Comparative safety and efficacy of ozanimod versus fingolimod for relapsing multiple sclerosis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Ozanimod and fingolimod are sphingosine 1-phosphate receptor–modulating therapies for relapsing multiple sclerosis. Patients & methods: Comparative effectiveness was assessed by matching adjusted indirect comparisons of safety and efficacy trial outcomes at first-dose cardiac monitoring, 1 year and 2 years. Results: After adjustment, baseline characteristics were similar. Ozanimod was associated with a lower risk of extended first-dose monitoring, conduction abnormalities including atrioventricular block. One-year risks of any adverse event (AE), mean lymphocyte count reductions and abnormal liver enzymes were lower with ozanimod. Two-year risks of AEs leading to discontinuation, any AEs, herpetic infections, bradycardia and abnormal liver enzymes were lower with ozanimod. Analyses of efficacy outcomes were similar. Conclusion: Ozanimod appears to have a favorable benefit-risk profile versus fingolimod.
Multiple sclerosis (MS) is a chronic autoimmune and neurodegenerative disease of the central nervous system. It is characterized by inflammation, demyelination, neuronal and oligodendrocyte loss, disruption of the blood–brain barrier, as well as debilitating symptoms such as fatigue, depressive symptoms and cognitive impairment [1,2]. MS may present as a clinically isolated syndrome, relapsing MS (RMS), secondary progressive MS or primary progressive MS [3,4]. RMS, the most prevalent type of MS, is characterized by episodes of relapses followed by a remission period. Approximately 85% of individuals with MS present with RMS [5]. Complete physical recovery from relapse can occur, but approximately 50% of relapses are associated with residual neurological deficits resulting in a sustained increase in disability [6], typically measured in Phase III MS trials using the Expanded Disability Status Scale (EDSS) [7,8]. MS often has a highly debilitating impact on quality of life for individuals and their families [9], and is associated with considerable economic burden [10].
Currently, MS has no cure, but treatment options exist. Anti-inflammatory agents, such as corticosteroids, are used as symptomatic treatment during acute relapses. Disease-modifying therapies (DMTs), such as immunomodulators, are used to alter the disease course by reducing relapses, with the goal of preventing or slowing long-term disability [11–14]. Fingolimod is a nonselective sphingosine 1-phosphate (S1P) receptor modulator that binds to the receptor subtypes S1PR1, S1PR3, S1PR4 and S1PR5, and was the first oral DMT approved (US, 2010; EU, 2011) for the treatment of RMS. However, fingolimod may be associated with cardiovascular, ophthalmologic, pulmonary and hepatic safety concerns, as listed in its drug label [15]. Ozanimod is an investigational oral DMT and a selective S1P receptor modulator designed to target only the receptor subtypes S1PR1 and S1PR5 [16]; it is currently under review by regulatory agencies for the treatment of RMS. The clinical efficacy, safety and tolerability of ozanimod for the treatment of patients with RMS have been demonstrated in the Phase III RADIANCE [17] and SUNBEAM [18] clinical trials.
The comparative efficacy of these two S1P receptor–modulating agents in the treatment of RMS has not yet been fully characterized. In the absence of a head-to-head randomized trial between ozanimod and fingolimod, the current study was designed to indirectly compare the key safety and efficacy outcomes between these two therapies for the treatment of patients with RMS using a matching-adjusted indirect comparison (MAIC) [19,20] to adjust for cross-trial differences in patient data from their pivotal clinical trials. The outcomes assessed in this analysis include first-dose cardiac monitoring outcomes as well as 1-year and 2-year safety and efficacy outcomes.
MAIC methodology was recently used to compare delayed-release dimethyl fumarate and fingolimod for the treatment of patients with RMS [21]. Results showed that the efficacy of dimethyl fumarate was similar to that of fingolimod on clinical measures of relapse and disability progression [21]. In addition, MAIC methodology was recently used to assess the comparative efficacy of cladribine versus alemtuzumab in adults with RMS [22]. Results of that study showed that the efficacy of cladribine was comparable to alemtuzumab in the treatment of patients with RMS based on 6-month confirmed disability progression (CDP) and annualized relapse rates (ARRs) [22].
Patients & methods
Data source
Individual patient data from the RADIANCE-B (NCT02047734 [RPC01-201B]) [23] and SUNBEAM (NCT02294058 [RPC01-301]) [24,25] ozanimod trials were used in this analysis. RADIANCE-B was a randomized, IFN β-1a–controlled, Phase III trial of ozanimod in patients with RMS. Eligible participants were randomly assigned in a 1:1:1 ratio to ozanimod HCI (daily oral 0.5 or 1 mg) or IFN β-1a for 2 years. The trial enrolled 1313 patients with RMS. SUNBEAM was also a randomized (1:1:1 ratio), controlled study of ozanimod HCI (0.5 and 1 mg) versus IFN β-1a in patients with RMS over a minimum 12-month period. The study enrolled 1346 patients with RMS. To attenuate potential first-dose cardiac effects with ozanimod HCI, in both trials, a dose-escalation regimen was applied for all participants, consisting of 0.25 mg on days 1–4, 0.5 mg on days 5–7 and then the assigned dose of 0.5 or 1 mg from day 8 through week 24.
In addition, the published summary-level data from the TRANSFORMS (NCT00340834 [D2302]) [26], FREEDOMS (NCT00289978 [D2301]) [27] and FREEDOMS II (NCT00355134 [D2309]) [28] fingolimod Phase III trials were used, along with pooled safety data from the TRANSFORMS, FREEDOMS and FREEDOMS II trials [29], as well as the trial data reported in clinicaltrials.gov. TRANSFORMS was a randomized, IFN β-1a–controlled, Phase III trial of fingolimod in patients with RMS. Eligible participants were randomly assigned in a 1:1:1 ratio to fingolimod (oral 0.5 or 1.25 mg) or IFN β-1a for 1 year. The trial enrolled 1292 patients with RMS. FREEDOMS I and FREEDOMS II were two randomized, placebo-controlled, Phase III trials of fingolimod in patients with RMS. Eligible participants were randomly assigned in a 1:1:1 ratio to fingolimod (oral 0.5 or 1.25 mg) or placebo for 2 years. The trials enrolled 1292 and 1083 patients with RMS, respectively. Only the approved and recommended dose of fingolimod 0.5 mg was considered for these analyses. No institutional review was required as this was a post hoc analysis of previously published, de-identified data.
Inclusion criteria
For the ozanimod trials, patients were required to be 18–55 years of age; have a diagnosis of RMS, as defined by the 2010 revised McDonald criteria [30]; have had at least one documented relapse in the previous year before screening (or prior 2 years with at least one gadolinium-enhancing lesion); and have a score between 0.0 and 5.0 on the EDSS [31]. In the fingolimod trials, patients were required to be 18–55 years of age; have a diagnosis of RMS, as defined by the 2005 revised McDonald criteria [30]; have had at least one confirmed relapse during the preceding 1 year (or at least two during the preceding 2 years); and have a score between 0.0 and 5.5 on the EDSS.
Study outcomes
Outcomes assessed at the first-dose cardiac monitoring included heart rate, electrocardiographic findings and change in blood pressure (BP) from baseline and whether patients received extended monitoring after 6 h, received Day 2 monitoring, or discontinued treatment on Day 1.
Safety and efficacy outcomes assessed at 1 and 2 years included adverse events (AEs), AEs leading to discontinuation, any serious AE, patient death, liver enzymes (alanine aminotransferase) at least three-times the upper limit of normal, macular edema, absolute lymphocyte count, lymphocyte count <0.2 K/μl, ARR and 3-month and 6-month confirmed CDP. Because data for the 6-month CDP at 1 year was not reported in the fingolimod trial, a comparison between ozanimod and fingolimod on this outcome was not feasible.
Comparisons of first-dose cardiac monitoring outcomes
Both ozanimod HCI doses (0.5 and 1 mg) from RADIANCE-B and SUNBEAM were pooled because the initial dose of ozanimod on Day 1 in both studies for both dose groups was 0.25 mg, according to identical protocol-specified dose escalation regimens [17,18]. Each fingolimod treatment group was pooled across the TRANSFORMS, FREEDOMS and FREEDOMS II studies. Before and after matching, baseline patient characteristics and selected outcomes were described and compared for the pooled ozanimod doses versus fingolimod (0.5 mg dose).
Comparisons of 1-year outcomes
Both of the ozanimod HCI 1 mg dose groups from RADIANCE-B and SUNBEAM were pooled. The ozanimod clinical trials and the TRANSFORMS trial all included a randomized comparison to IFN β-1a intramuscular (Avonex). An anchor-based comparison was conducted for 1-year safety and efficacy outcomes using the IFN β-1a arm as an anchor. Before and after matching, baseline patient characteristics and selected outcomes were described and compared for (1) the pooled IFN β-1a arms from the ozanimod trials (RADIANCE-B and SUNBEAM) versus IFN β-1a arm from the fingolimod trial (TRANSFORMS), to assess the consistency of outcomes before and after matching; and (2) the pooled ozanimod HCI 1 mg arms (RADIANCE-B and SUNBEAM) versus the fingolimod 0.5 mg arm (TRANSFORMS), with the comparison anchored on IFN β-1a.
Comparisons of 2-year outcomes
The patient group receiving ozanimod HCI 1 mg was obtained from RADIANCE-B. The fingolimod groups were pooled across the FREEDOMS and FREEDOMS II studies. Before and after matching, baseline patient characteristics and selected outcomes were described and compared for the ozanimod HCI 1 mg arm (RADIANCE-B) versus the pooled fingolimod 0.5 mg arms (FREEDOMS and FREEDOMS II). Because of a lack of data at 2 years comparing fingolimod versus IFN β-1a, the comparisons of 2-year outcomes were nonanchored.
Assessment of cross-trial similarities & differences
The trial designs included in this post hoc analysis were determined to be highly similar and suitable for an adjusted cross-trial comparison. Patients in all trials were 18–55 years of age and discontinued prior treatment (e.g., IFN β, glatiramer acetate and other DMTs) before randomization. For the first-dose cardiac monitoring assessment, all patients had hourly assessments of heart rate and BP available, and the duration of assessment was ≥6 h. In addition, the definitions of and assessment methodologies for relapse were similar across trials.
Several differences between the trials existed. An RMS diagnosis was based on the 2010 revised McDonald criteria in the ozanimod trials and on the 2005 revised McDonald criteria in the fingolimod trials [30]. The ozanimod trials required either one documented relapse in the prior year or one in the prior 2 years along with gadolinium-enhancing lesions, whereas the fingolimod trials required either one confirmed relapse during the prior year or at least two during the prior 2 years. The upper threshold for the EDSS score for inclusion in the ozanimod trials was 5.0, whereas the upper threshold was a score of 5.5 in the fingolimod trials. Heart rate and BP were measured hourly for the first 6 h after the first dose in both trials; however, the ozanimod trials measured patients in the supine position (as well as the standing position), whereas the fingolimod trials measured patients in the sitting position. Other differences between the trials included their time periods and geography. The ozanimod trials were multinational, conducted between 2013 and 2017, and included higher proportions of patients from Eastern Europe (∼90%) than the fingolimod trials (∼2%), which were also multinational but were conducted between 2006 and 2011.
Statistical methods
MAIC methodology was used to adjust for baseline patient differences for each treatment comparison and outcome period [19,20]. Individual patients in the ozanimod trials were assigned weights such that weighted mean baseline patient characteristics in the ozanimod trials exactly matched those reported for the fingolimod trials. Patients’ weights were equal to their estimated odds of enrollment in an ozanimod trial versus a fingolimod trial, conditional on enrollment within either of the trial populations.
A logistic regression model using the method of moments [20] was used to estimate the weights for the propensity of enrollment in the ozanimod trials versus the fingolimod trials. Based on data availability and clinical considerations, all MAICs adjusted for cross-trial differences in the following baseline characteristics: age (mean), sex (proportion who were female), duration of MS since first symptom (mean), relapses within previous year (mean), relapses within previous 2 years (mean), EDSS score (mean), prior DMTs (percentage) and absence of gadolinium-enhancing lesions (percentage). For first-dose monitoring outcomes, resting heart rate (mean), cardiac disorders (percentage) and any conduction abnormality (percentage) were also adjusted for cross-trial differences. In addition, for 1-year outcomes, lymphocyte count at baseline was adjusted for cross-trial differences.
Baseline patient characteristics (i.e., demographic and clinical characteristics) before and after matching were compared between the ozanimod and fingolimod groups. Means and standard deviations were reported for continuous variables; frequencies and percentages were reported for categorical variables. Comparisons of binary variables before matching were conducted via χ2 tests, and Wald tests were used for the comparisons of binary variables after matching and the comparisons of continuous variables both before and after matching. A p-value of 0.05 was used to determine statistical significance.
Results
Baseline characteristics before & after matching
Before MAIC adjustment, some of the clinically relevant differences between patients receiving ozanimod (N = 1773) compared with those receiving fingolimod (N = 1212) included shorter MS duration (6.8 vs 8.5 years, respectively) and lower likelihood of prior DMT use (29.0 vs 56.4%) (Supplementary Table 1). After adjustment, baseline averages for all included patient characteristics were balanced between the ozanimod and fingolimod trials. The anchor-based and nonanchor-based comparisons of the 1-year safety outcomes are listed in Table 1 and Supplementary Table 2, respectively.
| Characteristic | Before matching | p-value: [A] vs [C] | p-value: [B] vs [D] | After matching | p-value: [A] vs [C] | p-value: [B] vs [D] | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RADIANCE-B (RPC01-201B) and SUNBEAM (RPC01-301) | TRANSFORMS (D2302) | RADIANCE-B (RPC01-201B) and SUNBEAM (RPC01-301) | TRANSFORMS (D2302) | |||||||||
| Ozanimod HCI 1 mg (N = 882) [A] | IFN β-1a (N = 885) [B] | Fingolimod 0.5 mg (N = 429) [C] | IFN β-1a (N = 431) [D] | Ozanimod HCI 1 mg (ESS = 276) [A] | IFN β-1a (ESS = 317) [B] | Fingolimod 0.5 mg (N = 429) [C] | IFN β-1a (N = 431) [D] | |||||
| Age, mean (SD), years | 35.4 (9.1) | 35.6 (9.1) | 36.7 (8.8) | 36.0 (8.3) | <0.05‡ | 0.41 | 36.7 (9.2) | 36.0 (9.4) | 36.7 (8.8) | 36.0 (8.3) | 1.0 | 1.0 |
| Female, n (%) | 576 (65.3) | 602 (68.0) | 281 (65.4) | 292 (67.8) | 0.99 | 0.97 | 65.4 | 67.8 | 65.4 | 67.8 | 1.0 | 1.0 |
| Duration of MS since first symptom, mean (SD), years | 6.9 (6.3) | 6.6 (6.0) | 7.5 (6.2) | 7.4 (6.3) | 0.1 | <0.05‡ | 7.5 (6.5) | 7.4 (6.4) | 7.5 (6.2) | 7.4 (6.3) | 1.0 | 1.0 |
| Relapses within previous year, mean (SD) | 1.3 (0.6) | 1.3 (0.6) | 1.5 (1.2) | 1.5 (0.8) | <0.001‡ | <0.001‡ | 1.5 (0.7) | 1.5 (0.7) | 1.5 (1.2) | 1.5 (0.8) | 1.0 | 1.0 |
| Relapses within previous 2 years, mean (SD) | 1.7 (0.8) | 1.7 (0.9) | 2.3 (2.2) | 2.3 (1.2) | <0.001‡ | <0.001‡ | 2.3 (1.2) | 2.3 (1.2) | 2.3 (2.2) | 2.3 (1.2) | 1.0 | 1.0 |
| EDSS score, mean (SD) | 2.6 (1.2) | 2.6 (1.2) | 2.2 (1.3) | 2.2 (1.3) | <0.001‡ | <0.001‡ | 2.2 (1.1) | 2.2 (1.1) | 2.2 (1.3) | 2.2 (1.3) | 1.0 | 1.0 |
| Patients with prior DMTs, n (%) | 252 (28.6) | 276 (31.2) | 237 (55.2) | 243 (56.3) | <0.001‡ | <0.001‡ | 55.2 | 56.3 | 55.2 | 56.3 | 1.0 | 1.0 |
| Absence of Gd-enhancing lesions, n (%) | 488 (55.3) | 475 (53.7) | 289 (67.4) | 272 (63.1) | <0.001‡ | <0.01‡ | 67.4 | 63.1 | 67.4 | 63.1 | 1.0 | 1.0 |
| Lymphocyte count at baseline, mean (SD), K/μl | 1.8 (0.6) | 1.9 (0.6) | 1.8 (0.5) | 1.7 (0.5) | 0.2 | <0.001‡ | 1.8 (0.6) | 1.7 (0.5) | 1.8 (0.5) | 1.7 (0.5) | 1.0 | 1.0 |
†
For this analysis, the fingolimod and IFN β-1a arms from the TRANSFORMS trial (Cohen et al. [26]) were compared to the pooled ozanimod HCI 1 mg and IFN β-1a arms from the RADIANCE-B and SUNBEAM clinical trials.
‡
Denotes a statistically significant difference.
DMTs: Disease-modifying therapy; EDSS: Expanded disability status scale; ESS: Effective sample size; Gd: Gadolinium; MS: Multiple sclerosis; SD: Standard deviation.
Adjusted analyses of first-dose cardiac monitoring outcomes
Compared with ozanimod, the adjusted absolute increases in the percentages of patients whose lowest hourly recorded heart rate was <45 bpm (45–54 bpm) in the first 6 h were +1.4% (+12.1%) for fingolimod 0.5 mg (p < 0.001) (Table 2), indicating that the adjusted risk difference (RD) was more favorable for ozanimod.
| Outcome | Adjusted risk difference for ozanimod HCI 1 mg vs fingolimod 0.5 mg | ||
|---|---|---|---|
| Δ‡ | 95% CI | p-value | |
| Heart rate, bpm | |||
| – <45 | −1.4 | (−2.0, −0.7) | <0.001¶ |
| – 45–54 | −12.1 | (−14.7, −9.5) | <0.001¶ |
| – 55–64 | −3.5 | (−7.9, 0.9) | 0.12 |
| – ≥65 | 17.2 | (13.0, 21.3) | <0.001¶ |
| Decrease in heart rate (bpm) from baseline, hour 5§ | 6.6 | (5.8, 7.5) | <0.001¶ |
| Decrease in heart rate (bpm) from baseline, hour 6§ | 7.5 | (6.7, 8.3) | <0.001¶ |
| ECG findings | |||
| – Any conduction abnormality | −3.5 | (−5.3, −1.8) | <0.001¶ |
| – Atrioventricular block | |||
| – First-degree atrioventricular block | −3.0 | (−4.4, −1.7) | <0.001¶ |
| – Second-degree atrioventricular block (Wenckebach/Mobitz type I, Mobitz type II, 2:1) | −0.2 | (−0.5, 0.1) | 0.12 |
| Received extended monitoring beyond 6 hours | −8.3 | (−10.6, −6.0) | <0.001¶ |
| Received Day 2 monitoring | −2.6 | (−3.5, −1.7) | <0.001¶ |
| Discontinued on Day 1 | 0.1 | (−0.3, 0.4) | 0.72 |
| BP, mmHg | |||
| – Change in mean sitting systolic BP | 2.2 | (1.3, 3.1) | <0.001¶ |
| – Change in mean sitting diastolic BP | 5.0 | (4.3, 5.7) | <0.001¶ |
†
First-dose cardiac monitoring outcomes for both fingolimod arms were extracted from the pooled analysis reported in DiMarco et al. [29]. Patient characteristics for ozanimod were extracted from the patient-level data from the RADIANCE-B and SUNBEAM trials; data for the 0.5 mg arm and the 1 mg arm were pooled for this analysis.
‡
Δ represents the change in risk between the two arms.
§
Decrease in heart rate from baseline to nadir for both fingolimod arms was compared with decrease in heart rate from baseline to hours 5 and 6 for ozanimod. Hour 5 represents the nadir for ozanimod, whereas hour 6 represents the end of the monitoring period.
¶
Denotes a statistically significant difference.
BP: Blood pressure; bpm: Beats per minute; ECG: Electrocardiogram; SD: Standard deviation.
The rates of the studied safety outcomes during first-dose cardiac monitoring were generally lower with ozanimod than with fingolimod. Compared with fingolimod, ozanimod was associated with significantly lower rates of conduction abnormalities (RD: −3.5%) and first-degree atrioventricular block (RD: −3.0%), as well as a lower risk of requiring monitoring beyond 6 h (RD −8.3%) and of requiring Day 2 monitoring (RD −2.6%; all p < 0.001) (Figure 1 & Table 2). Ozanimod was associated with significantly less reduction in systolic (difference in means: 2.2 mm Hg) and diastolic (difference in means: 5.0 mm Hg) BP compared with fingolimod at first dose (both p < 0.001) (Table 2).
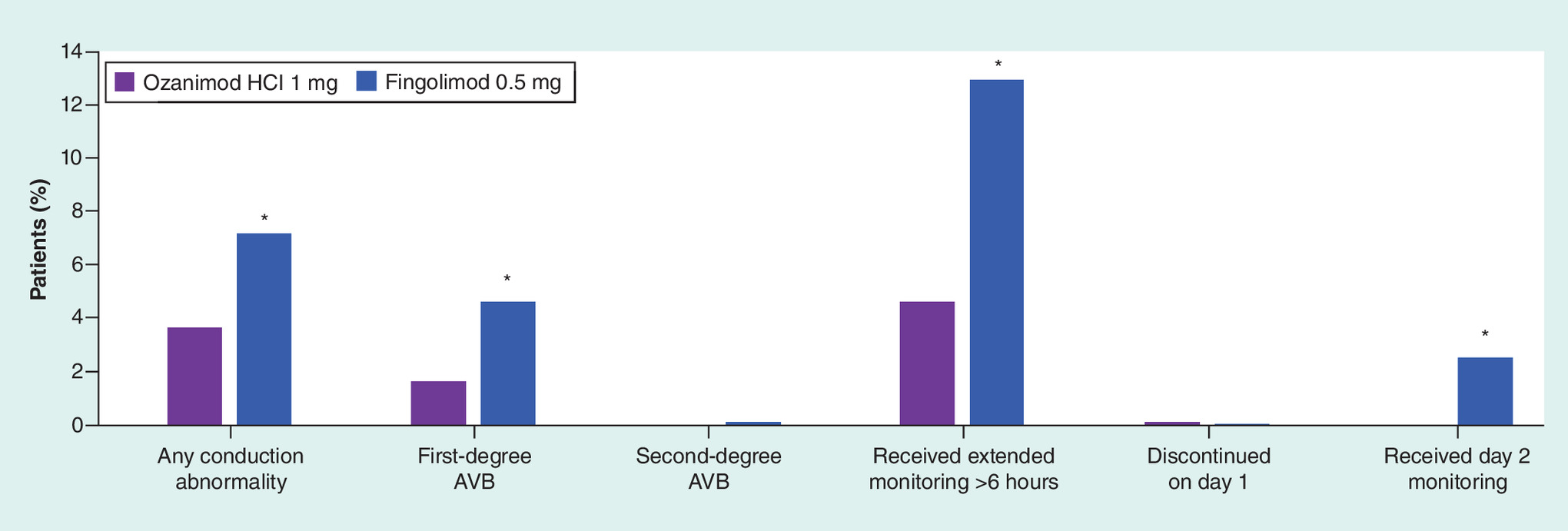
Figure 1. First-dose monitoring outcomes for ozanimod HCI 1 mg versus fingolimod 0.5 mg after baseline adjustment.
*p < 0.05 vs ozanimod.
AVB: Atrioventricular block.
Adjusted analyses of 1-year outcomes
After adjustment for baseline patient characteristics, ozanimod was associated with a significantly lower risk of any AEs (RD: −9.9%), higher absolute mean lymphocyte count (difference in means: 0.4 × 109/l) and lower risk of abnormal liver enzyme (alanine aminotransferase) elevations (alanine aminotransferase ≧3x upper limit of normal; RD: −6.8%) compared with fingolimod (all p < 0.05) (Table 3). No significant differences were observed in ARRs between the two groups (ARR ratio: 1.08; p = 0.80), and similar proportions of patients were free of 3-month CDP (difference in proportions: 1.1%; p = 0.72). A comparison between ozanimod and fingolimod for 6-month CDP at 1 year was not feasible as data were not reported in the fingolimod trial.
| Outcome | Adjusted risk difference for ozanimod HCI 1 mg vs fingolimod 0.5 mg | ||
|---|---|---|---|
| Δ† | 95% CI | p-value | |
| AE leading to discontinuation (%) | −1.2 | (−5.7, 3.3) | 0.61 |
| Death (%) | 0.0 | (0.0, 0.0) | – |
| Any AE (%) | −9.9 | (−18.0, −1.8) | <0.05¶ |
| – Herpesvirus infection | 2.2 | (−1.6, 6.0) | 0.25 |
| – Depression | 3.1 | (−0.9, 7.1) | 0.13 |
| Any SAE (%) | 0.4 | (−4.4, 5.3) | 0.86 |
| Infection SAE (%) | |||
| – Appendicitis | 0.6 | (−0.1, 1.2) | 0.1 |
| – Herpesvirus infection (serious) | 0.0 | (−0.6, 0.6) | 1.0 |
| Neoplasm SAE (%) | |||
| – Basal-cell carcinoma | −0.5 | (−1.4, 0.4) | 0.27 |
| – Melanoma (including in situ) | −0.7 | (−1.5, 0.1) | 0.08 |
| – Breast cancer (including in situ) | −0.5 | (−1.2, 0.2) | 0.14 |
| Cardiac SAE (%) | |||
| – Bradycardia or sinus bradycardia | −0.4 | (−1.1, 0.3) | 0.23 |
| – Atrioventricular block first degree | −0.2 | (−0.6, 0.2) | 0.35 |
| – Atrioventricular block second degree | −0.2 | (−0.6, 0.2) | 0.35 |
| – Myocardial infarction | −0.2 | (−0.5, 0.2) | 0.32 |
| Mean absolute lymphocyte count (109/l) at 1 year§ | 0.4 | (0.3, 0.5) | <0.001¶ |
| Absolute lymphocyte count <0.2 K/μl (%) | −13.8 | (−17.3, −10.3) | <0.001¶ |
| Liver enzymes: ALT ≥ 3x ULN (%) | −6.8 | (−10.6, −3.1) | <0.001¶ |
| Macular edema (%) | −0.3 | (−1.0, −0.5) | 0.50 |
| Annualized relapse rate‡ | 1.08 | (0.64, 1.82) | 0.78 |
| Proportion free of CDP, 3 months (%) | 1.1 | (−4.4, 6.5) | 0.72 |
†
Difference in the proportion of patients with events, unless otherwise noted.
‡
Annualized relapse rate ratios for ozanimod vs fingolimod.
§
Difference in means.
¶
Denotes a statistically significant difference.
AE: Adverse event; ALT: Alanine aminotransferase; CDP: Confirmed disability progression; SAE: Serious adverse event; ULN: Upper limit of normal.
Adjusted analyses of 2-year outcomes
After adjustment for baseline patient characteristics, ozanimod was associated with a significantly lower risk of any AE (RD: −22.7%), AEs leading to discontinuation (RD: −7.4%), herpetic infection (RD: −4.9%), basal-cell carcinoma (RD: −1.8%), bradycardia (−0.5%) and abnormal liver enzyme elevations (RD: −3.0%) compared with fingolimod (all p < 0.05) (Table 4). No significant differences were observed in ARRs between groups (ARR ratio: 1.06; p = 0.78). Similar proportions of patients in both groups were free of 3-month (difference in proportions: 5.2%; p = 0.12) and 6-month CDP (difference in proportions: 0.9%; p = 0.76).
| Outcome | Adjusted risk difference for ozanimod HCI 1 mg vs fingolimod 0.5 mg | ||
|---|---|---|---|
| Δ† | 95% CI | p-value | |
| AE leading to discontinuation (%) | −7.4 | (−12.3, −2.5) | <0.01¶ |
| Death (%) | 0.0 | (0.0, 0.1) | 0.34 |
| Any AE (%) | −22.7 | (−29.2, −16.2) | <0.001¶ |
| – Herpetic infection | −4.9 | (−8.9, −0.9) | <0.05¶ |
| – Depression | −2.7 | (−6.3, 0.9) | 0.15 |
| Any SAE (%) | −4.7 | (−9.8, 0.5) | 0.07 |
| Infection SAE (%) | |||
| – Appendicitis | −0.1 | (−0.6, 0.5) | 0.83 |
| – Herpesvirus infection (serious) | −0.3 | (−0.7, 0.1) | 0.12 |
| Neoplasm SAE (%) | |||
| – Basal-cell carcinoma | −1.8 | (−2.7, −0.9) | <0.001¶ |
| – Melanoma (including in situ) | −0.1 | (−0.3, 0.1) | 0.38 |
| – Breast cancer (including in situ) | 0 | (−0.3, 0.3) | 0.96 |
| Cardiac SAE (%) | |||
| – Bradycardia or sinus bradycardia | −0.5 | (−1.0, 0.0) | <0.05¶ |
| – Atrioventricular block first degree | 0 | (0.0, 0.0) | – |
| – Atrioventricular block second degree | 0 | (0.0, 0.0) | – |
| – Myocardial infarction | 0 | (0.0, 0.0) | – |
| Mean absolute lymphocyte count (109/l) at 1 year§ | 0.2 | (−,−) | – |
| Liver enzymes: ALT ≥ 3x ULN, % | −3.0 | (−5.8, −0.1) | <0.05¶ |
| Macular edema (%) | −0.4 | (−0.8, 0.0) | 0.08 |
| Annualized relapse rate‡ | 1.06 | (0.70, 1.62) | 0.78 |
| Proportion free of CDP, 3 months (%) | 5.2 | (−1.3, 11.7) | 0.12 |
| Proportion free of CDP, 6 months (%) | 0.9 | (−4.8, 6.7) | 0.76 |
†
Difference in the proportion of patients with events, unless otherwise noted.
‡
Annualized relapse rate ratios for ozanimod vs fingolimod.
§
Difference in means; standard errors were not reported for fingolimod and thus statistical comparison was not possible.
¶
Denotes a statistically significant difference.
AE: Adverse event; ALT: Alanine aminotransferase; CDP: Confirmed disability progression; SAE: Serious adverse event; ULN: Upper limit of normal.
Comparisons of risk outcomes based on odds ratios were consistent with the results described for RDs.
Discussion
Evidence on the comparative effectiveness of ozanimod and fingolimod in the treatment of RMS will be important for decision makers to assess the relative clinical value of these therapies. In the absence of head-to-head randomized trials of these treatments, indirect comparisons can provide valuable comparative evidence. This analysis used data from the pivotal clinical trials of ozanimod and fingolimod and adjusted for cross-trial differences in patient populations to assess the comparative efficacy of these therapies in RMS.
In this adjusted comparison, ozanimod was associated with a significantly lower risk of any AEs than fingolimod 0.5 mg. In addition, lower risks of heart rate reduction, any conduction abnormalities and atrioventricular block during first-dose monitoring were observed among patients receiving ozanimod, as well as a less frequent need for extended first-dose monitoring.
Ozanimod was also differentiated from fingolimod in the 1- and 2-year safety outcomes. Specifically, in the 1-year outcomes, patients receiving ozanimod had a lower risk of any AEs, lymphocyte count reductions and abnormal liver enzymes elevations than patients receiving fingolimod. In the 2-year outcomes, patients receiving ozanimod had a lower risk of AEs leading to discontinuation, any AEs, herpetic infections, bradycardia and abnormal liver enzymes elevation than patients receiving fingolimod. Regarding efficacy outcomes, no statistically significant differences in ARRs or rates of 3-month and 6-month CDP were found between ozanimod and fingolimod. Of note, the directions and magnitudes of differences in outcomes were generally consistent both before and after matching, indicating that the trial findings were robust to the adjustment for multiple patient characteristics.
The current analysis of pivotal trial data sheds light on the comparative safety and efficacy of ozanimod, an investigational drug and fingolimod in the treatment of RMS. While ozanimod and fingolimod were comparable in terms of effects on the ARR and CDP, ozanimod was associated with significantly lower risk of the safety outcomes currently assessed. In relation to this, it is worth noting that the mechanism by which ozanimod exerts therapeutic effects in MS is unknown but may involve the reduction of lymphocyte migration into the central nervous system. This evidence suggests that ozanimod has a favorable benefit-risk profile compared with fingolimod in terms of first-dose monitoring and safety outcomes for S1P receptor modulation over 1–2 years.
Results of this post hoc analysis should be interpreted in light of several limitations. As this study included comparisons of nonrandomized treatment groups, results may be biased by differences between patient populations that could not be adjusted for, such as the differences in the location of study sites; however, adjustment for observed baseline characteristics minimizes this risk. For the 2-year comparisons, due to lack of a common comparator arm, there is less opportunity to assess confounding bias in the nonanchored based comparison of ozanimod and fingolimod. Some differences in measurement standards between trials existed. For example, the ozanimod trials measured heart rate and BP in the supine position or standing position whereas the fingolimod trials measured patients in the sitting position. Heart rate is commonly lower when measured in the supine position while BP is commonly higher when measured in the supine position. Also, there were differences in the initial dosing regimens between the ozanimod and fingolimod trials; the ozanimod trials used a dose-escalation regimen not present in the fingolimod trials, which could potentially have led to fewer first-dose cardiac AEs in the ozanimod arms. Rates of any AEs should be interpreted with caution when comparing across trials because event ascertainment and reporting may differ, especially for lower-severity events. Given the 2-year follow up data, this analysis could not evaluate the long-term safety or efficacy of these treatments.
Conclusion
In this MAIC analysis of pivotal registration clinical trial data, although ozanimod and fingolimod were comparable in terms of key efficacy outcomes, ozanimod was associated with a more favorable benefit–risk profile compared with fingolimod when considering outcomes of first-dose cardiac monitoring, potential safety outcomes for S1P receptor modulation and key efficacy outcomes over 1–2 years.
What is already known about this subject?
•
Fingolimod is a nonselective sphingosine 1-phosphate (S1P) receptor modulator for the treatment of relapsing multiple sclerosis (RMS).
•
Ozanimod, a selective S1P receptor modulator designed to target only the receptor subtypes S1PR1 and S1PR5, is currently under investigation for the treatment of RMS.
•
The superior efficacy of these two treatments compared with IFN β-1a has been demonstrated in clinical trials.
•
No head-to-head trials directly compare the safety and efficacy of ozanimod versus fingolimod for the treatment of RMS.
What are the new findings?
•
In this indirect comparison across separate clinical trials, ozanimod was associated with significantly lower risks of adverse outcomes during first dose monitoring outcomes and over 1–2 years of follow-up compared with fingolimod.
•
Ozanimod and fingolimod were comparable in terms of reducing annualized relapse rates and the proportion of patients with confirmed disability progression.
•
Overall, ozanimod appears to have a superior benefit–risk profile to fingolimod.
Impact on clinical practice
•
Ozanimod is an investigational drug under review for the treatment of RMS.
•
This evidence will help decision makers to assess the relative clinical value of these therapies.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
All authors were involved in the design and conduction of the study, as well as in drafting the manuscript or revising it critically for intellectual content. All authors had access to the data and interpreted the data.
Financial & competing interests disclosure
Research support was provided by Celgene, a wholly-owned subsidiary of Bristol-Myers Squibb (Summit, NJ, USA). E Swallow, O Patterson-Lomba, L Yin and J Signorovitch are employees of Analysis Group, Inc., which has received consulting fees from Bristol-Myers Squibb. R Mehta, C Pelletier, D Kao, JK Sheffield and T Stonehouse are employees of Bristol-Myers Squibb. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by S Batts, a professional medical writer employed by Analysis Group, Inc. Funding for this assistance was provided by Bristol-Myers Squibb. The authors also received editorial support in the preparation of this article from Peloton Advantage, LLC (Parsippany, NJ, USA), an OPEN Health company, sponsored by Bristol-Myers Squibb, Summit, NJ, USA. The authors, however, directed and are fully responsible for all content and editorial decisions for this article.
Ethical conduct of research
No institutional review was required as this was a post hoc analysis of previously published, de-identified data. This study adhered to the principles outlined in the Declaration of Helsinki.
Data sharing statement
Celgene is committed to responsible and transparent sharing of clinical trial data with patients, healthcare practitioners and independent researchers for the purpose of improving scientific and medical knowledge as well as fostering innovative treatment approaches. For more information, please visit: https://www.celgene.com/research-development/clinical-trials-data-sharing/.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_data.zip)
- Download
- 36.20 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Von Bismarck O, Dankowski T, Ambrosius B et al. Treatment choices and neuropsychological symptoms of a large cohort of early MS. Neurol. Neuroimmunol. Neuroinflamm. 5(3), e446 (2018).
2.
Krieger SC, Cook K, De Nino S, Fletcher M. The topographical model of multiple sclerosis: a dynamic visualization of disease course. Neurol. Neuroimmunol. Neuroinflamm. 3(5), e279 (2016).
3.
Lublin FD, Reingold SC, Cohen JA et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology 83(3), 278–286 (2014).
4.
Olek M, Howard J. Clinical presentation, course, and prognosis of multiple sclerosis in adults. https://www.uptodate.com/contents/clinical-presentation-course-and-prognosis-of-multiple-sclerosis-in-adults
5.
European Medicines Agency. Guideline on clinical investigation of medicinal products for the treatment of multiple sclerosis. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-multiple-sclerosis_en-0.pdf
6.
Lublin FD, Baier M, Cutter G. Effect of relapses on development of residual deficit in multiple sclerosis. Neurology 61(11), 1528–1532 (2003).
7.
Giovannoni G, Butzkueven H, Dhib-Jalbut S et al. Brain health: time matters in multiple sclerosis. Mult. Scler. Relat. Disord. 9(Suppl. 1), S5–S48 (2016).
8.
Ziemssen T, Derfuss T, De Stefano N et al. Optimizing treatment success in multiple sclerosis. J. Neurol. 263(6), 1053–1065 (2016).
9.
Aronson KJ. Quality of life among persons with multiple sclerosis and their caregivers. Neurology 48(1), 74–80 (1997).
10.
Tremlett HL, Luscombe DK, Wiles CM. Prescribing for multiple sclerosis patients in general practice: a case-control study. J. Clin. Pharm. Ther. 26(6), 437–444 (2001).
11.
Gehr S, Kaiser T, Kreutz R, Ludwig W-D, Paul F. Suggestions for improving the design of clinical trials in multiple sclerosis—results of a systematic analysis of completed phase III trials. EPMA J. 10(4), 425–436 (2019).
12.
Finkelsztejn A. Multiple sclerosis: overview of disease-modifying agents. Perspect. Medicin. Chem. 6, 65–72 (2014).
13.
Straus Farber R, Harel A, Lublin F. Novel agents for relapsing forms of multiple sclerosis. Annu. Rev. Med. 67, 309–321 (2016).
14.
Doshi A, Chataway J. Multiple sclerosis, a treatable disease. Clin. Med. (Lond.) 17(6), 530–536 (2017).
15.
Gilenya [package insert]. Novartis Pharmaceuticals Corporation, East Hanover, NJ (2019). https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.com/files/gilenya.pdf
16.
Rasche L, Paul F. Ozanimod for the treatment of relapsing remitting multiple sclerosis. Expert Opin. Pharmacother. 19(18), 2073–2086 (2018).
17.
Cohen JA, Comi G, Selmaj KW et al. Safety and efficacy of ozanimod versus interferon beta-1a in relapsing multiple sclerosis (RADIANCE): a multicentre, randomised, 24-month, phase 3 trial. Lancet Neurol. (2019) (Epub ahead of print).
•• In RADIANCE, a 2-year, Phase III clinical trial of ozanimod versus IFNβ-1a in patients with relapsing multiple sclerosis, ozanimod demonstrates greater efficacy on both MRI and clinical disease measures.
18.
Comi G, Kappos L, Selmaj KW et al. Safety and efficacy of ozanimod versus interferon beta-1a in relapsing multiple sclerosis (SUNBEAM): a multicentre, randomised, minimum 12-month, phase 3 trial. Lancet Neurol. (2019) (Epub ahead of print).
•• In SUNBEAM, a Phase III clinical trial comparing ozanimod versus IFNβ-1a in patients with relapsing multiple sclerosis, ozanimod demonstrates superiority to IFNβ-1a on relapse and MRI end points.
19.
Signorovitch J, Erder MH, Xie J et al. Comparative effectiveness research using matching-adjusted indirect comparison: an application to treatment with guanfacine extended release or atomoxetine in children with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder. Pharmacoepidemiol. Drug Saf. 21(Suppl. 2), 130–137 (2012).
20.
Signorovitch JE, Wu EQ, Yu AP et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics 28(10), 935–945 (2010).
• In the absence of head-to-head trials, matching-adjusted indirect comparisons can be performed. An example applied to psoriasis treatment is explained here.
21.
Fox RJ, Cutter G, Chan A et al. Comparative effectiveness using a matching-adjusted indirect comparison between delayed-release dimethyl fumarate and fingolimod for the treatment of relapsing-remitting multiple sclerosis [abstract PND10]. Value Health 18(7), A750 (2015).
22.
Berardi A, Siddiqui MK, Treharne C, Harty G, Wong SL. Estimating the comparative efficacy of cladribine tablets versus alternative disease modifying treatments in active relapsing-remitting multiple sclerosis: adjusting for patient characteristics using meta-regression and matching-adjusted indirect treatment comparison approaches. Curr. Med. Res. Opin. 35(8), 1371–1378 (2019).
23.
Cohen JA, Comi G, Selmaj KW et al. Ozanimod vs interferon β-1a: clinical and MRI results of RADIANCE part B - a 2-year phase 3 trial in relapsing multiple sclerosis [abstract 280]. Mult. Scler. J. 23(Suppl. 3), 981–982 (2017).
24.
Cree B, Selmaj K, Kopicko J et al. The RADIANCE and SUNBEAM phase 3 studies of ozanimod in relapsing multiple sclerosis: study design and baseline characteristics [abstract]. Neurology 88(Suppl. 16), P6.344 (2017).
25.
Comi G, Kappos L, Selmaj KW et al. Ozanimod demonstrates efficacy and safety in a phase 3 trial of relapsing multiple sclerosis (SUNBEAM) [abstract 232]. Mult. Scler. J. 23(Suppl. 3), 73–74 (2017).
26.
Cohen JA, Barkhof F, Comi G et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N. Engl. J. Med. 362(5), 402–415 (2010).
• A Phase II study in patients with multiple sclerosis that shows the superior efficacy of oral fingolimod with respect to relapse rates and MRI outcomes in patients with multiple sclerosis, as compared with intramuscular IFNβ-1a.
27.
Kappos L, Radue EW, O'connor P et al. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N. Engl. J. Med. 362(5), 387–401 (2010).
• In a 2-year analysis of Phase II and III studies of patients with relapsing-remitting multiple sclerosis, oral fingolimod improved the relapse rate, the risk of disability progression and end points on MRI compared with placebo.
28.
Calabresi PA, Radue EW, Goodin D et al. Safety and efficacy of fingolimod in patients with relapsing-remitting multiple sclerosis (FREEDOMS II): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 13(6), 545–556 (2014).
• A Phase III clinical trial in patients with relapsing-remitting multiple sclerosis, in which fingolimod was associated with reductions in clinical and MRI disease activity compared with placebo.
29.
Dimarco JP, O'connor P, Cohen JA et al. First-dose effects of fingolimod: Pooled safety data from three phase 3 studies. Mult. Scler. Relat. Disord. 3(5), 629–638 (2014).
30.
Polman CH, Reingold SC, Banwell B et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 69(2), 292–302 (2011).
31.
Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33(11), 1444–1452 (1983).
Information & Authors
Information
Published In
Pages: 275 - 285
PubMed: 31948278
Copyright
© 2020 Elyse Swallow. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 13 November 2019
Accepted: 19 December 2019
Published online: 17 January 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative safety and efficacy of ozanimod versus fingolimod for relapsing multiple sclerosis. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0169
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- David T Rubin, Silvio Danese, Hiroshi Nakase, Ryan C Ungaro, Douglas C Wolf, Olga Alekseeva, AnnKatrin Petersen, Zhaohui Liu, Dimpy Mehra, Anjali Jain, Mark T Osterman, Anthony Krakovich, Jon V Riolo, Erik DeBoer, James Appio, Preetika Sinh, Bruce A C Cree, Jeffrey A Cohen, Peter Irving, Integrated long-term safety of 10-year ozanimod treatment: results from clinical trials in patients with moderate-to-severe ulcerative colitis or relapsing multiple sclerosis, Inflammatory Bowel Diseases, 10.1093/ibd/izaf319, (2026).
- Jessica Cooperrider, Jeffrey Lambe, Michelle Chu, Mengke Du, Jennifer Reardon, Burhan Chaudry, Andrew Thorpe, Carrie M. Hersh, Devon Conway, Real-world experience of ozanimod in adults with multiple sclerosis, Neurodegenerative Disease Management, 10.1080/17582024.2026.2622078, 16, 4, (401-409), (2026).
- Qinhui Tang, Xiaowei Tang, Xinyue Hu, Wenmeng Yin, Lian Luo, Yantong Li, Xiaolin Zhong, A real-world data analysis of Ozanimod in the FDA Adverse Event Reporting System (FAERS) database, Medicine, 10.1097/MD.0000000000044535, 104, 37, (e44535), (2025).
- Giorgia Teresa Maniscalco, Maddalena Sparaco, Maria Di Gregorio, Giuseppina Cafasso, Elisabetta Signoriello, Felice Romano, Rosa Iodice, Roberta Fantozzi, Paolo Bellantonio, Aurora Zanghi, Leonardo Sinisi, Alessandro D’Ambrosio, Vincenzo Busillo, Valentina Scarano, Rocco Capuano, Luigi Lavorgna, Michela Williams, Antonio De Martino, Maria Elena Di Battista, Daniele Di Giulio Cesare, Giacomo Lus, Emanuele Cassano, Paola Sofia Di Filippo, Grazia Sibilia, Gianmarco Abbadessa, Vincenzo Andreone, Simona Bonavita, Real-world comparison of lymphopenia profiles in S1P receptor modulators for multiple sclerosis: a multicenter retrospective study, Journal of Neurology, 10.1007/s00415-025-13300-z, 272, 9, (2025).
- Elisabetta Signoriello, Giuseppe Romano, Matteo Foschi, Aurora Zanghì, Emanuele D’Amico, Roberta Fantozzi, Diego Centonze, Giacomo Lus, Switch from fingolimod to ozanimod for safety or intolerance reasons, Therapeutic Advances in Neurological Disorders, 10.1177/17562864251328191, 18, (2025).
- Federica Galota, Simone Marcheselli, Sara De Biasi, Lara Gibellini, Francesca Vitetta, Alessia Fiore, Krzysztof Smolik, Giulia De Napoli, Martina Cardi, Andrea Cossarizza, Diana Ferraro, Impact of High-Efficacy Therapies for Multiple Sclerosis on B Cells, Cells, 10.3390/cells14080606, 14, 8, (606), (2025).
- Nunzia Balzano, Raffaella Di Napoli, Federica Fraenza, Daniele Di Giulio Cesare, Ornella Moreggia, Mirko Cardillo, Cristina Scavone, Giorgia Teresa Maniscalco, Annalisa Capuano, Liberata Sportiello, Lymphopenia associated with sphingosine 1-phosphate receptor modulators (S1PRMs) in multiple sclerosis: analysis of European pharmacovigilance data, Pharmacological Reports, 10.1007/s43440-025-00725-6, 77, 3, (775-788), (2025).
- Ying Li, Jingmin Zhang, Guangrui Yang, Shujie Jiao, Mingyuan Guan, Identifying cardiovascular toxicity associated with sphingosine 1-phosphate receptor modulators: A case-control study based on the FDA adverse event reporting system, International Immunopharmacology, 10.1016/j.intimp.2025.114520, 153, (114520), (2025).
- Nicola Humphry, Ozanimod in Relapsing Multiple Sclerosis: New Insights, American Medical Journal Neurology, 10.33590/neurolamj/NITU6060, (2024).
- Tina Nie, Yahiya Y. Syed, Ozanimod: A Review in Relapsing Forms of Multiple Sclerosis, CNS Drugs, 10.1007/s40263-024-01116-w, 38, 11, (931-941), (2024).
- See more