Intracardiac echocardiography use and outcomes after catheter ablation of ventricular tachycardia
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare outcomes among patients with implantable cardioverter defibrillator/cardiac resynchronization therapy-defibrillator undergoing outpatient ventricular tachycardia (VT) catheter ablation using intracardiac echocardiography (ICE) versus no ICE. Patients & methods: Patients were classified into ICE (n = 1143)/non-ICE (n = 1677) groups based on ICE procedure codes. Patients in each group were propensity matched on study covariates. Survival analyses were used to assess outcomes. To examine residual confounding, falsification outcomes were evaluated. Results: ICE patients had a 24% lower risk of all-cause readmissions, 24% lower risk of cardiovascular-related and 20% lower risk of VT-related readmissions compared with non-ICE patients. Falsification analyses for ICE use association were nonsignificant. Conclusion: Patients with implantable cardioverter defibrillator/cardiac resynchronization therapy-defibrillator undergoing VT ablation with ICE use had significantly lower likelihood of VT-related readmission.
Catheter ablation is an important treatment option for patients with ventricular tachycardia (VT) when antiarrhythmic medications are ineffective or not tolerated [1]. Randomized clinical trials have shown that VT ablation decreases the incidence of implantable cardioverter–defibrillator (ICD) therapy and time to recurrence of VT/ventricular fibrillation [2,3], reduces hospitalization and overall healthcare utilization [4] and reduces a composite incidence of death, VT storm or appropriate ICD shock compared with antiarrhythmic-drug therapy in patients with ischemic cardiomyopathy [5].
Several adjunctive imaging techniques, including intracardiac echocardiography (ICE), have improved the approach to VT ablation. ICE has an important role during VT ablation by providing real-time visualization of cardiac structures [6], detailed imaging of the akinetic and dyskinetic regions [7,8] and rapid identification of intraprocedural complications [9]. In addition, ICE allows for continuous assessment of catheter–tissue contact, which is the key for effective energy delivery, potentially increasing effectiveness and limiting collateral damage [10,11]. A recent heart rhythm society (HRS) consensus document has provided several recommendations for the use of ICE during VT ablation [12]. However, whether ICE use improves outcomes during VT ablation in patients with ICD/cardiac resynchronization therapy-defibrillator (CRT-D) remains unknown.
Patients & methods
Data source
The CMS Medicare Standard Analytic Files (SAF) database, which captures healthcare claims for Medicare enrollees in USA, was used for this study. The database includes information on diagnosis and procedure, date of service and patient demographics.
We limited our analyses to fee-for-service Medicare beneficiaries ≥65 years of age and living in USA. The use of CMS Medicare SAF database was reviewed by the New England Institutional Review Board (IRB) and was determined to be exempt from broad IRB approval, as the database does not allow for identifiable human subjects. All patient records remained deidentified, and study reports contained only aggregate data without individual patient or physician names.
Study population
We searched carrier claims submitted between 1 January 2008 and 31 December 2017 for reports of an outpatient ablation procedure with a primary diagnosis of VT. The first such ablation was classified as the index procedure. Patients were required to have 6-month pre-index continuous enrollment. Study inclusion/exclusion criteria were established to identify patients with structural heart disease and exclude idiopathic VT ablations and therefore we restricted the analysis to patients with an ICD/CRT-D. Patients were required to have procedure codes for ICD/CRT-D device implantation, lead implantation or device follow-up within 6 months before ablation. Patients were also excluded if they were enrolled in Medicare due to disability or had end stage renal disease. Patients were classified into ICE and non-ICE groups based on the presence or absence of procedure codes for ICE during index ablation encounter. Table 1 depicts study attrition based on inclusion and exclusion criteria. Procedure and/or diagnosis codes for key study inclusion factors are listed in Supplementary Material 1.
| Step | Criteria | Sample (N) |
|---|---|---|
| 1 | Number of ablations (primary or secondary) with primary diagnosis of VT between 2008 and 2017 in an outpatient setting | 9942 |
| 2 | Patients with an VT ablation between 2008 and 2017 (Index) | 7129 |
| 3 | Patients ≥65 years | 5792 |
| 4 | Patients with at least 6 months CE before VT ablation (pre-index) | 5635 |
| 5 | Patients who did not receive care outside USA; service is in USA only | 5625 |
| 6 | Patients who did not have ESRD | 5579 |
| 7 | ICD/CRT-D implantation, lead implantation or device follow-up within 6-month pre-index | 2820 ICE Use: 1143 (40.53%) |
| 8 | Trans-septal puncture performed at index (included in subgroup analysis) | 846 ICE Use: 560 (66.19%) |
CE: Continuous enrollment; ESRD: End stage renal disease; ICD/CRT-D: Implantable cardioverter–defibrillator/cardiac resynchronization therapy-defibrillator; ICE: Intracardiac echocardiography; VT: Ventricular tachycardia.
We performed several prespecified subanalyses. We restricted the group of VT ablation patients to those who had transseptal puncture, and compared outcomes between the ICE and non-ICE groups. In addition, because studies have reported a positive correlation between hospital or operator volume and procedural outcomes in several therapeutic areas including catheter ablation [13,14], we attempted to account for potential confounding of procedural volume which might account for associated difference in outcomes with ICE use. When examining the distribution of the number of VT ablation procedures per hospital setting within a 6-month window, the mean distribution was observed to be approximately four. Thus, we performed a sensitivity analysis by restricting the sample of patients to those who had their index ablation at a hospital with at least four VT ablation procedures in a 6-month pre-index period (excluding the index ablation). Lastly, to further attempt to control for unmeasured confounders that could have influenced study results, we did falsification analysis [15]. Specifically, because ICE use would not be expected to influence rates of pneumonia, urinary tract infection (UTI) or hip fracture, we selected these as falsification end points. We compared the rates of 12-month postindex ablation inpatient admission for pneumonia, UTI or hip fracture among patients in the ICE and non-ICE group.
Study covariates
Study characteristics including patient demographics (age at the time of index ablation [categorized as 65–74 years, ≥75 years], gender, race [white, nonwhite]), year of the index procedure, provider region (northeast, north central, west, south) and patient comorbidity status (extended-Charlson comorbidity index score categorized as 0 or 1, 2 or 3, ≥4) [16,17], CHA2DS2-VASc score (categorized as 1, ≥2) and specific comorbidities. The comorbidities evaluated were cardiomyopathy, diabetes, heart failure, hypertension, renal disease, valvular heart disease, prior myocardial infarction, coronary artery disease, peripheral vascular disease, chronic pulmonary disease, liver disease and premature ventricular contractions, as documented during the 6-month pre-index period.
Study outcomes
Outcome measures were assessed in the 12-month period following hospital discharge for the index ablation. These included all-cause inpatient readmission, cardiovascular (CV)-related inpatient readmission, VT-related inpatient readmission and repeat catheter ablation for VT. Incidence of complications including cardiac perforation (cardiac tamponade, pericardiocentesis or hemopericardium), vascular complications and major bleeding within 30 days from index discharge were also assessed and compared between the ICE and non-ICE groups. Complications were assessed during the index admission plus 30-day postindex discharge.
Statistical analysis
A 1:1 propensity score matching (greedy match nearest neighbor matching without replacement with 0.10 caliper width) was performed for patients in the ICE and non-ICE groups. A propensity analysis was performed for the main analysis and additionally for the hospital volume-based sensitivity analysis and for the use of transseptal puncture. Pre- and postmatch balance of the study covariates included in the propensity score model was assessed using standardized mean difference (standardized difference ≥0.10 or ≤-0.10 indicating imbalance).
Time-to-event analysis was performed to compare outcomes between the matched ICE and non-ICE groups. Patients were censored if they died, were lost to follow-up (defined as a gap of >30 days in enrollment) or if they reached the end of the study period (12 months) without the occurrence of study outcomes. Kaplan–Meier survival curves with log-rank test were used to depict bivariate comparison of outcomes between the two groups. A Cox regression model was used for outcomes comparison in the matched groups. Outcomes for patients receiving care within the same hospital could correlate and differ from patients at another hospital. To alleviate the potential effect of hospital-level clustering, we used cox regression analyses with cluster function, wherein hospital clusters were accounted. In addition, any covariates that emerged significantly different postmatching were controlled for in the regression analyses.
For all analyses, a two-sided p < 0.05 was considered to be statistically significant. Analyses were conducted using SAS for Windows, Version 9.4 (SAS Institute Inc., NC, USA).
Results
Study sample
A total of 2820 patients met the study eligibility criteria (ICE group: 1143 [40.53%]; non-ICE group: 1677 [59.47%]). A comparison of the two groups is shown in Table 2. In the prematch sample, most of the patients were 65–74 years of age (mean age: ICE group: 72.59 years; non-ICE group: 73.10 years), male (ICE group: 93.4%; non-ICE group: 91.1%) and white (ICE group: 93.1%; non-ICE group: 91.3%). Based on propensity matching, 2152 patients were included, with 1076 in each group. Examination of standardized differences postmatching indicated an excellent balance between the two groups with regards to study covariates, with no significant differences (Table 2).
| Characteristics | Before matching | After matching | ||||
|---|---|---|---|---|---|---|
| ICE (n = 1143) | Non-ICE (n = 1677) | Std diff. | ICE (n = 1076) | Non-ICE (n = 1076) | Std diff. | |
| Age, n (%) | ||||||
| − Mean (SD) | 72.59 (5.17) | 73.10 (5.52) | -0.09 | 72.68 (5.24) | 72.67 (5.39) | 0.00 |
| − 65 to 74 | 761 (66.58) | 1033 (61.60) | -0.10 | 702 (65.24) | 714 (66.35) | 0.02 |
| − ≥75 | 382 (33.42) | 644 (38.40) | 374 (34.76) | 362 (33.64) | ||
| Gender, n (%) | ||||||
| − Male | 1067 (93.35) | 1528 (91.12) | -0.08 | 1001 (93.03) | 1001 (93.03) | 0.00 |
| Race | ||||||
| − White, n (%) | 1064 (93.09) | 1531 (91.29) | 0.06 | 998 (92.75) | 995 (92.47) | 0.01 |
| Year, n (%) | ||||||
| − 2008 | 20 (1.75) | 59 (3.52) | -0.11 | 20 (1.86) | 11 (1.02) | 0.07 |
| − 2009 | 27 (2.36) | 77 (4.59) | -0.12 | 27 (1.25) | 28 (2.60) | 0.00 |
| − 2010 | 35 (3.06) | 144 (8.59) | -0.23 | 34 (3.16) | 38 (3.53) | -0.02 |
| − 2011 | 53 (4.64) | 137 (8.17) | -0.14 | 53 (2.46) | 49 (4.55) | 0.01 |
| − 2012 | 77 (6.74) | 117 (6.98) | 0.00 | 77 (7.16) | 88 (8.18) | -0.03 |
| − 2013 | 124 (10.85) | 180 (10.73) | 0.00 | 122 (11.34) | 139 (12.92) | -0.04 |
| − 2014 | 187 (16.36) | 190 (11.33) | 0.14 | 177 (16.45) | 174 (16.17) | 0.00 |
| − 2015 | 197 (17.24) | 208 (12.40) | 0.13 | 182 (16.91) | 186 (17.29) | 0.00 |
| − 2016 | 273 (23.88) | 217 (12.94) | 0.28 | 234 (21.75) | 207 (19.24) | 0.06 |
| − 2017 | 150 (13.12) | 348 (20.75) | -0.20 | 150 (13.94) | 156 (14.50) | -0.01 |
| Provider region, n (%) | ||||||
| − Northeast | 278 (24.32) | 426 (25.40) | 0.07 | 158 (14.68) | 155 (14.41) | 0.00 |
| − North Central | 174 (15.22) | 211 (12.58) | -0.02 | 263 (24.44) | 264 (24.54) | 0.00 |
| − South | 451 (39.46) | 699 (41.68) | -0.04 | 431 (40.06) | 438 (40.71) | -0.01 |
| − West | 240 (21.00) | 341 (20.33) | 0.01 | 224 (20.82) | 219 (20.35) | 0.01 |
| CCI Score, n (%) | ||||||
| Mean (SD) | 3.18 (1.59) | 3.16 (1.58) | 0.01 | 3.16 (1.59) | 3.16 (1.60) | 0.00 |
| − 0 or 1 | 162 (14.17) | 239 (14.25) | 0.00 | 154 (14.31) | 158 (14.68) | -0.01 |
| − 2 or 3 | 517 (45.23) | 791 (47.17) | -0.03 | 489 (45.45) | 499 (46.38) | -0.01 |
| − ≥4 | 464 (40.59) | 647 (38.58) | 0.04 | 433 (40.24) | 419 (38.94) | 0.02 |
| CHA2DS2-VASc, n (%) | ||||||
| − Mean (SD) | 3.94 (1.26) | 3.97 (1.27) | -0.02 | 3.93 (1.25) | 3.93 (1.26) | 0.00 |
| − 1 | 17 (1.49) | 16 (0.95) | -0.04 | 15 (1.39) | 14 (1.30) | 0.00 |
| − ≥2 | 1,126 (98.51) | 1,661 (99.05) | 1061 (98.61) | 1062 (98.70) | ||
| Comorbidities, n (%) | ||||||
| − Cardiomyopathy | 464 (40.59) | 791 (47.17) | -0.13 | 454 (42.19) | 466 (43.31) | -0.02 |
| − Diabetes | 410 (35.87) | 570 (33.99) | 0.03 | 380 (35.32) | 372 (34.57) | 0.01 |
| − Heart failure | 972 (85.04) | 1431 (85.33) | 0.00 | 911 (84.67) | 916 (85.13) | -0.01 |
| − Hypertension | 1005 (87.93) | 1446 (86.23) | 0.05 | 941 (87.45) | 942 (87.55) | 0.00 |
| − Renal disease | 301 (26.33) | 493 (29.40) | -0.06 | 290 (26.95) | 292 (27.14) | 0.00 |
| − Valvular disease | 361 (31.58) | 508 (30.29) | 0.02 | 339 (31.51) | 332 (30.86) | 0.01 |
| − Myocardial infarction | 692 (60.54) | 966 (57.60) | 0.05 | 650 (60.41) | 641 (59.57) | 0.01 |
| − Coronary artery disease | 1030 (90.11) | 1488 (88.73) | 0.04 | 966 (89.78) | 967 (89.87) | 0.00 |
| − Peripheral vascular disease | 618 (54.07) | 797 (47.53) | 0.13 | 564 (52.42) | 546 (50.74) | 0.03 |
| − Chronic pulmonary disease | 305 (26.68) | 511 (30.47) | -0.08 | 299 (27.79) | 294 (27.32) | 0.01 |
| − Liver disease | 36 (3.15) | 60 (3.58) | -0.02 | 35 (3.25) | 38 (3.53) | -0.01 |
| − Premature ventricular contractions | 217 (18.99) | 276 (16.46) | 0.06 | 198 (18.40) | 189 (17.57) | 0.02 |
CCI: Charlson comorbidity index; ICE: Intracardiac echocardiography; SD: Standard deviation; Std diff.: Standard difference.
Use of ICE & rates of readmission & repeat ablation
Time-to-event analysis showed that the likelihood of 12-month all-cause readmission (44.89 vs 52.51%; p < 0.0001), CV-related readmission (33.74 vs 40.15%; p = 0.0001) and VT-related readmission (19.33 vs 21.84%; p = 0.0263) postindex ablation discharge were significantly lower in the ICE group compared with the non-ICE group. The difference in rates of repeat catheter ablation for VT was not statistically significant between the ICE and non-ICE groups (5.02 vs 4.65%; p = 0.9405; Figure 1).
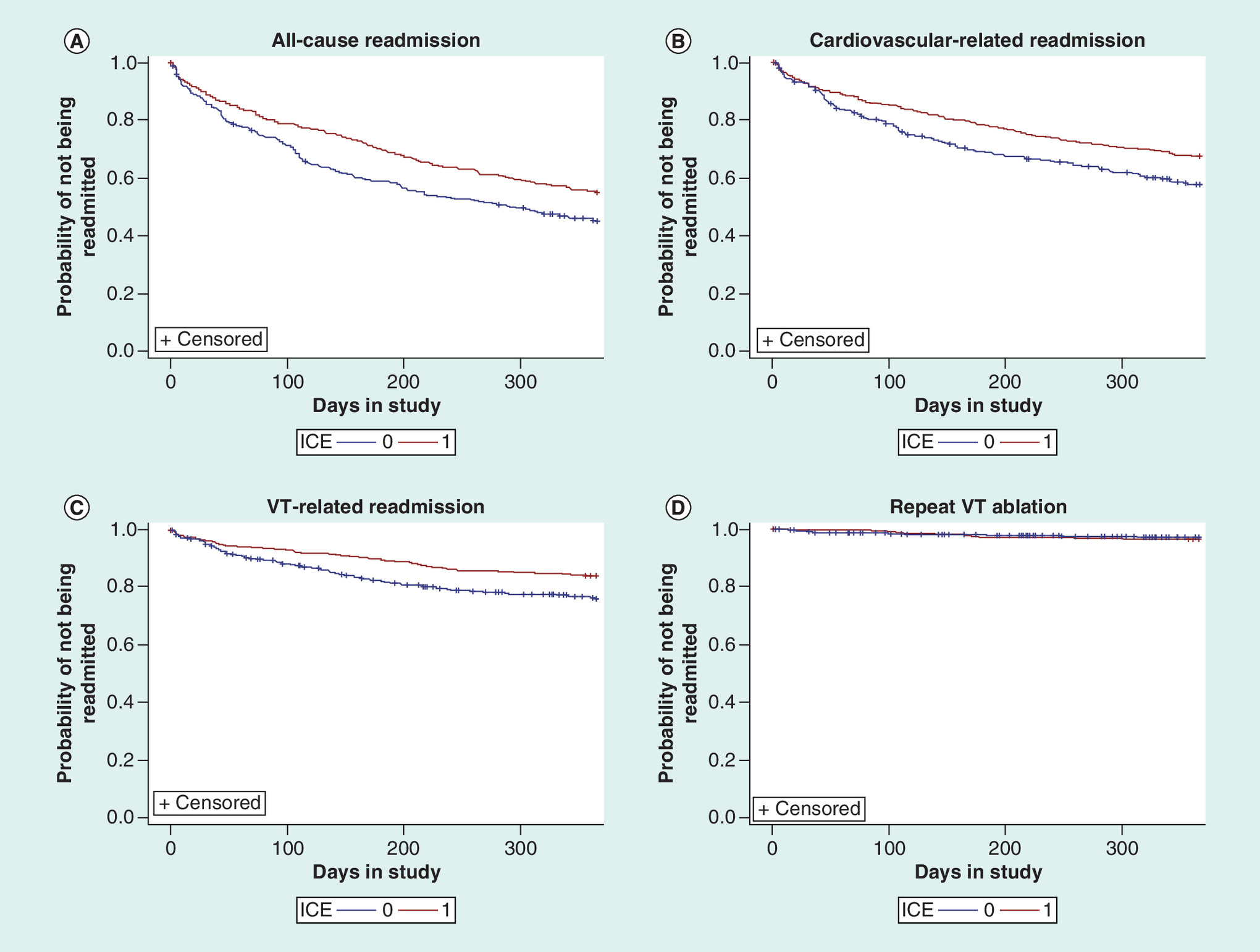
Figure 1. Kaplan–Meier survival curves for time to readmission (0–12 months) among elderly patients undergoing ventricular tachycardia ablation.
(A) All-cause readmission. (B) Cardiovascular-related readmission. (C) VT-related readmission. (D) Repeat VT ablation.
ICE: Intracardiac echocardiography; VT: Ventricular tachycardia.
Similar to the time-to-event analysis, Cox regression analysis showed that patients in the ICE group had a 24% lower risk of all-cause readmission (hazard ratio [HR]: 0.76; 95% CI: 0.67–0.86), 24% lower risk of CV-related readmission (HR: 0.76; 95% CI: 0.66–0.87) and 20% lower risk of VT-related readmission (HR: 0.81; 95% CI: 0.67–0.97) compared with the non-ICE group. Again, the risk of repeat catheter ablation for VT was not statistically different between the two groups (HR: 0.99; 95% CI: 0.67–1.44).
Use of ICE & rates of complications
Rates of complications were generally low, and no significant difference in ICE and non-ICE group was observed for cardiac perforation (0.19 vs 0.46%; p = 0.2534), vascular complications (1.30 vs 0.86%; p = 0.2972) and major bleeding (3.53 vs 3.35%; p = 0.8325).
Consistent with bivariate results, no significant difference in 30-day complications were observed including cardiac perforation (HR: 0.40; 95% CI: 0.07–2.04), vascular complication (HR: 1.55; 95% CI: 0.67–3.59) or major bleeding (HR: 1.05; 95% CI: 0.66–1.65) was observed between the ICE and non-ICE groups in the cox regression model.
Transseptal puncture subgroup analysis
A total of 846 patients (Table 1, step 8) met eligibility criteria for the subgroup analysis of patients who had transseptal puncture during their index ablation procedure (ICE group: 560 [66.19%], non-ICE group: 286 [33.81%]). Propensity score matching led to 462 patients (231 each in the ICE and non-ICE groups). Examination of standardized differences (Table 3) depicted a generally good balance between the two matched groups except for differential in CHA2DS2-VASc (standardized difference = 0.11). Given the significant difference in mean CHA2DS2-VASc score in the postmatch ICE and non-ICE groups, we controlled for CHA2DS2-VASc score in our regression analysis.
| Characteristics | Before matching | After matching | ||||
|---|---|---|---|---|---|---|
| ICE (n = 560) | Non-ICE (n = 286) | Std diff. | ICE (n = 231) | Non-ICE (n = 231) | Std diff. | |
| Age, n (%) | ||||||
| − Mean (SD) | 72.83 (5.19) | 73.76 (5.76) | -0.16 | 73.86 (5.20) | 73.76 (5.96) | 0.01 |
| − 65 to 74 | 371 (66.25) | 165 (57.69) | -0.17 | 130 (56.28) | 137 (59.31) | 0.06 |
| − ≥75 | 189 (33.75) | 121 (42.31) | 101 (43.72) | 94 (40.69) | ||
| Gender, n (%) | ||||||
| − Male | 533 (95.18) | 260 (90.91) | -0.16 | 16 (6.93) | 18 (7.79) | -0.03 |
| Race, n (%) | ||||||
| − White | 528 (94.29) | 268 (93.71) | 0.02 | 220 (95.24) | 216 (93.51) | 0.07 |
| Year, n (%) | ||||||
| − 2011 | 28 (5.00) | 15 (5.24) | -0.01 | 17 (7.36) | 15 (6.49) | 0.03 |
| − 2012 | 45 (8.04) | 20 (6.99) | 0.03 | 18 (7.79) | 20 (8.66) | -0.03 |
| − 2013 | 75 (13.39) | 24 (8.39) | 0.16 | 22 (9.52) | 24 (10.39) | -0.02 |
| − 2014 | 92 (16.43) | 34 (11.89) | 0.13 | 38 (16.45) | 34 (14.72) | 0.04 |
| − 2015 | 100 (17.86) | 40 (13.99) | 0.10 | 38 (16.45) | 39 (16.88) | -0.01 |
| − 2016 | 153 (27.32) | 38 (13.29) | 0.35 | 39 (16.88) | 38 (16.45) | 0.01 |
| − 2017 | 67 (11.96) | 115 (40.21) | -0.67 | 59 (25.54) | 61 (26.41) | -0.01 |
| Provider region, n (%) | ||||||
| − Northeast | 86 (15.36) | 38 (13.29) | 0.05 | 28 (12.12) | 33 (14.29) | -0.06 |
| − North Central | 135 (24.11) | 69 (24.13) | 0.00 | 54 (23.38) | 56 (24.24) | -0.02 |
| − South | 220 (39.29) | 119 (41.61) | -0.04 | 99 (42.86) | 95 (41.13) | 0.03 |
| − West | 119 (21.25) | 60 (20.98) | 0.00 | 50 (21.65) | 47 (20.35) | 0.03 |
| CCI Score, n (%) | ||||||
| − Mean (SD) | 3.40 (1.57) | 3.56 (1.57) | -0.09 | 3.52 (1.55) | 3.49 (1.60) | 0.01 |
| − 0 or 1 | 59 (10.54) | 22 (7.69) | 0.09 | 19 (8.23) | 19 (8.23) | 0 |
| − 2 or 3 | 245 (43.75) | 131 (45.80) | -0.04 | 103 (44.59) | 109 (47.19) | -0.05 |
| − ≥4 | 256 (45.71) | 133 (46.50) | -0.01 | 109 (47.19) | 103 (44.59) | 0.05 |
| CHA2DS2-VASc, n (%) | ||||||
| Mean (SD) | 4.05 (1.30) | 4.15 (1.21) | -0.08 | 4.26 (1.28) | 4.11 (1.16) | 0.11 |
| − 1 | † | † | † | † | † | † |
| ≥2 | † | † | † | † | ||
| Comorbidities, n (%) | ||||||
| − Cardiomyopathy | 207 (36.96) | 124 (43.36) | -0.13 | 94 (40.69) | 101 (43.72) | -0.06 |
| − Diabetes | 212 (37.86) | 97 (33.92) | 0.08 | 87 (37.66) | 77 (33.33) | 0.09 |
| − Heart failure | 477 (85.18) | 257 (89.86) | -0.14 | 204 (88.31) | 205 (88.74) | -0.01 |
| − Hypertension | 503 (89.82) | 254 (88.81) | 0.03 | 206 (89.18) | 202 (87.45) | 0.05 |
| − Renal disease | 162 (28.93) | 105 (36.71) | -0.16 | 79 (34.20) | 80 (34.63) | 0.00 |
| − Valvular disease | 194 (34.64) | 107 (37.41) | -0.05 | 94 (40.69) | 88 (38.10) | 0.05 |
| − Myocardial infarction | 372 (66.43) | 168 (58.74) | 0.15 | 137 (59.31) | 138 (59.74) | 0.00 |
| − Coronary artery disease | 531 (94.82) | 264 (92.31) | 0.10 | 217 (93.94) | 217 (93.94) | 0.00 |
| − Peripheral vascular disease | 334 (59.64) | 189 (66.08) | -0.13 | 143 (61.90) | 141 (61.04) | 0.01 |
| − Chronic pulmonary disease | 164 (29.29) | 92 (32.17) | -0.06 | 76 (32.90) | 78 (33.77) | -0.01 |
| − Liver disease | 17 (3.04) | 11 (3.85) | -0.04 | 11 (4.76) | † | 0.02 |
| − Premature ventricular contractions | 98 (17.50) | 38 (13.29) | 0.11 | 43 (18.61) | 35 (15.15) | 0.09 |
†
Numbers are suppressed as cell size is less than 11 as per the Centers for Medicare and Medicaid data reporting requirements.
CCI: Charlson comorbidity index; ICE: Intracardiac echocardiography; SD: Standard deviation; Std diff.: Standard difference.
Consistent with our findings for the overall cohort, VT ablation patients who had transseptal puncture performed with ICE, as depicted in Figure 2, had significantly lower rates of 12-month all-cause inpatient readmissions (45.89 vs 63.63%; p < 0.0001), CV-related readmissions (32.90 vs 53.25%; p < 0.0001) and VT-related readmissions (15.15 vs 26.84%; p < 0.0001) compared with transseptal puncture without ICE. No significant difference in rate of 12-month repeat VT ablation was observed between the ICE and non-ICE groups (3.46 vs 3.46%; p = 0.5917).
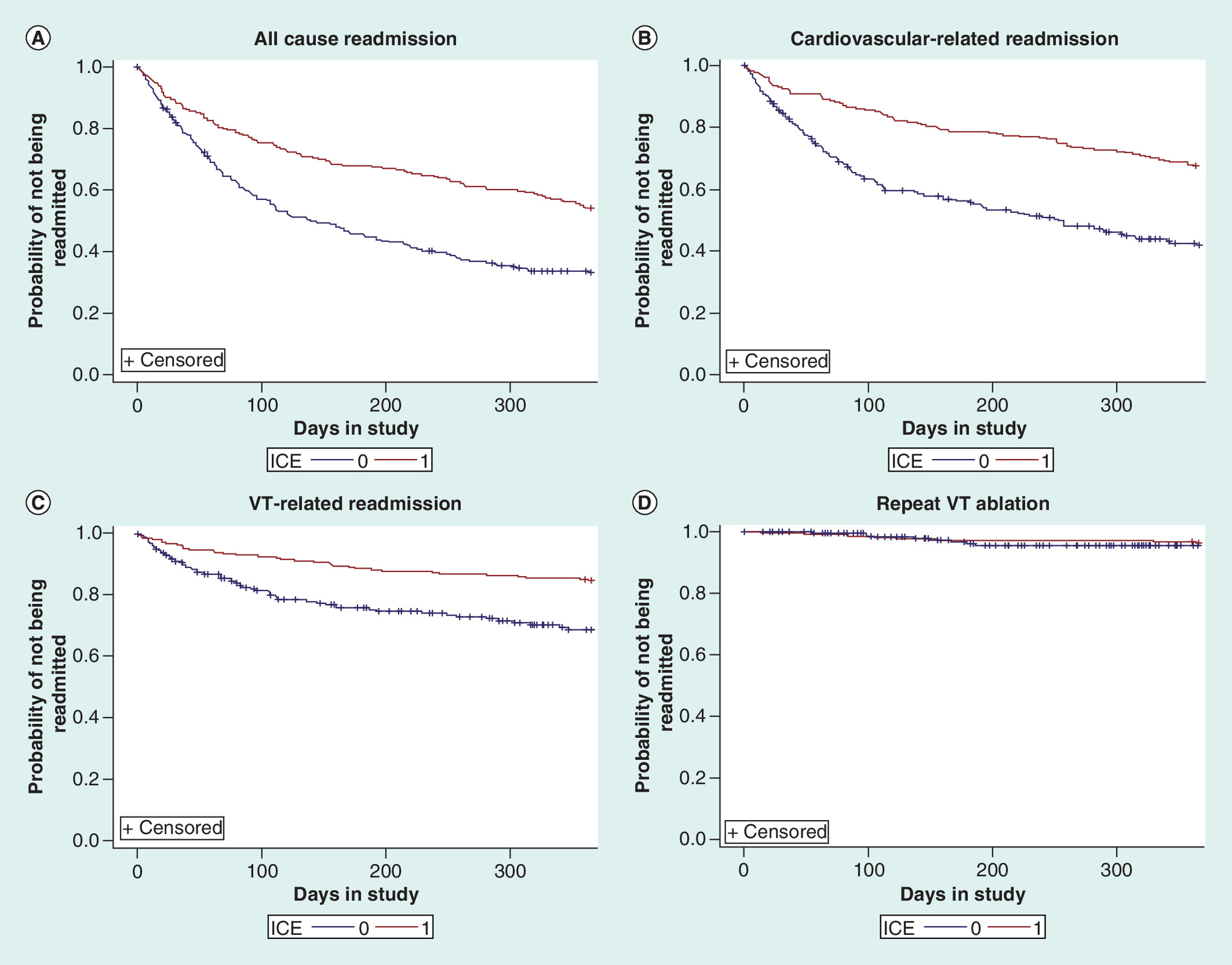
Figure 2. Kaplan–Meier survival curves for time to readmission (0–12 months) among elderly patients undergoing ventricular tachycardia ablation with transseptal puncture.
(A) All-cause readmission. (B) Cardiovascular-related readmission. (C) VT-related readmission. (D) Repeat VT ablation.
ICE: Intracardiac echocardiography; VT: Ventricular tachycardia.
Sensitivity analysis
When limiting the patient sample by hospital volume (i.e., restricting to patients who had index VT ablation at a hospital above the mean number of VT ablation procedures in the 6-month pre-index period), 1029 patients were identified (ICE group: 474; non-ICE group: 555). When matched on study covariates, 714 patients were included, with 357 each in the ICE and non-ICE groups. Pre- and postmatch characteristics are listed in Supplementary Table 1. The Kaplan–Meier survival curves for 12-month inpatient readmission outcomes (Supplementary Figure 1) showed that patients who had VT ablation with ICE had a significantly lower rate of all-cause readmission (44.82 vs 53.50%; p = 0.0041), CV-related readmission (32.21 vs 40.34%; p = 0.0056) and VT-related readmission (15.69 vs 22.13%; p = 0.0074). No significant difference in the rate of 12-month repeat VT ablation (3.36 vs 2.52%; p = 0.6396) was observed. In addition, there was no significant difference observed in the 30-day complications including cardiac perforation (0.00 vs 0.28%; p = 0.3153), vascular complications (0.56 vs 1.40%; p = 0.2541) and major bleeding (4.20 vs 3.92%; p = 0.8712) between volume-based matched ICE and non-ICE groups.
Falsification analysis
When comparing the rates of 12-month postindex ablation inpatient admission rate between the ICE and non-ICE group for pneumonia (2.42 vs 2.14%; p = 0.6646), UTI (0.56 vs 0.46%; p = 0.7624) and hip fracture (0.37 vs 0.46%; p = 0.7384), respectively, among propensity matched patients in the main analysis (1076 each in the ICE and non-ICE groups), no significant difference emerged.
Discussion
In this study of Medicare fee-for-service patients undergoing VT ablation, use of ICE was associated with lower likelihood of 12-month all-cause, CV-related and VT-related readmission compared with those who had ablation without ICE. The results were consistent when we controlled for potential influence of hospital volume. To the best of our knowledge, this is the first study to examine outcomes including readmissions, rates of repeat ablation and complications associated with ICE use during VT ablation procedures in a large administrative database.
ICE plays an important role during VT ablation procedures by providing real-time intraprocedural visualization of the catheter–tissue interface and monitoring for complications. However, there is limited evidence demonstrating improved outcomes associated with ICE use with VT ablation. ICE is increasingly being utilized during many types of cardiac procedures, including ablation of atrial and ventricular arrhythmias [10,18]. A few studies have demonstrated improvement in outcomes and reduction in complications associated with ICE use with other ablation procedures, mostly ablation for atrial fibrillation. In a Medicare dataset of patients undergoing AF ablation, ICE use was associated with lower rates (HR: 0.68; 95% CI: 0.57–0.82) of repeat ablation at 6 months associated with ICE use [19]. Another report from a medium-volume training center, which included some patients undergoing VT ablation, reported the benefit of ICE for optimization of transseptal puncture and early detection of cardiac tamponade, as well as enabling more accurate radiofrequency (RF) catheter visualization and stability during the delivery of RF energy [20]. Most of the evidence supporting ICE use is based on results from single-center settings, which limits their generalizability [21].
In our study, ICE use was associated with significant reduction in 12-month all-cause, CV-related and VT-related readmission. These improvements are presumably due to improved efficacy of the ablation procedure with the visualization afforded due to ICE use. We did not observe significant difference in VT-related repeat ablation in any of our analysis sample. The results were consistent when we controlled for potential influence of hospital volume. Further research in a broader patient sample across all age groups is needed to better understand the role of ICE in reducing repeat ablation.
In addition to improved efficacy, ICE has the potential to reduce the rate of complications particularly related to cardiac tamponade related to transseptal puncture, an approach that is increasingly being used for ablation of VT originating from the left ventricle. However, in our study, we did not observe any difference in the rates of complications in the overall cohort or in the predefined subgroup analysis of VT ablation patients who had a transseptal puncture. It is worth noting that the overall rate of complications was generally low, reflecting the overall safety of VT ablation. Given the low rate of complications, this study was likely underpowered to detect a statistical difference. Although it has been suggested that the use of ICE could potentially increase the risk of vascular access site complications due to the need for additional femoral venous access [19], it is reassuring that we did not observe any significant difference in vascular complications and major bleeding among patients undergoing ablation with or without ICE use.
Limitations
This study is subject to limitations inherent to all claims-based studies, including unidentified confounders, coding errors and reporting bias. While our analyses employed propensity score matching to minimize the influence of potential measured confounders, we cannot exclude the possibility of residual or unmeasured confounding. We tested the robustness of our results by doing falsification analysis, wherein we observed no difference in ICE and non-ICE group on end points including 12-month inpatient readmission associated with pneumonia, UTI and hip fracture, respectively. We attempted to address one important potential source of confounding, ICE as a marker of more experienced operators or ablation centers, by controlling for hospital and operator volume in the sensitivity analysis, which did not change the findings. Additionally, the lack of granularity in administrative data prevents assessment of important clinical and procedural characteristics, including VT mechanism and substrate, cardiac site of the VT origin, echocardiographic parameters such left ventricular ejection fraction and procedural equipment such as specific ablation catheter or approach. Though we studied outcomes among VT patients undergoing transseptal puncture, we could not restrict our analysis specifically to those who had transaortic retrograde VT ablation. It should be noted though that our sample consisted of elderly patients in whom retrograde transaortic approach may be contraindicated [22]. The influence of these variables on the studied outcomes could not be estimated. Moreover, information on drug use including oral anticoagulants and anti-arrhythmic drugs was also not available.
We restricted our analysis to patients who were identified in CMS Medicare outpatient SAF, and did not consider those in the CMS Medicare inpatient SAF file. It should be noted that in the context of CMS Medicare, outpatient may not necessarily reflect same day discharge, and could include patients who may have stayed overnight in a hospital. The reason we restricted our analysis to the former setting was due to the undercoding of ICE codes in CMS SAF inpatient data. In our feasibility work, we observed ICE use to be approximately 14% among VT ablation patients identified in CMS SAF inpatient file, which was considerably lower than ICE use observed for VT ablation among patients in the CMS Medicare outpatient file. Further, we looked at ICE use among elderly patients who had undergone VT ablation in an inpatient setting in another dataset (IBM MarketScan Medicare Supplemental) and found the rate (∼45%) to be substantially higher as well as compared with the rate in CMS SAF inpatient file. As our study focused on patients aged 65 years and above enrolled in Medicare fee-for-service payment system who had VT ablation in an outpatient setting, our results may have limited generalizability to other patient populations, such as younger patients or inpatients.
Conclusion
Using a nationally representative dataset of elderly patients in USA, this study compared outcomes including readmission, repeat ablation and complications among patients undergoing VT ablation with versus without ICE guidance. Our results showed a significantly lower risk of readmissions (all-cause, CV-related and VT-related) associated with ICE use. No significant difference in repeat ablation and complications was observed by ICE use status. Study results were consistent across different analysis approaches, and together with results from falsification analysis, highlight the role of ICE in improving outcomes. Our results based on examination of real-world observational data suggest improved outcomes associated with ICE use; however, further research is needed to better understand the influence of ICE use on outcomes during VT ablation. Though we used propensity matched technique to better match the patients in our two groups, unmeasured confounders could still have influenced our study results, as also stated in the limitation section. If feasible, randomized controlled trials could be conducted to better understand the role ICE plays in influencing outcomes among patients undergoing VT ablation. Together with contact force RF catheter and 3D electro-anatomical mapping, ICE use has the potential to improve patient outcomes significantly, while at the same time reducing the need for fluoroscopy and the radiation exposure associated with fluoroscopy for both patients and healthcare professionals.
•
Real-time visualization of cardiac anatomy can be achieved during ventricular tachycardia (VT) ablation procedures using intracardiac echocardiography (ICE).
•
This study used an observational health claims analysis to compare outcomes among patients with implantable cardioverter defibrillator/cardiac resynchronization therapy-defibrillator undergoing VT ablation using ICE versus no ICE.
•
Patients with ICE use had a 24% lower risk of all-cause readmissions at 1 year, 24% lower risk of cardiovascular-related readmission and 20% lower risk of VT-related readmissions compared with non-ICE patients.
•
Given the patient and physician benefits associated with ICE, its adoption will be critical in guiding the continuous improvements in the field of cardiac ablation and minimizing radiation exposure hazard.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
ME Field, L Goldstein, SHY Lee, I Kalsekar and R Khanna contributed to the conception and design of the study. The collection and assembly of data was done by C Wong, I Kalsekar and R Khanna. Data analysis and interpretation was done by ME Field, L Goldstein, SHY Lee, I Kalsekar, C Wong and R Khanna. All the authors contributed to manuscript writing and the final approval of the manuscript.
Acknowledgments
The authors wish to acknowledge P Pandey for his editorial assistance.
Financial & competing interests disclosure
This study was sponsored by Johnson and Johnson. ME Field received research support from Johnson and Johnson, Boston Scientific and Medtronic. MR Gold received research grants from and is a consultant to Boston Scientific and Medtronic. JR Winterfield received research support from Abbott, Biosense Webster, and is a consultant to Abbott, Biosense Webster, and Acutus. MR Reynolds is a consultant to Medtronic and Abbott. L Goldstein, SHY Lee, I Kalsekar, C Wong and R Khanna are employees of Johnson and Johnson. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Third party editorial assistance under guidance of R Khanna was provided by P Pandey of SIRO ClinPharm Pvt Ltd and was funded by Biosense Webster.
Ethical conduct of research
The study protocol was reviewed by New England Institutional Review Board (IRB) and determined to be exempt from broad IRB approval, as the study did not involve identifiable human subjects.
Supplementary Material
References
Papers of special note have been highlighted as: • of interest
1.
Al-Khatib SM, Stevenson WG, Ackerman MJ et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation 138(13), e272–e391 (2018).
2.
Reddy VY, Reynolds MR, Neuzil P et al. Prophylactic catheter ablation for the prevention of defibrillator therapy. N. Engl. J. Med. 357(26), 2657–2665 (2007).
3.
Kuck KH, Schaumann A, Eckardt L et al. Catheter ablation of stable ventricular tachycardia before defibrillator implantation in patients with coronary heart disease (VTACH): a multicentre randomised controlled trial. Lancet 375(9708), 31–40 (2010).
• This multicenter study shows that prophylactic catheter ablation before implantation of a cardioverter defibrillator may prolong time to recurrence of ventricular tachycardia (VT).
4.
Winterfield JR, Kent AR, Karst E et al. Impact of ventricular tachycardia ablation on health care utilization. Heart Rhythm 15(3), 355–362 (2018).
• This retrospective study demonstrated that catheter ablation seems to reduce hospitalization and overall healthcare utilizations in VT patients with implantable cardioverter defibrillator/cardiac resynchronization therapy-defibrillator.
5.
Sapp JL, Wells GA, Parkash R et al. Ventricular tachycardia ablation versus escalation of antiarrhythmic drugs. N. Engl. J. Med. 375(2), 111–121 (2016).
• This randomized study shows that catheter ablation was associated with a significantly lower rate of death, VT storm or appropriate implantable cardioverter defibrillator shock among with ischemic cardiomyopathy and cardioverter defibrillator who were refrctory to antiarrythmic drug therapy.
6.
Jongbloed MR, Bax JJ, Van Der Burg AE, Van Der Wall EE, Schalij MJ. Radiofrequency catheter ablation of ventricular tachycardia guided by intracardiac echocardiography. Eur. J. Echocardiogr. 5(1), 34–40 (2004).
7.
Bala R, Ren JF, Hutchinson MD et al. Assessing epicardial substrate using intracardiac echocardiography during VT ablation. Circ. Arrhythm. Electrophysiol. 4(5), 667–673 (2011).
8.
Callans DJ, Ren JF, Michele J, Marchlinski FE, Dillon SM. Electroanatomic left ventricular mapping in the porcine model of healed anterior myocardial infarction. Correlation with intracardiac echocardiography and pathological analysis. Circulation 100(16), 1744–1750 (1999).
9.
Ren JF, Marchlinski FE. Early detection of iatrogenic pericardial effusion: importance of intracardiac echocardiography. JACC Cardiovasc. Interv. 3(1), 127 (2010).
10.
Enriquez A, Saenz LC, Rosso R et al. Use of intracardiac echocardiography in interventional cardiology: working with the anatomy rather than fighting it. Circulation 137(21), 2278–2294 (2018).
• This review article provides technical details about intracardiac echocardiography.
11.
Kalman JM, Fitzpatrick AP, Olgin JE et al. Biophysical characteristics of radiofrequency lesion formation in vivo: dynamics of catheter tip-tissue contact evaluated by intracardiac echocardiography. Am. Heart J. 133(1), 8–18 (1997).
12.
Cronin EM, Bogun FM, Maury P et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. Europace 21(8), 1143–1144 (2019).
13.
Katz DF, Turakhia MP, Sauer WH et al. Safety of ventricular tachycardia ablation in clinical practice: findings from 9699 hospital discharge records. Circ. Arrhythm. Electrophysiol. 8(2), 362–370 (2015).
14.
Deshmukh A, Patel NJ, Pant S et al. In-hospital complications associated with catheter ablation of atrial fibrillation in the United States between 2000 and 2010: analysis of 93 801 procedures. Circulation 128(19), 2104–2112 (2013).
15.
Prasad V, Jena AB. Prespecified falsification end points: can they validate true observational associations? JAMA 309(3), 241–242 (2013).
16.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 45(6), 613–619 (1992).
17.
Quan H, Li B, Couris CM et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
18.
Vitulano N, Pazzano V, Pelargonio G, Narducci ML. Technology update: intracardiac echocardiography – a review of the literature. Med. Devices (Auckl.) 8, 231–239 (2015).
19.
Steinberg BA, Hammill BG, Daubert JP et al. Periprocedural imaging and outcomes after catheter ablation of atrial fibrillation. Heart 100(23), 1871–1877 (2014).
20.
Filgueiras-Rama D, De Torres-Alba F, Castrejon-Castrejon S et al. Utility of intracardiac echocardiography for catheter ablation of complex cardiac arrhythmias in a medium-volume training center. Echocardiography 32(4), 660–670 (2015).
• A prospective study that shows that use of intracardiac echocardiography during abalation of complex cardiac substrate may decrease complications and increase accuracy.
21.
Sharma PS, Padala SK, Gunda S, Koneru JN, Ellenbogen KA. Vascular complications during catheter ablation of cardiac arrhythmias: a comparison between vascular ultrasound guided access and conventional vascular access. J. Cardiovasc. Electrophysiol. 27(10), 1160–1166 (2016).
22.
Pluta S, Lenarczyk R, Pruszkowska-Skrzep P et al. Transseptal versus transaortic approach for radiofrequency ablation in patients with cardioverter–defibrillator and electrical storm. J. Intervent. Cardiac Electrophysiol. 28(1), 45–50 (2010).
Information & Authors
Information
Published In
Pages: 375 - 385
PubMed: 32134325
Copyright
© 2020 Future Medicine Ltd.
History
Received: 24 October 2019
Accepted: 8 January 2020
Published online: 5 March 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Intracardiac echocardiography use and outcomes after catheter ablation of ventricular tachycardia. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0156
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Devi Nair, Jeffrey Winterfield, Jonathan C. Hsu, Rakesh Gopinathannair, Larry Chinitz, Naga Venkata K. Pothineni, Frederick T. Han, Bishnu P. Dhakal, Chirag Barbhaiya, Amish S. Dave, Fermin Garcia, Matthew C. Hyman, Travis Dahlen, Kristi Tanouye, Jason Yao, Shubhadarshini Pawar, Judith Buckland, Anna Gilgur, Raphael Elspas, Aakriti Gupta, Roman A. Sandler, Joseph Z. Sokol, Accuracy of a Deep Learning Model in Intracardiac Echocardiography, JACC: Advances, 10.1016/j.jacadv.2026.102867, 5, 7, (102867), (2026).
- Albert J. Rogers, Olga Reynbakh, Adnan Ahmed, Mina K. Chung, Rishi Charate, Hirad Yarmohammadi, Rakesh Gopinathannair, Hassan Khan, Dhanunjaya Lakkireddy, Miguel Leal, Uma Srivatsa, Natalia Trayanova, Elaine Y. Wan, Cardiovascular imaging techniques for electrophysiologists, Nature Cardiovascular Research, 10.1038/s44161-025-00648-8, 4, 5, (514-525), (2025).
- Piotr Gardziejczyk, Roman Piotrowski, Tomasz Kryński, Agnieszka Sikorska, Piotr Kułakowski, Jakub Baran, Bipolar catheter ablation with dedicated radiofrequency system for highly refractory ventricular arrhythmia—Does the rate of success depend on arrhythmia origin?, Journal of Cardiovascular Electrophysiology, 10.1111/jce.16186, 35, 4, (667-674), (2024).
- Auras R. Atreya, Sachin D. Yalagudri, Muthiah Subramanian, Vickram Vignesh Rangaswamy, Daljeet Kaur Saggu, Calambur Narasimhan, Best Practices for the Catheter Ablation of Ventricular Arrhythmias, Cardiac Electrophysiology Clinics, 10.1016/j.ccep.2022.08.007, 14, 4, (571-607), (2022).
- Dimitrios Asvestas, Theodoros Xenos, Stylianos Tzeis, The contribution of intracardiac echocardiography in catheter ablation of ventricular arrhythmias, Reviews in Cardiovascular Medicine, 10.31083/j.rcm2301025, 23, 1, (2022).
- Richard G. Bennett, Timothy Campbell, Ashish Sood, Ashwin Bhaskaran, Kasun De Silva, Lloyd Davis, Pierre Qian, Gopal Sivagangabalan, Mark J. Cooper, Clara K. Chow, Aravinda Thiagalingam, A. Robert Denniss, Stuart P. Thomas, Eddy Kizana, Saurabh Kumar, Remote magnetic navigation compared to contemporary manual techniques for the catheter ablation of ventricular arrhythmias in structural heart disease, Heliyon, 10.1016/j.heliyon.2021.e08538, 7, 12, (e08538), (2021).
- Richard Bennett, Timothy Campbell, Yasuhito Kotake, Samual Turnbull, Ashwin Bhaskaran, Kasun De Silva, Geoffrey Lee, Jonathan Kalman, Saurabh Kumar, Catheter ablation of idiopathic outflow tract ventricular arrhythmias with low intraprocedural burden guided by pace mapping, Heart Rhythm O2, 10.1016/j.hroo.2021.05.008, 2, 4, (355-364), (2021).
- Pierre C. Qian, Usha B. Tedrow, Intracardiac Echocardiography to Guide Catheter Ablation of Ventricular Arrhythmias in Ischemic Cardiomyopathy, Cardiac Electrophysiology Clinics, 10.1016/j.ccep.2021.02.002, 13, 2, (285-292), (2021).