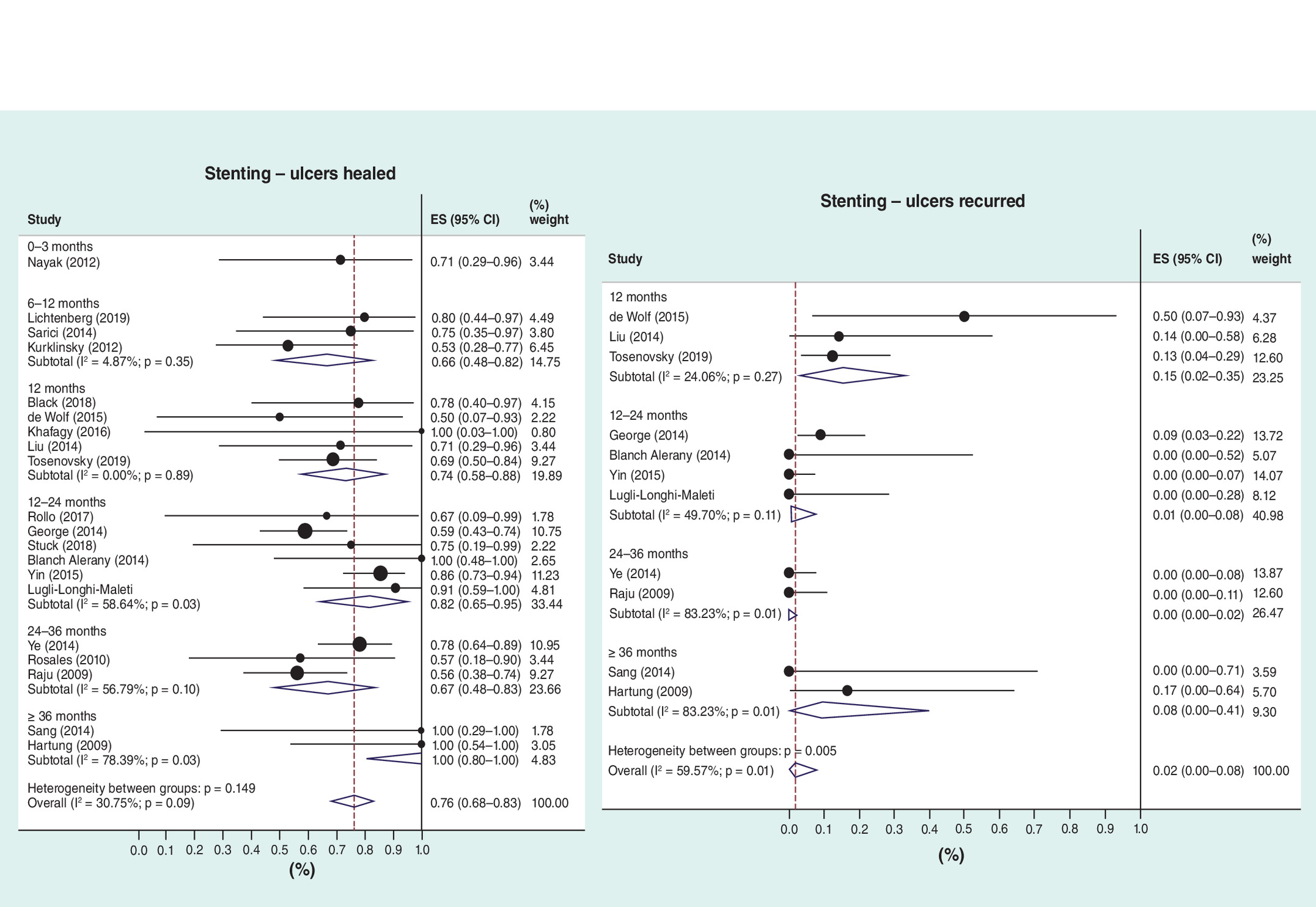
For SMT the percentage of ulcers healed was 62% (mean healing time 3 months), with 10% of recurrences, while for stenting those values were 76% (mean healing time 2.2 months) and 2%. The higher heterogeneity among studies was reported for ulcers healed with SMT.
The model
A CEA model has been developed with TreeAge Pro Software (TreeAge Software, Inc., MA, USA) in order to compare venous stenting with SMT from the National Healthcare Service perspective in Italy. The analysis was reported according to Consolidated Health Economic Evaluation Reporting Standards (CHEERS) [41]. The CHEERS checklist is reported in Supplementary Material 2.
A Markov multistate model has been developed to estimate quality-adjusted life years (QALYs) and economic outcomes associated with stenting procedure and SMT in an adult population with deep venous outflow obstruction and leg ulcers. Markov models, which are frequently used in economic evaluations, allow to represent the possible consequences of the options of interest. The model has been informed by percentages of ulcers healed and recurred obtained from the meta-analyses. As the longest mean follow-up considered in the studies was about 36 months, this time horizon has been considered in the model. A discount rate of 3% has been applied to QALYs and costs [42] and 1-month Markov cycle length has been chosen.
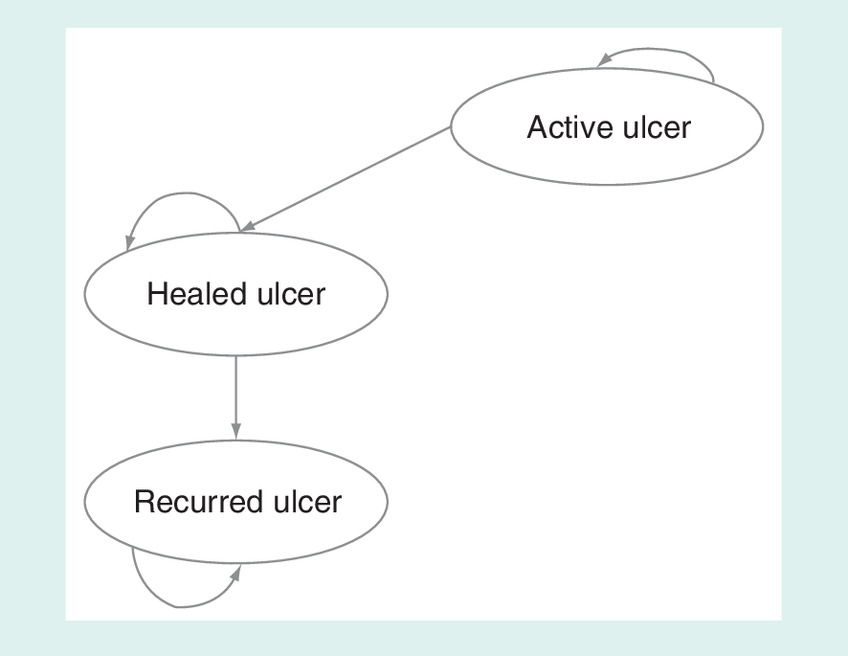
The health states considered in the implemented model were: ‘active ulcer’, ‘healed ulcer’ and ‘recurred ulcer’. Because in the literature there is insufficient evidence for an increased risk of mortality with venous leg ulcers [43], a death state has not been included in the model. No mortality has been shown also in Hesperia Hospital, which has the largest case-series on endovascular stenting in Italy for this kind of patients. In the view of the limited time horizon of the model and the mean age of the indicated population, also overall mortality has not been considered. Moreover, considering that no complications [32,36] or low rates of complications (2%) [35] are reported for stenting in more recent studies, also a complication health state has been excluded from the model.
Adult patients with deep venous outflow obstruction and leg ulcers enter the Markov model in the ‘active ulcer’ health state; they may stay in the ‘active ulcer’ state or, in case of healing, may move to the ‘healed ulcer’ state. In case of ulcer recurrence, patients will move from ‘healed ulcer’ to ‘recurred ulcer’ health state.
Transition probabilities between health states for patients undergoing SMT or stenting have been estimated according to percentages of ulcers healed and recurred retrieved by the meta-analyses (Supplementary Table 1). Exponential functions have been considered leading to constant transition probabilities. For the health state ‘healed ulcer’ the model considers a healing time of 2 and 3 months for stenting and SMT, respectively, so transition probabilities for these states are set equal to 0 in the subsequent period. The model structure is presented in Figure 3, while Supplementary Figure 1 reports patients’ distributions (Markov cohort analysis) over time among the health states for SMT and stenting.
Healthcare resource consumption & costs
The model included only direct healthcare resource consumption (direct costs; Eur, 2019). For the endovascular procedure two models of care were considered, in other words, regular hospital admission and day-hospital care. The Italian NHS uses the DRG system to remunerate hospital services. DRG 479 refers to vascular procedure but its tariff differs according to whether it is delivered in day-hospital (€2258) or through a regular admission (€4742).
The cost of compression therapy and anticoagulants has been estimated in €14.3 per week from [44] (€16.02 uplifted to year 2019). Because compression therapy is often combined with endovascular treatment, this cost has been computed in both treatment strategies.
For both compared options, the management cost for a healed ulcer has been estimated in 2981£ (€3450) per patient from a published study in the UK context [45]. The same study reported a mean cost per patient for unhealed ulcer of £13,455 (€15,574) that in the model has been considered for active ulcer and for ulcer recurrence. These costs include visits, exams, dressings and drugs (e.g., analgesics and anti-infectives) and cover a time horizon of 1 year.
Costs related to the healthcare resource consumption are summarized in Table 3.
| Item | Cost | Ref. |
|---|---|---|
| Endovascular procedure (stenting) | €2258 (day-hospital setting for stenting) €4742 (regular hospital admission for stenting) | Diagnosis Related Group 479: Other vascular procedures without complications |
| Compression therapy and anticoagulants | €16.02 per week | [44] |
| Ulcer management | Healed ulcer €3450 Unhealed ulcer €15,574 | [45] |
Quality-of-life estimates
For the utility coefficients for the health states of the model we made reference to a published study [46] which collected health utility data from 200 people with venous leg ulcers using the standard gamble method. We considered 0.73 (range 0.70–0.76) for active ulcer, 0.64 for recurred ulcer (range 0.61–0.68) and 1 for healed ulcer.
Cost–effectiveness analysis
The incremental cost-utility ratio (ICUR) has been calculated as the difference in mean expected costs (i.e., incremental cost, ΔC) between endovascular treatment and SMT divided by the difference in mean expected outcomes (i.e., incremental QALYs, ΔE) between these strategies (ICUR = ΔC/ΔE).
Deterministic and probabilistic sensitivity analyses (PSA) have been performed in order to test the robustness of the model. Univariate analyses have been performed according to the monthly cost of compression and anticoagulants, the cost for the management of healed ulcer and unhealed ulcer, the cost for the endovascular procedure, utility coefficients for active ulcer, healed ulcer and recurred ulcer and discount rate. The discount rate has been varied between 0 and 10%, while the other parameters have been varied of ±20% of their baseline values. The results of the analyses have been reported as tornado diagrams for the ICUR according to both settings for stenting (regular hospital admission and day-hospital). The PSA has been conducted by assigning distributions to model parameters (beta for utilities and gamma for costs, with a standard deviation of 20% of the baseline value). In Monte Carlo simulations, all parameters were randomly sampled from their assigned distributions considering a cohort of 10,000 patients. Results have been presented graphically as scatterplots in the cost–effectiveness plane considering a cost–effectiveness threshold of €30,000. Supplementary Table 2 reports the details on the parameters used in these analyses.
In absence of strong evidences that report lower recurrence rates for stenting than SMT, the structural uncertainty of the model has been explored by using one pooled estimate for this parameter for both strategies. Consequently, a meta-analysis has been performed on percentage of ulcers recurred by pooling the studies on SMT and stenting retrieved from the systematic literature search. This meta-analysis yielded a percentage of ulcers recurred equal to 4% (Supplementary Figure 2).
Another structural uncertainty has been evaluated by including a death state in the model representing overall mortality according to Italian life tables [47]. A population aged 60 years as evaluated by Cheng and colleagues [43] has been considered entering the model since vein obstruction and leg ulcers mainly affect the elderly population.
Budget impact analysis
A budget impact model has been developed based on the CEA model in order to estimate the expected changes in the next 5 years in the public healthcare expenditure for the Italian Healthcare Service in the hypothesis of an increased utilization of stenting over SMT for patients experiencing deep vein obstruction and ulceration. The analysis has been conducted in accordance with the ISPOR Principles of Good Practice for Budget Impact Analysis [48].
The model has been developed according to the following steps:
•
Research and analysis of epidemiological data (i.e., incidence) relating to patients with deep vein obstruction and ulceration in Italy;
•
Definition of the current scenario of distribution of patients among the two alternative options;
•
Definition of future scenarios with appropriate increased use of stenting over SMT, considering different annual penetration rates.
The incidence of venous leg ulcers in Italy in people aged over 65 years accounts for about 0.76/100 person-years in men and 1.42/100 person-years in women [1], meaning that about 156,000 patients are affected each year.
As the use of stenting for deep vein obstruction and ulceration is an emerging technology in Italy, the current scenario of patients’ distribution between the two alternative options considered 100% of use of SMT. For the same reason, future scenarios considered small increased proportions of stenting over SMT of 0.5, 1, 2, 3 and 5% for the following 5 years. However, additional scenario analyses have been performed by considering a more significant adoption of stenting in the next 5 years (scenario 1: 1, 2, 4, 6, 10%; scenario 2: 2, 4, 8, 12 and 20%).
The model applies the variations of the market share to the new incident cohorts (naive treatments). Constant yearly incident cohorts of 156,000 patients were considered in the analysis. The costs for current and future scenarios were estimated by multiplying yearly costs of each option by the proportion of the eligible population using that option and by the number of patients in the eligible population, taking into account subsequent yearly incident cohorts. As the focus was on the expected budget at each point in time, the financial streams were presented as undiscounted costs [48].
Results
Cost–effectiveness analysis
Considering a time horizon of 3 years, the average estimated QALYs were 2.66 and 2.51 respectively for patients undergoing stenting and SMT regimens. For stenting, in the scenario considering the DH setting (tariff €2258), the estimated mean cost per patient was €8935, while considering the regular hospital admission the mean cost per patient was €11,419. The mean cost per patient for SMT was €9,566. The model results for the two scenarios are summarized in Table 4. When the DH setting for stenting was considered, stenting was the dominant strategy (lower cost and higher QALYs), while considering the regular hospital admission for stenting, the ICUR of stenting versus SMT was €12,388/QALY, highlighting the cost–effectiveness of the endovascular procedure (ICUR <€30,000).
| Scenario | Option | Costs | QALYs | Incremental cost | Incremental QALYs | ICUR |
|---|---|---|---|---|---|---|
| DH setting for stenting | Stenting | €8935 (7092; 11,010) | 2.66 (2.30; 2.79) | -€631 (-2227; 906) | 0.15 (0.03; 0.27) | Stenting dominant |
| SMT | €9566 (6995; 12,601) | 2.51 (2.06; 2.74) | ||||
| Regular hospital admission for stenting | Stenting | €11,419 (9300; 14,165) | 2.66 (2.30; 2.79) | €1853 (-306; 4,219) | 0.15 (0.03; 0.27) | €12,388/QALY |
| SMT | €9566 (6995; 12,601) | 2.51 (2.06; 2.74) |
DH: Day-hospital; ICUR: Incremental cost-utility ratio; QALY: Quality-adjusted life-years; SMT: Standard medical treatment.
Tornado diagrams for both scenarios (DH and regular hospital admission for stenting) reporting one-way sensitivity analyses for the ICUR, according to variations of the model parameters, are reported in Figure 4. Because stenting was the dominant option in the scenario considering the DH setting for the endovascular procedure, the represented ICUR is negative. We chose to represent the ICUR for both scenarios, instead of net monetary benefit [49], in order to present analyses on the same outcome considered in the CEA. The parameters for both scenarios reporting the greater variations on the ICUR were the costs for the endovascular procedure and for the management of an unhealed ulcer, and the utility coefficients for ‘healed ulcer’ and ‘active ulcer’ health states. For the scenario considering the DH tariff for stenting (A), an annual cost for the management of an unhealed ulcer lower than €12,487.6 lead stenting to loose dominance but it remains cost-effective compared with SMT (ICUR = €39 considering a management cost for unhealed ulcer of €12,459, see lower value in Supplementary Table 2).
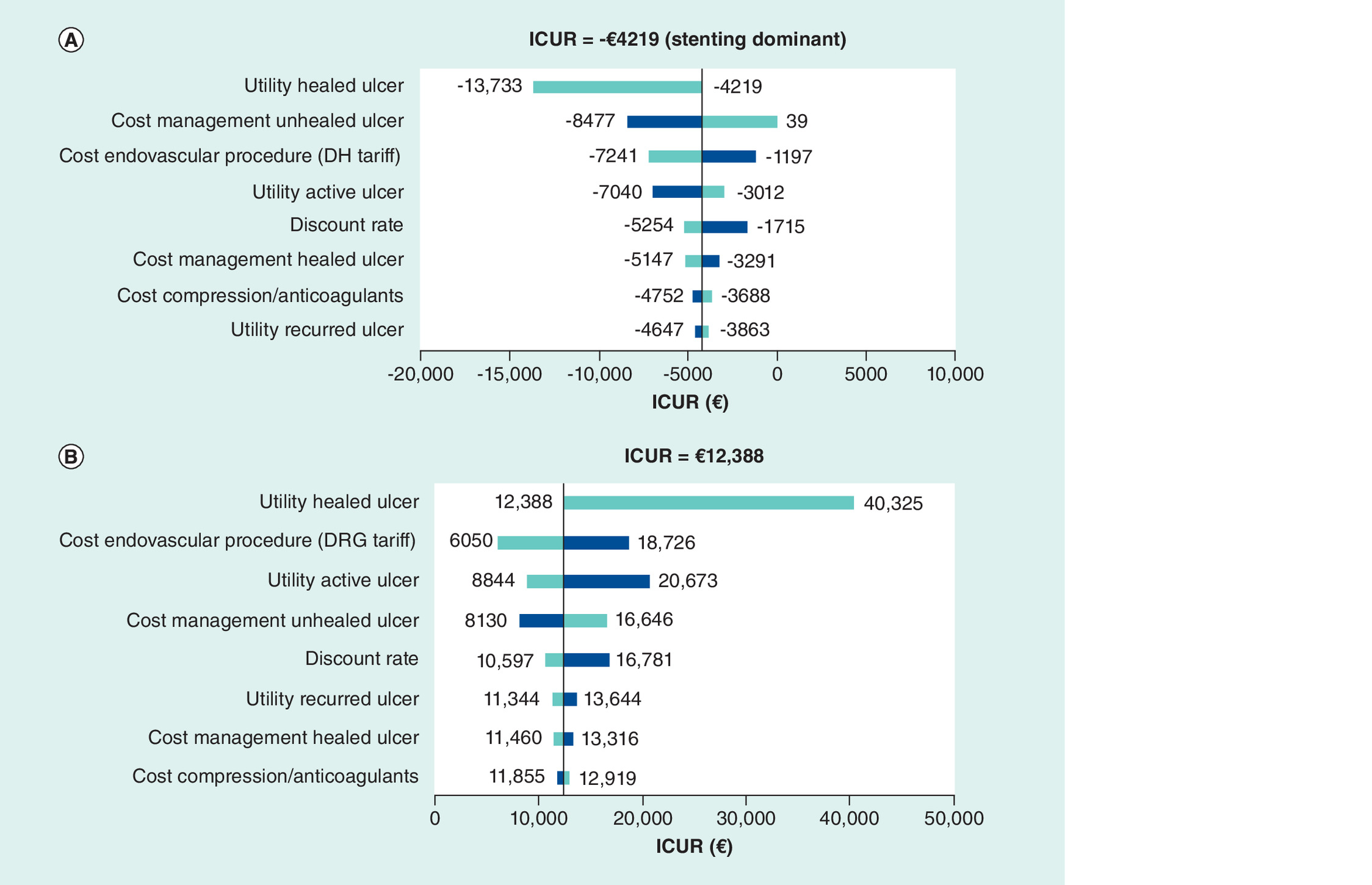
Figure 4. Tornado diagram reporting one-way sensitivity analyses: (A) DH setting for stenting; (B) regular hospital admission for stenting.
The vertical line in the middle represents the incremental value between the two strategies using the base-case value for each parameter. As the parameters deviate from their base-case values, the ICUR changes. A dark bar represents the variation of the ICUR when the parameter ranges from the base-case to the high uncertainty value, conversely, a light bar shows the ICUR variation when the parameter ranges from the low uncertainty value to the base-case value.
ICUR: Incremental cost-utility ratio; DH: Day-hospital; DRG: Diagnosis related group.
Regarding PSA, the plots of incremental costs versus incremental QALYs obtained from the Monte Carlo simulations are shown in Figure 5 (A: DH setting for stenting; B: Regular hospital admission for stenting). Dotted lines represent a theoretical cost–effectiveness threshold of 30,000€/QALY; 99.6% and 83.6% of points lie below this line for A and B scenarios, respectively. Table 4 reports 95% credible intervals for all relevant outcomes of the model according to PSA.
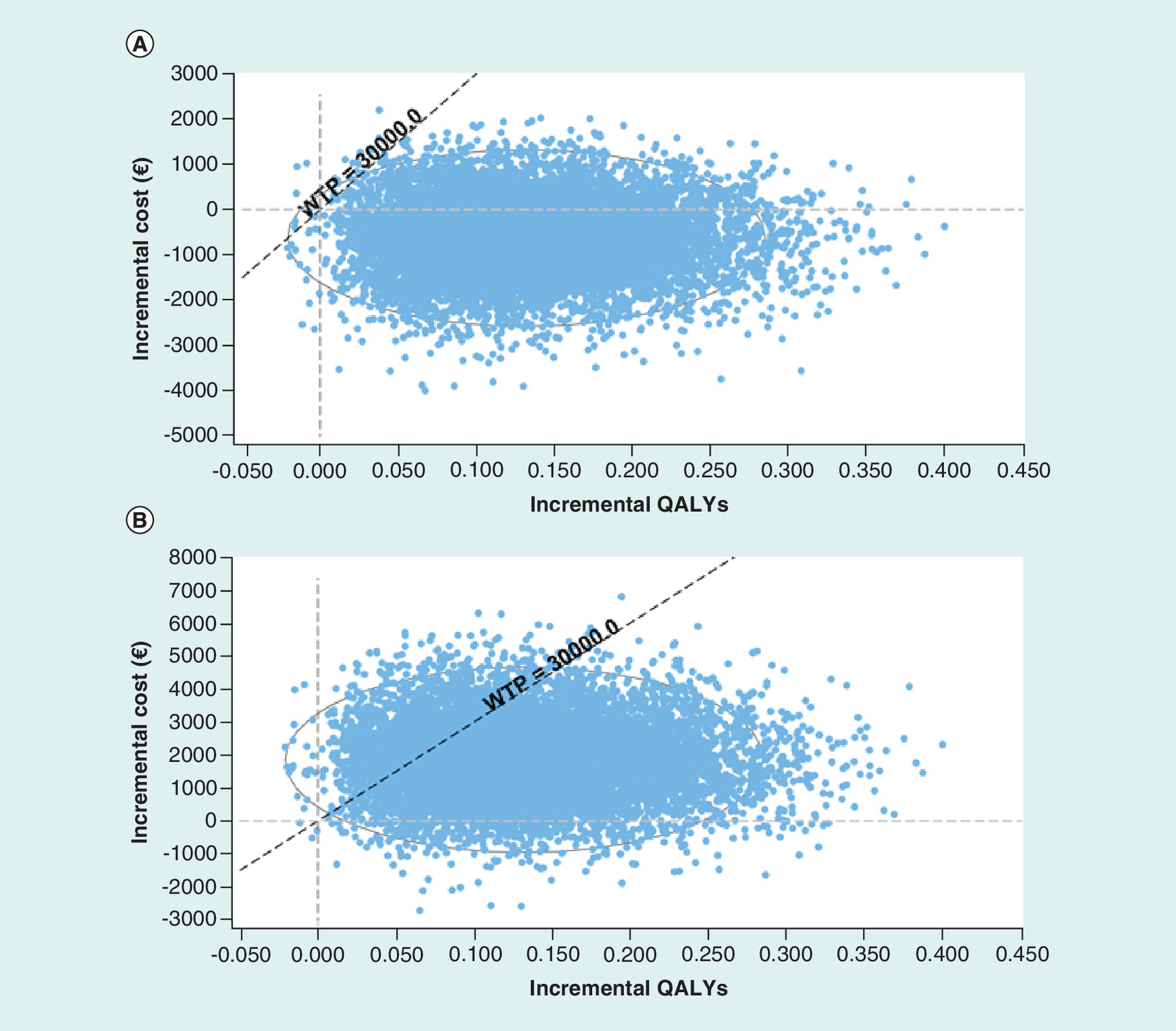
Figure 5. Scatterplots of incremental costs versus incremental QALYs.
(A) Day-hospital setting for stenting; (B) regular hospital admission for stenting.
QALY: Quality-adjusted life-years; WTP: Willingness To Pay.
In order to explore the structural uncertainty of the model on the representation of ulcer recurrences, a scenario analysis has been evaluated by considering the same percentage of ulcers recurred, equal to 4% for both SMT and stenting strategies. In this setting, the ICUR of stenting versus SMT was €3544 and €26,012, for the scenario considering DH and DRG tariff for stenting, respectively, thus confirming the cost–effectiveness of the endovascular procedure (ICUR <€30,000). In this case the PSA showed the cost–effectiveness of stenting versus SMT in 92.4 and 47.6% of simulations for A and B scenarios, respectively.
The scenario analysis that considered the inclusion of a death state for overall mortality reported an ICUR of €15,295 of stenting versus SMT in case the DRG tariff for the endovascular procedure was applied, while stenting was the dominant option in case the DH tariff was considered instead. According to these scenarios, the PSA showed the cost–effectiveness of stenting versus SMT in 99.3 and 76.1% of simulations, respectively.
Budget impact analysis
In the scenario with regular hospital admission for stenting, the mean cost (undiscounted) per patient was higher tha0n SMT, leading to higher costs for the NHS considering increased uses of the endovascular technology. Conversely, in the scenario with DH setting for stenting, this cost was lower than SMT, leading to budget savings for the healthcare service. Yearly costs for the two options, obtained from the CEA model, are reported in Supplementary Table 3.
Compared with the current scenario (year 0), by progressively increasing the use of stenting for patients with deep vein obstruction and ulceration to 0.5, 1, 2, 3 and 5%, in the scenario which considers the regular hospital admission for stenting the incremental expenditure for the Italian Healthcare Service would be €39,458,060 over the next 5 years. If conversely the procedure is delivered in day-hospital, the increasing use of stenting would save to the Italian NHS €5,104,900 over the next 5 years (Table 5).
| Scenario considering regular hospital admission for stenting | ||||||||
|---|---|---|---|---|---|---|---|---|
| Current scenario | ||||||||
| Year | SMT | Stenting | ||||||
| Market share | Users cohort | Cost | Market share | Users cohort | Cost | Total budget impact | ||
| 0 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 1 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 2 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 3 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 4 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 5 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| Future scenario | ||||||||
| Year | SMT | Stenting | ||||||
| Market share | Users cohort | Cost | Market share | Users cohort | Cost | Total budget impact | Incremental expenses in comparison to current scenario | |
| 0 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | €0 |
| 1 | 99.5% | 155,220 | €1,604,658,535 | 0.5% | 780 | €8,915,593 | €1,613,574,128 | €2,039,574 |
| 2 | 99% | 154,440 | €1,597,191,966 | 1% | 1,560 | €18,048,060 | €1,615,240,026 | €3,705,472 |
| 3 | 98% | 152,880 | €1,582,258,274 | 2% | 3,120 | €36,316,601 | €1,618,574,876 | €7,040,322 |
| 4 | 97% | 151,320 | €1,566,734,033 | 3% | 4,680 | €54,802,016 | €1,621,536,049 | €10,001,496 |
| 5 | 95% | 148,200 | €1,536,866,650 | 5% | 7,800 | €91,339,099 | €1,628,205,749 | €16,671,195 |
| Total incremental expenditure | €39,458,060 | |||||||
| Scenario considering day-hospital setting for stenting | ||||||||
| Current scenario | ||||||||
| Year | SMT | Stenting | ||||||
| Market share | Users cohort | Cost | Market share | Users cohort | Cost | Total budget impact | ||
| 0 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 1 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 2 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 3 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 4 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| 5 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | |
| Future scenario | ||||||||
| Year | SMT | Stenting | ||||||
| Market share | Users cohort | Cost | Market share | Users cohort | Cost | Total budget impact | Incremental expenses in comparison to current scenario | |
| 0 | 100% | 156,000 | €1,611,534,553 | 0% | 0 | €0 | €1,611,534,553 | €0 |
| 1 | 99.5% | 155,220 | €1,604,658,535 | 0.5% | 780 | €6,978,073 | €1,611,636,608 | €102,054 |
| 2 | 99% | 154,440 | €1,597,191,966 | 1% | 1,560 | €14,173,020 | €1,611,364,986 | -€169,568 |
| 3 | 98% | 152,880 | €1,582,258,274 | 2% | 3,120 | €28,566,521 | €1,610,824,796 | -€709,758 |
| 4 | 97% | 151,320 | €1,566,734,033 | 3% | 4,680 | €43,176,896 | €1,609,910,929 | -€1,623,624 |
| 5 | 95% | 148,200 | €1,536,866,650 | 5% | 7,800 | €71,963,899 | €1,608,830,549 | -€2,704,005 |
| Total savings | €5,104,900 | |||||||
SMT: Standard medical treatment.
The scenarios which consider a more significant adoption of stenting showed incremental costs for the NHS of €78,916,119 (scenario 1: 1, 2, 4, 6 and 10%) and €157,832,239 (scenario 2: 2, 4, 8, 12 and 20%) when considering a full DRG tariff for stenting, while in the setting of DH possible savings were €10,209,801 (scenario 1) and €20,419,601 (scenario 2).
Discussion
Despite preventive strategies, deep vein outflow obstruction, primary or more frequently secondary, is a hemodynamic alteration leading to substantial morbidity. Although current epidemiological data are lacking, it is estimated that 1–2% of people over the age of 65 years suffer leg ulceration [50], one of the worst symptoms of PTS. Chronic wounds are more difficult to heal and the treatment of leg ulcers is associated with the use of considerable healthcare resources.
Besides the standard conservative treatment performed with compression items, the endovascular approach through stenting has become a broadly accepted treatment strategy in chronic venous obstruction reporting minimal complications, high technical success rates and short hospital stay [51].
The literature reports studies evaluating the cost–effectiveness of different types of compression therapy for the treatment of venous leg ulcers [17,52,53] but to our knowledge only one abstract published a cost–benefit analysis comparing stenting versus compression therapy for patients with chronic total venous occlusion in USA [54]. This study, although performed on a limited number of patients (9 stenting+compression, 17 compression alone), analyzed the actual costs from the hospital perspective and quality of life data for the two treatment strategies and showed that iliac stenting for venous leg ulcers resulted in less cost (US$1913 per patient) and increase in quality of life (0.01 QALYs) compared with compression alone, over a time horizon of 3 years.
The present study showed that, according to different models of care (i.e., regular admission and day-hospital), stenting procedure for the treatment of deep vein occlusion and ulceration may be a cost-effective or cost-saving option in comparison to SMT. The clinical effectiveness for stenting and SMT was derived by meta-analyses starting from data reported in the literature and the robustness of the results has been shown through one-way and probabilistic sensitivity analyses. Uncertainty on rates of recurred ulcers has been explored, as well. The budget impact analysis (BIA) clearly highlighted that the endovascular procedure delivered in a day-hospital setting would save public healthcare expenditure of nearly 5 million Euros in the next 5 years. Given that day hospital regime seems to be as safe as regular hospital admissions, our recommendation is to adopt this treatment option in order to provide patients with a more effective treatment and the Italian NHS with a cost-saving strategy. The present study raises considerations about the setting of applicability of DRG tariffs for stenting. The vast majority of countries are trying to reduce as much as they can the number of hospital beds (e.g. in Italy from 4.7/1000 inhabitants in 2000 to 3.2/1000 inhabitants in 2017 [55]) in order to contain costs and improve patients’ experience outcomes and quality of life. In this way, they carry out a progressive shift of services from in-patient assistance to outpatient and territorial care. In this context if from one hand the in-patient assistance may be appropriate for stenting procedure at the beginning, when this new technology is first introduced in the clinical practice, needing more time to supervise the patients, from the other hand, once clinicians have completely learned the endovascular technique and how to manage the patients, the day-hospital may be the adequate setting for this procedure, being consistent with the strategy of healthcare systems to apply care also economically sustainable.
Our study has a number of limitations. First of all, the model did not consider possible complications due to the endovascular procedure. Although studies reported very high frequencies of technical success for stenting, in case of complications the management cost may increase, potentially compromising the cost–effectiveness results. This concept is related also to the experience of the operators who perform the interventions; it has been demonstrated that clinical outcomes and resource consumption related to patients managed with new technologies, such as stenting, may be strongly influenced by the underlying learning curve of operators. Continuous data collecting and monitoring could provide more robust data also for the evaluation of this aspect.
Second, in the base-case model we did not consider patients’ mortality as in the literature there is lack of evidence reporting an increased risk of death in patients with venous leg ulcers [43]; however, the analysis of a scenario including all-causes mortality confirmed the cost–effectiveness of stenting compared with SMT. Third, In the cost–effectiveness analysis we used a relatively short time horizon based on the follow-up from studies retrieved by the systematic literature search; a similar approach has been followed also by other published studies that evaluated the cost–effectiveness of different technologies or models of care for the treatment of venous leg ulcers. They considered a time horizon for the analyses ranging from 4 to 12 months [17,46,52,53,56] according to the follow-up of studies providing input data for the model. A longer time horizon, equal to 5 years, has been considered in the study by Cheng and colleagues [43]; nevertheless the authors recognized to have assumed a constant risk of recurrence over time in the absence of long-term follow-up data, and to have limited the time horizon to 5 years in order to avoid events overestimation. In light of these considerations, economic evaluations or budget impact analyses have the primary objective to support the policy makers in the healthcare resource allocation process; although decision makers recognize the value of models to obtain cost projections, they require that these models are populated with solid clinical evidence. In the context of medical devices, where innovation is often stepwise, short-term analyses based on the available clinical data may be more relevant and useful to support the decision process [57]. Fourth, the considered studies often did not distinguish the type of vein occlusion, thus if it was a primary (May-Thurner) or a secondary disease (PTS). Subgroup analysis considering different disease causes might have provided more precise results, likely with better clinical outcomes and less costs for patients with primary disease. Another point relates to the treatment's indications. Although the model compares SMT and stenting, these options may not be indicated for the same population. Compression therapy is considered the mainstay of the treatment approach for venous ulcers, while invasive treatments can be considered generally in the failure of compression therapy; nevertheless, the available evidence-based scientific literature reports heterogeneity whenever comparing different treatment guidelines of different countries and sometimes even of different institutions in the same nation [58]. In this context, the definition of the best target population for SMT and stenting may be very challenging and a comprehensive evaluation of the patient and ulcer is required to determine etiology and to frame an appropriate management strategy [59]. Finally, data on patients’ quality of life were derived from a study [46] conducted in UK and the transferability of the retrieved utility values to an Italian context was not considered.
Our findings showed that stenting for the management of deep vein obstruction and ulceration may be a cost-effective option compared with SMT. An additional treatment option is therefore now available to clinicians who may offer an appropriate and individualized management plan for the patients in a view to improve their health. For now, decision-makers may use the preliminary results of the present study in order to support stenting procedure in defined target patient populations. Future studies comparing SMT to stenting will be able to increase the clinical body of evidence in order to confirm or reject the validity of this preliminary evaluation.
Future perspective
Venous ulceration is a common devastating problem that is often the result of obstruction of the iliac veins and inferior vena cava. Venous ulceration is associated with substantial pain, morbidity and cost. Intervention on veins with subsequent stenting has proven to be a low-risk procedure effective in alleviating symptoms and in healing ulcers. However, the widespread use of venous stents without defining exactly which patients may benefit most from the therapy may be problematic. Future research should focus on the development of efficient diagnostic therapeutic pathways in order to offer patients an early diagnosis and timely appropriate treatment interventions. Any potential sign and symptom of venous disorder should be identified early so that an appropriate management can be started as soon as possible. Moreover, the patient should be assessed holistically, preferably with a multidisciplinary team, taking into account all patient-related factors, such as lifestyle, quality of life and overall health factors, including his/her medical history.
•
Post-thrombotic syndrome (PTS) is a common long-term complication of deep vein thrombosis, which consists in chronic venous symptoms and/or signs. Among these, ulcer occurrence is the ultimate and most severe presentation of PTS.
•
Compression therapy, with or without anticoagulants, is considered the standard medical treatment (SMT) modality for patients with deep venous obstruction and venous ulceration. In the last years, the endovascular approach to outflow obstruction treatment opened the way to minimally invasive recanalization of the obstructed vein through stent placement, thus drawing the attention on this therapeutic opportunity.
•
In this study, we performed a cost–effectiveness analysis comparing endovascular venous stenting procedure to SMT for patients with deep venous obstruction and leg ulcers from the Italian Healthcare Service perspective. Moreover, a BIA was undertaken considering different scenarios of increased utilization rates of venous stenting over SMT.
•
A Markov model was developed to project costs and QALYs associated to the considered strategies over 3 years. Proportions of ulcers healed and recurred were derived from published literature and combined with real-world data, while the consumption of healthcare resources was monetized through DRG tariffs or published figures.
•
According to in-patient or day-hospital (DH) settings, respectively, endovascular stenting can be considered a cost-effective (ICUR €12,388/QALY) or dominant option in comparison to SMT for the management of patients with deep venous obstruction and venous ulceration, over a time horizon of 3 years.
•
Compared with the current SMT scenario, increasing utilization rates of stenting over SMT from 0.5 to 5%, in the next 5 years, is expected to increase the total budget of about 39.5 million Euros in the scenario considering the in-patient setting for stenting. In case the DH setting is considered instead, the increasing use of stenting would allow savings of about 5.1 million Euros in the same period. The scenarios considering a more significant adoption of stenting (10 or 20% at 5 years) showed incremental costs for the NHS of 78.9–157.8 million Euros (in-patient setting for stenting), or savings of 10.2–20.4 million Euros (DH setting for stenting).
•
The present study supports the use of venous stenting in patients with deep venous obstruction and venous ulceration. Future studies comparing SMT to stenting will be able to increase the clinical body of evidence to confirm these conclusions.
Financial & competing interests disclosure
The present study was funded by Confindustria Dispositivi Medici Servizi Srl through an unrestricted grant to CERGAS, SDA Bocconi School of Management, Via Roentgen 1, 20136 Milan, Italy. No interferences by the funding provider occurred in carrying out the research project and in writing the manuscript for which the authors have sole responsibility. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.zip)
- Download
- 327.14 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Margolis DJ, Bilker W, Santanna J, Baumgarten M. Venous leg ulcer: incidence and prevalence in the elderly. J. Am. Acad. Dermatol. 46(3), 381–386 (2002).
• Provides background on epidemiology of venous leg ulcers.
2.
Wik HS, Ghanima W, Sandset PM, Kahn SR. Scoring systems for postthrombotic syndrome. Semin. Thromb. Hemost. 43(5), 500–504 (2017).
3.
Ten Cate-Hoek AJ. Prevention and treatment of the post-thrombotic syndrome. Res. Pract. Thromb. Haemost. 2(2), 209–219 (2018).
4.
Brandjes DP, Büller HR, Heijboer H et al. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet Lond. Engl. 349(9054), 759–762 (1997).
5.
Prandoni P, Lensing AWA, Prins MH et al. Below-knee elastic compression stockings to prevent the post-thrombotic syndrome: a randomized, controlled trial. Ann. Intern. Med. 141(4), 249–256 (2004).
6.
Aschwanden M, Jeanneret C, Koller MT, Thalhammer C, Bucher HC, Jaeger KA. Effect of prolonged treatment with compression stockings to prevent post-thrombotic sequelae: a randomized controlled trial. J. Vasc. Surg. 47(5), 1015–1021 (2008).
7.
Kahn SR, Shapiro S, Wells PS et al. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet Lond. Engl. 383(9920), 880–888 (2014).
8.
Amsler F, Willenberg T, Blättler W. In search of optimal compression therapy for venous leg ulcers: a meta-analysis of studies comparing diverse [corrected] bandages with specifically designed stockings. J. Vasc. Surg. 50(3), 668–674 (2009).
•• Provides rationale for treatment of venous leg ulcers.
9.
Raju S, Owen S, Neglen P. The clinical impact of iliac venous stents in the management of chronic venous insufficiency. J. Vasc. Surg. 35(1), 8–15 (2002).
•• Provides rationale for the use of stenting for chronic venous insufficiency.
10.
Sang H, Li X, Qian A, Meng Q. Outcome of endovascular treatment in postthrombotic syndrome. Ann. Vasc. Surg. 28(6), 1493–1500 (2014).
11.
Tarricone R, Torbica A, Drummond M. MedtecHTA Project Group. Key recommendations from the MedtecHTA project. Health Econ. 26(Suppl. 1), 145–152 (2017).
12.
Berger ML, Sox H, Willke RJ et al. Good practices for real-world data studies of treatment and/or comparative effectiveness: recommendations from the joint ISPOR-ISPE Special Task Force on real-world evidence in health care decision making. Pharmacoepidemiol. Drug Saf. 26(9), 1033–1039 (2017).
13.
Adderley U, Stubbs N. Stockings or bandages for leg-ulcer compression? Nurs. Times. 110(15), 19–20 (2014).
14.
Alden PB, Lips EM, Zimmerman KP et al. Chronic venous ulcer: minimally invasive treatment of superficial axial and perforator vein reflux speeds healing and reduces recurrence. Ann. Vasc. Surg. 27(1), 75–83 (2013).
15.
Dolibog P, Franek A, Taradaj J et al. A comparative clinical study on five types of compression therapy in patients with venous leg ulcers. Int. J. Med. Sci. 11(1), 34–43 (2014).
16.
O'Hare JL, Earnshaw JJ. Randomised clinical trial of foam sclerotherapy for patients with a venous leg ulcer. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 39(4), 495–499 (2010).
17.
Pham B, Harrison MB, Chen MH, Carley ME. Canadian Bandaging Trial Group. Cost–effectiveness of compression technologies for evidence-informed leg ulcer care: results from the Canadian Bandaging Trial. BMC Health Serv. Res. 12, 346 (2012).
18.
Szewczyk MT, Jawień A, Cierzniakowska K, Cwajda-Białasik J, Mościcka P. Comparison of the effectiveness of compression stockings and layer compression systems in venous ulceration treatment. Arch. Med. Sci. AMS. 6(5), 793–799 (2010).
19.
Taradaj J, Franek A, Brzezinska-Wcislo L, Blaszczak E, Polak A. Randomized trial of medical compression stockings versus two-layer short-stretch bandaging in the management of venous leg ulcers. Phlebologie 38(4), 157–163 (2009).
20.
Yin M, Shi H, Ye K et al. Clinical assessment of endovascular stenting compared with compression therapy alone in post-thrombotic patients with iliofemoral obstruction. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 50(1), 101–107 (2015).
21.
Black S, Gwozdz A, Karunanithy N et al. Two year outcome after chronic iliac vein occlusion recanalisation using the Vici Venous Stent®. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 56(5), 710–718 (2018).
22.
Blanch Alerany M, Izquierdo Lamoca LM, Ramirez Ortega M, Lago Rivas I, Zotta Desboeufs R, Stefanov Kiuri S. Endovascular treatment of iliofemoral chronic post-thrombotic venous flow obstruction. J. Vasc. Surg. Venous Lymphat. Disord. 2(1), 2–7 (2014).
23.
de Wolf MaF, de Graaf R, Kurstjens RLM, Penninx S, Jalaie H, Wittens CHA. Short-term clinical experience with a dedicated venous nitinol stent: initial results with the sinus-venous stent. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 50(4), 518–526 (2015).
24.
George R, Verma H, Ram B, Tripathi R. The effect of deep venous stenting on healing of lower limb venous ulcers. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 48(3), 330–336 (2014).
25.
Hartung O, Loundou AD, Barthelemy P, Arnoux D, Boufi M, Alimi YS. Endovascular management of chronic disabling ilio-caval obstructive lesions: long-term results. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 38(1), 118–124 (2009).
26.
Khafagy T, Regal S, Fahmy D. Iliofemoral stenting for chronic venous occlusive disease: initial and mid-term outcomes in single institution. Egypt. J. Radiol. Nucl. Med. 47(4), (2016). https://cyberleninka.org/article/n/685010
27.
Kurklinsky AK, Bjarnason H, Friese JL et al. Outcomes of venoplasty with stent placement for chronic thrombosis of the iliac and femoral veins: single-center experience. J. Vasc. Interv. Radiol. JVIR. 23(8), 1009–1015 (2012).
28.
Lichtenberg MKW, de Graaf R, Stahlhoff WF, Özkapi A, Rassaf T, Breuckmann F. Venovo venous stent in the treatment of nonthrombotic or post-thrombotic iliac vein lesions – short-term results from the Arnsberg venous registry. VASA Z. Gefasskrankheiten. 48(2), 175–180 (2019).
29.
Liu Z, Gao N, Shen L et al. Endovascular treatment for symptomatic iliac vein compression syndrome: a prospective consecutive series of 48 patients. Ann. Vasc. Surg. 28(3), 695–704 (2014).
30.
Nayak L, Hildebolt CF, Vedantham S. Postthrombotic syndrome: feasibility of a strategy of imaging-guided endovascular intervention. J. Vasc. Interv. Radiol. JVIR. 23(9), 1165–1173 (2012).
31.
Raju S, Neglén P. Percutaneous recanalization of total occlusions of the iliac vein. J. Vasc. Surg. 50(2), 360–368 (2009).
32.
Rollo JC, Farley SM, Jimenez JC, Woo K, Lawrence PF, DeRubertis BG. Contemporary outcomes of elective iliocaval and infrainguinal venous intervention for post-thrombotic chronic venous occlusive disease. J. Vasc. Surg. Venous Lymphat. Disord. 5(6), 789–799 (2017).
33.
Rosales A, Sandbaek G, Jørgensen JJ. Stenting for chronic post-thrombotic vena cava and iliofemoral venous occlusions: mid-term patency and clinical outcome. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 40(2), 234–240 (2010).
34.
Sarici IS, Yanar F, Agcaoglu O et al. Our early experience with iliofemoral vein stenting in patients with post-thrombotic syndrome. Phlebology 29(5), 298–303 (2014).
35.
Stuck AK, Reich T, Engelberger RP, Sebastian T, Kucher N. Endovascular treatment of post-thrombotic and nonthrombotic iliofemoral venous outflow obstructions with self-expanding nitinol stents. VASA Z. Gefasskrankheiten. 47(4), 319–325 (2018).
36.
Tosenovsky P. One-year results of iliocaval stenting. Ann. Vasc. Surg. 59, 208–216 (2019).
37.
Ye K, Lu X, Jiang M et al. Technical details and clinical outcomes of transpopliteal venous stent placement for postthrombotic chronic total occlusion of the iliofemoral vein. J. Vasc. Interv. Radiol. JVIR. 25(6), 925–932 (2014).
38.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 50(6), 683–691 (1997).
39.
Introduction to Meta-Analysis. Wiley Online Books (2009). https://onlinelibrary.wiley.com/doi/book/10.1002/9780470743386
40.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 327(7414), 557–560 (2003).
41.
Husereau D, Drummond M, Petrou S et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)–explanation and elaboration: a report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health J. Int. Soc. Pharmacoeconomics Outcomes Res. 16(2), 231–250 (2013).
42.
PE Guidelines Around The World: Italy. https://tools.ispor.org/PEguidelines/countrydet.asp?c=13&t=4
43.
Cheng Q, Gibb M, Graves N, Finlayson K, Pacella RE. cost–effectiveness analysis of guideline-based optimal care for venous leg ulcers in Australia. BMC Health Serv. Res. 18(1), 421 (2018).
44.
Mosti G, Mattaliano V, Polignano R, Masina M. Compression therapy in the treatment of leg ulcers. Acta-Vulnologica 7(3), 113–135 (2009).
• Provides Italian costs of compression therapy.
45.
Guest JF, Fuller GW, Vowden P. Venous leg ulcer management in clinical practice in the UK: costs and outcomes. Int. Wound J. 15(1), 29–37 (2018).
46.
Clegg JP, Guest JF. Modelling the cost-utility of bio-electric stimulation therapy compared to standard care in the treatment of elderly patients with chronic non-healing wounds in the UK. Curr. Med. Res. Opin. 23(4), 871–883 (2007).
47.
Tavole di mortalità (2019). http://dati.istat.it/Index.aspx?DataSetCode=DCIS_MORTALITA1
48.
Sullivan SD, Mauskopf JA, Augustovski F et al. Budget impact analysis-principles of good practice: report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health J. Int. Soc. Pharmacoeconomics Outcomes Res. 17(1), 5–14 (2014).
49.
Briggs AH, O'Brien BJ, Blackhouse G. Thinking outside the box: recent advances in the analysis and presentation of uncertainty in cost–effectiveness studies. Annu. Rev. Public Health 23, 377–401 (2002).
50.
Evans CJ, Fowkes FG, Ruckley CV, Lee AJ. Prevalence of varicose veins and chronic venous insufficiency in men and women in the general population: Edinburgh Vein Study. J. Epidemiol. Community Health. 53(3), 149–153 (1999).
51.
Hartung O, Otero A, Boufi M et al. Mid-term results of endovascular treatment for symptomatic chronic nonmalignant iliocaval venous occlusive disease. J. Vasc. Surg. 42(6), 1138–1144 (2005).
52.
Guest JF, Fuller GW, Vowden P. Clinical outcomes and cost–effectiveness of three different compression systems in newly-diagnosed venous leg ulcers in the UK. J. Wound Care. 26(5), 244–254 (2017).
53.
Ashby RL, Gabe R, Ali S et al. Clinical and cost–effectiveness of compression hosiery versus compression bandages in treatment of venous leg ulcers (Venous leg Ulcer Study IV, VenUS IV): a randomised controlled trial. Lancet Lond. Engl. 383(9920), 871–879 (2014).
54.
Tangney E, O'Donnell T, Iafrati M. Cost and benefit analysis of stenting versus compression therapy for patients with chronic total venous occlusion. J. Vasc. Surg. Venous Lymphat. Disord. 4(1), 137 (2016).
•• Provides a cost–benefit analysis comparing stenting versus compression therapy.
55.
Health equipment – Hospital beds – OECD Data (2019). http://data.oecd.org/healtheqt/hospital-beds.htm
56.
Gordon L, Edwards H, Courtney M, Finlayson K, Shuter P, Lindsay E. A cost–effectiveness analysis of two community models of care for patients with venous leg ulcers. J. Wound Care. 15(8), 348–353 (2006).
57.
Blüher M, Saunders SJ, Mittard V, Torrejon Torres R, Davis JA, Saunders R. Critical Review of European Health-Economic Guidelines for the Health Technology Assessment of Medical Devices. Front. Med. 6 (2019). /
58.
Gianesini S, Obi A, Onida S et al. Global guidelines trends and controversies in lower limb venous and lymphatic disease: narrative literature revision and experts’ opinions following the vWINter international meeting in Phlebology, Lymphology & Aesthetics, 23–25 January 2019. Phlebology 34(Suppl. 1), 4–66 (2019).
59.
Franks PJ, Barker J, Collier M et al. Management of patients with venous leg ulcers: challenges and current best practice. J. Wound Care. 25(Suppl. 6), S1–S67 (2016).
Information & Authors
Information
Published In
Pages: 705 - 720
PubMed: 32686480
Copyright
© 2020 Carla Rognoni. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 13 February 2020
Accepted: 19 May 2020
Published online: 20 July 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Venous stenting for patients with outflow obstruction and leg ulcers: cost–effectiveness and budget impact analyses. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0030
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jennifer Benner, Roy Arguello, Peter Pappas, Mark Meissner, Kush Desai, Josh Epstein, Cost-effectiveness of a prosthetic venous valve versus compression therapies and wound care for treatment of infra-inguinal deep vein reflux, Journal of Vascular Surgery: Venous and Lymphatic Disorders, 10.1016/j.jvsv.2026.102565, 14, 6, (102565), (2026).
- S.G. Gavrilov, A.V. Vasilyev, S.V. Chubchenko, Economic Aspects of Endovascular Treatment of Pelvic Venous Disorders, Journal of Venous Disorders, 10.17116/flebo20262001116, 20, 1, (16), (2026).
- Marzia Lugli, Oscar Maleti, Endovascular Treatment for Venous Obstructions, VAS European Book on Angiology/Vascular Medicine, 10.1007/978-3-031-82232-2_75, (905-912), (2026).
- Oscar Maleti, Marzia Lugli, Deep Venous Valve Reconstruction Indications and Results, VAS European Book on Angiology/Vascular Medicine, 10.1007/978-3-031-82232-2_64, (757-765), (2026).
- Anthony Teta, Jay Mohan, Vincent Varghese, Jon C. George, Jacqueline Powers, Ehrin J. Armstrong, Yulanka Castro-Dominguez, Iliofemoral Acute Deep Venous Thrombosis, Chronic Deep Venous Thrombosis, and May-Thurner Syndrome, Interventional Cardiology Clinics, 10.1016/j.iccl.2024.11.014, 14, 2, (297-310), (2025).
- Dwayne Boyers, Moira Cruickshank, Lorna Aucott, Charlotte Kennedy, Paul Manson, Paul Bachoo, Miriam Brazzelli, Automated devices for identifying peripheral arterial disease in people with leg ulceration: an evidence synthesis and cost-effectiveness analysis, Health Technology Assessment, 10.3310/TWCG3912, (1-158), (2024).
- Kush R. Desai, Saher S. Sabri, Steve Elias, Paul J. Gagne, Mark J. Garcia, Kathleen Gibson, Misaki M. Kiguchi, Santhosh J. Mathews, Erin H. Murphy, Eric A. Secemsky, Windsor Ting, Raghu Kolluri, Consensus Statement on the Management of Nonthrombotic Iliac Vein Lesions From the VIVA Foundation, the American Venous Forum, and the American Vein and Lymphatic Society, Circulation: Cardiovascular Interventions, 10.1161/CIRCINTERVENTIONS.124.014160, 17, 8, (2024).
- Oscar Maleti, Massimiliano Orso, Marzia Lugli, Michel Perrin, Systematic review and meta-analysis of deep venous reflux correction in chronic venous insufficiency, Journal of Vascular Surgery: Venous and Lymphatic Disorders, 10.1016/j.jvsv.2023.07.003, 11, 6, (1265-1275.e5), (2023).
- Tina Moon, Thomas F O’Donnell, Derek Weycker, Mark Iafrati, Impact of lymphedema in the management of venous leg ulcers, Phlebology: The Journal of Venous Disease, 10.1177/02683555231197597, 38, 9, (613-621), (2023).
- Carla Rognoni, Alessandro Furnari, Marzia Lugli, Oscar Maleti, Alessandro Greco, Rosanna Tarricone, Time-Driven Activity-Based Costing for Capturing the Complexity of Healthcare Processes: The Case of Deep Vein Thrombosis and Leg Ulcers, International Journal of Environmental Research and Public Health, 10.3390/ijerph20105817, 20, 10, (5817), (2023).